
Abstract
Background
Chronic inflammation plays a crucial role in developing various cardiovascular and metabolic disorders. Obstructive sleep apnea (OSA) is a unique condition characterized by the coexistence of cardiovascular and metabolic disturbances, where chronic inflammation may exacerbate disease progression and severity. This study investigated how different hematological inflammatory cells and mediators can serve as predictive indicators of severe OSA.
Methods
In a retrospective cohort study, 150 patients suspected of having obstructive sleep apnea (OSA) underwent polysomnography (PSG) to confirm the diagnosis. Based on their apnea-hypopnea index (AHI), the patients were categorized into three groups: mild, moderate, and severe OSA. Blood samples were collected for the assessment of inflammatory blood cells and mediators at the time of diagnosis.
Results
Among the 150 patients studied, 90 were diagnosed with OSA, and 43 had severe OSA, representing a prevalence rate of 47.7%. Patients with severe OSA were notably older and more likely to have diabetes mellitus and hypertension. After adjusting for age and sex, each one-unit increase in Systemic Inflammatory Response Index (SIRI), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) levels was associated with a doubling in the likelihood of having moderate and severe OSA (p < 0.05 for all). However, hypertension was linked to a 16-fold increase in the likelihood of moderate and severe OSA (p = 0.01).
Conclusion
Our research indicates that comorbidity and inflammatory cells and markers (SIRI, CRP, and ESR) are significantly related to the severity of OSA.
Similar content being viewed by others

Introduction
Sleep apnea is a prevalent sleep disorder that can impact individuals of all ages, although it is more frequently observed in older adults [1]. This condition is defined by repeated interruptions in breathing during sleep, potentially resulting in various complications. These complications may include daytime fatigue, excessive drowsiness, a heightened risk of cardiovascular disease, sudden drops in blood oxygen levels, challenges with specific medications like sedatives and painkillers, and an elevated likelihood of post-surgical complications due to the relaxing effects of general anesthetics on the upper airway [2].
Sleep apnea is a complex condition with various risk factors such as obesity, family history, allergies, and enlarged tonsils. Healthcare professionals typically conduct an overnight sleep study to diagnose this condition. During this study, they closely monitored for more than five episodes per hour, classified as “apneas” when there is a complete or near-complete cessation of breathing and “hypopneas” when there is a partial reduction in breathing [3].
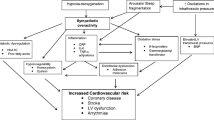
Obstructive Sleep Apnea (OSA) occurs when the upper airway is partially or completely blocked during sleep, causing irregular or interrupted breathing patterns, it can lead to decreased oxygen levels and increased carbon dioxide levels in the bloodstream, which can trigger various physiological responses such as heightened oxidative stress, adrenergic activation, endothelial dysfunction, metabolic dysregulation, endocrine system activation, increased clotting tendencies, and chronic systemic inflammation [4, 5]. Additionally, chemoreceptors in the bloodstream detect elevated carbon dioxide levels, signaling the brain to awaken the person. This arousal clears the airway, resuming normal breathing and restoring oxygen levels. Afterward, the person typically falls back asleep [4].
Obstructive sleep apnea (OSA) severity and treatment outcomes are commonly assessed using AHI [6]. AHI calculates the average number of apneas and hypopneas per hour of sleep. The American Academy of Sleep Medicine (AASM) defines three severity categories based on AHI scores [7]: mild (5–15 events/h), moderate (15–30 events/h), and severe (> 30 events/h).
Chronic inflammation is pooled in various diseases, including metabolic disorders, neurodegenerative disorders, cancer, and cardiovascular diseases [8]. The inflammatory response involves a complex sequence of events, including cellular and vascular changes and the release of specific humoral secretions [9]. Immune cells release mediators such as histamine, prostaglandins, leukotrienes, free radicals, and serotonin as part of this process [10].
Chronic inflammation is characterized by the infiltration of mononuclear cells, such as monocytes and lymphocytes, fibroblast proliferation, and collagen formation [8]. In chronic inflammation, tissue damage is often caused by nitrogen and oxygen-reactive species from infiltrated inflammatory cells [11].
Systemic inflammatory markers like the platelet/lymphocyte ratio (PLR), neutrophil/lymphocyte ratio (NLR), monocyte/lymphocyte ratio (MLR), and the systemic inflammation response index (SIRI) have emerged as valuable independent prognostic indicators in various diseases [12,13,14,15]. SIRI, introduced in 2016, is calculated using routine blood samples and effectively reflects cancer-related inflammatory responses, making it a noninvasive, cost-effective, and readily accessible tool [16].
Initially developed for predicting survival in advanced pancreatic cancer patients following chemotherapy, SIRI's utility has expanded to assess systemic inflammation in multiple cancer types [16, 17]. By 2019, eleven studies and a systematic review had collectively established that pretreatment SIRI is a useful predictive marker for adverse prognosis in cancer patients [18].
Recent research discovered the connection between obstructive sleep apnea (OSA) and specific inflammatory biomarkers. Two noteworthy biomarkers, C-reactive protein (CRP) and fibrinogen, which play crucial roles in inflammation and coagulation [19,20,21], have shown a direct relationship with the severity of OSA as measured by the apnea-hypopnea index (AHI) and arousal index (AI). Conversely, these biomarkers exhibit an inverse association with mean and lowest oxygen saturation levels during sleep [22]. Another biomarker under investigation is erythrocyte sedimentation rate (ESR), which gauges the tendency of red blood cells to clump together [23, 24]. Fleming et al. have postulated that various combinations of these biomarkers may offer more robust insights into OSA, potentially serving as physiological signatures of the disorder that could benefit initial OSA screening and subsequent monitoring [25].
The present study highlighted the inflammatory aspects of patients with severe OSA and tried to find some independent predictors of disease severity.
Methods
Patients and study design
A retrospective cohort study was conducted at the sleep lab of King Fahad Specialist Hospital in Buraidah, Qasim, Saudi Arabia, between June 2022 and 2023. The study included OSA-confirmed cases (27), via PSG (Alice 6 LDx Machine connected with Sleepware G3 program from Philips company), excluding those under 18 years and with autoimmune disease, hepatic and renal dysfunction, malignancy, and other sleep-related disorders.
Measurement and endpoint
The endpoint of the study was detecting severe OSA group; the severity of OSA was classified according to the AHI index [7].
The basic demographic data of the recruited patients were collected in an Excel sheet. Additionally, the full and differential blood count at the time of diagnosis was collected from the patient’s file as well as the CRP and ESR. The inflammatory ratios were measured automatically via the specialized formula in an Excel sheet. Hence, NLR was equal to (Neutrophil/Lymphocyte) number, PLR was equal to (Platelets/Lymphocyte) number, and SIRI was equal to (Neutrophil × Monocytes)/lymphocytes.
Ethics approval, IRB number, and consent to participate
Ethical approval has been obtained from the ethical committee office, King Fahad Specialist Hospital, Buraidah, Qasim, Saudi Arabia, (No: 607-45-3465) in accordance with the Helsinki Declaration protocol. Informed consent has been obtained from all participants involved in the study, as well as their legal guardians, to ensure that they are fully aware of the nature and purpose of the research, and have given their voluntary and informed consent to participate.
Statistical analysis
The data was collected in an Excel sheet and analyzed using Sigma Plot for Windows version 12.5.0.38 (Systat Software, Inc, UK, 2011). The normality of the data was measured using the Shapiro-Wilk test. A one-way ANOVA test or Kruskal Wallis test was used to compare means, while a Chi-square test was used to compare frequencies. The Pearson correlation coefficient was used to find the correlation between AHI and other inflammatory cells and markers. General linear model and Logistic regression analysis with backward elimination technique were used to evaluate the impact of inflammatory cells and markers on AHI and detecting severe OSA. All tests were two-sided, and a p value < 0.05 was considered significant.
Results
Characteristics of patients with OSA
Table 1 showed that patients with moderate and severe OSA were significantly older and had associated comorbidities such as diabetes mellitus (DM) and hypertension (HTN) compared to those with mild OSA. The p values were 0.02 and 0.001 for age, and 0.03 and 0.001 for DM and HTN, respectively. However, there was no significant difference between males and females (p = 0.76).
Inflammatory aspect of OSA in correlation with disease severity
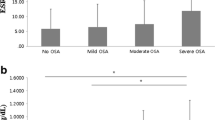
Table 2 revealed that across the different severity groups of OSA, lymphocyte count, platelet count, and PLR showed a significant difference between the groups, p = 0.01 for all; however, considering their linear relationship with AHI, only PLT has a significant negative correlation, r = − 0.23, p = 0.03 (Fig. 1) (Supplementary Table 1). On the other hand, neither neutrophils nor NLR revealed any significant difference across the groups of OSA, yet, in Fig. 2, both neutrophils and NLR showed a significant positive linear relationship, r = 0.31 and 0.37, respectively, p = 0.001 for both. Moreover, despite an insignificant difference in SIRI between the OSA groups, it showed a significant positive correlation with AHI; r = 0.39, p = 0.001 (Fig. 3). Furthermore, the inflammatory markers CRP and ESR, which are first-phase reactants, significantly increased in moderate and severe OSA compared to mild OSA (Table 2, p < 0.05). Both markers demonstrated a significant positive linear relationship with AHI (Fig. 4), with r = 0.61 and 0.54 and p < 0.001 for both, respectively.

PLT in correlation with AHI. *The test of significance: Pearson correlation coefficient, the direction before "r" denoting the direction of relationship, p < 0.05 considered significant

Neutrophils and NLR in correlation with AHI. *The test of significance: Pearson correlation coefficient, the direction before “r” denoting the direction of relationship, p < 0.05 considered significant

SIRI in correlation with AHI. *The test of significance: Pearson correlation coefficient, the direction before “r” denoting the direction of relationship, p < 0.05 considered significant

Inflammatory markers in correlation with AHI. *The test of significance: Pearson correlation coefficient, the direction before “r” denoting the direction of relationship, p < 0.05 considered significant
Factors influencing the degree of AHI and predict moderate to severe OSA
The results presented in Table 3 indicate that a general linear model with a backward elimination technique found that being hypertensive and having higher SIRI, CRP, and ESR levels all independently affected AHI, with p values less than 0.05 for all. However, an increase in monocyte levels had a significant negative impact. Furthermore, Table 4 revealed that for every one-unit increase in SIRI, CRP, and ESR levels, the likelihood of moderate and severe OSA doubled with p-values less than 0.05 for all. On the other hand, being hypertensive increased the likelihood of moderate and severe OSA by sixteen times, with a p value of 0.01.
Discussion
The exact role of chronic inflammation in the development of obstructive sleep apnea has yet to be fully understood. However, it is believed that multiple factors cause the pathogenesis of OSA. Precisely, it is thought that activation of certain inflammatory pathways occurs in response to the activity of the sympathetic nervous system and oxidative stress. These pathways can lead to vascular endothelial dysfunction and metabolic dysregulation, contributing to the development and progression of OSA [26].
The present study revealed that patients with moderate to severe OSA were generally older and had associated conditions like DM and HTN. Additionally, being hypertensive positively influences the degree of AHI, and the likelihood of moderate to severe OSA increases by 16 times in hypertensive patients. A supportive study found that older patients with OSA were more prone to severe disease and could benefit from positional therapy [27]. Moreover, moderate to severe OSA was significantly linked to DM or its complications, and could also be related to co-association with hypertension [28, 29].
The frequent drops in oxygen levels and brief awakenings during sleep in patients with OSA, potentially affect a patient’s overall health. It has been linked to cardiovascular complications, including high blood pressure, pulmonary hypertension, heart failure, irregular heartbeats, heart attacks, and strokes [30]. In contrary, many clinical studies involving OSA patients have been hindered by inadequate control for co-morbid conditions, such as obesity, pre-existing cardiovascular disease, or medication use. This limitation can make it difficult to isolate the specific impact of OSA on cardiovascular health. Moreover, study results related to OSA and its impact on cardiovascular health often showed substantial variability, making it challenging to establish transparent cause-and-effect relationships and identify consistent mechanisms [31]; therefore, the most acceptable explanation for this variability is related to variations in the morphology and duration of nocturnal airflow cessations and oxygen desaturation, which may be not fully captured by the traditional AHI.
Obesity is a common risk factor for OSA and DM. However, if patients have an array of clusters of metabolic syndrome such as obesity, HTN, and DM, the condition may be further exacerbated. Metabolic syndrome is higher in OSA patients due to commonly shared risks, and studies indicate that metabolic syndrome is significantly associated with severe OSA [32].
Many literatures have discussed the coexistence of a chronic inflammatory state in patients with OSA. The mechanism of developing this chronic inflammatory state is still controversial [26, 33]; one of these mechanisms is the effect of intermittent hypoxia in association with oxidative stress, which may increase the sympathetic response [34, 35]. The other alternative pathway may be due to the release of many inflammatory cells and mediators from the upper airways into the systemic circulation by the effect of endothelial injury [36].
In this study, it was shown that OSA has an inflammatory aspect. The results indicated a positive correlation between AHI and neutrophilis. However, as the severity of the disease increased, lymphocyte count decreased, which could be explained by the significant positive correlation between NLR and AHI. Additionally, NLR independently predicts moderate to severe OSA.
Neutrophils are innate inflammatory cells that serve as a first-line immune response during acute inflammation. However, research has found that neutrophils also play a crucial role in chronic inflammation [37]. They contribute to the development of coronary atherosclerosis by activating macrophages [37, 38]. Additionally, the average level of neutrophils in the blood does not necessarily indicate the absence of underlying immune system activation, as seen in acute myocardial infarction and heart failure [39]. Studies have shown a significant correlation between NLR and AHI, which supports our findings [40, 41]. This link may be due to subclinical inflammation in the respiratory tract system and the chronic inflammatory state of associated comorbidities such as diabetes and hypertension.
Our study found that blood monocytes have an inverse correlation with AHI. Monocyte cells are mainly synthesized in the bone marrow, and their circulation period in the blood does not exceed 3 days before they immigrate to different tissues, where they are transformed into activated macrophages [42]. When exposed to hypoxia, these macrophages release a pro-inflammatory cytokine called macrophage migration inhibitory factor (MIF). This cytokine has a dual action on the hypothalamic-pituitary-adrenal axis [43], significantly regulating inflammation.
In recent studies, the Systemic Inflammatory Response Index (SIRI) has been used to predict the poor prognosis of cancer [15,16,17,18], and cardiovascular disease patients [44, 45]. Our study found a positive correlation between SIRI and AHI, indicating that the likelihood of moderate to severe OSA doubled with every unit increase in SIRI. SIRI comprises three essential blood cells: neutrophils, monocytes, and lymphocytes, contributing to its effectiveness. These findings are consistent with a recent study [46].
As a part of systemic inflammation response, CRP and ESR, a first-phase inflammatory marker, were easy to measure as a routine workup. In our work, CRP and ESR correlated positively with AHI and particulate a high prediction power for moderate to severe OSA.
A supportive study found that individuals with sleep apnea and those with a high risk of heart problems had similar levels of CRP. The study matched patients and controls carefully and suggested a possible causal link between sleep apnea and elevated CRP [47], which was recently supported by another study [48]; the authors referred the possible causality to the constant inflammatory state of upper airway mucosa due to repeated closure and opening. Additionally, intermittent hypoxia leads to the generation of reactive oxygen species that trigger inflammatory pathways like TNF-α [49]. Moreover, OSA has a notable impact on the composition of the protein component in CRP, which could play a role in OSA-related damage [50]. Moreover, a recent meta-analysis considered CRP as a predictive marker of OSA [21]. In the same line of CRP, ESR was closely related to moderate to severe OSA in different studies [24, 51, 52, 53].
This study has a noteworthy limitation: the relatively small sample size. However, the single-center nature of the study might account for the limited sample. Additionally, retrospective data provided valuable insights into the association between various factors and the study’s outcomes. Nevertheless, it is essential to acknowledge that the small sample size remains a limitation, and further prospective research is advisable to enhance the depth of prognosis reporting.
Conclusion
This study highlights several key findings. Patients with moderate and severe OSA were older and had comorbidities like diabetes and hypertension. CRP and ESR were significantly elevated in these severe OSA cases and positively correlated with AHI. Additionally, higher SIRI levels were associated with higher AHI. Being hypertensive and having elevated SIRI, CRP, and ESR levels were independently linked to increased OSA severity, while increased monocyte levels had a negative impact. These findings underscore the intricate relationship between inflammation, comorbidities, and the severity of OSA.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
References
Silva MDS, Poyares D, Silva LO, Souza KM, Andersen ML, Ohayon MM, Tufik S, Piovezan RD (2022) Associations of the severity of obstructive sleep apnea with age-related comorbidities: a population-based study. Front Neurol 10(13):802554. https://doi.org/10.3389/fneur.2022.802554. (PMID: 35620781; PMCID: PMC9128480)
Devulapally K, Pongonis R Jr, Khayat R (2009) OSA: the new cardiovascular disease: part II: Overview of cardiovascular diseases associated with obstructive sleep apnea. Heart Fail Rev 14(3):155–164. https://doi.org/10.1007/s10741-008-9101-2. (Epub 2008 Aug 29. PMID: 18758946; PMCID: PMC2698954)
Rundo JV, Downey R 3rd (2019) Polysomnography. Handb Clin Neurol 160:381–392. https://doi.org/10.1016/B978-0-444-64032-1.00025-4. (PMID: 31277862)
Bangash A, Wajid F, Poolacherla R, Mim FK, Rutkofsky IH (2020) Obstructive sleep apnea and hypertension: a review of the relationship and pathogenic association. Cureus 12(5):e8241. https://doi.org/10.7759/cureus.8241. (PMID: 32582500; PMCID: PMC7306640)
Stanek A, Brożyna-Tkaczyk K, Myśliński W (2021) Oxidative stress markers among obstructive sleep apnea patients. Oxidative Med Cell Longev 19(2021):9681595. https://doi.org/10.1155/2021/9681595. (PMID: 34336121; PMCID: PMC8321764)
Park JG, Ramar K, Olson EJ (2011) Updates on definition, consequences, and management of obstructive sleep apnea. Mayo Clin Proc 86(6):549–554. https://doi.org/10.4065/mcp.2010.0810. (quiz 554-5. PMID: 21628617; PMCID: PMC3104914)
Kirk V, Baughn J, D’Andrea L, Friedman N, Galion A, Garetz S, Hassan F, Wrede J, Harrod CG, Malhotra RK (2017) American Academy of Sleep Medicine position paper for the use of a home sleep apnea test for the diagnosis of OSA in children. J Clin Sleep Med 13(10):1199–1203
Abdulkhaleq LA, Assi MA, Abdullah R, Zamri-Saad M, Taufiq-Yap YH, Hezmee MNM (2018) The crucial roles of inflammatory mediators in inflammation: a review. Vet World 11(5):627–635. https://doi.org/10.14202/vetworld.2018.627-635. (Epub 2018 May 15. PMID: 29915501; PMCID: PMC5993766)
Gleeson M, Bishop NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MA (2011) The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol 11(9):607–615. https://doi.org/10.1038/nri3041. (PMID: 21818123)
Curcic S, Holzer M, Frei R, Pasterk L, Schicho R, Heinemann A, Marsche G (2015) Neutrophil effector responses are suppressed by secretory phospholipase A2 modified HDL. Biochim Biophys Acta 1851(2):184–193. https://doi.org/10.1016/j.bbalip.2014.11.010. (Epub 2014 Nov 24. PMID: 25463476; PMCID: PMC4789498)
Mittal M, Siddiqui MR, Tran K, Reddy SP, Malik AB (2014) Reactive oxygen species in inflammation and tissue injury. Antioxid Redox Signal 20(7):1126–1167. https://doi.org/10.1089/ars.2012.5149. (Epub 2013 Oct 22. PMID: 23991888; PMCID: PMC3929010)
Qiu W, Shi Q, Chen F, Wu Q, Yu X, Xiong L (2022) The derived neutrophil to lymphocyte ratio can be the predictor of prognosis for COVID-19 Omicron BA.2 infected patients. Front Immunol 2(13):1065345. https://doi.org/10.3389/fimmu.2022.1065345. (PMID: 36405724; PMCID: PMC9666892)
Inanli I, Aydin M, Çaliskan AM, Eren I (2019) Neutrophil/lymphocyte ratio, monocyte/lymphocyte ratio, and mean platelet volume as systemic inflammatory markers in different states of bipolar disorder. Nord J Psychiatry 73(6):372–379. https://doi.org/10.1080/08039488.2019.1640789. (Epub 2019 Jul 13. PMID: 31304832)
Albayrak H (2023) Neutrophil-to-lymphocyte ratio, neutrophil-to-monocyte ratio, platelet-to-lymphocyte ratio, and systemic immune-inflammation index in psoriasis patients: response to treatment with biological drugs. J Clin Med 12(17):5452. https://doi.org/10.3390/jcm12175452. (PMID: 37685519; PMCID: PMC10488109)
Hou Q, Su S, You W, Wang T, Ren T, Zhu L (2021) Systemic inflammation response index as a prognostic marker in cancer patients: a systematic review and meta-analysis of 38 cohorts. Dose-Response 19(4):15593258211064744. https://doi.org/10.1177/15593258211064744. (PMID: 34987341; PMCID: PMC8689621)
Qi Q, Zhuang L, Shen Y, Geng Y, Yu S, Chen H, Liu L, Meng Z, Wang P, Chen Z (2016) A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer 122(14):2158–2167. https://doi.org/10.1002/cncr.30057. (Epub 2016 May 6. PMID: 27152949)
Zheng Y, Chen Y, Chen J, Chen W, Pan Y, Bao L, Gao X (2019) Combination of systemic inflammation response index and platelet-to-lymphocyte ratio as a novel prognostic marker of upper tract urothelial carcinoma after radical nephroureterectomy. Front Oncol 18(9):914. https://doi.org/10.3389/fonc.2019.00914. (PMID: 31620369; PMCID: PMC6759944)
Zhang Y, Liu F, Wang Y (2020) Evidence of the prognostic value of pretreatment systemic inflammation response index in cancer patients: a pooled analysis of 19 cohort studies. Dis Markers 31(2020):8854267. https://doi.org/10.1155/2020/8854267. (PMID: 32934755; PMCID: PMC7479458)
Al-Mughales J, Wali SO, Manzar MD, Alhejaili F, Gozal D (2022) Pro-inflammatory markers in patients with obstructive sleep apnea and the effect of Continuous Positive Airway Pressure therapy. Sleep Sci 15(Spec 1):20–27. https://doi.org/10.5935/1984-0063.20200117. (PMID: 35273744; PMCID: PMC8889979)
Imani MM, Sadeghi M, Farokhzadeh F, Khazaie H, Brand S, Dürsteler KM, Brühl A, Sadeghi-Bahmani D (2021) Evaluation of blood levels of C-reactive protein marker in obstructive sleep apnea: a systematic review, meta-analysis and meta-regression. Life (Basel) 11(4):362. https://doi.org/10.3390/life11040362. (PMID: 33921787; PMCID: PMC8073992)
Li K, Wei P, Qin Y, Wei Y (2017) Is C-reactive protein a marker of obstructive sleep apnea?: A meta-analysis. Medicine (Baltimore) 96(19):e6850. https://doi.org/10.1097/MD.0000000000006850. (PMID: 28489776; PMCID: PMC5428610)
Archontogeorgis K, Nena E, Papanas N, Steiropoulos P (2014) Biomarkers to improve diagnosis and monitoring of obstructive sleep apnea syndrome: current status and future perspectives. Pulm Med 2014:930535. https://doi.org/10.1155/2014/930535. (Epub 2014 Nov 27. PMID: 25538852; PMCID: PMC4265695)
Bouloukaki I, Mermigkis C, Tzanakis N, Kallergis E, Moniaki V, Mauroudi E, Schiza SE (2017) Evaluation of inflammatory markers in a large sample of obstructive sleep apnea patients without comorbidities. Mediators Inflamm 2017:4573756. https://doi.org/10.1155/2017/4573756. (Epub 2017 Jul 31. PMID: 28831208; PMCID: PMC5555019)
Lee WH, Wee JH, Rhee CS, Yoon IY, Kim JW (2016) Erythrocyte sedimentation rate may help predict severity of obstructive sleep apnea. Sleep Breath 20(1):419–424. https://doi.org/10.1007/s11325-015-1245-4. (Epub 2015 Aug 28. PMID: 26315467)
Fleming WE, Holty JC, Bogan RK, Hwang D, Ferouz-Colborn AS, Budhiraja R, Redline S, Mensah-Osman E, Osman NI, Li Q, Azad A, Podolak S, Samoszuk MK, Cruz AB, Bai Y, Lu J, Riley JS, Southwick PC (2018) Use of blood biomarkers to screen for obstructive sleep apnea. Nat Sci Sleep 14(10):159–167. https://doi.org/10.2147/NSS.S164488. (PMID: 29942168; PMCID: PMC6005302)
McNicholas WT (2009) Obstructive sleep apnea and inflammation. Prog Cardiovasc Dis 51(5):392–399. https://doi.org/10.1016/j.pcad.2008.10.005. (PMID: 19249445)
Ann L, Lee CH, Immen R, Dyken ME, Im K (2023) Older age is associated with positional obstructive sleep apnea. Am J Geriatr Psychiatry S1064-7481(23):311–311. https://doi.org/10.1016/j.jagp.2023.05.010. (Epub ahead of print. PMID: 37316373)
Siwasaranond N, Nimitphong H, Manodpitipong A, Saetung S, Chirakalwasan N, Thakkinstian A, Reutrakul S (2018) The relationship between diabetes-related complications and obstructive sleep apnea in type 2 diabetes. J Diabetes Res 7(2018):9269170. https://doi.org/10.1155/2018/9269170. (PMID: 29707586; PMCID: PMC5863325)
Jean-Louis G, Zizi F, Clark LT, Brown CD, McFarlane SI (2008) Obstructive sleep apnea and cardiovascular disease: role of the metabolic syndrome and its components. J Clin Sleep Med 4(3):261–272 (PMID: 18595441; PMCID: PMC2546461)
Tietjens JR, Claman D, Kezirian EJ, De Marco T, Mirzayan A, Sadroonri B, Goldberg AN, Long C, Gerstenfeld EP, Yeghiazarians Y (2019) Obstructive sleep apnea in cardiovascular disease: a review of the literature and proposed multidisciplinary clinical management strategy. J Am Heart Assoc 8(1):e010440. https://doi.org/10.1161/JAHA.118.010440. (PMID: 30590966; PMCID: PMC6405725)
Ryan S (2018) Mechanisms of cardiovascular disease in obstructive sleep apnoea. J Thorac Dis 10(Suppl 34):S4201
Parish JM, Adam T, Facchiano L (2007) Relationship of metabolic syndrome and obstructive sleep apnea. J Clin Sleep Med 3(5):467–472 (PMID: 17803009; PMCID: PMC1978322)
Vicente E, Marin JM, Carrizo SJ, Osuna CS, González R, Marin-Oto M, Forner M, Vicente P, Cubero P, Gil AV, Soler X (2016) Upper airway and systemic inflammation in obstructive sleep apnoea. Eur Respir J 48(4):1108–1117
Ryan S, McNicholas WT (2008) Intermittent hypoxia and activation of inflammatory molecular pathways in OSAS. Arch Physiol Biochem 114(4):261–266
Jelic S, Le Jemtel TH (2008) Inflammation, oxidative stress, and the vascular endothelium in obstructive sleep apnea. Trends Cardiovasc Med 18(7):253–260
Devouassoux G, Lévy P, Rossini E, Pin I, Fior-Gozlan M, Henry M, Seigneurin D, Pépin JL (2007) Sleep apnea is associated with bronchial inflammation and continuous positive airway pressure–induced airway hyperresponsiveness. J Allergy Clin Immunol 119(3):597–603
Soehnlein O (2012) Multiple roles for neutrophils in atherosclerosis. Circ Res 110(6):875–888. https://doi.org/10.1161/CIRCRESAHA.111.257535. (PMID: 22427325)
Franck G, Mawson T, Sausen G, Salinas M, Masson GS, Cole A, Beltrami-Moreira M, Chatzizisis Y, Quillard T, Tesmenitsky Y, Shvartz E, Sukhova GK, Swirski FK, Nahrendorf M, Aikawa E, Croce KJ, Libby P (2017) Flow perturbation mediates neutrophil recruitment and potentiates endothelial injury via TLR2 in mice: implications for superficial erosion. Circ Res 121(1):31–42. https://doi.org/10.1161/CIRCRESAHA.117.310694. (Epub 2017 Apr 20. PMID: 28428204; PMCID: PMC5488735)
Shah AD, Thornley S, Chung SC, Denaxas S, Jackson R, Hemingway H (2017) White cell count in the normal range and short-term and long-term mortality: international comparisons of electronic health record cohorts in England and New Zealand. BMJ Open 7(2):e013100. https://doi.org/10.1136/bmjopen-2016-013100. (PMID: 28213596; PMCID: PMC5318564)
Uygur F, Tanriverdi H, Aktop Z, Erboy F, Altinsoy B, Damar M, Atalay F (2016) The neutrophil-to-lymphocyte ratio in patients with obstructive sleep apnoea syndrome and its relationship with cardiovascular disease. Heart Lung 45(2):121–125
Oyama J, Nagatomo D, Yoshioka G, Yamasaki A, Kodama K, Sato M, Komoda H, Nishikido T, Shiraki A, Node K (2016) The relationship between neutrophil to lymphocyte ratio, endothelial function, and severity in patients with obstructive sleep apnea. J Cardiol 67(3):295–302. https://doi.org/10.1016/j.jjcc.2015.06.005. (Epub 2015 Sep 4. PMID: 26343754)
Italiani P, Boraschi D (2014) From monocytes to M1/M2 macrophages: phenotypical vs. functional differentiation. Front Immunol 17(5):514. https://doi.org/10.3389/fimmu.2014.00514. (PMID: 25368618; PMCID: PMC4201108)
Edwards KM, Tomfohr LM, Mills PJ, Bosch JA, Ancoli-Israel S, Loredo JS, Dimsdale J (2011) Macrophage migratory inhibitory factor (MIF) may be a key factor in inflammation in obstructive sleep apnea. Sleep 34(2):161–163. https://doi.org/10.1093/sleep/34.2.161. (PMID: 21286497; PMCID: PMC3022935)
Yang YL, Wu CH, Hsu PF, Chen SC, Huang SS, Chan WL, Lin SJ, Chou CY, Chen JW, Pan JP, Charng MJ, Chen YH, Wu TC, Lu TM, Huang PH, Cheng HM, Huang CC, Sung SH, Lin YJ, Leu HB (2020) Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Investig 50(5):e13230. https://doi.org/10.1111/eci.13230. (Epub 2020 May 11. PMID: 32291748)
Huang J, Zhang Q, Wang R, Ji H, Chen Y, Quan X, Zhang C (2019) Systemic immune-inflammatory index predicts clinical outcomes for elderly patients with acute myocardial infarction receiving percutaneous coronary intervention. Med Sci Monit 18(25):9690–9701. https://doi.org/10.12659/MSM.919802. (PMID: 31849367; PMCID: PMC6930700)
Díaz-García E, García-Tovar S, Alfaro E, Jaureguizar A, Casitas R, Sánchez-Sánchez B, Zamarrón E, Fernández-Lahera J, López-Collazo E, Cubillos-Zapata C, García-Río F (2022) Inflammasome activation: a keystone of proinflammatory response in obstructive sleep apnea. Am J Respir Crit Care Med 205(11):1337–1348. https://doi.org/10.1164/rccm.202106-1445OC. (PMID: 35363597)
Shamsuzzaman AS, Winnicki M, Lanfranchi P, Wolk R, Kara T, Accurso V, Somers VK (2002) Elevated C-reactive protein in patients with obstructive sleep apnea. Circulation 105(21):2462–2464. https://doi.org/10.1161/01.cir.0000018948.95175.03. (PMID: 12034649)
Yi M, Zhao W, Tan Y, Fei Q, Liu K, Chen Z, Zhang Y (2022) The causal relationships between obstructive sleep apnea and elevated CRP and TNF-α protein levels. Ann Med 54(1):1578–1589. https://doi.org/10.1080/07853890.2022.2081873. (PMID: 35652886; PMCID: PMC9176672)
Zhang H, Yang F, Guo Y et al (2018) The contribution of chronic intermittent hypoxia to OSAHS: from the perspective of serum extracellular microvesicle proteins. Metabolism 85:97–108
Ryan S, Taylor CT, McNicholas WT (2005) Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 112(17):2660–2667. https://doi.org/10.1161/CIRCULATIONAHA.105.556746. (PMID: 16246965)
Suliman LA, Morsy NE, El-Sebaie AH, Omar NM, Fathy A (2017) Modelling obstructive sleep apnea susceptibility using non-invasive inflammatory biomarkers. Egypt J Chest Dis Tuberc 66(4):657–661
Shamsuzzaman A, Amin RS, Somers V (2011) Elevated erythrocyte sedimentation rate (ESR) during morning and evening hours in patients with obstructive sleep apnea. InD40. Sleep disordered breathing outcomes. American Thoracic Society, pp A6070–A6070
Al-Rasheedi AN, Thirunavukkarasu A, Almutairi A, Alruwaili S, Alotaibi H, Alzaid W, Albalawi F, Alwadani O, Dilli A (2022) Knowledge and attitude towards obstructive sleep apnea among primary care physicians in northern regions of saudi arabia: a multicenter study. Healthcare (Basel) 10(12):2369. https://doi.org/10.3390/healthcare10122369. (PMID: 36553893; PMCID: PMC9778346)
Acknowledgements
Not applicable
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Seham Ezzat Fathy Elfeky and A. Ali have contributed equally to this study. Nouf Mubarak Alazmi and A. Ali worked on data collection. A. Ali analyzed and interpreted the results and helped in writing the paper. Eman M. Moazen, Mohammad Hamad Alhassoon, Nesma A. Elzanaty, Nouf Mubarak Alazm, Liang Wu, and Mai M. Saleh were significant contributors to writing the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical approval has been obtained from the ethical committee office, King Fahad Specialist Hospital, Buraidah, Qasim, Saudi Arabia, (No: 607-45-3465).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elfeky, S.E.F., Ali, A., Moazen, E.M. et al. Systemic inflammatory response index as an independent predictor of severity in patients with obstructive sleep apnea. Egypt J Bronchol 18, 1 (2024). https://doi.org/10.1186/s43168-023-00253-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00253-y