
Abstract
Background
Over decades, improvements in presymptomatic screening and awareness of surgical benefits have changed the presentation and management of primary hyperparathyroidism (PHPT). Unrecognized multiglandular disease (MGD) remains a major cause of operative failure. We hypothesized that during parathyroid surgery the initial finding of a mildly enlarged gland is now frequent and predicts both MGD and failure.
Methods
A prospective database was queried to examine the outcomes of initial exploration for sporadic PHPT using intraoperative PTH monitoring (IOPTH) over 15 years. All patients had follow-up ≥6 months (mean = 1.8 years). Cure was defined by normocalcemia at 6 months and microadenoma by resected weight of <200 mg.
Results
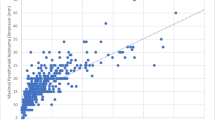
Of the 1,150 patients, 98.9 % were cured and 15 % had MGD. The highest preoperative calcium level decreased over time (p < 0.001) and varied directly with adenoma weight (p < 0.001). Over time, single adenoma weight dropped by half (p = 0.002) and microadenoma was increasingly common (p < 0.01). MGD risk varied inversely with weight of first resected abnormal gland. Microadenoma required bilateral exploration more often than macroadenoma (48 vs. 18 %, p < 0.01). When at exploration the first resected gland was <200 mg, the rates of MGD (40 vs. 11 %, p = 0.001), inadequate initial IOPTH drop (67 vs. 79 %, p = 0.002), operative failure (6.6 vs. 0.7 %, p < 0.001), and long-term recurrence (1.6 vs. 0.3 %, p = 0.007) were higher.
Conclusions
Single parathyroid adenomas are smaller than in the past and require more complex pre- and intraoperative management. During exploration for sporadic PHPT, a first abnormal gland <200 mg should heighten suspicion of MGD and presages a tenfold higher failure rate.


Similar content being viewed by others


References
Pasieka JL, Parsons L, Jones J (1998) Prospective surgical outcome study of relief of symptoms following surgery in patients with primary hyperparathyroidism. World J Surg 122:513–518. doi:10.1007/s002689900428
Mazzaglia PJ, Berber E, Kovach A et al (2008) The changing presentation of hyperparathyroidism over 3 decades. Arch Surg 143:260–266
Perrier ND, Balachandran D, Wefel JS et al (2009) Prospective, randomized, controlled trial of parathyroidectomy versus observation in patients with “asymptomatic” primary hyperparathyroidism. Surgery 146:1116–1122
Silverberg SJ, Bilezikian JP, Bone HG et al (1999) Therapeutic controversies in primary hyperparathyroidism. J Clin Endocrinol Metab 84:2275–2285
Lo CY, Chan WF, Kung AW et al (2004) Surgical treatment of primary hyperparathyroidism: changes in clinical pattern over 3 decades. Arch Surg 139:77–82
Bindlish V, Freeman JL, Witterick IJ et al (2002) Correlation of biochemical parameters with single parathyroid adenoma weight and volume. Head Neck 24:1000–1003
Moretz WH, Watts TL, Virgin FW et al (2007) Correlation of intraoperative parathyroid hormone levels with parathyroid gland size. Laryngoscope 117:1957–1960
Mozes G, Curlee KJ, Rowland CM et al (2002) The predictive value of laboratory findings in patients with primary hyperparathyroidism. J Am Coll Surg 194:126–130
Mazeh H, Chen H, Leverson G et al (2012) Creation of a “Wisconsin Index” nomogram to predict the likelihood of additional hyperfunctioning parathyroid glands during parathyroidectomy. Ann Surg 257:138–141
Hamidi S, Aslani A, Nakhjavani M et al (2006) Are biochemical values predictive of adenoma’s weight in primary hyperparathyroidism? ANZ J Surg 76:882–885
Randhawa PS, Mace AD, Houraei SAR et al (2007) Primary hyperparathyroidism: do perioperative biochemical variables correlate with parathyroid adenoma weight or volume? Clin Otolaryngol 32:179–184
Calva-Cerqueira D, Smith BJ, Hostetler ML et al (2007) Minimally invasive parathyroidectomy and preoperative MIBI scan: correlation of gland weight and preoperative PTH. J Am Coll Surg 205:S38–S44
Udelsman R (2002) Six hundred fifty-six consecutive explorations for primary hyperparathyroidism. Ann Surg 235:665–672
Irvin GL, Carneiro DM, Solorzano CC (2004) Progress in the operative management of sporadic primary hyperparathyroidism over 34 years. Ann Surg 239:704–711
Westerdahl J, Bergenfelz A (2007) Unilateral vs bilateral neck exploration for primary hyperparathyroidism: five year follow-up of a randomized controlled trial. Ann Surg 246:976–981
Russell CF, Dolan SJ, Laird JD (2006) Randomized clinical trial comparing scan directed unilateral vs bilateral cervical exploration for primary hyperparathyroidism due to solitary adenoma. Br J Surg 93:418–421
Carty SE, Worsey J, Virji MA et al (1997) Concise parathyroidectomy: the impact of preoperative SPECT 99 mTc sestamibi scanning and intraoperative quick parathormone assay. Surgery 122:1107–1114
Melck AL, Armstrong MJ, Yip L et al (2012) Case-controlled comparison of video-assisted and conventional minimally invasive parathyroidectomy. Am Surg 78:125–132
Mitchell J, Milas M, Barbosa G et al (2008) Avoidable operations for thyroid and parathyroid surgery: effect of hospital volume. Surgery 144:899–907
Lew JI, Rivera M, Irvin GL et al (2010) Operative failure in the era of focused parathyroidectomy. Arch Surg 145:628–633
Merlino JI, Ko K, Minotti A et al (2003) The false negative technetium-99 m-sestamibi scan in patients with primary hyperparathyroidism: correlation with clinical factors and operative findings. Am Surg 69:225–230
Chiu B, Sturgeon C, Angelos P (2006) What is the link between nonlocalizing sestamibi scans, multigland disease and persistent hypercalcemia? A study of 401 consecutive patients undergoing parathyroidectomy. Surgery 140:418–422
Kebebew E, Hwang J, Reiff E et al (2006) Predictors of single-gland vs multigland parathyroid disease in primary hyperparathyroidism: a simple and accurate scoring model. Arch Surg 141:777–782
Dy BM, Richards ML, Vazquez BJ et al (2012) Primary hyperparathyroidism and negative Tc99 sestamibi imaging: to operate or not? Ann Surg Oncol 19:2272–2278
Yip L, Pryma DA, Yim JH et al (2009) Sestamibi SPECT intensity scoring system in sporadic primary hyperparathyroidism. World J Surg 33:426–433. doi:10.1007/s00268-008-9841-0
Miccoli P, Bendinelli C, Berti P et al (1999) Video-assisted versus conventional parathyroidectomy in primary hyperparathyroidism: a prospective randomized study. Surgery 126:1117–1122
Sosa JA, Udelsman R (2003) Minimally invasive parathyroidectomy. Surg Oncol 12:125–134
Johnson LR, Doherty G, Lairmore T et al (2001) Evaluation of the performance and clinical impact of a rapid intraoperative parathyroid hormone assay in conjunction with preoperative imaging and concise parathyroidectomy. Clin Chem 47:919–925
Irvin GL, Prudhomme DL, Deriso GT et al (1994) A new approach to parathyroidectomy. Ann Surg 219:574–581
Wang TS, Paieka JL, Carty SE (2014) Techniques of parathyroid exploration at North American endocrine surgery fellowship programs: what the next generation is being taught. Am J Surg [Epub ahead of print]
Rasbach DA, Monchik JM, Geelhoed GW et al (1984) Solitary parathyroid microadenoma. Surgery 96:1092–1098
Leichty RD, Teter A, Suba EJ (1986) The tiny parathyroid adenoma. Surgery 100:1048–1052
Goasguen N, Chirica M, Roger N et al (2010) Primary hyperparathyroidism from parathyroid microadenoma: specific features and implications for a surgical strategy in the era of minimally invasive parathyroidectomy. J Am Coll Surg 210:456–462
Almquist M, Bergenfelz A, Martensson H et al (2010) Changing biochemical presentation of primary hyperparathyroidism. Langenbecks Arch Surg 395:925–928
Gilat H, Cohen M, Feinmesser R et al (2005) Minimally invasive parathyroidectomy for resection of a parathyroid adenoma: the role of preoperative high-resolution ultrasonography. J Clin Ultrasound 33:283–287
Cheung K, Wang TS, Farrokhyar F et al (2012) A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann Surg Oncol 19:577–583
Berber E, Parikh RT, Ballem N et al (2008) Factors contributing to negative parathyroid localization: an analysis of 1000 patients. Surgery 144:74–79
Barczynski M, Golkowski F, Konturek A et al (2006) Technetium-99m-sestamibi subtraction scintigraphy vs. ultrasonography combined with rapid parathyroid hormone assay in parathyroid aspirates in preoperative localization of parathyroid adenomas and in directing surgical approach. Clin Endocrinol 65:106–113
Masatsugu T, Yamashita H, Noguchi S et al (2005) Significant clinical differences in primary hyperparathyroidism between patients with and those without concomitant thyroid disease. Surg Today 35:351–356
Doherty GM, Weber B, Norton JA (1994) Cost of unsuccessful surgery for primary hyperparathyroidism. Surgery 116:954–957
Jaskoiak N, Norton JA, Alexander HR et al (1996) A prospective trial evaluating a standard approach to reoperation for missed parathyroid adenoma. Ann Surg 224:308–320
Zarebczan B, Chen H (2011) Influence of surgical volume on operative failures for hyperparathyroidism. Adv Surg 45:237–248
Wang TS, Roman SA, Sosa JA (2009) Predictors of outcomes following pediatric thyroid and parathyroid surgery. Curr Opin Oncol 21:23–28
Stavrakis AI, Ituarte PHG, Ko CY et al (2007) Surgeon volume as a predictor of outcomes in inpatient and outpatient endocrine surgery. Surgery 142:887–899
Hodin R, Angelos P, Carty S et al (2012) No need to abandon unilateral parathyroid surgery. J Am Coll Surg 215:297
Chiu B, Sturgeon C, Angelos P (2006) Which intraoperative parathyroid hormone assay criterion best predicts operative success? A study of 352 consecutive patients. Arch Surg 141:483–488
Carneiro DM, Solorzano CC, Nader MC et al (2003) Comparison of intraoperative iPTH assay (QPTH) criteria in guiding parathyroidectomy: which criterion is the most accurate? Surgery 134:973–981
Reiher AE, Schafer S, Chen H et al (2012) Does the final intraoperative PTH really have to fall into the normal range to signify cure? Ann Surg Oncol 19:1862–1867
Richards ML, Thompson GB, Farley DR et al (2011) An optimal algorithm for intraoperative parathyroid hormone monitoring. Arch Surg 146:280–285
McGill J, Sturgeon C, Kaplan SP et al (2008) How does the operative strategy for primary hyperparathyroidism impact the findings and cure rate? J Am Coll Surg 207:246–249
Milas M, Wagner K, Easley KA et al (2003) Double adenomas revisited: nonuniform distribution favors enlarged superior parathyroids (fourth pouch disease). Surgery 134:995–1004
Miccoli P, Berti P, Materazzi G et al (2008) Endoscopic bilateral neck exploration versus quick intraoperative parathormone assay (qPTHa) during endoscopic parathyroidectomy: a prospective randomized trial. Surg Endosc 22:398–400
Acknowledgments
The authors gratefully acknowledge the adept assistance and continued expertise of Mohamed A. Virji, MD, with regard to the development, interpretation, and understanding of IOPTH use at our institution.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McCoy, K.L., Chen, N.H., Armstrong, M.J. et al. The Small Abnormal Parathyroid Gland is Increasingly Common and Heralds Operative Complexity. World J Surg 38, 1274–1281 (2014). https://doi.org/10.1007/s00268-014-2450-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2450-1