
Abstract
Background
It has been clearly shown that after elective colorectal surgery patients benefit from multimodal perioperative care programs. The Dutch Institute for Health Care Improvement started a breakthrough project to implement a multimodal perioperative care program of enhanced recovery after surgery (ERAS). This pre/post noncontrolled study evaluated the success of large-scale implementation of the ERAS program for elective colonic surgery using the breakthrough series.
Methods
A total of 33 hospitals participated in this breakthrough project during 2005–2009. Each hospital performed a retrospective chart review to gather information on traditionally treated patients (pre-ERAS group, n = 1,451). During the subsequent year patients were treated according to the ERAS program (ERAS group, n = 1 034). Outcomes were length of stay (LOS), functional recovery, adherence to the protocol, and determinants of reduced LOS.
Results
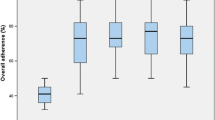
Median LOS decreased significantly from 9 to 6 days (p < 0.001). In the ERAS group, functional recovery was reached within 3 days. Adherence to the protocol elements was high during the preoperative and perioperative phases but slightly lower during the postoperative phase. Younger age, female sex, American Society of Anesthesiologists grades I/II, and laparoscopic surgery were associated with decreased LOS. Care elements that positively influenced LOS were cessation of intravenous fluids and mobilization on postoperative day 1 and administration of laxatives postoperatively.
Conclusions
The ERAS program was successfully implemented in one-third of all Dutch hospitals using the breakthrough series. Participating hospitals reduced the LOS by a median 3 days and were able to improve their standard of care in elective colonic surgery.







Similar content being viewed by others


References
Schoetz DJ Jr, Bockler M, Rosenblatt MS et al (1997) “Ideal” length of stay after colectomy: whose ideal? Dis Colon Rectum 40:806–810
Kehlet H, Mogensen T (1999) Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation program. Br J Surg 86:227–230
Basse L, Hjort Jakobsen D, Billesbolle P et al (2000) A clinical pathway to accelerate recovery after colonic resection. Ann Surg 232:51–57
Basse L, Raskov HH, Hjort Jakobsen D et al (2002) Accelerated postoperative recovery program after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 89:446–453
Basse L, Thorbol JE, Lossl K et al (2004) Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum 47:271–277 discussion 277–278
Kehlet H (1997) Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 78:606–617
Kehlet H (2000) Manipulation of the metabolic response in clinical practice. World J Surg 24:690–695
Kehlet H, Wilmore DW (2002) Multimodal strategies to improve surgical outcome. Am J Surg 183:630–641
Varadhan KK, Neal KR, Dejong CH et al (2010) The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 29:434–440
Bradshaw BG, Liu SS, Thirlby RC (1998) Standardized perioperative care protocols and reduced length of stay after colon surgery. J Am Coll Surg 186:501–506
Schwenk W (2001) Perioperative management influences the results of laparoscopic colonis surgery: arguments for a fast track program. Presented at the 1st hvidovre symposium on perioperative care—colorectal surgery, Copenhagen
Henriksen MG, Hansen HV, Hessov I (2002) Early oral nutrition after elective colorectal surgery: influence of balanced analgesia and enforced mobilization. Nutrition 18:263–267
Anderson AD, McNaught CE, MacFie J et al (2003) Randomized clinical trial of multimodal optimization and standard perioperative surgical care. Br J Surg 90:1497–1504
Delaney CP, Zutshi M, Senagore AJ et al (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46:851–859
Soop M, Carlson GL, Hopkinson J et al (2004) Randomized clinical trial of the effects of immediate enteral nutrition on metabolic responses to major colorectal surgery in an enhanced recovery protocol. Br J Surg 91:1138–1145
Gatt M, Anderson AD, Reddy BS et al (2005) Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 92:1354–1362
Maessen J, Dejong CH, Hausel J et al (2007) A protocol is not enough to implement an enhanced recovery program for colorectal resection. Br J Surg 94:224–231
Lassen K, Soop M, Nygren J et al (2009) Consensus review of optimal perioperative care in colorectal surgery: enhanced recovery after surgery (ERAS) group recommendations. Arch Surg 144:961–969
Lassen K, Hannemann P, Ljungqvist O et al (2005) Patterns in current perioperative practice: survey of colorectal surgeons in five northern European countries. BMJ 330:1420–1421
Nygren J, Hausel J, Kehlet H et al (2005) A comparison in five European centres of case mix, clinical management and outcomes following either conventional or fast-track perioperative care in colorectal surgery. Clin Nutr 24:455–461
Hannemann P, Lassen K, Hausel J et al (2006) Patterns in current anaesthesiological peri-operative practice for colonic resections: a survey in five northern-European countries. Acta Anaesthesiol Scand 50:1152–1160
Polle SW, Wind J, Fuhring JW et al (2007) Implementation of a fast-track perioperative care program: what are the difficulties? Dig Surg 24:441–449
Grimshaw JM, Eccles MP, Walker AE et al (2002) Changing physicians’ behavior: what works and thoughts on getting more things to work. J Contin Educ Health Prof 22:237–243
Grol R, Wensing M (2004) What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust 180(6 Suppl):S57–S60
Wilson KD, Kurz RS (2008) Bridging implementation and institutionalization within organizations: proposed employment of continuous quality improvement to further dissemination. J Public Health Manag Pract 14:109–116
Fearon KC, Ljungqvist O, Von Meyenfeldt M et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24:466–477
Kilo CM (1998) A framework for collaborative improvement: lessons from the Institute for Healthcare Improvement’s Breakthrough Series. Qual Manag Health Care 6:1–13
Schouten LM, Hulscher ME, van Everdingen JJ et al (2008) Evidence for the impact of quality improvement collaboratives: systematic review. BMJ 336:1491–1494
Maessen JM, Dejong CH, Kessels AG et al (2008) Length of stay: an inappropriate readout of the success of enhanced recovery programs. World J Surg 32:971–975
Tjeerdsma HC, Smout AJ, Akkermans LM (1993) Voluntary suppression of defecation delays gastric emptying. Dig Dis Sci 38:832–836
Hansen CT, Sorensen M, Moller C et al (2007) Effect of laxatives on gastrointestinal functional recovery in fast-track hysterectomy: a double-blind, placebo-controlled randomized study. Am J Obstet Gynecol 196:e311–e317
Hendry PO, van Dam RM, Bukkems SF et al (2010) Randomized clinical trial of laxatives and oral nutritional supplements within an enhanced recovery after surgery protocol following liver resection. Br J Surg 97:1198–1206
Andersen J, Christensen H, Pachler JH et al (2011) Effect of the laxative magnesium oxide on gastrointestinal functional recovery in fast-track colonic resection: a double-blind, placebo-controlled randomized study. Colorectal Dis 14:776–782
Zingg U, Miskovic D, Pasternak I et al (2008) Effect of bisacodyl on postoperative bowel motility in elective colorectal surgery: a prospective, randomized trial. Int J Colorectal Dis 23:1175–1183
Van Bree S, Vlug M, Bemelman W et al (2011) Faster recovery of gastrointestinal transit after laparoscopy and fast-track care in patients undergoing colonic surgery. Gastroenterology 141(872–880):e871–e874
Vlug MS, Wind J, Hollmann MW et al (2011) Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). Ann Surg 254:868–875
Acknowledgments
The authors thank the Perioperative Care Breakthrough Project Group for collection of data: C.L.H. van Berlo, VieCurie Medisch Centrum, Venlo; A.J.A. Bremers, Universitair Medisch Centrum St. Radboud, Nijmegen; M.A.M. Brouwers, Haga Ziekenhuis, Den Haag; D. Cobben, Medisch Centrum Leeuwarden; P.P.L.O. Coene, Medisch Centrum Rijnmond Zuid, Rotterdam; K.C.A. van Engelenburg, Slingeland Ziekenhuis, Doetinchem; S.J. van der Hagen, Refaja Ziekenhuis, Stadskanaal; K.Havenga, Universitair Medisch Centrum Groningen; E.J. Hesselink, Gelre Ziekenhuizen, Apeldoorn; I.H.J.T. de Hingh, Catharina Ziekenhuis, Eindhoven; A.P.J. Houdijk, Medisch Centrum Alkmaar; J.M. Klaase, Medisch Spectrum Twente, Enschede; E.A.G.L. Lagae, Ziekenhuis Zeeuws Vlaanderen; F. Logeman, Beatrix Ziekenhuis, Winterswijk; E.J. Mulder, Antonius Ziekenhuis Sneek; K.H. Ong, Rivierenland Ziekenhuis, Tiel; R.J. Oostenbroek, Albert Schweitzer Ziekenhuis, Dordrecht; J.W.A. Oosterhuis, Isala Klinieken, Zwolle; R.T. Ottow, Groene Hart Ziekenhuis, Gouda; A.J. den Outer †, Rijnland Ziekenhuis, Leiderdorp; B. van Ramshort, St Antonius Ziekenhuis, Nieuwegein; P.H.M. Reemst, Maxima Medisch Centrum, Eindhoven; C. Rosman, Canisius Wilhelmina Ziekenhuis, Nijmegen; G.A. Vos, Waterland Ziekenhuis, Purmerend; F. Wit, Ziekenhuis de Tjongerschans, Heereveen; R.J. Zijlstra, Ziekenhuis Nij Smellinghe, Drachten; J.F.M. Reinders, Ijsselmeerziekenhuizen, Lelystad; R.A. Schasfoort, Scheper Ziekenhuis, Emmen; R. van Hillegersberg, Universitair Medisch Centrum, Utrecht; H.E. Lont, Vlietland Ziekenhuis, Vlaardingen; J. Jansen, Ziekenhuis Walcheren.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Elements of the ERAS protocol
Elements | Conditions |
|---|---|
Preoperative phase | |
Preoperative counseling | Extensive information on the ERAS protocol |
Bowel preparation | No or single phosphate enema |
Carbohydrate drink | 400 ml of Pre-op® (or comparable) 2 h before operation, unless diabetic |
Sedation | No sedation (short-acting if extremely anxious) |
Perioperative phase | |
Thoracic epidural analgesia/anesthesia | For all elective bowel surgery |
Prevention of hypothermia | Temperature ≥36.0 °C at end of operation |
Thromboembolic prophylaxis | Started 2 h after epidural and continued until mobilization |
Nasogastric tube | Removed before return to ward on day 0 |
Abdominal drains | No drains |
Prophylactic antibiotics | Two drugs, given before incision |
Incision | Short midline or transverse incisions |
Oral fluid intake | 800 ml on day 0 (400 ml if operated on in the afternoon) |
Sitting up | At least 15 min on day 0 |
Postoperative phase | |
IV fluids | Stopped on day 1 |
Normal diet | Resumed on day 1 |
Oral supplements | 200 ml twice daily from day 1 |
Sitting up | At least 3 times 30 min in chair on day 1 |
Oral laxatives | MgO tablets 1,000 mg from day 1 |
Oral analgesics | Paracetamol from day 0; NSAID started before removal of epidural catheter |
Removal of epidural catheter | On day 2 |
Removal of urinary catheter | At the time of removing the epidural catheter |
Rights and permissions
About this article
Cite this article
Gillissen, F., Hoff, C., Maessen, J.M.C. et al. Structured Synchronous Implementation of an Enhanced Recovery Program in Elective Colonic Surgery in 33 Hospitals in The Netherlands. World J Surg 37, 1082–1093 (2013). https://doi.org/10.1007/s00268-013-1938-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-1938-4