
Summary
Abstract
Lenograstim is the glycosylated recombinant form of human granulocyte colony stimulating factor. The drug is used to reduce the risk of life-threatening infection in patients with neutropenia, particularly after cytotoxic chemotherapy.
Lenograstim accelerates neutrophil recovery significantly after chemotherapy, with beneficial effects on clinical end-points such as incidence of laboratory-confirmed infection and length of hospital stay. Chemotherapy dose intensity has also been increased in patients receiving lenograstim, notably those with breast or small cell lung cancer, although improvements in tumour response and survival have not been demonstrated.
Lenograstim also assists neutrophil recovery in patients undergoing bone marrow transplantation, and stimulates the production of peripheral blood stem cells (PBSCs) for autologous transfusion after aggressive chemotherapy. Lenograstim also mobilises CD34+ cells more efficiently in unit dose terms than filgrastim and has been used successfully to mobilise PBSCs from healthy donors for allogeneic transplantation.
Randomised trials have shown increases in rates of disease remission after lenograstim therapy in patients with acute myeloid leukaemia, with no evidence of stimulation of malignant blasts. The drug has also shown potential in the mobilisation of nonmalignant PBSCs for autotransplantation in patients with chronic myeloid leukaemia. Other studies show efficacy of lenograstim in patients with acute lymphoblastic leukaemia, aplastic anaemia, in children with severe chronic neutropenia and in the reversal of neutropenia related to antiviral therapy in patients with AIDS, although data are not extensive.
Cost analyses of lenograstim have been carried out from a hospital perspective, although results have been inconclusive. Cost-effectiveness or cost-benefit data are lacking at present.
Lenograstim is well tolerated, with bone pain and injection site reactions being reported most frequently in clinical trials.
Conclusions: Lenograstim has been confirmed as a valuable adjunct to minimise the haematological toxicity of myelosuppressive chemotherapy in patients with malignant disease. The drug also enhances neutrophil recovery in patients undergoing stem cell rescue, and assists PBSC mobilisation. Data indicate clinical benefit with lenograstim in myeloid disorders, with no evidence of malignant blast cell proliferation. Further studies are required to assess more fully the pharmacoeconomic implications of the use of lenograstim and other recombinant growth factors, to provide more data on the efficacy of the drug in the management of disease-related neutropenia, and to clarify fully its position relative to filgrastim.
Pharmacological Properties
Lenograstim is the glycosylated recombinant form of human granulocyte colony stimulating factor (rHuG-CSF). The drug supports the differentiation of neutrophil-committed colony-forming cells and increases absolute neutrophil counts (ANC) in a dose-dependent manner.
Postulated functional effects of lenograstim on neutrophils include increased phagocytic activity, activation, recruitment and adhesion. These effects appear to be mediated by changes in a variety of neutrophil surface proteins. Current data suggest that rHuG-CSFs do not stimulate the proliferation of leukaemic blasts in vivo, although the safety of these agents in patients with myeloid conditions remains to be fully confirmed.
Lenograstim exhibits dose-dependent pharmacokinetic characteristics, with peak serum levels being proportional to the injected dose. There is no evidence of accumulation after repeated administration. Absolute bioavailability after subcutaneous doses of 2 to 5 μg/kg is approximately 30%, and the apparent volume of distribution is approximately 1 L/kg. Serum elimination half-lives after subcutaneous or intravenous injection are approximately 3 or 1 to 1.5 hours, respectively. Routes of metabolism and excretion have not been fully ascertained, but a very small proportion only of each dose is excreted unchanged in urine.
Therapeutic Use
Standard Dose Chemotherapy. A phase II randomised placebo-controlled study in 64 patients showed significant reductions (p < 0.05) in the median duration of neutropenia after chemotherapy with 14-day courses of subcutaneous lenograstim 0.5, 2, 5 or 10 μg/kg/day, and the authors recommended the 5 μg/kg/day dosage for future use.
Results from 2 randomised placebo-controlled phase III trials showed significant reductions in median duration of neutropenia (<1.0 × 109/L) after 8- to 10-day courses of lenograstim 5 μg/kg/day subcutaneously between chemotherapy cycles in patients with inflammatory breast cancer or non-Hodgkin’s lymphoma (NHL). Effects persisted throughout all 4 treatment cycles in both studies, and there were significant reductions in incidence of laboratory-confirmed infection, duration of hospital stay for treatment of infection and use of antibiotics. Increases in dose intensity made possible by treatment with lenograstim did not translate into improvements in tumour response or 3-year survival, however.
Similar efficacy in terms of rate of hospitalisation for febrile leucopenia has been shown for subcutaneous lenograstim 263 μg/day compared with oral ciprofloxacin 500 mg/day plus amphotericin B 2 g/day in a nonblind randomised comparison in 40 patients with breast cancer. The incidence of leucopenia (<1.0 × 109/L) after chemotherapy was significantly lower, but that of febrile leucopenia significantly higher, with lenograstim.
Chemotherapy Dose Intensification. The use of subcutaneous lenograstim 5 μg/kg/day on day 2 to day 14 of treatment cycles based on fluorouracil, epirubicin and cyclophosphamide in patients with breast cancer resulted in a reduction in cycle time from 3 to 2 weeks. Encouraging tumour response rates have been reported in anthracycline-resistant or heavily pretreated patients receiving lenograstim with docetaxel or paclitaxel. Preliminary reports from phase III studies in patients with breast cancer also show increases in relative dose intensity in patients receiving lenograstim, although subsequent effects on tumour response and survival are not clear.
Reductions in cycle length have also been achieved with the addition of lenograstim in patients with small cell lung cancer (SCLC) undergoing cisplatinor anthracycline-based chemotherapy. Phase III data from 280 patients with SCLC have shown the addition of lenograstim 150 μg/m2/day subcutaneously to each of 6 cycles of doxorubicin, cyclophosphamide and etoposide to be associated with a significantly decreased requirement for chemotherapy dose reduction (≥1 reduction in 17.3 vs 27.7% of patients receiving chemotherapy alone; p = 0.037), although there was no significant increase in median survival time in patients who received lenograstim. Intensification of chemotherapy regimens has also been achieved with lenograstim in patients with soft tissue sarcoma, NHL or ovarian cancer, although clinical benefit in terms of improved tumour response and survival requires further investigation.
High Dose Chemotherapy with Stem Cell Rescue. After significantly accelerated neutrophil recovery was observed in patients undergoing bone marrow transplantation (BMT) who received lenograstim in a phase II trial, a phase III randomised, double-blind and placebo-controlled study has shown 30 and 41% reductions, respectively, in median times to achieve ANC ≥0.5 and 1.0 × 109/L (both p < 0.001 vs placebo) with lenograstim 5 μg/kg/day intravenously after BMT. In this study of 298 evaluable patients with lymphoma, myeloma, acute lymphoblastic leukaemia or other malignancies, there were also significant reductions relative to placebo in median durations of hospitalisation, antibiotic use, total parenteral nutrition (TPN; intravenous hyperalimentation), infection and febrile neutropenia, although there were no significant effects of lenograstim on the actuarial risk of disease relapse or the 1-year survival rate.
As well as assisting neutrophil recovery after BMT, lenograstim has been used to stimulate the production of peripheral blood stem cells for autologous transfusion after aggressive chemotherapy. Two studies in 141 previously treated patients with lymphoma showed median times to achieve ANC ≥0.5 × 109/L of 11 to 12 days after chemotherapy followed by lenograstim-assisted autologous PBSC transplantation (PBSCs collected after mobilisation with lenograstim 263 μg/day subcutaneously after cyclophosphamide 1.5 g/m2 on day 1). Approximately half the patients enrolled received filgrastim 10 μg/kg/day in 1 study; although results were presented collectively, stem cell mobilisation effects were stated to be similar between agents.
Similar median neutrophil recovery times (13 to 15 days to ANC >0.5 × 109/L) were shown with PBSC transplantation after subcutaneous lenograstim 5, 7.5 or 10 μg/kg/day with cyclophosphamide for mobilisation in 29 children with solid tumours treated with high dose melphalan in a double-blind dose-finding study.
Data from a randomised nonblind comparison in 61 patients receiving stem cell support from matched sibling donors indicate similar efficacy of lenograstim and filgrastim (median dosages 4 and 10.3 μg/kg/day, respectively) when either drug was given after stem cell transplantation.
The feasibility of using lenograstim to mobilise PBSCs from healthy donors for allogeneic transplantation has been demonstrated in Japanese and European trials, and reflects a trend towards allogeneic PBSC transplantation since the early 1990s. In dose-response terms, lenograstim mobilises CD34+ cells (the number of which affects the probability of successful engraftment) more efficiently than filgrastim in healthy volunteers. In a pilot study, 54 patients with leukaemia or myelodysplasia received PBSCs obtained from sibling donors who had received a priming regimen of lenograstim 10 μg/kg/day subcutaneously for 5 days. After initial myeloablation with high intensity chemo- and/or radiotherapy, 51 patients achieved an ANC of 0.5 × 109/L within 15 days. The rate of survival was 50% after a median 25-month follow-up.
Myeloid Leukaemias. Although the use of rHuG-CSF in patients with myeloid conditions is controversial because of fears of stimulation of leukaemic blast cells, clinical studies of lenograstim have been carried out in this setting.
Randomised placebo-controlled trials carried out in Japan have shown accelerated neutrophil recovery and evidence of infection-related clinical benefit with lenograstim 5 μg/kg/day intravenously for 14 days after consolidation chemotherapy in patients with acute myeloid leukaemia (AML). In addition, European placebo-controlled trials have shown significant improvements in neutrophil recovery times, together with increased rates of complete remission of disease, with lenograstim after induction chemotherapy in patients with AML. Increases over placebo in complete haematological remission in 2 of these studies were 49 and 38% with lenograstim, although the reason for this effect has not been determined: high rates of complete remission of AML have also been reported after treatment with idarubicin-based protocols with and without addition of lenograstim. Integrated European data show reductions against placebo in incidence and duration of infection in lenograstim recipients aged 55 years and over.
Data are also available to indicate a potential role for lenograstim in the mobilisation of PBSCs for autotransplantation as an alternative to autologous BMT in patients with AML.
Studies conducted recently show that lenograstim might be used for the mobilisation of Philadelphia chromosome (Ph)-negative (i.e. nonmalignant) PBSCs for autotransplantation in patients with chronic myeloid leukaemia (CML) who are not eligible for conventional allogeneic BMT. Administration of lenograstim 150 μg/m2/day subcutaneously or intravenously as part of a cytarabine-based mobilisation protocol resulted in complete cytogenetic remission in the leucapheretic product in 21% of 29 patients in 1 study; the same dosage of lenograstim was associated with a Ph-positive cell content of less than 35% in 91% of 47 evaluable leucaphereses from 20 patients in a second trial.
Increases from baseline in leucocyte counts have been achieved after 7 to 14 days’ lenograstim therapy (5 μg/kg/day or 263 μg/day) in 2 small studies in patients with myelodysplasia, with no evidence of progression to AML.
Acute Lymphoblastic Leukaemia. Augmentation of neutrophil recovery, but no effect on patterns of infection or antibiotic use, was shown with intravenous or subcutaneous lenograstim in 2 randomised studies in patients with acute lymphoblastic leukaemia (ALL) or acute undifferentiated leukaemia (AUL).
Increased chemotherapy dose intensities with decreased duration of fever, hospitalisation and intravenous antibiotic treatment were achieved in children with ALL receiving lenograstim 5 μg/kg/day, but there was no improvement in 3-year disease-free survival.
Aplastic Anaemia. Addition of lenograstim 5 μg/kg/day subcutaneously to immunosuppressive therapy with antilymphocyte globulin, methylprednisolone and cyclosporin in 40 patients with severe aplastic anaemia (SAA) resulted in trilineage-complete responses and transfusion independence in 82% of participants, with actuarial survival of 92% after median follow-up of 428 days. Phase III data have shown addition of subcutaneous lenograstim 5 μg/kg/day in 53 of 102 patients undergoing immunosuppressive therapy with cyclosporin and antithymocyte globulin to increase the proportion of patients with complete ANC response (≥1.5 × 109/L) significantly after 112 days (83 vs 44.9% without lenograstim; p = 0.001). There was no apparent effect of lenograstim on long term haematopoietic recovery or survival after a median follow-up of 23 months.
Other Neutropenic Conditions. Rates of infection and hospitalisation were reduced significantly relative to figures obtained before lenograstim treatment in a phase II study in 19 children with severe chronic neutropenia who received subcutaneous therapy with lenograstim. An induction dosage of 5 μg/kg/day was sufficient to obtain a neutrophil response in 15 patients. Clinical improvement has also been noted in children with glycogen storage disease Ib who received subcutaneous lenograstim at a median initial dosage of 5 μg/kg/day.
Encouraging results have been obtained with lenograstim therapy in a small number of patients with Felty’s syndrome, and subcutaneous treatment has been used successfully to manage immunosuppressant-induced leucopenia after renal transplantation. In addition, preliminary data from a randomised single-blind phase II study have indicated lenograstim 50 μg/m2/day subcutaneously to be suitable for the management of ganciclovir-induced neutropenia in patients with AIDS.
Pharmacoeconomic Considerations
Pharmacoeconomic studies of lenograstim have to date focused on cost issues from a hospital perspective. Attempts have not been made to assign values to health outcomes such as improvements in quality of life or years of life gained.
Pharmacoeconomic evaluations of lenograstim in 3 phase III studies showed lenograstim therapy to be associated with reductions in hospitalisation and total direct costs in patients with breast cancer or NHL, and reduced cost of antibiotic therapy in patients with breast cancer, NHL or SCLC. Intensification of chemotherapy in patients who received lenograstim to assist neutrophil recovery resulted in an increase in chemotherapy drug costs. Increasing interest in allogeneic PBSC transplantation in preference to BMT has led to a case control study (n = 17) in which the direct medical costs associated with transplantation of lenograstim-mobilised PBSCs were shown to be substantially (29%; p = 0.006) lower than those in a historical control group of 17 patients undergoing allogeneic BMT.
Results are available from a well designed and robust cost analysis in which children with NHL were randomised to receive 2 courses of intensive induction chemotherapy with (n = 75) or without (n = 72) lenograstim 5 μg/kg/day subcutaneously for 6 to 15 days. The total cost from a hospital perspective of lenograstim-assisted induction therapy was $US29 765 per patient; without lenograstim, the cost was $US30 774 (1996 values). Overall, the acquisition cost of lenograstim was balanced by 2 additional days in hospital in patients who did not receive the drug.
A saving of approximately $US1800 (1997 values) per course of chemotherapy from a hospital perspective was indicated when lenograstim 150 μg/m2/day rather than filgrastim 10 μg/kg/day was used after autologous BMT in a series of 36 patients (55 chemotherapy courses) with solid tumours undergoing intensive chemotherapy. This saving was attributed to a difference in acquisition cost between the 2 growth factors.
Tolerability
Data from clinical studies indicate overall adverse reaction rates with lenograstim therapy to be similar with those seen with placebo. Bone pain and injection site reactions were the most commonly reported events in patients receiving lenograstim for chemotherapy-induced neutropenia, and were more frequent than with placebo. A database of pooled adverse reaction reports from 1495 patients shows incidences of adverse events attributed to lenograstim as follows: fever 1.2%; lumbar pain 1.1%; increased blast cell counts in patients with AML 0.9%; hepatic disturbances 0.5%; bone pain 0.4%; eruptions/rashes 0.4%.
No association has been found between clonal cytogenetic abnormalities and dysplasia of bone marrow in patients receiving lenograstim, but all rHuG-CSFs have been linked to isolated episodes of interstitial pneumonia and respiratory distress syndrome. There are no tolerability data relevant to the use of lenograstim in pregnant or nursing women, the elderly, infants or patients with hepatic or renal dysfunction.
Dosage and Administration
There are variations between Western countries and Japan in the recommended dosages and licensed indications for lenograstim. International dosage and administration guidelines for Western patients recommend a dosage of 150 μg/m2/day (equivalent to 5 μg/kg/day as used in clinical trials) to reduce the duration of chemotherapy-induced neutropenia and to assist PBSC mobilisation. Subcutaneous administration is recommended, except after BMT where a 30-minute intravenous infusion should be used to assist recovery from neutropenia.
Lenograstim should not be given at the same time as cytotoxic chemotherapy, and the drug is not recommended in patients with severe hepatic or renal insufficiency, or in nursing mothers. There are no dosage recommendations for the elderly, infants or pregnant women.













Similar content being viewed by others

References
MacConnachie AM. Colony stimulating factors: G-CSFs — filgrastim (Neupogen) and lenograstim (Granocyte). Intensive Crit Care Nurs 1998 Feb; 14: 49–50
Hollingshead LM, Goa KL. Recombinant granulocyte colony-stimulating factor (rG-CSF): a review of its pharmacological properties and prospective role in neutropenic conditions. Drugs 1991 Aug; 42: 300–30
Souza LM, Boone TC, Gabrilove JL, et al. Recombinant human granulocyte colony-stimulating factor: effects on normal and leukemic myeloid cells. Science 1986; 232: 61–5
Kubota N, Orita T, Hattori K, et al. Structural characterization of natural and recombinant human granulocyte colony-stimulating factors. J Biochem 1990; 107: 486–92
Frampton JE, Yarker YE, Goa KL. Lenograstim: a review of its pharmacological properties and therapeutic efficacy in neutropenia and related clinical settings. Drugs 1995 May; 49: 767–93
Oh-eda M, Hasegawa M, Hattori K, et al. O-linked sugar chain of human granulocyte colony-stimulating factor protects it against polymerization and denaturation allowing it to retain its biological activity. J Biol Chem 1990 July; 265(20): 11432–5
Kishita M, Motojima H, Oh-eda M, et al. Stability of granulocyte colony stimulating factor (rHuG-CSF) in serum. The Clinical Report 1992; 26: 221–4
Ono M. Physicochemical and biochemical characteristics of glycosylated recombinant human granulocyte colony stimulating factor (lenograstim). Eur J Cancer A 1994; 30A Suppl. 3: S7–S11
Hasegawa M. A thermodynamic model for denaturation of granulocyte colony-stimulating factor: O-linked sugar chain suppresses not the triggering of deprotonation but the succeeding denaturation. Biochem Biophys Acta 1993; 1203: 295–7
Ema H, Suda T, Nagayoshi K, et al. Target cells for granulocyte colony-stimulating factor, interleukin-3, and interleukin-5 in differentiation of pathways of neutrophils and eosinophils. Blood 1990 Nov; 76(10): 1956–61
Watts MJ, Addison I, Ings SJ, et al. Optimal timing for collection of PBPC after glycosylated G-CSF administration. Bone Marrow Transplant 1998; 21: 365–8
World Health Organization (WHO). International collaborative study for the proposed international standards for granulocyte-macrophage colony-stimulating factor and granulocyte-colony-stimulating factor. BS/92. 1711. World Health Organization Technical Reports Series; 1994
Gervais V, Zerial A, Oschkinat H. NMR investigations of the role of the sugar moiety in glycosylated recombinant human granulocyte-colony-stimulating factor. Eur J Biochem 1997; 247: 386–95
Löwenberg B. Proliferative activity of rG-CSFs in cell line bioassays. Int J Hematol 1996; 64 Suppl. 2: S13–4
Nissen C, Dalle Carbonare V, Moser Y In vitro comparison of the biological potency of glycosylated versus non-glycosylated rG-CSF. Drug Invest 1994; 7(6): 346–52
Azzarà A, Carulli G, Rizzuti-Gullaci N, et al. Effects of lenograstim and filgrastim on neutrophil chemotaxis in patients undergoing chemotherapy [abstract no. SS-1084]. Haematologica 1999; 84
Decleva E, Cramer R, Zabucchi G. Glycosylation improves the priming effect exerted by recombinant human granulocyte colony-stimulating factor (lenograstim) on human neutrophil Superoxide production. Int J Tissue React 1995; 17(5–6): 191–8
Scheinberg DA, Maslak P, Weiss M. Acute leukemias. In: DeVita Jr VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 5th ed. Philadelphia: Lippincott-Raven, 1997: 2293–321
de Arriba F, Lozano ML, Ortũno F, et al. Prospective randomized study comparing the efficacy of bioequivalent doses of glycosylated and nonglycosylated rG-CSF for mobilizing peripheral blood progenitor cells. Br J Haematol 1997 Feb; 96: 418–20
Höglund M, Smedmyr B, Bengtsson M, et al. Mobilization of CD34+ cells by glycosylated and nonglycosylated G-CSF in healthy volunteers — a comparative study. Eur J Haematol 1997 Sep; 59: 177–83
Höglund M, Håkansson L, Venge P. Effects of in vivo administration of G-CSF on neutrophil functions in healthy volunteers. Eur J Haematol 1997 Mar; 58: 195–202
Håkansson L, Höglund M, Jönsson U-B, et al. Effects of in vivo administration of G-CSF on neutrophil and eosinophil adhesion. Br J Haematol 1997 Sep; 98(3): 603–11
Turzanski J, Crouch SPM, Fletcher J, et al. Ex vivo neutrophil function in response to three different doses of glycosylated rHuG-CSF (Lenograstim). Br J Haematol 1997 Jan; 96: 46–54
Roilides E, Walsh TJ, Pizzo PA, et al. Granulocyte colony-stimulating factor enhances the phagocytic and bactericidal activity of normal and defective human neutrophils. J Infect Dis 1991 Mar; 163: 579–83
Spiekermann K, Emmendoerffer A, Eisner J, et al. Altered surface marker expression and function of G-CSF-induced neutrophils from test subjects and patients under chemotherapy. Br J Haematol 1994 May; 87(1): 31–8
de Haas M, Kerst JM, van der Schoot CE, et al. Granulocyte colony-stimulating factor administration to healthy volunteers: analysis of the immediate activating effects on circulating neutrophils. Blood 1994 Dec; 84(11): 3885–94
Kerst JM, de Haas M, van der Schoot CE, et al. Recombinant granulocyte colony-stimulating factor administration to healthy volunteers: induction of immunophenotypically and functionally altered neutrophils via an effect on myeloid progenitor cells. Blood 1993; 82: 3265–72
Yong KL. Granulocyte colony-stimulating factor (G-CSF) increases neutrophil migration across vascular endothelium independent of an effect on adhesion: comparison with granulocyte-macrophage colony-stimulating factor (GM-CSF). Br J Haematol 1996; 94: 40–7
Adachi S, Kubota M, Lin YW, et al. In vivo administration of granulocyte colony-stimulating factor promotes neutrophil survival in vitro. Eur J Haematol 1994 Sep; 53(3): 129–34
Xu SY, Höglund M, Venge P. The effect of granulocyte colony-stimulating factor (G-CSF) on the degranulation of secondary granule proteins from human neutrophils in vivo may be indirect. Br J Haematol 1996 Jun; 93(3): 558–68
Marty M. The optimal dose of glycosylated recombinant human granulocyte colony stimulating factor for use in clinical practice: a review. Eur J Cancer A 1994; 30A Suppl. 3: S20–5
Watts MJ, Addison I, Long SG, et al. Crossover study of the haematological effects and pharmacokinetics of glycosylated and non-glycosylated G-CSF in healthy volunteers. Br J Haematol 1997 Aug; 98(2): 474–9
Houston AC, Stevens LA, Cour V. Pharmacokinetics of glycosylated recombinant human granulocyte colony-stimulating factor (lenograstim) in healthy male volunteers. Br J Clin Pharmacol 1999 Mar; 47: 279–84
Chugai Pharma UK Ltd. Granocyte. ABPI Compendium of Data Sheets and Summaries of Product Characteristics 1998–1999. London: Datapharm Publications Ltd
Bodey GP, Buckley M, Sathe YS, et al. Quantitative relationships between circulating leukocytes and infection in patients with acute leukemia. Ann Intern Med 1966; 64: 328–40
Faulds D, Lewis NJW, Milne RJ. Recombinant granulocyte colony-stimulating factor (rG-CSF). Pharmacoeconomic considerations in chemotherapy-induced neutropenia. Pharmacoeconomics 1992 Apr; 1: 231–49
Goa K, Bryson H. Recombinant granulocyte-macrophage colony-stimulating factor (rGM-CSF). An appraisal of its pharmacoeconomic status in neutropenia associated with chemotherapy and autologous bone marrow transplant. Pharmacoeconomics 1994; 5(1): 56–77
Hughes WT, Armstrong D, Bodey GP, et al. From the Infectious Diseases Society of America. Guidelines for the use of antimicrobial agents in neutropenic patients with unexplained fever. J Infect Dis 1990 Mar; 161(3): 381–96
NCCN practice guidelines for fever and neutropenia. Oncology 1999 May; 13 Suppl.: 197–257
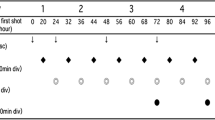
Soda H, Oka M, Fukuda M, et al. Optimal schedule for administering granulocyte colony-stimulating factor in chemotherapy-induced neutropenia in non-small-cell lung cancer. Cancer Chemother Pharmacol 1996 May; 38: 9–12
Seymour A-M, de Campos E, Thatcher N, et al. A single- blind, randomised, vehicle-controlled dose-finding study of recombinant human granulocyte colony-stimulating factor (lenograstim) in patients undergoing chemotherapy for solid cancers and lymphoma. Eur J Cancer 1995 Dec; 31A: 2157–63
Toner GC, Shapiro JD, Laidlaw CR, et al. Low-dose versus standard-dose lenograstim prophylaxis after chemotherapy: a randomized, crossover comparison. J Clin Oncol 1998 Dec; 16: 3874–9
Yamaguchi T, Kurita Y, Saito R, et al. Clinical effect of recombinant human G-CSF on neutropenia induced by chemotherapy in small-cell lung cancer patients [in Japanese]. Biotherapy 1994 Nov; 8: 1423–9
Tominaga T, Ohta K, Yamaguchi S, et al. Clinical effect of recombinant human G-CSF on neutropenia induced by adriamycin-containing chemotherapy in patients with advanced and recurrent breast cancer [in Japanese]. Biotherapy 1993 Nov; 7: 1709–16
Taguchi T, Morioka Y, Orita K, et al. Clinical trial of lenograstim on neutropenia induced by chemotherapy for advanced and recurrent gastric cancer: second report [in Japanese]. Biotherapy 1992 Aug; 6: 1425–32
Tsukimoto I, Hanawa Y, Takaku F, et al. Clinical evaluation of recombinant human G-CSF in children with cancer [in Japanese]. Rinsho Ketsueki 1990; 31(10): 1647–55
Kotake T, Usami M, Miki T, et al. Effect of recombinant human granulocyte colony stimulating factor (lenograstim) on chemotherapy induced neutropenia in patients with urothelial cancer. Int J Urol 1999 Feb; 6: 61–7
Chevallier B, Chollet P, Merrouche Y, et al. Lenograstim prevents morbidity from intensive induction chemotherapy in the treatment of inflammatory breast cancer. J Clin Oncol 1995 Jul; 13: 1564–71
Gisselbrecht C, Haioun C, Lepage E, et al. Placebo-controlled phase III study of lenograstim (glycosylated recombinant human granulocyte colony-stimulating factor) in aggressive non-Hodgkin’s lymphoma: factors influencing chemotherapy administration. Leuk Lymphoma 1997 Apr; 25: 289–300
Kosmidis P, Skarlos D, Kourossis C, et al. Benefit of Granocyte® (lenograstim) in patients treated with Campto® (CPT-11) in 1st or 2nd line metastatic colorectal cancer (MCRC): preliminary results of a phase III multicenter trial [abstract]. Ann Oncol 1998; 9 Suppl. 4: 34
Schröder CP, de Vries EGE, Mulder NH, et al. Prevention of febrile leucopenia after chemotherapy in high-risk breast cancer patients: no significant difference between granulocyte-colony stimulating growth factor or ciprofloxacin plus amphotericin B. J Antimicrob Chemother 1999 May; 43: 741–3
Gurney H, Dodwell D, Thatcher N, et al. Escalating drug delivery in cancer chemotherapy: a review of concepts and practice — Part 2. Ann Oncol 1993 Feb; 4(2): 103–15
Woll PJ, Hodgetts J, Lomax L, et al. Can cytotoxic dose-intensity be increased by using granulocyte colony-stimulating factor? A randomized controlled trial of lenograstim in small-cell lung cancer. J Clin Oncol 1995 Mar; 13: 652–9
Bissett D, Jodrell D, Harnett AN, et al. Phase I study of accelerated FEC with granulocyte colony-stimulating factor (lenograstim) support. Br J Cancer 1995 Jun; 71: 1279–82
Constenla M, Carrete N, Lorenzo I, et al. Phase II trial of docetaxel (TXT) and lenograstim in anthracycline-resistant metastatic breast cancer [abstract]. Ninth International Congress on Anti-Cancer Treatment 1999 Feb 2: Paris, France, 134
Constenla M, Lorenzo I, Garcia-Arroyo FR, et al. Phase II trial of paclitaxel 96-hour infusion with G-CSF in anthracycline-resistant metastatic breast cancer [abstract]. 33rd Proc Am Soc Clin Oncol 1997 May 17; 16: Denver, 165a
Bonadonna G, Pannuti F, Robustelli G, et al. Phase III study comparing standard dose FNC (5-fluorouracil, mitoxantrone, cyclophosphamide) versus dose-intensive FNC + rHuG-CSF (lenograstim) versus time-intensive FNC + lenograstim in advanced breast cancer (ABC) patients: preliminary results of the (CSF-001) study [abstract]. 33rd Proc Am Soc Clin Oncol 1997 May 17; 16: Denver, 149
Garrone O, Venturini M, Del Mastro L, et al. Dose-intensity and dose density in metastatic breast cancer: final results from GONOMIG-3 randomized study [abstract]. Tumori 1998 Sep–Oct; 84 Suppl. 1: 58
Takada M, Fukuoka M, Ariyoshi Y, et al. The use of granulocyte colony-stimulating factor to shorten the interval between cycles of mitomycin C, vindesine, and cisplatin chemotherapy in non-small-cell lung cancer. Cancer Chemother Pharmacol 1992; 31: 182–6
Mori K, Saitoh Y, Tominaga K. Recombinant human granulocyte colony-stimulating factor in patients receiving intensive chemotherapy for non-small cell lung cancer. Eur J Cancer 1993; 29A(5): 677–80
Thatcher N, Bleehen NM, Girling DJ, et al. Feasibility of using glycosylated recombinant human granulocyte colony stimulating factor (G-CSF) to increase the dose intensity of doxorubicin, cyclophosphamide and etoposide (ACE) in small cell lung cancer (SCLC) [abstract]. Thorax 1994 Apr; 49: 428P
Gatzemeier U, Kleisbauer JP, Drings P, et al. Lenograstim as support for chemotherapy of small cell lung cancer: a phase III, multicentre, randomized study. Am J Clin Oncol (In press)
Chevreau C, Bui BN, Chevallier B, et al. Phase I–II trial of intensification of the MAID regimen with support of lenograstim (rHuG-CSF) in patients with advanced soft-tissue sarcoma (STS). Am J Clin Oncol 1999 Jun; 22: 267–72
Bui BN, Chevallier B, Chevreau C, et al. Efficacy of lenograstim on hematologic tolerance to MAID chemotherapy in patients with advanced soft tissue sarcoma and consequences on treatment dose-intensity. J Clin Oncol 1995 Oct; 13: 2629–36
Niitsu N, Umeda M. Biweekly COP-BLAM (cyclophosphamide, vincristine, prednisone, bleomycin, doxorubicin and procarbazine) regimen combined with granulocyte colony-stimulating factor (G-CSF) for intermediate-grade non-Hodgkin’s lymphoma. Eur J Haematol 1996 Mar; 56: 163–7
Pignata S, Lauria R, Perrone F, et al. Phase I study of carboplatin, cisplatin, and cyclophosphamide without and with lenograstim for the treatment of ovarian cancer. Int J Oncol 1997 Jul; 11: 175–80
Smith BR. Stem cell transplantation. In: DeVita Jr VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 5th ed. Philadelphia: Lippincott-Raven, 1997: 2621–39
Gianni AN, Bregni N, Stern AC, et al. Granulocyte-macrophage colony-stimulating factor to harvest circulating haemopoietic stem cells for autotransplantation. Lancet 1990; 3: 580–5
Gianni AM, Bregni M, Siena S, et al. Rapid and complete haemopoietic reconstitution following combined transplantation of autologous blood and bone marrow cells. A changing role for high dose chemo-radiotherapy? Hematol Oncol 1989; 7: 139–48
Sheridan WP, Begley CG, Juttner CA, et al. Effect of peripheral-blood progenitor cells mobilised by filgrastim (G-CSF) on platelet recovery after high-dose chemotherapy. Lancet 1992 Mar 14; 339: 640–4
Jones UM, Jones SA, Watts MJ, et al. Development of a simplified single apheresis approach for peripheral blood progenitor cell transplantation in previously treated patients with lymphoma. J Clin Oncol 1994; 12: 1693–702
Beyer J, Schwella N, Zingsem J, et al. Hematopoietic rescue after high-dose chemotherapy using autologous peripheral-blood progenitor cells or bone marrow: a randomized comparison. J Clin Oncol 1995; 13: 1328–35
Schmitz N, Linch DC, Dreger P, et al. Randomised trial of filgrastim-mobilised peripheral blood progenitor cell transplantation versus autologous bone-marrow transplantation in lymphoma patients. Lancet 1996; 347: 353–7
Asano S, Masaoka T, Takaku F Beneficial effect of recombinant human glycosylated granulocyte colony-stimulating factor in marrow-transplanted patients: results of multicenter phase II–III studies. Transplant Proc 1991 Feb; 23 (1 Pt 2): 1701–3
Takahashi S, Asano S, Masaoka T, et al. Clinical evaluation of recombinant human granulocyte colony-stimulating factor (rhG-CSF) in autologous bone marrow transplantation [in JAPANESE]. Rinsho Ketsueki 1991 Mar; 32: 221–6
Linch DC, Scarffe H, Proctor S, et al. Randomised vehicle-controlled dose-finding study of glycosylated recombinant human granulocyte colony-stimulating factor after bone marrow transplantation. Bone Marrow Transplant 1993 Apr; 11: 307–11
Gisselbrecht C, Prentice HG, Bacigalupo A, et al. Placebo-controlled phase III trial of lenograstim in bone-marrow transplantation. Lancet 1994 Mar 19; 343: 696–700
Campilho F, Campos A, Vaz CP, et al. Filgrastim versus lenograstim after allogeneic stem cell transplantation: a prospective randomised study [abstract]. Bone Marrow Transplant 1999 Mar; 23 Suppl. 1: S81
Kinsey SE, Williams D, Will A, et al. Lenograstim (rHuG-CSF) in the mobilisation of PBSC in children with solid tumours — the result of a double blind dose-ranging study [abstract]. Blood 1998 Nov 15; 92 (Suppl. 1 Pt 2): 301b
Kinsey SE, Williams D, Will A, et al. Results of a randomised double blind dose ranging study of lenograstim (rHuG-CSF) for the mobilisation of PBSC in children with solid tumours [abstract]. Br J Haematol 1998 May; 101 Suppl. 1: 73
Linch DC, Milligan DW, Winfield DA, et al. G-CSF after peripheral blood stem cell transplantation in lymphoma patients significantly accelerated neutrophil recovery and shortened time in hospital: results of a randomized BNLI trial. Br J Haematol 1997 Dec; 99(4): 933–8
Ciernik IF, Schanz U, Gmür J. Delaying treatment with granulocyte colony-stimulating factor after allogeneic bone marrow transplantation for hematological malignancies: a prospective randomized trial. Bone Marrow Transplant 1999 Jul; 24(2): 147–51
Gratwohl A, Passweg J, Baldomero H, et al. Blood and marrow transplantation activity in Europe 1997. European Group for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant 1999 Aug; 24: 231–45
Watts MJ, Sullivan AM, Jamieson E, et al. Progenitor-cell mobilization after low-dose cyclophosphamide and granulocyte colony-stimulating factor: an analysis of progenitor-cell quantity and quality and factors predicting for these parameters in 101 pretreated patients with malignant lymphoma. J Clin Oncol 1997 Feb; 15: 535–46
O’Callaghan A, Smartt P, Smith R, et al. Peripheral blood progenitor cell (PBPC) mobilisation with cyclophosphamide and single vial dose (263MCG) lenograstim (G-CSF) in patients with malignant lymphoma receiving BEAM chemotherapy with PBPC transplantation [abstract]. Bone Marrow Transplant 1997 Mar; 19 Suppl. 1: S108
Matsunaga T, Sakamaki S, Kohgo Y, et al. Recombinant human granulocyte colony-stimulating factor can mobilize sufficient amounts of peripheral blood stem cells in healthy volunteers for allogeneic transplantation. Bone Marrow Transplant 1993 Feb; 11: 103–8
Höglund M, Bengtsson M, Simonsson B, et al. Leukapheresis with peripheral blood progenitor cell (PBPC) harvest in healthy volunteers receiving different doses of lenograstim — evidence of a dose-response effect [abstract]. Blood 1994 Nov; 84(10) Suppl. 1: 348a
Schmetzer B, Basara N, Blau W, et al. Lenograstim (Granocyte®) mobilised allogeneic stem cells in related transplants: a dose escalation study [abstract]. Bone Marrow Transplant 1999 Mar; 23 Suppl. 1: S219
Blaise D, Jourdan E, Michallet M, et al. Mobilisation of healthy donors with lenograstim and transplantation of HLA-genoidentical blood progenitors in 54 patients with hematological malignancies: a pilot study. Bone Marrow Transplant 1998 Dec; 22(12): 1153–8
Deisseroth AB, Kantarjian H, Andreeff M, et al. Chronic Leukemias. In: DeVita Jr VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 5th ed. Philadelphia: Lippincott-Raven, 1997: 2321–43
Reiffers J, Taylor K, Gluckman E, et al. Collection of Ph-negative progenitor cells with granulocyte-colony stimulating factor in patients with chronic myeloid leukaemia who respond to recombinant alpha-interferon. Br J Haematol 1998 Aug; 102(No 3): 639–46
Takeshita A, Ohno R, Hiroshima K, et al. A randomized double-blind controlled study of recombinant human granulocyte colony-stimulating factor in patients with neutropenia induced by consolidation chemotherapy for acute myeloid leukemia [in Japanese]. Rinsho Ketsueki 1995; 36(6): 606–14
Nakajima H, Ikeda Y, Hirashima K, et al. A randomized controlled study of rG CSF in patients with neutropenia after induction therapy for acute myelogenous leukemia [in Japanese]. Rinsho Ketsueki 1995; 36(6): 597–605
Dombret H, Chastang C, Fenaux P, et al. A controlled study of recombinant human granulocyte colony-stimulating factor in elderly patients after treatment for acute myelogenous leukemia. N Engl J Med 1995 Jun 22; 332: 1678–83
Link H, Wandt H, Schönrock-Nabulsi P, et al. G-CSF (lenograstim) after chemotherapy for acute myeloid leukemia: a placebo controlled trial [abstract]. Blood 1996 Nov 15; 88 Suppl. 1: 666a
Granocyte in acute myeloid leukaemia. Rhône-Poulenc Rorer, 1999 (Data on file)
Lowenthal RM, Bradstock KM, Matthews JP, et al. Idarubicin, cytarabine in standard or high-dose, and etoposide ± lenograstim (G-CSF): combinations giving high remission rates in acute myeloid leukaemia (AML) [abstract]. Aust N Z J Med 1996 Apr; 26: 329
Additional therapeutic indication: acceleration of neutrophil recovery in patients undergoing chemotherapy for acute myeloid leukaemia: written summaries on the clinical documentation. Chugai-Rhône-Poulenc, 2000 (Data on file)
Vellenga E, van Putten WLJ, Boogaerts MA, et al. Peripheral blood stem cell transplantation as an alternative to autologous marrow transplantation in the treatment of acute myeloid leukemia? Bone Marrow Transplant 1999; 23: 1279–82
Carella AM, Simonsson B, Link H, et al. Mobilization of Philadelphia-negative peripheral blood progenitor cells with chemotherapy and rhuG-CSF in chronic myelogenous leukaemia patients with a poor response to interferon-alpha. Br J Haematol 1998 Apr; 101: 111–8
McGlave PB, De Fabritiis P, Deisseroth A, et al. Autologous transplants for chronic myelogenous leukaemia: results from eight transplant groups. Lancet 1994; 343: 1486–8
O’Brien SG, Goldman JM. Autografting in chronic myeloid leukaemia. Blood Rev 1994; 8: 63–9
Carella AM, Cunningham I, Lerma E, et al. Mobilization and transplantation of Philadelphia-negative peripheral-blood progenitor cells early in chronic myelogenous leukemia. J Clin Oncol 1997 Apr; 15: 1575–82
Carella AM, Lerma E, Celesti L, et al. Effective mobilization of Philadelphia-chromosome-negative cells in chronic myelogenous leukaemia patients using a less intensive regimen. Br J Haematol 1998 Feb; 100: 445–8
Carella AM, Lerma E, Corsetti MT, et al. Autografting with Philadelphia chromosome-negative mobilized hematopoietic progenitor cells in chronic myelogenous leukemia. Blood 1999; 93: 1534–9
Hughes TP, Grigg A, Szer J, et al. Mobilization of predominantly Ph-negative blood progenitors using cyclophosphamide and lenograstim in early chronic phase CML: correlation with sokal prognostic index and hematological control premobilisation [abstract]. Blood 1996 Nov 15; 88 (Suppl. 1 Pt 1): 235a
Scheinberg DA, Maslak P, Weiss M. Myelodyplastic syndromes. In: DeVita Jr VT, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 5th ed. Philadelphia: Lippincott-Raven, 1997: 2388–96
Yoshida Y, Hirashima K, Asano S, et al. Hematological effect of 14 days treatment of recombinant human granulocyte colony-stimulating factor for neutropenia in myelodysplastic syndromes [in Japanese]. Rinsho Ketsueki 199 Jul; 32: 743–50
Yoshida Y, Hirashima K, Assano S, et al. A phase-II trial of recombinant human granulocyte colony-stimulating factor in the myelodysplastic syndromes. Br J Haematol 1991 Jul; 78: 378–84
Panagopoulos J, Petrogiannopoulos C, Zaharof A, et al. The effect of lenograstim (G-CSF) in patients with infection and myelodysplastic syndrome [abstract]. Br J Haematol 1996 Jun; 93 Suppl. 2: 276
Schriber JR, Negrin RS. Use and toxicity of the colony-stimulating factors. Drug Saf 1993 Jun; 8: 457–68
Izumi T, Muroi K, Takatoku M, et al. Development of acute myeloblastic leukaemia in a case of aplastic anaemia treated with granulocyte colony-stimulating factor. Br J Haematol 1994 Jul; 87: 666–8
Ohno R, Tomonaga M, Ohshima T, et al. A randomized controlled study of granulocyte colony stimulating factor after intensive induction and consolidation therapy in patients with acute lymphoblastic leukemia. Int J Hematol 1993 Aug; 58: 73–81
Smedmyr B. Lenograstim as supportive treatment in newly diagnosed acute lymphoblastic leukaemia [abstract]. In: Current consensus and future uses of granulocyte colony stimulating factors: advantages of a human-identical glycosylated rG-CSF, lenograstim. Proceedings of the 18th International Congress on Chemotherapy; 1993 Jun 30; Stockholm, 18–21
Michel G, Landman J, Leblanc T, et al. The use of lenograstim (G-CSF) to increase the chemotherapy dose-intensity (CDI): a randomized trial in very high risk childhood acute lymphoblastic leukemia (ALL) [abstract]. Blood 1998 Nov 15; 92 (Suppl. 1 Pt 1): 399a
Gale RP, Champlin RE, Feig SA, et al. Aplastic anemia: biology and treatment. Ann Intern Med 1981; 95: 477–94
Camitta BM, Storb R, Thomas ED. Aplastic anemia: pathogenesis, diagnosis, treatment, and prognosis. N Engl J Med 1982; 306: 645–52
Young NS, Barrett AT. The treatment of severe acquired aplastic anemia. Blood 1995; 85: 3367–77
Storb R, Thomas ED, Buckner CD, et al. Marrow transplantation for aplastic anemia. Semin Hematol 1984; 21: 27–35
Rosenfeld SJ, Kimball J, Vining D, et al. Intensive immuno-suppression with antithymocyte globulin and cyclosporine as treatment for severe acquired aplastic anemia. Blood 1995; 11: 3058–65
Bacigalupo A, Broccia G, Corda G, et al. Antilymphocyte globulin, cyclosporin, and granulocyte colony-stimulating factor in patients with acquired severe aplastic anemia (S AA): a pilot study of the EBMT SAA Working Party. Blood 1995 Mar 1; 85: 1348–53
Marsh JCW, Gordon-Smith ED. Treatment of aplastic anaemia with antilymphocyte globulin and cyclosporin. Int J Hematol 1995; 62: 133–44
Asano S, Hirashima K, Yoshida Y, et al. Clinical effect of recombinant human granulocyte colony-stimulating factor on aplastic anemia [in Japanese]. Rinsho Ketsueki 1990; 31(9): 1456–62
Gluckman E, Rokicka-Milewska R, Gordon-Smith EC, et al. Results of a randomized study of gluycosylated rHuG-CSF lenograstim in severe aplastic anemia [abstract]. Blood 1998 Nov 15; 92 (Suppl. 1 Pt 1): 376
Bessho M, Hirashima K, Asano S, et al. Treatment of the anemia of aplastic anemia patients with recombinant human erythropoietin in combination with granulocyte colony-stimulating factor: a multicenter randomized controlled study. Eur J Haematol 1997 Apr; 58: 265–72
Horwitz M, Benson KF, Person RE, et al. Mutations in ELA2, encoding neutrophil elastase, define a 21 -day biological clock in cyclic haematopoiesis. Nature Genet 1999 Dec; 23: 433–6
Annabi B, Hiraiwa H, Mansfield BC, et al. The gene for glycogen-storage disease type 1b maps to chromosome 11q 23. Am J Hum Genet 1998 Feb; 62: 400–5
Donadieu J, Boutard P, Bernatowska E, et al. A European phase II study of recombinant human granulocyte colony-stimulating factor (lenograstim) in the treatment of severe chronic neutropenia in children. Eur J Pediatr 1997 Sep; 156: 693–700
Donadieu J, Bader-Meunier B, Bertrand Y, et al. Recombinant human G-CSF (Lenograstim) for infectious complications in glycogen storage disease type IB — report of 7 cases. Nouv Rev Fr Hematol 1993 Dec; 35: 529–34
DMARDs, splenectomy or colony-stimulating factors for neutropenia in Felty’s syndrome? Drug Ther Perspect 1997 Sep 15; 10 6: 6-9
Stanworth SJ, Bhavnani M, Chattopadhya C, et al. Treatment of Felty’s syndrome with the haemopoietic growth factor granulocyte colony-stimulating factor (G-CSF). Q J Med 1998 Jan; 91: 49–56
Ota K, Teraoka S, Takahashi K, et al. Aprospective randomized dose finding study of lenograstim on leukocytopenia in kidney transplant recipients [in Japanese]. Ishoku 1995; 30(1): 17–29
Ota K, Teraoka S, Takahashi K, et al. A double-blind placebo-controlled study of lenograstim on leukocytopenia in kidney transplant recipients [in Japanese]. Ishoku 1995; 30(1): 30–46
van der Wouw PA, van Leeuwen R, van Oers RHJ, et al. Effects of recombinant human granulocyte colony-stimulating factor on leucopenia in zidovudine-treated patients with AIDS and AIDS related complex, a phase-I/II study. Br J Haematol 1991 Jul; 78: 319–24
Gharakhanian S, Dubreuil-Lenaire M-L, Gori A, et al. A multicentre European, randomised, single-blind, phase Ha study of lenograstim (rHuG-CSF) to allow optimal ganciclovir treatment of CMV infection in neutropenic AIDS patients [abstract]. Proceedings of the 12th World AIDS Conference; 1998 Jun 28–Jul 3; Geneva, Switzerland, 549
Oster G, Menzin J, Richard D, et al. Overview of the lenograstim pharmacoeconomics programme. Pharmacoeconomics 1994; 6 Suppl. 2: 9–17
Mapelli V, Graf von der Schulenberg J-M, Laaser U, et al. Economic evaluation of lenograstim (glycosylated rHuG-CSF) in the treatment of inflammatory breast cancer for Germany and Italy. Pharmacoeconomics 1994; 6 Suppl. 2: 27–35
Souêtre E, Qing W. Economic analysis of lenograstim in the correction of neutropenia following chemotherapy for non-Hodgkin’s lymphoma. Pharmacoeconomics 1994; 6 Suppl. 2: 36–43
Drummond M, Davies L. Economic evaluation of lenograstim for prophylaxis of chemotherapy-induced neutropenia in patients with small cell lung cancer. Pharmacoeconomics 1994; 6 Suppl. 2: 44–52
Brice P, Godin S, Libert O, et al. Effect of lenograstim on the cost of autologous bone marrow transplantation: a preliminary communication. Pharmacoeconomics 1995 Mar; 7: 238–41
Duncan N, Hewetson M, Atra A, et al. An economic evaluation of the use of granulocyte colony-stimulating factor after bone marrow transplantation in children. Pharmacoeconomics 1997 Feb; 11: 169–74
Faucher C, Fortanier C, Viens P, et al. Clinical and economic comparison of lenograstim-primed blood cells (BC) and bone marrow (BM) allogeneic transplantation. Bone Marrow Transplant 1998 Jun; 21 Suppl. 3: S92–8
Rubino C, Laplanche A, Patte C, et al. Cost-minimization analysis of prophylactic granulocyte colony-stimulating factor after induction chemotherapy in children with non-Hodgkin’s lymphoma. J Natl Cancer Inst 1998 May 20; 90: 750–5
Vellenga E, Uyl de Groot CA, de Wit R, et al. Randomized placebo-controlled trial of granulocyte-macrophage colony-stimulating factor in patients with chemotherapy-related febrile neutropenia. J Clin Oncol 1996; 14: 619–27
Webster PJ. Drug utilisation review of filgrastim and lenograstim at Westmead Hospital (WMH) from introduction of Section 100 reimbursement (10/93) to the present [abstract]. Aust J Hosp Pharm 1996 Feb; 26: 156–7
Debrix I, Ait Ben Ali S, Lotz JP, et al. Economic evaluation of the use of two granulocyte colony-stimulating factors in patients treated by intensive chemotherapy. Eur Hosp Pharm 1999 Feb; 5: 24–8
Neutrogin Injection. Lenograstim prescribing information (2nd revised edition). Chugai Pharmaceutical Co. Ltd, Japan, February 1998
Bessho M, Hirashima K, Tomonaga M, et al. Prospective study on clonal complications in adult aplastic anemia patients treated with therapies including recombinant human granulocyte colony-stimulating factor (lenograstim) [abstract]. Blood 1998 Nov 15; 92 (Suppl. 1 Pt 2): 176b
Fatal G-CSF ADRs in Japan. Scrip 1998 Apr 8(2324): 22
Probability of interstitial pneumonia caused by G-CSF reported. Pharm Jpn 996 Aug 19(1512): 10
Falzetti F, Aversa F, Minelli O, et al. Spontaneous rupture of spleen during peripheral blood stem-cell mobilisation in a healthy donor [letter]. Lancet 1999 Feb 13; 353: 555
Richard MA, Grob JJ, Laurans R, et al. Sweet’s syndrome induced by granulocyte colony-stimulating factor in a woman with congenital neutropenia. J Am Acad Dermatol 1996 Oct; 35: 629–31
Norol F, Bonin P, Charpentier F, et al. Apparent reactivation of a red cell alloantibody in a healthy individual after G-CSF administration. Br J Haematol 1998 Oct; 103: 256–8
Anderlini P, Przepiorka D, Körbling M, et al. Blood stem cell procurement: donor safety issues. Bone Marrow Transplant 1998; 21 Suppl. 3: S35–9
Chugai Aventis. Prescribing information Granocyte. International version. Antony, France, Dec 1999
AMRAD Pharmaceuticals Pty Ltd. Data sheet: Granocyte. Kew, Victoria, Australia, Nov 1998
American Society of Clinical Oncology. Update of recommendations for the use of hematopoietic colony-stimulating factors: evidence-based clinical practice guidelines. J Clin Oncol 1996 Jun; 14: 1957–60
Kulkarni S, Powles R, Treleaven J, et al. Comparison of equal doses of lenograstim and filgrastim for mobilization of peripheral blood stem cells in patients with hematologic malignancies [abstract]. Blood 1997 Nov 15; 90 (Suppl. 1 Pt 2): 328b
Author information
Authors and Affiliations
Corresponding author
Additional information
Various sections of the manuscript reviewed by: F. Bertolini, European Institute of Oncology, Milan, Italy; D. Bissett, Department of Clinical Oncology, Aberdeen Royal Infirmary, Aberdeen, Scotland; L.A. Boxer, Department of Pediatric Hematology/Oncology, University of Michigan Hospital, Ann Arbor, Michigan, USA; A.M. Carella, Universitaire Convenzionate, Ospedale San Martino, Genoa, Italy; C. Chevreau, Institut Claudius Regaud, Toulouse, France; J. Donadieu, Service d’Hémato-Oncologie, Hôpital Trousseau, Paris, France; V.V. Garcia, Unidad de Hematología y Oncología Clínica, Hospital General Universitario, Murcia, Spain; M. Höglund, Department of Internal Medicine, University Hospital, Uppsala, Sweden; F. Huguet, Clinique Dieulafoy, Hôpital Purpan, Toulouse, France; N. Niitsu, First Department of Internal Medicine, Toho University School of Medicine, Tokyo, Japan; M. Watts, Haematology Department, University College London, London, England.
Data Selection
Sources: Medical literature published in any language since 1995 on Lenograstim, identified using AdisBase (a proprietary database of Adis International, Auckland, New Zealand) and Medline. Additional references were identified from the reference lists of published articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.
Search strategy: AdisBase search terms were ‘Lenograstim’. Medline search terms were ‘Lenograstim’. Searches were last updated 28.2.2000.
Selection: Studies in patients with neutropenia who received lenograstim. Inclusion of studies was based mainly on the methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred. Relevant pharmacodynamic and pharmacokinetic data are also included.
Index terms: Lenograstim, recombinant human granulocyte colony stimulating factor, rHuG-CSF, cancer, chemotherapy, bone marrow transplantation, peripheral blood stem cell transplantation, leukaemia, aplastic anaemia, congenital neutropenia, AIDS, pharmacodynamics, pharmacokinetics, therapeutic use, pharmacoeconomics, tolerability, dosage and administration.
Rights and permissions
About this article
Cite this article
Dunn, C.J., Goa, K.L. Lenograstim. Drugs 59, 681–717 (2000). https://doi.org/10.2165/00003495-200059030-00017
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-200059030-00017