
Abstract
From diagnostics to prognosis to response prediction, new applications for radiomics are rapidly being developed. One of the fastest evolving branches involves linking imaging phenotypes to the tumor genetic profile, a field commonly referred to as “radiogenomics.” In this review, a general outline of radiogenomic literature concerning prominent mutations across different tumor sites will be provided. The field of radiogenomics originates from image processing techniques developed decades ago; however, many technical and clinical challenges still need to be addressed. Nevertheless, increasingly accurate and robust radiogenomic models are being presented and the future appears to be bright.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Medical imaging plays a major role in the clinical decision-making process in oncology. In the past, that role was limited to diagnosis and staging. However, in recent years, imaging markers derived from routine clinical images have increasingly been researched to provide insight into the tumor in a non-invasive manner.
Imaging features may be either qualitative, sometimes referred to as semantic [1,2,3], where a reader, often an experienced radiologist, will assign a score to certain parameters stemming from expertise-based observation, or quantitative, for example, tumor dimensions, attenuation, or radiomics where the values are derived directly from the image. In radiomics, features are extracted mathematically with the aid of specialized computer algorithms. Radiomic features reflect a wide array of parameters in the image and have been shown to capture distinct imaging phenotypes beyond what is discernible to the naked eye [2].
Radiomics is the rapidly growing field of radiological research where routine patient images/scans are converted into mineable quantitative data [4] that can then be leveraged to decode the tumor phenotype for applications ranging from improved diagnostics to prognostication to therapeutic response prediction [5]. Radiomics refers to the general field in which patient scans are converted into quantitative data while radiogenomics is a specific application where imaging features, radiomic or otherwise, are linked to genomic profiles [6]. For the purpose of this review, we will focus on the above definition.
Interestingly, the term “radiogenomics” initially belonged to the realm of radiation oncology where it reflected the prediction of radiotherapy-induced toxicity based on the genetic profile of the tumor [7]. In recent years, radiogenomics has come to carry the connotation of linking radiomic features to even broader biological parameters beyond genomics such as proteomics and metabolomics [8]. While this is most likely the ultimate destiny of the field, it has yet to become the standard definition.
The radiomics pipeline
The workflow where quantitative features are extracted from radiological images and linked to specific outcomes has often been termed in literature as the “radiomics pipeline” [9,10,11]. This workflow is composed of a number of broad steps, beginning with image acquisition. Based on the device [12], image reconstruction algorithm [13], and protocol settings [14], the value of the extracted radiomic features can differ greatly. Following the image acquisition step, two broad approaches emerge, depending on how radiomic features are derived and at what step artificial intelligence is applied, if at all: classical radiomics [15, 16], with or without machine learning [17,18,19], and deep learning radiomics [20, 21].
Classical/conventional radiomics
Considering that radiomics is a novel field, the term “classical radiomics” may be something of a misnomer. Alternate descriptions such as “conventional radiomics” have been put forth [22]; however, the majority of literature still refers to this method as “classical.” In this approach, regions of interest are delineated, either manually or automatically, and handcrafted features are extracted using specialized algorithms (see Fig. 1a). Handcrafted imaging features attempt to describe lesions by capturing intuitive parameters reflecting the shape, morphology, and texture [23]. This dependence on delineation and handcrafted features is characteristic of conventional radiomics.

Outline of the two kinds of radiomics pipeline. a The classical/conventional radiomics model where, after image acquisition, areas of interest are delineated and handcrafted features are extracted. Subsequently, models are built around these predefined features using either statistical or machine learning methodologies. b The deep learning radiomics pipeline where, after image acquisition, neural networks automatically perform feature extraction, selection, and classification
The image-derived features are then processed, either using statistical models or machine learning, to link them to specific outcomes. Statistical models, such as univariate and multivariate analysis, are largely used to determine mathematical relationships between variables and outcomes, whereas machine learning is primarily focused on the construction of systems capable of learning from the data without explicitly programmed instructions. Machine learning models are widely considered superior for predictive purposes and rely on fewer mathematical assumptions, are built from more comprehensive datasets, and require minimal human involvement.
Deep learning radiomics
Newer deep learning radiomic workflows (Fig. 1b) can now process the image, automatically extract features, and perform classification without the need for a detailed delineation, if at all [24]. This approach is founded on the concept that deep learning classifiers should not only be used for data mining but also for data generation [25]. Convolutional neural networks (CNNs), a class of deep learning networks, have risen to prominence in the field of medical image analysis due to their independence from humans in feature design. The number of quantitative features extracted within a CNN is several orders of magnitude greater than older handcrafted feature extraction algorithms used in classical/conventional radiomics. Another significant advantage is that within the same convolutional neural network, feature extraction, selection, and classification occur across different layers.
Value of the genetic profile in cancer
Genomic instability and mutations are a hallmark of cancer and the accumulation of genetic and epigenetic mutations results in unchecked cell proliferation [26]. Gene profiles are often used to predict survival, as a prognostic biomarker, or response to treatment, as a predictive biomarker, helping to guide clinical decisions, particularly treatment selection [27].
Genetic mutations have been shown to be predictive of response/resistance to or recurrence after chemotherapy in breast cancer [28], hepatocellular carcinoma [29], and ovarian cancer [30] among others. In addition to traditional chemoradiotherapy, targeted molecular therapy has become a mainstay in the management of a wide range of tumors. Targeted therapy harnesses tumor-specific biology to inhibit the action of particular enzymes, target tumor-associated proteins, mutated receptors, or leverages other oncogenic molecular vulnerabilities. Detailed knowledge of the genetic composition, for instance driver mutations, resistance signatures, and so on can provide much-needed guidance on the selection of an optimal therapy.
In the rapidly evolving field of cancer immunology and immunotherapy, high tumor mutational load, a measure of the number of mutations within the tumor genome, has been associated with increased potential response to immunotherapy, especially immune checkpoint blockade [31, 32]. This association has been explained by the fact that an increased mutational burden results in a wider variety of neoantigens, to which the immune system has not been exposed, being expressed by the tumor [33, 34]—making them more recognizable by the immune system as foreign.
With the increased use of precision medicine and the establishment of guidelines around biomarkers, knowledge of the tumor genetic profile is advantageous to clinicians. Normally, insight into the tumor genome requires biopsies, an invasive procedure that may increase patient morbidity. The field of science that has risen to non-invasively identify specific imaging features (or signatures) that can predict tumor genomic alterations is termed “radiogenomics.”
Review of radiogenomic studies
Between 2017 and 2018 alone, there have been more than five hundred radiomics publications listed in the PubMed/MEDLINE database. Radiogenomics forms a rapidly growing subset of this research activity and as such, a general overview of the accumulating literature is needed. This review aims to provide a broad outline of the radiogenomic literature. Considering that cancer mutations are very often shared among different abdominal and extra-abdominal tumors, we have opted to study the various projects that have aimed to correlate imaging features with specific genetic signatures across different tumor types. (Literature search methodology in “Appendix 1” and Supplemental Fig. 1).
Brain
The overwhelming bulk of literature within radiogenomics has concerned the brain (Table 1). As early as 2008, Diehn et al. combined glioblastoma multiforme (GBM) neuroimaging with microarray DNA data in order to non-invasively map gene expression within the tumor [35]. Colen et al. subsequently used the scans of 82 treatment-naïve TCGA (The Cancer Genome Atlas) GBM patients to successfully correlate semantic imaging features to gene and microRNA expression—specifically those associated with edema-genesis, cell migration, and increased inflammatory response [36]. Alongside semantic and radiomic imaging features, even volumetrics—the analysis of volumes within the tumor compartments—have been associated with PERIOSTIN expression, a gene linked with decreased survival, shorter time to recurrence (p < 0.001), and the mesenchymal GBM subtype (p < 0.0001) [37].
Radiogenomics research in the brain was initially focused on the use of imaging features for molecular subtype prediction. Molecular subtypes are based on genome-wide profiling and large-scale genomic analysis and can used to provide diagnostic, prognostic, and therapeutic options [38]. MRI-derived texture features were shown to non-invasively predict whether a tumor would belong to one of four distinct molecular subtypes: classical (AUC = 0.72), neural (AUC = 0.75), proneural (AUC = 0.82), or mesenchymal (AUC = 0.70) [39]. Tumor shape [40, 41] and tumor-associated edema on T2-FLAIR (AUC = 0.61) [42] have also been reported as possible imaging discriminators of molecular subtype in GBM.
With the promising results of radiomics in molecular subtype prediction, more specific biological associations were pursued. The attention of the field turned towards the prediction of gene mutations that were already being used as biomarkers in daily clinical practice.
A number of prominent somatic mutations (namely TP53, RB1, NF1, EGFR, and PDGFRA) were found to be associated with volumetric parameters on T1 contrast and T2 FLAIR MR images [43]. The first purely quantitative analysis integrated GBM “multi-omics” data, containing multiple “-omes” such as the genome, transcriptome, and proteome, from the TCGA and their corresponding images from The Cancer Imaging Archive (TCIA) [44, 45]. Zinn et al. identified “radiomic profiles” that helped to discriminate the mutational landscape (i.e., TP53, PTEN, and EGFR) on a dataset of 29 TCGA patients [46]. Hu et al. performed an exceptional study where multiparametric MRI features extracted specifically from biopsy sites were used to predict various driver mutations (namely EGFR, PDGFRA, PTEN, CDKN2A, RB1, and TP53) via random forest [47]. This approach cleverly mitigated the impact of tumor heterogeneity and was one of only two radiogenomic studies to do so. Radiomics features were also identified that directly correlated with the overall mutational burden/load [48].
Different groups quickly moved away from broad genetic analyses to the characterization of imaging phenotypes for specific mutations in GBM. Isocitrate dehydrogenase-1 (IDH) mutation is commonly used in the clinic to stratify patients, often in conjunction with other co-mutations [49] and it received the most attention in brain radiogenomic research. IDH-mutated gliomas occurred most frequently in the rostral extension of the lateral ventricles of the frontal lobe [50] and were linked to tumor size [51], local pattern of intensities [52], PET features [53, 54], angular standard deviation (tumor boundary irregularity) [41], mean diffusional kurtosis [55], and apparent diffusion coefficient (ADC) [56] as well as part of “radiomic signatures” in artificial intelligence models [20, 57,58,59,60,61,62]. Similarly, 1p/19q co-deletion [62,63,64,65], a widely used prognostic biomarker for brain tumors [66], and EGFR mutation [67,68,69,70] were thoroughly covered by different teams, having been linked to a wide array of MRI features. Additional imaging markers were also found that were predictive for the expression of clinically relevant genes such as BCAT [71], PDGFR2a [72], ATRX [73], hypoxia-associated genes [74], Ki67 [75], CD49d [76], and CD3RNA expression [77]. Going beyond genomic parameters, Lehrer et al. performed a “radioproteomics” study where semantic MRI features were correlated with proteins expressed in lower grade glioma [78].
Interestingly, attempts were made to subgroup these tumors with radiomics alone, irrespective of their mutational landscape and clinical features [79]—strongly suggesting that much more information than anticipated could be extracted from quantitative features. In support of this point, MGMT methylation status, another prognostic biomarker [66], predicted by AI models even when clinical data were excluded and only radiomics were used [80].
Other brain tumors have also been studied where, especially in meningioma, radiomic features were shown to be capable of good patient stratification, based on grade (AUC = 0.86) [81], phenotype [81], or risk of relapse (AUC = 0.72, p = 0.28) [82]. Semantic features were also correlated with the molecular subtype in medulloblastoma [83] and to the genomic profile of neuroblastoma [84].
As the site that was most extensively studied, brain radiogenomic literature reflects what is seen across a wide variety of tumor types, namely that the field is still in its early stages. Radiogenomic features have been linked to genomics-derived molecular subtypes, gene groups, and specific somatic mutations. Most studies, however, are performed on limited, usually single-center, patient cohorts in an exploratory, proof-of-concept manner. Agreement between studies on independent radiogenomic features remains to be achieved before mainstream clinical application can be pursued.
Lung
In non-small cell lung cancer (NSCLC), genetic mutational status plays a pivotal role in the clinical decision-making process—especially since targeted agents received FDA approval in NSCLC [85]. Around 10–15% of NSCLC patients have an activating EGFR mutation [86], where receptor blockers or tyrosine kinase inhibitors (TKIs) would be valid treatment options. Moreover, a quarter of lung adenocarcinoma patients have a KRAS mutation [87], which would confer resistance to the aforementioned treatments (see Fig. 2). KRAS and EGFR mutations are mutually exclusive [88] and the presence of one or the other strongly influences the choice of treatment. Furthermore, up to 7% of NSCLC patients harbor an ALK rearrangement, potentially making them candidates for crizotinib, a multi-targeted tyrosine kinase inhibitor with potent activity against ALK [89].

An illustration of the role of genetic mutational status in treatment decisions. a The RAS pathway connects EGFR to cell proliferation and survival (via transcription of effector genes). b Anti-EGFR based treatments block signal transduction from the receptor and hence counter the effects of the pathway. c Activating mutations in KRAS allow the cell to constantly exert the effect of this pathway irrespective of whether the ligand has bound to the receptor. Such mutations could mediate resistance to anti-EGFR therapies
Given the fact that genomic analysis is becoming more routine in this cohort of patients, there has been significant research interest in seeing whether radiomics could predict the genetic status of the tumor, especially in KRAS, EGFR, and ALK. (Table 2). Gevaert et al. started the flurry of radiogenomic lung research by correlating PET/CT features to metagenes, aggregated patterns of gene expression, with encouraging preliminary results [90]. However, the first article that most resembled a conventional radiogenomics study by linking specific imaging features to specific mutations was the work of Halpenny et al, investigating the predictive value of CT radiomics for ALK rearrangements [91]. Early on, different projects selected clinically relevant mutations, like ALK [92], EGFR [93, 94], and KRAS [88]), with various technical methodologies (purely correlative studies vs. predictive models [95]).
As a predictive marker, KRAS has been linked to round shape [96], nodules in non-tumor lobes [96], multiple small nodules [97], as well as general radiomic profiles [98, 99]. Interestingly, some studies reported the ability to predict EGFR, but not KRAS [100, 101]. ALK rearrangement was linked to pleural effusion [96] and lobulated margin [102]. HER2, a gene often amplified during acquired resistance to EGFR-targeting therapy, was also studied [103]. Halpenny et al. also studied qualitative features in the prediction of a BRAF mutation in lung cancer—citing pleural metastases as a key difference (p = 0.045) [104].
By far, the most researched genetic mutation in NSCLC was EGFR (both exon 19 and exon 21 mutations) having been linked to contrast [105], Laws-Energy [94], median Hounsfield Unit (HU) [88], SUVmax [106], pleural retraction [96], small size [96, 97], speculation [97], irregular nodules [107], poorly defined margins [107], ground glass [107, 108], emphysema [109], locoregional infiltration [109], “normalized inverse difference moment” [101], as well as combined radiomic profiles [98,99,100, 110,111,112,113].
Interestingly, the semantic features “small size” and “ground glass appearance” were the only two imaging markers that were reproducibly shown to be associated with the EGFR mutation [96, 97, 107, 108]. Quantitative features are often referred to as being more objective, however, based on image acquisition and feature extraction methods, the values can vary greatly [12,13,14]. In addition to large multicenter studies, the methods used at different points of the radiomics pipeline need to be standardized, otherwise a direct comparison may not possible. Achieving direct comparison is especially helpful in the case of other, less prevalent, tumors that would share the same driver mutation. A model trained on more easily acquired data from lung cancer may in the future be generalized to a different less prevalent tumor.
In addition to mutational status prediction, radiomic as well as genomic parameters have been combined in prognostication models [114]. Emaminejad et al. reported that while radiomics (AUC = 0.78) and genomics (AUC = 0.78) models were capable of predicting survival, accuracy significantly improved (AUC = 0.84) when both data were integrated [115]. The future of data-driven diagnostics will be the integration of complementary data generated from different sources (the “-omics”) to improve the performance of predictive models by unlocking further hidden information.
As in brain radiogenomic literature, lung studies seldom agreed on features, either semantic or radiomic, that were predictive for specific genetic mutations. This lack of reproducibility/generalizability is one of the largest hurdles for radiogenomics to overcome in order to be implemented into the clinical workflow. Until recently, most studies relied on monocentric patient cohorts using basic statistical methodologies to identify associations between certain features and the gene/molecule of interest. In order to identify truly reproducible radiogenomic features or signatures, large heterogeneous patient cohorts would need to be collected from multiple centers, ideally prospectively and would need to be analyzed using modern methods capable of addressing data heterogeneity.
Breast and ovaries
Since the 1970′s, mammograms have been used to assess breast cancer risk, through qualitative [116] and quantitative analysis of the breast parenchyma [117]. However, Li et al. were among the very first to apply texture analysis to discriminate between high-risk BRCA-mutated and low-risk wild-type patients [118]. AI methods were subsequently leveraged to improve the performance of these radiogenomic predictive models—first with Bayesian artificial neural networks, a framework for different machine learning algorithms [119, 120], and then with convoluted neural networks (AUC = 0.86) [121].
While radiogenomic research in the breast had initially started with mammograms, the interest of researchers in this field also spanned MRIs (Table 3). Yamamoto et al. studied 353 patients with breast cancer and obtained their gene expression profiles (MRI n = 10) [122]. Given that the ACR does not recommend breast MRIs as screening for the general population, this low sample size is understandable [123]. Nonetheless, 21 imaging traits were found that were globally correlated (p < 0.05) with 71% of the genes measured. In the MOSCATO-01 trial, voxel intensity was significantly associated with HER2 amplification on a patient group (n = 20) composed of gastrointestinal tumors, HNSCC, lung cancer, breast cancer, and urogenital cancer [124]. Considering that a number of mutations are relevant across multiple tumor types, for instance BRCA and HER2 in both breast cancer and ovarian cancer, further validation studies should be performed to test whether these imaging markers are tumor agnostic.
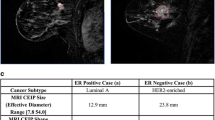
Quantitative imaging features were not only linked to specific mutations but also genomics-derived molecular subtypes [125, 126]. Wang et al. were able to further broaden the molecular subtypes that were predicted by imaging features: luminal A (p = 0.00473), HER2-enriched (p = 0.00277), and basal-like (p = 0.0117) [127]. Machine learning models capable of discerning luminal A molecular subtype (AUC = 0.697), triple-negative breast cancer (AUC = 0.654), estrogen receptor (ER) mutational status (AUC = 0.649), and progesterone receptor (PR) status (AUC = 0.622) were subsequently built [128]. Imaging markers were also directly correlated with survival in breast cancer [129]. With increasingly thorough analyses [130], novel imaging markers may be found that can be readily used in the clinic alongside existing risk-stratification scoring systems [131].
Molecular subtyping has also gained importance in ovarian cancer. Due to the significant risk of recurrence in high-grade serous ovarian carcinoma, prognostic biomarkers are of critical importance for clinicians [132]. A prognostic model called the “Classification of Ovarian Cancer” (CLOVAR) was developed by combining subtype and survival gene expression signatures in order to better profile patients into risk groups [133]. In one of the few radiogenomic multicenter studies, semantic features from a cohort of 92 high-grade serous ovarian carcinoma patients were found to be associated with subtypes of the CLOVAR system as well as time to progression [134]. In epithelial ovarian cancer, where 5-year survival is approximately 35–40%, a similar need for patient stratification exists [135]. Lu et al. engaged in a very thorough and methodical study where machine learning was used to derive a score they termed as the “Radiomic Prognostic Vector” (RPV) [136]. The RPV was shown to identify patients with less than 24 months of survival. This is also one of the very few predictive radiogenomic models that has been validated on independent multicenter cohorts and has received further complementary genetic and transcriptomic analysis to rationalize the predictions.
As mentioned in the previous section, when different data sources are combined, further information may potentially be unlocked. This was also observed when imaging features were combined with the recurrence scores of the OncotypeDX and PAM50 gene panels, the predictive performance of models improved significantly [137]. Integration of data from multiple domains may well be the necessary next step to bring the performance of these predictive models up to a clinically feasible level.
Liver
Liver cancer is the second leading cause of cancer mortality worldwide [138], with 80–90% of primary liver cancer being hepatocellular carcinoma (HCC). Radiogenomics in HCC developed rather curiously in the sense that two parallel research lines arose simultaneously (Table 4)—one searching for predictive imaging markers (therapeutic response) versus another searching for prognostic imaging markers (survival and recurrence rate).
Doxorubicin is one of the earliest developed anthracyclines and while systemic administration of the agent has shown limited benefit, 30–70% of HCC patients respond to transarterial chemoembolization (TACE) with doxorubicin [139]. Early radiogenomic studies successfully identified six predefined semantic imaging phenotypes on standard CE-CT images that were associated with doxorubicin response gene expression patterns [140]. West et al. subsequently performed the first quantitative radiogenomic study in liver cancer where they acquired CT images from 27 treatment-naïve HCC TCGA patients and correlated radiomic features with specific genes known to confer doxorubicin chemoresistance (namely TP53, TOP2A, CTNNB1, CDKN2A, and AKT1, AUC = 0.72–0.86) [141].
The other major focus in HCC radiogenomic literature was the development of a proxy imaging marker for Microvascular Invasion (MVI), an independent predictor of early recurrence and poor postoperative overall survival [142] identifiable only by histology of excised tissue. Having a non-invasive means of determining preoperative MVI would provide significant clinical benefit to these patients. Previous attempts were made to directly correlate conventional imaging features with histopathological MVI [143,144,145]. However, the most researched imaging marker was “Radiogenomic Venous Invasion” (RVI), a contrast-enhanced CT marker linked to a 91-gene HCC venous invasion gene expression signature that was prognostic for survival following surgical resection or liver transplantation [146]. Banerjee et al. validated the RVI for its correlation with MVI (accuracy = 89%, sensitivity = 76%, specificity = 94%) and moreover for its prognostic value (OS (p < 0.001), 3-year recurrence-free survival (p = 0.001) [146]). It should be noted that liver cirrhosis may impact the ability of these radiogenomic markers to predict MVI or even outcome [147]. Considering that the overwhelming majority of HCC patients have chronic liver disease [148], with 80–90% of cases suffering from liver cirrhosis [149], this is a sizable limitation. Further efforts would be needed in hepatic radiogenomic studies to identify cirrhosis-independent predictors.
In cholangiocarcinoma, FGFR2, a potentially suitable target for molecular therapy, was also studied from a radiogenomics perspective, albeit with conflicting results. An initial study (n = 66) using semantic features was unable to find any significant association to the genetic mutation [150]; however, a second smaller study (n = 33) using machine learning successfully predicted FDFR2 mutation in 90% of the cases (sensitivity = 87%, specificity = 94%) despite having only half the sample size [151]. This makes a compelling argument in favor of using machine learning to build better-performing predictive models.
Kidneys
As a result of the widespread use of abdominal imaging, renal cell carcinoma (RCC) is increasingly being detected at earlier stages where surgery is a therapeutic option [152]. Prognostic biomarkers are important for treating clinicians to help mitigate the risk of postoperative recurrence. In the clinic, von Hippel–Lindau (VHL) mutational status is often used as both a prognostic and predictive biomarker for RCC [153], given its role in hypoxia signaling [154]. VHL mutations were found to be significantly associated with well-defined tumor margins (p = 0.013), nodular tumor enhancement (p = 0.021), and gross appearance of intratumoral vascularity (p = 0.018) [155]. In addition to these features (Table 5), machine learning classifiers, trained on local datasets and validated on TCGA patients, were built that could identify not only mutations in VHL (accuracy = 0.75) but also in BAP1 (accuracy = 0.83) and PBRM1 (accuracy = 0.83) [156].
BAP1 mutation, particularly with a concomitant loss of PBRM1 [157], has been shown to be a significant negative prognostic parameter for RCC patients [158] and as such, has received attention in radiogenomic research alongside VHL [159]. BAP1-mutated RCCs tended to display CT renal vein invasion (p = 0.046) [155], ill-defined tumor margins (p = 0.002) [160], and a higher Fuhrman (pathological) grade (p = 0.026) [161]. BAP1 also featured in the work of Vikram et al. where they extracted quantitative features from 78 clear cell RCC from the TCGA and used machine learning methods to predict the mutational status (AUC = 0.78, pre-contrast) [162]. Beyond individual genes, CT radiomic features were also correlated, at the epigenetic level, with DNA methylation in RCC [163].
Colorectal carcinoma
As in lung cancer, the RAS gene family functions as a group of molecular switches controlling transcription factors and cell cycle proteins. Deregulation of RAS signaling results in increased cell proliferation, angiogenesis, and heightened metastatic potential. In colorectal cancer (CRC), 30–50% of cases are KRAS mutated [164] while 3–5% are NRAS mutated [165]—they are largely considered to be mutually exclusive [166, 167]. As in NSCLC, an activating RAS mutation is considered indicative of EGFR antibody resistance and hence serves as a predictive biomarker in the clinic [168, 169] (see Fig. 2).
Different imaging modalities have been tested to provide predictive imaging markers for KRAS mutational status. On CT, conventional radiomics has shown that KRAS mutations are associated with skewness (p = 0.02) [170]. More robust machine learning classifiers have also identified radiomic signatures capable of predicting KRAS (AUC = 0.829), NRAS (AUC = 0.686), and BRAF mutations (AUC = 0.857) in a cohort of 117 CRC patients [171]. Magnetic resonance imaging has also been analyzed where it was observed that, in rectal cancer, KRAS mutations were associated with N stage, axial tumor length, and a polypoid pattern [172]. DCE MR parameters, however, were not associated with either KRAS mutation or microsatellite instability, an important prognostic and predictive biomarker for colorectal cancer [173]. F18 FDG PET/CT imaging has also been tested in the search for colorectal radiogenomic markers albeit with mixed results. On one hand, first-order features such as maximum SUV [174], mean SUV, SUV standard deviation, and SUV coefficient of variation [175], have been significantly associated with KRAS mutation. On the other hand, a growing body of literature is reporting that uptake may not be reflective of KRAS mutational status [176, 177].
EGFR, KRAS, and BRAF mutations are clinically relevant in a number of carcinomas; however, due to lack of standardization, direct comparison of radiomic features linked to the same mutation across different tumor types is not meaningful. Tumor agnostic radiogenomic features need to be found using large multicenter datasets and harnessing advanced classification methods.
Outside the domain of image analysis, Pershad et al. used a purely text-based approach to process the descriptive words used by radiologists in their reports in order to predict KRAS mutational status [178]. The trained classifier determined the word frequency within both mutant and wild-type radiology report. Tumors with a KRAS mutant were described more often as “innumerable,” “confluent,” and “numerous,” whereas wild-type tumors were more “few,” “discrete,” and “[no] recurrent.”
Prostate
Radiogenomics carries great potential in the setting of prostate cancer given that clinical outcome is closely linked to one prominent tumor suppressor gene, PTEN (Table 5). Loss of PTEN in prostate cancer has been correlated with a clinically aggressive phenotype and increased mortality [179]. While multiparametric MR scans failed to yield any predictive/correlated features [180], contrast uptake on DCE-MRI (p < 0.01) and T2-weight signal-intensity skewness (p < 0.1) were correlated with PTEN expression [181].
Stoyanova et al. took a unique approach and performed radiogenomic analysis on patients with prostate cancer who had undergone MR-guided biopsies. The biopsy site was identified on the scan and radiomic features were extracted only from the specific area of interest—allowing for a more accurate radiomic–biological correlation to be made. Radiomic features associated with prognostic biomarkers were identified with this approach [182, 183].
Limitations and challenges facing radiogenomics
While the field of radiogenomics holds great promise, there are a number of limitations that the field, as a whole, needs to overcome [184].
Radiomics pipeline
Up until fairly recently, the radiomic pipeline consisted of image acquisition, delineation of regions of interest, extraction of handcrafted features, and correlation with simple statistics. Every step in the pipeline is prone to error, which can accumulate in a phenomenon known as “propagation of the error.” Manual delineations require significant time commitment by trained radiologists, often serving as a rate limiting step for the number of scans/patients included in a study. Furthermore, inter-observer variability of manual segmentations is hard to control—impacting the features derived from the image [185]. Notwithstanding the annotation/delineation step, the process of handcrafted feature extraction introduces an element of bias since they are built on predefined mathematical formulas meant to capture specific morphological and textural phenotypes. Based on the extraction technique and software used, these features can change [186]. Most handcrafted features were designed in the realm of computer vision for general image decoding tasks and were not intended to address clinical research questions.
At the model building step of the pipeline, more robust classification methods need to be leveraged. Simple correlative studies often are not reproducible, leading to conflicting results from different datasets meant to predict the same mutation in the same disease. With such simple statistical methodologies, basic radiomic studies run the risk of overfitting (i.e., being protocol-specific, scanner-specific, or hospital-specific or all of the above) or underfitting (i.e., exploring only linear models).
Reproducibility of radiomic features
In order for radiomics to gain clinical application, the identified imaging biomarkers need to be independent, informative, and reproducible. Typically, robust biomarkers are derived from large heterogeneous datasets with a methodical testing process and external validation. Currently, literature has shown that radiomic features can be influenced by many parameters such as scanning equipment [187, 188], image pre-processing [189], acquisition protocols [190, 191], image reconstruction algorithms [13, 192, 193], and delineation [194, 195] among others. These changes can subsequently impact the radiomic predictive models. In lung cancer, the diagnostic performance of a radiomic signature for solitary pulmonary nodules fluctuates based on slice thickness, contrast enhancement, and the convolutional kernel [196]. Changes in pixel resolution and contrast injection rates decreased the proportion of reproducible features in liver cancer [197]. Reproducibility testing is becoming more routine in the radiomic biomarker identification process [187, 198,199,200,201,202,203]. Associations such as the Quantitative Imaging Biomarker Alliance have begun to advocate for the technical standardization of patient scans to help ensure inter- and intra-machine reproducibility of imaging features [204, 205].
Tumor heterogeneity
From the biological perspective, radiogenomic studies rely on information derived from a biopsy to serve as a gold standard. In addition to being invasive, biopsies suffer from a bias where it is assumed that the sample reflects entire tumor burden. Tumor heterogeneity poses a serious challenge to this approach and the clinical decisions based on them. Radiogenomics aims to bypass both the issue of invasiveness and the sampling bias by using non-invasive radiological images to analyze the full tumor burden. If predictive radiogenomic models are built using biopsies where the sampling bias is passed on, one could argue that the second objective has yet to be achieved. This is a critical challenge for radiogenomics as the reliability of predictive models is dictated by the credibility of ground truth biological data. The next generation of radiogenomic research has become more acutely aware of this where Hu et al. and Stoyanova et al. extracted radiomic features only from the biopsy sites in brain and prostate tumors, respectively [47, 182, 183]. Better radiomic–biological correlations are built with such an approach and would be the next step forward in identifying robust radiogenomic features.
Need for multidisciplinarity
The difference of approach to radiomics, seen between clinical and technical researchers, should also be taken into consideration. Groups that are more clinically oriented tend to look at problems from a very clinical perspective, often at the sacrifice of the methodology. This would explain the continued presence of simple correlative radiogenomic studies despite numerous methodological disadvantages, such as multiple comparison errors, difficulty to make decisions based on a feature, and lack of robustness. Conversely, highly technical groups often tend to be driven by the development of novel methodologies, whereas the clinical relevance is of secondary importance. Due to limited direct translational potential, technical studies often suffer from being limited to a niche. Better inter-disciplinary collaboration will help bring about technically novel research that serves a greater clinical impact—to the benefit of everyone involved.
Future directions
The technical challenges listed in the previous section can be mitigated, to varying degrees, with the implementation of novel artificial intelligence techniques.
Deep learning radiomics
As highlighted earlier, the radiomics pipeline currently exists in a loosely dichotomous state between the two different approaches in radiomics. Classical/conventional radiomics relies on tumor delineations followed by the extraction of predefined handcrafted imaging features. Early radiomics research has been hindered by a lack of reproducibility partly due to different extraction algorithms being used to derive the features. Deep learning neural networks, specifically CNNs, have enjoyed significantly increased interest in medical imaging analysis. CNNs are capable of “learning” important features from within the image directly without needing to manually define them. The added advantage of CNNs is that the classification process, where the extracted features are linked to each other as well as the desired outcomes, is fully automated.
Deep learning is not without its own set of challenges. As the entire process of feature extraction and classification takes place within the same network, a great number of samples are needed to build robust models with satisfactory performance. For purposes like facial recognition, deep learning models are ordinarily trained on datasets numbering in the tens of thousands. However, in oncological imaging, the availability of standardized imaging data suitable for AI purposes remains rather limited. In this review, the overwhelming majority of radiogenomic studies had low sample sizes (n < 100). Data augmentation strategies that are optimized for medical images need to be developed to overcome this limitation [206].
Another concern raised by researchers using this newer generation radiomics pipeline is the fear of an “artificial intelligence black box” where even neural network architects are unsure how the most relevant features are selected and the predictions are made. Regardless of accuracy, clinicians are unlikely to embrace a technology that requires blind faith.
Various approaches have been proposed to shed light on this black box. Saliency mapping has gained attention in AI research, where the impact of each individual pixel on the prediction is measured and “areas of importance” for the prediction of the neural network are visualized [207]. This effectively generates a heat-map highlighting where in the image the model bases its prediction. An alternative approach put forth was the decoupling of the segmentation and classification tasks into two different neural networks [208]. This would allow the clinician to inspect and confirm the automatically segmented area prior to the feature extraction and subsequent diagnosis/prediction.
Automated segmentation
Tumor delineation is considered a bottleneck in the radiomics pipeline [209], as it can only be reliably performed by experienced radiologists, who are already burdened with clinical duties. AI can address this problem in two ways: automatic segmentation and deep learning. Automatic segmentation uses the algorithm’s ability to detect patterns to delineate structures, pathological, or otherwise. These automatically segmented areas would then have their features extracted and would flow into the next step of the radiomics pipeline. This approach has the added advantage of minimizing inter(/intra)-observer variability—where obtaining agreement on the delineations is notoriously difficult [210].
Another way the delineation bottleneck can be bypassed is with the use of convolutional neural networks in image processing. The network can either process the entire image to detect “global” imaging markers on the whole image or, if a region of interest is needed, the lesion is simply “pointed out” as opposed to being fully delineated. Within a convolutional neural network, feature extraction/selection happens automatically, on a much grander scale than any number of handcrafted features, and enjoys consistent optimization with each iteration. The malleability of these networks allows for the construction of more complex, robust, and generalizable architectures which can correct for known biases.
Experimental radiology
While the overwhelming majority of radiogenomic research is performed on routine clinical scans, there is a limit on the type of analyses that can be performed on patient-derived obtained tissue samples and patient scans. As in the case of fundamental oncology, preclinical experiments may also be advantageous considering that the whole tumor burden can be modulated, excised, and studied [211]. There is still a debate on the usefulness of preclinical models in the drug development process especially considering the differences in physiology, tumor heterogeneity, and disease progression. However, preclinical tumor models may prove to be a valuable development platform for imaging protocols dedicated to specific biological situations, for example, oxygenation that might not be readily induced in a human subject.
As our understanding of imaging markers improves, preclinical experiments can help identify better radiological–biological correlates to help provide non-invasive insight into the tumor biology. Once the inner workings of the neural networks are better elucidated, we may transcend the need to constantly link the imaging marker back to a biological parameter.
Integration systems in healthcare
Radiomic predictive models have the potential to assist clinical teams make more precise diagnoses, more rapidly, with less time needed to be spent on each scan. In addition to patient stratification, radiogenomics could potentially have a major impact on selection of candidates for targeted therapies where expression of the target molecule can be measured non-invasively for the entire tumor burden, without having to rely on a single biopsy to represent all the cancer lesions within a patient. Before this can happen though, a number of challenges and growth opportunities need to be addressed.
As mentioned in the brain section, most of the research performed in radiogenomics was exploratory or proof-of-concept in nature using simple methods on single-center data. Large-scale multicenter projects are needed to identify reproducible radiomic features that might be not only scanner/protocol/hospital independent but ultimately tumor agnostic. Artificial intelligence provides a unique opportunity to not only extract more meaningful features and create better predictive models but also to integrate multiple data sources. A number of projects have begun to see the value of combining complementary information, such as radiomics and genomics, to boost predictive performance [114, 115, 137]. Within such an integration system, a future could be envisioned where computational biologists would work in close collaboration with radiologists to select the most suitable patient image, validate the region of interest generated by the AI prior to prediction, and lead discussions in the multidisciplinary tumor boards.
Conclusions
In this review, we endeavored to encapsulate all the major radiogenomic research and cover the challenges that lie ahead along with what we believe to be the future prospects. While the field of radiogenomics does have its roots in research performed decades ago, it is still very much in its infancy. Many challenges still need to be addressed, however, there has already been significant progress made across a number of tumor types. With the rise of artificial intelligence in medicine, especially deep learning, more complex models combining multiple data sources could overcome many of the challenges that stand between radiogenomics and clinical implementation. Radiologists need to embrace this new technology and adapt to the changes that it will bring to the clinical workflow.
References
Coroller TP, Bi WL, Huynh E, Abedalthagafi M, Aizer AA, Greenwald NF, Parmar C, Narayan V, Wu WW, de Moura SMJPo (2017) Radiographic prediction of meningioma grade by semantic and radiomic features. 12 (11):e0187908
Yip SS, Liu Y, Parmar C, Li Q, Liu S, Qu F, Ye Z, Gillies RJ, Aerts HJ (2017) Associations between radiologist-defined semantic and automatically computed radiomic features in non-small cell lung cancer. Scientific reports 7 (1):3519
Gillies RJ, Kinahan PE, Hricak H (2016) Radiomics: Images Are More than Pictures, They Are Data. Radiology 278 (2):563-577. https://doi.org/10.1148/radiol.2015151169
Aerts HJ, Velazquez ER, Leijenaar RT, Parmar C, Grossmann P, Carvalho S, Bussink J, Monshouwer R, Haibe-Kains B, Rietveld D, Hoebers F, Rietbergen MM, Leemans CR, Dekker A, Quackenbush J, Gillies RJ, Lambin P (2014) Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nature communications 5:4006. https://doi.org/10.1038/ncomms5006
Court LE, Rao A, Krishnan S (2016) Radiomics in cancer diagnosis, cancer staging, and prediction of response to treatment. Translational cancer research 5 (4):337-339
Rutman AM, Kuo MD (2009) Radiogenomics: creating a link between molecular diagnostics and diagnostic imaging. European journal of radiology 70 (2):232-241. https://doi.org/10.1016/j.ejrad.2009.01.050
Kang J, Rancati T, Lee S, Oh JH, Kerns SL, Scott JG, Schwartz R, Kim S, Rosenstein BS (2018) Machine Learning and Radiogenomics: Lessons Learned and Future Directions. Frontiers in oncology 8:228. https://doi.org/10.3389/fonc.2018.00228
Peeken JC, Bernhofer M, Wiestler B, Goldberg T, Cremers D, Rost B, Wilkens JJ, Combs SE, Nusslin F (2018) Radiomics in radiooncology - Challenging the medical physicist. Physica medica: PM: an international journal devoted to the applications of physics to medicine and biology: official journal of the Italian Association of Biomedical Physics (AIFB) 48:27-36. https://doi.org/10.1016/j.ejmp.2018.03.012
Park JE, Kim HS (2018) Radiomics as a Quantitative Imaging Biomarker: Practical Considerations and the Current Standpoint in Neuro-oncologic Studies. Nuclear medicine and molecular imaging 52 (2):99-108. https://doi.org/10.1007/s13139-017-0512-7
Zhang Y, Oikonomou A, Wong A, Haider MA, Khalvati F (2017) Radiomics-based Prognosis Analysis for Non-Small Cell Lung Cancer. Scientific reports 7:46349. https://doi.org/10.1038/srep46349
Shaikh F, Franc B, Allen E, Sala E, Awan O, Hendrata K, Halabi S, Mohiuddin S, Malik S, Hadley D, Shrestha R (2018) Translational Radiomics: Defining the Strategy Pipeline and Considerations for Application-Part 2: From Clinical Implementation to Enterprise. Journal of the American College of Radiology: JACR 15 (3 Pt B):543-549. https://doi.org/10.1016/j.jacr.2017.12.006
Ger RB, Zhou S, Chi P-CM, Goff DL, Zhang L, Lee HJ, Fuller CD, Howell RM, Li H, Stafford RJ Quantitative image feature variability amongst CT scanners with a controlled scan protocol. In: Medical Imaging 2018: Computer-Aided Diagnosis, 2018. International Society for Optics and Photonics, p 105751O
Kim H, Park CM, Lee M, Park SJ, Song YS, Lee JH, Hwang EJ, Goo JM (2016) Impact of reconstruction algorithms on CT radiomic features of pulmonary tumors: analysis of intra-and inter-reader variability and inter-reconstruction algorithm variability. PloS one 11 (10):e0164924
Lu L, Ehmke RC, Schwartz LH, Zhao B (2016) Assessing agreement between radiomic features computed for multiple CT imaging settings. PloS one 11 (12):e0166550
Paul R, Hawkins SH, Schabath MB, Gillies RJ, Hall LO, Goldgof DB (2018) Predicting malignant nodules by fusing deep features with classical radiomics features. Journal of medical imaging (Bellingham, Wash) 5 (1):011021. https://doi.org/10.1117/1.jmi.5.1.011021
Afshar P, Mohammadi A, Plataniotis KN, Oikonomou A, Benali HJapa (2018) From Hand-Crafted to Deep Learning-based Cancer Radiomics: Challenges and Opportunities.
Zhang B, He X, Ouyang F, Gu D, Dong Y, Zhang L, Mo X, Huang W, Tian J, Zhang SJCl (2017) Radiomic machine-learning classifiers for prognostic biomarkers of advanced nasopharyngeal carcinoma. 403:21-27
Parmar C, Grossmann P, Bussink J, Lambin P, Aerts HJWL (2015) Machine Learning methods for Quantitative Radiomic Biomarkers. Scientific reports 5:13087. https://doi.org/10.1038/srep13087. https://www.nature.com/articles/srep13087#supplementary-information
Parmar C, Grossmann P, Rietveld D, Rietbergen MM, Lambin P, Aerts HJJFio (2015) Radiomic machine-learning classifiers for prognostic biomarkers of head and neck cancer. 5:272
Li Z, Wang Y, Yu J, Guo Y, Cao W (2017) Deep Learning based Radiomics (DLR) and its usage in noninvasive IDH1 prediction for low grade glioma. Scientific reports 7 (1):5467. https://doi.org/10.1038/s41598-017-05848-2
Chaunzwa TL, Christiani DC, Lanuti M, Shafer A, Diao N, Mak RH, Aerts H (2018) A deep-learning radiomics model for predicting survival in early-stage non-small cell lung cancer. 36 (15_suppl):8528-8528. https://doi.org/10.1200/jco.2018.36.15_suppl.8528
Antropova N Deep Learning and Radiomics of Breast Cancer on DCE-MRI in Assessment of Malignancy and Response to Therapy.143. https://doi.org/10.6082/3jah-5j51
Wang H, Cruz-Roa A, Basavanhally A, Gilmore H, Shih N, Feldman M, Tomaszewski J, Gonzalez F, Madabhushi A (2014) Mitosis detection in breast cancer pathology images by combining handcrafted and convolutional neural network features. Journal of medical imaging (Bellingham, Wash) 1 (3):034003. https://doi.org/10.1117/1.jmi.1.3.034003
Aerts HJ (2016) The Potential of Radiomic-Based Phenotyping in Precision Medicine: A Review. JAMA oncology 2 (12):1636-1642. https://doi.org/10.1001/jamaoncol.2016.2631
Kalra M, Wang G, Orton CGJMp (2018) Radiomics in lung cancer: Its time is here. 45 (3):997-1000
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144 (5):646-674. https://doi.org/10.1016/j.cell.2011.02.013
Berger MF, Mardis ER (2018) The emerging clinical relevance of genomics in cancer medicine. Nat Rev Clin Oncol 15 (6):353-365. https://doi.org/10.1038/s41571-018-0002-6
Pereira CB, Leal MF, de Souza CR, Montenegro RC, Rey JA, Carvalho AA, Assumpcao PP, Khayat AS, Pinto GR, Demachki S, de Arruda Cardoso Smith M, Burbano RR (2013) Prognostic and predictive significance of MYC and KRAS alterations in breast cancer from women treated with neoadjuvant chemotherapy. PloS one 8 (3):e60576. https://doi.org/10.1371/journal.pone.0060576
Cox J, Weinman S (2016) Mechanisms of doxorubicin resistance in hepatocellular carcinoma. Hepat Oncol 3 (1):57-59. https://doi.org/10.2217/hep.15.41
Cheon DJ, Orsulic S (2014) Ten-gene biomarker panel: a new hope for ovarian cancer? Biomark Med 8 (4):523-526. https://doi.org/10.2217/bmm.14.16
Chan TA, Yarchoan M, Jaffee E, Swanton C, Quezada SA, Stenzinger A, Peters S (2019) Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann Oncol 30 (1):44-56. https://doi.org/10.1093/annonc/mdy495
Goodman AM, Kato S, Bazhenova L, Patel SP, Frampton GM, Miller V, Stephens PJ, Daniels GA, Kurzrock R (2017) Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol Cancer Ther 16 (11):2598-2608. https://doi.org/10.1158/1535-7163.mct-17-0386
Efremova M, Finotello F, Rieder D, Trajanoski Z (2017) Neoantigens Generated by Individual Mutations and Their Role in Cancer Immunity and Immunotherapy. Front Immunol 8:1679. https://doi.org/10.3389/fimmu.2017.01679
Yarchoan M, Johnson BA, 3rd, Lutz ER, Laheru DA, Jaffee EM (2017) Targeting neoantigens to augment antitumour immunity. Nat Rev Cancer 17 (4):209-222. https://doi.org/10.1038/nrc.2016.154
Diehn M, Nardini C, Wang DS, McGovern S, Jayaraman M, Liang Y, Aldape K, Cha S, Kuo MD (2008) Identification of noninvasive imaging surrogates for brain tumor gene-expression modules. Proc Natl Acad Sci U S A 105 (13):5213-5218. https://doi.org/10.1073/pnas.0801279105
Colen RR, Mahajan B, Jolesz FA, Zinn PO (2011) Radiogenomic mapping in GBM in patients with high versus low edema/tumor infiltration using an image-genomic analysis of 12,764 genes and 555 micrornas. Neuro-oncology 3):iii142-iii143. doi:http://dx.doi.org/10.1093/neuonc/nor162
Zinn PO, Mahajan B, Sathyan P, Singh SK, Majumder S, Jolesz FA, Colen RR (2011) Radiogenomic mapping of edema/cellular invasion MRI-phenotypes in glioblastoma multiforme. PloS one 6 (10):e25451. https://doi.org/10.1371/journal.pone.0025451
Zhao L, Lee VH, Ng MK, Yan H, Bijlsma MFJBib (2018) Molecular subtyping of cancer: current status and moving toward clinical applications.
Yang D, Rao G, Martinez J, Veeraraghavan A, Rao A (2015) Evaluation of tumor-derived MRI-texture features for discrimination of molecular subtypes and prediction of 12-month survival status in glioblastoma. Medical physics 42 (11):6725-6735. https://doi.org/10.1118/1.4934373
Czarnek NM, Clark K, Peters KB, Collins LM, Mazurowski MA Radiogenomics of glioblastoma: A pilot multi-institutional study to investigate a relationship between tumor shape features and tumor molecular subtype. In: Tourassi GD, Armato SG (eds), 2016. SPIE. https://doi.org/10.1117/12.2217084
Mazurowski MA, Clark K, Czarnek NM, Shamsesfandabadi P, Peters KB, Saha A (2017) Radiogenomics of lower-grade glioma: algorithmically-assessed tumor shape is associated with tumor genomic subtypes and patient outcomes in a multi-institutional study with The Cancer Genome Atlas data. Journal of neuro-oncology 133 (1):27-35. https://doi.org/10.1007/s11060-017-2420-1
Grossmann P, Gutman DA, Dunn WD, Jr., Holder CA, Aerts HJ (2016) Imaging-genomics reveals driving pathways of MRI derived volumetric tumor phenotype features in Glioblastoma. BMC cancer 16:611. https://doi.org/10.1186/s12885-016-2659-5
Gutman DA, Dunn WD, Jr., Grossmann P, Cooper LA, Holder CA, Ligon KL, Alexander BM, Aerts HJ (2015) Somatic mutations associated with MRI-derived volumetric features in glioblastoma. Neuroradiology 57 (12):1227-1237. https://doi.org/10.1007/s00234-015-1576-7
Gevaert O, Mitchell L, Achrol A, Xu J, Steinberg G, Cheshier S, Napel S, Zaharchuk G, Plevritis S (2013) Creating a radiogenomics map of multi-omics and quantitative image features in glioblastoma multiforme. Neuro-oncology 3):iii140-iii141. doi:http://dx.doi.org/10.1093/neuonc/not183
Gevaert O, Mitchell LA, Achrol AS, Xu J, Echegaray S, Steinberg GK, Cheshier SH, Napel S, Zaharchuk G, Plevritis SK (2014) Glioblastoma multiforme: exploratory radiogenomic analysis by using quantitative image features. Radiology 273 (1):168-174. https://doi.org/10.1148/radiol.14131731
Zinn PO, Singh SK, Kotrotsou A, Abrol S, Thomas G, Mosley J, Elakkad A, Hassan I, Kumar A, Colen RR (2017) Distinct Radiomic Phenotypes Define Glioblastoma TP53-PTEN-EGFR Mutational Landscape. Neurosurgery 64 (CN_suppl_1):203-210. https://doi.org/10.1093/neuros/nyx316
Hu LS, Ning S, Eschbacher JM, Baxter LC, Gaw N, Ranjbar S, Plasencia J, Dueck AC, Peng S, Smith KA, Nakaji P, Karis JP, Quarles CC, Wu T, Loftus JC, Jenkins RB, Sicotte H, Kollmeyer TM, O’Neill BP, Elmquist W, Hoxworth JM, Frakes D, Sarkaria J, Swanson KR, Tran NL, Li J, Mitchell JR (2017) Radiogenomics to characterize regional genetic heterogeneity in glioblastoma. Neuro-oncology 19 (1):128-137. https://doi.org/10.1093/neuonc/now135
Hassan I, Kotrotsou A, Matsuoka CK, Alfaro-Munoz K, Elshafeey N, Zinn P, De Groot J, Colen R (2017) Increased mutation burden (Hypermutation) in gliomas is associated with a unique radiomic texture signature in magnetic resonance imaging. Neuro-oncology 19 (Supplement 6):vi147-vi148. doi:http://dx.doi.org/10.1093/neuonc/nox168
Miller JJ, Shih HA, Andronesi OC, Cahill DP (2017) Isocitrate dehydrogenase-mutant glioma: Evolving clinical and therapeutic implications. Cancer 123 (23):4535-4546. https://doi.org/10.1002/cncr.31039
Wang Y, Zhang T, Li S, Fan X, Ma J, Wang L, Jiang T (2015) Anatomical localization of isocitrate dehydrogenase 1 mutation: a voxel-based radiographic study of 146 low-grade gliomas. European journal of neurology 22 (2):348-354. https://doi.org/10.1111/ene.12578
Eichinger P, Alberts E, Delbridge C, Trebeschi S, Valentinitsch A, Bette S, Huber T, Gempt J, Meyer B, Schlegel J, Zimmer C, Kirschke JS, Menze BH, Wiestler B (2017) Diffusion tensor image features predict IDH genotype in newly diagnosed WHO grade II/III gliomas. Scientific reports 7 (1):13396. https://doi.org/10.1038/s41598-017-13679-4
Hsieh KL, Chen CY, Lo CM (2017) Radiomic model for predicting mutations in the isocitrate dehydrogenase gene in glioblastomas. Oncotarget 8 (28):45888-45897. https://doi.org/10.18632/oncotarget.17585
Lohmann P, Lerche C, Bauer E, Steger J, Stoffels G, Filss CP, Stegmayr C, Neumaier B, Shah NJ, Langen K, Galldiks N (2017) Predicting isocitrate dehydrogenase genotype in malignant glioma using fet pet radiomics. Neuro-oncology 19 (Supplement 3):iii88-iii89. doi:http://dx.doi.org/10.1093/neuonc/nox036
Lohmann P, Lerche C, Bauer EK, Steger J, Stoffels G, Blau T, Dunkl V, Kocher M, Viswanathan S, Filss CP, Stegmayr C, Neumaier B, Shah NJ, Fink GR, Langen KJ, Galldiks N (2018) Radiomics for prediction of the IDH genotype in gliomas. NuklearMedizin 57 (2):A36. doi:http://dx.doi.org/10.1055/s00839473
Bisdas S, Shen H, Thust S, Katsaros V, Stranjalis G, Boskos C, Brandner S, Zhang J (2018) Texture analysis- and support vector machine-assisted diffusional kurtosis imaging may allow in vivo gliomas grading and IDH-mutation status prediction: a preliminary study. Scientific reports 8 (1):6108. https://doi.org/10.1038/s41598-018-24438-4
Hong EK, Choi SH, Shin DJ, Jo SW, Yoo RE, Kang KM, Yun TJ, Kim JH, Sohn CH, Park SH, Won JK, Kim TM, Park CK, Kim IH, Lee ST (2018) Radiogenomics correlation between MR imaging features and major genetic profiles in glioblastoma. European radiology. https://doi.org/10.1007/s00330-018-5400-8
Zhang X, Tian Q, Wu YX, Xu XP, Li BJ, Liu YX, Liu Y, Lu HB IDH mutation assessment of glioma using texture features of multimodal MR images. In: Petrick NA, Armato SG (eds), 2017. SPIE. https://doi.org/10.1117/12.2254212
Arita H, Kinoshita M, Kawaguchi A, Takahashi M, Narita Y, Terakawa Y, Tsuyuguchi N, Okita Y, Nonaka M, Moriuchi S, Takagaki M, Fujimoto Y, Fukai J, Izumoto S, Ishibashi K, Nakajima Y, Shofuda T, Kanematsu D, Yoshioka E, Kodama Y, Mano M, Mori K, Ichimura K, Kanemura Y (2018) Lesion location implemented magnetic resonance imaging radiomics for predicting IDH and TERT promoter mutations in grade II/III gliomas. Scientific reports 8 (1):11773. https://doi.org/10.1038/s41598-018-30273-4
Jakola AS, Zhang YH, Skjulsvik AJ, Solheim O, Bo HK, Berntsen EM, Reinertsen I, Gulati S, Forander P, Brismar TB (2018) Quantitative texture analysis in the prediction of IDH status in low-grade gliomas. Clinical neurology and neurosurgery 164:114-120. https://doi.org/10.1016/j.clineuro.2017.12.007
Papp L, Poetsch N, Grahovac M, Mitterhauser M, Wadsak W, Beyer T, Hacker M, Traub-Weidinger T (2018) Prediction of IDH1-R132H mutation status of glioma patients from 11-C-Methionine-PET radiomics features utilizing machine learning approaches. NuklearMedizin 57 (2):A78. doi:http://dx.doi.org/10.1055/s00839473
Zhang X, Tian Q, Wang L, Liu Y, Li B, Liang Z, Gao P, Zheng K, Zhao B, Lu H (2018) Radiomics Strategy for Molecular Subtype Stratification of Lower-Grade Glioma: Detecting IDH and TP53 Mutations Based on Multimodal MRI. Journal of magnetic resonance imaging: JMRI. https://doi.org/10.1002/jmri.25960
Shofty B, Artzi M, Ben Bashat D, Liberman G, Haim O, Kashanian A, Bokstein F, Blumenthal DT, Ram Z, Shahar T (2018) MRI radiomics analysis of molecular alterations in low-grade gliomas. International journal of computer assisted radiology and surgery 13 (4):563-571. https://doi.org/10.1007/s11548-017-1691-5
Van Der Voort SR, Gahrmann R, Van Den Bent MJ, Vincent AJPE, Niessen WJ, Smits M, Klein S Radiogenomic classification of the 1p/19q status in presumed low-grade gliomas. In, 2017. IEEE Computer Society, pp 638-641. https://doi.org/10.1109/isbi.2017.7950601
Yu J, Shi Z, Lian Y, Li Z, Liu T, Gao Y, Wang Y, Chen L, Mao Y (2017) Noninvasive IDH1 mutation estimation based on a quantitative radiomics approach for grade II glioma. European radiology 27 (8):3509-3522. https://doi.org/10.1007/s00330-016-4653-3
Zhou H, Vallieres M, Bai HX, Su C, Tang H, Oldridge D, Zhang Z, Xiao B, Liao W, Tao Y, Zhou J, Zhang P, Yang L (2017) MRI features predict survival and molecular markers in diffuse lower-grade gliomas. Neuro-oncology 19 (6):862-870. https://doi.org/10.1093/neuonc/now256
Boots-Sprenger SHE, Sijben A, Rijntjes J, Tops BBJ, Idema AJ, Rivera AL, Bleeker FE, Gijtenbeek AM, Diefes K, Heathcock L, Aldape KD, Jeuken JWM, Wesseling P (2013) Significance of complete 1p/19q co-deletion, IDH1 mutation and MGMT promoter methylation in gliomas: use with caution. Modern Pathology 26:922. https://doi.org/10.1038/modpathol.2012.166
Li Y, Liu X, Xu K, Qian Z, Wang K, Fan X, Li S, Wang Y, Jiang T (2018) MRI features can predict EGFR expression in lower grade gliomas: A voxel-based radiomic analysis. European radiology 28 (1):356-362. https://doi.org/10.1007/s00330-017-4964-z
Kickingereder P, Bonekamp D, Nowosielski M, Kratz A, Sill M, Burth S, Wick A, Eidel O, Schlemmer HP, Radbruch A, Debus J, Herold-Mende C, Unterberg A, Jones D, Pfister S, Wick W, von Deimling A, Bendszus M, Capper D (2016) Radiogenomics of Glioblastoma: Machine Learning-based Classification of Molecular Characteristics by Using Multiparametric and Multiregional MR Imaging Features. Radiology 281 (3):907-918. https://doi.org/10.1148/radiol.2016161382
Akbari H, Bakas S, Pisapia JM, Nasrallah MP, Rozycki M, Martinez-Lage M, Morrissette JJD, Dahmane N, O’Rourke DM, Davatzikos C (2018) In vivo evaluation of EGFRvIII mutation in primary glioblastoma patients via complex multiparametric MRI signature. Neuro-oncology 20 (8):1068-1079. https://doi.org/10.1093/neuonc/noy033
Lee J, Narang S, Martinez JJ, Rao G, Rao A (2015) Associating spatial diversity features of radiologically defined tumor habitats with epidermal growth factor receptor driver status and 12-month survival in glioblastoma: methods and preliminary investigation. Journal of medical imaging (Bellingham, Wash) 2 (4):041006. https://doi.org/10.1117/1.jmi.2.4.041006
Cho H, Hong B, Park C, Park S, Choi S (2017) Is BCAT1 a new MR imaging-related biomarker for prognosis prediction in IDH1-wildtype glioblastoma patients?: Radiogenomics study. Neuro-oncology 19 (Supplement 3):iii41. doi:http://dx.doi.org/10.1093/neuonc/nox036
Maraka S, Kotrotsou A, Abrol S, Hassan A, Elshafeey N, Starostina O, Alfaro-Munoz K, Colen R, De Groot J (2017) Radiomic analysis on apparent diffusion coefficient (ADC) maps predicts platelet-derived growth factor receptor alpha (PDGFRA) gene amplification for newly diagnosed glioblastoma patients. Neuro-oncology 19 (Supplement 6):vi148. doi:http://dx.doi.org/10.1093/neuonc/nox168
Li Y, Liu X, Qian Z, Sun Z, Xu K, Wang K, Fan X, Zhang Z, Li S, Wang Y, Jiang T (2018) Genotype prediction of ATRX mutation in lower-grade gliomas using an MRI radiomics signature. European radiology 28 (7):2960-2968. https://doi.org/10.1007/s00330-017-5267-0
Beig N, Patel J, Prasanna P, Partovi S, Varadan V, Madabhushi A, Tiwari P Radiogenomic analysis of hypoxia pathway reveals computerized MRI descriptors predictive of overall survival in glioblastoma. In: Petrick NA, Armato SG (eds), 2017. SPIE. https://doi.org/10.1117/12.2255694
Li Y, Qian Z, Xu K, Wang K, Fan X, Li S, Liu X, Wang Y, Jiang T (2017) Radiomic features predict Ki-67 expression level and survival in lower grade gliomas. Journal of neuro-oncology 135 (2):317-324. https://doi.org/10.1007/s11060-017-2576-8
Jeon H, Cho HR, Park CK, Park SH, Kumarir N, Thakur N, Chung J, Choi SH (2017) CD49D correlated with apparent diffusion coefficient as a promising biomarker for prognosis prediction of glioblastoma: Radiogenomics study. Neuro-oncology 19 (Supplement 6):vi157. doi:http://dx.doi.org/10.1093/neuonc/nox168
Narang S, Kim D, Aithala S, Heimberger AB, Ahmed S, Rao D, Rao G, Rao A (2017) Tumor image-derived texture features are associated with CD3 T-cell infiltration status in glioblastoma. Oncotarget 8 (60):101244-101254. https://doi.org/10.18632/oncotarget.20643
Lehrer M, Bhadra A, Ravikumar V, Chen JY, Wintermark M, Hwang SN, Holder CA, Huang EP, Fevrier-Sullivan B, Freymann JB, Rao A (2017) Multiple-response regression analysis links magnetic resonance imaging features to de-regulated protein expression and pathway activity in lower grade glioma. Oncoscience 4 (5-6):57-66. https://doi.org/10.18632/oncoscience.353
Rathore S, Akbari H, Rozycki M, Abdullah KG, Nasrallah MP, Binder ZA, Davuluri RV, Lustig RA, Dahmane N, Bilello M, O’Rourke DM, Davatzikos C (2018) Radiomic MRI signature reveals three distinct subtypes of glioblastoma with different clinical and molecular characteristics, offering prognostic value beyond IDH1. Scientific reports 8 (1):5087. https://doi.org/10.1038/s41598-018-22739-2
Li ZC, Bai H, Sun Q, Li Q, Liu L, Zou Y, Chen Y, Liang C, Zheng H (2018) Multiregional radiomics features from multiparametric MRI for prediction of MGMT methylation status in glioblastoma multiforme: A multicentre study. European radiology 28 (9):3640-3650. https://doi.org/10.1007/s00330-017-5302-1
Bi WL, Corroller T, Greenwald NF, Huynh E, Aizer MAA, Santagata S, Al-Mefty O, Alexander B, Dunn IF, Huang R, Aerts H (2017) Radiographic prediction of meningioma grade and genomic profile. Journal of Neurological Surgery Part B: Skull Base Conference: 27th Annual Meeting North American Skull Base Society United States 78 (Supplement 1). doi:http://dx.doi.org/10.1055/s-0037-1600633
Coroller T, Bi W, Greenwald N, Zeleznik R, Huynh E, Parmar C, Huang R, Aerts H (2018) Predicting meningioma tumor recurrence using radiogenomics data. Medical physics 45 (6):e678. doi:http://dx.doi.org/10.1002/mp.12938
Dasgupta A, Gupta T, Pungavkar S, Janu A, Shirsat N, Chinnaswamy G, Jalali R (2014) Can we predict molecular subtypes of medulloblastoma based on MRI? Encouraging data from a blinded study. Journal of Cancer Research and Therapeutics 1):S5-S6
Brisse HJ, Blanc T, Schleiermacher G, Mosseri V, Philippe-Chomette P, Janoueix-Lerosey I, Pierron G, Lapouble E, Peuchmaur M, Freneaux P, Galmiche L, Algret N, Peycelon M, Michon J, Delattre O, Sarnacki S (2017) Radiogenomics of neuroblastomas: Relationships between imaging phenotypes, tumor genomic profile and survival. PloS one 12 (9):e0185190. https://doi.org/10.1371/journal.pone.0185190
Sun YW, Xu J, Zhou J, Liu WJ (2018) Targeted drugs for systemic therapy of lung cancer with brain metastases. Oncotarget 9 (4):5459-5472. https://doi.org/10.18632/oncotarget.23616
Chan BA, Hughes BG (2015) Targeted therapy for non-small cell lung cancer: current standards and the promise of the future. Transl Lung Cancer Res 4 (1):36-54. https://doi.org/10.3978/j.issn.2218-6751.2014.05.01
Roman M, Baraibar I, Lopez I, Nadal E, Rolfo C, Vicent S, Gil-Bazo I (2018) KRAS oncogene in non-small cell lung cancer: clinical perspectives on the treatment of an old target. Mol Cancer 17 (1):33. https://doi.org/10.1186/s12943-018-0789-x
De Jong EEC, Van Elmpt W, Hendriks LEL, Leijenaar RTH, Dingemans AMC, Lambin P (2016) Radiomic CT features for evaluation of EGFR and KRAS mutation status in patients with advanced NSCLC. Radiotherapy and Oncology 119 (Supplement 1):S290-S291
Dagogo-Jack I, Shaw ATJTo (2016) Screening for ALK rearrangements in lung cancer: time for a new generation of diagnostics? 21 (6):662-663
Gevaert O, Xu J, Hoang CD, Leung AN, Xu Y, Quon A, Rubin DL, Napel S, Plevritis SK (2012) Non-small cell lung cancer: identifying prognostic imaging biomarkers by leveraging public gene expression microarray data--methods and preliminary results. Radiology 264 (2):387-396. https://doi.org/10.1148/radiol.12111607
Halpenny DF, Riely GJ, Hayes S, Yu H, Zheng J, Moskowitz CS, Ginsberg MS (2014) Are there imaging characteristics associated with lung adenocarcinomas harboring ALK rearrangements? Lung cancer (Amsterdam, Netherlands) 86 (2):190-194. https://doi.org/10.1016/j.lungcan.2014.09.007
Yoon HJ, Sohn I, Cho JH, Lee HY, Kim JH, Choi YL, Kim H, Lee G, Lee KS, Kim J (2015) Decoding Tumor Phenotypes for ALK, ROS1, and RET Fusions in Lung Adenocarcinoma Using a Radiomics Approach. Medicine 94 (41):e1753. https://doi.org/10.1097/md.0000000000001753
Caramella C, Bluthgen MV, Rosellini S, Leduc C, Facchinetti F, Haspinger E, Ferte C, Michiels S, Soria JC, Besse B (2015) Prognostic value of texture analysis and correlation with molecular profile in EGFR mutated/ALK rearranged advanced non-small cell lung cancer (NSCLC). European Journal of Cancer 3):S647-S648
Aerts HJ, Grossmann P, Tan Y, Oxnard GR, Rizvi N, Schwartz LH, Zhao B (2016) Defining a Radiomic Response Phenotype: A Pilot Study using targeted therapy in NSCLC. Scientific reports 6:33860. https://doi.org/10.1038/srep33860
Weiss GJ, Ganeshan B, Miles KA, Campbell DH, Cheung PY, Frank S, Korn RL (2014) Noninvasive image texture analysis differentiates K-ras mutation from pan-wildtype NSCLC and is prognostic. PloS one 9 (7):e100244. https://doi.org/10.1371/journal.pone.0100244
Rizzo S, Petrella F, Buscarino V, De Maria F, Raimondi S, Barberis M, Fumagalli C, Spitaleri G, Rampinelli C, De Marinis F, Spaggiari L, Bellomi M (2016) CT Radiogenomic Characterization of EGFR, K-RAS, and ALK Mutations in Non-Small Cell Lung Cancer. European radiology 26 (1):32-42. https://doi.org/10.1007/s00330-015-3814-0
Lv J, Zhang H, Ma J, Ma Y, Gao G, Song Z, Yang Y (2018) Comparison of CT radiogenomic and clinical characteristics between EGFR and KRAS mutations in lung adenocarcinomas. Clinical radiology 73 (6):590.e591-590.e598. https://doi.org/10.1016/j.crad.2018.01.009
Sorensen J, Erasmus Jr J, Shroff G, Rao A, Stingo F, Court L, Gold KA, Lee J, Heymach JV, Swisher S, Godoy M (2015) Combining CT texture analysis with semantic imaging descriptions for the radiogenomic detection of EGFR and KRAS mutations in NSCLC. Journal of Thoracic Oncology 2):S700
Rios Velazquez E, Parmar C, Liu Y, Coroller TP, Cruz G, Stringfield O, Ye Z, Makrigiorgos M, Fennessy F, Mak RH, Gillies R, Quackenbush J, Aerts H (2017) Somatic Mutations Drive Distinct Imaging Phenotypes in Lung Cancer. Cancer research 77 (14):3922-3930. https://doi.org/10.1158/0008-5472.can-17-0122
Yip SSF, Parmar C, Kim J, Huynh E, Mak RH, Aerts H (2017) Impact of experimental design on PET radiomics in predicting somatic mutation status. European journal of radiology 97:8-15. https://doi.org/10.1016/j.ejrad.2017.10.009
Yip SS, Kim J, Coroller TP, Parmar C, Velazquez ER, Huynh E, Mak RH, Aerts HJ (2017) Associations Between Somatic Mutations and Metabolic Imaging Phenotypes in Non-Small Cell Lung Cancer. Journal of nuclear medicine: official publication, Society of Nuclear Medicine 58 (4):569-576. https://doi.org/10.2967/jnumed.116.181826
Kim TJ, Lee CT, Jheon SH, Park JS, Chung JH (2016) Radiologic Characteristics of Surgically Resected Non-Small Cell Lung Cancer With ALK Rearrangement or EGFR Mutations. The Annals of thoracic surgery 101 (2):473-480. https://doi.org/10.1016/j.athoracsur.2015.07.062
Sawan P, Plodkowski AJ, Li AE, Li BT, Drilon A, Capanu M, Ginsberg MS (2018) CT features of HER2-mutant lung adenocarcinomas. Clinical imaging 51:279-283. https://doi.org/10.1016/j.clinimag.2018.05.028
Halpenny DF, Plodkowski A, Riely G, Zheng J, Litvak A, Moscowitz C, Ginsberg MS (2017) Radiogenomic evaluation of lung cancer - Are there imaging characteristics associated with lung adenocarcinomas harboring BRAF mutations? Clinical imaging 42:147-151. https://doi.org/10.1016/j.clinimag.2016.11.015
Ozkan E, West A, Dedelow JA, Chu BF, Zhao W, Yildiz VO, Otterson GA, Shilo K, Ghosh S, King M, White RD, Erdal BS (2015) CT Gray-Level Texture Analysis as a Quantitative Imaging Biomarker of Epidermal Growth Factor Receptor Mutation Status in Adenocarcinoma of the Lung. AJR American journal of roentgenology 205 (5):1016-1025. https://doi.org/10.2214/ajr.14.14147
Moon H, Choi JH, Park JH, Byun BH, Lim I, Kim BI, Choi CW, Lim SM (2015) Differences of < sup > 18 </sup > F-FDG PET tumor texture parameters according to the presence of epidermal growth factor receptor mutation in non-small cell lung cancer. Journal of Nuclear Medicine Conference: Society of Nuclear Medicine and Molecular Imaging Annual Meeting, SNMMI 56 (SUPPL. 3)
Zhou M, Leung A, Echegaray S, Gentles A, Shrager JB, Jensen KC, Berry GJ, Plevritis SK, Rubin DL, Napel S, Gevaert O (2018) Non-Small Cell Lung Cancer Radiogenomics Map Identifies Relationships between Molecular and Imaging Phenotypes with Prognostic Implications. Radiology 286 (1):307-315. https://doi.org/10.1148/radiol.2017161845
Gevaert O, Echegaray S, Khuong A, Hoang CD, Shrager JB, Jensen KC, Berry GJ, Guo HH, Lau C, Plevritis SK, Rubin DL, Napel S, Leung AN (2017) Predictive radiogenomics modeling of EGFR mutation status in lung cancer. Scientific reports 7:41674. https://doi.org/10.1038/srep41674
Sacconi B, Anzidei M, Leonardi A, Boni F, Saba L, Scipione R, Anile M, Rengo M, Longo F, Bezzi M, Venuta F, Napoli A, Laghi A, Catalano C (2017) Analysis of CT features and quantitative texture analysis in patients with lung adenocarcinoma: a correlation with EGFR mutations and survival rates. Clinical radiology 72 (6):443-450. https://doi.org/10.1016/j.crad.2017.01.015
Rios Velazquez E, Liu Y, Parmar C, Narayan V, Gillies R, Aerts H (2016) Radiomic CT features complement semantic annotations to predict EGFR mutations in lung adenocarcinomas. Medical physics 43 (6 PART2):3706
Jia T, Xiong J, Li X, Ma J, Ren Y, Xu Z, Cai X, Zhang J, Zhao J, Fu X (2017) Detecting epidermal growth factor receptor mutation status in patients with lung adenocarcinoma using radiomics and random forest. Journal of Thoracic Oncology 12 (11 Supplement 2):S1860
Clay R, Johnson T, Bartholmai BJ, Karwoski R, Maldonado F, Rajagopalan S, Peikert T (2018) Canary (computer aided nodule analysis and risk yield) as a radiologic biomarker to predict tumor response to EGFR-targeted therapy in adenocarcinoma of the lung. American Journal of Respiratory and Critical Care Medicine Conference: American Thoracic Society International Conference, ATS 197 (MeetingAbstracts)
Zhang L, Chen B, Liu X, Song J, Fang M, Hu C, Dong D, Li W, Tian J (2018) Quantitative Biomarkers for Prediction of Epidermal Growth Factor Receptor Mutation in Non-Small Cell Lung Cancer. Translational oncology 11 (1):94-101. https://doi.org/10.1016/j.tranon.2017.10.012
Grossmann P, Stringfield O, El-Hachem N, Bui MM, Rios Velazquez E, Parmar C, Leijenaar RT, Haibe-Kains B, Lambin P, Gillies RJ, Aerts HJ (2017) Defining the biological basis of radiomic phenotypes in lung cancer. eLife 6. https://doi.org/10.7554/elife.23421
Emaminejad N, Qian W, Guan Y, Tan M, Qiu Y, Liu H, Zheng B (2016) Fusion of Quantitative Image and Genomic Biomarkers to Improve Prognosis Assessment of Early Stage Lung Cancer Patients. IEEE Trans Biomed Eng 63 (5):1034-1043. https://doi.org/10.1109/tbme.2015.2477688
Boyd NF, Guo H, Martin LJ, Sun L, Stone J, Fishell E, Jong RA, Hislop G, Chiarelli A, Minkin S, Yaffe MJ (2007) Mammographic density and the risk and detection of breast cancer. N Engl J Med 356 (3):227-236. https://doi.org/10.1056/nejmoa062790
McCormack VA, dos Santos Silva I (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 15 (6):1159-1169. https://doi.org/10.1158/1055-9965.epi-06-0034
Li H, Giger ML, Lan L, Yuan Y, Bhooshan N, Olopade OI Effect of variable gain on computerized texture analysis on digitalized mammograms. In: Summers RM, Karssemeijer N (eds), 2010. SPIE. https://doi.org/10.1117/12.845321
Gierach GL, Li H, Loud JT, Greene MH, Chow CK, Lan L, Prindiville SA, Eng-Wong J, Soballe PW, Giambartolomei C, Mai PL, Galbo CE, Nichols K, Calzone KA, Olopade OI, Gail MH, Giger ML (2014) Relationships between computer-extracted mammographic texture pattern features and BRCA1/2 mutation status: a cross-sectional study. Breast cancer research: BCR 16 (4):424. https://doi.org/10.1186/preaccept-1744229618121391. https://doi.org/10.1186/s13058-014-0424-8
Li H, Giger ML, Lan L, Janardanan J, Sennett CA (2014) Comparative analysis of image-based phenotypes of mammographic density and parenchymal patterns in distinguishing between BRCA1/2 cases, unilateral cancer cases, and controls. Journal of medical imaging (Bellingham, Wash) 1 (3):031009. https://doi.org/10.1117/1.jmi.1.3.031009
Li H, Giger ML, Huynh BQ, Antropova NO (2017) Deep learning in breast cancer risk assessment: evaluation of convolutional neural networks on a clinical dataset of full-field digital mammograms. Journal of medical imaging (Bellingham, Wash) 4 (4):041304. https://doi.org/10.1117/1.jmi.4.4.041304
Yamamoto S, Maki DD, Korn RL, Kuo MD (2012) Radiogenomic analysis of breast cancer using MRI: a preliminary study to define the landscape. AJR American journal of roentgenology 199 (3):654-663. https://doi.org/10.2214/ajr.11.7824
Lee CH, Dershaw DD, Kopans D, Evans P, Monsees B, Monticciolo D, Brenner RJ, Bassett L, Berg W, Feig S (2010) Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. Journal of the American college of radiology 7 (1):18-27
Haspinger ER, Rosellini S, Ammari S, Dercle L, Bluthgen MV, Besse B, Caramella C, Massard C, Lacroix L, De Baere T, Deschamps F, Michiels S, Soria JC, Ferte C (2015) Radiomics to identify HER2 amplification or mutation in metastatic patients with solid tumors prospectively enrolled in MOSCATO-01. European Journal of Cancer 3):S101
Mazurowski MA, Zhang J, Grimm LJ, Yoon SC, Silber JI (2014) Radiogenomic analysis of breast cancer: luminal B molecular subtype is associated with enhancement dynamics at MR imaging. Radiology 273 (2):365-372. https://doi.org/10.1148/radiol.14132641
Grimm LJ, Zhang J, Mazurowski MA (2015) Computational approach to radiogenomics of breast cancer: Luminal A and luminal B molecular subtypes are associated with imaging features on routine breast MRI extracted using computer vision algorithms. Journal of magnetic resonance imaging: JMRI 42 (4):902-907. https://doi.org/10.1002/jmri.24879
Wang S, Fan M, Zhang J, Zheng B, Wang X, Li L Radiogenomic analysis of breast cancer: Dynamic contrast enhanced - Magnetic resonance imaging based features are associated with molecular subtypes. In: Cook TS, Zhang J (eds), 2016. SPIE. https://doi.org/10.1117/12.2217658
Saha A, Harowicz MR, Grimm LJ, Kim CE, Ghate SV, Walsh R, Mazurowski MA (2018) A machine learning approach to radiogenomics of breast cancer: a study of 922 subjects and 529 DCE-MRI features. British journal of cancer. https://doi.org/10.1038/s41416-018-0185-8
Wu J, Li B, Sun X, Cao G, Rubin DL, Napel S, Ikeda DM, Kurian AW, Li R (2017) Heterogeneous Enhancement Patterns of Tumor-adjacent Parenchyma at MR Imaging Are Associated with Dysregulated Signaling Pathways and Poor Survival in Breast Cancer. Radiology 285 (2):401-413. https://doi.org/10.1148/radiol.2017162823
Zhu Y, Li H, Guo W, Drukker K, Lan L, Giger ML, Ji Y (2015) Deciphering Genomic Underpinnings of Quantitative MRI-based Radiomic Phenotypes of Invasive Breast Carcinoma. Scientific reports 5:17787. https://doi.org/10.1038/srep17787
Li H, Zhu Y, Burnside ES, Drukker K, Hoadley KA, Fan C, Conzen SD, Whitman GJ, Sutton EJ, Net JM, Ganott M, Huang E, Morris EA, Perou CM, Ji Y, Giger ML (2016) MR Imaging Radiomics Signatures for Predicting the Risk of Breast Cancer Recurrence as Given by Research Versions of MammaPrint, Oncotype DX, and PAM50 Gene Assays. Radiology 281 (2):382-391. https://doi.org/10.1148/radiol.2016152110
Hutchinson L (2013) CLOVAR validates prognostic gene-expression signature. Nat Rev Clin Oncol 10:68. https://doi.org/10.1038/nrclinonc.2013.2
Winterhoff B, Hamidi H, Wang C, Kalli KR, Fridley BL, Dering J, Chen H-W, Cliby WA, Wang H-J, Dowdy SJGo (2016) Molecular classification of high grade endometrioid and clear cell ovarian cancer using TCGA gene expression signatures. 141 (1):95-100
Vargas HA, Huang EP, Lakhman Y, Ippolito JE, Bhosale P, Mellnick V, Shinagare AB, Anello M, Kirby J, Fevrier-Sullivan BJR (2017) Radiogenomics of high-grade serous ovarian cancer: multireader multi-institutional study from the Cancer Genome Atlas Ovarian Cancer Imaging Research Group. 285 (2):482-492
Anuradha S, Webb PM, Blomfield P, Brand AH, Friedlander M, Leung Y, Obermair A, Oehler MK, Quinn M, Steer CJMJoA (2014) Survival of Australian women with invasive epithelial ovarian cancer: a population‐based study. 201 (5):283-288
Lu H, Arshad M, Thornton A, Avesani G, Cunnea P, Curry E, Kanavati F, Liang J, Nixon K, Williams STJNc (2019) A mathematical-descriptor of tumor-mesoscopic-structure from computed-tomography images annotates prognostic-and molecular-phenotypes of epithelial ovarian cancer. 10 (1):764
Tamez-Pena JG, Rodriguez-Rojas JA, Gomez-Rueda H, Celaya-Padilla JM, Rivera-Prieto RA, Palacios-Corona R, Garza-Montemayor M, Cardona-Huerta S, Trevino V (2018) Radiogenomics analysis identifies correlations of digital mammography with clinical molecular signatures in breast cancer. PloS one 13 (3):e0193871. https://doi.org/10.1371/journal.pone.0193871
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68 (6):394-424. https://doi.org/10.3322/caac.21492
Tam K (2013) The roles of doxorubicin in hepatocellular carcinoma. ADMET and DMPK 1 (3):29-44
Kuo MD, Gollub J, Sirlin CB, Ooi C, Chen X (2007) Radiogenomic analysis to identify imaging phenotypes associated with drug response gene expression programs in hepatocellular carcinoma. Journal of vascular and interventional radiology: JVIR 18 (7):821-831. https://doi.org/10.1016/j.jvir.2007.04.031
West DL, Kotrotsou A, Niekamp AS, Idris T, Camejo DG, Mazal NJ, Cardenas NJ, Goldberg JL, Colen RR (2017) CT-based radiomic analysis of hepatocellular carcinoma patients to predict key genomic information. Journal of Clinical Oncology Conference 35 (15 Supplement 1)
Lim KC, Chow PK, Allen JC, Chia GS, Lim M, Cheow PC, Chung AY, Ooi LL, Tan SB (2011) Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Annals of surgery 254 (1):108-113. https://doi.org/10.1097/sla.0b013e31821ad884
Chou CT, Chen RC, Lee CW, Ko CJ, Wu HK, Chen YL (2012) Prediction of microvascular invasion of hepatocellular carcinoma by pre-operative CT imaging. The British journal of radiology 85 (1014):778-783. https://doi.org/10.1259/bjr/65897774
Chandarana H, Robinson E, Hajdu CH, Drozhinin L, Babb JS, Taouli B (2011) Microvascular invasion in hepatocellular carcinoma: is it predictable with pretransplant MRI? AJR American journal of roentgenology 196 (5):1083-1089. https://doi.org/10.2214/ajr.10.4720
Segal E, Sirlin CB, Ooi C, Adler AS, Gollub J, Chen X, Chan BK, Matcuk GR, Barry CT, Chang HY, Kuo MD (2007) Decoding global gene expression programs in liver cancer by noninvasive imaging. Nat Biotechnol 25 (6):675-680. https://doi.org/10.1038/nbt1306
Banerjee S, Wang DS, Kim HJ, Sirlin CB, Chan MG, Korn RL, Rutman AM, Siripongsakun S, Lu D, Imanbayev G, Kuo MD (2015) A computed tomography radiogenomic biomarker predicts microvascular invasion and clinical outcomes in hepatocellular carcinoma. Hepatology (Baltimore, Md) 62 (3):792-800. https://doi.org/10.1002/hep.27877
Tang H, Bai HX, Su C, Lee AM, Yang L (2016) The effect of cirrhosis on radiogenomic biomarker’s ability to predict microvascular invasion and outcome in hepatocellular carcinoma. Hepatology (Baltimore, Md) 64 (2):691-692. https://doi.org/10.1002/hep.28620
Simonetti RG, Camma C, Fiorello F, Politi F, D’Amico G, Pagliaro L (1991) Hepatocellular carcinoma. A worldwide problem and the major risk factors. Dig Dis Sci 36 (7):962-972
Davis GL, Dempster J, Meler JD, Orr DW, Walberg MW, Brown B, Berger BD, O’Connor JK, Goldstein RM (2008) Hepatocellular carcinoma: management of an increasingly common problem. Proc (Bayl Univ Med Cent) 21 (3):266-280
Aherne EA, Pak LM, Goldman DA, Gonen M, Jarnagin WR, Simpson AL, Do RK (2018) Intrahepatic cholangiocarcinoma: can imaging phenotypes predict survival and tumor genetics? Abdominal radiology (New York). https://doi.org/10.1007/s00261-018-1505-4
DeLeon T, Borad MJ, Wu T, Li J, Zwart CM, Yang G, Holeman S, Silva AC (2017) Utility of CT texture for identification of FGFR2 fusion in cholangiocarcinoma: A radiogenomic pilot study. Journal of Clinical Oncology Conference 35 (15 Supplement 1)
Gudbjartsson T, Thoroddsen A, Petursdottir V, Hardarson S, Magnusson J, Einarsson GV (2005) Effect of incidental detection for survival of patients with renal cell carcinoma: results of population-based study of 701 patients. Urology 66 (6):1186-1191. https://doi.org/10.1016/j.urology.2005.07.009
Cowey CL, Rathmell WK (2009) VHL gene mutations in renal cell carcinoma: role as a biomarker of disease outcome and drug efficacy. Curr Oncol Rep 11 (2):94-101
Zhang J, Zhang Q (2018) VHL and Hypoxia Signaling: Beyond HIF in Cancer. Biomedicines 6 (1). https://doi.org/10.3390/biomedicines6010035
Karlo CA, Di Paolo PL, Chaim J, Hakimi AA, Ostrovnaya I, Russo P, Hricak H, Motzer R, Hsieh JJ, Akin O (2014) Radiogenomics of clear cell renal cell carcinoma: associations between CT imaging features and mutations. Radiology 270 (2):464-471. https://doi.org/10.1148/radiol.13130663
Chen X, Zhou Z, Thomas K, Wang J (2016) Predicting gene mutations in renal cell carcinoma based on CT imaging features: Validation using TCGA-TCIA datasets. Medical physics 43 (6 PART2):3705
da Costa WH, da Cunha IW, Fares AF, Bezerra SM, Shultz L, Clavijo DA, da Silva DV, Netto GJ, Guimaraes GC, Cassio Zequi S (2018) Prognostic impact of concomitant loss of PBRM1 and BAP1 protein expression in early stages of clear cell renal cell carcinoma. Urol Oncol 36 (5):243 e241-243 e248. https://doi.org/10.1016/j.urolonc.2018.01.002
Wi YC, Moon A, Jung MJ, Kim Y, Bang SS, Jang K, Paik SS, Shin SJ (2018) Loss of Nuclear BAP1 Expression Is Associated with High WHO/ISUP Grade in Clear Cell Renal Cell Carcinoma. J Pathol Transl Med 52 (6):378-385. https://doi.org/10.4132/jptm.2018.09.21
Sohrabi S, Vikram R (2017) Correlation of CT derived textual features with mutational status of clear cell renal cell carcinoma-preliminary findings. Abdominal Radiology 42 (8):2030-2031. doi:http://dx.doi.org/10.1007/s00261-017-1192-6
Shinagare AB, Vikram R, Jaffe C, Akin O, Kirby J, Huang E, Freymann J, Sainani NI, Sadow CA, Bathala TK, Rubin DL, Oto A, Heller MT, Surabhi VR, Katabathina V, Silverman SG (2015) Radiogenomics of clear cell renal cell carcinoma: preliminary findings of The Cancer Genome Atlas-Renal Cell Carcinoma (TCGA-RCC) Imaging Research Group. Abdominal imaging 40 (6):1684-1692. https://doi.org/10.1007/s00261-015-0386-z
Winer AG, Hoetker A, Vacchio MJ, Zabor EC, Ostravnaya I, Russo P, Hsieh JJ, Akin O, Hakimi AA (2015) Radiogenomics of clear cell renal cell carcinoma: Associations between imaging, molecular alterations and pathologic features. Journal of Urology 1):e423
Vikram R, Ghosh P, Tamboli P, Rao A (2014) Image texture analysis to predict bap1 mutational status in patients with clear cell renal carcinoma. Abdominal imaging 39 (3):668. doi:http://dx.doi.org/10.1007/s00261-014-0161-6
Duddalwar V, Liang G, Siegmund K, Cen S, Varghese B, Hwang D, Desai B, Desai M, Aron M, Gill I (2018) Association of computed tomography-based radiomic features with epigenetic variation of clear cell renal cell carcinoma using dna methylation. Journal of Urology 199 (4 Supplement 1):e959
Guo F, Gong H, Zhao H, Chen J, Zhang Y, Zhang L, Shi X, Zhang A, Jin H, Zhang J, He Y (2018) Mutation status and prognostic values of KRAS, NRAS, BRAF and PIK3CA in 353 Chinese colorectal cancer patients. Scientific reports 8 (1):6076. https://doi.org/10.1038/s41598-018-24306-1
Irahara N, Baba Y, Nosho K, Shima K, Yan L, Dias-Santagata D, Iafrate AJ, Fuchs CS, Haigis KM, Ogino S (2010) NRAS mutations are rare in colorectal cancer. Diagn Mol Pathol 19 (3):157-163. https://doi.org/10.1097/pdm.0b013e3181c93fd1
Fernández-Medarde A, Santos E (2011) Ras in Cancer and Developmental Diseases. Genes & Cancer 2 (3):344-358. https://doi.org/10.1177/1947601911411084
Zhang J, Zheng J, Yang Y, Lu J, Gao J, Lu T, Sun J, Jiang H, Zhu Y, Zheng Y, Liang Z, Liu T (2015) Molecular spectrum of KRAS, NRAS, BRAF and PIK3CA mutations in Chinese colorectal cancer patients: analysis of 1,110 cases. Scientific reports 5:18678. https://doi.org/10.1038/srep18678
Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH, Hayes DF, McAllister PK, Morton RF, Schilsky RL (2009) American Society of Clinical Oncology provisional clinical opinion: testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J Clin Oncol 27 (12):2091-2096. https://doi.org/10.1200/jco.2009.21.9170
Douillard JY, Oliner KS, Siena S, Tabernero J, Burkes R, Barugel M, Humblet Y, Bodoky G, Cunningham D, Jassem J, Rivera F, Kocakova I, Ruff P, Blasinska-Morawiec M, Smakal M, Canon JL, Rother M, Williams R, Rong A, Wiezorek J, Sidhu R, Patterson SD (2013) Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 369 (11):1023-1034. https://doi.org/10.1056/nejmoa1305275
Lubner MG, Stabo N, Lubner SJ, del Rio AM, Song C, Halberg RB, Pickhardt PJ (2015) CT textural analysis of hepatic metastatic colorectal cancer: pre-treatment tumor heterogeneity correlates with pathology and clinical outcomes. Abdominal imaging 40 (7):2331-2337. https://doi.org/10.1007/s00261-015-0438-4
Yang L, Dong D, Fang M, Zhu Y, Zang Y, Liu Z, Zhang H, Ying J, Zhao X, Tian J (2018) Can CT-based radiomics signature predict KRAS/NRAS/BRAF mutations in colorectal cancer? European radiology 28 (5):2058-2067. https://doi.org/10.1007/s00330-017-5146-8
Shin YR, Kim KA, Im S, Hwang SS, Kim KJAr (2016) Prediction of KRAS mutation in rectal cancer using MRI. 36 (9):4799-4804
Hong H-S, Kim SH, Park H-J, Park M-S, Kim KW, Kim WH, Kim NK, Lee JM, Cho HJJYmj (2013) Correlations of dynamic contrast-enhanced magnetic resonance imaging with morphologic, angiogenic, and molecular prognostic factors in rectal cancer. 54 (1):123-130
He J (2018) Comparison of PET conventional parameters and PET texture parameters for predicting KRAS gene mutation in colorectal cancer. Journal of Nuclear Medicine Conference: Society of Nuclear Medicine and Molecular Imaging Annual Meeting, SNMMI 59 (Supplement 1)
Lovinfosse P, Koopmansch B, Lambert F, Jodogne S, Kustermans G, Hatt M, Visvikis D, Seidel L, Polus M, Albert A, Delvenne P, Hustinx R (2016) (18)F-FDG PET/CT imaging in rectal cancer: relationship with the RAS mutational status. The British journal of radiology 89 (1063):20160212. https://doi.org/10.1259/bjr.20160212
Song B, Zhang G, Lu H, Wang H, Zhu W, Pickhardt PJ, Liang ZJIjocar, surgery (2014) Volumetric texture features from higher-order images for diagnosis of colon lesions via CT colonography. 9 (6):1021-1031
Chen S-W, Lin C-Y, Ho C-M, Chang Y-S, Yang S-F, Kao C-H, Chang J-GJCnm (2015) Genetic alterations in colorectal Cancer have different patterns on 18F-FDG PET/CT. 40 (8):621-626
Pershad Y, Govindan S, Hara A, Borad M, Bekaii-Saab T, Wallace A, Albadawi H, Oklu RJD (2017) Using Naïve Bayesian Analysis to Determine Imaging Characteristics of KRAS Mutations in Metastatic Colon Cancer. 7 (3):50
Jamaspishvili T, Berman DM, Ross AE, Scher HI, De Marzo AM, Squire JA, Lotan TL (2018) Clinical implications of PTEN loss in prostate cancer. Nat Rev Urol 15 (4):222-234. https://doi.org/10.1038/nrurol.2018.9
McCann SM, Jiang Y, Fan X, Wang J, Antic T, Prior F, VanderWeele D, Oto A (2016) Quantitative Multiparametric MRI Features and PTEN Expression of Peripheral Zone Prostate Cancer: A Pilot Study. AJR American journal of roentgenology 206 (3):559-565. https://doi.org/10.2214/ajr.15.14967
Vander-Weele DJ, McCann S, Fan X, Antic T, Jiang Y, Oto A (2015) Radiogenomics of prostate cancer: Association between quantitative multi-parametric MRI features and PTEN. Journal of Clinical Oncology Conference 33 (7 SUPPL. 1)
Stoyanova R, Pollack A, Lynne C, Jorda M, Erho N, Lam LLC, Buerki C, Davicioni E, Ishkanian A (2015) Using radiogenomics to characterize MRI-guided prostate cancer biopsy heterogenity. Journal of Clinical Oncology Conference 33 (7 SUPPL. 1)
Stoyanova R, Pollack A, Takhar M, Lynne C, Parra N, Lam LL, Alshalalfa M, Buerki C, Castillo R, Jorda M, Ashab HA, Kryvenko ON, Punnen S, Parekh DJ, Abramowitz MC, Gillies RJ, Davicioni E, Erho N, Ishkanian A (2016) Association of multiparametric MRI quantitative imaging features with prostate cancer gene expression in MRI-targeted prostate biopsies. Oncotarget 7 (33):53362-53376. https://doi.org/10.18632/oncotarget.10523
Shaikh FA, Kolowitz BJ, Awan O, Aerts HJ, von Reden A, Halabi S, Mohiuddin SA, Malik S, Shrestha RB, Deible C (2017) Technical challenges in the clinical application of radiomics. JCO Clinical Cancer Informatics 1:1-8
Leijenaar RT, Carvalho S, Velazquez ER, Van Elmpt WJ, Parmar C, Hoekstra OS, Hoekstra CJ, Boellaard R, Dekker AL, Gillies RJJAo (2013) Stability of FDG-PET Radiomics features: an integrated analysis of test-retest and inter-observer variability. 52 (7):1391-1397
Traverso A, Wee L, Dekker A, Gillies RJIJoROBP (2018) Repeatability and reproducibility of radiomic features: a systematic review. 102 (4):1143-1158
Fave X, Mackin D, Yang J, Zhang J, Fried D, Balter P, Followill D, Gomez D, Jones AK, Stingo FJMp (2015) Can radiomics features be reproducibly measured from CBCT images for patients with non‐small cell lung cancer? 42 (12):6784-6797
Mackin D, Fave X, Zhang L, Fried D, Yang J, Taylor B, Rodriguez-Rivera E, Dodge C, Jones AK, Court LJIr (2015) Measuring CT scanner variability of radiomics features. 50 (11):757
Shafiq‐ul‐Hassan M, Zhang GG, Latifi K, Ullah G, Hunt DC, Balagurunathan Y, Abdalah MA, Schabath MB, Goldgof DG, Mackin DJMp (2017) Intrinsic dependencies of CT radiomic features on voxel size and number of gray levels. 44 (3):1050-1062
Berenguer R, Pastor-Juan MdR, Canales-Vázquez J, Castro-García M, Villas MV, Mansilla Legorburo F, Sabater SJR (2018) Radiomics of CT features may be nonreproducible and redundant: influence of CT acquisition parameters. 288 (2):407-415
Lecler A, Duron L, Balvay D, Savatovsky J, Bergès O, Zmuda M, Farah E, Galatoire O, Bouchouicha A, Fournier LS (2019) Combining Multiple Magnetic Resonance Imaging Sequences Provides Independent Reproducible Radiomics Features. Scientific reports 9 (1):2068. https://doi.org/10.1038/s41598-018-37984-8
Shiri I, Rahmim A, Ghaffarian P, Geramifar P, Abdollahi H, Bitarafan-Rajabi AJEr (2017) The impact of image reconstruction settings on 18F-FDG PET radiomic features: multi-scanner phantom and patient studies. 27 (11):4498-4509
Zhao B, Tan Y, Tsai WY, Qi J, Xie C, Lu L, Schwartz LH (2016) Reproducibility of radiomics for deciphering tumor phenotype with imaging. Scientific reports 6:23428. https://doi.org/10.1038/srep23428
van Velden FH, Kramer GM, Frings V, Nissen IA, Mulder ER, de Langen AJ, Hoekstra OS, Smit EF, Boellaard RJMi, biology (2016) Repeatability of radiomic features in non-small-cell lung cancer [18 F] FDG-PET/CT studies: impact of reconstruction and delineation. 18 (5):788-795
Parmar C, Velazquez ER, Leijenaar R, Jermoumi M, Carvalho S, Mak RH, Mitra S, Shankar BU, Kikinis R, Haibe-Kains BJPo (2014) Robust radiomics feature quantification using semiautomatic volumetric segmentation. 9 (7):e102107
He L, Huang Y, Ma Z, Liang C, Liang C, Liu Z (2016) Effects of contrast-enhancement, reconstruction slice thickness and convolution kernel on the diagnostic performance of radiomics signature in solitary pulmonary nodule. Scientific reports 6:34921. https://doi.org/10.1038/srep34921. https://www.nature.com/articles/srep34921#supplementary-information
Perrin T, Midya A, Yamashita R, Chakraborty J, Saidon T, Jarnagin WR, Gonen M, Simpson AL, Do RKJAR (2018) Short-term reproducibility of radiomic features in liver parenchyma and liver malignancies on contrast-enhanced CT imaging. 43 (12):3271-3278
Khalvati F, Zhang Y, Baig S, Lobo-Mueller EM, Karanicolas P, Gallinger S, Haider MA (2019) Prognostic Value of CT Radiomic Features in Resectable Pancreatic Ductal Adenocarcinoma. Scientific reports 9 (1):5449. https://doi.org/10.1038/s41598-019-41728-7
Altazi BA, Zhang GG, Fernandez DC, Montejo ME, Hunt D, Werner J, Biagioli MC, Moros EGJJoacmp (2017) Reproducibility of F18‐FDG PET radiomic features for different cervical tumor segmentation methods, gray‐level discretization, and reconstruction algorithms. 18 (6):32-48
Coroller TP, Agrawal V, Narayan V, Hou Y, Grossmann P, Lee SW, Mak RH, Aerts HJJR, Oncology (2016) Radiomic phenotype features predict pathological response in non-small cell lung cancer. 119 (3):480-486
Fiset S, Welch ML, Weiss J, Pintilie M, Conway JL, Milosevic M, Fyles A, Traverso A, Jaffray D, Metser UJR, Oncology (2019) Repeatability and reproducibility of MRI-based radiomic features in cervical cancer. 135:107-114
Qiu Q, Duan J, Duan Z, Meng X, Ma C, Zhu J, Lu J, Liu T, Yin YJQIiM, Surgery (2019) Reproducibility and non-redundancy of radiomic features extracted from arterial phase CT scans in hepatocellular carcinoma patients: impact of tumor segmentation variability.
Zhang J, Qiu Q, Duan J, Gong G, Jiang Q, Sun G, Yin YJTCR (2019) Variability of radiomic features extracted from multi-b-value diffusion-weighted images in hepatocellular carcinoma. 8 (1):130-140
Buckler AJ, Mozley PD, Schwartz L, Petrick N, McNitt-Gray M, Fenimore C, O’Donnell K, Hayes W, Kim HJ, Clarke LJAr (2010) Volumetric CT in lung cancer: an example for the qualification of imaging as a biomarker. 17 (1):107-115
Wiki FQ, Body QF-PW The Radiological Society of North America (RSNA) Quantitative Imaging Biomarker Alliance (QIBA) FDG-PET Technical Committee: Proffered Protocol for Quantifying the Standard Uptake (SUV) in Patients with Cancer.
Hussain Z, Gimenez F, Yi D, Rubin D Differential data augmentation techniques for medical imaging classification tasks. In: AMIA Annual Symposium Proceedings, 2017. American Medical Informatics Association, p 979
Banerjee S, Mitra S, Shankar BU, Hayashi Y (2016) A Novel GBM Saliency Detection Model Using Multi-Channel MRI. PloS one 11 (1):e0146388. https://doi.org/10.1371/journal.pone.0146388
De Fauw J, Ledsam JR, Romera-Paredes B, Nikolov S, Tomasev N, Blackwell S, Askham H, Glorot X, O’Donoghue B, Visentin D, van den Driessche G, Lakshminarayanan B, Meyer C, Mackinder F, Bouton S, Ayoub K, Chopra R, King D, Karthikesalingam A, Hughes CO, Raine R, Hughes J, Sim DA, Egan C, Tufail A, Montgomery H, Hassabis D, Rees G, Back T, Khaw PT, Suleyman M, Cornebise J, Keane PA, Ronneberger O (2018) Clinically applicable deep learning for diagnosis and referral in retinal disease. Nature Medicine 24 (9):1342-1350. https://doi.org/10.1038/s41591-018-0107-6
Velazquez ER, Parmar C, Jermoumi M, Mak RH, van Baardwijk A, Fennessy FM, Lewis JH, De Ruysscher D, Kikinis R, Lambin P, Aerts HJ (2013) Volumetric CT-based segmentation of NSCLC using 3D-Slicer. Scientific reports 3:3529. https://doi.org/10.1038/srep03529
Joskowicz L, Cohen D, Caplan N, Sosna J (2018) Inter-observer variability of manual contour delineation of structures in CT. European radiology. https://doi.org/10.1007/s00330-018-5695-5
Binder ZA, Thorne AH, Bakas S, Wileyto EP, Bilello M, Akbari H, Rathore S, Ha SM, Zhang L, Ferguson CJ, Dahiya S, Bi WL, Reardon DA, Idbaih A, Felsberg J, Hentschel B, Weller M, Bagley SJ, Morrissette JJD, Nasrallah MP, Ma J, Zanca C, Scott AM, Orellana L, Davatzikos C, Furnari FB, O’Rourke DM (2018) Epidermal Growth Factor Receptor Extracellular Domain Mutations in Glioblastoma Present Opportunities for Clinical Imaging and Therapeutic Development. Cancer cell 34 (1):163-177.e167. https://doi.org/10.1016/j.ccell.2018.06.006
Beig N, Patel J, Prasanna P, Hill V, Gupta A, Correa R, Bera K, Singh S, Partovi S, Varadan V, Ahluwalia M, Madabhushi A, Tiwari P (2018) Radiogenomic analysis of hypoxia pathway is predictive of overall survival in Glioblastoma. Scientific reports 8 (1):7. https://doi.org/10.1038/s41598-017-18310-0
Colen R, Foster I, Gatenby R, Giger ME, Gillies R, Gutman D, Heller M, Jain R, Madabhushi A, Madhavan S, Napel S, Rao A, Saltz J, Tatum J, Verhaak R, Whitman G (2014) NCI Workshop Report: Clinical and Computational Requirements for Correlating Imaging Phenotypes with Genomics Signatures. Translational oncology 7 (5):556-569. https://doi.org/10.1016/j.tranon.2014.07.007
Colen R, Hatami M, Kotrotsou A, Chaddad A, Bakhtiari A, Luedi M, Zinn PO (2015) Radiomic subclassification of glioblastoma. Neuro-oncology 5):v155. http://dx.doi.org/10.1093/neuonc/nov225.11
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no sources of funding or conflicts to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
CME activity This article has been selected as the CME activity for the current month. Please visit https://ce.mayo.edu/node/83629 and follow the instructions to complete this CME activity.
Electronic supplementary material
Below is the link to the electronic supplementary material.
261_2019_2028_MOESM1_ESM.eps
Supplementary material 1 (EPS 1435 kb). Supplemental Fig. 1. Flowchart depicting the results of the enforcement of inclusion and exclusion criteria on biomedical articles procured from major databases. The final number of articles at the bottom of the flow chart reflects the number of articles that were subjected to an extensive evaluation
Appendix 1
Appendix 1
Methodology
For the purpose of this review, MEDLINE (PubMed), EMBASE, and Scopus served as the basis for our literature search. The search terms and strategies used for each of the databases are listed in Appendix 1. All literature searches were performed on August 17, 2018. The search results were compiled and saved as a standardized result list for further analysis, during the review process, specific topics of literature were included. Additional literature from later timepoints was included based on feedback from reviewers. Due to the specific nature of our research topic, no time frame filters were applied. Supplemental Fig. 1 is a schematic depiction of the enforcement of the inclusion/exclusion criteria on the search results from the respective databases. The end result of the flow chart is the number of articles that would undergo a thorough evaluation.
Search terms and strategies used in the literature search
(a) MEDLINE/PubMed
Search | Query |
|---|---|
#19 | Search (#15 OR #18) |
#18 | Search (#16 AND #17) |
#17 | Search ((texture analys* [tiab] OR radiomic* [tiab])) |
#16 | Search (“Genomics” [Mesh] OR genomic* [tiab] OR “Mutation” [Mesh] OR mutation* [tiab] OR “Mutagenesis” [Mesh] OR mutagenes* [tiab]) |
#15 | Search radiogenomic* [tiab] |
(b) EMBASE
Search | Query |
|---|---|
#7 | 5 or 6 |
#6 | radiogenomics.ti,ab. |
#5 | 3 and 4 |
#4 | (texture analys* or radiomic*).ti,ab. |
#3 | 1 or 2 |
#2 | (genomic* or mutation* or mutagenes*).ti,ab. |
#1 | exp genomics/or exp mutation/ |
(c) Scopus
(TITLE-ABS-KEY (radiogenomic*)) OR ((TITLE-ABS-KEY (genomic* OR mutation* OR mutagenes*) AND TITLE-ABS-KEY (“texture analys*” OR radiomic*)))
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Bodalal, Z., Trebeschi, S., Nguyen-Kim, T.D.L. et al. Radiogenomics: bridging imaging and genomics. Abdom Radiol 44, 1960–1984 (2019). https://doi.org/10.1007/s00261-019-02028-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-019-02028-w