
Abstract
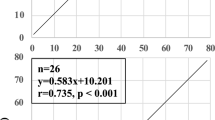
To determine whether single breath end-tidal carbon dioxide (Pe’CO2) measurements accurately estimate arterial PCO2 (PaCO2) in infants and children, 68 healthy infants and children, ASA physical status I or II scheduled for peripheral and lower abdominal surgery requiring endotracheal intubation were studied. A3 ml single breath sample was obtained with a 23-gauge needle which was inserted through the wall of the endotracheal tube below the connector. The mean ± SD Pe’CO233.6 ± 6.9 mmHg did not differ significantly from the corresponding mean ± SD PaCO2 33.6 ± 5.6 mmHg. The coefficient of determination, r2, was 0.97. The authors conclude that single breath Pe’CO2 measurements from the proximal end of the endotracheal tube accurately estimate the PaCO2 in infants and children.
Résumé
Ľétude du CO2 en fin ďexpiration (Pe’CO2) par la technique ďéchantillonage unique chez les jeunes enfants a été développée dans le but ďestimer la tension artérielle du CO2. Soixante-huit jeunes enfants avec un état physique I ou II de la classification ASA ayant été cedulés pour chirurgie abdominale basse ou périphériques sous anesthésie générale avec intubation endotrachéale ont été étudiés. La procédure ďéchantillonage respiratoire simple était obtenue a ľaide ďune ajuille #23 insérée sous le connecteur dans le tube endotracheal en fin ďexpiration. Le et Pe’CO2 ± DS33.6 ± 6.9 mmHg n’était pas significativement différent de la moyenne ± DS 33.6 ± 5.6 mmHg observée pour PaCO2. Le coefficient de détermination, r2, était 0.97. Les auteurs conclurent que la technique de mesure du Pe’CO2 par échantillonage simple peut adéquatement estimer la PaCO2 chez les jeunes enfants même eu ľabsence Ľun moniteur et Pe’CO2 à debit continue.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Fletcher R Deadspace, invasive and non-invasive (Editorial). Br J Anaesth 1985; 57: 245–9.
Brandom BW, Brandom RB, Cook DR. Uptake and distribution in infants: in vivo measurements and computer simulations. Anesth Analg 1983; 62: 404–10.
Fletcher R, Niklason L, Drefeldt B. Gas exchange during controlled ventilation in children with normal and abnormal pulmonary circulation: a study using the single breath test for carbon dioxide. Anesth Analg 1986; 65: 645–52.
Fletcher R, Werner O, Nordstrom L, Jonson B. Sources of error and their correction in the measurement of carbon dioxide elimination using the Siemens-Elema CO2 analyzer. Br J Anaesth 1983; 55: 177–85.
Kaplan RF, Paulus DA. Error in sampling of exhaled gases. Anesth Analg 1983; 62: 955–6.
Badgwell JM, McLeod ME, Lerman J, Creighton RE. End-tidal PCO2 measurements sampled at the distal and proximal ends of the endotracheal tube in infants and children. Anesth Analg 1987; 66: 959–64.
Rose DK, Froese AB. The regulation of PaCO2 during controlled ventilation of children with a t-piece. Can Anaesth Soc J 1979; 26: 104–13.
Ream AK, Reitz BA, Silverberg G. Temperature correction of PCO2 and pH in estimating acid-base status: an example of the emperor’s new clothes? Anesthesiology 1982; 56: 41–4.
Takki S, Aromaa U, Kauste A. The validity and usefulness of the end-tidal PCO2 during anaesthesia. Ann Clin Res 1972; 4: 278–84.
Raemer DB, Francis D, Philip JH, Gabel RA. Variation in PCO2 between arterial blood and peak expired gas during anesthesia. Anesth Analg 1983; 62: 1065–9.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bissonnette, B., Lerman, J. Single breath end-tidal CO2 estimates of arterial PCO2 in infants and children. Can J Anaesth 36, 110–112 (1989). https://doi.org/10.1007/BF03011429
Issue Date:
DOI: https://doi.org/10.1007/BF03011429