
Abstract
Background
Pulmonary arterial hypertension (PAH) is a common complication of chronic obstructive pulmonary disease (COPD), which can lead to shorter survival and poor clinical outcomes. Patients suffering from PAH display a cardiopulmonary exercise testing (CPET) profile with several atypical factors, such as decreased work rate, limited ability to do aerobic activities, and ventilatory insufficiency.
Objectives
To assess and compare exercise tolerance by CPET in COPD patients with secondary PAH receiving cGMP-specific phosphodiesterase type-5 (PDE-5) inhibitor (sildenafil) versus those who are receiving standard-of-care only.
Patients and methods
This is a prospective, cross-sectional research in which a total of 30 COPD patients with mild to severe obstruction and secondary PAH were recruited; all patients were treated with standard-of-care treatment for COPD; moreover, half of the recruited patients were also on sildenafil 60 mg/day for at least 3 months at the time of recruitment (sildenafil users) as specific therapy for PAH while the other half were not (non-users). All patients underwent CPET to assess their exercise capacity.
Results
No significant statistical differences were observed between sildenafil users and non-users in all CPET parameters except in respiratory exchange ratio (RER) during both exercise and recovery with sildenafil users showing a lower RER in both phases compared to non-users (p = 0.02, 0.01, respectively). Also, resting diastolic blood pressure (DBP) was significantly lower in sildenafil users (p = 0.02). In addition, sildenafil users did not exhibit significant differences compared to non-users in terms of Modified Medical Research Council (mMRC) score, COPD assessment test (CAT) score, or spirometric parameters.
Conclusion
Our findings suggest that there were no significant differences in overall exercise capacity, nor in symptoms or spirometric parameters between COPD patients with secondary PAH receiving sildenafil and those who were not.
Similar content being viewed by others

Introduction
PAH, a common complication in COPD, is categorized as group three in the World Health Organization (WHO) categorization and is linked to low oxygen levels. It is characterized by elevation in resting mean pulmonary artery pressure (mPAP) more than 20–25 mmHg [1]. It can lead to shorter survival and poor clinical outcomes [2].
Though it usually develops slowly and is usually moderate in severity, transient elevations in pulmonary artery pressure may transpire during exacerbations, physical activity, or sleep. Despite PAH, there is only a mild impairment in right ventricular function, and cardiac output remains unchanged [3].
Similar to patients who have idiopathic PAH, a subgroup of COPD patients with mild airflow obstruction exhibits severe PAH that reaches disproportionate high values. Clinical judgement, using a multidimensional evaluation, is required to differentiate between cases exhibiting a “pulmonary vascular phenotype” and those with co-existing PAH [3].
There is evidence that the presence of pulmonary endothelial dysfunction, occurring in the early phases of the disease, initiates a sequence of alterations that result in PAH; this dysfunction is usually in the form of an imbalance which occurs in the endothelial synthesis, with an increase in levels of factors that induce vasoconstriction, facilitate the deposition of extracellular matrix in the arterial wall, and promote cell proliferation [3].
This pulmonary vessel remodeling is the primary cause of PAH, and it has been detected in various stages of disease severity mainly affecting small and precapillary arteries [4].
The most characteristic feature of pulmonary vascular remodeling in patients with COPD is hyperplasia of the muscular arteries’ intimal layer. This is caused by the deposition of elastic and collagen fibers and smooth muscle cells (SMC) proliferation, which in their progressed phases form bundles of longitudinal muscle which are different from the typical circumferential arrangement [5].
Recent research highlights the association of endothelial inflammation and dysfunction to the presence and progression of PAH in patients with COPD [6].
Sildenafil is a well-known pulmonary vasodilator primarily used to manage PAH by relaxing the smooth muscles in the pulmonary arteries, leading to vasodilation and improved blood flow [7].
This work aimed to assess and compare exercise tolerance via CPET in COPD patients with secondary PAH receiving cGMP-specific phosphodiesterase type-5 (PDE-5) inhibitor (sildenafil) as specific therapy for PAH versus those who are not.
Patients and methods
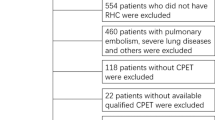
This study is a prospective cross-sectional research which was conducted at Ain Shams University Hospital, Chest Department, during the period between July 2022 and January 2024; a total of 30 COPD patients with mild to severe obstruction according to Global Initiative for Chronic Obstructive Lung Diseases (GOLD) 2022 [8] and secondary PAH as assessed by echocardiography (ECHO) (right ventricular systolic pressure (RVSP) > 30 mmHg) were recruited to the study; 15 patients (50%) were already receiving sildenafil 60 mg/day for at least 3 months at the time of recruitment (sildenafil users) in addition to standard COPD treatment, while the other 15 patients (50%) were not on any pulmonary hypertension-specific medication (non-users).
All patients underwent CPET, performed at CPET Unit, Ain Shams Specialized Hospital, with selected protocol according to the European Respiratory Society (ERS) guidelines, 2019 [9]: RA_(20W-min) (EFVL-3, BP-2) in which there is automated increase by 20 W in workload every 1 min, assessment of exercise flow volume loop every 3 min, and measurement of blood pressure every 2 min with automated workload. The test was terminated if any of the following occurred:
-
Cardiac events such as chest pain or ischemic echocardiographic changes, arrhythmias, and second or third-degree heart block
-
Hemodynamic events: systolic pressure decreases > 20 mmHg from the highest value recorded, systolic blood pressure increases > 250 mmHg; diastolic blood pressure increases > 120 mmHg
-
Respiratory events: arterial oxygen desaturation, (\(\leq\) 80%) especially if associated with symptoms and signs of severe hypoxemia, respiratory failure;and also if there is loss of coordination; dizziness or fainting ; mental confusion; or sudden pallor [10]
Exclusion criteria
Patients with very severe COPD (FEV1 < 30%), severe PAH (RVSP > 60 mmHg), patients with respiratory failure or receiving oxygen therapy, and patients with severe systemic disease (heart failure, advanced renal or liver disease) were all excluded from the study, also if there is an absolute contraindication to CPET [10].
Data collection
The data included are: full history, clinical examination, CAT score, mMRC score, echocardiographic parameters, post-bronchodilator spirometry, and CPET measurements (usingVyntus TM CPX, serial number 42630285, Vyaire Medical products Ltd,UK).
Ethical considerations
All participants gave informed written consent before participating in the study, and the study protocol was accepted by the Institutional Research & Medical Ethics Committee, Ain Shams University (with serial number FMASU MD 182/2022).
Statistical methods
Data were initially gathered in an Excel spreadsheet before being encoded in preparation for additional analysis utilizing version 26 of the SPSS statistical software (IBM Corp., Armonk, NY, USA). Data normality was examined via the Shapiro–Wilk test. Numerical data were represented as mean and standard deviation (SD), while categorical data were conveyed as number and percentage. Comparing the means of both groups was done using independent t-test, while a chi-square test was used to examine the frequencies of both groups. P-values less than 0.05 were deemed to be statistically significant.
Results
Table 1 shows that there was not a statistically significant difference among sildenafil users and non-users in most of the demographic characteristics, CAT score, mMRC score, spirometric parameters, and ECHO findings except for RVSP where sildenafil users exhibited a statistically significant higher mean RVSP compared to non-users, (44.33 ± 7.04 and 35.6 ± 5.5 mmHg, respectively, with p = 0.001).
Also in comorbidities, only one patient (sildenafil user) exhibited hepatic dysfunction (before administering sildenafil), in contrast to six patients (non-users), three patients with old tuberculosis (TB), two cases had chronic kidney disease (CKD), and one patient with hepatic dysfunction) (p = 0.03).
Table 2 demonstrates that most CPET parameters, including measures of exercise capacity and cardiovascular function, do not show significant differences between sildenafil users and non-users; however, there was a statistically significant reduction in RER during exercise as well as during recovery among sildenafil users compared to non-users; the mean of RER during exercise was 1 ± 0.08 in users versus 1.09 ± 0.12 in non-users (p = 0.02), while in recovery, the mean RER was 1.04 ± 0.09 in users versus 1.15 ± 0.03 in non-users (p = 0.01).Moreover, resting diastolic blood pressure was significantly lower in sildenafil users compared to non -users with a mean of 66.87 ± 9.18 versus 75.3 ± 10.4 mmHg respectively (p = 0.02).
Moreover, resting diastolic blood pressure (DBP) was significantly lower in sildenafil users with a mean of 66.87 ± 9.18 versus 75.3 ± 10.4 mmHg in non-users, p = 0.02).
Table 3 displays the CPET data of the of all the 30 enrolled patients; the mean MVV was 55.96 ± 16.46 L/min, the mean VO2/kg was 14.63 ± 3.61 ml/min/kg (normal range > 20 ml/min/kg), the mean percentage of VO2/kg% Pred Max was 54.60% ± 9.36 (normal range > 85%), the mean VE max was 38.70 ± 9.36 L/min with VE max% pred 47.33% (normal range > 85%), the average peak workload reaching 62.03 Watts, the mean percentage of peak workload% pred max was 48.57% ± 13.97 (normal range > 80%), and the oxygen saturation levels, both before and after exercise, consistently fell within normal ranges.
Discussion
Our study enrolled 30 patients with mild to severe COPD obstruction. These patients were also diagnosed with secondary PAH, based on echocardiography, with an estimated RVSP of more than 30 mmHg. Fifty percent of the recruited patients were on standard-of-care for COPD without any pulmonary hypertension-specific medication, while the other half were receiving sildenafil 60 mg/day for at least 3 months in addition to conventional COPD treatment. All patients underwent CPET to assess their exercise capacity, with the aim of comparing the exercise tolerance in those receiving sildenafil (as PAH-specific therapy) versus those who were not. In COPD patients, disease severity is typically assessed through clinical features and spirometry at rest, yet this often fails to predict exertional tolerance accurately, and this highlights the importance of CPET which stands as the gold standard for evaluating exercise tolerance in providing insights into cardiopulmonary function in this group of patients [11].
Comparison between patients utilizing sildenafil and those who were not showed insignificant difference regarding most of the demographic features, apart from certain comorbidities where one patient in the sildenafil group exhibited hepatic dysfunction (before administering sildenafil), in contrast to six patients, three patients with old tuberculosis (TB), two cases with chronic kidney disease, and one patient with hepatic dysfunction in the non-sildenafil users (p = 0.03). Moreover, both groups were harmonized with respect to CAT score, mMRC, spirometric parameters, and echocardiographic data. Yet, sildenafil users had a higher mean RVSP compared to non-users, with a statistically significant difference, p = 0.001. Similarly, in a randomized control trial by Lederer et al. [12] which focused on COPD patients without secondary pulmonary hypertension, sildenafil use for 4 weeks did not show a significant alteration in mMRC, CAT score, and pulmonary function compared to placebo users. They concluded that the use of sildenafil does not significantly impact pulmonary function in cases with COPD, unrelatedly of the occurrence of secondary pulmonary hypertension. They added that, while sildenafil may have effects on pulmonary vasculature and gas exchange, it does not appear to substantially influence overall pulmonary function parameters such as FEV1 or FVC in these patients.
Additionally, a study by Vitulo and coworkers [13], in which they evaluated the efficacy of sildenafil on pulmonary hemodynamics in severe PAH related to chronic obstructive pulmonary disease (by right heart catheter, 6MWT, DLco), found significant reduction in pulmonary vascular resistance (PVR) with enhancement in mMRC, cardiac index, BODE index, stroke volume, 6MWD, and quality of life (QOL) without change in pulmonary functions in the sildenafil group in comparison with the placebo group following 16 weeks of management. While in our study, there was no difference between sildenafil users and non-sildenafil users regarding CPET parameters and spirometric parameters.
The CPET multifaceted assessment data of the 30 recruited COPD patients in the present study revealed valuable insights into their functional capacities. Notably, the average minute ventilation during peak exercise stood at 55.96 L/min, reflecting their respiratory effort, characterized by a moderate degree of variability. Concurrently, the average oxygen consumption per kilogram of body weight reached 14.63 ml/min/kg(normal range > 20 ml/min/kg); the mean percentage of predicted maximum oxygen consumption reached 54.60% (normal range > 85%), which means that oxygen consumption was moderately impaired in all patients; the average maximum minute ventilation was 38.70 L/min, with the corresponding average percentage of predicted maximum minute ventilation standing at 47.33% (normal range > 85%), and this means that there was moderate to severe decrease in maximum minute ventilation; the average peak workload reached 62.03 Watts, with the corresponding average percentage of predicted maximum 48.57% (normal range > 80%), which was decreased in all patients. In brief, there was a decrease in most of the exercise capacity parameters (such as peak oxygen consumption, maximum workload, and maximum minute ventilation) in all enrolled patients. In the recovery phase, the average oxygen consumption was 11.79 ml/min/kg. The oxygen saturation levels both before and after exercise consistently fell within normal ranges, attesting to the effective delivery and utilization of oxygen throughout the testing.
Furthermore, most CPET parameters, including measures of exercise capacity and cardiovascular function, do not prove significant statistical differences between sildenafil users and non-users (p-value > 0.05), except for the significant reduction in respiratory exchange rate (RER) during both exercise and recovery phases among sildenafil users compared to non-users (p = 0.02, 0.01, respectively). Also, resting diastolic blood pressure (DBP) was significantly decreased in sildenafil users compared to non-users (p = 0.02). These findings suggested that there may be some influence of sildenafil on the respiratory response during exercise recovery. Also, sildenafil use might have an impact on baseline blood pressure. Moreover, the lower recovery RER in sildenafil users might suggest a metabolic shift favoring fat utilization during the recovery phase. This metabolic pattern could have implications for energy metabolism, endurance, and recovery processes in individuals using sildenafil.
In agreement of the above-mentioned findings, Torres-Castro et al. [14] found that patients with COPD and pulmonary hypertension exhibit significantly lower exercise tolerance compared to those with COPD but without pulmonary hypertension. Key indicators of exercise capacity, such as peak oxygen consumption, maximum workload, and oxygen pulse, were notably reduced in the COPD patients suffering from pulmonary hypertension. The authors underscored the effects of pulmonary hypertension on the exercise tolerance of COPD patients.
On the other hand, in line with our research, Abdel Kader et al. [15], who evaluated the effect of sildenafil as a modality of treatment in cases with chronic pulmonary hypertension via CPET, found no significant improvement after sildenafil therapy among patients with COPD as regards CPET parameters.
Another prospective cross-sectional research done by Mohamed et al. [16] evaluating the effect of pulmonary hypertension on exercise capacity among cases with COPD showed significantly lower CPET parameters (VO2, oxygen pulse) among COPD-pulmonary hypertension patients in comparison to COPD patients only. Nevertheless, the scope of the present research was different, as we concentrated on the effect of Sildenafil use on patients with secondary PAH attributed to COPD on CPET parameters.
Rietema et al. [17], in their randomized controlled trial (RCT) which consisted of overall 15 stable COPD cases, evaluated the enrolled patients by right heart catheterization, magnetic resonance imaging (MRI), a CPET, and a test of 6-min walking distance. MRI and exercise tests occurred again 12 weeks following initiating oral treatment with 50 mg of sildenafil three times daily. It was determined that sildenafil medication had no discernible impact on either stroke volume or exercise capacity. While COPD cases with related PAH had a lower stroke volume than those without PAH, there was no significant variance in response to therapy among both groups, and these results are also consistent with ours.
Also, Holverda et al. [18] researched the immediate effects of a single dose of sildenafil on the changes in pulmonary artery pressure (mPAP) and exercise capacity in individuals with COPD and PAH. They also used right heart catheter, MRI, CPET, and 6MWD for assessment. They found that sildenafil attenuated the rise in MPAP within submaximal exercise, regardless of baseline MPAP levels. However, it does not translate into significant improvements in exercise performance or cardiovascular function.
It is worth mentioning that both aforementioned studies focused on investigating the impacts of sildenafil on exercise capacity and cardiovascular function in COPD patients; they focus on different aspects. They primarily examine the impact of sildenafil on PAP within exercise, while the current study explored a broader range of parameters, including metabolic responses and blood pressure changes associated with sildenafil use.
A meta-analysis had been conducted by Chen et al. [19] evaluating the effectiveness of (PAH)-specific therapies in (COPD) by right heart catheterization and 6MWT. The study included nine trials with an average of 365 subjects for analysis, most of them treated with sildenafil or bosentan for 4 to 18 months. The main findings were that PAH-specific therapy enhanced exercise capacity and reduced PAP, especially in COPD cases with severe PAH, although it did not significantly improve hypoxemia or life quality, though dyspnea was alleviated. It came with contrast with our results.
Limitations
A single-center research design was utilized with a rather small sample size and a relatively brief duration. However, it is worth noting that there were no statistically significant variances in baseline characteristics among both groups, so this factor did not impact the results.
Conclusion
Our findings suggest that sildenafil usage did not significantly impact overall CPET variables, nor symptoms, or spirometric parameters in COPD patients with secondary PAH.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author.
Abbreviations
- 6MWD:
-
6-Minute walking distance
- AIDS:
-
Acquired immunodeficiency syndrome
- BODE:
-
Body mass index, lung obstruction, dyspnea, and exercise capacity
- BMI:
-
Body mass index
- BR:
-
Breathing reserve
- BP:
-
Blood pressure
- CAT:
-
COPD assessment test
- COPD:
-
Chronic obstructive pulmonary disease
- CKD:
-
Chronic kidney disease
- CPET:
-
Cardiopulmonary exercise testing
- CGMP:
-
Cyclic guanosine monophosphate
- DLCO:
-
Diffusion capacity of the lungs for carbon monoxide
- DBP:
-
Diastolic blood pressure
- DM:
-
Diabetes mellitus
- e.g.:
-
Exempli gratia
- ECHO:
-
Echo cardiography
- EFVL:
-
Exercise flow volume loop
- ERS:
-
European Respiratory Society
- FVC:
-
Forced vital capacity
- FEVI:
-
Forced expiratory volume in the first second
- GOLD:
-
Global Initiative for Chronic Obstructive Lung Disease
- HIV:
-
Human immunodeficiency virus
- HR:
-
Heart rate
- HRmax:
-
Maximal heart rate
- HRR:
-
Heart rate reserve
- HTN:
-
Hypertension
- LVESD:
-
Left ventricular end-systolic dimension
- LVEDD:
-
Left ventricular end-diastolic dimension
- LVEF:
-
Left ventricular ejection fraction
- MEF50%:
-
Maximal expiratory flow at 50%
- MG:
-
Milligram
- mPAP:
-
Mean pulmonary artery pressure
- MMRC:
-
Modified Medical Research Council
- MRI:
-
Magnetic resonance imaging
- MVV:
-
Maximal voluntary ventilation
- N:
-
Number
- O2 pulse:
-
Oxygen pulse
- PAP:
-
Pulmonary artery pressure
- PDE5:
-
Phosphodiesterase type-5
- PETCO2:
-
End-tidal carbon dioxide partial pressure
- PAH:
-
Pulmonary arterial hypertension
- PREd max:
-
Predicted maximum
- QOL:
-
Quality of life
- PVR:
-
Pulmonary vascular resistance
- RA:
-
Ramp
- RCTs:
-
Randomized controlled trial
- RR:
-
Respiratory rate
- RER:
-
Respiratory exchange ratio
- RVSP:
-
Right ventricular systolic pressure
- SD:
-
Standard deviation
- SL:
-
Slope
- SMC:
-
Smooth muscle cells
- SPO2:
-
Oxygen saturation
- T.b:
-
Tuberculosis
- TID:
-
Three times a day
- V.E:
-
Minute ventilation
- VC:
-
Vital capacity
- VO2:
-
Oxygen uptake or oxygen consumption
- VCO2:
-
Carbon dioxide output or production
- VEmax:
-
Maximal minute ventilation
- VT:
-
Tidal volume
- WHO:
-
World Health Organization
- WR:
-
Work rate
References
Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M et al (2019) Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 2019(53):1801913
Gredic M, Blanco I, Kovacs G, Helyes Z, Ferdinandy P, Olschewski H et al (2021) Pulmonary hypertension in chronic obstructive pulmonary disease. Br J Pharmacol. 178(1):132–151
Blanco I, Tura-Ceide O, Peinado VI, Barberà JA (2020) Updated perspectives on pulmonary hypertension in COPD. Int J Chron Obstruct Pulmon Dis. 15:1315–1324
Santos S, Peinado VI, Ramirez J, Melgosa T, Roca J, Rodriguez-Roisin R, Barbera JA (2002) Characterization of pulmonary vascular remodeling in smokers and patients with mild COPD. Eur Respir J 19(4):632–638
Peinado VI, Gómez FP, Barberà JA, Roman A, Montero MA, Ramírez J, Rodriguez-Roisin R (2013) Pulmonary vascular abnormalities in chronic obstructive pulmonary disease undergoing lung transplant. J Heart Lung Transplant 32(12):1262–1269
Shujaat A, Bajwa AA, Cury JD (2012) Pulmonary hypertension secondary to COPD. Pulm Med 2012:203952. https://doi.org/10.1155/2012/203952
Hao Y, Zhu Y, Mao Y, Xu J, He X, Huang S, Qiu J (2020) Efficacy and safety of sildenafil treatment in pulmonary hypertension caused by chronic obstructive pulmonary disease: a meta-analysis. Life Sci 257:118001
Global Initiative for Chronic Obstructive Lung Disease (GOLD) (2022): global strategy for the diagnosis, management and prevention of COPD. Retrieved from http://www.goldcopd.org/
Radtke T, Crook S, Kaltsakas G, Louvaris Z, Berton D, Urquhart DS et al (2019) ERS statement on standardization of cardiopulmonary exercise testing in chronic lung diseases. Eur Respir Rev 28:180101. https://doi.org/10.1183/16000617.0101-2018
Datta D, Normandin E, ZuWallack R (2015) Cardiopulmonary exercise testing in the assessment of exertional dyspnea. Ann Thorac Med 10(2):77–86. https://doi.org/10.4103/1817-1737.151438
Arena R, Sietsema KE (2011) Cardiopulmonary exercise testing in the clinical evaluation of patients with heart and lung disease. Circulation 123(6):668–680
Lederer DJ, Bartels MN, Schluger NW, Brogan F, Jellen P, Thomashow BM, Kawut SM (2012) Sildenafil for chronic obstructive pulmonary disease: a randomized crossover trial. COPD 9(3):268–275
Vitulo P, Stanziola A, Confalonieri M, Libertucci D, Oggionni T, Rottoli P et al (2017) Sildenafil in severe pulmonary hypertension associated with chronic obstructive pulmonary disease: a randomized controlled multicenter clinical trial. J Heart Lung Transplant. 36(2):166–174
Torres-Castro R, Gimeno-Santos E, Vilaró J, Roqué-Figuls M, Moisés J, Vasconcello-Castillo L et al (2021) Effect of pulmonary hypertension on exercise tolerance in patients with COPD: a prognostic systematic review and meta-analysis. Eur Respir Rev 30(160):200321
Abd Elkader MA, Khattab AM, Mohamed Y M, GAD MH, Galal IHE (2011). Role of cardiopulmonary exercise testing in assessment of patients with chronic pulmonary hypertension http://srv3.eulc.edu.eg/eulc_v5/Libraries/Thesis/BrowseThesisPages.aspx?fn=PublicDrawThesis&BibID=12181036.
Mohamed AZE, Shaaban L, Abdalah AEE, Tohamy AM, Khaleel WG (2024) Evaluation of exercise capacity in chronic obstructive pulmonary disease patients with pulmonary hypertension. Egypt J Chest Dis Tuber 73(1):54–64
Rietema H, Holverda S, Bogaard HJ, Marcus JT, Smit HJ, Westerhof N et al (2008) Sildenafil treatment in COPD does not affect stroke volume or exercise capacity. Eur Respir J 31(4):759–764
Holverda S, Rietema H, Bogaard HJ, Westerhof N, Postmus PE, Boonstra A, Vonk-Noordegraaf A (2008) Acute effects of sildenafil on exercise pulmonary hemodynamics and capacity in patients with 558–56l. Pulm Pharmacol Ther 21(3):558–564
Chen X, Tang S, Liu K, Li Q, Kong H, Zeng X, Wang H (2015) Therapy in stable chronic obstructive pulmonary disease patients with pulmonary hypertension: a systematic review and meta-analysis. J Thorac Dis 7(3):309–319
Acknowledgements
The authors would like to acknowledge all those who shared in data acquisition.
Funding
Nil.
Author information
Authors and Affiliations
Contributions
DI collected the patients data, performed the analytical methods and drafted the initial manuscript. YM, HM, RM reviewed the collected data and statistical analysis, contributed in writing and finalizing the manuscript. The authors read and approved the final manuscript. RM published the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The ethics committee of Ain Shams University, Faculty of Medicine, approved the study, ethical approval number FMASU MD 182/2022. All participants gave written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Darwish, D.I., Moustafa, Y., Abdel-Hamid, H.M. et al. Assessment of exercise tolerance using cardiopulmonary exercise test in patients with chronic obstructive pulmonary disease and secondary pulmonary arterial hypertension treated with Sildenafil versus those receiving only standard-of-care. Egypt J Bronchol 18, 57 (2024). https://doi.org/10.1186/s43168-024-00307-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-024-00307-9