
Abstract
The present study evaluated the effect of different configuration setups of the Flow-Through Cell (USP IV) dissolution tester in developing in vitro–in vivo correlation (IVIVC). A Biopharmaceutics Classification System (BCS) Class I Diltiazem (DTZ), formulated in extended-release (ER) gel-matrix system, was employed for this purpose. The study also assessed the validity and predictability of IVIVC employing both deconvolution- and convolution-based approaches. In vitro release was conducted in USP IV as open- or closed-loop setups, while the pharmacokinetic (PK) data were obtained from a previous fasted-state cross-over study conducted on 8 healthy male volunteers, after oral administration of ER matrix tablets against market product (Tildiem Retard® 90 mg). PK parameters (Cmax, AUC0-t and AUC0-∞) were predicted, and compared with actual data to establish the strength of correlation models. Results showed that DTZ release from ER products was influenced by operating the FTC in different configuration-setups, where ≥ 75% of labeled DTZ was released after 6 h and 12 h using the open- and closed-loop settings, respectively. Correlation between fraction-dissolved versus fraction-absorbed for both ER products displayed linear relation upon employing FTC open-loop setup. Convolution-based approach was more discriminative in predicting DTZ in vivo PK parameters with a minimal prediction error, compared to deconvolution-based approach. A successful trial to predict DTZ PKs from individual in vitro data performed in USP IV dissolution model was established, employing convolution technique. Basic principle of the convolution approach provides a simple and practical method for developing IVIVC, hence could be utilized for other BCS Class I extended-release drug products.
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Development of an in vitro/in vivo correlation (IVIVC) model is essential for assessing in vivo relevance of a given in vitro dissolution data as well as exploiting the ability of dissolution data to address regulatory bioequivalence concerns. Establishment of IVIVC is usually a complex process as the time-course of in vivo drug release is an irregular, multi-phasic process that cannot be precisely described. As stated by US- FDA, IVIVC allows predictive mathematical modeling for the relation between a given in vitro property of dosage form and its corresponding in vivo response [1]. The international regulatory guidelines describe internal and external methods for validating an IVIVC along with their extrapolative criteria to assess such validity [2]. Once the predictability of IVIVC was established, hence, the in vitro dissolution acts as a surrogate for future in vivo trials. Assessment of IVIVC is an essential requirement for the development of extended-release (ER) dosage forms and is nowadays US-FDA regulated [3].
Several correlation levels are available, including Level A, B, C, and multiple Level C. Level A provides the most advantageous level of correlation, as it signifies point-to-point relationship between drug in vitro dissolution against its in vivo input [2, 3]. Level C correlation allows single time-point relation between any dissolution parameter to an equivalent PK one. Multiple level C provides correlation between multiple PK parameters and multiple dissolution at several time-points along the course of dissolution [3].
Various approaches were described for evaluating IVIVC, including the deconvolution analysis using the traditional Wagner Nelson (WN) [4] and Loo-Riegelman [5]. Model independent methods based on numerical deconvolution were also developed as a common approach for calculating drug input rates [6,7,8]. Deconvolution represents a classical two-stage based approach where a fraction dissolved, obtained from the in vitro dissolution data, is used together with its corresponding in vivo fraction absorbed, derived by the deconvolution of observed plasma concentrations [2]. Although, deconvolution approach is numerously cited in literature, yet, it suffers from certain limitations, for example, deriving of an in vivo dissolution data from plasma profile requires elaborative mathematical and/or computing experience. Also, this approach requires blood data for the test products to correlate it to in vitro data; hence, it might not be appropriate for the product development phase. The deconvolution model is usually suited for the method and/or apparatus development phase [9].
The convolution-based approach provides a one-stage method, where the in vitro dissolution data is directly used to derive plasma drug concentrations, using PK parameters easily extracted from literature [9]. Employment of convolution-based approach to predict IVIVC is less commonly cited in literature, although it provides simple method for product evaluation as well as addresses most of the limitations associated with deconvolution method [9].
Dissolution testing is a crucial requirement for development and quality control assessment of solid dosage forms. Appropriate selection of a dissolution model is essential to establish a proper method to discriminate between products with potential bioavailability problems [10]. The flow through cell (FTC) dissolution tester (USP IV) provides several advantages compared to conventional dissolution testers; i.e., USP apparatus I and II [10]. FTC apparatus is operated as either a closed-loop setup, where fixed volume of the medium is recycled, or an open-loop setup, where fresh solvent is continuously pumped through the cell containing the dosage form, which in turn, allows possible sink conditions for longer periods. Intraluminal hydrodynamics are powerfully simulated in the FTC, with flexible change of medium and flow rate during the run [11]. Evaluation of ER tablets, microspheres, nano-suspensions, and implants exhibited appropriate results when evaluated using the FTC [12].
Diltiazem hydrochloride (DTZ), a calcium channel blocker, is generally used in the treatment of various cardiovascular disorders, particularly angina pectoris, systemic hypertension, and supraventricular tachycardia [13]. It is subjected to an extensive first pass metabolism, with 2–4% of unchanged form excreted in urine. DTZ exhibits short biological half-life of about 3.2 ± 1.3 h after oral dose of 60 mg [14], with a rapid elimination. Oral bioavailability (F) of DTZ is reported to be 25–74% (mean 42% ± 18%) in humans [15]. DTZ is a ‘Class I’ drug, according to the Biopharmaceutics Classification System (BCS), with high solubility/high permeability characteristics [16]. Development of DTZ ER formulations is frequently recommended due to its low bioavailability and short biological half-life, which favor an extended clinical pattern and reduced dosing frequency [17,18,19].
Although, numerous ER formulations were previously reported for DTZ, yet limited examples of validated IVIVC models were presented, which might be due to being a highly variable drug, with irregular absorption and extensive first pass elimination; hence, challenges usually arise in the development and/or validation of a correlation for such ER formulations [20, 21]. Most of the published IVIVC models assessed for DTZ were employed using the deconvolution approach, which necessitate the presence of drug in vivo plasma concentration–time data to assess such correlation [22,23,24,25,26]. Also, the in vitro testings of the aforementioned IVIVCs were carried out using the traditional paddle method (USP II) [27].
In a previous study, in vitro release and in vivo bioavailability of a newly developed DTZ ER gel-matrix tablets were compared to, the innovator product (Tildiem Retard ® 90 mg, Sanofi Winthrop Industries, France) [28]. The in vivo pilot study was carried-out as an oral dose (2 × 90 mg) of each product in a two-period, two-treatment crossover design in 8 healthy volunteers under fasting conditions. The above-mentioned gel-matrix tablets allowed extended DTZ release for up to 8 h with excellent shelf-life stability for 5 years [29]. The PK results of both gel-matrix tablets and Tildiem Retard ® showed no statistically significant differences regarding Cmax, AUC0–48 and AUC0–∞, although DTZ-plasma profiles were different between the two tested products [28].
The purpose of the present study is to assess the IVIVC for two DTZ ER products; a previously developed gel-matrix tablet against the market product, Tildiem Retard®. The role of employing different configuration setups of the Flow-Through Cell (USP IV) dissolution tester will be evaluated, to come to terms which configuration setup is more appropriate to correlate with the in vivo data.
Materials and Methods
Materials
Diltiazem hydrochloride (DTZ) was purchased from EIPICO Pharmaceutical, Egypt. Polyethylene oxide (PEO) of molecular weight 900,000 (Aldrich, Germany), microcrystalline cellulose (Avicel PH-101, Fluka, Switzerland), and potassium chloride (KCl, Winlab, UK) were used for preparation of ER gel-matrix tablets. Ultra-purified water (Millipore Corp., MA, USA) was used as dissolution medium. Chemicals used otherwise were of analytical grade.
Batches Used in the Study
DTZ ER reference product, Tildiem Retard® 90 mg (Sanofi Winthrop Industries, France, Batch no. 11KVWA), was used as the bioavailability batch (batch A-Ref).
Methods
Preparation of ER Formulation of DTZ
The composition of DTZ ER gel-matrix tablets used in this study was shown in Table I. Direct compression method was used for preparation of the gel-matrix tablets employing a Single Punch Press Tablet Machine (Stokes-Merrill Model 511–7-A, USA) at 14,710-N compression force, fitted with a 13-mm flat-faced punch. Drug, polymer, and electrolyte were screened through sieve # 25, blended with avicel, magnesium stearate, and talc in a polyethylene bag. Round tablets were produced, each containing 90 mg of DTZ. Physical examinations of tablets, including luster, appearance, weight variation, diameter, thickness, hardness, and content uniformity, were checked and all were in acceptable range. The prepared gel-matrix tablets were named Batch B-Test.
In Vitro Release Studies
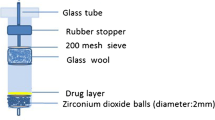
Dissolution studies of DTZ from reference and test batches, each equivalent to 2 × 90 mg DTZ, were performed using the Flow-Through Cell (FTC) dissolution tester (USP # IV, a Dissotest CE-6 equipped with a CY 7–50 piston pump, Sotax, Switzerland). A built-in filtration system with 0.7-μm Whatman glass microfiber (GF/F and GF/D) and glass wool was used throughout the study. Tested tablets were placed in the 22.6-mm diameter cell according to the design described previously [29]. The dissolution medium (ultrapure water of pH 6.4, kept at 37°C) was de-aerated and filtered on Millipore filter (0.45 um), then pumped at a turbulent flow rate of 8 ± 0.2 ml/min. The sampling times were 0.5, 1, 1.5, 2, 3, 4, 6, 8, 9, and 12 h. The amount of DTZ released was measured by UV spectrophotometry using (UV–Visible spectrophotometer, Beckman, DU-650, USA) at 235 nm against water of pH 6.4 as blank. Release studies were conducted in triplicate, and the mean values were plotted versus time.
The FTC dissolution system was operated as follows:
Open-Loop Setup
Fresh dissolution medium was continuously pumped through the system, to ensure proper sink conditions. Volume fractions were collected at the specified time intervals and measured spectrophotometrically.
Closed-Loop Setup
Constant volume of dissolution medium was recycled (900 mL), and a total of 10 mL samples were collected at each time interval and replaced by the same volume of the fresh dissolution medium.
Comparison of Release Profiles of Studied Batches
Dissolution Efficiency
The dissolution efficiency (DE) was obtained from the ratio between the areas under DTZ release curve up to time t (12 h), in relation to the total area of the rectangle, which refers to 100% dissolution in the same time-frame [30, 31]. The DE values were presented in Eq. (1):
Difference Factor (f1)
Difference factor evaluates the percentage difference between the two release curves, according to Eq. (2):
where, n defines the number of time points and Rt and Tt refer to the release value of the reference and test batches at time t, respectively. f1 values ranging from 0 to 15 indicate similar release profiles, while value > 15 indicate dissimilar profiles [32, 33].
Similarity Factor (f2)
The similarity factor, which indicates the closeness between the two profiles, was calculated according to Eq. (3):
Mean Dissolution Time
MDT was calculated, as described by Costa & Lobo, 2001 [32], according to Eq. (4):
where j is the sample number, n is the number of release sample times, t^j is the time at midpoint between tj and tj−1 and ΔMj is the additional amount of drug released between tj and tj−1.
Student’s t-test was selected for comparison between the two groups, for MDT and % DE12h, where statistical significant was considered at p ≤ 0.05. Data analysis was calculated using SPSS software (Version 17.0).
In Vivo Pharmacokinetic Study
The PK data of DTZ plasma concentrations versus time profiles for the reference product (Batch A-Ref) and the prepared ER gel-matrix tablet (Batch B-Test) were obtained from a previous fasted state pilot PK study conducted on 8 healthy male volunteers [28]. The study was performed as a randomized single dose (180 mg DTZ), two treatment (T and R), two-period, two-sequence, crossover design under fasting conditions with 1 week wash-out period between the two treatments.
Development of IVIVC
IVIVC for the reference product (Batch A-Ref) and the prepared ER gel-matrix tablet (Batch B-Test) was established using the Wagner – Nelson (WN) approach [34]. The plasma concentration versus time profiles for each batch obtained from the previous in vivo pilot study [28] was transformed to an in vivo oral fraction absorbed (Fabs), according to WN Eq. (5):
where, Fα(t) represents fraction of drug absorbed at time t, At is the amount of drug absorbed at time t, A∞ is amount of drug absorbed at infinite time, Ct represents the concentration at any time point and Ke is the elimination rate constant. AUC0-t equals to the area under the plasma concentration time curve from time zero to time t and AUC0-∞ is the total area under the plasma concentration versus time curve. Values of Ke, AUC0-all and AUC0-∞ were extracted from Emara et al., 2018 [28].
Also, the fraction dissolved (Fdiss) for each product in the FTC operated either as open or closed loop setups were evaluated, to determine which configuration provided the best correlation with the in vivo results. Hence, IVIVC model was plotted between the DTZ in vitro fraction released (Fdiss) from each batch against the in vivo fraction absorbed (Fabs). The relationship between Fabs and Fdiss was described by linear regression and presented by R2, slope, and intercept values [35].
Prediction of In Vivo Plasma Data
Two different approaches were used for prediction of in vivo DTZ plasma concentration from the in vitro release data.
Deconvolution-Based Approach
Where, in vitro release data were converted into predicted plasma concentration–time curve, based on back-calculation of WN equation [36,37,38], according to Eq. (6):
where: D = dose, ΔFa = Fa(t+1) – Fa(t) and Δt = t(t+1) – t(t).
Convolution-Based Approach
Where fraction dissolved for each in vitro batch was directly convoluted to its equivalent predicted plasma levels. Convolution method requires general knowledge of PK parameters of ER DTZ, which is easily extracted from previous published literature [2, 9, 39].
The predicted AUC0-∞, AUC0-t and Cmax derived from the deconvolution- and convolution-based approaches were estimated.
Validation of Prediction Models
In order to validate the two predictive mathematical approaches describing the relation between the in vitro property and the in vivo response, the proposed evaluation approaches focus on the estimation of prediction error [40]. FDA guidance specifies the importance of assessment of internal and/or external predictability/validity as a requirement for the application of IVIVC models for regulatory submissions [36, 40]. The % prediction error (PE) for AUC0-∞, AUC0-t, and Cmax was calculated according to Eq. (7):
Predicted PK parameters, derived from both above approaches, were compared to actual observed PK parameters, to evaluate which of the two approaches were more likely to detect the actual values for both studied batches (Batch A-Ref and Batch B-Test).
Results and Discussion
The present study investigated the in vitro performances of two DTZ ER products using the FTC (USP IV), operated as open- and closed-loop setups, to come to terms which configuration setup is more appropriate to correlate with in vivo data. A direct 1:1 IVIVC was assessed using the traditional WN method. Predicted primary PK parameters were calculated employing both the deconvolution (back-calculation of WN) as well as the convolution-based approaches. The performances of the two approaches were compared to detect which was more able to accurately predict the plasma concentration–time course for the tested DTZ products. The validity of the correlation was assessed by computing internal predictability.
In Vitro Release Results
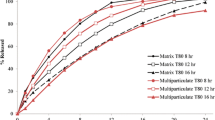
A discriminating release model is a significant in vitro test for evaluating any change in drug product formulation and/or processing. USP monograph for DTZ ER products is carried-out in 900 mL water using the official beaker (USP I) and paddle (USP II) methods [27]. As presented in the experimental part, FTC dissolution tester (USP IV) was operated in either open-loop or closed-loop setup. The release profiles for DTZ ER batches were illustrated in Figs. 1 and 2, while Table II tabulated DTZ release rate in 2, 6, and 12 h (Q2h, Q6h & Q12h) as well as the % dissolution efficiency at 12 h (% DE12h), and the mean dissolution time (MDT).

Release profiles of DTZ from ER batches in USP IV dissolution tester employing different configuration setups (mean ± SD, n = 3). Batch A-Ref: Tildiem Retard® 2 × 90 mg (Sanofi Winthrop Industries, France); Batch B-Test: DTZ Gel-Matrix Tablets (2 × 90 mg)

Comparison of different FTC configuration setups on DTZ release patterns from ER batches using similarity (f2) and difference (f1) factors, at different sampling intervals (mean ± SD, n = 3). Batch A-Ref: Tildiem Retard® 2 × 90 mg (Sanofi Winthrop Industries, France); Batch B-Test: DTZ Gel-Matrix Tablets (2 × 90 mg)
Generally, the release behaviors of both ER batches were in accordance with the acceptance criterion in the USP and the dissolution requirement for DTZ ER products (not less than 70% of the labeled amount is released in 12 h [27]. As presented in Fig. 1 and Table II, the release of DTZ from the two ER batches was higher in open-loop configuration setup versus the closed-loop setup, where ≥ 75% of labeled DTZ was released after 6 h and 12 h using the open- and closed-loop settings, respectively.
Upon using the open-loop setting, acceptable f1 (13) and f2 (52) values were calculated as per international acceptance limits (i.e., for curves to be considered similar, f1 and f2 values must be within the range of 0–15 and 50–100, respectively), indicating similarity of release profiles of tested batches with respect to the studied in vitro release models (Fig. 1). Also, similar release profiles were observed between ER batches using the closed-loop configuration of the FTC, with f1 and f2 values equal to 66 and 9, respectively (Fig. 1). This result was supported by calculating the statistical significance between the two ER batches regarding values of % DE12h and MDT, which indicated the absence of significant differences (p > 0.05) between the test and reference products (Table II).
Employing open-loop configuration of the FTC was previously reported to be of prime importance for BCS II drugs, where dissolution is considered the rate limiting step for absorption. Possible sink condition is easily maintained in the open FTC for longer periods, which is an important criterion for investigating the release of poorly soluble drugs [10]. Although, the release of DTZ, a BCS I drug with high solubility / high permeability characteristics, supposedly should not differ upon using either open- or close-loop setup of the FTC, yet opposing results were observed in the current study, which calls for some comments. Comparing both setups of the FTC, for the reference product (Batch A-Ref), f1 values of 20 and 18, and f2 values of 49 and 46, were attained after 6 and 12 h of release, respectively (Fig. 2). Also, for the gel-matrix tablets (Batch B-Test), both f1 and f2 values were not within the acceptance criteria along the duration of release (Fig. 2).
DTZ release rate from the ER batches was influenced by changing the amount of dissolution medium introduced during the release study, which in turn might influence the absorption step. This might be attributed to the fact that the concentration-buildup in release studies performed at fixed volume of medium (close-loop setup) is dissimilar from the actual in vivo process, where fraction of dissolved drug is immediately removed from the liquid by absorption [41]. On the other hand, the open system of FTC provides a progressive, continuous dissolution that closely mimic the actual absorption process.
In Vivo Results
Mean plasma concentrations of DTZ following oral administration of both ER batches were obtained from a previous pilot study conducted in 8 healthy volunteers [28]. The mean values of Cmax, AUC0-t and AUC0-∞ for both ER tablets were in agreement with other literature [42, 43]. DTZ, a highly variable drug, is known to exhibit irregular absorption and extensive first pass elimination [42, 43]. Development of an ER formulation for DTZ with a successfully validated IVIVC is of great importance.
Development of IVIVC
During the early steps of the development of a pharmaceutical product, proper search of a characteristic in vitro dissolution model that could reflect product in vivo performance is of prime importance. Developing a successful IVIVC allows reduction of the in vivo trials conducted in humans, hence accelerating the development of various drug products [9].
Figure 3 illustrated fraction absorbed (Fabs) profiles obtained following the deconvolution of the plasma profiles of the two DTZ ER batches employing WN method, against fraction dissolved (Fdiss) in both open and closed configuration setups. Results showed that Fabs for both ER batches was more comparable with the release profiles using the open-loop configuration of the FTC (Fig. 3). Also, it was observed that the in vitro release of Batch B-Test was higher in the open-loop setup than Batch A-Ref, which was in line with its higher in vivo rate and extent of absorption (Fabs of Batch B-Test ˃ Fabs of Batch A-Ref).

DTZ mean fraction dissolved and fraction absorbed (obtained using the Wagner- Nelson deconvolution method) for reference (Batch A-Ref) and Test (Batch B-Test) tablets
Successful IVIVC models were established between the in vitro Fdiss and the in vivo Fabs, employing different FTC setups as shown in Fig. 4. As presented in Fig. 4, the shift observed in the correlation shape emphasizes the sensitivity of the IVIV relation to the two different FTC configuration setups. As stated previously, a slope value of 1 and intercept value closer to 0 indicate a 1:1 correlation [35]. The best correlation with highest slope values close to unity and lowest intercept values close to 0 was obtained for Batch A-Ref and Batch B-Test, employing open-loop setup of FTC, with R2 values of 0.959 and 0.954, respectively. The FTC with open-loop configuration presented a better advantage in terms of IVIVC than the closed-loop model.

IVIVC attempts for both DTZ ER batches employing the open- and closed- loop configurations of the FTC, with their corresponding equations
Prediction and Validation of PK Parameters
Two different approaches are available for establishing IVIVC as well as predicting PK parameters, i.e., convolution and deconvolution techniques. The deconvolution-based approach extracts the in vitro release profile from the plasma concentration time profile. Alternatively, in the convolution-based approach, plasma concentration time profile is derived from the dissolution data and well authenticated PK parameters. Convolution technique utilizes a single stage approach to provide a relation between in vitro release and in vivo data, rather than the indirect deconvolution two stage approach [2, 9].
Figure 5 illustrated predicted DTZ HCL plasma profiles for the two studied batches, employing the two mathematical approaches against their actual in vivo plasma profiles, obtained from Emara et al., 2018 [28]. Predicted and actual PK parameters and the percentage prediction error (% PE) for Reference (Batch A-Ref) and Test (Batch B-Test), employing deconvolution and convolution approaches, were presented in Table III. It was quite apparent that there was a difference in the PK values calculated by the two approaches (convolution and deconvolution).

Comparison of DTZ plasma concentrations-time profiles predicted by two different approaches against actual in vivo data from (2 × 90 mg) ER tablets
For the deconvolution-based approach, Cmax, AUC0-t and AUC0-∞ attained values of 195.46 ng/mL, 2695.5 ng.h/mL, and 3076.2 ng.h/mL for Batch A-Ref, respectively and 232.33 ng/mL, 3184.45 ng.h/mL, and 3508.13 ng.h/mL for Batch B-Test, respectively (Table III).
On the other hand, the PK parameters (Cmax, AUC0-t and AUC0-∞) of Batch A-Ref were found to be 158.29 ng/mL, 2133.5 ng h/mL, and 2300.32 ng h/mL and for Batch B-Test were found to be 209.90 ng/mL, 2459.10 ng h/mL, and 2712.54 ng h/mL, respectively employing the convolution-based approach (Table III).
Moreover, %PE was employed for determining the predictability of the models [35]. As presented in Table III, employing the deconvolution-based approach provided %PE greater than 20% for AUCs of both studied batches, which suggest lack of predictability of the suggested model [35], while Cmax of Batch A-Ref and Batch B-Test attained % PE values of − 14.89% and − 2.14%, respectively.
On the other hand, as tabulated in Table III, convolution-based approach presented % PE for Cmax, AUC0-t and AUC0-∞ of values less than 10% for both studied ER tablets, which met with the US FDA acceptance limit [36, 40]. Observed Cmax values for Batch A-Ref and Batch B-Test were higher than predicted values by 6.95% and 7.72%, respectively. While on the other hand, observed AUCs values for both batches were lower than the predicted values by less than 10% (Table III).
From these results, it was clear that the convolution-based approach was more discriminative in predicting DTZ in vivo PK parameters with a minimal prediction error, compared to the deconvolution-based approach. The present study outlined a successful trial to predict DTZ PKs after an oral dose, from individual in vitro data performed in USP IV dissolution model. Employing the convolution approach might provide a precise prediction of in vivo performance from in vitro release data for other BCS Class I ER products.
Previously published reports discussing possible IVIVC models for DTZ usually employ the Wagner Nelson approach, which demand the presence of drug in vivo plasma concentration–time data for fulfillment of correlation [22,23,24,25,26]. Also, it is worth noting that in vitro testings of those correlations were carried out in either USP I or II dissolution models. Existence of IVIVC was confirmed for DTZ hydrocolloidal-based matrix tablet and Dilacor XR 240 mg under fed and/or fasting conditions against their in vitro dissolution in USP II models [23]. On the other hand, employing USP II model, using purified water, was more discriminative than USP III, in developing IVIVC for DTZ ER beads against oral solution [2]. Also, linear correlation was confirmed, by plotting % in vivo absorption versus % in vitro dissolution in USP I and II, for DTZ ER solid and semi-solid matrices against the reference product Herbesser SR (90 mg) [25].
Qureshi [9] stated that the deconvolution approach is the most widely cited method in the literature for estimating IVIVC, with various limitations including obtaining in vivo dissolution data from blood profile requires elaborative computing skills. The deconvolution approach is not best suited during product development stage, yet better applicable during method/apparatus development [9].
Extensive investigation is on-going for discovering the usefulness of convolution-based approach for proper estimation of IVIVC and assessment of drug PKs from valid in vitro dissolution data [44]. The convolution technique, less commonly cited in literature, uses simple spreadsheet software to assess IVIVC, and addresses all the limitations encountered by the deconvolution approach [9]. Another benefit of employing the convolution approach is that it is product independent (does not require data from an in vivo study of the test product), which is of great importance during product development, as we would only need a dissolution profile, together with few simple PK parameters to obtain predicted blood drug levels [9].
Furthermore, for optimizing a novel formulation, the convolution technique allows the prediction of blood levels of the test formulation from its in vitro data; hence, the formulation with the predicted blood levels equivalent to the innovator product will only be further incorporated for the animal/human in vivo trials. Hence, convolution-based approach benefits in reduction in number of experimental animal or human used for the in vivo PK studies, which is economically ideal.
CONCLUSION
Proper selection of dissolution test conditions is essential to establish an appropriate IVIVC, which in turn is quite imperative for waiver of costly bioequivalence trials. In the current study, employing the open-loop setup of the FTC provided a progressive, continuous dissolution that closely mimic the actual absorption process, and hence presented a better IVIVC than the closed-loop configuration for DTZ ER gel-matrix system. Moreover, the deconvolution-based approach has been previously proposed to establish IVIVC for different DTZ ER products. Herein, a simple and practical mathematical method was described to obtain DTZ plasma concentration–time profiles from in vitro release data, employing the flexible and easy to implement convolution-based approach. The percent prediction error values for Cmax, AUC0-t, and AUC0-∞ for tested ER products were less than 10%, which met with the US-FDA acceptance limit. Hence, the convolution technique could provide a powerful tool for establishing IVIVC and predicting blood levels of other ER products, which could help in saving valuable resources in terms of budgets and rise in total cost during product development of pharmaceutical industries.
References
Gomeni R, Bressolle-Gomeni F. Deconvolution analysis by non-linear regression using a convolution-based model: comparison of nonparametric and parametric approaches. AAPS J. 2019; Dec 9;22(1):9. https://doi.org/10.1208/s12248-019-0389-8
Sirisuth N, Augsburger LL, Eddington ND. Development and validation of a non-linear IVIVC model for a diltiazem extended release formulation. Biopharm Drug Dispos. 2002 Jan;23(1):1–8. https://doi.org/10.1002/bdd.270 (PMID: 11891668).
U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER). Guidance for industry: extended release oral dosage forms: development, evaluation, and application of invitro/ in-vivo correlations. 1997. http://www.fda.gov/downloads/drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm070239.pdf.
Wagner JG, Nelson E. Percent absorbed time plots derived from blood level and/or urinary excretion data. J Pharm Sci. 1963;52(6):610–1. https://doi.org/10.1002/jps.2600520629.
Loo JCK, Riegelman S. New method for calculating the intrinsic absorption rate of drugs. J Pharm Sci. 1968;57(6):918–28. https://doi.org/10.1002/jps.2600570602.
Cutler DJ. Numerical deconvolution by least squares: use of prescribed input functions. J Pharmacokinet Biopharm. 1978;6(3):227–41. https://doi.org/10.1007/BF01312264.
Veng-Pedersen P. Linear and Nonlinear system approaches in pharmacokinetics: how much do they have to offer? I General considerations J Pharmacokinet Biopharm. 1988;16(5):413–32. https://doi.org/10.1007/BF01062554.
Madden FN, Godfrey KR, Chappell MJ, Hovorka R, Bates RA. A comparison of six deconvolution techniques. J Pharmacokinet Biopharm. 1996;24(3):283–99. https://doi.org/10.1007/BF02353672.
Qureshi SA. In vitro-in vivo correlation (IVIVC) and determining drug concentrations in blood from dissolution testing – a simple and practical approach. The Open Drug Deliv J. 2010;4:38–47.
Emara LH, Taha NF, Mursi NM. Investigation of the effect of different flow through cell designs on the release of diclofenac sodium SR tablets. Dissolution Technol. 2009; May:23–31.
Kakhi M. Mathematical modeling of the fluid dynamics in the flow-through cell. Int J Pharm. 2009 Jul 6;376(1–2):22–40. https://doi.org/10.1016/j.ijpharm.2009.04.012.
Chiou WL, Riegelman S. Pharmaceutical applications of solid dispersion systems. J Pharm Sci. 1971 Sep;60(9):1281–302. https://doi.org/10.1002/jps.2600600902.
Claas SA, Glasser SP. Long-acting diltiazem HCl for the chronotherapeutic treatment of hypertension and chronic stable angina pectoris. Expert Opin Pharmacother. 2005 May;6(5):765–76. https://doi.org/10.1517/14656566.6.5.765 (PMID: 15934903).
Ammar HO, Haider M, Ibrahim M, El Hoffy NM. In vitro and in vivo investigation for optimization of niosomal ability for sustainment and bioavailability enhancement of diltiazem after nasal administration. Drug Deliv. 2017 Nov;24(1):414–21. https://doi.org/10.1080/10717544.2016.1259371.
Becker D, Zhang J, Heimbach T, Penland RC, Wanke C, Shimizu J, Kulmatycki K. Novel orally swallowable IntelliCap(®) device to quantify regional drug absorption in human GI tract using diltiazem as model drug. AAPS PharmSciTech. 2014 Dec;15(6):1490–7. doi: https://doi.org/10.1208/s12249-014-0172-1. Epub 2014 Jul 15.
Amidon G, Lennernas H, Shah VP, Crison JR. A theoretical basis for a biopharmaceutical drug classification: the correlation of in vitro drug product dissolution and in vivo bioavailability. Pharm Res. 1995;12:413–20.
Han X, Wang L, Sun Y, Liu X, Liu W, Du Y, Li L, Sun J. Preparation and evaluation of sustained-release diltiazem hydrochloride pellets. Asian J Pharm Sci. 2013;8(4):244–51. https://doi.org/10.1016/j.ajps.2013.09.007.
Follonier N, Doelker E, Cole ET. Various ways of modulating the release of diltiazem hydrochloride from hot-melt extruded sustained release pellets prepared using polymeric materials. J Control Release. 1995;36:243–50. https://doi.org/10.1016/0168-3659(95)00041-6.
Al-Saidan SM, Krishnaiah YS, Patro SS, Satyanaryana V. In vitro and in vivo evaluation of guar gum matrix tablets for oral controlled release of water-soluble diltiazem hydrochloride. AAPS Pharm Sci Tech. 2005;6(1):E14–21. https://doi.org/10.1208/pt060105.
Hermann P, Rodger SD, Remones G, Thenot JP, London DR, Morselli PL. Pharmacokinetic of diltiazem after intravenous and oral administration. Eur J Clin Pharmacol. 1983;24:349–52. https://doi.org/10.1007/BF00610053.
Murata K, Noda K, Kohno K, Samejima M. Pharmacokinetic analysis of concentration data of drugs with irregular absorption profiles using multi-fraction absorption models. J Pharm Sci. 1987;76:109–13. https://doi.org/10.1002/jps.2600760205.
Caramella C, Ferrari F, Bonferoni MC, Sangalli ME, De Bernardi di Valserra M, Feletti F, Galmozzi MR. In vitro/in vivo correlation of prolonged release dosage forms containing diltiazem HCI. Biopharm Drug Dispos 1993; 14: 143–160. https://doi.org/10.1002/bdd.2510140206.
Yu K, Gebert M, Altaf SA, Wong D, Friend DR. Optimization of sustained-release diltiazem formulations in man by use of an in-vitro/in-vivo correlation. J Pharm Pharmacol. 1998 Aug;50(8):845–50. https://doi.org/10.1111/j.2042-7158.1998.tb03998.x.
Korhonen O, Kanerva H, Vidgren M, Urtti A, Ketolainen J. Evaluation of novel starch acetate-diltiazem controlled release tablets in healthy human volunteers. J Control Release. 2004;95:515–20. https://doi.org/10.1016/j.jconrel.2003.12.026.
Rafiq M, Wahab A,Rehman N-Ur, Hussain A, Muhammad S. In vitro and in vivo evaluation of two sustained release formulations of diltiazem HCl. AJPP. 2010; Sep 4(9):678–694. https://doi.org/10.5897/AJPP.9000178.
Mircioiu C, Anuta V, Mircioiu I, Nicolescu A, Fotaki N. In vitro-in vivo correlations based on in vitro dissolution of parent drug diltiazem and pharmacokinetics of its metabolite. Pharmaceutics. 2019; Jul16;11(7):344. https://doi.org/10.3390/pharmaceutics11070344.
USP. Diltiazem Tablets and Extended-Release Capsules monogrphs. USP 28 - The United States Pharmacopeial Convention, Inc. Rockville, MD. 2005:655–658.
Emara LH, El-Ashmawy AA, Taha NF. Stability and bioavailability of diltiazem/polyethylene oxide matrix tablets. Pharm Dev Technol. 2018 Dec;23(10):1057–66. https://doi.org/10.1080/10837450.2017.1341523.
Emara LH, El-Ashmawy AA, Taha NF. A five-year stability study of controlled-release diltiazem hydrochloride tablets based on polyethylene oxide. J App Pharm Sci. 2015;5:012–22. https://doi.org/10.7324/JAPS.2015.50703.
Anderson N, Bauer M, Boussac N, Malek RK, Munden P, Sardaro M. An evaluation of fit factors and dissolution efficiency for the comparison of in-vitro dissolution profiles. J Pharm Biomed Anal. 1998;17:811–22. https://doi.org/10.1016/s0731-7085(98)00011-9.
Khan K, Rhodes CT. Effect of compaction pressure on the dissolution efficiency of some direct compression systems. Pharm Acta Helv. 1972;47(10):594–607.
Costa P, Sousa Lobo JM. Modeling and comparison of dissolution profiles. Eur J Pharm Sci. 2001;13(2):123–33. https://doi.org/10.1016/S0928-0987(01)00095-1.
Moore JW, Flanner HH. Mathematical comparison of dissolution profiles. Pharm Technol. 1996;20:64–74.
Wagner JG. Biopharmaceutics and relevant pharmacokinetics. Hamilton: Drug Intelligence; 1971.
Taha NF, Emam MF, Emara LH. A novel combination of Soluplus®/Poloxamer for Meloxicam solid dispersions via hot melt extrusion for rapid onset of action. Part 2: comparative bioavailability and IVIVC, Drug Dev Ind Pharm. 2020;46:8, 1362–1372. https://doi.org/10.1080/03639045.2020.1791164.
Ostrowski M, Wilkowska E, Baczek T. The influence of averaging procedure on the accuracy of IVIVC predictions: immediate release dosage form case study. J Pharm Sci. 2010;99(12):5040–5. https://doi.org/10.1002/jps.22209.
Gohel M, Delvadia RR, Parikh DC, Zinzuwadia MM, Soni CD, Sarvaiya KG, Mehta NR, Joshi BR, Dabhi AS. Simplified mathematical approach for back calculation in Wagner-Nelson method. Pharmaceutical reviews. 2005;3 (2).
Wagner JG, Nelson E. Kinetic analysis of blood levels and urinary excretion in the absorptive phase after single dose of drugs. J Pharm Sci. 1964;53:1392–403. https://doi.org/10.1002/jps.2600531126.
Bendas ER. Two different approaches for the prediction of in vivo plasma concentration-time profile from in vitro release data of once daily formulations of diltiazem hydrochloride. Arch Pharm Res. 2009 Sep;32(9):1317–29. https://doi.org/10.1007/s12272-009-1918-2.
CDER (Center for Drug Evaluation and Research), Guidance for Industrial Extended-Release Oral Dosage Forms: Development, Evaluation and Application of In Vitro/In Vivo Correlations, Food and Drug Administration, Rockville, MD (1997).
Banaker UV (Ed.). Pharmaceutical dissolution testing, Marcel Dekker, New York, 1992:53–107.
Gordin A, Pohto P, Sundberg S, Nykanen S, Haataja H, Mannisto P. Pharmacokinetics of slow-release diltiazem and its effect on atrioventricular conduction in healthy volunteers. Eur J Clin Pharmacol. 1986;31:423–6. https://doi.org/10.1007/BF00613518.
Della Paschoa OE, Luckow V, Trenk D, Jahnchen E, Santos SR. Prolongation of the PQ interval as a measure of therapeutic inequivalence between two formulations of diltiazem. Eur J Clin Pharmacol. 1995;48:45–9.
Rastogi V, Yadav P, Lal N, Rastogi P, Singh BK, Verma N, Verma A. Mathematical prediction of pharmacokinetic parameters-an in-vitro approach for investigating pharmaceutical products for IVIVC. Future J Pharm Sci. 2018;4(2):175–84. https://doi.org/10.1016/j.fjps.2018.03.001.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB).
Author information
Authors and Affiliations
Contributions
All the authors contributed to the design and implementation of the research, to the analysis of the results, and to the writing of the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Taha, N.F., Emara, L.H. Convolution- and Deconvolution-Based Approaches for Prediction of Pharmacokinetic Parameters of Diltiazem Extended-Release Products in Flow-Through Cell Dissolution Tester. AAPS PharmSciTech 23, 202 (2022). https://doi.org/10.1208/s12249-022-02361-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12249-022-02361-2