
Abstract
Aims/hypothesis
The aim of the study was to examine the impact of statin or omega-3-acid ethyl esters 90 (omega-3 EE90; omega-3-acid ethyl esters 90 refers to a mixture of ethyl esters of n-3 fatty acids) on estimated cardiovascular disease (CVD) risk in community-based people with type 2 diabetes but without known CVD and not taking lipid-lowering therapy.
Methods
A central computer randomised 800 patients in 59 UK general practices to atorvastatin (n = 401, 20 mg/day) or placebo (n = 399) and omega-3 EE90 (n = 397, 2 g/day) or placebo (n = 403) in a concealed factorial manner. Participants with LDL-cholesterol <2.6 mmol/l, triacylglycerol <1.5 mmol/l and estimated 10-year CVD risk <20% were compared at 4 months.
Results
Mean (SD) age was 63.5 (11.7) years, HbA1c 6.9 (1.1) % and known diabetes duration (median [interquartile range]) was 4 (2–8) years. Fifty-seven per cent were men, 90% white and 74% had an estimated 10-year CVD risk ≥20%. Of 732 patients with 4-month data, more allocated atorvastatin (n = 371) compared with placebo (n = 361) achieved LDL-cholesterol <2.6 mmol/l (91% vs 24%, p < 0.001) and had estimated 10-year CVD risks <20% (38% vs 26%, p < 0.001). No differences were seen between those allocated omega-3 EE90 (n = 371) compared with placebo (n = 361) for participants achieving triacylglycerol <1.5 mmol/l (65% vs 60%, p = 0.18) or estimated 10-year CVD risks <20% (34% vs 30%, p = 0.18). There were no side effects of note.
Conclusions/interpretation
Many community-based diabetic patients without known CVD remain at high CVD risk despite statin treatment and require additional risk-reduction strategies. The impact of omega-3 EE90 on CVD risk will remain uncertain until clinical endpoint trial results are available.
Trial registration: ISRCT no. 76737502
Funding: The study was funded by Pfizer.
Similar content being viewed by others


Introduction
People with type 2 diabetes mellitus have a cardiovascular disease (CVD) risk two to four times greater than the general population [1]. Some studies indicate they are at equivalent risk to non-diabetic individuals who have survived a myocardial infarction [2], although this depends on the population studied [3]. Reducing cardiovascular risk to improve clinical outcomes for patients with type 2 diabetes is therefore a major priority, particularly since the incidence of this condition is likely to double over the next two decades [4].
In addition to the benefits of improved glucose and blood-pressure control in reducing diabetic complications [5, 6], 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG CoA) reductase inhibitors can reduce major vascular events by more than one-third by reducing LDL-cholesterol [7]. As trials have been carried out predominately in hospital-based populations, the extent to which people with type 2 diabetes managed in primary care are at sufficiently high CVD risk to require routine LDL-cholesterol (LDL-C) lowering, as guidelines recommend [8, 9], is unclear.
There is also increasing interest in treating other lipoprotein abnormalities in type 2 diabetes by reducing triacylglycerol [10, 11] and/or raising HDL-cholesterol (HDL-C) [12, 13]. Fibrate therapy can improve both of these, but there are concerns about combining them with statins because of adverse events [14] and the failure of the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) trial to demonstrate CVD-risk reduction with fenofibrate [15]. Omega-3 (n-3) polyunsaturated fatty acids (PUFA) are an alternative triacylglycerol-lowering therapy; there is strong epidemiological evidence suggesting favourable outcomes in people with type 2 diabetes with high omega-3 PUFA intake [16] and improvements in CVD-risk-factor profiles [17, 18]. Studies involving wider populations have been less supportive [19], and a prospective primary-care trial is required to establish whether omega-3 PUFA, alone or with a statin, can improve risk-factor levels and reduce estimated CVD risk as a prelude to cardiovascular-outcome studies.
We report here the primary 4 month results of the 1 year Atorvastatin in Factorial with Omega-3 EE90 Risk Reduction in Diabetes (AFORRD) Trial, which examined the impact of statin or omega-3-acid ethyl esters 90 (omega-3 EE90; omega-3-acid ethyl esters 90 refers to a mixture of ethyl esters of n-3 fatty acids) treatment on lipid profiles and estimated CVD risk in people with type 2 diabetes.
Methods
AFORRD was a 1 year randomised controlled trial, designed and run by the University of Oxford Diabetes Trials Unit (DTU) in an academic collaboration with Pfizer (see Electronic supplementary material [ESM]). Only the primary results at 4 months are reported here. The protocol was approved by local and national ethics committees and regulatory agencies, and the study was carried out in accordance with the Declaration of Helsinki and good clinical practice guidelines.
Subjects
A total of 883 patients with type 2 diabetes for at least 3 months, aged ≥18 years, with no known CVD events, and not thought by their general practitioner to be at high enough CVD risk to require immediate lipid-lowering therapy, were recruited in primary care and gave written informed consent. Exclusion criteria were: taking lipid-lowering therapy; triacylglycerol >8 mmol/l; impaired hepatic function (alanine aminotransferase [ALT] greater than two times upper limit of normal), uncontrolled diabetes (HbA1c > 10%), uncontrolled hypertension (blood pressure persistently >160/100 mmHg) or elevated creatine kinase (greater than three times upper limit of normal). The degree to which the general-practices enrolment was representative was assessed by comparing the practices’ 2005 Quality and Outcomes Framework assessment data [20] with those from all English general practices.
Trial design
Eight-hundred eligible patients were randomised to double-blind study medication 2 weeks after their screening visit. Computerised central randomisation was used to allocate them in a two-by-two factorial manner to atorvastatin (Lipitor, 20 mg/day; Pfizer, Tadworth, UK) or matching placebo and, simultaneously, to omega-3 EE90 (Omacor, 2 g/day; Pronova BioPharma Norge AS, Lysaker, Norway) or matching placebo (olive oil, 2 g/day, Pronova BioPharma Norge AS). Omega-3 EE90 capsules contained 46% eicosapentaenoic acid and 38% docosahexaenoic acid. Patients and study staff were masked to study medication group assignment and patients were asked to swallow capsules whole to avoid unmasking. Lipid profiles were measured at entry and at 4 months, with CVD risks estimated using the UK Prospective Diabetes Study (UKPDS) risk engine.[21, 22]
Biochemical and clinical assessments
Ambient-temperature plasma samples were mailed overnight to the DTU laboratory, which has clinical pathology accreditation and participates in the UK National External Quality Assessment Scheme (Wolfson EQA Laboratory, Birmingham, UK) and the Welsh External Quality Assessment Scheme (Quality Laboratory, Cardiff and Vale NHS Trust, Cardiff, UK). HbA1c was measured by high-performance liquid chromatography (Bio-Rad Variant II Automated Glycosylated Hemoglobin Analyzer, Bio-Rad Laboratories, Hemel Hempstead, UK), normal range 4.5–6.2%, and certified by the National Glycohaemoglobin Standardisation Programme [23]. Other biochemical analyses were performed on an Olympus AU400 automated chemistry analyser (Olympus Optical, Southall, UK). Total cholesterol was measured by an enzymatic colorimetric endpoint method (CHOD-PAP method) using cholesterol oxidase and esterase and a peroxidase-catalysed reaction for production of quinoneimine. LDL-C was measured directly using a Genzyme kit (Biostat, Stockport, UK) with lipoproteins other than LDL disrupted and removed enzymically. HDL-C was measured directly with anti-human beta lipoprotein antibody to bind to lipoproteins other than HDL-C (LDL-C, very-low-density-lipoprotein-cholesterol and chylomicrons) using the Olympus system HDL-C kit. Triacylglycerol was measured using the enzymatic, colorimetric, GPO-PAP method with hydrolysis by lipases and quinoneimine as the indicator. Fasting plasma glucose was measured by an enzymatic UV test (hexokinase method) using hexokinase and glucose-6-phosphate dehydrogenase for production of NADH.
Blood pressure was measured with an automated sphygmomanometer (Omron 705CP-II, Omron Healthcare, Kyoto, Japan). BMI was calculated as weight (kg) divided by the square of the height (m).
Trial management
The DTU co-ordinating centre had overall responsibility for the day-to-day conduct of AFORRD. Pfizer supplied study medication, monitored clinical centres and undertook adverse-event reporting. The DTU trials management system (TMS) used an internet-based electronic data capture platform (MACRO v3; Infermed, London, UK) to collect study data. Patient questionnaire data were double entered and laboratory results transferred electronically to the TMS, which validated entered data, tracked resolution of discrepancies, monitored protocol compliance and audited study performance metrics.
Endpoints
At 4 months, the two prespecified co-primary endpoints were: (1) proportion of patients in the atorvastatin arm achieving LDL-C levels <2.6 mmol/l, irrespective of their omega-3 EE90 allocation; (2) proportion of patients in the omega-3 EE90 arm achieving triacylglycerol <1.5 mmol/l, irrespective of their atorvastatin allocation. A pre-specified secondary endpoint for both arms was the proportion of patients with an estimated 10 year CVD risk <20%.
Sample size
Sample-size calculations assumed atorvastatin 20 mg/day would reduce LDL-cholesterol by 35%, compared with 6% for placebo, irrespective of omega-3 EE90 allocation. It was anticipated from a population thought representative of those to be studied that 69.3% and 22.5%, respectively, would achieve LDL-C <2.6 mmol/l. A total of 800 participants were randomised: this ensured that there were 704 evaluable patients, allowing for a maximum 12% loss to follow-up to give >99% power (α = 5%) to detect an anticipated 46.8% difference in proportions (95% CI 41.3–52.3%).
Sample size calculations for omega-3 EE90 assumed that 2 g/day would reduce triacylglycerol levels by 15%, compared with no change for placebo, irrespective of atorvastatin allocation. It was anticipated that 61.2% and 49.5% of patients, respectively, would achieve triacylglycerol <1.5 mmol/l, giving 92% power (α = 5%) to detect an anticipated 11.7% difference in proportions (95% CI 5.6–17.8%) with 704 evaluable patients.
Statistical analysis
Demographic and clinical data were summarised for screened and randomised patients using appropriate measures of central tendency and dispersion or number (%). The χ 2 and Wilcoxon tests were used for categorical and continuous variables respectively to compare between-group differences. Ten year CVD risk was estimated from age, duration of diagnosed diabetes, sex, self-reported ethnicity, smoking status, HbA1c, systolic BP and total cholesterol to HDL-C ratio using the UKPDS risk engine [21, 22]. Adherence to study medication was defined as a returned tablet count commensurate with 80–120% of those dispensed. Between-group risk-factor levels were compared for patients with LDL-C above and below 2.6 mmol/l, and above and below 2.0 mmol/l, and for those with and without the metabolic syndrome (National Cholesterol Education Program Third Adult Treatment Panel criteria [24]). Possible study medication interaction effects were sought using a general linear model for LDL-C and a generalised linear model (γ distribution) for positively skewed triacylglycerol. Statistical analyses used SAS 9.1.3 (SAS Institute, Cary, NC, USA).
Results
General practices
The 59 practices had 589,091 registered type 2 diabetic patients whose clinical characteristics did not differ significantly from patients registered with English general practices as a whole. Quality and Outcomes Framework returns showed similar mean (±1SD) proportions of their patients to have HbA1c values < 10% (90.6 ± 5.4% vs 88.6 ± 5.4%) and <7.5% (60.1 ± 8.4% vs 58.7 ± 12.1%), and total cholesterol values <5.0 mmol/l (72.0 ± 8.4% vs 71.3 ± 11.9%). Patient enrolment data were monitored in 25 practices who approached 70.4% of their patients with type 2 diabetes who were not on lipid-lowering therapy and had no history of a CVD event. Of these patients, 54% returned expressions of interest of whom 90% were invited to attend an AFORRD screening visit. Forty-six per cent did not reply or were unwilling to participate. Of 883 screened patients, 83 were excluded, mainly because of elevated ALT (22.9%), triacylglycerol (4.8%) and/or HbA1c (30.1%) values (Fig. 1). These patients differed from the 800 randomised patients (Table 1) otherwise only in that the mean age was 6 years younger (p < 0.001) and there was a higher prevalence of smokers (23.2% vs 11.9%).

Flow chart for study
Randomised patients
The 800 randomised patients had mean age 63.5 ± 11.7 years, HbA1c 6.9 ± 1.1%, blood pressure 138/78 ± 16/9 mmHg, LDL-C 3.2 ± 0.8 mmol/l, HDL-C 1.2 ± 0.3 mmol/l, body mass index 30.8 ± 6.2 kg/m2 and waist circumference 103 ± 14 cm (Table 1). Median (interquartile range [IQR]) triacylglycerol was 1.5 (1.1–2.2) mmol/l, duration of known diabetes was 4 (2–8) years; 90% were white and 57% were men. The number of patients randomised per practice ranged from two to 56. There were no statistically significant between-group baseline differences.
At entry, median estimated 10 year CVD risk was 29.7% for all patients, 36.4% for men and 21.9% for women (Table 1). Overall, 74.1% of patients had an estimated 10 year CVD risk ≥20% (87.1% of men, 56.5% of women) and 94.4% had risk ≥10% (98.9% of men, 88.2% of women). The distribution of estimated 10 year CVD risks was similar whether patients had LDL-C above or below 2.6 mmol/l and whether they had, or did not have, metabolic syndrome. Of the 22.1% patients with LDL-C <2.6 mmol/l, 72.3% (82.5% of men, 47.1% of women) had estimated 10 year CVD risks ≥20%. Of the 25.8% patients without metabolic syndrome, 69.9% (79.3% of men, 47.5% of women) had estimated 10 year CVD risks ≥20%. Comparison of demographic, clinical and biochemical data for those with LDL-C above or below 2.6 mmol/l and for those with or without metabolic syndrome revealed few differences beyond the criteria used to distinguish them. There were 732 patients with the requisite 4 month data for post-interventional atorvastatin and omega-3 EE90 analyses. Antihypertensive therapies did not change between baseline and 4 months in these patients and none received open-label lipid-lowering therapies.
Atorvastatin intervention
At 4 months, adherence to atorvastatin study medication was 91.8%. More patients in the atorvastatin group (n = 371) than the placebo group (n = 361) achieved LDL-C <2.6 mmol/l (91% vs 24%, p < 0.0001), triacylglycerol <1.5 mmol/l (71% vs 55%, p < 0.0001) and estimated 10 year CVD risk <20% (38% vs 26%, p < 0.0001; Table 2). Corresponding proportions achieving LDL-C <2.0 mmol/l were 70.1% vs 6.6% (p < 0.0001).
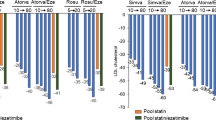
Mean reductions (relative to placebo) were: LDL-C 1.4 mmol/l (44%, p < 0.0001); triacylglycerol 0.44 mmol/l (21%, p < 0.0001); and estimated 10 year CVD risk 6.7% (21%, p < 0.0001; Table 2, Fig. 2a). There were also mean reductions in total cholesterol of 1.6 mmol/l (32%, p < 0.001), systolic blood pressure 4.3 mmHg (3%, p = 0.0002) and diastolic blood pressure 1.5 mmHg (2%, p = 0.008), but there was an increase in HbA1c of 0.3% (4%, p < 0.0001).

Mean percentage change, from baseline to 4 months, in systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (Total-C), LDL-C, HDL-C, triacylglycerol, HbA1c and estimated 10 year CVD risk (eCVD risk) in (a) patients allocated to atorvastatin (black) or placebo (white), irrespective of their omega-3 EE90 allocation; and (b) patients allocated to omega-3 EE90 (black) or placebo (white), irrespective of their atorvastatin allocation. Baseline values for SBP, DBP, Total-C, LDL-C, HDL-C, triacylglycerol, HbA1c and eCVD risk: a 139 mmHg, 78 mmHg, 5.1 mmol/l, 3.2 mmol/l, 1.15 mmol/l, 1.5 mmol/l, 7.0% and 30%, respectively; b 137 mmHg, 77 mmHg, 5.0 mmol/l, 3.2 mmol/l, 1.16 mmol/l, 1.5 mmol/l, 6.9%, 29%. Percentage change in SBP, DBP, Total-C, LDL-C, HDL-C, triacylglycerol, HbA1c and eCVD risk: a −3 (p = 0.0002), −2 (p = 0.008), −32 (p < 0.0001), −44 (p < 0.0001), −6 (p < 0.0001), −21 (p < 0.0001), +4 (p < 0.0001), −21 (p < 0.0001); b +0.5 (p = 0.83), +0.7 (p = 0.33), +0.3 (p = 0.93), 0.0 (p = 0.82), +1.4 (p = 0.08), −5.6 (p = 0.003), 0.0 (p = 0.62), −0.2 (p = 0.6)
Omega-3 EE90 intervention
At 4 months, adherence to omega-3 EE90 study medication was 91.3%. No difference was seen in the proportion of patients between the omega-3 EE90 group (n = 371) and the placebo group (n = 361) who achieved LDL-C <2.6 mmol/l (58% vs 57%, p = 0.87); similarly, no differences were seen in the proportions who achieved triacylglycerol <1.5 mmol/l (65% vs 60%, p = 0.18) or estimated 10 year CVD risk <20% (34% vs 30%, p = 0.18; Table 2).
There was a mean reduction (relative to placebo) in triacylglycerol of 0.09 mmol/l (5.6%, p = 0.003) but no significant changes in LDL-C, estimated 10 year CVD risk, total cholesterol, systolic or diastolic blood pressure or HbA1c (Table 2, Fig. 2b).
Study medication interaction effects
No statistical interactions were observed between atorvastatin and omega-3 EE90 with regard to changes in LDL-C (p = 0.28), triacylglycerol (p = 0.13) or estimated 10 year CVD risk (p = 0.09).
Safety data
There were no deaths or episodes of myositis or rhabdomyolysis, and the numbers of serious or non-serious adverse events reported did not differ between groups (Table 3). In the omega-3 EE90 arm there was a mean 2.3 U/l increase in ALT (p = 0.012), relative to placebo, but no significant difference in creatine kinase. In the atorvastatin arm there was a mean 1.5 U/l increase in alanine aminotransferase (p = 0.0014) and 3.7 U/l increase in creatine kinase (p = 0.0138), relative to placebo.
Discussion
This trial showed that most patients with type 2 diabetes of short duration and without overt CVD in primary care are at high risk of CVD. Despite recruiting patients not considered by their general practitioner to meet the then current indications for statin treatment, we found 74% to be at high estimated 10 year CVD risk (≥20%) and 94% to be at moderate to high risk (≥10%). Treatment with atorvastatin 20 mg/day for 4 months resulted in highly significant relative reductions in LDL-C (44%) and triacylglycerol (21%), together with small but significant reductions in both systolic and diastolic blood pressure and a 21% relative reduction in 10 year CVD risk. Nevertheless, despite statin therapy, most patients remained at high residual CVD risk, with 62% having an estimated 10 year CVD risk ≥20%. This degree of untreated risk suggests that lipid-lowering drug therapy needs to be intensified and that other cardioprotective interventions are required. In this study, however, 4 months’ treatment with omega-3 EE90 2 g/day did not demonstrate any significant improvements in lipid, lipoproteins, blood pressure or estimated CVD risk.
AFORRD was a multi-centre, rigorously designed and conducted, randomised, placebo-controlled, two-by-two factorial trial. Patients were recruited exclusively from primary care to avoid potential selection bias associated with secondary-care recruitment. Unlike most clinical outcome trials of statin therapy in type 2 diabetes, there was no placebo or active run-in period that could have complicated assessment of tolerability and therapy compliance with an observed study medication adherence of 92%. Clinical measurements, including blood pressure, were carefully standardised [25]. CVD risk was assessed using the UK Prospective Diabetes Study risk engine [22], which provides more accurate risk assessments for patients with diabetes than the Framingham study risk equation [26], and has been validated using Collaborative Atorvastatin Diabetes Study (CARDS) data [27]. A potential limitation, in common with other risk equations, is that it was not designed specifically to assess the impact of changes in risk factors on CVD risk. The 21% estimated relative CVD risk reduction observed was, however, consistent with the Cholesterol Treatment Trialist Collaborators’ (CTTC) systematic prospective meta-analysis [28] that reported cholesterol-lowering treatment efficacy in 90,056 participants (18,686 with diabetes) in 14 randomised trials of statins. Overall, the CTTC showed a 21% reduction (95% CI 16–26%) in major vascular events per 1.0 mmol/l reduction in LDL-C in diabetic patients. Since our observed LDL-C reduction was 1.4 mmol/l, the observed 21% estimated relative CVD risk reduction may underestimate the potential benefit of treatment.
The effects of atorvastatin on lipid and lipoprotein concentrations were consistent with previous findings. A meta-analysis of 164 short-term statin trials reported a 43% reduction in LDL-C with atorvastatin 20 mg/day, compared with the 44% reduction we observed [29]. The 21% reduction in triacylglycerol concentration was similar to the 19% reduction reported with atorvastatin 10 mg/day by CARDS in patients with type 2 diabetes [7]. However, the 4.3 mmHg systolic and 1.6 mmHg reduction in diastolic blood pressure was unexpected. There is limited short-term trial evidence that atorvastatin treatment may reduce blood pressure in hypertensive and dyslipidaemic patients [30–33], possibly by improving endothelium-dependent vascular function [34]. A single uncontrolled trial [35] in patients with type 2 diabetes showed a 10 mmHg reduction in diastolic blood pressure, but this may partly be explained by habituation and regression to the mean. Equally, although our results were based on a rigorously conducted short-term trial, we cannot exclude the possibility that they are due to chance. Unfortunately, longer-term outcome trials are not particularly helpful in assessing the possible impact of atorvastatin on blood pressure since they are likely to be confounded by the introduction and uptitration of antihypertensive agents during their time course. Antihypertensive therapies did not change in AFORRD between baseline and 4 months, so our results provide an unconfounded assessment of the short-term impact of atorvastatin on both blood pressure and glycaemic control.
No consistent relationship between atorvastatin treatment and changes in glycated haemoglobin or other glycaemic measure has been reported in short-term trials that have examined the efficacy and safety of statin therapy in diabetic patients [30, 36–39]. These small studies, however, did not have the statistical power to identify HbA1c changes as small as the 0.3% increase observed in AFORRD. In longer-term outcome trials, increases in antihyperglycaemic agents may mask any small atorvastatin-associated glycaemic changes. Nevertheless, in CARDS, which involved 2838 patients, the mean HbA1c was 0.1% higher (p < 0.05) after 4 years of treatment with atorvastatin 10 mg/day compared with placebo and the prevalence of insulin therapy alone, or in combination with oral antihyperglycaemic agents, was 2% higher in the group receiving atorvastatin compared with the group receiving placebo by the end of the trial.[7] In the Atorvastatin Study for Prevention of coronary heart disease ENdpoints in non-insulin dependent diabetes mellitus (ASPEN) trial, both atorvastatin 10 mg/day and placebo were associated with an increase in HbA1c of 0.2%, but interpretation of these findings is complicated by the high statin drop-in therapy rate in the placebo group [40]. In the Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT TIMI 22) sub-study, among 3,382 patients without pre-existing diabetes, HbA1c increased over a median of 2 years by 0.12 ± 1.41% among those randomised to pravastatin 40 mg/day, and by 0.30 ± 0.56% among those randomised to atorvastatin 80 mg/day (p < 0.0001) [41]. Although it is not possible to conclude definitively that atorvastatin treatment is associated with a deterioration in glycaemic control, and there is no known mechanism that might explain this, our findings and the evidence from other large-scale clinical trials suggest that use of atorvastatin may be associated with a small deterioration in glycaemic control. Nevertheless, such an effect would be more than offset by a substantial reduction, of more than one-third, in CVD risk [7].
The lack of effect of omega-3 EE90 2 g/day on total cholesterol, HDL-C and LDL-C is consistent with the results of our recent meta-analysis examining the effect of non-dietary supplementation with omega-3 PUFA on lipids and lipoproteins in 18 trials involving a total of up to 999 patients with type 2 diabetes [17]. However, the small but statistically significant reduction in triacylglycerol of 0.09 mmol/l (5.6%) in AFORRD was substantially less than the 0.46 mmol/l (95% CI 0.33–0.59) reduction shown in the meta-analysis. This may be because the median fasting triacylglycerol in AFORRD patients at entry was only modestly elevated at 1.5 mmol/l and triacylglycerol lowering is greater with higher baseline levels. As triacylglycerol lowering appears to be dose dependent, with up to a 30% reduction reported in hypertriacylglycerolaemic patients given omega-3 EE90 4 g/day daily [42], the 2 g/day dose used in AFORRD may have been too small. On the other hand, putative cardioprotective mechanisms other than triacylglycerol lowering may explain the post-myocardial infarction mortality risk reduction observed in non-diabetic patients in the Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI) Prevenzione trial [43] and the hypercholesterolaemic patients in the Japan Eicosapentaenoic acid Lipid Intervention Study (JELIS) trial [44]. These include anti-arrhythmic, haemostatic and anti-inflammatory effects and blood-pressure lowering [45]. AFORRD showed no change in systolic or diastolic blood pressure, but in our meta-analysis, omega-3 PUFA supplementation decreased diastolic blood pressure by 1.8 mmHg in patients with diabetes, with no effect on systolic blood pressure [18]. Blood-pressure reduction with omega-3 PUFA appears to be dose-dependent [46] and again the omega-3 EE90 2 g/day dose used in AFORRD may have been too small. The role of omega-3 EE90 in helping to manage CVD risk in type 2 diabetes remains unclear [47], but the results of two ongoing 10,000 patient clinical endpoint trials, A Study of Cardiovascular Events iN Diabetes (ASCEND) [48] and Outcome Reduction with Initial Glargine Intervention (ORIGIN) [49], which are both using omega-3 EE90 1 g/day, may help to clarify it.
The AFORRD trial results have a number of important implications for clinical practice. They show that most patients in primary care with type 2 diabetes of short duration without known CVD are at high CVD risk. Our findings extend the evidence base for current clinical guidelines and support their recommendations that all patients with type 2 diabetes aged 40 years or older should be treated with a statin, unless there is a specific contraindication [8, 50]. AFORRD found, however, that despite statin treatment, many patients remain at high residual CVD risk and require additional risk-reduction strategies, including intensification of lipid-lowering drug therapy and the introduction of other cardioprotective interventions.
Abbreviations
- ALT:
-
alanine aminotransferase
- AFORRD:
-
Atorvastatin in Factorial with Omega-3 EE90 Risk Reduction in Diabetes
- CARDS:
-
Collaborative Atorvastatin Diabetes Study
- CVD:
-
cardiovascular disease
- DTU:
-
Diabetes Trials Unit
- HDL-C:
-
HDL-cholesterol
- LDL-C:
-
LDL-cholesterol
- omega-3 EE90:
-
omega-3-acid ethyl esters 90
- omega-3 PUFA:
-
omega-3 (n-3) polyunsaturated fatty acid
- TMS:
-
trial management system
- UKPDS:
-
UK Prospective Diabetes Study
References
Stamler J, Vaccaro O, Neaton J, Wentworth D (1993) Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care 16:434–444
Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M (1998) Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 339:229–234
Evans JM, Ogston SA, Emslie-Smith A, Morris AD (2006) Risk of mortality and adverse cardiovascular outcomes in type 2 diabetes: a comparison of patients treated with sulfonylureas and metformin. Diabetologia 49:930–936
King H, Aubert RE, Herman WH (1998) Global burden of diabetes, 1995–2025: prevalence, numerical estimates, and projections. Diabetes Care 21:1414–1431
UK Prospective Diabetes Study (UKPDS) Group (1998) Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352:837–853
UK Prospective Diabetes Study Group (1998) Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ 317:703–713
Colhoun HM, Betteridge DJ, Durrington PN et al (2004) Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. The Lancet 364:685–696
British Cardiac Society, British Hypertension Society, Diabetes UK, HEART UK, Primary Care Cardiovascular Society, Stroke Association (2005) JBS 2: Joint British Societies’ guidelines on prevention of cardiovascular disease in clinical practice. Heart 91(Suppl 5):v1–52
Department of Health (2000) National service framework for coronary heart disease. Department of Health, London
American Diabetes Association (2005) Standards of medical care in diabetes. Diabetes Care 28(Suppl 1):S4–S36
Sarwar N, Danesh J, Eiriksdottir G et al (2007) Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 western prospective studies. Circulation 115:450–458
Rubins HB, Robins SJ, Collins D et al (1999) Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. N Engl J Med 341:410–418
Asztalos BF, Collins D, Cupples LA et al (2005) Value of high-density lipoprotein (HDL) subpopulations in predicting recurrent cardiovascular events in the Veterans Affairs HDL Intervention Trial. Arterioscler Thromb Vasc Biol 25:2185–2191
Jacobson TA, Zimmerman FH (2006) Fibrates in combination with statins in the management of dyslipidemia. J Clin Hypertens 8:35–41
Keech A, Simes RJ, Barter P et al (2005) Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial [erratum in Lancet 2006;368:1415]. Lancet 366:1849–1861
Hu FB, Cho E, Rexrode KM, Albert CM, Manson JE (2003) Fish and long-chain omega-3 fatty acid intake and risk of coronary heart disease and total mortality in diabetic women. Circulation 107:1852–1857
Hartweg J, Farmer AJ, Holman RR, Neil HA (2007) Meta-analysis of the effects of n-3 polyunsaturated fatty acids on haematological and thrombogenic factors in type 2 diabetes. Diabetologia 50:250–258
Hartweg J, Farmer AJ, Perera R, Holman RR, Neil HA (2007) Meta-analysis of the effects of n-3 polyunsaturated fatty acids on lipoproteins and other emerging lipid cardiovascular risk markers in patients with type 2 diabetes. Diabetologia 50:1593–1602
Hooper L, Thompson RL, Harrison RA et al. (2004) Omega 3 fatty acids for prevention and treatment of cardiovascular disease. Cochrane Database of Syst Rev, Issue 4, Art. no.: CD003177. doi:10.1002/14651858.CD003177.pub2
Department of Health (2003) Investing in general practice: the new general medical services contract. Department of Health, London. Available from http://www.dh.gov.uk/en/Healthcare/Primarycare/Primarycarecontracting/GMS/DH_4125637?, accessed 6 October 2008
Stevens RJ, Kothari V, Adler AI, Stratton IM, United Kingdom Prospective Diabetes Study (UKPDS) Group (2001) The UKPDS risk engine: a model for the risk of coronary heart disease in type II diabetes (UKPDS 56). Clin Sci (Lond) 101:671–679 [erratum in: Clin Sci (Lond) 102:679]
UKPDS Risk Engine version 2.0. Available from http://www.dtu.ox.ac.uk/riskengine/index.php, accessed 6 October 2008
UK Prospective Diabetes Study Group (1994) UK Prospective Diabetes Study (UKPDS) XI: biochemical risk factors in type 2 diabetic patients at diagnosis compared with age-matched normal subjects. Diabet Med 11:534–544
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). J Am Med Assoc 285:2486–2497
Coleman A, Freeman P, Steel S, Shennan A (2006) Validation of the Omron 705IT (HEM-759-E) oscillometric blood pressure monitoring device according to the British Hypertension Society protocol. Blood Press Monit 11:27–32
Song SH, Brown PM (2004) Coronary heart disease risk assessment in diabetes mellitus: comparison of UKPDS risk engine with Framingham risk assessment function and its clinical implications. Diabet Med 21:238–245
Mount Hood 4 Modeling Group (2007) Computer modeling of diabetes and its complications: a report on the Fourth Mount Hood Challenge Meeting. Diabetes Care 30:1638–1646
Baigent C, Keech A, Kearney PM et al (2005) Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 366:1267–1278 [erratum in Lancet 2005;366:1358]
Law M, Wald N, Rudnicka A (2003) Quantifying effect of statins on low density lipoprotein cholesterol, ischaemic heart disease, and stroke: systematic review and meta-analysis. Br Med J 326:1323–1427
Ferrier KE, Muhlmann MH, Baguet JP et al (2002) Intensive cholesterol reduction lowers blood pressure and large artery stiffness in isolated systolic hypertension. J Am Coll Cardiol 39:1020–1025
Kanbay M, Yildirir A, Bozbas H et al (2005) Statin therapy helps to control blood pressure levels in hypertensive dyslipidemic patients. Ren Fail 27:297–303
Strazzullo P, Kerry SM, Barbato A, Versiero M, D’Elia L, Cappuccio FP (2007) Do statins reduce blood pressure? A meta-analysis of randomised, controlled trials. Hypertension 49:792–798
Golomb BA, Dimsdale JE, White HL, Ritchie JB, Criqui MH (2008) Reduction in blood pressure with statins: results from the UCSD Statin Study, a randomized trial. Arch Intern Med 168:721–727
Chopra V, Choksi PU, Cavusoglu E (2007) Beyond lipid lowering: the anti-hypertensive role of statins. Cardiovasc Drugs Ther 21:161–169
Velussi M (2002) Long-term (18-month) efficacy of atorvastatin therapy in type 2 diabetes at cardiovascular risk. Nutr Metab Cardiovasc Dis 12:29–35
Best JD, Nicholson GC, O’Neal DN et al (1996) Atorvastatin and simvastatin reduce elevated cholesterol in non-insulin dependent diabetes. Diabet Nutr Metab 9:74–80
Diabetes Atorvastin Lipid Intervention Study Group (2001) The effect of aggressive versus standard lipid lowering by atorvastatin on diabetic dyslipidemia: the DALI study: a double-blind, randomized, placebo-controlled trial in patients with type 2 diabetes and diabetic dyslipidemia. Diabetes Care 24:1335–1341
Aguilar-Salinas CA, Gomez-Perez FJ, Posadas-Romero C et al (2000) Efficacy and safety of atorvastatin in hyperlipidemic, type 2 diabetic patients. A 34-week, multicenter, open-label study. Atherosclerosis 152:489–496
Freed MI, Ratner R, Marcovina SM et al (2002) Effects of rosiglitazone alone and in combination with atorvastatin on the metabolic abnormalities in type 2 diabetes mellitus. Am J Cardiol 90:947–952
Knopp RH, d’Emden M, Smilde JG, Pocock SJ (2006) Efficacy and safety of atorvastatin in the prevention of cardiovascular end points in subjects with type 2 diabetes: the Atorvastatin Study for Prevention of Coronary Heart Disease Endpoints in non-insulin-dependent diabetes mellitus (ASPEN). Diabetes Care 29:1478–1485
Sabatine MS WS, Morrow DA, McCabe CH, Cannon P (2004) High-dose atorvastatin associated with worse glycemic control: A PROVE-IT TIMI 22 substudy. American Heart Association Scientific Sessions 10 November 2004, Abstract 3848. Circulation 110(Suppl 111):834
Durrington PN, Bhatnagar D, Mackness MI et al (2001) An omega-3 polyunsaturated fatty acid concentrate administered for one year decreased triglycerides in simvastatin treated patients with coronary heart disease and persisting hypertriglyceridaemia. Heart 85:544–548
GISSI-Prevenzione Investigators (1999) Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione Trial. Lancet 354:447–455
Yokoyama M, Origasa H, Matsuzaki M et al (2007) Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis. Lancet 369:1090–1098 [erratum appears in Lancet. 2007;370:220]
Din JN, Newby DE, Flapan AD (2004) Omega 3 fatty acids and cardiovascular disease—fishing for a natural treatment. BMJ 328:30–35
Morris MC, Sacks F, Rosner B (1993) Does fish oil lower blood pressure? A meta-analysis of controlled trials. Circulation 88:523–533
De Caterina R, Madonna R, Bertolotto A, Schmidt EB (2007) n-3 fatty acids in the treatment of diabetic patients: biological rationale and clinical data. Diabetes Care 30:1012–1026
The ASCEND Trial (A Study of Cardiovascular Events iN Diabetes) (2008). Available from http://www.ctsu.ox.ac.uk/ascend/, accessed 6 October 2008
The ORIGIN Trial (Outcome Reduction with Initial Glargine Intervention) (2008) Available from http://www.clinicaltrials.gov/ct2/results?term = NCT00069784, accessed 6 October 2008
American Diabetes Association (2008) Standards of medical care in diabetes—2008. Diabetes Care 31(Suppl 1):S12–S54
Acknowledgements
We are grateful to Pfizer for provision of funding, atorvastatin study medication and matching placebo tablets and to Pronova BioPharma Norge AS for provision of omega-3 EE90 study medication and matching olive oil capsules. Steering committee members, coordinating centre staff and clinical investigators are listed elsewhere (see ESM).
Duality of interest
Pfizer, the trial Sponsor, had no role in data analysis or interpretation. The company was able to comment on but could not amend this manuscript, which was reviewed and approved by the AFORRD Steering Committee (see ESM). R. R. Holman had full access to all study data and had final responsibility for the decision to submit for publication. R. R. Holman reports receiving grant support from Asahi Kasei Pharma, Bayer Healthcare, Bayer Schering Pharma, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Merck Serono, Novartis, Novo Nordisk, Pfizer, and Sanofi-Aventis, consulting fees from Amylin, Eli Lilly, GlaxoSmithKline, Merck, and Novartis, and lecture fees from Astella, Bayer, GlaxoSmithKline, King Pharmaceuticals, Eli Lilly, Merck, Merck Serono, Novo Nordisk, Takeda and Sanofi-Aventis, and owning shares in Glyme Valley Technology, Glyox and Oxtech. S. Paul reports receiving consulting fees from Amylin. H. A. W. Neil reports receiving consulting fees from Merck, Pfizer, Schering-Plough and Solvay Healthcare.
Author information
Authors and Affiliations
Consortia
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 14.2 KB)
Rights and permissions
About this article
Cite this article
Holman, R.R., Paul, S., Farmer, A. et al. Atorvastatin in Factorial with Omega-3 EE90 Risk Reduction in Diabetes (AFORRD): a randomised controlled trial. Diabetologia 52, 50–59 (2009). https://doi.org/10.1007/s00125-008-1179-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-008-1179-5