
Abstract
Purpose
Human ageing is associated with a regional reduction in cerebral neuronal activity as assessed by numerous studies on brain glucose metabolism and perfusion, grey matter (GM) density and white matter (WM) integrity. As glucose metabolism may impact energetics to maintain myelin integrity, but changes in functional connectivity may also alter regional metabolism, we conducted a cross-sectional simultaneous FDG PET/MR study in a large cohort of healthy volunteers with a wide age range, to directly assess the underlying associations between reduced glucose metabolism, GM atrophy and decreased WM integrity in a single ageing cohort.
Methods
In 94 healthy subjects between 19.9 and 82.5 years (mean 50.1 ± 17.1; 47 M/47F, MMSE ≥ 28), simultaneous FDG-PET, structural MR and diffusion tensor imaging (DTI) were performed. Voxel-wise associations between age and grey matter (GM) density, RBV partial-volume corrected (PVC) glucose metabolism, white matter (WM) fractional anisotropy (FA) and mean diffusivity (MD), and age were assessed. Clusters representing changes in glucose metabolism correlating significantly with ageing were used as seed regions for tractography. Both linear and quadratic ageing models were investigated.
Results
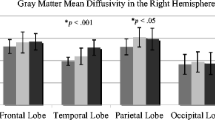
An expected age-related reduction in GM density was observed bilaterally in the frontal, lateral and medial temporal cortex, striatum and cerebellum. After PVC, relative FDG uptake was negatively correlated with age in the inferior and midfrontal, cingulate and parietal cortex and subcortical regions, bilaterally. FA decreased with age throughout the entire brain WM. Four white matter tracts were identified connecting brain regions with declining glucose metabolism with age. Within these, relative FDG uptake in both origin and target clusters correlated positively with FA (0.32 ≤ r ≤ 0.71) and negatively with MD (− 0.75 ≤ r ≤ − 0.41).
Conclusion
After appropriate PVC, we demonstrated that regional cerebral glucose metabolic declines with age and that these changes are related to microstructural changes in the interconnecting WM tracts. The temporal course and potential causality between ageing effects on glucose metabolism and WM integrity should be further investigated in longitudinal cohort PET/MR studies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Human ageing is associated with a reduction in regional brain activity as well as grey (GM) and white matter (WM) degradation. Age-related GM has been investigated by many studies with generally consistent results, showing a decrease of GM volume in the prefrontal, temporal cortex and perirolandic areas. The rate of decrease varies by studies and region and is 1 to 8%/decade, with an increasing rate at ages over 50–60 years [1,2,3,4]. Cortical thinning and cortical grey matter loss is a robust finding across studies, but also subcortical GM loss has been reported [2, 5, 6]. Regarding WM changes with ageing, initial studies mainly focused on macrostructural changes and showed widespread WM atrophy with ageing, which affected all major WM tract areas, independent of atrophy [7, 8]. Also, an increased prevalence of WM hyperintensities (WMH) has been observed, which is associated with demyelination, axonal and capillary loss and disrupted WM microstructure [7]. More recently, both cross-sectional and longitudinal diffusion tensor imaging (DTI) studies have shown a global decrease in fractional anisotropy (FA), a measure of the orientational coherence of water diffusion, indexing WM integrity as it represents a directionally restricted component and an increase in mean diffusivity (MD), which is the directionally averaged magnitude of diffusion, in the vast majority of WM tracts of the brain. Microstructural changes were mostly present in association tracts, connecting cortical areas within the same hemisphere, in commissural tracts, connecting cortical areas in the two hemispheres, and in limbic tracts, and these changes start around the fourth to fifth decade [9,10,11,12,13].
Brain perfusion and glucose metabolism are indirect markers that allow global and regional evaluation of brain function. Since 1982, many studies have investigated changes with ageing by means of perfusion SPECT and FDG PET, with gradually improved spatial resolution, voxel-based instead of volume-of-interest based approaches and improved quantification especially by taking atrophy effects into account (partial volume correction or PVC) [14,15,16,17,18]. The most significant decline of glucose metabolism with ageing, on top of atrophy effects, was observed in the medial frontal lobe and anterior cingulate cortex [18,19,20,21,22,23]. In addition, a decline in the insular cortex, the temporal and parietal cortex as well as in the striatum was found, although these findings were less consistently reported [18,19,20,21,22]. Overall, the magnitude of the decline in cortical cerebral glucose metabolism ranges from 2 to 10% per decade [24,25,26]. Similarly, cerebral blood flow (CBF) also represents an indirect marker of regional neuronal activity and studies using perfusion SPECT [16, 27] or arterial spin labelling (ASL). Both techniques have also shown a similar reduction of 3–6% per decade in ageing, mainly located in the frontal, temporal and parietal lobes [15]. Whether the reduction of perfusion or glucose metabolism follows a linear, quadratic or “hockey-stick” course is still a matter of debate [22, 27, 28].
While initially this decreased regional cerebral neuronal activity was attributed to the loss of underlying neuronal and glial support cells, a residual effect after partial volume correction for GM atrophy is consistently documented [23, 26, 29]. Several recent studies have stressed the importance of using an appropriate PVC, as PVC methods with different approaches may lead to different conclusions with substantial loss in power to detect age-related changes, when CSF is excluded [26, 29] or appropriate modelling of the camera spread function is neglected [30,31,32]. Region-based voxel-wise PVC is a VOI-based PVC using the geometric transfer matrix (GTM) approach followed by voxel-wise correction such that it can be used for both subsequent voxel-based and VOI-based analysis. As it allows correction within as well as between the tissue classes GM, WM and CSF and between the ROIs, and incorporates the PET system’s spread function [32, 33], this method was used in the current study.
As glucose metabolism may impact energetics to maintain myelin integrity, but changes in functional connectivity may also alter regional metabolism (e.g. through disruption of neurotransmitter activity), it is of direct importance to investigate whether (regional) metabolic changes are directly related to WM tract integrity connecting cortical/subcortical regions. So far, the direct relationship between GM atrophy, atrophy-corrected cerebral glucose metabolism and microstructural WM changes in ageing has been investigated only in a limited amount of studies [34,35,36,37]. These were either based on a limited number of subjects, did not sample FDG PET and MR data simultaneously, focused on a priori defined fibre tracts and did not use a full data-driven approach or limited to WM tractography seeded from the region of maximal change in glucose metabolism during ageing.
Therefore, the primary aim of this work was to investigate whether the significant clusters of voxel-based cerebral glucose metabolism changes, accurately corrected for GM loss, are related to microstructural WM changes in ageing, using a simultaneous PET/MR approach. We hypothesized that brain regions demonstrating a significant age-related decline in regional FDG uptake are interconnected by WM tracts with the strongest changes in the WM microstructure. As a secondary aim, we investigated whether a quadratic model is more appropriate over a linear regression to describe age-related effects for each of the observed multimodal measures.
Materials and methods
Subjects
One hundred carefully screened healthy volunteers were recruited between December 2015 and February 2017 with the aim to balance gender and distribute ages evenly over 6 decades (19–29; 30–39; 40–49; 50–59; 60–69; 70–82). The main study exclusion criteria included major internal pathology or having (had) cancer, having a first-degree relative with dementia, a history of important neurological and/or psychiatric disorders, substance abuse or current use of centrally acting medication. Subjects with clinically relevant MRI abnormalities and a WMH load which was considered excessive for the subject’s age were also excluded. More specifically, in subjects < 60 years of age, no abnormalities were allowed, while in subjects ≥ 60 years of age WMH on T2-weighted images, corresponding to a WM lesion score of ≤ 2 (of 3) on the Fazekas scale were acceptable [38]. All subjects had a normal neurological examination. The Mini-Mental State Examination (MMSE) score was used to screen for gross cognitive deficits, and a cutoff value of ≥ 28 was used. All subjects had a score of ≤ 9 on the Beck’s Depression Inventory (BDI). Two subjects were excluded due to significant MRI abnormalities, and datasets of four subjects could be not included for the current analysis because of incomplete data, due to technical errors during data acquisition, excessive motion or problematic data processing. This resulted in the final inclusion of 94 subjects with complete and high-quality imaging data sets. The study was approved by the local university hospital ethics committee, and all participants gave written informed consent before entering the study.
PET data acquisition and reconstruction
All subjects fasted at least 4 h prior to FDG injection. Subjects received an intravenous bolus injection of FDG (150.9 ± 9.9 MBq) and underwent simultaneous FDG PET/MR scanning on a hybrid scanner (Signa PET/MR, GE Healthcare, Milwaukee, WI, USA) with integrated time-of-flight (TOF) PET acquisition and 3 T MR.
FDG PET images were acquired dynamically in list mode upon tracer injection in the scanner for 60 min. In the first 15 min of the scan, no MR sequences were acquired in order to avoid primary auditory cortex activation and subjects were asked to keep their eyes open. For this work, static acquisition data between 40 and 60 min post-injection was used and rebinned in 4 frames of 5 min to allow for verification of intra-scan motion and its correction. FDG data was corrected for deadtime, randoms, scatter and additionally for a recently discovered time-of-flight offset correction [39]. Data were corrected for attenuation was done using a vendor-proprietary, atlas-based method in software MP version 24. FDG PET images were reconstructed using an ordered subset expectation maximization (OSEM) with 4 iterations and 28 subsets and smoothed with a 4.5-mm FWHM (Full Width Half Maximum) isotropic Gaussian filter.
MR acquisition
Simultaneous to PET acquisition, the following MR sequences were acquired, using a vendor-supplied 8-channel phased array head coil: 3D volumetric T1-weighted BRAVO sequence (repetition time (TR)/echo time (TE) = 8.5/3.2 ms, 1 × 1 × 1 mm voxel size), fluid-attenuated inversion recovery (FLAIR) sequence (3D CUBE, TR/TE = 8500/130 ms, 1 × 1 × 1.4 mm voxel size), diffusion tensor imaging (DTI) and reversed DTI (TR/TE = 12,000/85 ms; b-value: 1500 s/mm2; 48 directions).
Voxel-based morphometry
Brain atrophy effects due to ageing were assessed using voxel-based morphometry (VBM). VBM was performed using the computational anatomy toolbox (CAT, version 12), implemented in SPM12 (Statistical Parametric Mapping, Wellcome Department of Imaging Neuroscience, London, UK). All 3D T1-weighted MRI scans were spatially normalized using the DARTEL algorithm, segmented into GM, WM and cerebrospinal fluid (CSF), and modulated to compensate for the effects of spatial normalization. Finally, the GM segmentation was smoothed with an 8-mm FWHM isotropic Gaussian kernel.
The whole-brain analysis of age-related absolute GM density differences was performed using a general linear model with age and also with age^2 as covariates and total intra-cranial volume (TIV) as a nuisance covariate with an explicit GM mask created out of the normalized GM probability maps, without applying any scaling. A significance threshold of Pheight = 0.05 (FWE corrected) for cluster height and threshold for cluster extent of kE > 0.8 cm3 (237 voxels, voxel size 1.5 × 1.5 × 1.5 mm3) were used. The reduction of GM density per decade (RPD; %) was calculated for the linear estimate as
with α = intercept and β = slope of the regression line.
FDG PET analysis
PET data were first corrected for motion effects using a rigid frame-by-frame coregistration, and a single static FDG image was obtained as the average of all motion-corrected frames using PMOD software (v3.9, PMOD Inc, Zurich, Switzerland). Subsequently, PET images were coregistered to the corresponding T1-weighteid MR image in SPM12. A region-based voxel-wise type (RBV) partial volume correction (PVC) was performed on the FDG images using FreeSurfer (Laboratory for Computational Neuroimaging v6.0, Boston, USA) [32] with the Desikan-Killany cortical atlas [40]. RBV PVC is a modified version of the Yang method, where regional mean uptake values are initially obtained using the geometric transfer matrix, and then the Yang correction is applied [41]. The geometric transfer matrix corrects for partial volume effects between different brain regions, followed by voxel-wise correction such that it can be used for a voxel-based analysis. This RBV approach has proven to be more accurate than the Müller-Gartner methods because the technique can correct for PVEs within as well as between tissue classes [32, 33]. For the PVC, the PET resolution was modelled as a Gaussian kernel with a FWHM of 4.5 mm, based on the scanner and reconstruction parameters.
All images were then spatially normalized to the Montreal Neurological Institute (MNI) space using the FDG PET template in SPM12 and smoothed with an 8-mm FWHM Gaussian isotropic kernel. Age-related changes in brain FDG PET images (with and without RBV PVC) were computed with a general linear model with age and age^2 as covariates, with an explicit GM mask created out of the normalized GM probability maps. All images were normalized to cerebellar grey matter as for brain FDG PET this is the preferred method in particular when comparing this to findings in neurodegenerative disorders such as AD [42]. A cerebellar grey matter VOI was delineated on the average T1-weighted image using PMODv3.9 (PMOD Technologies, Zurich, Switzerland) and applied to the spatially normalized individual FDG PET images. In order to test the robustness of the findings of regional intensity scaling to the cerebellum, a whole-brain intensity normalization approach was also followed.
The significance threshold for cluster height was set to Pheight = 0.05 (FWE corrected). We selected an arbitrary threshold of kE > 0.8 cm3 (100 voxels of size 2 × 2 × 2 mm3) as trade-off between sensitivity for very small clusters and specificity. Reduction per decade (RPD; %) was calculated similar as described above for VBM.
DTI analysis
DTI data were corrected for geometric distortion with the FMRIB Software Library (FSL) top-up tool (https://fsl.fmrib/ox/ac.uk; University of Oxford, Oxford, UK) using DTI reversed phase data. Images were then processed to remove Gibbs-ringing and corrected for motion and eddy current artefacts. Finally, all images were spatially normalized with tensor reorientation to the MNI-JHU DTI-based WM atlas in ExploreDTI (v4.8.6, http://www.exploredti.com) [43]. Fractional anisotropy (FA) and mean diffusivity (MD) maps were generated after fitting with the diffusion tensor model. Subsequently, the FA and MD maps were smoothed with an 8-mm FWHM Gaussian isotropic kernel and explored in SPM12 using a general linear model, with an explicit WM mask created out of the normalized WM probability maps (also thresholded at 0.3) and without applying any intensity scaling. Age and age^2 were used as covariates with thresholds for cluster height and extend set to Pheight = 0.05 (FWE corrected) and kE > 0.8 cm3 (100 voxels of voxel size 2 × 2 × 2 mm3), respectively.
In addition to the voxel-based analysis, the JHU-ICB tractography atlas consisting of 50 tracts was used to determine age-related changes in FA and MD within the entire tracts. We excluded cerebellar and brainstem tracts due to incomplete sampling within the FOV for some subjects.
To investigate the interaction between regional FDG PET decline and change in DTI measures changes with ageing, the FWE corrected clusters of the PVC FDG PET regression analysis with age were dilated to protrude into the WM and used as seed regions of interest (ROIs) on the DTI atlas. Then, a deterministic DTI-based Fiber Assignment by Continuous Tracking (FACT) tractography was performed between these seed ROIs to determine the involved WM tracts. FA and MD were evaluated as diffusion parameters within the identified WM tracts.
General statistics
The general level of significance was set at p < 0.05. Standard statistical analyses were performed using Prism (v5, GraphPad, San Diego, USA) or SPSS (v16, IBM, Corporation, Chicago, IL). Differences in distribution of gender, MMSE score, BDI score and handedness over the different age groups were assessed using the appropriate tests (Kruskal–Wallis test for continuous MMSE and BDI scores, and Mann–Whitney U for discrete gender and handedness scores). Regression models were fitted using unweighted linear and second-order polynomial (quadratic) nonlinear fits. The Bayesian information criterion (BIC) was used to select the best model, where the model with the lowest BIC is preferred [44]. The BIC was calculated using the “lmfit” Python package version 1.0.1 (Python Software Foundation, [45]). The strength of evidence against a higher order (in this case quadratic versus linear) model was calculated. When ΔBIC, the difference in BIC score, = BIC (linear) − BIC (quadratic) is positive, a quadratic model is preferred. The strength of evidence was categorized based on the absolute ΔBIC value as: from 0 to 2: low evidence, 2 to 6: moderate positive evidence, 6 to 10: strong evidence and higher than 10: very strong evidence [44].
Results
Subjects and demographic parameters
In total, 94 subjects were included: 47 males and 47 females, between 19.9 and 82.5 years (mean ± SD: 50.1 ± 17.1 years). Table 1 shows the demographic parameters and distribution over age in decades, including MMSE and BDI scores. Gender (p = 0.33), MMSE scores (p = 0.06), BDI scores (p = 0.07) and handedness (p = 0.37) were not significantly different between the six age groups, hence were not included as additional covariates.
Ageing effects on grey matter density
The VBM analysis showed significantly decreased GM density with ageing in bilaterally distributed regions including the dorsolateral prefrontal and lateral frontal cortex, the anterior temporal cortex, middle and superior temporal cortex, insular cortex, fusiform gyri, amygdala and parahippocampal gyrus, as well as the cerebellar cortex, with changes of − 4.7 to − 5.3% per decade (Table 2, Fig. 1A, Fig. 2). Also in the central grey matter nuclei, a cluster with the largest decrease with age was seen covering thalamus and striatum, with a change of − 6.4% per decade (Table 2). The same clusters and peak locations were found when using age^2 as a covariate in the general linear model. For the most significant clusters (Fig. 2), BIC values were higher for the quadratic model (ΔBIC = − 2 to − 4.5), indicating moderate preference towards a linear ageing model.

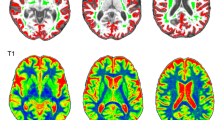
Voxel-wise linear correlation between age and grey matter density (A), fractional anisotropy (B) and glucose metabolism (C, PVC, scaled to cerebellum). Statistical parametric mapping displayed at pheight < 0.05 (FWE corrected) and cluster extent > 0.8 cm3. Images are shown in radiological orientation. The vertical lines on the coronal and sagittal image show position of the sagittal and coronal slices, respectively

Main negative correlations of grey matter density and age in the right thalamus and left middle temporal gyrus at the cluster peak location. Linear (solid line) and quadratic (dotted line) regressions of grey matter density with age are shown, with Bayesian information criterion (BIC) difference for evaluating the best fit (linear vs quadratic)
Ageing effects on relative cerebral glucose metabolism
The voxel-wise regression analysis of RBV-PVC corrected FDG data with age showed a highly significant inverse correlation between age and FDG uptake in a symmetrical cluster of decreased FDG uptake covering the orbitofrontal and midfrontal cortex, extending to the anterior and midcingulate cortex. Other clusters of reduced cerebral glucose metabolism with age were observed in a fairly symmetric fashion in the inferior frontal cortex, insular cortex, perisylvian frontal and temporal cortex (most outspoken on the right), posterior cingulate and high parietal cortex, as well as in central grey nuclei including caudate and medial thalamus (Fig. 1C and cluster peak locations and t-values in Table 3). The same clusters and peak locations were found when using age^2 as a covariate in the general linear model.
Intensity scaling of the PVC corrected FDG data to the whole-brain grey matter resulted in the same clusters for the correlation with age (Supplemental Fig. 1, Supplemental Table 1), albeit with lower cluster size but similar T-values, indicating robustness of the age-correlation findings but as expected a lower sensitivity for the whole-brain normalization. In particular, the perisylvian cluster bilaterally were less extensive in the whole-brain normalization approach.
Also here, similar results were found when using age^2 as a covariate in the general linear model. Figure 3 shows the dataplots of regional FDG uptake with age in the six significant clusters, with both linear and quadratic fits. Linear correlation coefficients in the significant clusters ranged from r = − 0.70 (p < 0.0001) in the putamen (− 5.3% per decade) to r = -0.58 (p < 0.0001) in the cluster located in midcingulum/precuneus (− 3.0% per decade) (Fig. 3). Linear regression analysis resulted in slightly lower R2 compared to quadratic regression analysis. ΔBIC values varied between − 3.6 and + 1.1 for most clusters, indicating no clear preference for a quadratic model. Only in the R caudate, however, a very strong preference towards the quadratic model was found (Fig. 3f), with a steeper decrease above 60 years of age.

Relative FDG uptake versus age for cluster peak location within the 6 main significant cluster showing age-related metabolic decline. Linear (solid line) and quadratic (dotted line) regressions of FDG uptake are shown, with a Bayesian information criterion (BIC) difference for evaluating the best fit (linear vs quadratic)
The inverse contrast indicating relative increases/preservation of glucose metabolism with ageing showed significant, symmetrical clusters in the cerebellum and putamen.
Ageing effects on WM tract microstructure
The voxel-based regression between FA and age showed a highly significant, homogeneous decrease over the entire brain WM (Fig. 1B). Similar results were found when using age^2 as a covariate in the general linear model. Similar results for the increase in MD were found (data not shown). When extracting all 50 tract regions from the JHU atlas, an extensive and significant age-related reduction in FA and increase in MD were found for 47 and 45 tracts, respectively. In this case, ΔBIC values were strongly positive (7.3 to 20.1 in most regions), indicating a strong preference for the quadratic model for both FA and MD values in the fornix, superior longitudinal fasciculus and right cingulum (MD only), with thus a steeper change with advanced age (Fig. 4). The age-related decrease in FA was most pronounced in the fornix (quadratic r = − 0.75) (Fig. 4A), left (r = − 0.73) and right (r = − 0.72) stria terminalis, left (r = − 0.73) (Fig. 4C) and right (r = − 0.70) superior longitudinal fasciculus, forceps minor (r = − 0.72) and the genu of the corpus callosum (r = − 0.69) (Fig. 4E). For MD, age-related increases were most pronounced in the right r = 0.75 (Fig. 4B) and left (r = 0.75) inferior fronto-occipital fasciculus, left (r = 0.75) (Fig. 4D) and right (r = 0.73) inferior longitudinal fasciculus, left (r = 0.73) and right (r = 0.72) superior longitudinal fasciculus and right cingulum (r = 0.73) (Fig. 4E).

Microstructural changes in WM tracts with age. Linear (solid line) and quadratic (dotted line) negative (FA) and positive (MD) correlations with age, with a Bayesian information criterion (BIC) difference for evaluating the best fit (linear vs quadratic)
Population-based tractography of metabolic declining regions
The FACT-based tractography with the significant partial volume corrected FDG clusters (pFWE < 0.05) as seed regions was investigated to get a data-driven analysis of these WM changes, based on the findings of most significant FDG clusters. This approach yielded streamlines (bundle parts) belonging to four distinct tracts WM tracts connecting those regions showing significant age-related decreases in cerebral glucose metabolism. Table 4 provides an overview of the identified tracts (genu of the corpus callosum, cingulum, right parieto-occipito-pontine tract and the left fasciculus arcuatus), together with their respective FDG ROI seeds. The identified parieto-occipito-pontine tract consists of the superior thalamic radiation and runs to the cerebellum through the pons. All four identified tracts are shown together in Fig. 5. Three out of the four identified WM tracts, including the genu of the corpus callosum (FA: top 13%, MD: top 46%), cingulum (FA: top 37%, MD: top 11%) and left fasciculus arcuatus (= superior longitudinal fasciculus) (FA: top 4%, MD: top 9%) were also amongst the tracts exhibiting the most pronounced ageing effects in the whole-brain FA/MD correlation analysis (Fig. 6 and Fig. 1B).

Tractography showing tracts originating from regions with significant age-related FDG decline. Red = anterior corpus callosum, green = cingulum, cingulate part, purple = fasciculus arcuatus (superior longitudinal fasciculus) (left) and blue = parieto-occipito-pontine tract). A anterior, I inferior, P posterior, S superior

Frequency histogram of the correlations between age and FA (A), and between age and MD (B). Three identified tracts are indicated with the arrows on the histograms. Left fasciculus arcuatus (full arrow), genu of the corpus callosum (dashed arrow with circles) and cingulum (dashed arrow with lines)
Figure 7 shows the effects of ageing within the four identified WM tracts. In all identified WM tracts, both FA and MD changed significantly with increasing age, except in the parieto-occipito-pontine tract. While FA decreased, MD showed a significant increase in older age in all connecting tracts. For the ageing effects on FA within these identified WM tracts, no preference for a quadratic was found. In contrast, for MD strong evidence for a quadric model was present with ΔBIC values of > 13 (Fig. 7). For FA, quadratic regression coefficients ranged from r = − 0.73 (p < 0.0001) in the genu of the corpus callosum to r = − 0.29 (p = 0.0206) for the parieto-occipito-pontine tract, and for MD, regression coefficients ranged from r = 0.72 (p < 0.0001) in the genu of the corpus callosum to r = 0.49 (p = 0.0004) in the parieto-occipito-pontine tract.

Microstructural changes within the four identified WM tracts connecting hypometabolic FDG regions with age. Linear (solid line) and quadratic (dotted line) negative (FA) and positive (MD) correlations with age within the four identified WM tracts, with Bayesian information criterion (BIC) difference for evaluating the best fit (linear vs quadratic)
Correlation between age-related changes in cerebral glucose metabolism and WM tract microstructure
Finally, to investigate the presence and strength of interrelated effects in glucose metabolism decrease and the intensity of WM microstructural changes, a correlation analysis was performed between FDG uptake in each seed and the FA and MD values within the identified tract that connects both FDG seeds. Regional FDG uptake for both the seeds correlated positively with FA (0.32 ≤ r ≤ 0.71) and negatively with MD (− 0.75 ≤ r ≤ − 0.40) for all these WM tracts, except in the parieto-occipito-pontine tract. When adding ageing as covariate and calculating partial correlation coefficients, the correlations weakened for both FA and MA, indicating that concomitant but possibly unrelated effects of age may play a role on WM microstructure and on glucose metabolism. Table 5 summarizes these (full and partial) correlation analysis results.
Discussion
In light of the ageing population and increasing prevalence of neurodegenerative diseases, an improved multiparametric and multimodal understanding of normal ageing effects on brain imaging markers can play an important role [46]. In this study, we aimed to investigate the relationship between atrophy, atrophy-corrected cerebral glucose metabolism and WM microstructure in ageing using simultaneous PET/MR. Overall, our results showed that atrophy-corrected cerebral glucose metabolism and WM FA both decline with ageing and that this rate of decline is correlated. To our knowledge, this is the first study performing DTI-FACT and identifying WM tracts between metabolically vulnerable regions. The vast majority of the tracts connecting the most metabolically vulnerable regions upon ageing were also identified as amongst the strongest correlating with age in the whole-brain tractography analysis.
As for changes in the grey matter, cerebral atrophy is a well-studied core feature associated with ageing [1, 2, 5, 6, 47,48,49] and is characterized by a regionally dependent loss of total intra-cranial volume, GM density, cortical thinning, decreases in WM volume and integrity, as well as volumetric increases of the cerebral ventricles [50]. Pathological studies have confirmed that during ageing GM loss and cortical thinning occur, but the direct loss of cortical neurons is limited. Observed macroscopic changes are more likely attributable to neuronal and dendritic architecture with reduction in neurites and nerve fibres, rather than neuronal number [51]. Whether this is also reflected in synaptic loss is unclear. Postmortem literature [52, 53] and recent in vivo PET findings using the SV2A tracer 11C-UCB-J indicate that regional synaptic density is preserved or at most minimal throughout the brain with ageing [54].
The overall vulnerability of the brain for age-related macrostructural changes varies regionally. Moreover, whereas frontal brain volumes decline linearly, other regions appear to show quadratic decline progressing over 50–60 years with steeper decline at high age [1]. Also for grey matter concentration or density, ageing is associated with regional decreases, although different analysis strategies have resulted in mixed findings on the particular involved brain regions. The prefrontal cortex and perirolandic areas are amongst the most consistently affected cortical regions in most studies [2, 55, 56]. Although the sample size in the current study is lower than some of the larger sMRI studies on ageing with up to several thousands of subjects [1, 3, 4], we also observed an age-related reduction in GM in the inferior frontal lobe, insular cortex, inferior, middle and superior temporal pole, but also in the postcentral and fusiform areas, as well as in the central grey matter nuclei regions and cerebellum. The involvement of subcortical regions and primary sensorimotor is still a matter of debate and may be dependent on the methodology used [3, 55,56,57]. Also, in some MR studies the total brain volume is normalized to the TIV [58], whereas in our study TIV was considered as a nuisance variable in the VBM analysis. Nevertheless, the percentage decline per decade in brain volume observed in our study (ranging from 4.7 to 6.4%) is in line with the results of a meta-analysis of 56 longitudinal MR studies [59].
As for glucose metabolism, and in line with previous FDG PET literature, extensive age-related decreased relative metabolism was found in mainly the frontal, cingulate cortex and temporal cortex, but also in subcortical GM nuclei [25, 60, 61]. In the current work, almost all regions that showed a decrease in regional metabolism survived PVC except for the right perisilvian cluster. Overall, we found remaining changes from − 3.0 to − 5.3% per decade for lateral frontal and subcortical grey matter, respectively. In our study, a strict threshold of pFWE < 0.05 was used, which may result in differences in the extent of the observed significant clusters. While some smaller and older studies have observed non-significant changes after PVC, concluding that atrophy alone could be sufficient to explain regionally decreased FDG uptake [37, 62, 63], most recent studies have shown that atrophy alone is not sufficient to explain the reduction with age [23, 26, 29, 64]. The used method of PVC is of high importance. Greve et al. discussed the advantages of the GTM-based RBV PVC method when performing voxel-wise analysis [29]. RBV PVC correction was demonstrated to be superior to the Müller-Gärtner method because it can correct for PVEs within as well as between tissue classes and between the ROIs while performing a voxel-based correction [32, 33].
As for the decline in WM integrity with ageing, our results from the FA and MD correlation analysis are in line with several large studies showing a consistent and widespread decline of microstructural integrity parameters in the vast majority of WM tracts with increasing age, which occurs fairly homogeneously over the brain in a direct regression analysis [8, 9, 11, 34, 65]. The underlying mechanism in myelination processes that lead to the observed alterations in WM anisotropy with age is still poorly understood [65]. Lower global FA at older age seems predominantly driven by a lower neurite density rather than greater tract complexity or outward dispersion of the WM tracts (fanning) [8, 11]. Higher MD at older age denotes a higher rate of diffusion, consistent with poorer local WM integrity [11].
As for the interrelation between glucose metabolism and WM integrity, we then assessed population-based tractography with tracts originating from those clusters showing a significant age-related decline in FDG as seed ROIs. From this analysis, we identified four interconnecting WM tracts. Two of these tracts are association fibre bundles: the left fasciculus arcuatus (a part of the superior longitudinal fasciculus) and the cingulum. The left fasciculus arcuatus connects frontotemporal and frontoparietal regions [66] and connects important language regions, including Broca’s and Wernicke’s area involved in producing and understanding language [66]. Although the overall language function remains relatively preserved in healthy ageing [67], age-related structural changes in the left fasciculus arcuatus have been reported [68]. The longest WM tracts, such as association fibres, maturate later and are thinly myelinated, in particular the frontal and temporal association fibres [8], making the myelination process most vulnerable. The so-called “last-in-first-out” or developmental hypothesis indicates that most vulnerable regions to age effects are the last ones to emerge. However, as shown by the partial correlation with age as covariate, significance of the fasciculus arcuatus was not significant anymore. Therefore, concomitant but different non-related effect of ageing on both fasciculus arcuatus integrity and frontotemporoparietal function may play a role that needs further investigation.
Also, the cingulum, connecting the frontal, parietal and medial temporal cortex [69], is centrally involved in cognitive control and executive functioning [69]. In addition, also the genu of the corpus callosum was involved, which is a commissural fibre connecting the left and right hemispheres [37]. Ageing is associated with a decline in working memory, motor function and problem solving skills, functions that are associated with FA in both the genu of the corpus callosum and the cingulate fibre bundle [70]. Finally, also parieto-occipito-pontine tract was identified, encompassing the superior thalamic radiation which is a projection fibre bundle connecting lateral thalamic nuclei to the cerebral cortex, that relays sensory and motor data to the pre- and postcentral cortex [71] and connects to the cerebellum which is metabolically preserved with ageing. When comparing the tractography-based analysis with the whole-brain regression analysis of WM integrity, three out of the four identified tracts (corpus callosum (genu), cingulum and fasciculus arcuatus) for the tractography analysis were also amongst the tracts with the highest correlation values with ageing in the whole-brain analysis, indicating they encompass bundles with high vulnerability.
Overall, our WM integrity results are in line with previous studies focussing on particular tracts. Chételat et al. investigated the relationship between decreased glucose metabolism in the left inferior frontal cortex, which showed the largest decrease in FDG uptake with ageing and its microstructural connectivity [34]. They found that decreasing metabolism with ageing here (uncorrected for partial volume effects) correlated with decreased FA in the uncinate fasciculus, inferior longitudinal fasciculus, cingulum, arcuate fasciculus and genu of the corpus callosum [34]. Inoue et al. correlated FA specifically in the genu and splenium of the corpus callosum with glucose metabolism in the whole brain and found that the vulnerability of the anterior corpus callosum fibres was associated with glucose metabolism decline in the PFC [35].
Although our results and previous literature point to significant ageing effects on both glucose metabolism and regionally associated structural WM connectivity, the temporal order and mechanism of this association remain unclear. Glucose metabolism may impact WM myelin integrity as reflected by FA measurements, as maintaining myelin is energy demanding. On the other hand, local metabolic dysfunction may be due to disruption in functional connectivity with distant brain regions by degeneration of myelin, leading to changes in neurotransmission activity and hence cerebral glucose metabolism [34, 72]. As ageing effects seem to be more global for all WM tracts, while the impact on glucose metabolism is spatially more restricted, this may indicate that degeneration of myelin WM fibres could precede changes in glucose metabolism, or that specific higher order function brain regions, such as the frontal cortical regions, are more vulnerable due to an independent mechanism.
The pattern observed with ageing (linear vs quadratic) can also indicate changes in vulnerability. For most brain regions ageing effects on GM density and metabolism could be explained by a linear fit, except for the caudate nucleus. As this small region is prone to partial volume effects and spatial normalization is less accurate for small central subcortical regions [73], this may be a false-positive finding. For FA, we also found a predominantly linear decrease with age except for the fornix and superior longitudinal fasciculus [13]. For MD, an acceleration of ageing effects in particular from 50 to 60 years on was observed with better fits (high BIC values) in nearly all tracts (Fig. 4). This also is in line with previous observations [8, 10, 47], implicating that MD changes are thus more sensitive to ageing. MD however is more susceptible to CSF contamination than FA; therefore, also here partial volume effects may drive nonlinear effects in periventricular regions [8, 10].
There are a number of limitations to this study that should be taken into account. First, subjects were screened to assess good health. We did not perform an extensive neuropsychological test battery on various cognitive subdomains such as memory, executive functioning and processing speed but only performed an MMSE that represents a basic evaluation of global cognitive status. A detailed evaluation of the above subdomains might have also led to a more detailed correlation with both metabolic and WM integrity values, enhancing the functional interpretation and specificity of the observed changes. Subclinical impairments and/or predementia stages cannot be fully excluded in this cohort [74]. Therefore, throughout the manuscript, we have refrained from using the term “healthy ageing”. Also, education, apoE status and physical activity levels were not available as potential nuisance variables, also having potential effects on WM integrity [75] and age-related decline in glucose metabolism or cognitive reserve [20, 23].
Second, this study had a cross-sectional design with subjects in different age groups who have various life trajectories regarding education/socio-economic possibilities/nutritional contexts etc. Assessment of changes in metabolism, atrophy and WM integrity within-subject across the individual’s life span, would likely enable a more sensitive assessment with lifestyle modifiers as potential extra factors that may interfere with ageing effects. Therefore, to fully address the temporal order and possible causality between regional FDG changes and WM integrity, a longitudinal FDG PET/MR study should be conducted with a within-subject follow-up, instead of the current and previous cross-sectional multimodal studies [17].
Third, we have not considered gender effects or interactions. Group analysis of the current VBM, PVC FDG and WM FA/MD maps did not show a significant group difference between men and women at the same FEW-corrected statistical thresholds. Moreover, in several previous studies significant but small gender differences throughout the span of normal ageing have been found, in particular in the prefrontal and parietal cortex [18, 19, 27]. As this is inconsistent over studies and likely a second-order effect, it was not further investigated in more regional detail in the current work. Fourth, the exact pathophysiological mechanism underlying microstructural ageing effects in WM remains to be better elucidated. FA and MD are the most commonly used DTI scalars, but DTI with a single b-value is known to be less accurate in regions where fibres cross, leading to an underestimation of fibre counts and directions, thereby affecting these DTI scalars [76]. To obtain more detailed information on axonal density, membrane integrity, diameter and intra-voxel coherence of fibre orientations, advanced diffusion MR techniques can nowadays be applied such as multishell data with high angular resolution diffusion imaging (HARDI) models and probabilistic tractography [76, 77], but these were not yet available at the time of acquisition for the Signa 3 T MR. Fifth, on the methodological level we performed attenuation correction using an atlas-based AC, implemented by the manufacturer on the GE Signa. This method can lead to slight regional bias of tracer uptake of a few percent, especially in the cranio-caudal direction, compared to CT, ZTE or 511-keV transmission based AC due to differences in bone classification [78]. However, since the same craniocaudal bias was present in all datasets, the overall effect on the regression with ageing is likely minimal. Finally, due to the limitations in the number of images that could be acquired in the diffusion sequence, the cerebellum was not fully captured in the field of view of the diffusion scan; thus, ageing modulation of WM tracts connecting the cerebellum with supratentorial regions might have been underestimated. For FDG PET studies of normal ageing, there is a debate regarding the most appropriate reference region as shown in a recent review by Nugent et al. [42]. Mostly, cerebellum, pons, brainstem, sensorimotor cortex or the whole brain have been used. In addition to the requirement of limited metabolic and volumetric variability during ageing, an optimal reference region should not be susceptible to external physiological stimuli, such as visual, tactile or auditory, and should be reliably segmented. As was shown from our PVE corrected FDG analysis, intensity normalization of the FDG data was quite robust for normalization approach (whole brain versus cerebellum), but cerebellar normalization is more sensitive as the whole-brain normalization includes the relatively large portion of the cortical and subcortical regions that change with age also in its normalization denominator.
Conclusion
In a large dataset of 94 healthy subjects, we demonstrated that cerebral glucose metabolism, corrected for atrophy using a state-of-the-art voxel-based method, and WM microstructural integrity both decrease during normal brain ageing. Furthermore, the amount of regional cerebral glucose metabolic decline is related to the intensity of the microstructural changes in the connecting WM tracts, indicating parallel and interconnected changes with ageing. Synchronicity or the sequentiality of these findings needs to be further addressed ideally by means of longitudinal designs which would now be easier to perform using simultaneous PET/MR.
Abbreviations
- GM:
-
Grey matter
- WM:
-
White matter
- FDG:
-
Fluorodeoxyglucose
- PET/MR:
-
Positron emission tomography/magnetic resonance
- DTI:
-
Diffusion tensor imaging
- MRI:
-
Magnetic resonance imaging
- FA:
-
Fractional anisotropy
- PVC:
-
Partial volume correction
- MD:
-
Mean diffusivity
- SPM:
-
Statistical parametric mapping
- WMH:
-
White matter hyperintensities
- SPECT:
-
Single photon emission computed tomography
- CBF:
-
Cerebral blood flow
- ASL:
-
Arterial spin labelling
- CSF:
-
Cerebrospinal fluid
- GTM:
-
Geometric transfer matrix
- VOI:
-
Volume-of-interest
- ROI:
-
Region of interest
- MMSE:
-
Mini-mental state examination
- BDI:
-
Beck’s depression inventory
- TOF:
-
Time of flight
- OSEM:
-
Ordered subset expectation maximization
- FWHM:
-
Full width half maximum
- TR:
-
Repetition time
- TE:
-
Echo time
- FLAIR:
-
Fluid-attenuated inversion recovery
- VBM:
-
Voxel-based morphometry
- TIV:
-
Total intra-cranial volume
- FWE:
-
Family wise error
- kE :
-
Cluster extent
- RPD:
-
Reduction per decade
- RBV:
-
Region-based voxel-wise
- FSL:
-
FMRIB software library
- BIC:
-
Bayesian information criterion
References
DeCarli C, Massaro J, Harvey D, Hald J, Tullberg M, Au R, et al. Measures of brain morphology and infarction in the Framingham heart study: establishing what is normal. Neurobiol Aging. 2005;26:491–510.
Walhovd KB, Westlye LT, Amlien I, Espeseth T, Reinvang I, Raz N, et al. Consistent neuroanatomical age-related volume differences across multiple samples. Neurobiol Aging. 2011;32:916–32.
Good CD, Johnsrude IS, Ashburner J, Henson RNA, Friston KJ, Frackowiak RSJ. A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage. 2001;14:21–36.
Crivello F, Tzourio-Mazoyer N, Tzourio C, Mazoyer B. Longitudinal assessment of global and regional rate of grey matter atrophy in 1,172 healthy older adults: modulation by sex and age. PLoS One. 2014;9:e114478.
Walhovd KB, Fjell AM, Reinvang I, Lundervold A, Dale AM, Eilertsen DE, et al. Effects of age on volumes of cortex, white matter and subcortical structures. Neurobiol Aging. 2005;26:1261–70.
Kennedy KM, Erickson KI, Rodrigue KM, Voss MW, Colcombe SJ, Kramer AF, et al. Age-related differences in regional brain volumes: a comparison of optimized voxel-based morphometry to manual volumetry. Neurobiol Aging. 2009;30:1657–76.
Liu H, Yang Y, Xia Y, Zhu W, Leak RK, Wei Z, et al. Aging of cerebral white matter. Ageing Res Rev. 2017;34:64–76.
Cox SR, Ritchie SJ, Tucker-Drob EM, Liewald DC, Hagenaars SP, Davies G, et al. Ageing and brain white matter structure in 3,513 UK Biobank participants. Nat Commun. 2016;7:1–13.
de Groot M, Ikram MA, Akoudad S, Krestin GP, Hofman A, van der Lugt A, et al. Tract-specific white matter degeneration in aging: the Rotterdam Study. Alzheimer’s Dement. 2015;11:321–30.
Hsu JL, Van Hecke W, Bai CH, Lee CH, Tsai YF, Chiu HC, et al. Microstructural white matter changes in normal aging: a diffusion tensor imaging study with higher-order polynomial regression models. Neuroimage. 2010;49:32–43.
Salami A, Eriksson J, Nilsson LG, Nyberg L. Age-related white matter microstructural differences partly mediate age-related decline in processing speed but not cognition. Biochim Biophys Acta - Mol Basis Dis. 2012;1822:408–15.
de Groot M, Cremers LGM, Ikram MA, Hofman A, Krestin GP, van der Lugt A, et al. White matter degeneration with aging: longitudinal diffusion MR imaging analysis. Radiology. 2016;279:532–41.
Sexton CE, Walhovd KB, Storsve AB, Tamnes CK, Westlye LT, Johansen-Berg H, et al. Accelerated changes in white matter microstructure during aging: a longitudinal diffusion tensor imaging study. J Neurosci. 2014;34:15425–36.
Lu H, Xu F, Rodrigue KM, Kennedy KM, Cheng Y, Flicker B, et al. Alterations in cerebral metabolic rate and blood supply across the adult lifespan. Cereb Cortex. 2011;21:1426–34.
Zhang N, Gordon ML, Ma Y, Chi B, Gomar JJ, Peng S, et al. The age-related perfusion pattern measured with arterial spin labeling MRI in healthy subjects. Front Aging Neurosci. 2018;10:214.
Pagani M, Salmaso D, Jonsson C, Hatherly R, Jacobsson H, Larsson SA, et al. Regional cerebral blood flow as assessed by principal component analysis and 99mTc-HMPAO SPET in healthy subjects at rest: normal distribution and effect of age and gender. Eur J Nucl Med. 2002;29:67–75.
Ishibashi K, Onishi A, Fujiwara Y, Oda K, Ishiwata K, Ishii K. Longitudinal effects of aging on 18F-FDG distribution in cognitively normal elderly individuals. Sci Rep. 2018;8:11557.
Kakimoto A, Ito S, Okada H, Nishizawa S, Minoshima S, Ouchi Y. Age-related sex-specific changes in brain metabolism and morphology. J Nucl Med. 2016;57:221–5.
Malpetti M, Ballarini T, Presotto L, Garibotto V, Tettamanti M, Perani D. Gender differences in healthy aging and Alzheimer’s dementia: a 18 F-FDG-PET study of brain and cognitive reserve. Hum Brain Mapp. 2017;38:4212–27.
Yoshizawa H, Gazes Y, Stern Y, Miyata Y, Uchiyama S. Characterizing the normative profile of 18F-FDG PET brain imaging: sex difference, aging effect, and cognitive reserve. Psychiatry Res - Neuroimaging. 2014;221:78–85.
Ishibashi K, Miura Y, Toyohara J, Ishii K, Ishiwata K. Comparison of imaging using 11 C-ITMM and 18 F-FDG for the detection of cerebellar ataxia. J Neurol Sci. 2017;375:97–102.
Fujimoto T, Matsumoto T, Fujita S, Takeuchi K, Nakamura K, Mitsuyama Y, et al. Changes in glucose metabolism due to aging and gender-related differences in the healthy human brain. Psychiatry Res - Neuroimaging. 2008;164:58–72.
Knopman DS, Jack CR, Wiste HJ, Lundt ES, Weigand SD, Vemuri P, et al. 18F-fluorodeoxyglucose positron emission tomography, aging, and apolipoprotein E genotype in cognitively normal persons. Neurobiol Aging. 2014;35:2096–106.
Greve DN, Svarer C, Fisher PM, Feng L, Hansen AE, Baare W, et al. Cortical surface-based analysis reduces bias and variance in kinetic modeling of brain PET data. Neuroimage. 2014;92:225–36.
Petit-Taboué MC, Landeau B, Desson JF, Desgranges B, Baron JC. Effects of healthy aging on the regional cerebral metabolic rate of glucose assessed with statistical parametric mapping. Neuroimage. 1998;7:176–84.
Bonte S, Vandemaele P, Verleden S, Audenaert K, Deblaere K, Goethals I, et al. Healthy brain ageing assessed with 18F-FDG PET and age-dependent recovery factors after partial volume effect correction. Eur J Nucl Med Mol Imaging. 2017;44:838–49.
Van Laere K, Versijpt J, Audenaert K, Koole M, Goethals I, Achten E, et al. 99mTc-ECD brain perfusion SPET: variability, asymmetry and effects of age and gender in healthy adults. Eur J Nucl Med. 2001;28:873–87.
Mozley PD, Sadek AM, Alavi A, Gur RC, Muenz LR, Bunow BJ, et al. Effects of aging on the cerebral distribution of technetium-99m hexamethylpropylene amine oxime in healthy humans. Eur J Nucl Med. 1997;24:754–61.
Greve DN, Salat DH, Bowen SL, Izquierdo-Garcia D, Schultz AP, Catana C, et al. Different partial volume correction methods lead to different conclusions: an 18F-FDG-PET study of aging. Neuroimage. 2016;132:334–43.
Thomas BA, Cuplov V, Bousse A, Mendes A, Thielemans K, Hutton BF, et al. PETPVC: a toolbox for performing partial volume correction techniques in positron emission tomography. Phys Med Biol. 2016;61:7975–93.
Oyama S, Hosoi A, Ibaraki M, McGinnity CJ, Matsubara K, Watanuki S, et al. Error propagation analysis of seven partial volume correction algorithms for [18F]THK-5351 brain PET imaging. EJNMMI Phys. 2020;7:57.
Thomas BA, Erlandsson K, Modat M, Thurfjell L, Vandenberghe R, Ourselin S, et al. The importance of appropriate partial volume correction for PET quantification in Alzheimer’s disease. Eur J Nucl Med Mol Imaging. 2011;38:1104–19.
Erlandsson K, Buvat I, Pretorius PH, Thomas BA, Hutton BF. A review of partial volume correction techniques for emission tomography and their applications in neurology, cardiology and oncology. Phys Med Biol. 2012;57:R119–59.
Chételat G, Landeau B, Salmon E, Yakushev I, Bahri MA, Mézenge F, et al. Relationships between brain metabolism decrease in normal aging and changes in structural and functional connectivity. Neuroimage. 2013;76:167–77.
Inoue K, Ito H, Uchida S, Taki Y, Kinomura S, Tsuji I, et al. Decrease in glucose metabolism in frontal cortex associated with deterioration of microstructure of corpus callosum measured by diffusion tensor imaging in healthy elderly. Hum Brain Mapp. 2008;29:375–84.
Kuczynski B, Targan E, Madison C, Weiner M, Zhang Y, Reed B, et al. White matter integrity and cortical metabolic associations in aging and dementia. Alzheimer’s Dement. 2010;6:54–62.
Kochunov P, Ramage AE, Lancaster JL, Robin DA, Narayana S, Coyle T, et al. Loss of cerebral white matter structural integrity tracks the gray matter metabolic decline in normal aging. Neuroimage. 2009;45:17–28.
De Leeuw FE, De Groot JC, Achten E, Oudkerk M, Ramos LMP, Heijboer R, et al. Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Rotterdam Scan Study. J Neurol Neurosurg Psychiatry. 2001;70:9–14.
Rezaei A, Schramm G, Van Laere K, Nuyts J. Estimation of crystal timing properties and efficiencies for the improvement of (joint) maximum-likelihood reconstructions in TOF-PET. IEEE Trans Med Imaging. 2020;39:952–63.
Desikan RS, Ségonne F, Fischl B, Quinn BT, Dickerson BC, Blacker D, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31:968–80.
Yang J, Huang SC, Mega M, Lin KP. Investigation of partial volume correction methods for brain FDG pet studies. IEEE Trans Nucl Sci. 1996;43:3322–7.
Nugent S, Croteau E, Potvin O, Castellano CA, Dieumegarde L, Cunnane SC, et al. Selection of the optimal intensity normalization region for FDG-PET studies of normal aging and Alzheimer’s disease. Sci Rep Nat Res. 2020;10:1–8.
Leemans A, Jeurissen B, Sijbers J, Jones D. ExploreDTI: a graphical toolbox for processing, analyzing, and visualizing diffusion MR data. Proc 17th Sci Meet Int Soc Magn Reson Med. 2009;3537.
Kass RE, Raftery AE. Bayes factors. J Am Stat Assoc. 1995;90:773–95.
van Rossum G. Python tutorial. Technical Report CS-R9526. Amsterdam; 1995.
Hou Y, Dan X, Babbar M, Wei Y, Hasselbalch SG, Croteau DL, et al. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol. 2019; 15: 565–81.
Allen JS, Bruss J, Brown CK, Damasio H. Normal neuroanatomical variation due to age: the major lobes and a parcellation of the temporal region. Neurobiol Aging. 2005;26:1245–60.
Bagarinao E, Watanabe H, Maesawa S, Mori D, Hara K, Kawabata K, et al. An unbiased data-driven age-related structural brain parcellation for the identification of intrinsic brain volume changes over the adult lifespan. Neuroimage. 2018;169:134–44.
McDonald CR, McEvoy LK, Gharapetian L, Fennema-Notestine C, Hagler DJ, Holland D, et al. Regional rates of neocortical atrophy from normal aging to early Alzheimer disease. Neurology. 2009;73:457–65.
Choy SW, Bagarinao E, Watanabe H, Ho ETW, Maesawa S, Mori D, et al. Changes in white matter fiber density and morphology across the adult lifespan: a cross‐sectional fixel‐based analysis. Hum Brain Mapp. 2020;41:3198–211.
Freeman SH, Kandel R, Cruz L, Rozkalne A, Newell K, Frosch MP, et al. Preservation of neuronal number despite age-related cortical brain atrophy in elderly subjects without alzheimer disease. J Neuropathol Exp Neurol. 2008;67:1205–12.
Scheff SW, Price DA, Sparks DL. Quantitative assessment of possible age-related change in synaptic numbers in the human frontal cortex. Neurobiol Aging. 2001;22:355–65.
Itoh Y, Yamada M, Suematsu N, Matsushita M, Otomo E. An immunohistochemical study of centenarian brains: a comparison. J Neurol Sci. 1998;157:73–81.
Michiels L, Delva A, van Aalst J, Ceccarini J, Vandenberghe W, Vandenbulcke M, et al. Synaptic density in healthy human aging is not influenced by age or sex: a 11C-UCB-J PET study. Neuroimage. 2021;232:117877.
Fjell AM, Westlye LT, Espeseth T, Reinvang I, Walhovd KB, Dale AM. Cortical gray matter atrophy in healthy aging cannot be explained by undetected incipient cognitive disorders: a comment on Burgmans et al. (2009). Neuropsychology. 2010;24:258–66.
Bakkour A, Morris JC, Wolk DA, Dickerson BC. The effects of aging and Alzheimer’s disease on cerebral cortical anatomy: specificity and differential relationships with cognition. Neuroimage. 2013;76:332–44.
Smith CD, Chebrolu H, Wekstein DR, Schmitt FA, Markesbery WR. Age and gender effects on human brain anatomy: a voxel-based morphometric study in healthy elderly. Neurobiol Aging. 2007;28:1075–87.
Oschwald J, Guye S, Liem F, Rast P, Willis S, Röcke C, et al. Brain structure and cognitive ability in healthy aging: a review on longitudinal correlated change. Rev Neurosci. 2019;31:1–57.
Hedman AM, van Haren NEM, Schnack HG, Kahn RS, Hulshoff Pol HE. Human brain changes across the life span: a review of 56 longitudinal magnetic resonance imaging studies. Hum Brain Mapp. 2012;33:1987–2002.
Herholz K, Salmon E, Perani D, Baron JC, Holthoff V, Frölich L, et al. Discrimination between Alzheimer dementia and controls by automated analysis of multicenter FDG PET. Neuroimage. 2002;17:302–16.
Pardo JV, Lee JT, Sheikh SA, Surerus-Johnson C, Shah H, Munch KR, et al. Where the brain grows old: decline in anterior cingulate and medial prefrontal function with normal aging. Neuroimage. 2007;35:1231–7.
Ibáñez V, Pietrini P, Furey ML, Alexander GE, Millet P, Bokde ALW, et al. Resting state brain glucose metabolism is not reduced in normotensive healthy men during aging, after correction for brain atrophy. Brain Res Bull. 2004;63:147–54.
Curiati PK, Tamashiro-Duran JH, Duran FLS, Buchpiguel CA, Squarzoni P, Romano DC, et al. Age-related metabolic profiles in cognitively healthy elders: results from a voxel-based [18F]fluorodeoxyglucose-positron-emission tomography study with partial volume effects correction. Am J Neuroradiol. 2011;32:560–5.
Nugent S, Tremblay S, Chen KW, Ayutyanont N, Roontiva A, Castellano CA, et al. Brain glucose and acetoacetate metabolism: a comparison of young and older adults. Neurobiol Aging. 2014;35:1386–95.
Rathee R, Rallabandi VPS, Roy PK. Age-related differences in white matter integrity in healthy human brain: evidence from structural MRI and diffusion tensor imaging. Magn Reson Insights. 2016;9:9–20.
Catani M, Mesulam M. The arcuate fasciculus and the disconnection theme in language and aphasia: history and current state. Cortex. 2008;44:953–61.
Teubner-Rhodes S, Vaden KI, Cute SL, Yeatman JD, Dougherty RF, Eckert MA. Aging-resilient associations between the arcuate fasciculus and vocabulary knowledge: microstructure or morphology? J Neurosci. 2016;36:7210–22.
Ikuta T, Gollnick HM, Rutledge AN. Age associated decline in the arcuate fasciculus and IQ. Brain Imaging Behav. 2020;14:362–7.
Bubb EJ, Metzler-Baddeley C, Aggleton JP. The cingulum bundle: anatomy, function, and dysfunction. Neurosci Biobehav Rev. 2018;92:104–27.
Zahr NM, Rohlfing T, Pfefferbaum A, Sullivan EV. Problem solving, working memory, and motor correlates of association and commissural fiber bundles in normal aging: a quantitative fiber tracking study. Neuroimage. 2009;44:1050–62.
Yuan R, Di X, Taylor PA, Gohel S, Tsai YH, Biswal BB. Functional topography of the thalamocortical system in human. Brain Struct Funct. 2016;221:1971–84.
Bartzokis G. Age-related myelin breakdown: a developmental model of cognitive decline and Alzheimer’s disease. Neurobiol Aging. 2004;25:5–18.
Suetens K, Nuttin B, Gabriëls L, Van Laere K. Differences in metabolic network modulation between capsulotomy and deep-brain stimulation for refractory obsessive-compulsive disorder. J Nucl Med. 2014;55:951–9.
Burgmans S, Van Boxtel MPJ, Vuurman EFPM, Smeets F, Gronenschild EHBM, Uylings HBM, et al. The prevalence of cortical gray matter atrophy may be overestimated in the healthy aging brain. Neuropsychology 2009;23:541–50.
Tseng BY, Gundapuneedi T, Khan MA, Diaz-Arrastia R, Levine BD, Lu H, et al. White matter integrity in physically fit older adults. Neuroimage. 2013;82:510–6.
Tournier J-D, Mori S, Leemans A, Morgan RH, Reson M, Author M. Diffusion tensor imaging and beyond NIH public access author manuscript. Magn Reson Med. 2011;65:1532–56.
Raffelt DA, Smith RE, Ridgway GR, Tournier JD, Vaughan DN, Rose S, et al. Connectivity-based fixel enhancement: whole-brain statistical analysis of diffusion MRI measures in the presence of crossing fibres. Neuroimage. 2015;117:40–55.
Schramm G, Koole M, Willekens SMA, Rezaei A, Van Weehaeghe D, Delso G, et al. Regional accuracy of ZTE-based attenuation correction in static 18F-FDG and dynamic 18F-PE2I brain PET/MR. Front Phys. 2019. https://doi.org/10.3389/fphy.2019.00211.
Acknowledgements
The authors acknowledge the contributions by Stefanie Willekens, PhD, on data acquisition, Kim Serdons, Pharm PhD and the radiopharmacy team for tracer production, Kwinten Porters, Jef Van Loock, Guido Putzeys, Kris Byloos and Stefan Ghysels for data acquisition, and Ronald Peeters, Nathalie Mertens from the PET/MR physics team.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed were in accordance with the ethical institutional standards and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Competing interests
All authors report no relevant financial interests or other potential conflicts of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Neurology.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
van Aalst, J., Devrome, M., Van Weehaeghe, D. et al. Regional glucose metabolic decreases with ageing are associated with microstructural white matter changes: a simultaneous PET/MR study. Eur J Nucl Med Mol Imaging 49, 664–680 (2022). https://doi.org/10.1007/s00259-021-05518-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-021-05518-6