
Abstract
Background
Prediabetes is considered a major risk factor for diabetes mellitus (DM), leading to microvascular and cardiovascular disorders. Myocardial performance index (MPI) is a non-invasive Doppler method for the determination of global ventricular activity. We have not enough knowledge about the effect of prediabetes on the left ventricular (LV) function. We aimed to assess the MPI in prediabetic patients without coronary artery disease (CAD) utilizing echocardiography tissue Doppler imaging (TDI).
Results
We conducted a randomized controlled study that included fifty prediabetic patients and fifty healthy participants as the control group. All the participants were subjected to laboratory tests and echocardiography TDI to evaluate the LV systolic and diastolic functions
We found that the isovolumic relaxation time (IVRT) and MPI values were significantly increased in the prediabetic patients compared to the control group (P < 0.001). In contrast, left ventricular ejection time (ET) was significantly longer in the control group than in prediabetic patients.
Conclusion
Prediabetes may adversely affect the LV function as assessed by MPI. Screening for prediabetes and early intervention is required for the prevention of cardiovascular morbidity and mortality.
Similar content being viewed by others


Background
DM has a long-term effect on the cardiovascular system through microvascular and macrovascular complications. Myocardial injury in DM occurs due to coronary macrovascular and microvascular diseases, autonomic dysfunction, and diabetic cardiomyopathy. These physiopathological mechanisms often coexist and potentiate the effects of each other [1]. Type 2 diabetes has a gradual onset, with most patients advancing through prediabetes, which is defined as one or more of the following: impaired glucose tolerance (IGT) (plasma glucose of 140 to 199 mg/dl 2 h after an oral load of 75 g dextrose), impaired fasting glucose (IFG) (plasma glucose of 100 to 125 mg/dl), or HbA1c 5.7 to 6.4% [2].
The prevalence of prediabetes is increasing rapidly worldwide; current projections indicate that by 2030, there will be more than 470 million prediabetic individuals. Today, more than 200 million people are affected by type 2 DM throughout the world. It is estimated that 5–10% of prediabetic patients will progress to diabetes every year, and the same number of people will return to normoglycemia [3].
Prediabetes is a significant risk factor for diabetes, leading to microvascular complications and cardiovascular disorders [4]. A 20% increase in the risk of developing cardiovascular disease is associated with DM compared to non-diabetic subjects. Insulin resistance and impaired beta-cell function, which are considered underlying pathophysiological disorders of the excess risk of prediabetes, are believed to be the same as those of DM [5]. Although DM is known to be related to LV dysfunction, even after hypertension and CAD are excluded, the association between prediabetes and LV function has not been comprehensively investigated [6].
TDI is utilized in fluctuating cardiovascular conditions with approval as a marker of LV systolic and diastolic dysfunction. It is useful in the evaluation of CAD and has prognostic implications. It is also more sensitive than conventional echocardiography for detecting early myocardial changes in primary (cardiomyopathies) and secondary (ischemia) myocardial disorders [7].
Tei Chuwa et al. reported that the myocardial performance index (MPI) reflects both the myocardium’s diastolic and systolic functions and has been associated with cardiovascular morbidity and mortality. It is simple to be calculated and has a narrow range in normal healthy individuals [8].
The MPI has been studied in numerous cardiovascular diseases, such as DM, hypertension, myocardial infarction, and heart failure, and showed a strong predictive relationship with morbidity and mortality [9].
We do not know enough about the effect of prediabetes on the LV functions. We aimed to assess the MPI in prediabetic patients without CAD utilizing echocardiography TDI.
Methods
The study was carried out in the Outpatient Clinic of the Internal Medicine Department. Fifty prediabetic patients and an equal number of healthy volunteers (normoglycemic subjects with normal glucose tolerance) as the control group were enrolled. An individual is diagnosed as prediabetic if he or she has one of the following criteria, according to the American Diabetes Association (ADA) guidelines [2]:
-
Patients with fasting blood glucose of 100–125 mg/dl
-
Postprandial 2-h oral glucose tolerance (OGTT) of 140–199 mg/dl
-
HbA1c of 5.7–6.4%
Patients with a history of hypertension, significant valvular heart disease or congenital heart disease, ischemic heart disease, DM, chronic pulmonary disease, and end-stage renal disease on regular dialysis and those with significant organ failure were excluded.
All the patients enrolled in the study were subjected to the following tests: fasting blood glucose level, postprandial 2-h OGTT, and HbA1c. The diagnosis of prediabetes was ensured according to the FPG level and/or OGTT results confirmed by repeating the tests on another day and/or measuring the HbA1c level based on American Diabetes Association (ADA) guidelines. Subjects with an FPG level of 100 to 125 mg/dl were convinced to have IFG. In patients with a normal or IFG level, OGTT was performed. OGTT measures the level of blood glucose after a person fasts for at least 8 h and 2 h after the subject drinks a beverage containing 75 g of glucose dissolved in water. If the 2-h blood glucose level is between 140 and 199 mg/dl, the person is considered to have IGT. In addition, individuals with HbA1c levels between 5.7 and 6.4% were diagnosed as having prediabetes.
Liver profile: alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum albumin, and total protein.
Lipid profile: total cholesterol, low-density lipoprotein, very-low-density lipoprotein, high-density lipoprotein, and triglycerides.
Renal function tests: serum creatinine.
Echocardiographic measurements
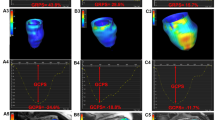
All patients were examined in detail using standard two-dimensional, pulse-wave Doppler, color flow Doppler, and M-mode echocardiographic methods. Echocardiographic measurements are performed in the left lateral decubitus position according to the American Echocardiography Society’s recommendations. The study was conducted using an ATL HDI 5000 colored echocardiographic machine (Philips IE 33 Colored Echocardiographic Machine, USA) with TDI software incorporated in the device using a 2.5–3.5-MHz transducer. According to the modified Simpson method, the LV ejection fraction (LV-EF) was calculated automatically using the echocardiography device’s software. Doppler recordings were provided at a recording rate of 10 cm/s. For all measurements, averages were recorded with three consecutive cycles. All Doppler measurements were made during expiration to minimize any effect of respiration on the measurements. Recordings were obtained by imaging the flow below the aortic valve for the LV outflow tract, and the diastolic flow was measured at the mitral valve tips in the apical four space for the mitral valve. The IVRT was calculated by measuring the time from the midpoint of the aortic closure click to the beginning of early mitral diastolic flow (in ms). The IVCT was determined as the time between the initial cardiac sound to the aortic sound of the second pulse minus the LV ET (in ms). We obtained ET by measuring the time from the start to the end of the recorded systolic flow below the aortic valve. The MPI value was calculated as follows: (IVRT + IVCT)/ET. The measurements were made by the same cardiologist who did not have patient data.
Statistical analysis
Data were studied utilizing a Statistical Program for Social Science (SPSS) version 18.0. Quantitative data were evinced as mean ± standard deviation (M ± SD), while qualitative data were evinced as frequency and percentage, no. (%). The chi-square test was utilized in comparison to non-parametric data. A one-way analysis of variance (ANOVA) was utilized in comparison of more than two means. P-values were established statistically significant at P < 0.05.
Results
Baseline characteristics
We found that 62% were males among the patient group, and the mean age was 42.8 ± 5.01 years. Sixty-six percent were smokers. The mean BMI was 31.4 ± 5 kg/m2. As regards the assessment of blood glucose, results showed that the mean of fasting blood glucose level, postprandial 2-h OGTT, and HbA1c were 113.4 mg/dl, 162.8 mg/dl, and 5.9%, respectively. Regarding the pretreatment laboratory profile, results showed that the mean of ALT, AST, S. Albumin, S. total protein, CRP, and S.creatinine were 45.7 U/l, 28.62 U/l, 4.1 g/dl, 6.9 g/dl, 5.6 mg/dl, and 0.95 mg/dl, respectively. Regarding lipid profile, results showed that the mean of total cholesterol, HDL, LDL, and triglyceride were 209.1 mg/dl, 39.1 mg/dL, 93.1 mg/dl, and 210 mg/dl, respectively. Regarding echographic measurements, the mean of ejection fraction and isovolumetric contraction time was 58.4% and 76.2 (msn), respectively. The mean of isovolumetric relaxation time, ejection time, and myocardial performance index were 83 (msn), 265.6 (msn), and 0.6, respectively.
Among the control group, 68% were males. The mean age was 43.4 ± 6.6 years, and 58% were smokers. The mean BMI was 29.1 ± 2.9 kg/m2. Regarding blood glucose assessment, results showed that the mean of fasting blood glucose level, postprandial 2-h OGTT, and HbA1c were 84.2 mg/dl, 113.4 mg/dl, and 5.2%, respectively. Regarding the pretreatment laboratory profile, results showed that the mean of ALT, AST, S. Albumin, S. total protein, CRP, and S.creatinine were 35.6 U/l, 28.6 U/l, 4.2 g/dl, 6.7 g/dl, 5.9 mg/dl, and 0.95 mg/dl, respectively. Regarding lipid profile, results showed that the mean of total cholesterol, HDL, LDL, and triglyceride were 162.6 mg/dl, 39.1 mg/dl, 92.1 mg/dl, and 144 mg/dl, respectively. Regarding echographic measurements, the mean of ejection fraction and isovolumetric contraction time was 56.1% and 77.4 (msn), respectively. The mean of isovolumetric relaxation time, ejection time, and myocardial performance index were 74.7 (msn), 283.2 (msn), and 0.53, respectively (Tables 1, 2, 3, and 4).
Analysis of the echocardiographic measurements
We found a statistically significant difference between prediabetic and control groups regarding IVRT, ET, and MPI values (all, P < . 001). IVRT and the ET were significantly longer in the prediabetic group than in the control group. MPI values were increased in the prediabetic group than in the control group.
Discussion
In the current study, we found a statistically significant difference between prediabetic and control groups regarding IVRT, ET, and MPI values (all, P < 0.001). IVRT and the ET were significantly longer in the prediabetic group than in the control group. MPI values were increased in the prediabetic group than in the control group.
This study’s results were supported by Aslan et al. [10], who studied 50 patients with prediabetes and 47 healthy controls of similar ages. The PW echocardiographic measurements demonstrated that the IVRT and deceleration time (DT) values were significantly longer, and the E waves were significantly lower in the patients with prediabetes, although the LA diameter was significantly larger in the patient group than in the control group (35.9 ± 3.9 cm vs. 33.7 ± 4.2 cm, respectively, P = 0.027) [10].
Akçay et al. [6] provide evidence about the high prevalence of subclinical LV systolic and diastolic dysfunction in patients with prediabetes evaluated by TDI. They evaluated 94 patients with prediabetes without known cardiovascular diseases and 70 healthy volunteers with similar demographic characteristics. The mean results of myocardial isovolumetric relaxation time (IVRTm), myocardial isovolumetric contraction time (IVCTm), and myocardial performance index (MPI) values were significantly higher in patients with prediabetes [6].
Bajraktari et al. [11] showed that insulin resistance is an independent correlate of LV diastolic dysfunction in subjects with IGT and type 2 DM. In this study, a significantly greater proportion of patients with echocardiographic evidence of LV diastolic dysfunction was observed in subjects with IGT and DM compared with subjects with normal glucose tolerance [11].
Our results were consistent with the results of a study performed by Ceyhan et al. [12] using tissue Doppler and strain/strain rate echocardiography which showed that LV longitudinal systolic and diastolic functions were impaired in normotensive diabetic and prediabetic patients [12].
Shimabukuro et al. [13] reported that the frequency of LV diastolic dysfunction in subjects with normal glucose tolerance and impaired glucose tolerance (IGT) was 13% and 50%, respectively (P = 0.0001). In this study, after adjusting for established risk factors, IGT was detected to be a predictor of LV diastolic dysfunction [13].
Our study results show that total cholesterol was significantly higher in the prediabetic group than in the control group (P < 0.001). The same trend was observed for triglyceride (P < 0.001). Our study demonstrated that BMI was significantly higher in the prediabetic group than in the control group (P < 0.001).
The current study results were supported by Askin et al. [3] in which 80 prediabetics (34 females and 46 males) and an equal number of sex-matched healthy volunteers (35 females and 45 males) were enrolled. They reported that prediabetes is associated with BMI. BMI was significantly higher in the prediabetic group than in the control group (P < 0.001). They also reported that TC and TG were higher in the prediabetic group (P = .002, .008, respectively) [3].
Aslan et al. [10] showed that the total cholesterol levels were significantly higher in the prediabetics than in the healthy controls (213.1 ± 47 mg/dl vs. 188.2 ± 37.2 mg/dl, respectively, P = 0.005). Moreover, the plasma triglyceride (TG) concentrations were significantly higher in the prediabetic group than in the control group (163.0 ± 93.2 mg/dl vs. 126.9 ± 70.7 mg/ dl, respectively, P = 0.035) [10].
These results disagreed with Akçay et al., which showed that body mass index (BMI), total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels were similar among the prediabetic patients and controls [6]. Also, Bajraktari et al. [11] observed that no significant differences between the prediabetic patients and normal subjects concerning BMI, total cholesterol, HDLs, LDLs, very-low-density lipoproteins [VLDL], and triglycerides [11].
Conclusion
Prediabetes is closely associated with subclinical LV diastolic dysfunction, as assessed by MPI. Dyslipidemia and increased BMI are associated with a significantly increased risk of prediabetes.
Availability of data and materials
All data generated or analyzed during this study are available on request from the corresponding author.
Abbreviations
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- CAD:
-
Coronary artery disease
- CVD:
-
Cardiovascular disease
- DM:
-
Diabetes mellitus
- HbA1c:
-
Hemoglobin A1c
- HDL:
-
High-density lipoprotein
- HTN:
-
Hypertension
- LDL:
-
Low-density lipoprotein
- TG:
-
Triglyceride
References
Ardahanlı İ, Turan Y, Turan E, Aktas A (2019) Evaluation of the myocardial performance ındex in prediabetic patients. Cumhuriyet Med J 41(2):348–356
American Diabetes Association (2012) Diagnosis and classification of diabetes mellitus. Diabetes Care 35(Suppl 1):S64–S71. https://doi.org/10.2337/dc12-s064
Askin L, Cetin M, Tasolar H, Akturk E (2018) Left ventricular myocardial performance index in prediabetic patients without coronary artery disease. Echocardiography. 35(4):445–449. https://doi.org/10.1111/echo.13822
Cheng YJ, Gregg EW, Geiss LS, Imperatore G, Williams DE, Zhang X, Albright AL, Cowie CC, Klein R, Saaddine JB (2009) Association of A1C and fasting plasma glucose levels with diabetic retinopathy prevalence in the US population: implications for diabetes diagnostic thresholds. Diabetes Care 32(11):2027–2032. https://doi.org/10.2337/dc09-0440
Barr EL, Boyko EJ, Zimmet PZ et al (2009) Continuous relationships between non-diabetic hyperglycaemia and both cardiovascular disease and all-cause mortality: the Australian diabetes, obesity, and lifestyle (AusDiab) study. Diabetologia. 52(3):415–424. https://doi.org/10.1007/s00125-008-1246-y
Akçay M, Aslan AN, Kasapkara HA, Ayhan H, Durmaz T, Keleş T, Bozkurt E (2016) Assessment of the left ventricular function in normotensive prediabetics: a tissue Doppler echocardiography study. Arch Endocrinol Metab 60(4):341–347. https://doi.org/10.1590/2359-3997000000136
Dini FL, Galderisi M, Nistri S, Buralli S, Ballo P, Mele D et al (2013) Abnormal left ventricular longitudinal function assessed by echocardiographic and tissue Doppler imaging is a powerful predictor of diastolic dysfunction in hypertensive patients: the SPHERE study. Int J Cardiol 107:1978–1984
Møller JE, Søndergaard E, Poulsen SH, Egstrup K (2001) The Doppler echocardiographic myocardial performance index predicts left-ventricular dilation and cardiac death after myocardial infarction. Cardiology. 95(2):105–111. https://doi.org/10.1159/000047355
Carluccio E, Biagioli P, Alunni G, Murrone A, Zuchi C, Biscottini E, Lauciello R, Pantano P, Gentile F, Nishimura RA, Ambrosio G (2012) Improvement of myocardial performance (Tei) index closely reflects intrinsic improvement of cardiac function: assessment in revascularized hibernating myocardium. Echocardiography. 29(3):298–306. https://doi.org/10.1111/j.1540-8175.2011.01575.x
Aslan AN, Ayhan H, Çiçek ÖF, Akçay M, Durmaz T, Keles T, Çakir B, Bozkurt E (2014) Relationship between aortic stiffness and the left ventricular function in patients with prediabetes. Intern Med 53(14):1477–1484. https://doi.org/10.2169/internalmedicine.53.1720
Bajraktari G, Koltai MS, Ademaj F et al (2006) Relationship between insulin resistance and left ventricular diastolic dysfunction in patients with impaired glucose tolerance and type 2 diabetes. Int J Cardiol 10(2):206–211
Ceyhan K, Kadi H, Koç F, Çelik A, Öztürk A, Önalan O (2012) Longitudinal left ventricular function in normotensive prediabetics: a tissue Doppler and strain/strain rate echocardiography study. J Am Soc Echocardiogr 25(3):349–356. https://doi.org/10.1016/j.echo.2011.11.018
Shimabukuro M, Higa N, Asahi T, Yamakawa K, Oshiro Y, Higa M, Masuzaki H (2011) Impaired glucose tolerance, but not impaired fasting glucose, underlies left ventricular diastolic dysfunction. Diabetes Care 34(3):686–690. https://doi.org/10.2337/dc10-1141
Acknowledgements
Not applicable
Funding
Not applicable
Author information
Authors and Affiliations
Contributions
The corresponding author “H.M” was a major contributor in writing the manuscript and practical work as regards imaging (echocardiography) for the cases, collected data from patients, wrote the methodology, made analysis of the data of the whole interpretation of the results, and shared in writing the discussion and the abstract. The author “M.A” analyzed and interpreted the patient data. The author “G.O” collected data from 100 patients and shared in writing the discussion and the abstract. “A.E” contributed to practical work as regards laboratory investigation. The author “A.S” collected data and wrote the background. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All subjects provided a written informed consent to participate in the study. The study protocol was approved by the Medical Research Ethics Committee, Qena Medical Ethics Committee, Qena Faculty of Medicine, South Valley University, and the date of approval was 20 July 2019. The committee reference number is not applicable.
The study was conducted in accordance with the Declarations of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This study aimed to evaluate the left ventricular myocardial performance index in prediabetic patients without coronary artery disease.
This manuscript has not been published previously, in any language, in whole or in part and is not under consideration for publication elsewhere.
So, please consider this manuscript entitled “Left Ventricular Myocardial Performance Index In Prediabetic Patients Without Coronary Artery Disease” for publication into your respectable journal.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mahmoud, H.E.M., Alsenbesy, M., Sayed, G.O.F. et al. Left ventricular myocardial performance index in prediabetic patients without coronary artery disease. Egypt J Intern Med 33, 28 (2021). https://doi.org/10.1186/s43162-021-00063-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-021-00063-y