
Abstract
Background
Diabetes mellitus (DM) has been documented among the strongest risk factors for developing heart failure with preserved ejection fraction (HFpEF). The earliest imaging changes in patients with DM are the left atrial (LA) functional and volumetric changes. The aim of this study was to determine the correlation between epicardial fat thickness (EFT) and longitudinal LA reservoir strain (LARS) in patients with type 2 DM (T2DM), as compared with non-diabetic controls.
Results
The study samples in this case-control study comprised of consecutive patients with T2DM (n=64) and matched non-diabetic controls (n=30). An echocardiography was performed on all patients and EFT, volumetric and longitudinal LARS, left ventricular (LV) global longitudinal strain (LVGLS), pulsed-wave Doppler-derived transmitral early (E wave) and late (A wave) diastolic velocities, and tissue-Doppler-derived mitral annular early diastolic (e′) and peak systolic (s') velocities were obtained. The study results demonstrated that the patients with T2DM had thicker EFT (5.96±2.13 vs. 4.10±3.11 mm) and increased LA volume index (LAVI) (43.05± 44.40 vs. 29.10±11.34 ml/m2) in comparison with the non-diabetic ones (p-value: 0.005 and 0.022, respectively). On the other hand, a direct association was observed between EFT and the E/e′ ratio, and an inverse correlation was established between EFT and LARS in patients with T2DM (r=0.299, p-value=0.020 and r=− 0.256, p-value=0.043, respectively). However, regression analysis showed only LV mass index (LVMI) (β=0.012, 95% CI 0.006–0.019, p-value<0.001), LAVI (β=− 0.034, 95% CI − 0.05–0.017, p-value<0.001), and EFT (β=− 0.143, 95% CI − 0.264–− 0.021, p-value=0.021) were independently correlated with LARS.
Conclusions
LARS is considered as an important early marker of subclinical cardiac dysfunction. Thickened epicardial fat may be an independent risk factor for decreased LA reservoir strain. Diabetics are especially considered as a high risk group due to having an increased epicardial adipose tissue thickness.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Diabetes mellitus (DM) has been documented among the strongest risk factors for developing heart failure with preserved ejection fraction (HFpEF), a sub-type of heart failure (HF), which represents almost half of the total number of patients with symptomatic HF [1]. Additionally, epicardial adipocyte infiltration has been associated with the mid and late stages of diastolic dysfunction in individuals with type 2 DM (T2DM). In spite of this, the correlation between epicardial fat thickness (EFT) and early dysfunction has not yet been well understood. The paucity of data might be thus attributable to some limitations in the detection of the very early changes in cardiac function [2]. The earliest imaging changes in patients with T2DM are the left atrial (LA) functional and volumetric changes. In this way, such variables can be assumed as useful tools during the early disease detection [3]. As well, T2DM seems to be an independent risk factor for LA enlargement and dysfunction. There is also an association between EFT and LA and left ventricular (LV) functional changes and increased LAVI [2]. The LA contribution to cardiac function is modulated by its effects as the reservoir, conduit, and booster pump function. The reservoir LA function is correlated with LV isovolumic contraction, ejection, and isovolumic relaxation, and is deeply influenced by LV systolic function, atrial size, and compliance. Phasic atrial function can be obtained by the assessment of volumetric or atrial deformation. The volumetric measurement of LA function is, however, limited by its lower sensitivity in an early disease state [4]. LA reservoir strain (LARS) is thus a significant marker of LA dysfunction, which is typically impaired in patients with LV diastolic dysfunction. Elevated LV pressure is associated with the retrograde transmission of pressures into LA, which gradually reduces the LA compliance and impairs atrial relaxation. The final results are reduction in LA reservoir function, LA dilatation, and mechanical failure [5]. The aim of our study was to determine the correlation between EFT and LARS in patients with T2DM and no apparent coronary artery disease (CAD) in comparison with a non-diabetic control group.
Methods
This study was a case-control study including 64 consecutive patients with T2DM with a left ventricular ejection fraction (LVEF) ≥50% and 30 matched non-diabetic controls, who were hospitalized in our hospital due to evidence of ischemia on non-invasive studies and had no apparent CAD on angiogram between 2021 and 2022. This study was conducted according to the Declaration of Helsinki (DoH) ethical principles, and was further approved by the Ethics Committee of Mazandaran University of Medical Sciences, Sari, Iran (ethics code no. IR.MAZUMS.REC.1400.628). All participants also signed an informed consent form. The patients with significant CAD, HF, severe valvular heart disease, valve replacement, an LVEF<50%, left bundle branch block, atrial flutter or fibrillation, cardiomyopathies, neoplastic illnesses, decreased glomerular filtration rate or serum creatinine ≥1.5 mg/dl, and different systemic diseases were excluded from the study. The serum levels of fasting blood sugar (FBS), cholesterol (Chol), triglyceride (TG), low-density lipoprotein (LDL), and hemoglobin A1c (HbA1c) were determined by the blood sample taken after a 10–12 h overnight fasting. Moreover, 2 h post-prandial serum BS was determined by the blood sample acquired 2 h after eating a meal. The ion exchange chromatography method (Bio Systems S.A, Barcelona, Spain) was used for determining HbA1c level. Body mass index (BMI) was explained as weight in kg divided by height in meters squared. DM was defined according to the guidelines of the American Diabetes Association (ADA), including FBS ≥126 mg/dl (7.0 mmol/L) or 2 h plasma BS during 75 g oral glucose tolerance test (OGTT) ≥200 mg/dl (11.1 mmol/L), or HbA1c ≥6.5% (48 mmol/mol), and included individuals who require to take insulin or oral hypoglycemic medications [6]. Hypertension (HTN) was explained as a systolic blood pressure (SBP) ≥140mmHg and/or a DBP ≥90mmHg, determined on three separate occasions or those receiving antihypertensive medications [7]. Hyperlipidemia (HLP) was characterized as the total Chol levels over 200 mg/dl, HDL-c levels less than 40 mg/dl in males, or less than 50 mg/dl in females [8]. Cigarette smoking was identified by a face-to-face survey. Coronary angiography was performed on all patients by a Siemens AG (Medical Solutions; Erlangen, Germany) within 24–48 h of admission. An experienced cardiologist blinded to the patient data then interpreted the angiograms. No apparent CAD was defined as a stenosis of less than 20% in all coronary artery territories or the presence of only luminal irregularities [9].
Echocardiography
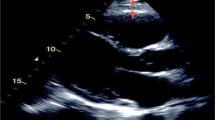
A transthoracic echocardiography was performed for all patients by the ACUSON SC2000 with a 4V1c transducer (Siemens Medical Solutions Inc., Mountain View, CA, USA) within 24–48 h after hospitalization. All movies and images were stored on a hard disk for further off-line analysis (using the eSie VVI software) by an expert echocardiographer blinded to the patients’data. Epicardial fat was identified as an echo-dense space between the outer wall of the myocardium and the visceral pericardium, anterior to the right ventricular wall in the parasternal long axis view. The point of measurement was vertical to the aortic annulus, and its thickness was measured at the end-systole in an average of three cardiac cycles [10] (Figure 1).

Transthoracic two-dimensional echocardiography in the parasternal long-axis view, showing epicardial fat thickness (arrow)
The two-dimensional (2D) grayscale movies were acquired in the apical four-, two-, and three-chamber views (three standard apical views) in three cardiac cycles. The peak longitudinal strain values from the basal, mid, and apical segments of the inferoseptal, anterolateral, inferior, anterior, inferolateral, and anteroseptal walls were measured by the tracking of the endocardial and epicardial walls. To identify the LV peak global longitudinal strain (LVGLS), the average value of all 18 myocardial segments was considered [11]. The LA diameter was identified as the vertical distance between the posterior wall of the aortic root and the posterior LA wall in the para-sternal long axis view at the end systole [12]. The eSie VVI software was used to trace the LA endocardial and epicardial borders in the apical four-chamber view. The average LARS in three segments containing left LA wall, roof, and right LA wall were used to determine LARS by the R-R gating method (Figure 2). After that, LARS was corrected for LVGLS (LARS/-LVGLS). Transmitral pulse-Doppler-derived early and late diastolic velocities (E and A waves) and deceleration time (DT) of the E-wave were determined by placing the cursor at the tip of mitral valve leaflets in the apical four-chamber view. To find the mean tissue-Doppler-derived mitral annulus septal and lateral early diastolic (e°) and peak systolic (s′) velocities, the cursor was inserted at the level of the mitral annulus. The M-mode echocardiography in the parasternal long-axis view was further employed to determine the end-systolic and -diastolic LV internal diameters and end-diastolic interventricular septal (IVS) and posterior wall thickness by inserting the cursor at the mitral valve leaflet tip. The LV mass index (LVMI) was calculated by the formula given below:

Speckle-tracking echocardiography in apical four chamber view represents longitudinal LA reservoir strain curves in three segments containing left LA wall, roof, and right LA wall by considering the QRS complex (R-R gating) as the initiation of the strain calculation (LA Left atrium)
In which, LVIDd, PWT, and SWT indicate the end-diastolic LV internal dimension and posterior and IVS wall thickness, respectively. We also obtained peak velocity of tricuspid regurgitation jet by continuous-Doppler from multiple views [11]. The reproducibility of the EFT and speckle-tracking-derived LVGLS and LARS measurements were determined according to repeated measurements in 10 randomly selected patients by an echocardiography within 48 h, and the intra-observer correlation coefficients were found to be 0.91, 0.90, and 0.92, respectively.
Statistical analysis
The categorical variables were presented as frequency and percentage. The quantitative variables were expressed as the mean± standard deviation (for the normally distributed continuous variables) or median [lower-upper quartile] (for Non-normally distributed continuous variables). Normality was determined by the Shapiro-Wilk test. An independent t-test was used to compare the continuous variables that were normally distributed and the Mann-Whitney U test was used to compare the continuous variables that were non-normally distributed. The categorical variables were compared by Chi-square test and Fisher’s exact test. Moreover, we used a Pearson correlation to find the correlation between different echocardiographic variables in the patients with T2DM and the non-diabetic ones, separately. Multiple linear regression analysis was also conducted on all study population, including the patients with T2DM and the non-diabetic controls to determine the independent correlation between different demographic, laboratory-based, and echocardiographic variables and LARS/-LVGLS. The statistical analyses were performed by the SPSS/PASW (Predictive Analytics Software) Statistics version 18 (SPSS, Chicago, IL, USA). The P value of less than 0.05 signified that the variable was significant. The sample size was determined based on the findings of Evin et al study [2]. According to mean and SD of LA longitudinal strain in case and control groups of the aforementioned study, the effect size was estimated to be 0.69. Considering a confidence level of 95%, the test power of 80%,, a one-tailed test for the comparison of two means, and using the G*power software, the minimum sample size was determined to be 54 individuals (viz., 27 in each group). Given the available facilities and the aim to increase the power of the statistical tests, more samples (that is, 64 individuals in the case group and 30 people as the controls) were included in this study.
Results
This study included 64 patients with T2DM and 30 non-diabetic controls, matched in terms of age and gender, with an LVEF ≥50% and no apparent CAD on angiogram. The mean age of the study population was 55.03±9.86 and their mean BMI was 28.14±3.77 kg/m2. In total, 71 patients (75.5%) were female, and 23 individuals (24.5%) were male. Moreover, 47 patients (50%) had HLP, 46 people (48.9%) were hypertensive, and 19 individuals (20.2%) were smokers. The demographic variables of the study population are presented in Table 1. As expected, the patients with T2DM had higher FBS, 2 h post-prandial BS, and HbA1c levels in comparison with the non-diabetic controls. Moreover, the TG level and BMI were higher in the patients with T2DM than the non-diabetic ones (p-value: 0.002 and 0.010, respectively). The echocardiographic characteristics of both study groups are depicted in Table 2. The mean EFT in the patients with T2DM was higher than that in the non-diabetic ones (5.96±2.13 vs. 4.10±3.11 mm, p-value=0.005). Furthermore, LAVI, the A-wave velocity, and the E/e’ ratio were higher (p-value: 0.022, 0.023, and 0.001; respectively), and the e’ and s’ velocities were lower (p-value: 0.019 and 0.006, respectively) in the patients with DM, as compared with the non-diabetic ones. The Pearson correlation coefficient was further utilized to determine the correlation between the echocardiographic variables in both groups, separately. The study results also showed a positive correlation between EFT and the E/e’ ratio (r=0.299, p-value=0.020), but a negative correlation between EFT and LARS (r=− 0.256, p-value=0.043) in the patients with T2DM. Such correlations were not seen in the non-diabetic controls (Table 3). To find the independent correlation between different demographic and echocardiographic variables and LARS/-LVGLS, multiple linear regression analysis with backward elimination process was conducted on all study population, including the patients with T2DM and the non-diabetic controls. The result of this analysis showed among different variables, only LVMI (β=0.012, 95% CI 0.006–0.019, p-value<0.001), LAVI (β=− 0.034, 95% CI − 0.05–− 0.017, p-value<0.001), and EFT (β=− 0.143, 95% CI − 0.264–− 0.021, p-value=0.021) had an independent correlation with LARS/LVGLS (Table 4).
Discussion
LAVI represents the long-standing effects of increased LV filling pressures [13]. LARS is a stronger predictor of outcome than LAVI and LV parameters [14]. Some studies have validated the prognostic and diagnostic values of LARS in the early detection of some cardiovascular diseases (CVDs) [15]. A powerful correlation exists between LAVI and its mechanical function, but alterations in LA deformation may frequently happen before cavity remodeling and enlargement, and LARS can be thus an important early marker of subclinical cardiac dysfunction [16]. In the atrial reservoir phase, LA is filled and stretched, and there is a positive atrial strain that reaches its peak during the LV systole. Decreased LARS is also a significant, independent predictor of LA fibrosis and remodeling [17]. The normal reference range for LARS is 39.4% (95% CI 38.0–40.8%) [4]. Kurt et al. reported that the patients with HFpEF had lower LARS as compared with those with LV diastolic dysfunction with no HF. They also reported that those with LARS <23% had worse New York Heart Association (NYHA) functional class and higher pulmonary capillary wedge pressure (PCWP) in comparison with those with a higher value [18]. LA also acts as a reservoir during the LV systole. The LA structural and functional changes are considered as the earliest imaging changes in patients with obesity and T2DM [2]. Since LARS could be strongly influenced by LV systolic function, it was corrected for LVGLS (LARS/-LVGLS) to better represent the LA function for any LV shortening, and demonstrate left atrioventricular interaction [19]. Previous studies have established a correlation between HbA1c level and mean BS level over the past three months [20]. For this reason, this variable was included in the present study. On the other hand, EFT is an active visceral adipose tissue located between the visceral pericardium and myocardium. In addition to its physiological roles, it can also lead to the secretion of multiple pro-inflammatory cytokines, and is correlated with metabolic syndrome pathogenesis and insulin resistance [21]. Its thickness can be simply and perfectly determined by standard echocardiographic views [10]. Elevated EFT is usually associated with metabolic syndrome and is considered as a risk marker of CVDs [22]. The correlation between EFT and T2DM has been also validated [23], and individuals with impaired FBS usually have thicker EFT in comparison with normoglycemic cases [24].
In 2018, Zhao et al conducted a prospective study on 130 people without CAD or atrial fibrillation. Indexed epicardial adipose tissue (EAT) volume was determined by cardiac computed tomography (CT). As well, three-dimensional (3D) volumetric measurements and 2D speckle-tracking echocardiography were performed. The study population were then divided into two groups of large and small EAT volume index. The individuals with larger EAT volume index had significantly impaired LAEF and longitudinal LARS. The total EAT volume index could be thus a predictor of impaired longitudinal LARS and reduced LAEF. They concluded that there was an independent association between EAT volume index and subclinical LA dysfunction [17]. Their findings were accordingly consistent with the results in the present study that EFT was an independent predictor of decreased LARS. In 2016, Evin et al. performed a study on 20 patients with obesity and T2DM and 19 healthy controls to assess the association between cardiac adipose tissue and LA function. Cardiac magnetic resonance imaging (MRI) data had been then acquired on all patients to determine systolic LV size and function, longitudinal LARS and strain rates, and radial motion fraction and velocities. They found that epicardial fat volume (EFV) was significantly higher in the patients with obesity and T2DM than controls. Moreover, there were significant correlations between LA functional parameters and both BMI and EFV [2], which were in agreement with the present study that the patients with T2DM had thicker EFT and there was an independent correlation between EFT and decreased LARS.
Mitral annular motion plays an important role in regulating blood movement in and out of LA. During systole, the mitral annulus descends and transfers more apically. These descending motions can further accelerate LV ejection. In addition, this motion can enlarge LA and increase its compliance, accompanied by a drop in LA pressure and a rise in the pulmonary blood flow during atrial reservoir phase [25]. Delayed relaxation further reduces the early diastolic transmitral gradient, and limits the early diastolic filling, which induces an increase in blood residue in LA. As a result, more blood should be ejected into LV during the atrial systole, which is associated with increased LA stroke volume and the peak A-wave velocity [26]. In the present study, the patients with T2DM had lower tissue-Doppler-derived mitral annular s' velocity and higher pulse-Doppler derived A-wave velocity, as compared with the non-diabetics.
During the rapid filling phase, LV is relaxed and mitral annulus ascends and gets away from the apex. The resultant drop in the LV pressure then opens the mitral valve and intensifies ventricular filling (in the atrial conduit phase) [27]. Previous studies have suggested that the E/e' ratio is helpful in estimating the mean LA pressure [28]. Indeed, E wave can be considered as a substitute for the LA-LV pressure gradient and the e' velocity indicates the extent of the gradient created by ventricular suction (29). Our patients with T2DM had larger LA volume, lower tissue-Doppler-derived mitral annular e' velocity, and higher E/e' ratio than the non-diabetics. These findings represent higher filling pressure and diastolic dysfunction in patients with T2DM compared with the non-diabetic ones.
Conclusion
LARS is considered as an important early marker of subclinical cardiac dysfunction. Thickened epicardial fat may be an independent risk factor for decreased LA reservoir strain. Diabetics are especially considered as a high risk group due to having an increased epicardial adipose tissue thickness.
Limitations
There were some limitations in this study, including the small sample size recruited in a single center. As well, the echocardiography, which is a relatively inexpensive and easily accessible modality, was used to determine EFT. However, measurement of the EFT volume by the CT scan and MRI techniques could lead to more accurate results. Moreover, LA volume and reservoir strain, but not the other components of LA function, were measured in this study. On the other hand, information on patient therapy, time since diabetes diagnosis, and creatinine values were not included for data analysis. In spite of this, the HbA1c level that could be correlated with the mean BS concentration over the past three months was included in this study.
Availability of data and materials
The datasets used and/or analysed during this study are available from the corresponding author on reasonable request.
References
Hogg K, Swedberg K, McMurray J (2004) Heart failure with preserved left ventricular systolic function: epidemiology, clinical characteristics, and prognosis. J Am College Cardiol 43(3):317–27
Evin M, Broadhouse KM, Callaghan FM, McGrath RT, Glastras S, Kozor R et al (2016) Impact of obesity and epicardial fat on early left atrial dysfunction assessed by cardiac MRI strain analysis. Cardiovasc Diabetol 15(1):1–10
Santos AB, Kraigher-Krainer E, Gupta DK, Claggett B, Zile MR, Pieske B et al (2014) Impaired left atrial function in heart failure with preserved ejection fraction. Eur J Heart Failure 16(10):1096–103
Pathan F, D’Elia N, Nolan MT, Marwick TH, Negishi K (2017) Normal ranges of left atrial strain by speckle-tracking echocardiography: a systematic review and meta-analysis. J Am Soc Echocardiogr 30(1):59–70
Lin J, Ma H, Gao L, Wang Y, Wang J, Zhu Z et al (2020) Left atrial reservoir strain combined with E/E’as a better single measure to predict elevated LV filling pressures in patients with coronary artery disease. Cardiovasc Ultra 18(1):1–13
Rossi G, Association AD (2018) Diagnosis and classification of diabetes mellitus. Diabetes Care 33(Suppl 1):S62–S9
Mancia G, Fagard R, Narkiewicz K, Redán J, Zanchetti A, Böhm M et al (2013) 2013 Practice guidelines for the management of arterial hypertension of the European society of hypertension (ESH) and the European Society of cardiology (ESC): ESH/ESC task force for the management of arterial hypertension. J hypertens 31(10):1925–38
Arnett DK, Jacobs DR, Luepker RV, Blackburn H, Armstrong C, Claas SA (2005) Twenty-year trends in serum cholesterol, hypercholesterolemia, and cholesterol medication use. Circulation 112(25):3884–91
Maddox TM, Stanislawski MA, Grunwald GK, Bradley SM, Ho PM, Tsai TT et al (2014) Nonobstructive coronary artery disease and risk of myocardial infarction. Jama. 312(17):1754–63
Iacobellis G, Willens HJ (2009) Echocardiographic epicardial fat: a review of research and clinical applications. J Am Soc Echocardiogr 22(12):1311–9
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA et al (2006) Recommendations for chamber quantification. Eur J Echocardiograph 7(2):79–108
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L et al (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the european association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging 16(3):233–71
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF, Dokainish H, Edvardsen T et al (2016) Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the american society of echocardiography and the european association of cardiovascular imaging. Eur J Echocardiogr 17(12):1321–60
Sun M, Xing Y, Guo Y, Cao X, Nie Y, Shu X (2022) Left atrial reservoir strain is an outstanding predictor of adverse cardiovascular outcomes in patients undergoing maintenance hemodialysis: assessment via three-dimensional speckle tracking echocardiography. Clin Cardiol 45(5):549–57
Cau R, Bassareo P, Suri JS, Pontone G, Saba L (2022) The emerging role of atrial strain assessed by cardiac MRI in different cardiovascular settings: an up-to-date review. Eur Radiol 1–11:4384
Cameli M, Mandoli GE, Lisi E, Ibrahim A, Incampo E, Buccoliero G et al (2019) Left atrial, ventricular and atrio-ventricular strain in patients with subclinical heart dysfunction. Int J Cardiovasc Imaging 35:249–58
Zhao L, Harrop DL, Ng AC, Wang WY (2018) Epicardial adipose tissue is associated with left atrial dysfunction in people without obstructive coronary artery disease or atrial fibrillation. Canadian J Cardiol 34(8):1019–25
Morris D, Belyavskiy E, Aravind-Kumar R, Kropf M, Frydas A, Braunauer K et al (2018) Potential usefulness and clinical relevance of adding left atrial strain to left atrial volume index in the detection of left ventricular diastolic dysfunction. JACC Cardiovasc Imaging 11(10):1405–15
Pugliese NR, Paneni F, Mazzola M, De Biase N, Del Punta L, Gargani L et al (2021) Impact of epicardial adipose tissue on cardiovascular haemodynamics, metabolic profile, and prognosis in heart failure. Eur J Heart Failure 23(11):1858–71
Hussain N (2016) Implications of using HBA1C as a diagnostic marker for diabetes. Diabetol Inter 7(1):18–24
Nabati M, Salehi A, Hatami G, Dabirian M, Yazdani J, Parsaee H (2019) Epicardial adipose tissue and its association with cardiovascular risk factors and mitral annular calcium deposits. Ultrasound 27(4):217–24
Iacobellis G, Ribaudo MC, Assael F, Vecci E, Tiberti C, Zappaterreno A et al (2003) Echocardiographic epicardial adipose tissue is related to anthropometric and clinical parameters of metabolic syndrome: a new indicator of cardiovascular risk. J Clin Endocrinol Metab 88(11):5163–8
Iacobellis G, Barbaro G, Gerstein HC (2008) Relationship of epicardial fat thickness and fasting glucose. Int J Cardiol 128(3):424–6
Iacobellis G, Leonetti F (2005) Epicardial adipose tissue and insulin resistance in obese subjects. J Clin Endocrinol Metab 90(11):6300–2
Carlsson M, Ugander M, Mosén H, Buhre T, Arheden H (2007) Atrioventricular plane displacement is the major contributor to left ventricular pumping in healthy adults, athletes, and patients with dilated cardiomyopathy. Am J Physiol-Heart Circul Physiol 292(3):H1452–H9
Gabriel RS, Klein AL (2009) Modern evaluation of left ventricular diastolic function using Doppler echocardiography. Current Cardiol Rep 11(3):231–8
Opdahl A, Remme EW, Helle-Valle T, Lyseggen E, Vartdal T, Pettersen E et al (2009) Determinants of left ventricular early-diastolic lengthening velocity: independent contributions from left ventricular relaxation, restoring forces, and lengthening load. Circulation 119(19):2578–86
Ommen SR, Nishimura RA, Appleton CP, Miller F, Oh JK, Redfield MM et al (2000) Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation 102(15):1788–94
Silbiger JJ (2019) Pathophysiology and echocardiographic diagnosis of left ventricular diastolic dysfunction. J Am Soci Echocardio 32(2):216–32
Acknowledgements
This study was Dr. Farideh Moradgholi postgraduate thesis. The authors hereby extend their gratitude to all participants and hospital staff for the time and work they put into this research.
Funding
There is no funding source.
Author information
Authors and Affiliations
Contributions
MN designed the study, collected data and approved final version of manuscript, MM did statistical analysis, FM did literature and clinical review and interpreted data, and HP collected data and drafted the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by Mazandaran University of Medical science ethical committee (ethics code no. IR.MAZUMS.REC.1400.628). Also, written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no Competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nabati, M., Moradgholi, F., Moosazadeh, M. et al. The correlation between epicardial fat thickness and longitudinal left atrial reservoir strain in patients with type 2 diabetes mellitus and controls. Ultrasound J 15, 37 (2023). https://doi.org/10.1186/s13089-023-00338-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13089-023-00338-1