
Abstract
Background
Nicolau syndrome is a rare adverse drug reaction clinically presented with painful erythema and tissue necrosis often accompanied by intramuscular injections of NSAIDS (diclofenac), penicillin, corticosteroids and local anesthetics.
Case presentation
This case report describes a 29-year-old male patient who was repeatedly hospitalized for the treatment of recalcitrant pemphigus vulgaris. When the patient visited for the fourth time to our hospital, he complained of unusual sharp pain over the right gluteal region ever since the administration of diclofenac 75 mg intramuscular injection for persistent back pain during his previous stay. On physical examination, the right gluteal region showed a globular swelling with erythema and pus filled necrosed tissue. The CT scan did not show any presence of hematoma, ruling out any possibility of compartment syndrome. Based on this clinical evidence he was diagnosed with Nicolau Syndrome secondary to diclofenac injection. The tissue injury necessitated surgical debridement and after a span of 2 months, it healed leaving a permanent scar. In addition, this case report highlights the treatment of recalcitrant pemphigus vulgaris with rituximab therapy.
Conclusion
Clinical pharmacist plays a vital role in educating healthcare professionals about following right protocol for administration of injectable drugs, early detection and management of the ADR. Similarly, patient receiving injections should be educated about warning signs and symptoms of such adverse drug reaction.
Similar content being viewed by others


Background
Pemphigus vulgaris is a rare non-contagious autoimmune disease, that clinically manifests with blisters and erosion of mucosal or mucocutaneous layer of skin. The worldwide incidence of pemphigus vulgaris is 0.1–0.5 per 100,000 population per year but India has a higher incidence of 4.4 per 100,000 population per year [1]. There are various types of pemphigus disease but pemphigus vulgaris and pemphigus foliaceous are more frequently encountered. The genetic susceptibility is demonstrated in people with HLA- DRB (human leucocyte antigen DR beta 1), HLA-DQA1 (human leucocyte antigen DQ alpha 1) and DQB1 (human leucocyte antigen DQ beta 1) along with increased frequencies of HLA-DRB1_0402 and HLA-DRB1_1404 [2]. Pemphigus has an estimated mortality rate of 60–90%, and if left untreated, the condition can worsen within one to three years [3]. The management of pemphigus mainly consists of treatment with corticosteroids, immunosuppressants and rituximab therapy [3]. Pemphigus patients frequently experience flare-up of symptoms, and one of the major contributing factors is poor compliance to the recommended therapy [4]. Nicolau syndrome is an unusual adverse drug reaction alternatively referred as embolia cutis medicamentosa or livedoid dermatitis. The first instance of nicolau syndrome due to bismuth salt was documented in 1924 [5]. Ever since then several theories have been put up, the widely supported hypothesis assumes to have a vascular origin, when an injection is administered it causes direct injury to the small arteries stimulating vasospasm, which further restricts the blood supply and results into necrosis of the surrounding. It initially presents with pain in the injection site, erythema, tenderness, local ischemia followed by necrosis and abscesses formation [6]. These serious complications can result by Intramuscular or intra- articular injections [7]. Although intramuscular injections are commonly used in hospitals, they are not always administered correctly. Most of the time, the drug is delivered into the subcutaneous region rather than muscle, resulting in adverse effects such as edema, granuloma formation, sciatic nerve injury, and tissue necrosis (Nicolau syndrome). [8]. This case report describes the presentation of a life-threatening disease with a rare adverse reaction and highlights the role of pharmacist in various clinical activities.
Case report
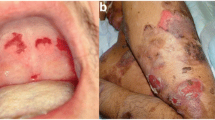
A 29-year-old male patient suddenly developed fluid filled blisters all over the left shoulder 6 months ago and the blisters spread to his right shoulder, back and face in a span of 10 days. He consulted a local doctor and only based on physical examination he was prescribed with oral corticosteroids (prednisolone 20 mg twice a day) and topical medications (Clobetasol propionate 0.05% once a day) for a period of 3 months, but he discontinued the treatment after 1 month as his symptoms had relieved. After few days, he again developed the blisters all over chest, upper and lower limbs and abdomen. He visited our hospital with well-defined hyperpigmented fluid filled lesions and erosions all over his shoulders, chest, back, abdomen and bilateral lower limbs (Fig. 1), which presented a positive marginal nikolsky sign. The Nikolsky sign is a diagnostic indicator which is demonstrated by applying lateral pressure on an intact blister, causing the overlying epidermis to remove and exposing a wet pink skin. This draws an inference of positive Nikolsky sign. Whereas negative sign reveals a dried skin [9]. All Hematological investigations and biochemistry reports were found to be normal. We assessed the severity of the disease using pemphigus disease area index (Table 1).

Fluid filled blisters in pemphigus vulgaris
A skin biopsy was performed and the features confirmed the diagnosis as pemphigus vulgaris. Along with the skin manifestations he presented signs of depression and anxiety with loss of 3kgs in the past 20 days. A psychiatric reference was taken and diagnosed with adjustment disorder secondary to the disease pemphigus vulgaris. For the management of pemphigus patient was treated with dexamethasone azathioprine pulse therapy for 3 days and as steroid sparing agent tablet azathioprine 50 mg was given once a day, to prevent infections in open skin erosions he was prescribed with ceftriaxone intravenous (IV) 1 g twice daily, metronidazole IV 400 mg twice daily and a combination of clobetasol propionate plus gentamycin sulfate topical ointment to be applied over the lesions twice daily, for depression he was prescribed with antidepressants sertraline 50 mg tablet once a day and clonazepam 0.25 mg tablet once a day. The patient stayed in hospital for 5 days and was later discharged with medications: prednisolone 10 mg tablet once daily, doxycycline 100 mg capsule twice daily for 5 days, azathioprine 50 mg tablet once daily, sertraline 50 mg tablet once a day and clonazepam 0.25 mg tablet once a day. Pharmacist counseled the patient about rinsing the oral cavity after administration of prednisolone tablet as it may cause oral candidiasis. Moreover, the pharmacist had also advised the patient to visit the hospital after 2 weeks for follow-up laboratory tests since prednisolone and azathioprine has the propensity to elevate the blood glucose levels and serum creatinine levels, respectively. However, he skipped the follow-up appointment and returned after one and a half month with same complaints but this time the lesions had progressed to the scalp and the lower limbs; fortunately, the laboratory investigations were normal. He was treated for 7 days with Dexamethasone azathioprine pulse 2 therapy, azathioprine 50 mg tablet once daily as maintenance dose, azithromycin 500 mg tablet once a day for 7 days and he was advised to apply the topical medication of combination clobetasol propionate and gentamycin sulfate over the scalp. After 14 days he was discharged with azathioprine 50 mg tablet once a day, clonazepam 0.25 mg tablet once a day and sertraline tablet was changed to escitalopram 10 mg tablet once a day which has less adverse effects when compared to sertraline. The patient came for follow-up after one month and this time the lesions had appeared on bilateral buccal mucosa and crusted lesions over scalp. He again underwent Dexamethasone azathioprine pulse 3 therapy and for maintenance of remission, he was prescribed with dexamethasone 100 mg IV once daily, azathioprine 50 mg tablet once a day, ceftriaxone IV 1 g twice daily, metronidazole 400 mg IV twice daily, clonazepam 0.25 mg tablet once a day, escitalopram 10 mg tablet once a day, for the crusted lesions in the scalp dressings soaked in normal saline with topical cream of clobetasol propionate and gentamycin sulfate were wrapped over the scalp. The pharmacist did not report any major drug interactions, all the drugs were well tolerated by the patient. He was discharged with azathioprine tablet 50 mg once a day, clonazepam 0.25 mg tablet once a day, escitalopram 10 mg tablet once a day, calcium 500 mg tablet once a day and a topical cream of clobetasol propionate and gentamycin sulfate. He visited the outpatient department after 3 weeks with complaints of new blisters all over his body. Upon interviewing we found he had discontinued the medication for 2 weeks and Morisky medication adherence scale was used to evaluate our patient's adherence, and it revealed a score of 4, indicating low adherence (Table 2) [10]. He was readmitted, laboratory investigations were normal and Dexamethasone azathioprine pulse 4 therapy was initiated and adjuvant maintenance therapy with dexamethasone 100 mg once daily, azathioprine 50 mg tablet once a day and framycetin cream was applied all over scalp twice a day along with povidone iodine 5% w/v solution in 1:2 dilution. On the last day of his hospital stay he complained of back pain for which he was administered diclofenac IM 75 mg on the gluteal muscle. He immediately experienced sharp pain which he neglected and did not inform the hospital staff. He was discharged with azathioprine 50 mg tablet once a day, clonazepam 0.25 mg tablet once a day, escitalopram 10 mg tablet once a day, and a topical cream of clobetasol propionate and gentamycin sulfate. After 10 days he came to the hospital complaining of pain in right gluteal region with erythema and necrosed area of 6 cm × 2 cm (Fig. 2). A CT scan was performed and no hematoma was found. Patient stated a history of IM diclofenac injection administration in right gluteal region. Clinical pharmacist classified the case as a probable adverse drug reaction (ADR) with a score of + 5 on the Naranjo ADR probability assessment scale [11], and using ADR Hartwig severity assessment scale the severity of ADR was graded as level 5 [12]. Finally, based on the clinical features it was diagnosed as a rare adverse drug reaction “Nicolau Syndrome” (NS). Clinical pharmacist provided the patient with precautionary yellow card (https://yellowcard.mhra.gov.uk) and this adverse drug reaction was reported to pharmacovigilance program of India (PvPI) (https://www.ipc.gov.in/PvPI/pv_home.html).

6 cm × 2 cm necrosed tissue following IM (Intramuscular) diclofenac injection
Patient got operated on the next day to drain the abscess. To prevent wound infection, he was prescribed antibiotics piperacillin and tazobactum 4.5 g IV four times a day, amikacin 500 mg IV twice a day, and injection metronidazole 500 mg thrice a day. Further, a combination of paracetamol 325 mg, serratiopeptidase 15 mg and acelofenac 100 mg tablet twice a day was prescribed to combat pain, inflammation and to promote wound healing. A hydrogel ointment of colloidal silver was prescribed for applying on the wound area. The wound healed after 2 months with a permanent scar. The PDAI scores were assessed during all follow-ups, initially the lesions predominantly involved only chest and scalp (follow-up 1 and 2), but due to lack of compliance to the therapy, the lesions progressed to thighs, face, oral mucous and buttocks. (Table 1 and Fig. 3). He got readmitted for the treatment of pemphigus vulgaris with rituximab therapy. Although, he was reluctant due to high cost of rituximab but eventually agreed when a proper explanation about the efficacy of the drug was given by the pharmacist. He was administered with slow IV infusion of rituximab 1 g in 400 ml normal saline. Patient was observed for 24 h for any adverse effects and rituximab therapy was well tolerated. He was discharged with prednisolone 10 mg tablet once daily, doxycycline 100 mg capsule twice daily for 5 days, and escitalopram 10 mg tablet once a day. Since, the patient was administered with rituximab therapy, he is more prone to opportunistic infections. Further, clinical pharmacist counseled the patient regarding side effects of doxycycline i.e., hypersensitivity reactions and escitalopram such as insomnia, flu like symptoms, constipation etc. The patient was called to remind a follow-up for 2nd dose rituximab therapy after 10 days. After administration of the 2nd dose of rituximab the lesions had subsided, leaving only dried crusts. The extent of pemphigus lesions had reduced after the treatment with rituximab. Figure 3 depicts reduction of pemphigus severity following the administration of rituximab therapy as solid lines, and Table 1 depicts the PDAI scores for follow-up 5 and 6.

Dotted lines represent DAP (Dexamethasone Azathioprine Pulse) therapy and Solid lines represent rituximab therapy
Discussion
Pemphigus vulgaris is a rare acantholytic vesiculobullous disease of autoimmune origin that primarily affects people aged between 45 and 65 years [13]. An unknown stimuli of the immune system triggers B lymphocytes to produce IgG antibodies, that binds with desmoglein protein and initiates apoptosis [14]. All the dead cells subsequently release protease enzymes, further breaking down desmoglein protein. Destruction of desmoglein protein results in acantholysis (loss of cell–cell adhesion). This causes eruption of blisters and erosions, often originating from oral cavity and spreading all over the body [15]. Various scoring systems are used to assess the severity of blistering disease and treatment response. We used pemphigus disease area index (PDAI) scoring system which is summarized in Table 1 and Fig. 3. The PDAI scale includes a total score of 263 points, with 250 reflecting disease activity, out of which 120 represents skin activity, 10 points for scalp activity, and 120 representing mucosal activity. The remaining scores, 12 and 1 reflect the skin and scalp damage scores, respectively. Pemphigus is classified as mild (0–15 points), substantial (15–45 points), or extensive (> 45 points) [16]. Management of pemphigus requires treatment with corticosteroids pulse therapy, and immunosuppressants. Pulse therapy involves administration of high dose corticosteroids through intravenous infusion given in 4 phases [17]. The available pulse therapies are dexamethasone cyclophosphamide pulse (DCP), Dexamethasone Azathioprine Pulse (DAP), Dexamethasone Methotrexate Pulse (DMP). But, when these are administered for a long time, patient tend to get resistant or acquire various adverse effects, making it difficult to control the disease [17]. Alternative treatment option like rituximab is very effective in controlling and preventing reoccurrence of the lesions. Rituximab is a monoclonal antibody, that directly attacks B lymphocytes by binding with CD20 protein, reduction in B cells results in suppression of IgG antibody production [18]. Similarly, our patient initially received Dexamethasone azathioprine pulse therapy for 4 months, but no improvement was seen and finally he was informed about rituximab therapy. The lesions subsided after administering two doses of rituximab leaving only dried crusts. Figure 3 depicts the severity of pemphigus disease and treatment with corticosteroid therapy and rituximab therapy during six months follow-up. Despite having a good efficacy profile, the high cost and little knowledge about long term side effects such as severe infections due to neutropenia makes rituximab an unpopular choice of treatment [19]. However, poor adherence to the recommended regimen is a significant contributor to disease recurrence. Additionally, non-compliance increases the duration of the treatment and also makes achieving remission a challenging task [20]. We used the Morisky medication adherence scale to assess the patient's adherence to therapy (Table 2. scoring 4, low adherence). Originally consisting of four questions (MMAS-4), it was later upgraded with eight questions (MMAS-8), which is effective for understanding medicine taking behavior [10]. Further, the NS was diagnosed as adverse drug reaction based on Naranjo ADR assessment scale it (probable, score + 5) and a severity level 5 using ADR Hartwig severity assessment scale. Naranjo algorithm consists of 10 questions that are answered as either Yes, No, or “Do not know”. Different point values (− 1, 0, + 1 or + 2) are assigned to each answer and is useful in assessment of causality for all adverse drug reactions [11]. Another instrument that was used to assess the severity of ADR is the Hartwig’s severity scale. The severity of ADRs is categorized into mild (level 1–2), moderate (level 3–4) and severe (level 5, 6 and, 7) [12]. Further, Table 3 summarizes clinical findings of diclofenac induced Nicolau syndrome case reports obtained from PUBMED and google scholar. NS is a rare and fatal adverse effect caused widely used non-steroidal anti-inflammatory drugs (diclofenac, ketoprofen, ibuprofen, piroxicam, phenylbutazone, ketorolac), penicillin derivatives, antihistamines, vaccines, corticosteroids, glatiramer acetate, local anesthetics and sometimes reported with bismuth salts, interferon-α [21, 22]. NSAIDs like diclofenac can inhibit cyclooxygenase enzyme and suppress prostaglandin synthesis resulting into vasospasm. Moreover, application of cold compress can aggravate the damage [23] and similarly our patient had applied cool pack, which might have aggravated the vasospasm effect. A study conducted by Chan et al. [24] revealed the majority of injections intended for intramuscular injections were actually administered in subcutaneous fat layer. In Table 3 we have summarized the clinical aspects of diclofenac induced nicolau syndrome. Majority of the cases were females; this might be due to excess fat deposited in the gluteal region [25,26,27]. In all the cases, we observed that patients experienced intense pain, with erythema and skin discoloration within two to four days, which subsequently progressed to plaque formation and necrosis of the tissue [27]. Diclofenac was used for headache, pain associated with bone related disorders (gout, arthroplasty, osteoarthritis), [21, 25, 28] post operative pain management and the predominant site of administered was either right or left buttock, perhaps in few cases, necrosis had spread to the other side as well [29]. The abscess and damaged area were infected with Pseudomonas aeruginosa, Streptococcus pneumoniae and Escherichia coli [7, 21, 30, 31]. Whereas in this case the culture sensitivity test was negative. There is no definite tool to identify nicolau syndrome and is often misdiagnosed as acute compartment syndrome, the clinical features are similar in both, except the presence of hematoma or occlusion in artery and involvement of femoral artery makes the differential diagnosis [25, 32]. A CT scan or MRI can also be used to rule of presence of hematoma. A CT scan was performed in our patient and no hematoma was found [31, 33]. The damaged area can be treated by surgical debridement, skin grafting, routine sterile dressings and antibiotics for prophylaxis of any secondary infection. Usually, the prognosis of the adverse reaction depends upon severity and affected area. The recovery period can vary from 1 to 8 months or may even result in death [7, 30, 34, 35]. There are a number of standard operating procedures (SOP) to be followed while administering intramuscular injection. Firstly, the needle used for intramuscular route of administration should be carefully selected based on individual’s physical structure, it is mostly not preferred in obese patient [36]. Usually, a 45 kg patient requires 1.45 inches needle whereas a 90 kg individual may require 2 inches needle [21]. Second, the Z-track method of intramuscular administration should be followed by slightly pulling the skin to leave a zigzag route to minimize the irritation and prevent leakage of the medication to subcutaneous tissue [21, 25]. Third, when a patient requires multiple or large volume of drug administration, same site should be avoided [37]. Although, reoccurrence is unusual in nicolau syndrome, still patient should be provided with precautionary yellow card [38]. Serious adverse reaction can prolong the hospital stay, adding needless healthcare costs and increasing the patient's financial burden. Several studies have suggested that pharmacist participation has reduced medication errors, adverse drug events, hospital readmission and have had a positive impact on treatment related outcomes [39]. In the present case clinical pharmacist played prominent roles like determining the appropriateness of medications prescribed, identifying drug interactions, detection of adverse drug reactions, patient counseling and telephonic follow-up reminders. Moreover, NSAIDs are frequently used in healthcare centers and relative serious adverse reaction can be avoided. Clinical pharmacist can take part in educating the health care workers and patients [38, 39], as well as monitor that proper technique for administration of injections is being followed to prevent future instances.
Conclusion
Nicolau syndrome is unpredictable and is caused by commonly used parenteral form of NSAIDs, local anesthetics, penicillin, corticosteroids. However, clinical pharmacist can conduct awareness program about following right protocol for administration of injectable drugs, early detection and management of adverse drug reactions among health care workers. Similarly, clinical pharmacist can provide patient education about warning signs and symptoms of such adverse drug reaction. This will minimize the hospital re-admission; length of hospital stays and additional health care cost.
Availability of data and materials
Not applicable.
Abbreviations
- ADR:
-
Adverse drug reaction
- CT:
-
Computed tomography
- HLA:
-
Human leucocyte antigen
- HLA-DRB:
-
Human leucocyte antigen DR beta 1
- HLA-DQA1:
-
Human leucocyte antigen DQ alpha 1
- HLA-DQB1:
-
Human leucocyte antigen DQ beta 1
- IM:
-
Intramuscular
- IV:
-
Intravenous
- DAP:
-
Dexamethasone azathioprine pulse therapy
- MMAS-4:
-
Morisky medication adherence scale 4
- MMAS-8:
-
Morisky medication adherence scale 8
- MRI:
-
Magnetic resonance imaging
- NSAID:
-
Non-steroidal anti-inflammatory drugs
- NS:
-
Nicolau syndrome
- PV:
-
Pemphigus vulgaris
- SOP:
-
Standard operating procedure
References
Kumar Chaudhary R, Bhandari R, Doshi B, Karoli SS, SpoorthiMarripalli S, Ganachari MS (2022) Gefitinib induced pemphigus vulgaris with PRIDE complex. J Oncol Pharm Pract 28(6):1465–1473
Petzl-Erler ML (2020) Beyond the HLA polymorphism: a complex pattern of genetic susceptibility to pemphigus. Genet Mol Biol 1:43
Kridin K (2018) Pemphigus group: overview, epidemiology, mortality, and comorbidities. Immunol Res 66(2):255–270
Popescu IA, Statescu L, Vata D, Porumb-Andrese E, Patrascu AI, Grajdeanu IA, Solovastru LG (2019) Pemphigus vulgaris-approach and management. Exp Ther Med 18(6):5056–5060
Kartal SP, Alper M, Gürçay N (2016) Nicolau syndrome: a rare complication of injection that should be kept in mind. Hong Kong J 1(24):201–204
Uri O, Behrbalk E (2009) Tissue necrosis following intramuscular administration of various drugs (Nicolau syndrome): clinical presentation, pathophysiology and treatment. Harefuah 148(3):186–188
Arslan MN, Melez DO, Akcay A, Gur A, Sam B, Guven AS (2016) Coincidence of nicolau syndrome and rhabdomyolysis: report of a forensic autopsy case and review of the literature. J Forensic Sci 61(5):1369–1374
Burbridge BE (2007) Computed tomographic measurement of gluteal subcutaneous fat thickness in reference to failure of gluteal intramuscular injections. Can Assoc Radiol J 58(2):72
Maity S, Banerjee I, Sinha R, Jha H, Ghosh P, Mustafi S (2020) Nikolsky’s sign: a pathognomic boon. J Fam Med Prim Care 9(2):526
Morisky DE, Green LW, Levine DM (1986) Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1:67–74
Naranjo C, Busto U, Sellers E, Sandor P, Ruiz I, Roberts E (1981) Naranjo ADR probability scale. Clin Pharmacol Ther 30:239–245
Hartwig SC, Siegel J, Schneider PJ (1992) Preventability and severity assessment in reporting adverse drug reactions. Am J Hosp Pharm 49(9):2229–2232
Banerjee I, Bhowmik B, Maji A, Sinha R (2018) Pemphigus vulgaris–a report of three cases and review of literature. J Fam Med Prim Care 7(5):1109
Rehman A, Huang Y, Wan H (2021) Evolving mechanisms in the pathophysiology of pemphigus vulgaris: a review emphasizing the role of desmoglein 3 in regulating p53 and the Yes-associated protein. Life 11(7):621
Burmester IA, Flaswinkel S, Thies CS, Kasprick A, Kamaguchi M, Bumiller-Bini V, Emtenani S, Feldmann N, Kridin K, Schmidt E, van Beek N (2020) Identification of novel therapeutic targets for blocking acantholysis in pemphigus. Br J Pharmacol 177(22):5114–5130
Murrell DF, Dick S, Ahmed AR, Amagai M, Barnadas MA, Borradori L, Bystryn JC, Cianchini G, Diaz L, Fivenson D, Hall R (2008) Consensus statement on definitions of disease, end points, and therapeutic response for pemphigus. J Am Acad Dermatol 58(6):1043–1046
Mustafi S, Sinha R, Hore S, Sen S, Maity S, Ghosh P (2019) Pulse therapy: opening new vistas in treatment of pemphigus. J Fam Med Prim Care 8(3):793
El Tal AK, Posner MR, Spigelman Z, Ahmed AR (2006) Rituximab: a monoclonal antibody to CD20 used in the treatment of pemphigus vulgaris. J Am Acad Dermatol 55(3):449–459
Cianchini G, Corona R, Frezzolini A, Ruffelli M, Didona B, Puddu P (2007) Treatment of severe pemphigus with rituximab: report of 12 cases and a review of the literature. Arch Derm 143(8):1033–1038
Ratnawidya W, Irmagita A (2016) Oral pemphigus vulgaris: the importance of patient's adherence. Paper presented at: International Dentistry Scientific Meeting; 2016, Depok, Indonesia. Accessed 26 December 2022. https://www.researchgate.net/publication/312408931_Oral_Pemphigus_Vulgaris_The_Importance_of_Patient's_Adherence
Lie C, Leung F, Chow SP (2006) Nicolau syndrome following intramuscular diclofenac administration: a case report. J Orthop Surg 14(1):104–107
Okan G, Canter HI (2010) Nicolau syndrome and perforator vessels: a new viewpoint for an old problem. Cutan Ocul Toxicol 29(1):70–72
Şenel E, Ada S, Güleç AT, Çağlar B (2008) Nicolau syndrome aggravated by cold application after im diclofenac. J Dermatol 35(1):18–20
Chan VO, Colville J, Persaud T, Buckley O, Hamilton S, Torreggiani WC (2006) Intramuscular injections into the buttocks: are they truly intramuscular? Eur J Radiol 58(3):480–484
Kim KK (2011) Nicolau syndrome in patient following diclofenac administration: a case report. Ann Dermatol 23(4):501–503
Kılıç İ, Kaya F, Özdemir AT, Demirel T, Çelik İ (2014) Nicolau syndrome due to diclofenac sodium (Voltaren®) injection: a case report. J Med Case Rep 8(1):1–4
Park HJ, Kim MS, Park NH, Jung SW, Park SI, Park CS (2011) Sonographic findings in Nicolau syndrome following intramuscular diclofenac injection: a case report. J Clin Ultrasound 39(2):111–113
Killedar RS, Gupta S, Shindhe P (2021) Ayurveda management of Nicolau syndrome WSR to Kotha–a case report. J Ayurveda Integr Med 12(1):165–168
Sasmal PK, Sahoo A, Singh PK, Vikram VS (2021) Nicolau syndrome: an unforeseen yet evadable consequence of intramuscular injection. Surg J 7(02):e62–e65
Rygnestad T, Kvam AM (1995) Streptococcal myositis and tissue necrosis with intramuscular administration of diclofenac (Voltaren). Acta Anaesthesiol Scand 39(8):1128–1130
Geerts JW, Siegel AM, Bosman A (2014) A woman with complaints after an injection of diclofenac. Ned Tijdschr Geneeskd 158:A7351
Hamilton B, Fowler P, Galloway H, Popovic N (2008) Nicolau syndrome in an athlete following intra-muscular diclofenac injection. Acta Orthop Belg 74(6):860
Maneshi A, Ravi S, Salehi MR, Hasannezhad M, Khalili H (2017) Nicolau syndrome. Arch Iran Med 20(1):60–64.
Bhanja DB, Sil A, Chakraborty S (2020) Intramuscular diclofenac-induced iatrogenic cutaneous necrosis. Postgrad Med J 96(1135):298–299
Gulseren D, Sahin EB, Bozdogan O, Artuz F (2017) An avoidable adverse drug reaction: nicolau syndrome. Int Wound J 14(2):440
Keen MF (1986) Comparison of intramuscular injection techniques to reduce site discomfort and lesions. J Nurs Res 35(4):207–210
Kara D, YapucuGüneş Ü (2016) The effect on pain of three different methods of intramuscular injection: a randomized controlled trial. Int J Nurs Pract 22(2):152–159
Chaudhary RK, Metgudmath AR, Bhandari R, Karoli SS (2021) Fixed drug eruptions secondary to fixed drug combination (ofloxacin/ornidazole): a cross sensitivity case report. Curr Drug Therapy 16(5):448–453
Phatak A, Prusi R, Ward B, Hansen LO, Williams MV, Vetter E, Chapman N, Postelnick M (2016) Impact of pharmacist involvement in the transitional care of high-risk patients through medication reconciliation, medication education, and postdischarge call-backs (IPITCH Study). J Hosp Med 11(1):39–44
Acknowledgments
We thank our Head of the Department, Pharmacy Practice, KLE College of Pharmacy Belagavi. We would like to thank Department of Dermatology, KLE Dr Prabhakar Kore Hospital for their Constant support and guidance.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
DA collected and assessed the case. DA wrote the final manuscript. S revised and edited the final version of manuscript. SW and BD supervised and approved the final version of manuscript. SW holds the responsibility of the final draft.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
The consent for publication of the content was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Avvaru, D., Patil, S., Doshi, B. et al. Nicolau syndrome with pemphigus vulgaris: a rare case report and review of literature. Futur J Pharm Sci 9, 60 (2023). https://doi.org/10.1186/s43094-023-00513-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-023-00513-0