
Abstract
Purpose
Anterior cruciate ligament (ACL) injury rate is low among children, but increases during adolescence, especially in girls. Increases in the knee valgus moment within 70 ms of contact with the ground (KFM0-70) may explain the sex-specific increase in the risk of ACL injury. The purpose of the study was to investigate sex-dependent changes in the KFM0-70 from pre-adolescence to adolescence during a cutting maneuver (CM).
Methods
Kinematic and kinetic data during the CM task, performed before and after physical exertion, were recorded using a motion capture system and a force plate. A total of 293 team handball and soccer players, aged 9–12 years, were recruited. A number of those who continued sports participation (n = 103) returned five years later to repeat the test procedure. Three mixed-model analysis of variance (ANOVA) for repeated measures tests were used to determine the effects of sex and age period on the KFM0-70 (1: with no adjustment, 2: adjusted for repeated measurements, and 3: additionally adjusted with hip and knee joint frontal plane kinematics).
Results
Boys had significantly higher KFM0-70 than girls at both age periods (p < 0.01 for all models). Girls, not boys, demonstrated significantly increased KFM0-70 from pre-adolescence to adolescence. Importantly, this was fully explained by kinematic variables.
Conclusion
Although the marked increase in KFM0-70 seen in girls may play a role in their risk of ACL rupture, the higher values demonstrated by boys during CM reflect the complexity of multifactorial biomechanical risk factor analysis. The role of kinematics in mediating the KFM0-70 provides means for modification of this risk factor, but as boys had higher joint moments, continued investigation into sex-dependent biomechanical risk factors is warranted.
Level of evidence
II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An ACL injury is one of the more serious knee injuries sustained by athletes participating in sports involving jumping and cutting tasks, with an injury incidence for individuals in their twenties reported as 154 per 100,000 [26]. The likelihood of concomitant injury to other knee structures is very high and the most younger individuals undergo ACL reconstruction surgery. This has serious consequences including high treatment costs, long-term absence of the athlete from training and competition, a decrease in the athlete’s performance, further joint injuries (e.g., osteoarthritis) [34] and greater risk of a second ACL injury, especially for young individuals [35]. Most ACL injuries occur in a non-contact mechanism [8] where there is a rapid change in speed and direction of movement (e.g., when landing from a jump and during cutting movements), which is commonly performed in multidirectional sports, such as team handball and soccer.
In recent decades, efforts have been made to identify risk factors and mechanisms of ACL injury to potentially screen and find individuals who are more prone to this injury. An increased rate of ACL ruptures is seen during adolescence, in particular for female athletes [26]. Changes that happen to female athletes during that time [1, 7, 12, 25, 27, 28, 36] are therefore targets for injury preventative measures and risk factor studies. Biomechanical [3, 9, 12] and neuromuscular [12, 18] factors have been the focus of research studies since that line of research is most likely to yield modifiable targets for preventative studies. Cross-sectional studies have shown sex-dependent kinematic and kinetic differences during cutting maneuvers (CM) [27] and drop jump tasks [4] in children. However, previous prospective studies conducted for age period differences were limited due to a short follow-up time (1–3 years) [12, 15, 28] or insufficient sample size [25].
Another difficulty with identifying changes in biomechanics that may lead to ACL injury is knowing what to look at. Recent studies have shed some light on the particulars of the injury mechanism such as how quickly (around 50 ms) after ground contact the injury occurs [19, 20]. The multi-planar nature of the injury has been demonstrated in a cadaver study [3] and combinations of trunk and lower limb kinematics during injury have been described [16]. The frontal plane knee moment (KFM) is a strong candidate risk factor although studies have shown mixed results [14, 22, 24]. Hewett et al. (2005) showed that some female athletes who demonstrated high peak knee valgus moment later went on to injure their ACL [14]. In contrast, Krosshaug et al. (2016) and Leppänen et al. (2017) observed that the peak knee valgus moment was not associated with the risk of ACL injury during vertical drop jump task [22, 24]. However, none of these studies extracted the peak joint moment within the specific timeframe relevant for ACL injury (immediately after foot–ground contact) or during the CM. Unlike the drop jump, a CM requires more contributions from the frontal plane. If the KFM during the ACL injury timeframe explains the increased injury risk observed for adolescent female athletes, it should be expected to increase markedly during maturation when performing movements with frontal plane requirements. Hence, the present study aimed to prospectively investigate if there are differences between female and male athletes in how the KFM changes during the transition from youth to adolescence. It was hypothesized that girls would display higher KFM than boys, and that these differences would become more pronounced after the transition from pre-adolescence to adolescence.
Materials and methods
The study was approved by the Icelandic National Bioethics Committee VSNb20112020011/03.7). This is a secondary analysis of a completed longitudinal laboratory study. Children involved in team sports (handball and soccer; n = 293), were recruited at age 9–12 years old. Five years later, 177 of them now aged 14–17 years old returned to participate in the test procedure again. Those who had not continued in their sport from pre-adolescence to adolescence (n = 74) were removed. Thus, the data of 103 participants were used for further analysis (demographic characteristics in Table 1).
Eligibility criteria
The inclusion criteria were active participation in team sports (soccer, team handball, or both) at the pre-adolescent age and in one of the five local participating clubs. The exclusion criteria were history of lower limb ligament or muscle rupture or any orthopedic problems precluding them from active participation. The subjects and their guardians provided written informed consent before commencing the test procedure during both visits.
Task procedure
After measuring height, weight, and distance from iliac crest to the lateral malleolus, athletes warmed up on a stationary bicycle for five minutes at a self-selected pace. A set of 46 retro-reflective markers were used to define and track body segments (trunk, pelvis, thighs, shanks, and feet) [4]. After a static measurement, 12 anatomical markers (malleoli, femoral condyles, trochanters, iliac crests) were removed to allow free movement of the subject. Data were collected with an eight-camera motion capture system (Qualisys Oqus, Gothenborg, Sweden) sampling at 200 Hz (pre-adolescent athletes) or 400 Hz (adolescents) and two force plates embedded in the floor (AMTI, Watertown, USA) sampling at 2000 Hz.
After 1–3 familiarization trials for each task, subjects performed five CM tasks against a dummy opponent for each leg [27] before and after completing a five minute physical exertion task [4]. The order of movement tasks was randomized. For the CM task procedure, participants stood in a ready-position and on a verbal signal performed a quick antero-lateral step in a self-selected cutting angle (range 10–170°) using their preferred technique. The distance of the athlete to the force plate was adjusted such that their preferred technique would have them land on the force plate.
Data processing
Visual3D software (C-Motion, USA, version 6) was used to construct a model and calculate joint kinematics and kinetics. The resultant signals were low-pass filtered at 20 Hz. The time of ground contact was defined as the first frame with a vertical ground reaction force greater than 5 N. Kinematic variables were extracted at the time of initial contact, including frontal plane hip angle (HFAIC) and sagittal and frontal plane knee angles (KSAIC and KFAIC, respectively). Also, the KFM was extracted as the peak value within the first 70 ms after ground contact and normalized by body mass (referred to as KFM0-70 for the remainder of this text). Time to reach peak KFM0-70 (TKFM0-70) was also calculated. The normalized trunk–foot distance at initial contact (NTFDIC) has been suggested as a potentially important variables in the ACL injury mechanism [30] and was therefore calculated at initial contact as the medio-lateral distance between the foot and trunk segment center of mass using Formula 1:
Statistical analysis
First the outcome variable (KFM0-70) was transformed (ln[1 + y]) to correct for skewness and variance heterogeneity. A mixed-model analysis of variance (ANOVA) was used to analyze the transformed KFM0-70 values. For all models, an initial full factorial model was used, where sex (girl and boy), age period (pre-adolescent and adolescent), leg (left and right), and exertion (before and after physical exertion) were factors, and the identification number was a random coefficient (random intercept) to adjust for repeated measurements (Model 1). Then random coefficients (random slopes) for age period, leg, and exertion factors were included to adjust for the variability in the effects of these factors on the outcome (Model 2). Models were compared using the Bayesian Information Criterion (BIC) index for mixed models to confirm that the random effects improved the model fit. Lastly, other biomechanical variables related to ACL injury (KSAIC, KFAIC, HFAIC, TKFM0-70, and NTFDIC) were added as covariates to evaluate the extent to which observable movement patterns influence the KFM0-70 (Model 3). Different combinations of these covariates were tested and the model that had the lowest BIC value was used. Non-significant 3- and 4-way interactions were removed from the models as they did not improve the model fit. All statistical tests were conducted with mixed models module (GAMLj version 1.5.0) [13] for Jamovi software (version 2.3.13) at the significance level of 0.05. Satterthwaite’s method was used to calculate p values. The sample size calculation for the first phase of this study (n = 293) did not include outcome variables that were used in the current (phase 2) secondary analysis. An attempt was made to recruit all participants who were still involved with team sports and 103 participants returned. Power calculation revealed that this sample size (39 boys and 64 girls) has statistical power to detect effect size (Cohens d) of 0.37 (alpha = 0.05, beta = 0.90).
Results
The demographic characteristics of subjects
The demographic characteristics for boys, girls, and overall groups in pre-adolescent and adolescent age periods are seen in Table 1.
The comparison of different mixed-model tests for transformed KFM0-70 values
Random components (slopes) for age period, leg, and exertion all yielded lower BIC values of the mixed-model fit (Supplementary file; Table I) and were included for Model 2 (Table 2). The lowest value of the BIC in mixed-model analysis was found when applying the KFAIC and HFAIC as covariates (Supplementary file; Table II). Based on these findings, age period, leg, and exertion were used as random coefficients and the KFAIC and HFAIC as covariates for Model 3 (Table 2).
The comparison of transformed KFM0-70 values among factors
There was a main effect of sex and leg in all three models and a main effect of age period in model 3 (Table 2). There were two-way interactions for sex*age period in Models 1 and 2 but not Model 3 (Table 2). Models 1 and 2 demonstrated an increase in transformed KFM0-70 values from pre-adolescence to adolescence for girls (from 0.19 ± 0.01 to 0.21 ± 0.01 and from 0.19 ± 0.01 to 0.23 ± 0.02 Nm/kg, respectively), while boys demonstrated a decrease from pre-adolescence to adolescence age period (from 0.25 ± 0.01 to 0.23 ± 0.02 and from 0.25 ± 0.02 to 0.24 ± 0.03 Nm/kg, respectively) (Fig. 1). However, when adjusting the mixed-model with random slopes and covariates (Model 3), both girls and boys showed an increase in transformed KFM0-70 values from pre-adolescence to adolescence (from 0.18 ± 0.01 to 0.25 ± 0.02 and from 0.25 ± 0.02 to 0.27 ± 0.03 N/kg, respectively) (Fig. 1).

Interactions between sex and age period for the KFM0-70 outcome variable in three different mixed models: no adjustment (a), three random slopes (b), and three random slopes plus two covariates (c). Back-transformed adjusted means and 95% confidence intervals are shown
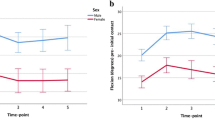
One significant 3-way interaction was found for KFM0-70 and that was in the adjusted Model 3 for sex*age period*exertion (P < 0.05) (Table 2). The interaction was due to a post-exertion decrease in KFM0-70 seen in adolescent boys but not girls (Fig. 2).

The effect of exertion in boys (a) and girls (b) in pre-adolescence and adolescence age periods. Back-transformed adjusted means are shown and 95% confidence intervals
Discussion
The most important finding of the present study was that boys had a greater KFM than girls during the 0–70 ms timeframe during which an ACL rupture would occur. While an increase over time was seen for females, this increase explained less than 4% of the variance and disappeared in statistical model that adjusted for kinematics. The results are congruent with previous studies that have identified longitudinal changes in the KFM for female athletes [12, 15]. Unlike those studies, the focus of this analysis was on the timeframe immediately following initial ground contact as well as a CM task to make the results more relevant for the ACL injury mechanism [19, 20]. This may, in part, explain the fact that female subjects in the current study did not have higher KFM values compared to the males at either time point and so the increase observed in the girls served only to close the gap between the sexes. During a drop jump, a movement pattern of dynamic valgus which is commonly observed for female athletes [12] may contribute to the much greater KFM differences reported previously for such a task [15]. During CM, there are some additional potential confounders which may differ between the sexes and explain the higher values for boys, such as cutting angle and movement speed [21]. In terms of injury risk, girls may have a lower threshold for tolerating sudden KFM loads as their ACL is smaller and not as stiff [6]. Girls are also more likely to experience concurrent forces after initial ground contact which may, in part, influence ACL injury risk [32].
Previous studies have hypothesized that the ability of female adolescents and adults to attenuate forces contributing to the KFM is decreased due to sex-dependent anatomical [17], muscular [1], neuromuscular [1, 23, 25, 28], and biomechanical [10, 23, 28] differences. In the present study, when the model was adjusted for hip and knee frontal angle, no differences in the KFM0-70 were detected between the sexes. The two frontal plane covariates (KFAIC and HFAIC) are considered biomechanical risk factors for ACL injuries [2, 11, 14]. One interpretation of this result is that sex-based differences in kinematics are driving the increase of KFM observed for female athletes. The models without kinematics had an explained variance of ~ 4% for the fixed effects of Model 1 (R-squared Marginal; Table 2), while the model with kinematics had an explained variance of ~ 20% for Model 3 (R-squared Marginal; Table 2). The sex and age group therefore only explain a fairly insignificant percentage of the KFM0-70 compared to the kinematics. The random effect structure explained a further 40% of the variance (R-squared Marginal vs. R-squared Conditional for Model 3, Table 2), indicating the possibility that there are variables not captured in the fixed effects which can be influential on the KFM0-70. Another paper based on the same adolescent girls as the current study reported that the KFM waveform was highly variable in this timeframe and that patterns with high KFM values were relatively rare [31]. The closer the peak values occur to the initial contact, the greater the influence of the impact with the ground must be and less the influence of joint angles. In the current study, the distance between foot and trunk did not influence the KFM value, but was associated with greater odds of showing the early peak waveform in the previous study [31].
There was a three-way interaction between sex, age group, and exertion because boys responded to the physical exertion with a lower KFM0-70. While the original intent of the physical exertion protocol was to produce fatigue [4], the effects in the adolescent age group might simply be a warm-up effect rather than fatigue. However, these differences were small and unlikely to be of clinical significance.
The strengths of this study include its prospective nature and a sample size allowing for the statistical approach taken. The primary limitation of the current study is the secondary, exploratory, design which makes it more prone to generate non-reproducible findings. Physical maturity and physical fitness are probable confounders when assessing the different changes with maturation, and these were not assessed in the study. The direction of this bias would be toward greater KFM for boys, as was observed in the study.
There are known limitations regarding the precision of optical marker-based motion capture systems such as those used in the current study [5]. While knee kinetics during cutting maneuvers is known to the fairly reliable [29], errors in the estimate of KFM may be as high as 0.375 Nm/kg. The results in the manuscript are reported with two decimals of precision, but it is not known whether the methods are precise enough to determine the last decimal. The calculation of the KFM depends on the frontal plane angle of the knee, which is known to have a systemic bias with increasing flexion angles [33]. Small errors in the placement of knee markers can also shift the center of rotation and artificially create a correlation between flexion and abduction. However, given the large sample size of the current study and the random uniform distribution of such errors, this effect is unlikely to affect the results.
These findings are clinically relevant for the potential attenuation of ACL injury risk. Targeting the frontal plane kinematics at the moment of impact has the potential to reduce the KFM of the impact phase of CMs. While girls showed more increases with age, the results indicate that interventions could be aimed at all athletes who show impact phase kinematics consistent with higher KFM. Despite girls having a higher risk of ACL injury, boys in the study had an overall higher KFM. Clinicians should be aware that addressing the KFM alone might not be sufficient to reduce the risk of ACL injuries.
Conclusion
Girls demonstrated an increased KFM0-70 during adolescence but to a smaller extent than previous studies have indicated. The increase seems driven by the knee and hip frontal plane kinematics, which still are unlikely to fully explain sex-dependent differences in risk of ACL injury. The clinical implications are that frontal plane kinematics should be targeted when attempting to influence the KFM0-70 while considering other biomechanical risk factors.
References
Barber-Westin SD, Noyes FR, Galloway M (2006) Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med 34:375–384. https://doi.org/10.1177/0363546505281242
Bates NA, Myer GD, Hale RF, Schilaty ND, Hewett TE (2020) Prospective frontal plane angles used to predict ACL strain and identify those at high risk for sports-related ACL injury. Orthop J Sport Med 8:1–10. https://doi.org/10.1177/2325967120957646
Bates NA, Schilaty ND, Nagelli CV, Krych AJ, Hewett TE (2018) Validation of noncontact anterior cruciate ligament tears produced by a mechanical impact simulator against the clinical presentation of injury. Am J Sports Med 46:2113–2121. https://doi.org/10.1177/0363546518776621
Briem K, Jónsdóttir KV, Árnason Á, Sveinsson Þ (2017) Effects of sex and fatigue on biomechanical measures during the drop-jump task in children. Orthop J Sport Med 5:1–7. https://doi.org/10.1177/2325967116679640
Camomilla V, Cereatti A, Cutti AG, Fantozzi S, Stagni R, Vannozzi G (2017) Methodological factors affecting joint moments estimation in clinical gait analysis: a systematic review. Biomed Eng Online 16:1–27. https://doi.org/10.1186/s12938-017-0396-x
Chandrashekar N, Mansouri H, Slauterbeck J, Hashemi J (2006) Sex-based differences in the tensile properties of the human anterior cruciate ligament. J Biomech 39:2943–2950. https://doi.org/10.1016/j.jbiomech.2005.10.031
Chia L, Myer GD, Hewett TE, McKay MJ, Sullivan J, Ford KR, Pappas E (2021) When puberty strikes: longitudinal changes in cutting kinematics in 172 high-school female athletes. J Sci Med Sport 24:1290–1295. https://doi.org/10.1016/j.jsams.2021.07.011
Chia L, De Oliveira SD, Whalan M, McKay MJ, Sullivan J, Fuller CW, Pappas E (2022) Non-contact anterior cruciate ligament injury epidemiology in team-ball sports: a systematic review with meta-analysis by sex, age, sport, participation level, and exposure type. Sport Med 52:2447–2467. https://doi.org/10.1007/s40279-022-01697-w
Cronström A, Creaby MW, Ageberg E (2020) Do knee abduction kinematics and kinetics predict future anterior cruciate ligament injury risk? A systematic review and meta-analysis of prospective studies. BMC Musculoskelet Disord 21:1–11. https://doi.org/10.1186/s12891-020-03552-3
DiCesare CA, Montalvo A, Barber Foss KD, Thomas SM, Ford KR, Hewett TE, Jayanthi NA, Stracciolini A, Bell DR, Myer GD (2019) Lower extremity biomechanics are altered across maturation in sport-specialized female adolescent athletes. Front Pediatr 7:1–11. https://doi.org/10.3389/fped.2019.00268
Dix C, Arundale A, Silvers-Granelli H, Marmon A, Zarzycki R, Snyder-Mackler L (2020) Biomechanical measures during two sport-specific tasks differentiate between soccer players who go on to anterior cruciate ligament injury and those who do not: a prospective cohort analysis. Int J Sports Phys Ther 15:928–935. https://doi.org/10.26603/ijspt20200928
Ford KR, Shapiro R, Myer GD, Van Den Bogert AJ, Hewett TE (2010) Longitudinal sex differences during landing in knee abduction in young athletes. Med Sci Sports Exerc 42:1923–1931. https://doi.org/10.1249/MSS.0b013e3181dc99b1
Gallucci M (2023) gamlj: GAMLj Suite for linear models. R package version 2.6.6. https://www.gamlj.github.io/. Accessed 15 Jan 2023
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, Van den Bogert AJ, Paterno MV, Succop P (2005) Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med 33:492–501. https://doi.org/10.1177/0363546504269591
Hewett TE, Myer GD, Kiefer AW, Ford KR (2015) Longitudinal increases in knee abduction moments in females during adolescent growth. Med Sci Sports Exerc 47:2579–2585. https://doi.org/10.1249/MSS.0000000000000700
Hewett TE, Torg JS, Boden BP (2009) Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med 43:417–422. https://doi.org/10.1136/bjsm.2009.059162
Hosseinzadeh S, Kiapour AM (2020) Sex differences in anatomic features linked to anterior cruciate ligament injuries during skeletal growth and maturation. Am J Sports Med 48:2205–2212. https://doi.org/10.1177/0363546520931831
Khayambashi K, Ghoddosi N, Straub RK, Powers CM (2016) Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: a prospective study. Am J Sports Med 44:355–361. https://doi.org/10.1177/0363546515616237
Koga H, Muneta T, Bahr R, Engebretsen L, Krosshaug T (2015) Video analysis of ACL injury mechanisms using a model-based image-matching technique. Sport Inj Prev. https://doi.org/10.1007/978-4-431-55318-2_9
Koga H, Nakamae A, Shima Y, Iwasa J, Myklebust G, Engebretsen L, Bahr R, Krosshaug T (2010) Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med 38:2218–2225. https://doi.org/10.1177/0363546510373570
Kristianslund E, Faul O, Bahr R, Myklebust G, Krosshaug T (2014) Sidestep cutting technique and knee abduction loading: implications for ACL prevention exercises. Br J Sports Med 48:779–783. https://doi.org/10.1136/bjsports-2012-091370
Krosshaug T, Steffen K, Kristianslund E, Nilstad A, Mok K-M, Myklebust G, Andersen TE, Holme I, Engebretsen L, Bahr R (2016) The vertical drop jump is a poor screening test for ACL injuries in female elite soccer and handball players: a prospective cohort study of 710 athletes. Am J Sports Med 44:874–883. https://doi.org/10.1177/0363546515625048
Landry SC, McKean KA, Hubley-Kozey CL, Stanish WD, Deluzio KJ (2007) Neuromuscular and lower limb biomechanical differences exist between male and female elite adolescent soccer players during an unanticipated side-cut maneuver. Am J Sports Med 35:1888–1900. https://doi.org/10.1177/0363546507300823
Leppänen M, Pasanen K, Kujala UM, Vasankari T, Kannus P, Äyrämö S, Krosshaug T, Bahr R, Avela J, Perttunen J (2017) Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. Am J Sports Med 45:386–393. https://doi.org/10.1177/0363546516665810
Myer GD, Ford KR, Divine JG, Wall EJ, Kahanov L, Hewett TE (2009) Longitudinal assessment of noncontact anterior cruciate ligament injury risk factors during maturation in a female athlete: a case report. J Athl Train 44:101–109. https://doi.org/10.4085/1062-6050-44.1.101
Nicholls M, Aspelund T, Ingvarsson T, Briem K (2018) Nationwide study highlights a second peak in ACL tears for women in their early forties. Knee Surg Sport Traumatol Arthrosc 26:648–654. https://doi.org/10.1007/s00167-017-4807-0
Petrovic M, Sigurðsson HB, Sigurðsson HJ, Sveinsson T, Briem K (2020) Effect of sex on anterior cruciate ligament injury-related biomechanics during the cutting maneuver in preadolescent athletes. Orthop J Sport Med 8:1–7. https://doi.org/10.1177/2325967120936980
Quatman CE, Ford KR, Myer GD, Hewett TE (2006) Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med 34:806–813. https://doi.org/10.1177/0363546505281916
Sankey SP, Azidin RMFR, Robinson MA, Malfait B, Deschamps K, Verschueren S, Staes F, Vanrenterghem J (2015) How reliable are knee kinematics and kinetics during side-cutting manoeuvres? Gait Posture 41:905–911. https://doi.org/10.1016/j.gaitpost.2015.03.014
Sheehan FT, Sipprell WH III, Boden BP (2012) Dynamic sagittal plane trunk control during anterior cruciate ligament injury. Am J Sports Med 40:1068–1074. https://doi.org/10.1177/0363546512437850
Sigurðsson HB, Karlsson J, Snyder-Mackler L, Briem K (2021) Kinematics observed during ACL injury are associated with large early peak knee abduction moments during a change of direction task in healthy adolescents. J Orthop Res 39:2281–2290. https://doi.org/10.1002/jor.24942
Sigurðsson HB, Sveinsson Þ, Briem K (2018) Timing, not magnitude, of force may explain sex-dependent risk of ACL injury. Knee Surg Sport Traumatol Arthrosc 26:2424–2429. https://doi.org/10.1007/s00167-018-4859-9
Tranberg R, Saari T, Zügner R, Kärrholm J (2011) Simultaneous measurements of knee motion using an optical tracking system and radiostereometric analysis (RSA). Acta Orthop 82:171–176. https://doi.org/10.3109/17453674.2011.570675
Webster KE, Hewett TE (2022) Anterior cruciate ligament injury and knee osteoarthritis: an umbrella systematic review and meta-analysis. Clin J Sport Med 32:145–152. https://doi.org/10.1097/JSM.0000000000000894
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD (2016) Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med 44:1861–1876. https://doi.org/10.1177/0363546515621554
Zebis MK, Aagaard P, Andersen LL, Hölmich P, Clausen MB, Brandt M, Husted RS, Lauridsen HB, Curtis DJ, Bencke J (2022) First-time anterior cruciate ligament injury in adolescent female elite athletes: a prospective cohort study to identify modifiable risk factors. Knee Surg Sport Traumatol Arthrosc 30:1341–1351. https://doi.org/10.1007/s00167-021-06595-8
Acknowledgements
The authors would like to thank all the participants who took part in this study.
Funding
This study was supported by grants from The Icelandic Research Fund (185359-051).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declate that they have no potential conflict of interest.
Ethical approval
The study was approved by the Icelandic National Bioethics Committee VSNb20112020011/03.7).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ghasemi, M., Sigurðsson, H.B., Sveinsson, Þ. et al. Boys demonstrate greater knee frontal moments than girls during the impact phase of cutting maneuvers, despite age-related increases in girls. Knee Surg Sports Traumatol Arthrosc 31, 1833–1839 (2023). https://doi.org/10.1007/s00167-023-07340-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-023-07340-z