
Abstract
Background
Current breast cancer care is based on high-level evidence from randomized, controlled trials. Despite these data, there continues to be variability of breast cancer care, including overutilization of some tests and operations. To reduce overutilization, the American Board of Internal Medicine Choosing Wisely ® Campaign recommends that professional organizations provide patients and providers with a list of care practices that may not be necessary. Shared decision making regarding these services is encouraged.
Methods
The Patient Safety and Quality Committee of the American Society of Breast Surgeons (ASBrS) solicited candidate measures for the Choosing Wisely ® Campaign. The resulting list of “appropriateness” measures of care was ranked by a modified Delphi appropriateness methodology. The highest-ranked measures were submitted to and later approved by the ASBrS Board of Directors. They are listed below.
Results
(1) Don’t routinely order breast magnetic resonance imaging in new breast cancer patients. (2) Don’t routinely excise all the lymph nodes beneath the arm in patients having lumpectomy for breast cancer. (3) Don’t routinely order specialized tumor gene testing in all new breast cancer patients. (4) Don’t routinely reoperate on patients with invasive cancer if the cancer is close to the edge of the excised lumpectomy tissue. (5) Don’t routinely perform a double mastectomy in patients who have a single breast with cancer.
Conclusions
The ASBrS list for the Choosing Wisely ® campaign is easily accessible to breast cancer patients online. These measures provide surgeons and their patients with a starting point for shared decision making regarding potentially unnecessary testing and operations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
When surveyed, nearly three of four U.S. physicians say “doctors” order unnecessary tests and procedures. A similar proportion report that they themselves order unnecessary studies and interventions as often as once per week and that almost half of their patients request unnecessary tests on a weekly basis as well.1 These personal observations from “doctors” are accompanied by objective evidence of variation in the quality and value of care delivered to breast cancer patients.2 Both underutilization of evidence-based care and overutilization of unnecessary services have been documented.3–18 The former can lead to worse cancer outcomes, whereas the latter increases the cost of care without increasing value.16 To address these concerns across all specialties, the American Board of Internal Medicine (ABIM) Foundation launched an initiative to improve “appropriateness” of medical care in the United States. The Choosing Wisely ® campaign was launched in 2012, and more than 70 professional organizations have now contributed lists of appropriateness of care.1 The goals of this program are to “promote conversations between clinicians and patients by helping patients choose care that is supported by evidence and truly necessary.” The campaign empowers patients to engage their care providers in a thoughtful discussion of the benefits, risks, and effectiveness of the services offered to patients.
The inspiration for Choosing Wisely ® came from Howard Brody in 2010, when he challenged specialty societies to create “top 5” lists of tests and procedures that had not been shown to provide meaningful benefits to some patients for which they were ordered.19 Nine societies submitted lists in 2012. An increasing number have joined each year since that time. The purpose of the report described herein is to describe the American Society of Breast Surgeons (ASBrS) effort to identify, create, and endorse five measures of appropriate care.
Methods
The ASBrS has more than 3000 surgeon and associate members.20 After approval from its Board of Directors, their Quality Committee (QC) solicited potential “appropriateness measures” of breast care from the general and QC membership in 2014 and 2015. The QC then corresponded with the ABIM to establish the scope and clarity of the ABIM mission. The QC (13 members) were provided with the Choosing Wisely ® goals and existing “choices” previously recommended by other organizations for breast cancer (Table 1).21 Committee members received the following instructions to rank our final list of 38 choices:
-
1.
To rank for appropriateness and value of care; value to be characterized by both quality of care and “burdens of care.”22,23
-
2.
To rank based on the “importance” criteria of the National Quality Forum for quality measures—importance, scientific acceptability, feasibility, and usability.24
Two rounds of modified Delphi process ranking were performed electronically: March 2014 and July 2015.25,26 A complete Delphi process of ranking continues until all participants are in uniform agreement; our process of two rounds was therefore a “modified” Delphi process.
Each potential choice for a measure of appropriateness was ranked on a scale of 1 (no value or importance) to 9 (highest possible value or importance). After the first round, a spreadsheet of median scores was provided to committee members, allowing opportunity for participants to lobby for either increasing or decreasing a choice’s “rank.”
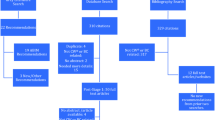
The final voting panel included nine QC members. Appropriateness of a measure is achieved in a panel of nine with a median score of 7–9, if there is no major “disagreement” between panelists, as defined by fewer than three panelists scoring the measure from 1 to 3.25 There were 16 choices deemed appropriate by this method. The top 5 choices had median ranks of 8 or 9. Four of these top 5 choices were already included in the Choosing Wisely ® Campaign from other organizations, based on ABIM policy, and these were excluded from our list. Their domains of appropriateness were to encourage needle biopsy as the preferred method of diagnosis, limit routine mammography of reconstructed breasts after mastectomy and discourage the use of pre- and postoperative systemic imaging in asymptomatic patients with breast cancer (Table 1). To finish our list of five, we used the next highest-ranked choices. The final list of five choices was then formatted in the style specified by the ABIM. The list was submitted to the ABIM and a manuscript was drafted and later approved by the ASBrS Research Committee and Board of Directors on April 12, 2016.
Results
Five Tests or Interventions Physicians and Patients Should Question
-
1.
Don’t routinely order breast magnetic resonance imaging (MRI) in new breast cancer patients.27–34
After a new diagnosis of breast cancer, breast MRI can be useful in selected patients, to aid treatment decisions, including but not limited to those with occult breast cancer presenting with axillary metastases or patients with genetic mutations predisposing to increased breast cancer risk. However, there is a lack of evidence that routine use of MRI lessens cancer recurrence, death from cancer, or the need for reoperation after partial breast removal (lumpectomy) surgery. The routine use of MRI is associated with an increased need for subsequent breast biopsy procedures, delays in time to treatment, and higher cost of care. In addition, more patients may undergo mastectomy with routine use of MRI due to MRI detection of findings of uncertain significance that result in increased patient anxiety and their subsequent decision to undergo mastectomy even without proof of other cancer(s).
-
2.
Don’t routinely excise all the lymph nodes beneath the arm in patients having partial breast removal (lumpectomy) for breast cancer when only one or two contain cancer.28,35,36
After a new diagnosis of invasive breast cancer, most patients undergoing partial breast removal (lumpectomy) benefit from a “sentinel node (SN) mapping surgery”—a procedure that removes a small number of lymph nodes beneath the arm that drains the known cancer. In the past, patients found to have cancer in any SN underwent extra surgery to remove more nodes. Recent evidence suggests that further node surgery is not necessary in patients with cancer found in fewer than three SN, if the patient receives other recommended cancer treatments.
-
3.
Don’t routinely order specialized tumor gene testing in all new breast cancer patients.28,37–41
There are multiple, new, tumor “multigene signature” tests that provide selected breast cancer patients with information about their risk of distant cancer recurrence, dying of cancer, or the likelihood that they will benefit from chemotherapy. These tests are helpful in selected patients, including those with early-stage, hormone-receptor–positive cancers with “low” scores on 21 gene recurrence testing, who can safely omit chemotherapy. There is no evidence that these types of tests should be used routinely. They should not be performed in patients who indicate that the test results would not change their choice of treatment.
-
4.
Don’t routinely reoperate on patients if the cancer is close to the edge of the excised lumpectomy tissue.28,42–45
Patients undergoing partial breast removal (lumpectomy) of the breast and whole breast radiation for invasive cancer benefit from reoperation to excise more breast tissue if microscopic review of the lumpectomy breast tissue indicates that cancer cells are present at the tissue edge. However, if cancer cells are close to the edge, but not at the actual edge, then recent evidence indicates that reoperation is not mandatory.
-
5.
Don’t routinely perform a double mastectomy in patients who have a single breast with cancer.46–53
After a new diagnosis of breast cancer in a single breast, many patients desire removal of both breasts, believing their cancer risk in the other breast is high and their cancer cure rate will be improved with double mastectomy. Double mastectomy should not be routinely performed in average-risk patients until they have been provided with adequate understandable information about the generally low risk that they will develop cancer in the other breast and the minimal effectiveness, if any, of double mastectomy to improve their life expectancy or survival from breast cancer.
Discussion
The Choosing Wisely ® campaign was launched to advance the patient-provider dialogue such that unnecessary medical tests, treatments, and procedures would be used less often.1 To accomplish this, the ABIM recommended that professional organizations provide the ABIM with “five things providers and patients should question.” 1 Conceptually, the provider stakeholders create lists of domains of care decisions intended to spur conversations between providers, patients, and payers about appropriate care, resulting in less “waste.”54,55 This process is in alignment with widely accepted principles to increase the “value” of healthcare, by lowering cost, promoting patient engagement, and creating a result that is measurable.56 If initiatives to increase adherence to Choosing Wisely ® choices are successful, then the national cost of healthcare is likely to decrease. In a cohort of 22,000 patients enrolled in a single insurance plan in the state of Washington, an estimated cost savings of $29 million was achieved through increased adherence to five Choosing Wisely ® choices.10
After first recognizing and then taking ownership of the effort to reduce overutilization of services, the ASBrS developed a list of measures that were intended to improve appropriateness of testing and surgery in patients with breast cancer. Measures were chosen that were deemed important by the criteria of the NQF for quality measure development.24 These criteria included but were not limited to scientific support, evidence of variability of care, and feasibility of use. In the ABIM campaign, all measure choices should be usable, because they only require the provider to discuss the measure with the patient. Patient use and understanding of the Choosing Wisely ® choices also is facilitated by the ABIM’s required formatting to include simple, understandable, and brief declarative statements, usually beginning the statement with “Don’t.”
Other organizations that care for patients with breast cancer have submitted their Choosing Wisely ® Lists to the ABIM (Table 1).21 All used different methods for developing and prioritizing their lists. None used our modified Delphi ranking process; yet, independent of these other organizations, 4 of our 5 top choices were already selected by them. This concordance between developers using different methodologies supports the importance and potential impact of these specific measures.
A systematic review of the literature for each of our Choosing Wisely ® choices is not the intent of this report. Background information, comprehensive reviews, and evidence-based support for each of our measures is referenced. It is important to note that our “choices” are not meant to infer that the test or procedure endorsed in our list is a “never should occur” event akin to “wrong site” surgery. For example, we recommend against “routine MRI” in new breast cancer patients, but MRI imaging can be useful in selected patients to aid treatment decisions, including but not limited to those with occult breast cancer presenting with Paget’s disease of the nipple or with axillary metastases or patients with mutations predisposing to increased breast cancer risk.27 Rather, the services listed should be discussed with patients and shared decision making should occur. There may be circumstances in which best, highest-quality care is different from the Choosing Wisely ® statement on a particular topic. Moreover, there are no benchmarks established for what level of compliance with our statements would be desirable. Three of our “choices”—on MRI usage, SN surgery, and margin status decisions—have a high level of evidence supporting them based on randomized, controlled trials and/or meta-analyses.27–36,42–45 For the other two choices—contralateral prophylactic mastectomy (CPM) and tumor multigene signature testing—there is evidence of increasing utilization that is not always accompanied by evidence of improving patient-reported and/or clinical outcomes.28,37–41,46–53
CPM rates have increased during the past decade.46–49 In average-risk patients, there is a lack of convincing evidence that CPM improves cancer-specific survival. These operations often are driven by patient requests for risk reduction or symmetry. Many patients with unilateral breast cancer request a CPM, because they perceive that their cancer risk in the other breast is higher than their actual risk.51 The inclusion of CPM in the ASBrS choices for Choosing Wisely ® does not mean that the ASBrS endorses a policy of never performing it. We are simply recommending full education regarding its risks and benefits, emphasizing the importance of a decision-making process shared by patients and providers. A full discussion of CPM, its indications and contraindications, is beyond the scope of this report, but the ASBrS held a consensus conference in 2016 to further characterize the reasons to consider or discourage CPM (J. Boughey, Program Director for the 2016 Annual Meeting of the American Society of Breast Surgeons, personal communication, April 12, 2016).
Tumor multigene signature panels that are prognostic for risk of distant recurrence and overall survival and predictive of benefit of chemotherapy are increasingly utilized after new breast cancers are diagnosed.39–41 In select patients with invasive cancer, the use of a “validated” tumor multigene signature testing panel is appropriate if the patient’s tumor characteristics were consistent with those used in the panel validation studies and if the results of testing would affect the patient’s decisions regarding adjuvant treatment. In this scenario, the test identifies patients in whom chemotherapy can be omitted, without harm to distant recurrence risk or overall survival.39,41 New and emerging tumor multigene panels hope to do the same, but not all have yet been validated. Panels also are available for patients with ductal carcinoma in situ.57 Industry, patients, and patients’ families may pressure surgeons to order these tests to help direct therapy. As a result, there is risk of overutilization of testing without concomitant patient benefit if validated tests are ordered for patient subgroups not included in the validation studies or if a patient has already decided to omit a specific adjuvant therapy due to age, comorbidities, or personal reasons.
The Choosing Wisely ® campaign is still in its relative infancy, having been in existence for less than 6 years. Enthusiasm for its potential impact on improving appropriate care and reducing waste is evidenced by the submission of appropriateness measures by more than 70 professional societies, increasing organizational participation each year, and the rapid emergence of research projects and publications measuring adherence to the Choosing Wisely ® choices. Many organizations and regional quality collaboratives are now auditing compliance with the Choosing Wisely ® choices, using them as a surrogate measure of quality.58 Most Choosing Wisely ® choices also could be crafted into metrics of value or efficiency. Although results are preliminary, some organizations have already implemented action plans to address compliance variability.59
We hope that our society’s endorsement of five new choices for the Choosing Wisely ® campaign will contribute to increased delivery of appropriate care and decreased overall cost of care for breast cancer patients. Plans to develop five additional measures of appropriateness in the management of benign breast disease are anticipated.
References
The American Board of Internal Medicine Foundation: Choosing Wisely® Campaign. http://www.choosingwisely.org/about-us/research-report/ (2015). Accessed 4 Dec 2015.
Hassett MJ, Neville BA, Weeks JC. The relationship between quality, spending and outcomes among women with breast cancer. J Natl Cancer Inst. 2014; doi:10.1093/jnci/dju242.
American Society of Clinical Oncology (ASCO). The state of cancer care in America, 2015: a report by the American Society of Clinical Oncology. J Oncol Pract. 2015;11(2):79–113.
Hewitt M, Simone JV. Ensuring quality cancer care. Washington, DC: The National Academies Press, 1999.
Institute of Medicine. Delivering high-quality cancer care: charting a new course for a system in crisis. Washington, DC: The National Academies Press, 2013. doi:10.17226/18359.
Malin JL, Schneider EC, Epstein AM, Adams J, Emanuel EJ, Kahn KL. Results of the National Initiative for Cancer Care Quality: how can we improve the quality of cancer care in the United States? J Clin Oncol. 2006;24:626–34.
Greenberg CC, Lipsitz SR, Neville B, et al. Receipt of appropriate surgical care for Medicare beneficiaries with cancer. Arch Surg. 2011;146(10):1128–34. doi:10.1001/archsurg.2011.141.
Cheng SH, Wang CJ, Lin JL, et al. Adherence to quality indicators and survival in patients with breast cancer. Med Care. 2009;47(2):217–25. doi:10.1097/MLR.0b013e3181893c4a.
Makarov DV, Soulos PR, Gold HT, et al. Regional-level correlations in inappropriate imaging rates for prostate and breast cancers: potential implications for the choosing wisely campaign. JAMA Oncol. 2015;1(2):185–94. doi:10.1001/jamaoncol.2015.37.
Ramsey SD, Fedorenko C, Chauhan R, et al. Baseline estimates of adherence to American Society of Clinical Oncology/American Board of Internal Medicine Choosing Wisely® initiative among patients with cancer enrolled with a large regional commercial health insurer. J Oncol Pract. 2015;11(4):338–43. doi:10.1200/JOP.2014.002717.
Wilke LG, Ballman KV, McCall LM, et al. Adherence to the National Quality Forum (NQF) breast cancer measures within cancer clinical trials: a review from ACOSOG Z0010. Ann Surg Oncol. 2010;17(8):1989–94. doi:10.1245/s10434-010-0980-9.
Jagsi R, Griffith KA, Heimburger D, et al. Choosing wisely? Patterns and correlates of the use of hypofractionated whole-breast radiation therapy in the state of Michigan. Int J Radiat Oncol Biol Phys. 2014;90(5):1010–6. doi:10.1016/j.ijrobp.2014.09.027.
Hahn EE, Tang T, Lee JS, et al. Use of imaging for staging of early-stage breast cancer in two integrated health care systems: adherence with a choosing wisely recommendation. J Oncol Pract. 2015;11(3):e320–8. doi:10.1200/JOP.2014.002998.
Crivello ML, Ruth K, Sigurdson ER, et al. Advanced imaging modalities in early stage breast cancer: preoperative use in the United States Medicare population. Ann Surg Oncol. 2013;20:102–10.
In H, Jiang W, Lipsitz SR, et al. Variation in the utilization of reconstruction following mastectomy in elderly women. Ann Surg Oncol. 2013;20:1872–9.
Erickson FJ, Velasco JM, Hieken TJ. Adverse outcomes associated with noncompliance with melanoma treatment guidelines. Ann Surg Oncol. 2008;15:2395–402.
The Darthmouth Institute. The Dartmouth Atlas of Health Care. www.dartmouthatlas.org (2015). Accessed 4 Dec 2015.
The Commonwealth Fund report on state health system scorecards. http://www.commonwealthfund.org/publications/press-releases/2015/dec/state-scorecard. Accessed 9 Dec 2015.
Brody H. Medicine’s ethical responsibility for health care reform—the Top Five list. N Engl J Med. 2010;362:283–5. doi:10.1056/NEJMp0911423.
The American Society of Breast Surgeons. https://www.breastsurgeons.org/new_layout/index.php (2014). Accessed 4 Dec 2015.
Choosing Wisely ®. Clinician list of “breast” choices. http://www.choosingwisely.org/clinician-lists/ (2015). Accessed 4 Dec 2015.
Berry, Leonard L. Discovering the Soul of Service: the nine drivers of sustainable business success. New York: The Free Press, a Division of Simon and Schuster, 1999.
Porter ME. What is value in health care? N Engl J Med. 2010;363:2477–81.
The National Quality Forum. ABC’s of measurement. http://www.qualityforum.org/Measuring_Performance/ABCs_of_Measurement.aspx (2015). Accessed 4 Dec 2015.
Fitch K, Bernstein SJ, Aguilar MD, et al. The Rand/UCLA appropriateness method user’s manual. Arlington: RAND, 2001.
Bilimoria KY, Raval MV, Bentrem DJ, Wayne JD, Balch CM, Ko CY. National assessment of melanoma care using formally developed quality indicators. J Clin Oncol. 2009;27(32):5445–51.
American Society of Breast Surgeons. Position statement on breast MRI. https://www.breastsurgeons.org/statements/index.php (2010). Accessed 2 Dec 2015.
National Comprehensive Cancer Network. Clinical Practice Guidelines for Breast Cancer, Version 3. http://www.nccn.org/ (2015). Accessed 2 Dec 2015.
Pilewskie M, Morrow M. Applications for breast magnetic resonance imaging. Surg Oncol Clin N Am. 2014;23(3):431–49. doi:10.1016/j.soc.2014.03.001.
Houssami N, Turner R, Macaskill P, et al. An individual person data meta-analysis of preoperative magnetic resonance imaging and breast cancer recurrence. J Clin Oncol. 2014;32(5):392–401.
Houssami N, Turner R, Morrow M. Preoperative magnetic resonance imaging in breast cancer: meta-analysis of surgical outcomes. Ann Surg. 2013;257(2):249–55. doi:10.1097/SLA.0b013e31827a8d17.
Peters NH, van Esser S, van den Bosch MA, et al. Preoperative MRI and surgical management in patients with nonpalpable breast cancer: the MONET—randomized controlled trial. Eur J Cancer. 2011;47(6):879–86.
Turnbull L, Brown S, Harvey I, et al. Comparative effectiveness of MRI in breast cancer (COMICE) trial: a randomised controlled trial. Lancet. 2010;375(9714):563–71.
Houssami N, Ciatto S, Macaskill P, et al. Accuracy and surgical impact of magnetic resonance imaging in breast cancer staging: systematic review and metaanalysis in detection of multifocal and multicentric cancer. J Clin Oncol. 2008;26(19):3248–58.
American Society of Breast Surgeons. Position statement on management of axillary lymph nodes. https://www.breastsurgeons.org/statements/index.php (2011). Accessed 2 Dec 2015.
Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis. A randomized clinical trial. Clinicaltrials.gov, Identifier: NCT00003855. JAMA. 2011;305:569–75.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351(27):2817–26.
Dowsett M, Cuzick J, Wale C, et al. Prediction of risk of distant recurrence using the 21-gene recurrence score in node negative and node-positive postmenopausal patients with breast cancer treated with anastrozole or tamoxifen: a TransATAC study. J Clin Oncol. 2010;28(11):1829–34.
Augustovski F, Soto N, Caporale J, et al. Decision-making impact on adjuvant chemotherapy allocation in early node-negative breast cancer with a 21-gene assay: systematic review and metaanalysis. Breast Cancer Res Treat. 2015;152(3):611–25. doi:10.1007/s10549-015-3483-3.
Carlson JJ, Roth JA. The impact of the Oncotype Dx breast cancer assay in clinical practice: a systematic review and meta-analysis. Breast Cancer Res Treat. 2013;141(1):13-22. doi:10.1007/s10549-013-2666-z.
Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373(21):2005–14. doi:10.1056/NEJMoa1510764.
Moran MS, Schnitt SJ, Giuliano AE, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole breast irradiation in stages I and II invasive breast cancer. Ann Surg Oncol. 2014;21:704–16.
American Society of Breast Surgeons. Position statement on lumpectomy margins. https://www.breastsurgeons.org/statements/index.php (2013). Accessed 2 Dec 2015.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21:717–30.
National Comprehensive Cancer Network. Clinical Practice Guidelines for Breast Cancer, Version 1. http://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (2016). Accessed 15 Dec 2015.
Angelos P, Bedrosian I, Euhus DM, Herrmann VM, Katz SJ, Pusic A. Contralateral prophylactic mastectomy: challenging considerations for the surgeon. Ann Surg Oncol. 2015;22(10):3208–12. doi:10.1245/s10434-015-4758-y.
Grimmer L, Liederbach E, Velasco J, Pesce C, Wang CH, Yao K. Variation in contralateral prophylactic mastectomy rates according to racial groups in young women with breast cancer, 1998 to 2011: a report from the National Cancer Data Base. J Am Coll Surg. 2015;221(1):187–96. doi:10.1016/j.jamcollsurg.2015.03.033.
Pesce CE, Liederbach E, Czechura T, Winchester DJ, Yao K. Changing surgical trends in young patients with early stage breast cancer, 2003 to 2010: a report from the National Cancer Data Base. J Am Coll Surg. 2014;219(1):19-28. doi:10.1016/j.jamcollsurg.2014.03.043.
Fayanju OM, Stoll CR, Fowler S, Colditz GA, Margenthaler JA. Contralateral prophylactic mastectomy after unilateral breast cancer: a systematic review and meta-analysis. Ann Surg. 2014;260(6):1000-10. doi:10.1097/SLA.0000000000000769; Review.
Giuliano AE, Boolbol S, Degnim AC, et al. Society of Surgical Oncology: position statement on prophylactic mastectomy. Ann Surg Oncol. 2007;14:2425–7.
Portschy PR, Abbott AM, Burke EE, et al. Perceptions of contralateral breast cancer risk: a prospective, longitudinal study. Ann Surg Oncol. 2015;22:3846–52.
Portschy PR, Kuntz KM, Tuttle TM. Survival outcomes after contralateral prophylactic mastectomy: a decision analysis. J Natl Cancer Inst. 2014;doi:10.1093/jnci/dju160.
Mutter RW, Frost MH, Hoskin TL, Johnson JL, Hartmann LC, Boughey JC. Breast cancer after prophylactic mastectomy (bilateral or contralateral prophylactic mastectomy), a clinical entity: presentation, management, and outcomes. Breast Cancer Res Treat. 2015;153(1):183–90. doi:10.1007/s10549-015-3515-z.
The American Board of Internal Medicine Foundation. Choosing Wisely Campaign: Collaborative activities of the ABIM. http://www.choosingwisely.org/in-action/ (2015). Accessed 4 Dec 2015.
The American Board of Internal Medicine Foundation. Choosing Wisely ® Campaign: Choosing Wisely Toolkits. http://www.nbch.org/choosing-wisely-employer-toolkit (2015). Accessed 7 Dec 2015.
Fayanju MO, Mayo TL, Spinks TE, et al. Value-based breast cancer care: a multidisciplinary approach for defining patient-centered outcomes. Ann Surg Oncol. 2016. doi:10.1245/s10434-016-5184-5.
Rakovitch E, Nofech-Mozes S, Hanna W, et al. A population-based validation study of the DCIS score predicting recurrence risk in individuals treated by breast-conserving surgery alone. Breast Cancer Res Treat. 2015;152(2):389–98. doi:10.1007/s10549-015-3464-6.
Wisconsin Collaborative for Healthcare Quality. WCHQ to Partner with Froedtert & the Medical College of Wisconsin and Monroe Clinic on New ABIM Foundation Grant Focusing on Reducing Overuse of Tests and Treatments Identified by Choosing Wisely ® Campaign. http://www.wchq.org/news/documents/choosing_wisely_062215.pdf (2015). Accessed 7 Dec 2015.
Gebhardt BJ, Rajagopalan MS, Gill BS, et al. Impact of dynamic changes to a bone metastases pathway in a large, integrated, National Cancer Institute-designated comprehensive cancer center network. Pract Radiat Oncol. 2015;5(6):398–405. doi:10.1016/j.prro.2015.06.013.
Acknowledgments
The authors acknowledge the support of Sharon Grutman for her assistance with committee communication and ranking methodology and Choua Vang for manuscript assistance.
Disclosures
Jeffrey Landercasper-none. General conflict of interest disclosures for the ASBrS Patient Safety and Quality Committee (PSQC), Research Committee and the ASBrS Board of Directors are on file with the ASBrS staff. The Chair of the PSQC reviewed, then asked for updates of COI during the ranking process and after its completion and determined there were no COI for the process and result.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Landercasper, J., Bailey, L., Berry, T.S. et al. Measures of Appropriateness and Value for Breast Surgeons and Their Patients: The American Society of Breast Surgeons Choosing Wisely ® Initiative. Ann Surg Oncol 23, 3112–3118 (2016). https://doi.org/10.1245/s10434-016-5327-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5327-8