
Abstract
Disseminated malignancy is the major cause of prostate cancer-related mortality. Circulating tumor cells (CTCs) are essential for the establishment of metastasis. Various contemporary and molecular methods using prostate-specific biomarkers have been applied to detect extraprostatic disease that is undetectable by conventional imaging techniques, assessing the risk for disease recurrence after therapy of curative intent. However, the clinical relevance of CTC detection is still controversial. We review current literature regarding molecular methods used for the detection of CTCs in the peripheral blood and bone marrow biopsies of patients with prostate cancer, and we discuss the methodological pitfalls that influence the clinical significance of molecular staging.
Similar content being viewed by others


Introduction
Adenocarcinoma of the prostate is the most commonly diagnosed cancer among men in Western countries (1). There is an approximate 88% 5-year survival rate for patients with localized prostate cancer, whereas only 29% of patients with metastatic disease survive for 5 years (2). Metastasis, particularly in bones, that is either preexisting at the time of diagnosis or develops after treatment with curative intent is the leading cause of substantial morbidity and mortality in patients with prostate cancer (3–6). Prostate cancer has a propensity for metastasizing to bone tissue. Bone metastasis occurs in more than 85% of cases, and patients with bone lesions cannot be cured (6–10). The development of metastasis is a complex, multistaged process in which the hematogenous spreading of tumor cells is considered to be an intermediate and essential step (11) for the spread of the disease beyond the prostate (6).
Crucial Steps in the Development of Metastasis in Prostate Cancer
Circulating tumor cells (CTCs), also known as the leukemic phase of solid tumors, constitute the hematogenous route of metastasis and are of utmost clinical importance for the establishment of distant metastasis during the metastatic cascade (12,13).
The seed-and-soil hypothesis for the mechanism of bone metastasis, first formulated in 1889 by Stephen Paget, proposes that during the metastatic process, specialized subpopulations of highly metastatic cells within the tumor, endowed with specific properties (13), detach from the primary tumor and migrate to the adjacent tissue. There the cells adhere to the walls of lymphatic and blood vessels, enter into vessels, and disseminate through the systemic vasculature (generally considered the third microenviroment), thus avoiding shear forces, and anchorage independence, ultimately arresting in specific tissues, extravasating, and proliferating in a permissive organ (14). Tumor cells can be protected from undergoing apoptosis by the loss of cell anchorage (anoikis) dependence, thus surviving in the circulation through acquired phenotypic and genotypic alterations (for example, expression of galectin-3) (15). A proposed hypothesis, which requires further evaluation, supports the view that the most invasive cancer cells (only a small minority of carcinoma cells in primary tumors) undergo epithelial-to-mesenchymal transition (EMT), adopt increased cell motility and enhanced invasive cell phenotypes that allow them to infiltrate adjacent tissues, cross endothelial barriers, and enter the circulation through blood and lymphatic vessels (16–18). EMT is presumed to be a highly conserved and fundamental process that achieves morphogenetic transformation conducive to tumor dissemination and metastatic spread and is considered to be characterized by decreased epithelial (for example, cytokeratin) markers, poor histologic differentiation, and increased mesenchymal (for example, vimentin) markers (19,20). EMT is considered a pathological process that contributes to cancer progression, particularly as it relates to invasion and metastasis (18,21). Dedifferentiation, loss of adhesive constraints, and enhanced motility and invasion are all hallmarks of increased malignancy, and EMT is supposed to provide a mechanism for carcinoma cells to acquire this more aggressive phenotype. Once target organs (host tissues) are reached, these mesenchymal cells may need to reverse to an epithelial identity via a mesenchymal-epithelial transition to regain their ability to proliferate (22). Data supporting the actual occurrence of EMT in specific carcinomas have been scant, however. Furthermore, no convincing in vivo evidence for EMT exists. In addition, carcinoma cells do not need to undergo a dramatic conversion in cell identity to achieve all the morphologic and phenotypic changes necessary for metastasis (23). This finding is consistent with the observations that molecular and morphologic characteristics indicative of well-differentiated epithelia, including high levels of E-cadherin expression, the presence of epithelial junctions, and apical-basolateral plasma membrane asymmetry, exist within metastatic lesions of prostate cancer (24,25). The entire process is even more complicated, however, because CTCs may reach multiple organ sites. Thus subsequent seeding by CTCs seems not to be at all random but seems to follow a kind of metastasis tropism, a specific nonrandom homing of prostate cancer cells. A number of significant host-tumor growth and survival factors acting via complex paracrine/autocrine cell interactions between prostate cancer cells and bone cells influence metastatic growth (3,7,26–31). This in turn means that the mobilization of cells from the primary tumor is necessary, but not sufficient, to produce distant metastasis (6,32,33). The mechanism of elimination of these tumor cells is often termed “metastatic inefficiency” (32,34). Thus, the presence of CTCs is a mandatory, but not sufficient, step in generating distant metastasis (mainly bone lesions) during the course of prostate cancer.
Solid tumors are heterogeneous, containing subpopulations of cancer cells with different invasive potential; consequently only a few tumor cells within the tumor mass will achieve successful metastatic implantation (35). Studies suggest that 0.01% of circulating tumor cells ultimately can produce a single bone metastasis, and at least 104 circulating tumor cells are required for the development of a metastatic focus (36,37).
Based on the striking degree of similarity noted between cancer cells and stem cells, including the fundamental abilities of self-renewal and multilineage differentiation, it has been proposed that tumors may originate from cancer “stem cells” that are caused by transforming mutations occurring in multipotential stem cells (38), tissue-specific stem cells (39), progenitor cells (40), mature cells, and cancer cells. The prostatic epithelium contains a spectrum of cells (luminal, basal, and neuroendocrine cells), and consensus exists concerning prostatic epithelial stem cells residing in the basal compartment of the prostate gland (41). Tumor cells escaping from the primary tumor can die by anchorage-dependent cell death (anoikis), become dormant for a number of years, or form macrometastasis (42,43). Contemporary laboratory methods can be used to trace CTCs in the bloodstream of prostate cancer patients, potentially providing useful clinical information with regard to evaluation of tumor progression, prediction of long-term prognosis, identification of patients who are likely to respond to therapies with curative intent, and assessment of likelihood of recurrence. The median survival for patients with bone metastasis and hormone-refractory disease is 16 to 18 months (44). Thus the early detection of CTCs seems to be a promising approach with significant clinical implications (45), such as use in stratification of prostate cancer patients with clinically localized disease into prognostic groups, which may influence therapeutic decisions.
This line of investigation has been actively pursued by several groups using various molecular approaches. Unexpectedly, there has been growing interest as well as confusing controversy over the diagnostic and prognostic implications of CTCs in prostate cancer. We review the current literature, in relation to our experience, regarding the molecular methods used for the detection of CTCs in the peripheral blood of patients with prostate cancer, address methodological pitfalls affecting the clinical significance of CTCs, and discuss the clinical impact of these studies.
Methods for CTC Isolation and Enrichment in Biological Fluids
The most important current methods for detecting CTCs in the peripheral blood of patients with prostate cancer are flow cytometry and qualitative and quantitative reverse transcriptase polymerase chain reaction (RT-PCR). In general, these methods lack specificity to some degree because of the presence of other cellular contaminants, such as red blood cells, normal epithelial cells, and leukocytes. Consequently, several approaches have employed the cancer cell-enrichment technique prior to the detection method (46). This first step allows us to obtain “pure” prostate cell populations, which provide more accurate detection from clinical samples. The most widely used techniques for CTC isolation and enrichment consist of density-gradient centrifugation, filtration, lysis, and positive and negative immunomagnetic selection (IMS).
Density-gradient centrifugation, based on the density of epithelial tumor cells, separates a layer of mononuclear blood cells with CTCs (density <1.077 g/mL) from the other cells (blood cells and granulocytes with density >1.077 g/mL) (47). Density-gradient solutions include the commonly used Ficoll-Hypaque and the less commonly used Lymphoprep. Tumor cell loss can occur with this technique, because tumor cells can sediment to the granulocytic fraction or form cell aggregates at the bottom of the test tube. In addition, whole blood can be mixed with the gradient solution if the centrifugation step is not performed immediately, causing contamination. OncoQuick is a porous barrier that is sometimes added above the density gradient to prevent mixing with whole blood. Mononuclear cells can also be extracted by ammonium-chloride-mediated lysis of red blood cells. Consequently, all of the above-mentioned techniques lead to low sensitivity because only a small proportion of the cancer cells in the clinical sample are recovered.
Alternatively, because of the size difference between circulating epithelial tumor cells and the surrounding blood cells, microfabricated membrane filters have been employed to reliably capture CTCs. In this technique a pair of electrodes is placed on both sides of the filter, thus ensuring the necessary electrical signal for the cell lysis. DNA amplification is then performed. This technology has been suggested to present a high recovery rate (up to 90% with paralyne filters) (48). The detection sensitivity is high, with the ability to capture as few as 1 CTC in 7.5 mL of whole blood.
IMS techniques enhance the sensitivity of RT-PCR as the proportion of the prostate cancer cells to the background nucleated blood cells increases and also enhance the specificity as the unwanted cells that possibly harbor illegitimate transcripts are removed. IMS techniques are based on the specificity of antibody-antigen interactions and the physical properties of magnetic beads that allow for the separation of cells in a heterogeneous cellular population, owing to the different expression in surface antigens among different cell subpopulations. One IMS technique is the positive selection of epithelial cells from mononuclear cells with antiepithelial antibodies. Usually peripheral blood cells, or mononuclear blood cells after red-blood-cell lysis, are incubated with nanometer-sized magnetic beads coated with cell-specific antibodies. Because prostate cancer cells are epithelial in origin, the most commonly used antibodies target either epithelial cell-specific antigens (such as cytokeratins [CK] CK8, CK18, or CK19; human epithelial antigen; and epithelial cell-adhesion molecule [EpCAM]) or organ- or tumor-specific antigens (such as prostate-specific antigen [PSA], prostate-specific membrane antigen [PSMA], carcinoembryonic antigen, and human epidermal growth factor receptor 2) (49). After separation in a magnetic field, sample volume reduction as well enrichment of epithelial cells of 104-fold to 2 × 105-fold is obtained (50). This step is essential in achieving the required sensitivity and low background. Then the epithelial cell-enriched magnetic fraction is subjected to mRNA isolation by use of oligo-deoxythymidine magnetic beads that can be used for downstreaming RT-PCR (51–54). The use of mRNA instead of total RNA decreases background from unspecific priming and helps avoid inhibitory effects due to high concentrations of total RNA. The enriched sample of circulating epithelial cells can also be subsequently used for DNA separation, cell isolation and detection, development of immunoassays, capture of biomolecules, and protein purification. Despite its advantages, IMS technique is limited by the possible loss of tumor cells during the enrichment steps (47). Furthermore, there is a risk of missing the most aggressive cancer cell subpopulations owing to the loss or reduction of the expression of epithelial markers during the EMT process (17,55). In addition, the expression levels of target antigens on cancer cells is potentially diverse. Moreover, some epithelial markers that are expressed by nonepithelial and non-prostate cancer cells could thus give rise to false-positive detections. Similarly, the limitations of the IMS system include a costly and time-consuming process, and variability owing to absence of standardized methods and reagents (56). The intrinsic advantage is that the immunomagnetic selection detects only intact cells, whereas PCR detects living cells, dead cells, and free DNA, resulting in potential false-positive detection results.
Alternatively, depletion of leukocytes with antileukocytic antibodies can be used. Specifically, negative IMS targets cell-surface antigens such as CD45 (expressed in leukocytes) or CD61 (expressed in megakaryocytes and platelets), and has been widely used to enrich tumor cells (57). To further increase enrichment of CTC, a combination of Ficoll-Hypaque centrifugation with negative and positive selection has been applied in many recent studies (47). A summary of the benefits and pitfalls of the current enrichment techniques is presented in Table 1.
The previously mentioned enrichment technologies are also used in the CellSearch system, an automated enrichment and immunocytochemical detection system. The CellSearch system, approved by the US Food and Drug Administration, uses a combination of immunomagnetic labeling and automated digital microscopy to detect CTCs. In the CellSearch system, microscopic iron particles (called ferrofluids) coated with anti-EpCAM antibodies are used to immunomagnetically enrich epithelial cells in a peripheral blood sample drawn from a patient (58). This cell enrichment is followed by immunostaining of captured cells with fluorescently labeled anticytokeratin and anti-CD45 antibodies, and then a semiautomated microscope is used for scanning and reading results (59). If a similar application of CTCs to prostate cancer were proven possible after independent and extensive validation, as has occurred with metastatic breast cancer and colorectal cancer, this method could prove useful in guiding the treatment of prostate cancer as well. Sufficient research has not been conducted, however, to prove the benefit of this system for patients with metastatic or localized prostate cancer. According to Davis et al. (60), in the setting of localized prostate cancer the number of detectable circulating tumor cells as determined using the CellSearch System was very low and did not correlate with tumor volume, pathological stage, and Gleason score.
Principal Prostate-Specific Markers Used for PCR-Based CTC Detection
Prostate-Specific Antigen
PSA is a member of the human kallikrein (hK) gene family (61). PSA can be detected with RT-PCR and has well-defined biologic properties and utility as a serum marker. Recently, a device structure of nanowire/nanotube sensors was successfully employed in the analysis of PSA biomolecules (62). PSA, undoubtedly the most useful clinical serum marker for prostate cancer (63), is expressed by the luminal epithelial cells of the normal prostate gland. PSA is also highly expressed in benign and malignant prostate epithelial cells, which is why it is generally thought of as prostate specific (64), but its expression has also been reported in non-prostate tissue such as pancreas, breast, endometrium, salivary gland, and normal and neoplastic female paraurethral ducts (65,66). PSA has been established as a marker for prostate cancer diagnosis and monitoring (67) and has also been reported to be a useful marker for breast cancer prognosis (68,69). Expression of mRNA for PSA has been shown to be androgen dependent and to be decreased in more poorly differentiated tumors (70). Recent evidence suggests that human tissue kallikrein genes are regulated by alternative splicing, and more recently seven splice variants of a classical KLK3 transcript that all encode for putative PSA-like proteins with homology at their N-terminal domains have been reported (71). Reisenberg et al. (72) showed that in bone marrow aspirates from patients with carcinomas of the prostate a fraction of CK18+ tumor cells in micrometastases do not express PSA, and Mueller et al. (73) have shown that only a few epithelial cytokeratin-positive cells coexpressed PSA.
Prostate-Specific Membrane Antigen
PSMA is a 750-amino acid type II membrane-bound glycoprotein (74). It is a folate γ glutamyl carboxypeptidase that is oriented to the plasma membrane of normal and prostate cancer cells. PSMA is located on the short arm of chromosome 11 (75) and functions both as a folate hydrolase and a neuropeptidase (76,77). PSMA is a highly specific marker of the prostate gland (78) and has been used as a marker gene, indicating hematogenous dissemination of the prostate cancer. PSMA is also highly expressed in the endothelium of tumor-associated neovasculature of non-prostatic solid tumors, but not expressed in that of normal tissue. Non-prostatic tissues also express lower amounts of PSMA, including in the epithelia of the small bowel and the proximal tubules of kidney, salivary gland, muscle, small intestine, and brain (79,80), and predominantly in all types of prostatic tissue, such as benign epithelium, benign prostatic hyperplasia, prostatic intraepithelial neoplasia, and carcinoma (78,81,82). In addition to predominant full-length PSMA, cytosolic PSMA′ has also been found as an alternative splice variant that lacks the encoded transmembrane domain located at the end of exon 1 (83). More recently two other alternatively spliced variants, PSM-C and PSM-D, have also been reported (84). PSMA and its three alternative splice variants are expressed in tissues of normal, benign, cancerous, and metastatic prostate cancer (84). One additional alternatively spliced variant of prostate-specific membrane antigen, PSM-E, has been described even more recently, and PSM-E mRNA levels are increased with an increasing Gleason score (85). The PSMA:PSMA′ mRNA ratio was substantially higher in a number of prostate cancer specimens compared with normal prostate cancer and benign prostatic hypertrophy specimens, and the increased expression of PSMA over PSMA′ also follows the progression from the normal to the tumor state (83). In 184 immuno-histochemically examined radical prostatectomy sections, representative of a study of previously untreated patients, PSMA expression increased incrementally from benign epithelium to highgrade prostatic intraepithelial neoplasia or adenocarcinoma (86). PSMA was expressed in all cases of prostate adenocarcinoma, with the greatest extent and intensity observed in the highest grades (86). Conversely, PSA showed the greatest staining in benign epithelium, with lesser expression, increasingly from benign epithelium to high-grade prostatic intraepithelial neoplasia or adenocarcinoma (86). As a marker, PSMA has an intrinsic advantage over PSA because PSMA is downregulated by androgens and its expression is regulated independently of PSA. Thus PSMA was found to be upregulated in patients with hormonerefractory disease or those treated with androgen ablation therapy (78,87,88). Immunohistochemical studies have proven that PSMA was expressed more intensely than PSA in poorly differentiated primary or secondary prostate cancer lesions. PSMA appears to be highly expressed in anaplastic cells, hormone-refractory cells, and bony metastases (78). If cells capable of hematogenous micrometastasis are the more aggressive and poorly differentiated cells, they may express a higher level of PSMA per cell compared with PSA, enhancing their detectability by RT-PCR (86,89).
Prostate Stem Cell Antigen
The prostate stem-cell antigen (PSCA) gene encodes a 123-amino acid glycoprotein and was first identified in the LAPC-4 prostate xenograft of human prostate cancer (90). This cell-surface antigen is predominantly prostate specific, but lower levels of expression were found in placenta, kidney, and the small intestine (90). PSCA is identified on chromosome 8q24.2 (90), which is often amplified in metastatic and recurrent PCA and is considered to indicate a poor prognosis (91–93). Like stem cell antigen 2 (Sca 2), PSCA also belongs to the Thy-1/Ly-6 family and is a glycosyl phosphatidyli-nositol-anchored cell surface glycoprotein (94,95). The biological function of PSCA remains poorly understood. The restricted expression of PSCA in the basal cells of the normal prostate, which are the putative stem cell compartment of prostatic epithelium, suggests that PSCA may play a role in stem/progenitor cell function, such as self-renewal and/or proliferation (90). PSCA mRNA and PSCA protein are overexpressed in a subset of prostate cancers including advanced, poorly differentiated, androgen independent, and metastatic cases (90,96,97). PSCA is expressed by most prostate cancer metastases (98). Moreover, PSCA is overexpressed at the protein and mRNA levels in the majority of bone metastases compared with lymph node or visceral metastases (98). PSCA expression in normal tissues is largely prostate specific, but PSCA transcripts and protein have been shown to be expressed in the transitional epithelium by most bladder and pancreatic cancers (96,99).
Cytokeratin 19
CK19 is a filamentous cytoskeletal protein that is abundantly expressed in the majority of tumor cells of epithelial origin (100), but interestingly is not expressed by lymph-node lymphocytes, peripheral blood cells, or bone marrow cells (101,102). CK19 expression has also been detected in endothelial cells and fibroblasts (102). CK19 mRNA appears to be a very sensitive tumor marker and has been widely used as an index of the existence of malignant epithelial tumor cells in blood, bone marrow, and lymph nodes of patients with major epithelial malignancies, including epithelial cancers of the lung, pancreas, gastric tissues (103–106), and especially breast (107,108). However, the use of CK19 is often hampered by low specificity because of false-positive results in normal blood attributed to amplification of this epithelial gene from contaminating nontumor cells (such as skin cells) during venipuncture (103), amplification of the known processed pseudogenes because of the primer design (109), or illegitimate or ectopic transcription by hematopoietic cells (110). The presence of two CK19 pseudogenes (CK19a and CK19b) that show a high degree of sequence homology to CK19 mRNA has been reported (109,111). Additionally, cytokines, which circulate at higher concentrations in inflammatory conditions, can cause induction of CK19 expression (112), and consequently prostatitis, an inflammation of the prostate gland, may contribute to false-positive results. Furthermore, CK19 expression has been detected in hematological malignancies such as chronic myelogenous leukemia, chronic lymphocytic leukemia, and myeloblastic syndrome (113). In contrast to breast cancer, for which CK19 is the most frequently used target to detect breast cancer cells in bone marrow or peripheral blood by use of RT-PCR, few studies have evaluated CK19 expression in the peripheral blood mononuclear cell fraction of prostate cancer patients.
Parathyroid Hormone-Related Protein
Parathyroid hormone-related protein (PTHrP) was first discovered as a systemic, tumor-derived, adenylate cyclase-stimulating factor, contributing to the endocrine neoplastic syndrome, humoral hypercalcemia of malignancy, which is associated with several cancers (114,115). PTHrP is a polypeptide hormone that shares N-terminal homology with PTH (114), with 8 of the first 13 amino acids common to the 2 proteins, which allows both to bind to the same receptor in bone and kidney, the PTH-1 receptor (116,117), and share identical biological actions (118). PTHrP elevates plasma calcium by promoting osteoclastic bone resorption and decreasing renal and or intestinal calcium excretion. The PTH and PTHrP genes are thought to have arisen from a common ancestral gene, through an ancient chromosomal duplication event. PTHrP has widespread expression in normal tissues such as heart, skin, parathyroid, skeletal muscle, prostate, lung, and so on, under normal physiologic conditions, and several actions in an autocrine or paracrine fashion have been reported in normal embryogenesis and neonatal development, cellular growth and differentiation, reproduction and lactation, epithelial calcium transport, and smooth muscle relaxation (119,120). The human PTHrP gene is located on chromosome 12, spans approximately 15 kb of genomic DNA, and consists of nine exons (121). Because of alternative splicings of the 3’ end, PTHrP has three isoforms, of 1-139, 1-141, and 1-173 amino acids in length, each containing a unique carboxyl-terminus (121). The transcription of the PTHrP gene is under the control of three distinct promoters located at the 5′ end, identified as P1, P2, and P3. Both P1 and P3 are TATA promoters 5′ to exons I and IV, respectively, and P2 is a GC-rich promoter 5′ to exon III (122). The PTH/PTHrP receptor is a seven-transmembrane domain, G-protein-linked receptor that signals via both adenylate cyclase and phospholipase C (116). Normal prostate expresses PTHrP at a low level (123). Agents that regulate PTHrP expression, such as angiotensin II, epidermal growth factor, estrogen, insulinlike growth factor 1, and transforming growth factor β have been found to upregulate PTHrP production (124,125), whereas dexamethasone profoundly downregulates PTHrP expression (126). PTHrP overexpression is frequently detected in tumors with skeletal metastasis, and it has been correlated to bone metastasis and prognosis in tumor patients. PTHrP expression correlates with increasing tumor grade (127–129). PTHrP overexpression has also been implicated in the pathogenesis of bone metastasis, a significant complication in patients with prostate cancer (127–129). Expression of PTHrP has been associated with the progression of prostate carcinoma (127,130) because it seems to be enhanced by immunohistochemical staining in prostate cancer tissue compared with benign prostatic hypertrophy and has greater intensity in poorly differentiated carcinoma compared with well-differentiated tumors (127). PTHrP expression in malignant prostate cell lines also correlates with tumor invasiveness and metastatic potential, well exemplified by the PC-3 prostate cancer cell line (131). The parathyroid hormone 1 receptor has been reported to be highly expressed in bone metastases from prostate cancer (132). Additionally, PTHrP and its receptor are frequently coexpressed in tumors (133).
PCR-Based Detection Protocols and Their Clinical Relevance
Peripheral blood is the most widely used tissue source for mRNA, due to the relative ease of obtaining the sample. Specifically, detection of prostate-specific mRNAs in the circulation indicates the existence of prostate epithelial cells and, therefore, tumor spread (134,135). RT-PCR, which is more sensitive than more conventional techniques, enables the detection of one tumor cell among 106, 107, or 108 nucleated hematopoeitic cells (136–138). A number of critical parameters for the effectiveness of this method have been noted at different times. The choice of the target marker is perhaps the most crucial, because the ideal market should have expression limited to the prostatic cells, with minimal or no expression in other cells such as leukocytes. Because reality is different from an ideal state, however, the ultrasensitivity of this method can also give rise to false-positive results because of illegitimate transcription or ectopic transcription (139,140). This pitfall is attributable to the fact that every promoter could be activated by ubiquitous transcription factors, leading to an expression level estimated to be 1 tumor marker gene transcript in 500 to 1000 noncancer cells (113). This level of expression is called “illegitimate” because at this level of expression these antigens are not expressed at the protein level and thus cannot be relevant for cellular functions. Therefore, a crucial factor in developing this method for clinical use is the determination of “tumor volume,” or the number of CTCs that possess clinical relevance (137).
Initially, the expression of PSA has been considered specific to prostate cancer, and this marker has been used primarily until now in successive clinical studies as a tissue-specific target for RT-PCR-based detection protocols (135,141–144). Paradoxically, RT-PCR is limited by the extremely high sensitivity of PCR conditions, because false-positive results plague the use of PCR in identifying CTCs (145). Smith et al. (146), Henke et al. (147), and Gala et al. (148) detected PSA mRNA by an ultrasensitive nested PCR-based protocol in non-prostatic cell lines and in blood from healthy males and females, and have clearly demonstrated that analytical sensitivity may compromise the specificity of this method. Other markers that have been used are PSMA and PSCA, which are highly expressed in metastatic tumors (149). However, Gala et al. (148) and Lintula et al. (150) detected the PSMA mRNA in the leukocyte fraction of blood from healthy donors by using ultrasensitive RT-PCR protocols.
In addition, the selection of the primer itself is decisive for analytical sensitivity (147). Primers should span an intron/ exon boundary or should be chosen to bind different exons so that any genomic DNA that might contaminate the RNA sample can be easily differentiated by size from the amplified cDNA. Furthermore, because pseudogenes lack introns, the primers should be well designed to avoid their amplification (151). Other researchers such as Eschwege et al. (152), Oefelein et al. (153), Koutsilieris et al. (154), and Olsson et al. (155) turned their attention to their investigation of the effect of the surgical procedure on CTC detection, showing that surgery can cause hematogenous dissemination of prostate cancer cells, inevitably leading to false-positive results. Furthermore, Koutsilieris et al. (154), Olsson et al. (155), and Hara et al. (156) presented findings suggesting that prostate biopsy might scatter prostate cells with no metastatic potential in the bloodstream, and consequently to avoid false-positive detection the time of PCR-based CTC detection should be at least 4 weeks after an invasive procedure. In contrast, findings reported by Ellis et al. (157) indicated that radical prostatectomy and prostate needle biopsy appeared to have a negligible effect on RT-PCR tests immediately following these procedures. In addition, Dumas et al. (158) reported that acute bacterial prostatitis induces hematogenous dissemination of prostate epithelial cells. Moreover, the specificity is largely influenced by carryover contamination or cross-contamination, illegitimate transcription, and marker expression by nontumor cells in the sample. In an effort to prevent epithelial cell contamination, the first several milliliters of peripheral blood drawn is usually discarded.
Furthermore, Gala et al. (148) reported the importance of repetitive testing in clinical samples, but also noted that decreasing the number of PCR cycles can help avoid the amplification of illegitimate transcripts. It is also important to consider that tumor cell shedding in the bloodstream may be intermittent, and this may be the explanation for the observation that RT-PCR-detection results on the same patient can vary, depending on the timing of blood sampling. Thus, Gala et al. (148) and McIntyre et al. (159) suggested that this problem could be overcome by sequential sampling. Moreover, because nucleic acids are fragile and susceptible to degradation during storage of blood at room temperature, the delay before processing can obviously affect the quality of RNA and influence the results (160,161). Furthermore, inhibitors that are likely to be present in some body tissues and fluids could result in nonamplifiable RNA and therefore produce false-negative detection results. Therefore, the concurrent amplification of certain housekeeping genes is being performed in an attempt to ensure sample quality. These housekeeping genes are constitutively expressed in all cells of the body, including CTCs. If certain levels of a housekeeping gene are detected, one can assume that the sample is in good condition and therefore the PCR-based protocols are performed on a qualified RNA sample. Some of the housekeeping genes used for prostate cancer PCR studies include ACTb and GAPDH. However, the hormonal treatment that some patients receive may cause down-regulation of the target gene; furthermore, poorly differentiated prostate cancer subclones may not express the tissue-specific gene, a situation that could give rise to false-negative results. Specifically, PSA mRNA expression is known to be decreased by androgen ablation therapy (162) and in poorly differentiated prostatic carcinoma (163).
The presence of CTCs has also been associated with clinically meaningful prognostic factors, such as stage, Gleason score, and seminal vesicle invasion (164,165). Furthermore, CTCs have been significantly correlated in some of these studies with time to PSA progression, disease-free survival, and overall survival (166–169). Other studies, however, have failed to confirm such findings (170,171).
Controversy exists regarding the ability of peripheral blood PSA RT-PCR testing to reflect pathological staging or treatment outcome. Katz et al. (135) identified a correlation between positive PSA RT-PCR in the peripheral circulation of surgical-candidate patients and the presence of capsular penetration (sensitivity 68%, specificity 84%) as well as strong correlation with positive surgical margins (sensitivity 87%, specificity 76%). Consequently, these investigators concluded that PSA RT-PCR assay is markedly superior to digital rectal examination, computed tomographic scan, endorectal coil magnetic resonance imaging, serum PSA, prostate-specific antigen density, or Gleason score for correctly staging apparent localized prostate cancer prior to radical prostatectomy (135) and predicting surgical pathology and postoperative biochemical recurrence (172). Cama et al. (149) demonstrated a significantly strong correlation between a positive PSA RT-PCR peripheral-blood assay in patients with clinically localized tumor invasion (67% sensitivity for detecting capsular penetration, 87% sensitivity for detecting disease to the surgical margin, and 83% sensitivity for detecting seminal vesicle invasion) and concluded that this technique is a highly sensitive staging modality for preoperative detection of extraprostatic disease. Katz et al. (173) reported a 65% sensitivity and 90% specificity of RT-PCR for PSA in detecting extracapsular disease and 69% sensitivity and 84% specificity in predicting potential surgical failure. According to Olsson et al. (174), a positive RT-PCR for PSA of candidates for radical prostatectomy appears to have a better predictive value of potential surgical failure and of disease recurrence compared with conventional preoperative modalities such as serum PSA or Gleason score. A combined PSA/PSMA RT-PCR in blood samples of patients with clinically localized prostatic carcinoma scheduled to undergo radical prostatectomy has been suggested as an independent predictor of time to biochemical failure following surgery (175). According to Sourla et al. (176), a conversion of RT-PCR positivity for PSA and PSMA to a negative status at the peripheral blood of patients with stage D2 disease during objective clinical response to androgen ablation therapy was associated with longer progressionfree survival. Additionally, a PSA RT-PCR assay made possible the preoperative identification of patients with positive surgical margins or invasion into the seminal vesicle among those patients who were scheduled for radical retropubic prostatectomy, thus providing for them unique prognostic information (177). Ghossein et al. (178) found the detection of PSA mRNA in the peripheral blood of patients with known metastatic (stage D2) androgen-independent prostatic carcinoma to be an indicator of their survival, and demonstrated PCR to be independent of and superior to serum PSA value in predicting biochemical failure among these patients. However, Ellis et al. (157) found that the RT-PCR results of patients with pT3 disease before and after radical prostatectomy failed to preoperatively predict the pathological stage of prostate cancer or treatment failure.
Okegawa et al. (179) showed that the results of nested RT-PCR using PSMA primers in the group of patients who eventually underwent radical prostatectomy were significantly correlated with the pathologic stage of the cancer, and their data indicated that RT-PCR can preoperatively distinguish organ-confined disease from extraprostatic disease. Nested RT-PCR using PSMA primers appears to predict the prostate cancer stage more accurately than does nested RT-PCR using PSA primers or conventional clinical staging modalities (179). According to Zhang et al. (180), the combined PSA/PSMA assay is more sensitive than the PSA assay alone in detecting circulating prostatic cells, shows correlation with the pathological stage, and provides staging information unavailable from other modalities, including the clinical stage, initial serum PSA, and Gleason score. The PSMA/PSA RT-PCR assay had a sensitivity of 67% and a specificity of 91% in predicting extracapsular disease (180). Grasso et al. (164) showed that PSA/PSMA nested RT-PCR had an 81% sensitivity and 63% specificity in predicting tumor extracapsular extension, and that RT-PCR was a better predictor of final pathological stage than clinical stage, serum PSA, and biopsy Gleason score. Nested PSMA RT-PCR identified more tumors with extracapsular extension, seminal vesicle invasion, and positive surgical margin than did RT-PCR for PSA (164). According to Cama et al. (149), an RT-PCR assay for prostate-specific membrane antigen did not correlate with pathological stage of prostate cancer. Loric et al. (181) suggested that the detection of PSMA-expressing cells in blood may predict the development of cancer in patients without clinically apparent prostate cancer. Noguchi et al. (182) found that the PSMA PCR-positive rate did not correlate with clinical stage, pathologic stage, tumor grade, or serum PSA levels. According to Sokoloff et al. (143), circulating PSMA PCR signals were identified mostly in patients with advanced prostate cancer and offered no benefit to preoperative staging. In our study (137) of patients with clinically localized prostate cancer and positive RT-PCR detection of PSA and PSMA transcripts in peripheral blood, the administration of combined androgen blockade can convert positive molecular staging status to negative, thus increasing the biochemical failure-free survival of those patients after subsequent curative treatment.
Elevated PSCA expression has been shown to correlate with increased Gleason score and tumor stage (96,183). Moreover, PSCA overexpression is also correlated with an increased risk of biochemical recurrence (184). Hara et al. (183) noted that patients with PSCA-positive circulating cells had a higher mean Gleason score than those who were PSCA negative. Furthermore, according to Hara et al. (183), in extraprostatic cases positive PSCA PCR indicated lower disease-progression-free survival than those with negative PSCA PCR. Finally, PSCA positivity correlated with extraprostatic extension; 47% of extraorgan disease cases were PSCA positive, whereas all cases of organ-confined prostate cancer were PSCA negative (183). A tissue microarray analysis constructed from 246 radical prostatectomy specimens has also shown that high PSCA intensity is associated with adverse prognostic factors such as a high Gleason score, seminal vesicle invasion, and capsular involvement (184). Joung et al. (185) reported that PSCA positivity in peripheral blood was identified more frequently in patients with extraprostatic disease and with a high Gleason score. Dannull et al. (186) also reported that PSCA mRNA expression was present in all metastatic prostate cancer tissues examined. Ross et al. (99) also showed that the percentage of metastatic prostate cancer cases positive for PSCA mRNA expression was higher (64%) than that of benign prostate disease and organ-confined prostate cancer (48%). Zhigang et al. (187) demonstrated that complete androgen blockade for prostate cancer can suppress PSCA mRNA expression with a tumor grade dependence, and the increased expression of PSCA mRNA after complete androgen blockade may be a clinically adverse predictor for tumor recurrence or distant metastases. Additional studies are required for an evaluation of PSCA as a diagnostic and therapeutic target for prostate cancer.
Although conflicting results have been obtained, results of several studies indicate that the CK19 mRNA is detectable in the blood of patients with cancers of the breast, lung, stomach, and pancreas, but not of those with benign lesions of these organs (103,105,188). Interestingly, the positivity of CK19 mRNA after, but not before, chemoradiation treatment appears to indicate a worse prognosis for patients. A possible explanation may host immune-system compromise following chemoradiation, so that the existing circulating tumor cells would have greater opportunity to avoid host immune surveillance and to survive (189). Consequently, stronger systemic therapies would be necessary to decrease or delay overt distant metastasis. It should be taken into consideration that a significant association exists between CK19-positive status and the presence of distant metastases. Several studies suggest the vast potential usefulness of CK19 mRNA detection in peripheral blood in the prediction of a poor clinical outcome (190,191). Kaneda et al. (192) evaluated the CK19 RT-PCR in the peripheral blood of patients with urogenital malignancy (bladder, renal, testicular, and penile cancer cases) and their findings suggested a significantly strong correlation between positive CK19 nested RT-PCR in the peripheral blood and the presence of distant metastasis. CK19 mRNA was not detected in any of 9 controls; 3 of 7 prostate cancer cases were positive, and all 3 cases had distant metastases (192). According to Machado et al. (193), CK19 mRNA expression was not detected in any of the 10 healthy control men, and among 44 prostate cancer patients, CK19 expression by RT-PCR correlated with time to PSA progression. A summary of the various clinically relevant markers is presented in Tables 2 and 3.
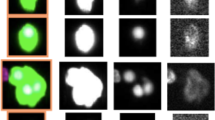
As a consequence of the variable technical approaches that have been applied, as well as the difficulty of determining the ratio of sensitivity to specificity of the PCR conditions, the lack of controlling for the detectable disease volume and its clinical relevance, as well as the number of patients versus controls and the data interpretation, it is very difficult to draw firm conclusions about the clinical applications of PCR-based protocols for the detection of CTCs in prostate cancer. Therefore, current investigations are focusing on the use of multiplexed PCR-based detection of CTCs using PSA, PSMA, PSCA, PTHrP, and CK19 molecular markers and analyzing clinical significance (see Figure 1). Some of the above-mentioned limitations of RT-PCR could be circumvented by multiplex RT-PCR based on the differential expression of different genes from different families used in combination. In conclusion, PCR-based methods should be sensitive enough to allow for the detection of CTCs and specific enough not to detect illegitimate transcripts and disease volume that do not have any clinical implications. Until these issues are resolved, PCR-based protocols remain primarily an investigative tool.

An example of a multiplex PCR protocol for the detection of prostate-specific antigen (PSA), prostate-specific membrane antigen (PSMA), prostate stemcell antigen (PSCA), parathyroid hormone-related protein (PTHrP), and cytokeratin 19 (CK19) mRNA in a peripheral blood sample from a prostate cancer patient. Lane M, size markers; lane A, sample from prostate cancer patient with metastatic disease; lane B, sample from healthy young male (negative control).
Ultimately, it is fair to consider that RT-PCR detection of CTCs in prostate cancer patients as an additional tool to be used in cases of “high probability for systemic disease,” such as in patients with Gleason scores ≥7–10, PSA ≥20 ng/mL or “suspicious uptakes” in bone scans. From a research standpoint, in such cases PCR-based detection of PSA/PSMA/PSCA/PTHrP/CK19 mRNA, mainly by multiplex PCR methods, would add to the selection of otherwise clinically localized prostate cancer patients for systemic therapy, an adjuvant or neoadjuvant approach to therapies with curative intent, such as radical prostatectomy and radiotherapy.
Disclosure
We declare that the authors have no competing interests as defined by Molecular Medicine, or other interests that might be perceived to influence the results and discussion reported in this paper.
References
Landis SH, Murray T, Bolden S, Wingo PA. (1999) Cancer statistics, 1999. CA Cancer J. Clin. 49:8–31.
Coffey DS. (1993) Prostate cancer: an overview of an increasing dilemma. Cancer 71:880–6.
Arya M, et al. (2006) The metastatic cascade in prostate cancer. Surg. Oncol. 15:117–28.
Pantel K, Brakenhoff RH. (2004) Dissecting the metastatic cascade. Nat. Rev. Cancer 4:448–56.
Weiss L. (2000) Metastasis of cancer: a conceptual history from antiquity to the 1990s. Cancer Metastasis Rev. 19:193–383.
Jacob K, Sollier C, Jabado N. (2007) Circulating tumor cells: detection, molecular profiling and future prospects. Expert Rev. Proteomics 4:741–56.
Msaouel P, Pissimissis N, Halapas A, Koutsilieris M. (2008) Mechanisms of bone metastasis in prostate cancer: clinical implications. Best Pract. Res. Clin. Endocrinol. Metab. 22:341–55.
Jacobs SC. (1983) Spread of prostatic cancer to bone. Urology 21:337–44.
Bubendorf L, et al. (2000) Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum. Pathol. 31:578–83.
Labrie F, et al. (1993) Optimized strategy for detection of early stage, curable prostate cancer: role of prescreening with prostate-specific antigen. Clin. Invest. Med. 16:425–39.
Glaves D. (1983) Correlation between circulating cancer cells and incidence of metastases. Br. J. Cancer 48:665–73.
Mocellin S, Keilholz U, Rossi CR, Nitti D. (2006) Circulating tumor cells: the “leukemic phase” of solid cancers. Trends Mol. Med. 12:130–9.
Poste G, Fidler IJ. (1980) The pathogenesis of cancer metastasis. Nature 283:139–46.
Koutsilieris M. (1995) Skeletal metastases in advanced prostate cancer: cell biology and therapy. Crit. Rev. Oncol. Hematol. 18:51–64.
Kim HR, Lin HM, Biliran H, Raz A. (1999) Cell cycle arrest and inhibition of anoikis by galectin-3 in human breast epithelial cells. Cancer Res. 59:4148–54.
Yang J, Mani SA, Weinberg RA. (2006) Exploring a new twist on tumor metastasis. Cancer Res. 66:4549–52.
Thompson EW, Newgreen DF, Tarin D. (2005) Carcinoma invasion and metastasis: a role for epithelial-mesenchymal transition? Cancer Res. 65:5991–5; discussion 5995.
Bates RC, Mercurio AM. (2005) The epithelial-mesenchymal transition (EMT) and colorectal cancer progression. Cancer Biol. Ther. 4:365–70.
Willipinski-Stapelfeldt B, et al. (2005) Changes in cytoskeletal protein composition indicative of an epithelial-mesenchymal transition in human micrometastatic and primary breast carcinoma cells. Clin. Cancer Res. 11:8006–14.
Lang SH, et al. (2002) Enhanced expression of vimentin in motile prostate cell lines and in poorly differentiated and metastatic prostate carcinoma. Prostate 52:253–63.
Arias AM. (2001) Epithelial mesenchymal interactions in cancer and development. Cell 105:425–31.
Christiansen JJ, Rajasekaran AK. (2006) Reassessing epithelial to mesenchymal transition as a prerequisite for carcinoma invasion and metastasis. Cancer Res. 66:8319–26.
Tarin D, Thompson EW, Newgreen DF. (2005) The fallacy of epithelial mesenchymal transition in neoplasia. Cancer Res. 65:5996–6000; discussion 6000–1.
Rubin MA, et al. (2000) Rapid (“warm”) autopsy study for procurement of metastatic prostate cancer. Clin. Cancer Res. 6:1038–45.
Christiansen JJ, et al. (2005) N-glycosylation and microtubule integrity are involved in apical targeting of prostate-specific membrane antigen: implications for immunotherapy. Mol. Cancer Ther. 4:704–14.
Koutsilieris M, et al. (2001) A combination therapy of dexamethasone and somatostatin analog reintroduces objective clinical responses to LHRH analog in androgen ablation-refractory prostate cancer patients. J. Clin. Endocrinol. Metab. 86:5729–36.
Fidler IJ. (2003) The pathogenesis of cancer metastasis: the “seed and soil” hypothesis revisited. Nat. Rev. Cancer 3:453–8.
Karamanolakis D, et al. (2002) Molecular evidence-based use of bone resorption-targeted therapy in prostate cancer patients at high risk for bone involvement. Mol. Med. 8:667–75.
Koutsilieris M. (1993) Osteoblastic metastasis in advanced prostate cancer. Anticancer Res. 13:443–9.
Mitsiades CS, Koutsilieris M. (2001) Molecular biology and cellular physiology of refractoriness to androgen ablation therapy in advanced prostate cancer. Expert Opin. Investig. Drugs 10:1099–15.
Tenta R, Sotiriou E, Pitulis N, Thyphronitis G, Koutsilieris M. (2005) Prostate cancer cell survival pathways activated by bone metastasis microenvironment. J. Musculoskelet. Neuronal Interact. 5:135–44.
Weiss L. (1990) Metastatic inefficiency. Adv. Cancer Res. 54:159–211.
Sugarbaker PH. (1993) Metastatic inefficiency: the scientific basis for resection of liver metastases from colorectal cancer. J. Surg. Oncol. Suppl. 3:158–60.
Fidler IJ. (1990) Critical factors in the biology of human cancer metastasis: twenty-eighth G.H.A. Clowes memorial award lecture. Cancer Res. 50:6130–8.
Fidler IJ, Kripke ML. (1977) Metastasis results from preexisting variant cells within a malignant tumor. Science 197:893–5.
Fidler IJ. (1970) Metastasis: guantitative analysis of distribution and fate of tumor embolilabeled with 125 I-5-iodo-2′-deoxyuridine. J. Natl. Cancer Inst. 45:773–82.
Liotta LA, Saidel MG, Kleinerman J. (1976) The significance of hematogenous tumor cell clumps in the metastatic process. Cancer Res. 36:889–94.
Reya T, Morrison SJ, Clarke MF, Weissman IL. (2001) Stem cells, cancer, and cancer stem cells. Nature 414:105–11.
Martinez-Climent JA, Andreu EJ, Prosper F. (2006) Somatic stem cells and the origin of cancer. Clin. Transl. Oncol. 8:647–63.
Jabbour MN, Matioli GT. (2006) Age dependent and cellular origin (stem versus progenitor) of a selected group of spontaneous brain tumors in humans. Med. Hypotheses 67:1437–42.
Tokar EJ, Ancrile BB, Cunha GR, Webber MM. (2005) Stem/progenitor and intermediate cell types and the origin of human prostate cancer. Differentiation 73:463–73.
Alix-Panabieres C, et al. (2005) Characterization and enumeration of cells secreting tumor markers in the peripheral blood of breast cancer patients. J. Immunol. Methods 299:177–88.
Alix-Panabieres C, et al. (2007) Detection and characterization of putative metastatic precursor cells in cancer patients. Clin. Chem. 53:537–9.
Oh WK, Kantoff PW. (1998) Management of hormone refractory prostate cancer: current standards and future prospects. J. Urol. 160:1220–9.
Mukamel E, Hanna J, deKernion JB. (1987) Pitfalls in preoperative staging in prostate cancer. Urology 30:318–21.
Makarovskiy AN, et al. (1997) Application of immunomagnetic beads in combination with RT-PCR for the detection of circulating prostate cancer cells. J. Clin. Lab. Anal. 11:346–50.
Morgan TM, Lange PH, Vessella RL. (2007) Detection and characterization of circulating and disseminated prostate cancer cells. Front Biosci. 12:3000–9.
Zheng S, et al. (2007) Membrane microfilter device for selective capture, electrolysis and genomic analysis of human circulating tumor cells. J. Chromatogr. A. 1162:154–61.
Kruger W, et al. (2000) Immunomagnetic tumor cell selection—implications for the detection of disseminated cancer cells. Transfusion 40:1489–1493.
Paterlini-Brechot P, Benali NL. (2007) Circulating tumor cells (CTC) detection: clinical impact and future directions. Cancer Lett. 253:180–204.
Zigeuner RE, Riesenberg R, Pohla H, Hofstetter A, Oberneder R. (2000) Immunomagnetic cell enrichment detects more disseminated cancer cells than immunocytochemistry in vitro. J. Urol. 164:1834–7.
Racila E, et al. (1998) Detection and characterization of carcinoma cells in the blood. Proc. Natl. Acad. Sci. U. S. A. 95:4589–94.
Meye A, et al. (2002) Isolation and enrichment of urologic tumor cells in blood samples by a semi-automated CD45 depletion autoMACS protocol. Int. J. Oncol. 21:521–30.
Ghossein RA, et al. (1999) Detection of prostatic specific membrane antigen messenger RNA using immunobead reverse transcriptase polymerase chain reaction. Diagn. Mol. Pathol. 8:59–65.
Kong D, et al. (2008) Platelet-derived growth factor-D overexpression contributes to epithelial-mesenchymal transition of PC3 prostate cancer cells. Stem Cells 26:1425–35.
Loberg RD, et al. (2004) Detection and isolation of circulating tumor cells in urologic cancers: a review. Neoplasia 6:302–9.
Ellis WJ, et al. (2003) Detection and isolation of prostate cancer cells from peripheral blood and bone marrow. Urology 61:277–81.
Riethdorf S, et al. (2007) Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin. Cancer Res. 13:920–8.
Cristofanilli M, et al. (2004) Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 351:781–91.
Davis JW, et al. (2008) Circulating tumor cells in peripheral blood samples from patients with increased serum prostate specific antigen: initial results in early prostate cancer. J. Urol. 179:2187–91.
Borgono CA, Diamandis EP. (2004) The emerging roles of human tissue kallikreins in cancer. Nat. Rev. Cancer 4:876–90.
Li C, et al. (2005) Complementary detection of prostate-specific antigen using In2O3 nanowires and carbon nanotubes. J. Am. Chem. Soc. 127:12484–5.
Crawford ED, Abrahamsson PA. (2008) PSA-based screening for prostate cancer: how does it compare with other cancer screening tests? Eur. Urol. 54:262–73.
Papsidero LD, et al. (1981) Prostate antigen: a marker for human prostate epithelial cells. J. Natl. Cancer Inst. 66:37–42.
Elgamal AA, et al. (1996) Detection of prostate specific antigen in pancreas and salivary glands: a potential impact on prostate cancer overestimation. J. Urol. 156:464–8.
Frazier HA, Humphrey PA, Burchette JL, Paulson DF. (1992) Immunoreactive prostatic specific antigen in male periurethral glands. J. Urol. 147:246–8.
Stenman UH, Leinonen J, Zhang WM, Finne P. (1999) Prostate-specific antigen. Semin. Cancer Biol. 9:83–93.
Black MH, Diamandis EP. (2000) The diagnostic and prognostic utility of prostate-specific antigen for diseases of the breast. Breast Cancer Res. Treat. 59:1–14.
Yu H, et al. (1995) Prostate-specific antigen is a new favorable prognostic indicator for women with breast cancer. Cancer Res. 55:2104–10.
Henttu P, Liao SS, Vihko P. (1992) Androgens up-regulate the human prostate-specific antigen messenger ribonucleic acid (mRNA), but down-regulate the prostatic acid phosphatase mRNA in the LNCaP cell line. Endocrinology 130:766–72.
Pampalakis G, Scorilas A, Sotiropoulou G. (2008) Novel splice variants of prostate-specific antigen and applications in diagnosis of prostate cancer. Clin. Biochem. 41:591–7.
Riesenberg R, et al. (1993) Immunocytochemical double staining of cytokeratin and prostate specific antigen in individual prostatic tumour cells. Histochemistry 99:61–6.
Mueller P, et al. (1998) Low frequency epithelial cells in bone marrow aspirates from prostate carcinoma patients are cytogenetically aberrant. Cancer 83:538–46.
Israeli RS, Powell CT, Fair WR, Heston WD. (1993) Molecular cloning of a complementary DNA encoding a prostate-specific membrane antigen. Cancer Res. 53:227–30.
O’Keefe DS, et al. (1998) Mapping, genomic organization and promoter analysis of the human prostate-specific membrane antigen gene. Biochim. Biophys. Acta 1443:113–27.
Pinto JT, et al. (1996) Prostate-specific membrane antigen: a novel folate hydrolase in human prostatic carcinoma cells. Clin. Cancer Res. 2:1445–51.
Luthi-Carter R, Barczak AK, Speno H, Coyle JT. (1998) Molecular characterization of human brain N-acetylated alpha-linked acidic dipeptidase (NAALADase). J. Pharmacol. Exp. Ther. 286:1020–5.
Israeli RS, Powell CT, Corr JG, Fair WR, Heston WD. (1994) Expression of the prostate-specific membrane antigen. Cancer Res. 54:1807–11.
Fair WR, Israeli RS, Heston WD. (1997) Prostate-specific membrane antigen. Prostate 32:140–8.
Gregorakis AK, Holmes EH, Murphy GP. (1998) Prostate-specific membrane antigen: current and future utility. Semin. Urol. Oncol. 16:2–12.
Silver DA, Pellicer I, Fair WR, Heston WD, Cordon-Cardo C. (1997) Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 3:81–5.
Sweat SD, Pacelli A, Murphy GP, Bostwick DG. (1998) Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology 52:637–40.
Su SL, Huang IP, Fair WR, Powell CT, Heston WD. (1995) Alternatively spliced variants of prostate-specific membrane antigen RNA: ratio of expression as a potential measurement of progression. Cancer Res. 55:1441–3.
Schmittgen TD, Teske S, Vessella RL, True LD, Zakrajsek BA. (2003) Expression of prostate specific membrane antigen and three alternatively spliced variants of PSMA in prostate cancer patients. Int. J. Cancer 107:323–9.
Cao KY, et al. (2007) High expression of PSM-E correlated with tumor grade in prostate cancer: a new alternatively spliced variant of prostate-specific membrane antigen. Prostate 67:1791–1800.
Bostwick DG, Pacelli A, Blute M, Roche P, Murphy GP. (1998) Prostate specific membrane antigen expression in prostatic intraepithelial neoplasia and adenocarcinoma: a study of 184 cases. Cancer 82:2256–2261.
Kawakami M, Nakayama J. (1997) Enhanced expression of prostate-specific membrane antigen gene in prostate cancer as revealed by in situ hybridization. Cancer Res. 57:2321–4.
Wright GL, et al. (1996) Upregulation of prostate-specific membrane antigen after androgen-deprivation therapy. Urology 48:326–34.
Ross JS, et al. (2003) Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin. Cancer Res. 9:6357–62.
Reiter RE, et al. (1998) Prostate stem cell antigen: a cell surface marker overexpressed in prostate cancer. Proc. Natl. Acad. Sci. U. S. A. 95:1735–40.
Visakorpi T, et al. (1995) Genetic changes in primary and recurrent prostate cancer by comparative genomic hybridization. Cancer Res. 55:342–7.
Sato K, et al. (1999) Clinical significance of alterations of chromosome 8 in high-grade, advanced, nonmetastatic prostate carcinoma. J. Natl. Cancer Inst. 91:1574–80.
Van Den Berg C, et al. (1995) DNAsequence amplification in human prostate cancer identified by chromosome microdissection: potential prognostic implications. Clin. Cancer Res. 1:11–8.
Antica M, Wu L, Scollay R. (1997) Stem cell antigen 2 expression in adult and developing mice. Immunol Lett. 55:47–51.
Classon BJ, Coverdale L. (1994) Mouse stem cell antigen Sca-2 is a member of the Ly-6 family of cell surface proteins. Proc. Natl. Acad. Sci. U. S. A. 91:5296–300.
Gu Z, et al. (2000) Prostate stem cell antigen (PSCA) expression increases with high Gleason score, advanced stage and bone metastasis in prostate cancer. Oncogene 19:1288–96.
Zhigang Z, Wenlv S. (2004) Prostate stem cell antigen (PSCA) expression in human prostate cancer tissues and its potential role in prostate carcinogenesis and progression of prostate cancer. World J. Surg. Oncol. 2:13.
Lam JS, et al. (2005) Prostate stem cell antigen is overexpressed in prostate cancer metastases. Clin. Cancer Res. 11:2591–6.
Ross S, et al. (2002) Prostate stem cell antigen as therapy target: tissue expression and in vivo efficacy of an immunoconjugate. Cancer Res. 62:2546–53.
Bartek J, et al. (1986) Differential expression of keratin 19 in normal human epithelial tissues revealed by monospecific monoclonal antibodies. Histochem. J. 18:565–75.
Datta YH, et al. (1994) Sensitive detection of occult breast cancer by the reverse-transcriptase polymerase chain reaction. J. Clin. Oncol. 12:475–82.
Traweek ST, Liu J, Battifora H. (1993) Keratin gene expression in non-epithelial tissues. Detection with polymerase chain reaction. Am. J. Pathol. 142:1111–8.
Peck K, et al. (1998) Detection and quantitation of circulating cancer cells in the peripheral blood of lung cancer patients. Cancer Res. 58:2761–5.
Yeh KH, et al. (1998) Detection of circulating cancer cells by nested reverse transcription-polymerase chain reaction of cytokeratin-19 (K19)—possible clinical significance in advanced gastric cancer. Anticancer Res. 18:1283–6.
Aihara T, et al. (1997) Detection of pancreatic and gastric cancer cells in peripheral and portal blood by amplification of keratin 19 mRNA with reverse transcriptase-polymerase chain reaction. Int. J. Cancer 72:408–11.
Hoffmann K, et al. (2007) Detection of disseminated pancreatic cells by amplification of cytokeratin-19 with quantitative RT-PCR in blood, bone marrow and peritoneal lavage of pancreatic carcinoma patients. World J. Gastroenterol. 13:257–63.
Stathopoulou A, et al. (2003) Real-time quantification of CK-19 mRNA-positive cells in peripheral blood of breast cancer patients using the lightcycler system. Clin. Cancer Res. 9:5145–51.
Balducci E, et al. (2005) A new nested primer pair improves the specificity of CK-19 mRNA detection by RT-PCR in occult breast cancer cells. Int. J. Biol. Markers 20:28–33.
Ruud P, Fodstad O, Hovig E. (1999) Identification of a novel cytokeratin 19 pseudogene that may interfere with reverse transcriptase-polymerase chain reaction assays used to detect micrometastatic tumor cells. Int. J. Cancer 80:119–25.
Krismann M, et al. (1995) Low specificity of cytokeratin 19 reverse transcriptase-polymerase chain reaction analyses for detection of hematogenous lung cancer dissemination. J. Clin. Oncol. 13:2769–75.
Savtchenko ES, Schiff TA, Jiang CK, Freedberg IM, Blumenberg M. (1988) Embryonic expression of the human 40-kD keratin: evidence from a processed pseudogene sequence. Am. J. Hum. Genet. 43:630–7.
Jung R, et al. (1998) Specificity of reverse transcriptase polymerase chain reaction assays designed for the detection of circulating cancer cells is influenced by cytokines in vivo and in vitro. Br. J. Cancer 78:1194–8.
Zieglschmid V, Hollmann C, Bocher O. (2005) Detection of disseminated tumor cells in peripheral blood. Crit. Rev. Clin. Lab. Sci. 42:155–96.
Suva LJ, et al. (1987) Aparathyroid hormone-related protein implicated in malignant hypercalcemia: cloning and expression. Science 237:893–6.
Rankin W, Grill V, Martin TJ. (1997) Parathyroid hormone-related protein and hypercalcemia. Cancer 80:1564–71.
Abou-Samra AB, et al. (1992) Expression cloning of a common receptor for parathyroid hormone and parathyroid hormone-related peptide from rat osteoblast-like cells: a single receptor stimulates intracellular accumulation of both cAMP and inositol trisphosphates and increases intracellular free calcium. Proc. Natl. Acad. Sci. U. S. A. 89:2732–6.
Juppner H, Hesch RD. (1991) Biochemical characterization of cellular hormone receptors. Curr. Top. Pathol. 83:53–69.
Strewler GJ, et al. (1987) Parathyroid hormonelike protein from human renal carcinoma cells. Structural and functional homology with parathyroid hormone. J. Clin. Invest. 80:1803–7.
de Papp AE, Stewart AF. (1993) Parathyroid hormone-related protein a peptide of diverse physiologic functions. Trends Endocrinol. Metab. 4:181–7.
Rodda CP, et al. (1988) Evidence for a novel parathyroid hormone-related protein in fetal lamb parathyroid glands and sheep placenta: comparisons with a similar protein implicated in humoral hypercalcaemia of malignancy. J. Endocrinol. 117:261–71.
Southby J, O’Keeffe LM, Martin TJ, Gillespie MT. (1995) Alternative promoter usage and mRNA splicing pathways for parathyroid hormone-related protein in normal tissues and tumours. Br. J. Cancer 72:702–7.
Campos RV, Wang C, Drucker DJ. (1992) Regulation of parathyroid hormone-related peptide (PTHrP) gene transcription: cell- and tissue-specific promoter utilization mediated by multiple positive and negative cis-acting DNA elements. Mol. Endocrinol. 6:1642–52.
Iwamura M, et al. (1994) Parathyroid hormone-related protein is expressed by prostatic neuroendocrine cells. Urology 43:667–74.
Kiriyama T, et al. (1993) Transforming growth factor beta stimulation of parathyroid hormone-related protein (PTHrP): a paracrine regulator? Mol. Cell. Endocrinol. 92:55–62.
Pirola CJ, et al. (1993) Angiotensin II regulates parathyroid hormone-related protein expression in cultured rat aortic smooth muscle cells through transcriptional and post-transcriptional mechanisms. J. Biol. Chem. 268:1987–94.
Glatz JA, et al. (1994) Dexamethasone regulation of parathyroid hormone-related protein (PTHrP) expression in a squamous cancer cell line. Mol. Cell. Endocrinol. 101:295–306.
Asadi F, et al. (1996) Enhanced expression of parathyroid hormone-related protein in prostate cancer as compared with benign prostatic hyperplasia. Hum. Pathol. 27:1319–23.
Iwamura M, et al. (1994) Parathyroid hormone-related protein: a potential autocrine growth regulator in human prostate cancer cell lines. Urology 43:675–9.
Rabbani SA, Gladu J, Harakidas P, Jamison B, Goltzman D. (1999) Over-production of parathyroid hormone-related peptide results in increased osteolytic skeletal metastasis by prostate cancer cells in vivo. Int. J. Cancer 80:257–64.
Deftos LJ. (2000) Prostate carcinoma: production of bioactive factors. Cancer 88:3002–8.
Deftos LJ, Barken I, Burton DW, Hoffman RM, Geller J. (2005) Direct evidence that PTHrP expression promotes prostate cancer progression in bone. Biochem. Biophys. Res. Commun. 327:468–72.
Bryden AA, Hoyland JA, Freemont AJ, Clarke NW, George NJ. (2002) Parathyroid hormone related peptide and receptor expression in paired primary prostate cancer and bone metastases. Br. J. Cancer 86:322–5.
Downey SE, et al. (1997) Expression of the receptor for parathyroid hormone-related protein in normal and malignant breast tissue. J. Pathol. 183:212–217.
Ghossein RA, Bhattacharya S. (2000) Molecular detection and characterisation of circulating tumour cells and micrometastases in solid tumours. Eur. J. Cancer 36:1681–94.
Katz AE, et al. (1994) Molecular staging of prostate cancer with the use of an enhanced reverse transcriptase-PCR assay. Urology 43:765–75.
Moreno JG, et al. (1992) Detection of hematogenous micrometastasis in patients with prostate cancer. Cancer Res. 52:6110–2.
Lembessis P, et al. (2007) Combined androgen blockade therapy can convert RT-PCR detection of prostate-specific antigen (PSA) and prostate-specific membrane antigen (PSMA) transcripts from positive to negative in the peripheral blood of patients with clinically localized prostate cancer and increase biochemical failure-free survival after curative therapy. Clin. Chem. Lab. Med. 45:1488–94.
Gomella LG, Raj GV, Moreno JG. (1997) Reverse transcriptase polymerase chain reaction for prostate specific antigen in the management of prostate cancer. J. Urol. 158:326–37.
Chelly J, Concordet JP, Kaplan JC, Kahn A. (1989) Illegitimate transcription: transcription of any gene in any cell type. Proc. Natl. Acad. Sci. U. S. A. 86:2617–21.
Fava TA, et al. (2001) Ectopic expression of guanylyl cyclase C in CD34+ progenitor cells in peripheral blood. J. Clin. Oncol. 19:3951–9.
Ghossein RA, et al. (1995) Detection of circulating tumor cells in patients with localized and metastatic prostatic carcinoma: clinical implications. J. Clin. Oncol. 13:1195–200.
Israeli RS, et al. (1994) Sensitive nested reverse transcription polymerase chain reaction detection of circulating prostatic tumor cells: comparison of prostate-specific membrane antigen and prostate-specific antigen-based assays. Cancer Res. 54:6306–10.
Sokoloff MH, et al. (1996) Quantitative polymerase chain reaction does not improve preoperative prostate cancer staging: a clinicopathological molecular analysis of 121 patients. J. Urol. 156:1560–6.
Gao CL, et al. (1999) Blinded evaluation of reverse transcriptase-polymerase chain reaction prostate-specific antigen peripheral blood assay for molecular staging of prostate cancer. Urology 53:714–21.
Gradilone A, et al. (2003) Detection of CK19, CK20 and EGFR mRNAs in peripheral blood of carcinoma patients: correlation with clinical stage of disease. Oncol. Rep. 10:217–22.
Smith MR, Biggar S, Hussain M. (1995) Prostate-specific antigen messenger RNA is expressed in non-prostate cells: implications for detection of micrometastases. Cancer Res. 55:2640–4.
Henke W, et al. (1997) Increased analytical sensitivity of RT-PCR of PSA mRNA decreases diagnostic specificity of detection of prostatic cells in blood. Int. J. Cancer 70:52–6.
Gala JL, et al. (1998) Expression of prostate-specific antigen and prostate-specific membrane antigen transcripts in blood cells: implications for the detection of hematogenous prostate cells and standardization. Clin. Chem. 44:472–81.
Cama C, et al. (1995) Molecular staging of prostate cancer; II: a comparison of the application of an enhanced reverse transcriptase polymerase chain reaction assay for prostate specific antigen versus prostate specific membrane antigen. J. Urol. 153:1373–8.
Lintula S, Stenman UH. (1997) The expression of prostate-specific membrane antigen in peripheral blood leukocytes. J. Urol. 157:1969–72.
Kaplan JC, Kahn A, Chelly J. (1992) Illegitimate transcription: its use in the study of inherited disease. Hum. Mutat. 1:357–60.
Eschwege P, et al. (1995) Haematogenous dissemination of prostatic epithelial cells during radical prostatectomy. Lancet 346:1528–30.
Oefelein MG, et al. (1996) Molecular detection of prostate epithelial cells from the surgical field and peripheral circulation during radical prostatectomy. J. Urol. 155:238–42.
Koutsilieris M, Lembessis P, Luu-The V, Sourla A. (1999) Repetitive and site-specific molecular staging of prostate cancer using nested reverse transcriptase polymerase chain reaction for prostate specific antigen and prostate specific membrane antigen. Clin. Exp. Metastasis 17:823–30.
Olsson CA, de Vries GM, Buttyan R, Katz AE. (1997) Reverse transcriptase-polymerase chain reaction assays for prostate cancer. Urol. Clin. North Am. 24:367–78.
Hara N, et al. (2001) Frequency of PSA-mRNA-bearing cells in the peripheral blood of patients after prostate biopsy. Br. J. Cancer 85:557–62.
Ellis WJ, et al. (1998) The value of a reverse transcriptase polymerase chain reaction assay in preoperative staging and followup of patients with prostate cancer. J. Urol. 159:1134–8.
Dumas F, Eschwege P, Loric S. (1997) Acute bacterial prostatitis induces hematogenous dissemination of prostate epithelial cells. Clin. Chem. 43:2007–8.
McIntyre IG, et al. (2000) Optimization of the reverse transcriptase polymerase chain reaction for the detection of circulating prostate cells. Br. J. Cancer 83:992–7.
Berteau P, et al. (1998) Influence of blood storage and sample processing on molecular detection of circulating prostate cells in cancer. Clin. Chem. 44:677–9.
Becker S, Becker-Pergola G, Fehm T, Wallwiener D, Solomayer EF. (2004) Time is an important factor when processing samples for the detection of disseminated tumor cells in blood/bone marrow by reverse transcription-PCR. Clin. Chem. 50:785–6.
Young CY, et al. (1991) Hormonal regulation of prostate-specific antigen messenger RNA in human prostatic adenocarcinoma cell line LNCaP. Cancer Res. 51:3748–52.
Qiu SD, et al. (1990) In situ hybridization of prostate-specific antigen mRNA in human prostate. J. Urol. 144:1550–6.
Grasso YZ, Gupta MK, Levin HS, Zippe CD, Klein EA. (1998) Combined nested RT-PCR assay for prostate-specific antigen and prostate-specific membrane antigen in prostate cancer patients: correlation with pathological stage. Cancer Res. 58:1456–9.
Shariat SF, et al. (2003) Early postoperative peripheral blood reverse transcription PCR assay for prostate-specific antigen is associated with prostate cancer progression in patients undergoing radical prostatectomy. Cancer Res. 63:5874–8.
Shariat SF, et al. (2002) Preoperative blood reverse transcriptase-PCR assays for prostate-specific antigen and human glandular kallikrein for prediction of prostate cancer progression after radical prostatectomy. Cancer Res. 62:5974–9.
Bianco FJ Jr, Powell IJ, Cher ML, Wood DP Jr. (2002) Presence of circulating prostate cancer cells in African American males adversely affects survival. Urol. Oncol. 7:147–52.
Kantoff PW, et al. (2001) Prognostic significance of reverse transcriptase polymerase chain reaction for prostate-specific antigen in men with hormone-refractory prostate cancer. J. Clin. Oncol. 19:3025–8.
Mejean A, et al. (2000) Detection of circulating prostate derived cells in patients with prostate adenocarcinoma is an independent risk factor for tumor recurrence. J. Urol. 163:2022–9.
Thiounn N, et al. (1997) Positive prostate-specific antigen circulating cells detected by reverse transcriptase-polymerase chain reaction does not imply the presence of prostatic micrometastases. Urology 50:245–50.
Martinez-Pineiro L, et al. (2003) Molecular staging of prostatic cancer with RT-PCR assay for prostate-specific antigen in peripheral blood and lymph nodes: comparison with standard histological staging and immunohistochemical assessment of occult regional lymph node metastases. Eur. Urol. 43:342–50.
Katz AE, et al. (1996) The role of the reverse-transcriptase polymerase chain reaction assay for prostate-specific antigen in the selection of patients for radical prostatectomy. Urol. Clin. North Am. 23:541–9.
Katz AE, et al. (1996) Molecular staging of genitourinary malignancies. Urology 47:948–58.
Olsson CA, et al. (1996) Preoperative reverse transcriptase polymerase chain reaction for prostate specific antigen predicts treatment failure following radical prostatectomy. J. Urol. 155:1557–62.
Mitsiades CS, et al. (2004) Molecular staging by RT-pCR analysis for PSA and PSMA in peripheral blood and bone marrow samples is an independent predictor of time to biochemical failure following radical prostatectomy for clinically localized prostate cancer. Clin. Exp. Metastasis 21:495–505.
Sourla A, et al. (2001) Conversion of nested reverse-transcriptase polymerase chain reaction from positive to negative status at peripheral blood during androgen ablation therapy is associated with long progression-free survival in stage D2 prostate cancer patients. Anticancer Res. 21:3565–70.
Olsson CA, et al. (1996) The use of RT-PCR for prostate-specific antigen assay to predict potential surgical failures before radical prostatectomy: molecular staging of prostate cancer. Br. J. Urol. 77:411–7.
Ghossein RA, et al. (1997) Prognostic significance of detection of prostate-specific antigen transcripts in the peripheral blood of patients with metastatic androgen-independent prostatic carcinoma. Urology 50:100–5.
Okegawa T, et al. (1998) Molecular staging of prostate cancer: comparison of nested reverse transcription polymerase chain reaction assay using prostate specific antigen versus prostate specific membrane antigen as primer. Int. J. Urol. 5:349–56.
Zhang Y, Zippe CD, Van Lente F, Klein EA, Gupta MK. (1997) Combined nested reverse transcription-PCR assay for prostate-specific antigen and prostate-specific membrane antigen in detecting circulating prostatic cells. Clin. Cancer Res. 3:1215–20.
Loric S, et al. (1995) Enhanced detection of hematogenous circulating prostatic cells in patients with prostate adenocarcinoma by using nested reverse transcription polymerase chain reaction assay based on prostate-specific membrane antigen. Clin. Chem. 41:1698–704.
Noguchi M, Miyajima J, Itoh K, Noda S. (1997) Detection of circulating tumor cells in patients with prostate cancer using prostate specific membrane-derived primers in the polymerase chain reaction. Int. J. Urol. 4:374–9.
Hara N, et al. (2002) Reverse transcription-polymerase chain reaction detection of prostate-specific antigen, prostate-specific membrane antigen, and prostate stem cell antigen in one milliliter of peripheral blood: value for the staging of prostate cancer. Clin. Cancer Res. 8:1794–9.
Han KR, et al. (2004) Prostate stem cell antigen expression is associated with Gleason score, seminal vesicle invasion and capsular invasion in prostate cancer. J. Urol. 171:1117–21.
Joung JY, et al. (2007) Reverse transcriptase-polymerase chain reaction and immunohisto-chemical studies for detection of prostate stem cell antigen expression in prostate cancer: potential value in molecular staging of prostate cancer. Int J. Urol. 14:635–43.
Dannull J, et al. (2000) Prostate stem cell antigen is a promising candidate for immunotherapy of advanced prostate cancer. Cancer Res. 60:5522–8.
Zhigang Z, Wenlu S. (2005) Complete androgen ablation suppresses prostate stem cell antigen (PSCA) mRNA expression in human prostate carcinoma. Prostate 65:299–305.
Kahn HJ, et al. (2000) RT-PCR amplification of CK19 mRNA in the blood of breast cancer patients: correlation with established prognostic parameters. Breast Cancer Res. Treat. 60:143–51.
Chen TF, et al. (2007) CK19 mRNAexpression measured by reverse-transcription polymerase chain reaction (RT-PCR) in the peripheral blood of patients with non-small cell lung cancer treated by chemo-radiation: an independent prognostic factor. Lung Cancer 56:105–14.
Stathopoulou A, et al. (2002) Molecular detection of cytokeratin-19-positive cells in the peripheral blood of patients with operable breast cancer: evaluation of their prognostic significance. J. Clin. Oncol. 20:3404–12.
Xenidis N, et al. (2007) Clinical relevance of circulating CK-19 mRNA-positive cells detected during the adjuvant tamoxifen treatment in patients with early breast cancer. Ann. Oncol. 18:1623–31.
Kaneda T, et al. (1998) Detection of urogenital malignant cells in the peripheral blood by nested RT-PCR using keratin 19 mRNA [in Japanese]. Nippon Hinyokika Gakkai Zasshi 89:33–42.
Tobias-Machado M, et al. (2005) Cytokeratin 19 expression by reverse transcriptase-polymerase chain reaction in the peripheral blood of prostate cancer patients. Tumori 91:248–52.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Panteleakou, Z., Lembessis, P., Sourla, A. et al. Detection of Circulating Tumor Cells in Prostate Cancer Patients: Methodological Pitfalls and Clinical Relevance. Mol Med 15, 101–114 (2009). https://doi.org/10.2119/molmed.2008.00116
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.2119/molmed.2008.00116