
Abstract
Background
Digital behaviour change interventions aiming to improve dietary intakes; specifically fruit and vegetable intake, in low-socioeconomic children are being developed and tested. However there is currently no synthesis of the characteristics or reported effectiveness of these interventions. This systematic review aims to: (1) identify existing digital interventions targeting fruit and vegetable intake in low-socioeconomic status children, (2) identify and synthesise characteristics and reported effectiveness of these interventions using the Behaviour Change Intervention Ontology.
Method
CINAHL, ERIC, PubMed, Cochrane Library, ACM Digital Library and Scopus were searched in December 2021 – February 2022 and in February–March 2024. Inclusion criteria for studies were: 1) children of low-SES families, aged between 5–11 years old; 2) Digital intervention to improve fruit and vegetable intake; 3) Comparison groups could be digital or non-digital; 4) Outcome measures were fruit and vegetable intake and antecedents to diet behaviours; 5) Randomised controlled trials (cluster and parallel designs). Characteristics of identified studies were coded using the Behaviour Change Techniques Taxonomy and Modes of Delivery, Setting and Source ontologies of the Behaviour Change Intervention Ontology.
Results
Five studies met all inclusion criteria, with majority reporting significant effects of interventions on improving fruit and vegetable intake. Most common Behaviour Change Techniques found were Goal Setting (k = 4), Problem Solving (k = 3), Instruction on how to perform a Behaviour (k = 3), and Prompts and Cues (k = 3). Characteristics relating to intervention source were unclear.
Conclusions
Digital interventions had positive outcomes in fruit and vegetable intake in children; particularly more for fruit than vegetable intake. Characteristics in digital interventions which have direct effects on child fruit and vegetable intake in low-socioeconomic families should be further investigated. Furthermore, clearer reporting on intervention characteristics is needed.
Similar content being viewed by others

Background
A nutritious and healthy diet plays a critical role in maintaining health and well-being [1]. Nutrition in childhood specifically, is essential for growth, development, activity, and healthy eating habits [2]. Consumption of at least 5 portions of fruit and vegetables (FV) a day can have long-term positive effects on children’s health, such as a decreasing risk of long-term chronic diseases including cardiovascular disease and cancer [3,4,5,6]. Conversely, evidence suggests that consuming < 1 portion daily of FV can result in increased risk in long-term chronic diseases [5, 7]. Despite this, Public Health England released a National Diet and Nutrition Survey (NDNS) which found both parents and children within the UK population consuming FV all below the current dietary recommendations of the EatWell Food Guide, with only 18% of children between 5 and 15 years of age meeting the recommendation fruit and vegetable intake daily [5, 8].
Barriers to FV consumption include child food preferences [9], lack of time for food preparation [10], family dynamics [11], and parental knowledge and food literacy [8]. Families in low-socioeconomic status (SES) communities are less likely to consume nutritious foods that are consistent with dietary guidelines compared to high-SES families [8, 12] due to these aforementioned barriers and increased cost of nutritious food such as FV [13, 14].
Behaviour Change Interventions have attempted to address these barriers by targeting interventions to a specific population and behaviour [15]. Digital Behaviour Change Interventions (DBCIs) specifically, are a popular method for addressing nutritional intake in children [16, 17]. DBCIs for improving child nutrition have targeted a wide range of outcomes, including antecedents of diet behaviour such as increasing nutritional knowledge [18] and self-efficacy [19, 20], as well as targeting behaviour itself in increasing FV [21], decreasing fat and sugar [22, 23], and decreasing sugar-sweetened beverages [21]. Despite the range of DBCIs aimed at a variety of nutrition outcomes, these interventions seemed to be most promising for improving FV intake compared with other nutrition outcomes, as existing reviews have found the significant impacts of DBCIs on adolescents and children [16, 24, 25]. However, DBCIs to increase FV intake in children within low-SES families have not yet been systematically reviewed for their characteristics of effectiveness.
Identifying the key characteristics of interventions; such as DCBIs, are essential to understand how an intervention is delivered, why an intervention may be effective, and to facilitate replication of intervention effectiveness [26]. Consistent classification of intervention characteristics are facilitated by standardised coding systems [27], such as the Behaviour Change Techniques Taxonomy (BCTTv1) [28] to code behaviour change techniques: the ‘active ingredients’ embedded within an intervention’s content. More recently, the Behaviour Change Intervention Ontology (BCIO) has been developed to extend standardised classification of Behaviour Change Interventions [26, 29]. Ontologies are defined as a data structure of; (1) unique identifiers representing types of entity, (2) labels and definitions corresponding to these identifiers and (3) specified relationships between the entities [30, 31]. The BCIO specifically, aims to classify interventions beyond Behaviour Change Techniques (BCTs) alone, including Intervention Source; how an intervention is delivered [32], Mode of Delivery; how content is provided to a target population [33]; and Intervention Setting; where an intervention is delivered [34].
DBCIs are evidently being adopted to address healthy eating behaviours, such as FV consumption in children [16, 25, 35]. Previous reviews exist which have synthesized evidence on the effectiveness of digital interventions to improve children’s diet [17, 25, 36]. However, these reviews focus solely on intervention effect sizes [36], intervention features, parent functionality and usability [25], and delivery methods and features such as health education, goal setting and self-monitoring towards adolescents [17]. To-date, no review has synthesised the evidence of DBCIs for FV consumption in low-SES children using an appropriate coding structure. Despite the BCIO being used to code intervention characteristics in two other previous studies, one of these interventions focused on digital tools targeting physical activity [37], and the second focused on smoking cessation interventions for those with physical disabilities [38]. Therefore, no review has identified common characteristics among effective and non-effective DBCIs for low-SES children’s FV intake, including using the Behaviour Change Intervention Ontology. Therefore, the aims of this systematic review were to: (1) identify existing digital interventions targeting fruit and vegetable intake in low-socioeconomic status children, (2) identify and synthesise characteristics or reported effectiveness of these interventions using the Behaviour Change Intervention Ontology.
Methods
The systematic review protocol was registered with PROSPERO (CRD42021291643). PRISMA 2020 Guidelines for reporting completed systematic reviews were followed [39] (see Additional file 1).
Search strategy
One search was conducted in February–March 2022 to capture studies published within the last 10 years (2011–2022) and a second conducted from February–March 2024, to capture all studies published between the years of 2022–2024. A systematic search was conducted using CINHAL, ERIC, PubMed, Cochrane Library, ACM Digital Library, and Scopus databases. The search strategy was supported by an information specialist librarian. Search terms included: 1) Digital Behaviour Change interventions, nutrition/dietary interventions, family-based interventions 2) Primary school children, low-SES communities, parental guidance 3) Dietary intakes, all combined with ‘AND’, with wildcards (*) also used. Search strategies used for each database can be seen in an additional file (see Additional file 2).
Inclusion criteria
Inclusion criteria were set in line with the PICOS framework (Population, Intervention, Comparison group, Outcome and Study Design) [40, 41]. Studies were included based on the following: 1) Participants were children of low-SES families, aged between 5–11 years old; 2) Featured a digital intervention to improve fruit and vegetable intake using any form of technology. Interventions could address fruit and vegetable consumption alone, or with additional diet behaviours such as consumption of sugar-sweetened beverages, and packing lunchboxes to include an increased range of nutritional foods, including fruits and vegetables; 3) Comparison groups could be digital or non-digital, address a diet behaviour other than fruit and vegetable consumption, or a placebo intervention group (e.g. a non-nutritional intervention focused on other curriculum, such as math or science); 4) Outcomes assessed included assessment of child fruit and vegetable intake as the primary outcome, whether subjective or objective. Assessment of antecedents to diet behaviours, such as nutrition knowledge and self-efficacy and other health behaviours, such as physical activity, were also included if reported; 5) Randomised controlled trial studies, including cluster and parallel designs were included. School, community, and home-based interventions were included. Studies were included if they were published in English, published in peer-reviewed journals, and published from 2011 onwards.
Study selection
Search results were imported into Zotero and duplicates removed. Titles, abstracts and full texts were screened by HF and EN and organised into a structured excel table. HF screened full texts for eligibility. If inconsistencies between two reviewers occurred, a third reviewer (KLC) was available to evaluate. No inconsistencies were apparent.
Data extraction
All data from included studies were extracted onto a standardised Excel form between February and March 2022 and February–March 2024. Data was extracted by the primary researcher (HF) and double-coded by a second reviewer (EN). Data extraction was informed by the Template for Intervention Description and Replication (TiDieR) checklist [42].
Overall study characteristics extracted included study design, length of intervention, participants, measurements of low-SES and direct parental involvement within the intervention. As child FV intake was the main outcome measure, parental behaviours were not assessed within the studies. Interventions that were considered multi-component; which included several approaches designed (2 or more) to improve behavioural outcomes, were also captured within this study [43].
Open science characteristics apparent within the paper were also coded: whether a study was pre-registration or had a protocol available, whether open data, open materials and open analysis scripts were available, whether the study was described as a replication of a previous intervention, whether a funding or conflict of interest statement was provided and whether the paper was open access [44].
Intervention characteristics of each study and each intervention group were extracted using the Behaviour Change Intervention Ontology [29], including the setting: where the intervention took place [34], modes of delivery: how the intervention was delivered [33], and source: who delivered the intervention [32]. Characteristics of the BCIO were coded onto the BCIO data extraction template v1 [45]. Intervention content of each study, in the form of BCTs, was extracted using the BCCTv1 [28]. Behaviour change theories reported as used within interventions were also extracted.
Outcome characteristics extracted included measures of dietary outcome assessment; such as 24-h dietary recall methods [46,47,48], dietitian assisted recalls [48], electronic food photos [23, 49]. Details of non-behavioural outcome measures were also extracted, including changes in attention, attitudes, acceptability towards healthy eating and digital interventions, barriers and facilitators to intervention implementation and participation (e.g., lack of sufficient resources, funding, time. lack of available facilities) and self-efficacy. Effectiveness characteristics extracted included statistical significance as reported within the papers, means and percentages of outcome change and changes to FV intake over time. Meta-analyses of intervention outcome data was not performed due to the heterogeneity of outcomes identified.
Quality appraisal
Risk of bias assessment was performed using the Cochrane Collaboration tool for assessing risk of bias in randomized trials [50, 51]. Assessment was performed for selection bias, study design, contamination, co-intervention, blinding, data collection and withdrawals and drop-outs. Studies were classified as high risk of potential bias if two or more of the categories are assessed as weak (high risk), moderate risk of potential bias if one category was assessed as weak (moderate) and low risk of potential bias if none of above categories were assessed as weak (low risk) [50, 52].
Results
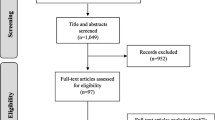
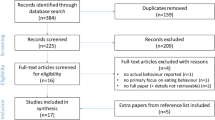
After duplicate removal, 10,311 papers were identified in the first searches conducted in February–March 2022 for title and abstract screening, with 5 studies included in the final review. In February–March 2024, after duplicate removal, a total of 7,124 papers were identified for title and abstract screening. After assessing full-text, no new papers were identified. Therefore, a total of 5 studies were included in the final review. This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews Flow Diagram (PRISMA 2020) for identifying papers [39]. Details on the PRISMA 2020 Flow Diagram for updated systematic reviews can be seen in Fig. 1.

The PRISMA 2020 diagram details the applied search and selection process
Overall study characteristics
Overall study characteristics are summarized in Table 1. All papers were randomized controlled trials, including two-group RCT (k = 3) [23, 46, 47], four-group RCT (k = 1) [25], and Cluster-RCT (k = 1) [49]. The length of the intervention including follow-up, ranged from 8 weeks [49] to 3 months [48, 49]. Participant ages ranged from 8–12 years, with participants most commonly being aged 9–11 (k = 4) [46,47,48,49]. Parents were directly involved in interventions within 2 of the 5 studies [23, 48].
Socio-economic status (SES) in participants were measured by identification of economically disadvantaged neighborhoods; demographic information collected to determine percentage of children living in poverty [46], highest household education and average annual household income [23, 47, 48], and children qualifying for free/reduced lunch [49].
One study pre-registered their research, using ClinicalTrials.gov [48]. One study had a study protocol available as a separate paper [48]. One study had their data, materials and analysis script fully open to the public where they provided the full code, data, and output available on the Open Science Framework [49]. No studies were replications of existing interventions. Majority of papers were Open Access [44, 46, 47] (Table 2).
Intervention characteristics
Theories described as used within these interventions included Social Cognitive Theory (k = 3) [23, 47, 48] and Self-determination Theory (k = 2) [47, 48]. No behaviour change theory was reported within two studies [46, 49]. Coding of intervention characteristics according to the Behaviour Change Intervention Ontology [29], include the intervention Setting [34], Modes of Delivery [33], and Source [32], are provided in an additional file (see Additional file 3). The Behaviour Change Intervention Data Extraction Coding Template [53] can be seen in an additional file (see Additional file 4). Coding of intervention content according to the Behaviour Change Techniques Taxonomy v1 [28], is provided in Table 3.
Intervention setting
All included studies took place in the United States and were considered low-income areas (k = 5) [23, 46,47,48,49]. In one study, while socioeconomic level of families were described as fairly high, average annual household income was < 61,000 [48], which is below the median household income [54]. One study is clearly described to take place in a primary school [49]. Due to unclear reporting, majority of these studies may take place within a household residential setting [23, 46,47,48], with two of these studies possibly being based in a primary school [46] and middle school [47]. Most studies were described to take place in urban areas [46,47,48,49], one in suburban [48] and one in a rural area [47].
Mode of delivery
All studies delivered their interventions using a form of electronic mode of delivery (k = 5) [23, 46,47,48,49]: conducive to them being DCBIs. Electronic modes of delivery used include mobile digital devices (k = 4) [23, 46, 55, 56]; including a handheld computer, mobile website and mobile communication app, computers (k = 3) [23, 47, 48], and electronic billboard and electronic environmental objects [49]. Digital content of interventions were delivered through text messaging (k = 1) [23], video game (k = 2) [47, 48], email (k = 1) [48], and website and mobile application such as a Facebook page [23, 46,47,48]. Information was described as delivered through audio- such as using a song-based reward system (k = 1) [46], visual- (k = 5), and textual information formats such as text messaging (k = 3) [23, 46, 48].
Some interventions were individual-based: aimed directly at either the child or parent (k = 3) [23, 46, 47], while other interventions were pair-based interventions; aimed at both child and parent (k = 1) [48], or group-based; involving participation within full school assemblies or classrooms (k = 1) [49]. Most studies featured asynchronous activities (k = 4) [23, 46,47,48]; different components of the intervention could be completed at different times. All interventions contained push components; notifications directly sent to participants to reinforce dietary intakes [23, 46,47,48,49]. For example, push components such as song-based reward systems [46], daily/weekly motivational text messages [23, 47], tips and feedback [48], and daily goals [49], all to be used as reminders, prompts and cues to complete daily goals and overcome barriers to FV intake [23, 46,47,48,49]. Some interventions contained pull messages, where participants needed to set their own goals and take electronic pictures of their foods (k = 3) [23, 46, 48]. Most interventions contained gamification features (k = 4) [46,47,48,49], including a song-based reward system [46], knowledge mini-games [47], goal setting and motivational messaging [47], problem solving and avatars or stories in order to encourage nutrition knowledge and FV intake [48, 49].
All interventions included used some form of Human Interactional mode of delivery (k = 5) [23, 46,47,48,49]. One study which included face-to-face human interactional mode of delivery, components of the intervention took place within a school environment, where teachers or research coordinators were directly involved delivering the nutrition content to the children [49]. As all interventions were digital, at-a-distance human interaction mode of delivery was more common among studies (k = 4), as the digital components of interventions took place in the home environment or with the participants themselves without the direct involvement of the researcher [23, 46,47,48]. Some studies found (k = 2) [23, 48] contained more than 2 varying digital components of the interventions. One of the studies, which found a significant increase in child FV intake and was maintained at the 3-month follow up, used an online video game for the kids, and electronic newsletters to parents [48]. The second study, which found a significant effect of vegetable intake over time (p < 0.001) and maintained at the 10-week follow-up, the intervention used contained a web site, social media and text messages in order to improve FV intake in children [23].
Intervention source
All studies described using a researcher (k = 5) [23, 46,47,48,49] to deliver the intervention to participants, with one directly also involving a primary school teacher (k = 1) [49]. However, in some studies the source of the intervention were unclear [46]. The Intervention Source Ontology is designed to only characterise people involved in intervention delivery, not the collection of outcome measurements. Dietitians (k = 3) [47], undergraduate and graduate students (k = 1) [23] were reported as involved in data collection, but were accordingly not coded as constituting an intervention’s source. While few studies used professionals in a trained profession; such as dietitians to assess dietary recalls [47] and the digital story within the intervention being written by a professional writer [48], one study clearly stated that the first author was a registered dietitian and a graduate nutritional sciences students, so is therefore familiar with nutrition around fruits and vegetables [23].
Behaviour Change Techniques (BCTs)
A total of 22 individual BCTs were present across the five interventions. All studies featured at least one identifiable behaviour change technique (Table 3). The most frequently used BCTs were Goal setting (k = 4) [46,47,48,49], Instruction on how to perform a behaviour (k = 3) [23, 47, 48], Prompts and Cues (k = 3) [23, 46, 49] and Problem Solving (k = 3) [23, 46, 48]. No studies directly mentioned coding BCTs using the Behaviour Change Technique Taxonomy v1 [23, 46,47,48,49].
Outcome and effectiveness characteristics
Primary outcomes of all studies were fruit and vegetable intake (k = 5) [23, 46,47,48,49]. Primary outcome measurement tools include 24-h dietary recall methods [46,47,48], telephone recalls [48], dietitian assisted recalls [48], electronic food photos [23, 49]. Outcome follow-up lengths ranged from 4 weeks [46] to 3 months [48, 49].
Antecedents and secondary outcomes of behaviour
Secondary outcomes among studies included physical activity [47], sugar-sweetened beverage intake [46], water intake [47], fruit and vegetable intake separately [23, 48, 49], sedentary behaviour, skin carotenoid concentrations [23, 48], and BMI [23, 46] as secondary outcomes. While antecedents to diet behaviour were not reported as secondary outcomes, nutritional knowledge [23, 47, 48], parental skills [23, 48], and self-efficacy were captured within all interventions in order for the participants to achieve the behavioural outcome. Parents and guardians were directly involved within some studies (k = 2) [23, 48], with intervention content aiming to improve parental knowledge and skills to overcome barriers that impact dietary outcomes; such as FV intake, and how to increase FV accessibility for children [23, 48].
Changes in overall FV consumption
Statistically significantly improvements in FV intake were found in majority of studies (k = 4), with majority being maintained at follow-up [23, 47, 48]. For example, one study found an almost 50% increase in FV intake (+ 0.72 servings). This increase was maintained at a 3-month follow-up, reporting a 41% increase over baseline FV intake [48]. Another study found an increase in FV intake of + 0.67 servings per day at 2-month follow-up compared to baseline (< 0.018) [47]. One study found a non-significant change in FV consumption from baseline to Week 4 follow-up (p = 008), although nearly leading to an increased FV portion per day (+ 0.88) [46]. Only one study with significant improvements in FV intake were not maintained at follow-up of 3-months, however still had significant improvements for fruits alone (p < 0.031) [49].
Differences in fruit versus vegetable consumption
Differing effects were observed when comparing fruit versus vegetable intake at last follow-up. One study significantly improved FV consumption by + 0.68 servings per day at 3 month follow-up (p < 0.001), although there was no significant effects observed for vegetables alone [48]. Similarly, another study with a 3-month follow-up found significant improvements in both FV with only fruits having significant improvements at follow up (p < 0.031) [49]. Conversely, another study with a 10-week follow-up found significant increases in vegetable intake in the intervention group compared to the control group (p > 0.0001), but no significant effects for fruits alone (p = 0.09) [23]. Differences in longevity of effects on fruit versus vegetable consumption were also observed. For example, one study found a statistically significant time main effect for fruit intake increasing over time both immediately post-intervention (p < 0.001) and at 3-months follow-up (p < 0.001). However, no significant interaction or main effects were observed for vegetables [48].
Risk of bias
All five studies were assessed to be high risk of bias on at least one domain, with some studies (k = 3) [23, 46, 47] having an additional high risk of bias in at least one other domain (Table 4). One study was considered having an overall high risk of bias due to being a high risk of bias in four domains [46]. Majority of studies had a medium risk of bias (k = 4) as they had either one [48, 49] or two domains that had a high risk of bias [23, 47] but were not at critical risk of bias in any other domain. The most consistent domain in which studies had a high risk of bias included performance bias, where participants in all studies were either aware of the intervention (k = 5) [23, 46,47,48,49], blinding was not attempted (k = 2) [48, 49], or blinding status was not described (k = 3) [23, 46, 47]. Lastly, two studies had a high levels of detection bias, where nothing was stated in the study [46], or assessors were not blinded to the outcomes [23].
Due to the small number of studies identified, heterogeneity of the outcome variables within these studies, and majority of studies having a high risk of bias in more than one domain, a meta-analysis was not considered necessary to conduct as this may produce an inappropriate summary of the findings.
Discussion
This systematic review identified five papers which emphasized digital tools can achieve small to moderate changes in FV intake with lasting effects up to 3-months and therefore, are promising interventions for improving FV intake in children within low-SES families [16, 23, 48]. While improvements in child FV intake remain promising; vegetable intake was identified as harder to maintain overtime [48, 49]. Long term effects of interventions (≥ 12-months) are still unclear [16].
This review captured characteristics embedded in these interventions using the Behaviour Change Intervention Ontology. The Intervention Source Ontology identifies how behaviour change interventions are delivered, including by whom [32]. The Mode of Delivery Ontology specifies the way in which these interventions are delivered [33], and the Intervention Setting Ontology identifies the different contexts in which interventions may change behaviour [34]. These ontologies all form one individual part of the Behaviour Change Intervention ontology, which aims to cover all aspects of behaviour change interventions and is a key to understanding intervention effectiveness [32].
While the digital Mode of Delivery varied among websites, computers and apps, common digital content of the interventions found were delivered through text messaging [23], video games (k = 2) [47, 48], and website and mobile application such as a Facebook page [23, 46,47,48]. Some of the interventions identified were considered multi-component [23, 48] which include two or more digital components designed to improve behavioural outcomes [43]. These multi-component interventions maintained their positive effects on FV intake in their follow-up period of 10 weeks to 3 months [23, 48].
Most papers contained ≥ 6 + BCTs, with Goal setting, Problem Solving, Instruction on how to Perform a Behaviour, and Prompts and Cues being the most common BCTs among these papers [46,47,48,49]. The mode of delivery of DBCIs, such as using a mix of text messaging and communication through mobile apps may be an effective interactive method to use when delivering interventions, and using gamification features have been shown to maintain behavioural outcomes during follow-up periods [18, 35, 57].
The findings of this review align with previous reviews which show digital interventions can significantly improve FV intake compared with interventions not using digital technologies [17, 25, 36]. Studies which assessed FV intake separately [48, 49], found FV consumption to significantly improve at a 3-month follow-up, however no significant effects were observed for vegetables alone [48]. These findings have also been seen in prior interventions, which have assessed fruit and vegetable intake separately, and found minimal impact on vegetable intake overtime compared to fruit [58]. Therefore, vegetable intake in children may be harder to maintain overtime than fruit intake, however is possible to maintain if vegetables are further prompted and emphasized for their importance in health [59].
The importance of an intervention setting and has been described in previous literature, with one RCT reporting significant increases in child FV intake up to 12 months after completion with the intervention being based in the home environment due to the possibility of having more access to digital interventions [60]. However, overall effects of dietary intervention settings have been unclear due to the lack of literature or mixed results [61]. Lastly, while this review did not directly show the impact that the intervention source may have on the reported effectiveness of interventions, majority of interventions reported in this review were delivered by the researcher. While impacts of parents as the source of the intervention were unclear, direct parental involvement were found in some studies (k = 2) [23, 47]. These studies aimed to teach parents how to assist their child in meeting goals and overcoming barriers to FV intake [47], and increasing accessibility to a variety of FV [23]. Both these studies found a significant effect in FV intake overtime. Therefore, more research is needed on understanding which setting and source; such as being delivered by a teacher or parent, should be further investigated.
As modes of delivery used within interventions are important to specify to facilitate replication [33], mobile digital devices and app-based interventions has been shown in current research to be accessible amongst all population groups [47, 49, 55, 56, 62,63,64]. For example, one existing digital intervention in this review which aimed to improve FV intake in children; and originally stated families were a mix of both high and low-SES, found significant increases in FV intake maintained for 3-months [65]. However, their long-term effects still remain mixed or unclear [17, 25, 36]. The significance of the mode of delivery have been supported within the literature, where a meta-analysis of RCTs found that text messages to deliver educational messages to families or parents were effective at promoting behaviour change, including children’s dietary intakes [66, 67]. For children specifically, the literature has shown that mobile apps with the use of gamification features; such as rewards games, goals, avatars and stories, can improve FV intake [18, 35, 68, 69]. The interventions found within this review which had the longest maintained effects at 3-months on child FV intake included a mix of text messaging, computers, and communication through mobile apps, which were highly accepted by parents in this review [48].
Behaviour Change Techniques embedded within interventions are important to specify to facilitate replication and understanding of intervention content [28, 31]. Within the literature, ‘Goal setting’, ‘Problem Solving’, ‘Instruction on how to Perform a Behaviour’, and ‘Prompts and Cues’ are BCTs have been specified in other related diet interventions [70, 71]. The majority of the papers found in this current study contained more than 6 + BCTS, with Goal setting, Problem Solving, Instruction on how to Perform a Behaviour, and Prompts and Cues being the most common BCTs among these papers [46,47,48,49]. Interventions which had the longest follow-up period of 3 months, also contained these BCTs [48, 49]. To further support the effect these BCTs have on dietary outcomes, the results of another existing study; which identified BCTs for dietary and physical activity interventions, found the most effective BCTs resulting in long-term facilitators being ‘goal setting’, ‘self-monitoring of behaviours’, ‘problem solving’, ‘feedback on outcome of behaviour’, ‘instruction on how to perform the behaviours’ and ‘adding objects to the environment’ [70].
Lastly, the effectiveness of multi-component interventions on dietary intakes have been supported in the literature; such as interventions which include education, environment, mode of delivery or parental components, and can be more successful than single-component interventions [72, 73]. Two prior existing studies within the literature which aimed to have parents pack healthier lunchboxes, contained a multi-component intervention consisting of both parent and child involvement in the intervention, digital mobile applications, curriculum lessons, and paper pamphlets [55, 56]. The significant changes in this study were maintained for up to 6 months [56]. This review has shown that multi-component interventions may improve FV intakes significantly, compared to single-component interventions [56]. The two interventions identified contained more than one digital component and maintained their follow-up period of 10-weeks to 3 months [23, 48]. Identifying what embedded components and characteristics of an intervention exist may help in understanding how interventions can be tailored to the population when informing future interventions and implementation policies [74].
Strengths and limitations of identified studies
Studies were only included in this review if they were randomized controlled trials, which are considered the gold standard for health intervention effectiveness research [75]. However, all interventions were assessed via the Cochrane tool for risk of bias and were shown to have high risk of bias on at least one domain, with some studies (k = 3) having an additional high risk of bias in at least one other domain. All the RCTs in this present study had a high risk of performance bias, which could mean that participants may have been aware of the intervention and the behavioural outcomes may have been due to outside influences. Therefore, the intervention may not be as effective to dietary intakes as the RCT has claimed. Additionally, although all papers were Open Access, only one study only one study had open data, materials and code to facilitate replication and transparency [49].
Strengths and limitations of this study
Strengths of this systematic review include its inclusion of RCTs and its novel use of the Behaviour Change Intervention Ontology to specify in-detail the characteristics of DCBIs to improve child fruit and vegetable intakes. This is one of the first systematic reviews to use the BCIO to code included papers, with one other review having coded DBCIs using the BCIO in the context of physical activity [37], and another scoping review which has used the BCIO in the context of smoking cessation [38]. Inclusion of the BCIO coding in future systematic reviews will facilitate greater clarity on the content, context and delivery of behaviour change interventions. This review is also one of the first to address the lack of digital tools aimed at low-SES families, and what characteristics may need to be implemented into digital interventions to result in outcome effectiveness for this population group. Understanding what characteristics benefit this population may help to limit digital intervention inequalities between populations.
Limitations of this systematic review include a lack of firm reported effectiveness conclusions based on a small number of eligible studies. Most included studies had relatively short follow-up periods (< 3 months), making it not possible to make firm conclusions on longer-term effectiveness. While this review covered an important topic around child FV intake in low-SES families, there were very limited studies that were found which focused directly on this behaviour and population. Additionally, majority of these studies were high risk studies, which may mean claims made about effectiveness are inaccurate. Only English language studies were included, which limits a wider range of studies globally. It is worth noting that all identified studies in this review took place within the United States (k = 5), which presents a significant limitation to understanding of the current findings. Additionally, as the population group is low-income families, issues related to digital interventions causing inequalities or a divide in the population need to be considered. While some studies exist which have found that low-SES families still have high access to smartphones [76], there is a lack of understanding in the current papers as to whether there were any limitations to accessing digital devices or whether developing digital interventions could result in widening inequality in relation to engagement within public health interventions [74].
Areas and implications for future research
Despite the evidence identified here that digital interventions have a significant impact on low-SES children’s fruit and vegetable intake, the long-term effect that digital interventions have on child FV intakes have yet to be established. While digital interventions themselves are an individual level mechanism for improving FV consumption in children, future intervention development research in low-SES families also needs to be aware of how digital interventions may generate inequalities within the population at the public health level, and how to use these interventions to overcome other influential factors to FV consumption; such as food insecurity and poverty [74]. Therefore, it is important to consider other influences of fruit and vegetable intake, such as influences from the socioecological framework including, family-level and social-structural influences [77].
While this review identified digital dietary tools aimed at low-SES families, an existing digital divide may create a gap between low-SES and high-SES populations on accessing these tools, and can exclude people who could benefit the most from these interventions [78]. How to design and develop digital interventions to meet the needs of the low-SES families appropriately should be considered for future research.
This study is the first to use the Behaviour Change Intervention Ontology to provide detailed and consistent specification of DBCI characteristics in relation to children’s diet. Future studies could provide further clarity on DBCI specification using the BCIO. Lastly, conducting further research using consistent outcome measurements would facilitate the ability to meta-analyse these interventions.
Conclusion
This systematic review has identified what characteristics are used in DBCIs for children in low-SES families to improve FV intake. The intervention found with the longest maintained effect of FV intake contained multi-component digital tools (e.g. text messaging, computers and mobile apps), parental involvement, school and household setting, and 6 + BCTs [48] While the majority of studies identified reported significant improvements to FV intake [23, 47, 48], the quality of these studies were relatively low, and due to the limited evidence identified in this review, this makes providing firm conclusions on the effectiveness of digital interventions challenging.
This is the first review to report characteristics of diet DCBIs using the Behaviour Change Intervention Ontology. However, there is still limited knowledge on how digital tools can be disseminated and appropriately used for a specific population group without creating a greater digital divide. Therefore, further research on identifying what imbedded characteristics of an intervention; such as taking place outside the United States, using different modes of delivery, intervention settings and sources, may help to understand what characteristics work best for this type of intervention and population. Lastly, there is a need for clearer reporting of interventions. Improved intervention reporting using the BCIO would strengthen the evidence when reporting the effectiveness of DBCIs aimed at dietary intakes [26].
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- FV:
-
Fruit and Vegetables
- DBCIs:
-
Digital Behaviour Change Interventions
- SES:
-
Socioeconomic status
- BCTTv1:
-
Behaviour Change Techniques Taxonomy v1
- BCIO:
-
Behaviour Change Intervention Ontology
- TiDieR:
-
Template for Intervention Description and Replication
- BCTs:
-
Behaviour Change Techniques
- BCW:
-
Behaviour Change Wheel
- MoD:
-
Mode of Delivery
References
Kesari, A., Noel, J.Y. Nutritional Assessment. National Library of Medicine. 2023; Available from: https://www.ncbi.nlm.nih.gov/books/NBK580496/
Public Health Agency. Nutrition Matters in the Early Years. 2018. Available from: https://www.publichealth.hscni.net/sites/default/files/Nutrition%20Matters%20for%20the%20early%20years%200118.pdf.
Wang X, Ouyang Y, Liu J, Zhu M, Zhao G, Bao W, et al. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ. 2014;29(349):g4490.
WHO. Healthy Diet. 2020. Available from: https://www.who.int/health-topics/healthy-diet#tab=tab_1.
Scheelbeek P, Green R, Papier K, Knuppel A, Alae-Carew C, Balkwill A, et al. Health impacts and environmental footprints of diets that meet the Eatwell Guide recommendations: analyses of multiple UK studies. BMJ Open. 2020;10(8):e037554.
NHS. 5 A Day portion Sizes. 2022. Available from: https://www.nhs.uk/live-well/eat-well/5-a-day/portion-sizes/#:~:text=Children%20should%20also%20eat%20at,the%20palm%20of%20their%20hand.
Cobiac LJ, Scarborough P, Kaur A, Rayner M. The Eatwell Guide: Modelling the Health Implications of Incorporating New Sugar and Fibre Guidelines. PLoS One. 2016;11(12):e0167859.
Public Health England. National Diet and Nutrition Survey. 2016. Available from: https://www.gov.uk/government/collections/national-diet-and-nutrition-survey.
Arthur S, Mitchell AE, Morawska A. Parent-reported barriers to establishing a healthy diet with young children in Australia. Child: Care, Health and Development. 2022;n/a(n/a). https://doi.org/10.1111/cch.13081. Cited 2023 May 19
Gerritsen S, Renker-Darby A, Harré S, Rees D, Raroa DA, Eickstaedt M, et al. Improving low fruit and vegetable intake in children: Findings from a system dynamics, community group model building study. PLoS One. 2019;14(8):e0221107.
Cason-Wilkerson R, Goldberg S, Albright K, Allison M, Haemer M. Factors influencing healthy lifestyle changes: a qualitative look at low-income families engaged in treatment for overweight children. Child Obes. 2015;11(2):170–6.
Roberts C. Fruit and Vegetable Consumption. 2013. Available from: http://healthsurvey.hscic.gov.uk/media/1092/_7-fruit-and-vegetable-consumption_7th-proof.pdf.
Alkerwi A, Vernier C, Sauvageot N, Crichton GE, Elias MF. Demographic and socioeconomic disparity in nutrition: application of a novel Correlated Component Regression approach. BMJ Open. 2015;5:e006814.
Pechey R, Monsivais P. Socioeconomic inequalities in the healthiness of food choices: Exploring the contributions of food expenditures. Prev Med. 2016;88:203–9. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4910945/.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Prowse R, Carsley S. Digital interventions to promote healthy eating in children: umbrella review. JMIR Pediatr Parent. 2021;4(4):e30160–e30160.
Rose T, Barker M, Jacob CM, Morrison L. A systematic review of digital interventions for improving the diet and physical activity and behaviours of adolescents. J Adolesc Health. 2017;61:669–77.
Holzmann SL, Schäfer H, Groh G, Plecher DA, Klinker G, Schauberger G, et al. Short-term effects of the serious game “Fit, Food, Fun” on nutritional knowledge: a pilot study among children and adolescents. Nutrients. 2019;11:2031.
Keller J, Motter S, Motter M, Schwarzer R. Augmenting fruit and vegetable consumption by an online intervention: Psychological mechanisms. Appetite. 2018;1(120):348–55.
Livingstone KM, Rawstorn JC, Partridge SR, Godrich SL, McNaughton SA, Hendrie GA, et al. Digital behaviour change interventions to increase vegetable intake in adults: a systematic review. Int J Behav Nutr Phys Act. 2023;20(1):36.
Majumdar DD, Koch PA, Lee H, Contento IR, Islas Ramos ADL, Fu. Creature 101: A Serious Game to Promote Energy Balance-Related Behaviours Among Middle School Adolescents. Games Health J. 2013;2. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3833376/pdf/g4h.2013.0045.pdf
Sharma SV, Shegog R, Chow J, Finley C, Pomeroy M, Smith C, et al. Effects of the quest to lava mountain computer game on dietary and physical activity behaviors of elementary school children: a pilot group-randomized controlled trial. J Acad Nutr Diet. 2015;115:1260–71.
Bakırcı-Taylor A, Reed D, McCool B, Dawson J. mHealth improved fruit and vegetable accessibility and intake in young children. J Nutr Educ Behav. 2019;51(5):556–66.
Chau MM, Burgermaster M, Mamykina L. The use of social media in nutrition interventions for adolescents and young adults—a systematic review. Int J Med Informatics. 2018;1(120):77–91.
Zarnowiecki RKD, Mauch CE, Middleton G, Matwiejczyk L, Watson WL, Dibbs J, Dessaix A, Golley RK. A systematic evaluation of digital nutrition promotion websites and apps for supporting parents to influence children’s nutrition. Int J Behav Nutr Phys Act. 2020;17:17.
Michie S, Thomas J, Johnston M, Aonghusa PM, Shawe-Taylor J, Kelly MP, et al. The Human Behaviour-Change Project: harnessing the power of artificial intelligence and machine learning for evidence synthesis and interpretation. Implement Sci. 2017;12:121.
Larsen KR, Michie S, Hekler EB, Gibson B, Spruijt-Metz D, Ahern D, et al. Behavior change interventions: the potential of ontologies for advancing science and practice. J Behav Med. 2017;40(1):6–22.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46:81–95.
Michie S, West R, Thomas J, Hastings J. Representation of behaviour change interventions and their evaluation: Development of the Upper Level of the Behaviour Change Intervention ontology [version 2; peer review; 2 approved]. Wellcome Open Res. 2021;5. Available from: https://wellcomeopenresearch.org/articles/5-123
Norris E, Finnerty AN, Hastings J, Stokes G, Michie S. A scoping review of ontologies related to human behaviour change. Nat Hum Behav. 2019;3(2):164–72.
Marques MM, Wright AJ, Corker E, Johnston M, West R, Hastings J, et al. The Behaviour Change Technique Ontology: Transforming the Behaviour Change Technique Taxonomy v1. Wellcome Open Res. 2023;8:308. Available from: https://wellcomeopenresearch.org/articles/8-308.
Norris E, Wright AJ, Hastings J, West R, Boyt N, Michie S. Specifying who delivers behaviour change interventions: development of an Intervention Source Ontology [version 1; peer review: 2 approved, 1 approved with reservations]. Wellcome Open Res. 2021;6:77.
Marques MM, Carey RN, Norris E, Evans F, Finnerty AN, Hastings J, Jenkins E, et al. Delivering behaviour change interventions: development of a mode of delivery ontology. Wellcome Open Res. 2020;5:125.
Norris E, Marques MM, Finnerty AN, Wright AJ, West R, Hastings J, et al. Development of an intervention setting ontology for behaviour change: Specifying where interventions take place. Wellcome Open Res. 2020;5:124.
Champion NCKE, Parmenter B, Cyanna M, Spring B, Wafford QE, Gardner LA, Thornton L, McBride N, Barrett EL, Teesson M, Newton NC. Effectiveness of School-Based eHealth Interventions to Prevent Multiple Lifestyle Risk Behaviours among Adolescents: A systematic review and meta-analysis. Lancet Digital Health. 2019;1:e206–21.
Rodriguez Rocha NP, Kim H. eHealth interventions for fruit and vegetable intake: a meta-analysis of effectiveness. Health Educ Behav. 2019;46(6):947–59.
Encantado J, Palmeira AL, Silva C, Sniehotta FF, Stubbs RJ, Gouveia MJ, et al. What goes on in digital behaviour change interventions for weight loss maintenance targeting physical activity: a scoping review. Digital Health. 2022;1(8):20552076221129090.
Wuerstl KR, Todd K, Lawrason S, Shwed A, Holmes B, Gainforth HL. Theoretical components of smoking cessation interventions for persons with physical disabilities: a scoping review. Addict Behav. 2023;1(145):107762.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29(372):n71.
Amir-Behghadami M, Janati A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg Med J. 2020;37:387.
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. 2014;14. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4310146/
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;7(348):g1687.
Center for Nutrition Policy and Promotion. A Series of Systematic Reviews on the Effects of Nutrition Education on Children’s and Adolescents’ Dietary Intake. Alexandria, Virginia; 2012. Available from: https://nesr.usda.gov/sites/default/files/2019-04/NutritionEducation-FullReport.pdf
Norris E, Sulevani I, Finnerty AN, Castro O. Assessing Open Science practices in physical activity behaviour change intervention evaluations. BMJ Open SP EX Med. 2022;8(2):e001282.
Norris E, Zhang L, Wuerstl K, et al. A data extraction template for the behaviour change intervention ontology [version 1; peer review: awaiting peer review]. Wellcome Open Res. 2024;9:168. https://doi.org/10.12688/wellcomeopenres.20872.1. https://wellcomeopenresearch.org/articles/9-168.
Nollen NL, Mayo MS, Carlson SE, Rapoff MA, Goggin KJ, Ellerbeck EF. Mobile technology for obesity prevention: a randomized pilot study in racial- and ethnic-minority girls. Am J Prev Med. 2014;46:404–8.
Baranowski T, Baranowski J, Thompson D, Buday R, Jago R, Griffith MJ, et al. Video game play, child diet, and physical activity behavior change a randomized clinical trial. Am J Prev Med. 2011;40:33–8.
Thompson D, Bhatt R, Vazquez I, Cullen KW, Baranowski J, Baranowski T, et al. Creating action plans in a serious video game increases and maintains child fruit-vegetable intake: a randomized controlled trial. Int J Behav Nutr Phy Act. 2015;12:39.
Wengreen H, Joyner D, Kimball S, Schwartz S, Madden G. A randomized controlled trial evaluating the fit game’s efficacy in increasing fruit and vegetable consumption. Nutrients. . 2021;13(8). Available from: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-02302174/full
Higgins JPT, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD. The Cochrane Collaboriation’s tool for assessing risk of bias in randomized trials. 2011. Available from: https://www.bmj.com/content/343/bmj.d5928.
Karrah K, Young K, Tunis MC, Zhao L. Risk of bias tools in systematic reviews of health interventions: an analysis of PROSPERO-registered protocols. 2019. Available from: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-019-1172-8#citeas
Higgins J, Thomas J. Cochrane Handbook for Systematic Reviews of Interventions. 2021. Available from: https://training.cochrane.org/handbook/current
Norris E, Zhang L, Froome H. Behaviour Change Ontology Data Extraction Template v1. 2023. Available from: https://doi.org/10.17605/OSF.IO/ERH75.
Semega, J., Kollar, M. Income in the United States. United States Census Bureau; 2021 Available from: https://www.census.gov/library/publications/2022/demo/p60-276.html
Sutherland R, Brown A, Nathan N, Janssen L, Reynolds R, Walton A, et al. Protocol for an effectiveness- implementation hybrid trial to assess the effectiveness and cost-effectiveness of an m-health intervention to decrease the consumption of discretionary foods packed in school lunchboxes: the “SWAP IT” trial. BMC Public Health. 2019;19(1):1510.
Sutherland R, Brown A, Nathan N, Yoong S, Janssen L, Chooi A, et al. A Multicomponent mHealth-Based Intervention (SWAP IT) to Decrease the Consumption of Discretionary Foods Packed in School Lunchboxes: type I Effectiveness-Implementation Hybrid Cluster Randomized Controlled Trial. J Med Internet Res. 2021;23(6):e25256.
Holzmann SL, Dischl F, Schafer H, Groh G, Hauner H, Holzapfel C. Digital gaming in nutritional education: a survey on preferences, motives, and need of children and adolescents. JMIR Form Res. 2019;3:e10284.
Evans CE, Christian MS, Cleghorn CL, Greenwood DC, Cade JE. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am J Clin Nutr. 2012;96:889–901.
Offringa LC, Stanton MV, Hauser ME, Gardner CD. Fruits and vegetables versus vegetables and fruits: rhyme and reason for word order in health messages. Am J Lifestyle Med. 2019;13(3):224–34.
Wolfenden L, Wyse R, Campbell E, Brennan L, Campbell KJ, Fletcher A, et al. Randomized controlled trial of a telephone-based intervention for child fruit and vegetable intake: long-term follow-up123. Am J Clin Nutr. 2014;99(3):543–50.
Touyz LM, Wakefield CE, Grech AM, Quinn VF, Costa DSJ, Zhang FF, et al. Parent-targeted home-based interventions for increasing fruit and vegetable intake in children: a systematic review and meta-analysis. Nutr Rev. 2018;76(3):154–73.
Habler SB, Major L, Hennessy S. Tablet use in schools: a critical review of the evidence for learning outcomes. J Comput Assisted Learn. 2015;32:139–56.
Western MJ, Armstrong MEG, Islam I, Morgan K, Jones UF, Kelson MJ. The effectiveness of digital interventions for increasing physical activity in individuals of low socioeconomic status: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2021;18(1):148.
Mair JL, Salamanca-Sanabria A, Augsburger M, Frese BF, Abend S, Jakob R, et al. Effective behavior change techniques in digital health interventions for the prevention or management of Noncommunicable diseases: an umbrella review. Ann Behav Med. 2023;57(10):817–35.
Rosi A, Scazzina F, Ingrosso L, Morandi A, Del Rio D, Sanna A. The, “5 a day” Game: A Nutritional Intervention Utilizing, Innovative Methodologies with Primary School Children. Int J Health Promot Educ. 2015;66:713–7.
Head KJ, Noar SM, Iannarino NT, Grant HN. Efficacy of text messaging-based interventions for health promotion: A meta-analysis. Soc Sci Med. 2013;1(97):41–8.
Chai L, Collins C, May C, Holder C, Brown L, Burrows T. An online telehealth nutrition intervention to support parents in child weight management - A randomised feasibility controlled trial. Obes Facts. 2019;12:111–2.
Schoeppe CS, Alley S, Lippevelde W, Bray NA, Williams SL, Duncan MJ, Vandelanotte C. Efficacy of Interventions that use Apps to Improve Diet, Physical Activity and Sedentary Behaviour: a systematic review. Int J Behav Nutr Phys Act. 2016;13:127.
Suleiman-Martos N, García-Lara RA, Martos-Cabrera MB, Albendín-García L, Romero-Béjar JL, De la CañadasFuente GA, et al. Gamification for the Improvement of Diet, Nutritional Habits, and Body Composition in Children and Adolescents: a systematic review and meta-analysis. Nutrients. 2021;13(7):2478.
Lin H, Xu D, Yang M, Ma X, Yan N, Chen H, et al. Behaviour change techniques that constitute effective planning interventions to improve physical activity and diet behaviour for people with chronic conditions: a systematic review. BMJ Open. 2022;12(8):e058229.
Samdal GB, Eide GE, Barth T, Williams G, Meland E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int J Behav Nutr Phys Act. 2017;14(1):42.
Nathan N, Yoong SL, Sutherland R, Reilly K, Delaney T, Janssen L, et al. Effectiveness of a multicomponent intervention to enhance implementation of a healthy canteen policy in Australian primary schools: a randomised controlled trial. Int J Behav Nutr Phys Act. 2016;13(1):106.
Verdonschot A, Follong BM, Collins CE, de Vet E, Haveman-Nies A, Bucher T. Effectiveness of school-based nutrition intervention components on fruit and vegetable intake and nutrition knowledge in children aged 4–12 years old: an umbrella review. Nutr Rev. 2023;81(3):304–21.
Lorenc T, Petticrew M, Welch V, Tugwell P. What types of interventions generate inequalities? Evidence from systematic reviews. J Epidemiol Community Health. 2013;67(2):190.
Hariton E, Locascio JJ. Randomised controlled trials – the gold standard for effectiveness research. BJOG. 2018;125(13):1716–1716.
Jäggi L, Aguilar L, Llatance MA, Castellanos A, Fink G, Hinckley K, et al. Digital tools to improve parenting behaviour in low-income settings: a mixed-methods feasibility study. Arch Dis Child. 2023;108(6):433.
Kaur J, Kaur M, Chakrapani V, Kumar R. Multilevel Influences on Fat, Sugar, Salt, Fruit, and Vegetable Consumption Behaviors Among Urban Indians: application of the social ecological model. SAGE Open. 2020;10(2):2158244020919526.
Jenkins CL, Imran S, Mahmood A, Bradbury K, Murray E, Stevenson F, et al. Digital Health Intervention Design and Deployment for Engaging Demographic Groups Likely to Be Affected by the Digital Divide: Protocol for a Systematic Scoping Review. JMIR Res Protoc. 2022;11(3):e32538.
Acknowledgements
Not applicable
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HF conceived and designed the study. HF and EN contributed to Additional file 4. EN, KLC and HF contributed and data analysis. EN, KLC and WM played a supervisory role in the review and editing of the manuscript. All authors provided input into the final version of the manuscript.
Author’s information
The research team are academics with a range of backgrounds in behavioural science, health psychology and sociology.
Corresponding authors
Ethics declarations
Ethics and approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
PRISMA 2020 checklist.
Additional file 2:
Search strategy.
Additional file 3:
Study intervention BCIO and BCT characteristics.
Additional file 4:
BCIO data extraction template.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Froome, H., Cheung, K.L., Martin, W. et al. Identifying and characterising digital behaviour change interventions to improve fruit and vegetable intake in low-socioeconomic status primary school children: a systematic review. BMC Digit Health 2, 29 (2024). https://doi.org/10.1186/s44247-024-00085-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44247-024-00085-w