
Abstract
Background
Claudin-18 (CLDN18) is a recently identified anticancer therapeutic target with promising results for various gastrointestinal malignancies. The role of CLDN18 in prostatic carcinoma has not been investigated. The aim of this study was to investigate CLDN18 and androgen receptor (AR) expression in prostatic carcinoma and to link these findings with other clinicopathological characteristics. This retrospective study was carried out on 120 cases of prostatic lesions, including 100 cases of prostatic carcinoma and 20 cases of benign prostatic hyperplasia. The immunohistochemical staining technique was used to evaluate the expression of both CLDN18 and AR in prostatic carcinoma in relation to clinicopathological parameters.
Results
CLDN18 expression was completely absent in benign prostatic tissue, while it was detected in the membrane of 30 (30%) of studied carcinoma cases, with a statistically significant difference (p = 0.046). In contrast to other variables, a statistically significant relationship was identified between CLDN18 expression and Gleason Grade group (p = 0.000), stage (p = 0.03), and nodal metastasis (p = 0.000). The expression of the androgen receptor was detected in the nucleus of 96 (96%) of the cancer cases under study, with no statistically significant difference between the studied groups (p = 0.427). A statistically significant relation was found between AR expression and Gleason Grade group (p = 0.03) and stage (p = 0.01), while no relation with other variables was detected. AR expression and CLDN18 expression were shown to be statistically significantly correlated (p = 0.002).
Conclusions
CLDN18 was expressed in prostatic carcinoma and correlated with an adverse tumor outcome. CLDN18 may be regulated by AR. CLDN18 could be a candidate therapeutic marker for the treatment of prostatic carcinoma.
Similar content being viewed by others


1 Background
Prostate cancer is the most common cancer among men in Western societies and the 2nd most diagnosed cancer in men worldwide [1]. There are an estimated 288,300 new prostate cancer cases and 34,700 deaths expected for 2023 in the United States [2].
In Egypt, according to GLOBOCAN 2020, prostate cancer is the 7th most prevalent cancer, with 4767 new cases and 2227 deaths. From the age of 50 onward, there is an estimated 22% frequency of prostate cancer among Egyptian men [3].
Age, family history, and a few genetic abnormalities (such as BRCA1 and BRCA2) are the only factors that have been proven to increase the risk of developing prostate cancer. Prostate cancer is significantly more likely in people over 50. Sixty to 70 years old is when the incidence peaks. Additional risk factors for advanced prostate cancer include smoking, being overweight, and certain dietary components [4].
Depending on the clinical context, multiple therapeutic approaches are needed for prostate cancer because it is a clinically and molecularly heterogeneous disease [5]. An important lineage-specific, carcinogenic transcriptional pathway in prostate cancer is triggered when the androgen steroid hormone interacts with the androgen receptor (AR). This fact has been used therapeutically for many years to treat de novo or recurrent metastatic disease following initial surgery or radiotherapy. Castration-resistant prostate cancer (CRPC) eventually develops in most patients who first respond to androgen deprivation therapies, even though these treatments stopped tumor growth initially [6].
Recently, new techniques were adopted for better understanding different pathways that promote tumor growth and progression, with the subsequent development of promising therapeutic strategies for the treatment of prostate cancer [5].
The Claudin family comprises at least 27 transmembrane proteins, which are important parts of tight junctions [7]. According to their sequence, they are classified into classic and non-classic types [8]. CLDNs 1–10 are examples of classic types, while CLDN16 and CLDN18 are examples of non-classic types [9]. CLDNs are expressed differentially in a variety of tissues, such as gastric, pancreatic, and lung tissues, and the formation of cancers in these tissues depends on their altered tissue function [10].
Claudin-18.1 is one of the two splicing variants of claudin-18, which is expressed in the lung, whereas claudin-18.2, which is only expressed in differentiated gastric mucosal cells, has very little expression in other healthy normal tissues [11]. Several gastrointestinal, ovarian, and non-small cell lung carcinomas expressed claudin-18.2 [12,13,14]. Recently created monoclonal antibodies (mAb) and chimeric antigen receptor modified T-cells (CAR-T) specific for claudin-18.2 have been used with encouraging outcomes for advanced pancreato-biliary tract and gastroesophageal tract malignancy management [15, 16].
The role of claudin-18 expression in prostatic carcinoma has not been evaluated.
The purpose of this study was to examine the expression of claudin-18 and the androgen receptor in prostatic carcinoma and to link these findings with other clinicopathological characteristics.
2 Methods
This retrospective observational study was carried out on 120 cases of prostatic lesions, including 100 cases of prostatic carcinoma and 20 cases of benign prostatic hyperplasia. The studied cases included archival formalin-fixed, paraffin-embedded tissue blocks processed during the years 2015–2023 by the Pathology Department of the Faculty of Medicine. All the specimens were obtained by prostatectomy. The research ethics committee of the faculty of medicine approved the study (NO:RC1-8-2023).
2.1 Histopathological analysis
Four-micron-thick sections of each tissue block were stained with hematoxylin and eosin (H&E) stain and revised by two independent pathologists to confirm the diagnosis. For grading, we applied the ISUP 2019 Gleason grading system [17] and staged using the American Joint Committee on Cancer (AJCC) 2017 TNM staging system [18].
2.2 Immunohistochemical analysis
Anti-claudin18 and anti-AR immunostaining were done for each case using the Avidin–Biotin complex technique according to the manufacturer's instructions. Antigen retrieval was performed using 10 mmol/1 citrate buffer (ph. 6.0). Primary antibodies, anti-claudin18 antibody (Invitrogen, Carlsbad, CA; polyclonal, 1:100), and Anti-AR antibody (Proteintech, Wuhan, China, monoclonal,1:100), were used. Primary antibodies were then added and incubated at room temperature overnight in a humidity chamber. Diaminobenzene (DAB) was used as a chromogen.
2.3 Positive control
Apparently normal gastric tissue was used as a positive control for CLDN18 [19], and for AR, apparently normal prostatic tissue was used [20]. Negative controls were prepared by omitting the primary antibody during staining and replacing it with saline or phosphate buffer.
2.4 Immunohistochemical assessment
2.4.1 Assessment of CLDN18 immunostaining
CLDN18 immunostaining was graded as negative, weakly positive, moderately positive, or strongly positive, according to Tanaka et al. [21].
2.4.2 Assessment of AR immunostaining
The immunostaining of AR was evaluated based on the percentage of nuclear positive staining cells; it is considered positive if (≥ 10%) of cells showed nuclear staining or negative (< 10%) [22].
2.5 Statistical analysis
The Statistical Package for the Social Sciences (SPSS) program, version 22 (SPSS Inc., Chicago, Illinois, USA), was used to analyze the results. Categorical data were presented as numbers and percentages using the Chi square test (χ2 test) or Fisher Exact test for their analysis. A P value < 0.05 was judged statistically significant, and a P value < 0.01 was considered statistically highly significant.
3 Results
3.1 Histopathological results
The current work included 120 cases of prostatic lesions, including 100 cases of prostatic carcinoma and 20 cases of benign prostatic hyperplasia. The mean age for prostatic carcinoma cases was 65 years. The clinicopathological data are detailed in Table 1.
3.2 Immunohistochemical Results
3.2.1 Immunohistochemical assessment results of claudin-18 expression
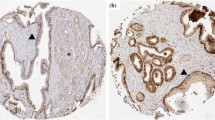
Claudin-18 expression was detected in the membrane of 30 (30%) of studied carcinoma cases. Benign prostatic hyperplasia cases showed complete absence of staining (Fig. 1). There was a statistically significant correlation between claudin-18 expression & the studied groups (p = 0.046) (Table 2).

Representative samples of claudin-18 expression: A, B Claudin-18 expression in prostatic carcinoma with a low Gleason score (A, ABC X200; B, ABC X200), C Claudin-18 expression in prostatic carcinoma with a high Gleason score (ABC X400), and D Benign prostatic hyerplasia showing negative expression for claudin-18 (ABC X200)
3.2.2 Comparison of Claudin-18 expression with the clinic-pathological data of the studied prostatic carcinoma cases
A statistically significant correlation was found between claudin-18 expression and nodal metastasis (p = 0.000), tumor stage (p = 0.03), and Gleason grade group (p = 0.000), while no correlation was found with other variables (Table 3).
3.2.3 Immunohistochemical assessment results of androgen receptor
The expression of Androgen receptor was detected in the nucleus of 96 (96%) of studied carcinoma cases and in 18 (90%) cases of benign prostatic hyperplasia (Fig. 2). No statistically significant correlation was found between the studied groups and AR expression (p = 0.427) (Table 4).

Representative samples of androgen receptor (AR) expression: (A), AR expression in prostatic carcinoma with a low Gleason score (A, ABC X200), B, C AR expression in prostatic carcinoma with a high Gleason score ( B, ABC X400; C,ABC X200), and D Benign prostatic hyerplasia showing positive expression for AR (ABC X200)
3.2.4 Comparison of androgen receptor expression with the clinic-pathological data of the studied prostatic carcinoma cases
A statistically significant correlation was found between AR expression and stage (p = 0.01), and Gleason grade group (p = 0.03), while no correlation was found with other variables (Table 5).
3.2.5 correlation between androgen recetor expression and claudin18 expression
A statistically significant correlation was found between androgen receptor expression and claudin18 expression (p = 0.002) (Fig. 3).

Correlation between Caudin18 and androgen receptor markers expression
4 Discussion
Claudin-18 is one of the claudin family that participates in tight junction strands in epithelial cells [11]. It was recognized in a variety of gastrointestinal, ovarian, and non-small cell lung carcinomas [13, 14, 23, 24]. The role of claudin-18 in prostatic carcinoma has not been clarified.
In the current study, benign prostatic tissue failed to stain with CLDN18, while in prostatic carcinoma, lower rates of CLDN18 positivity were recorded (30%), and this difference was of statistical significance (p = 0.046). The pattern of expression for CLDN18 from benign to malignant may suggest that CLDN18 could have a role in the genesis and development of prostatic carcinoma.
The claudin protein family has previously been examined, demonstrating a putative function for claudins in the development of prostatic cancer, which is compatible with our findings. Sheehan et al. [25] discovered that 41% of carcinomas had a higher level of claudin-1 than normal prostatic glands in 41% of tumors. Väre et al. [26] found claudin-1 positivity in 97% of cancers, with 43% showing strong immunostaining. According to Kind et al. [1], claudin-1 was overexpressed in a subset of prostate cancers. Landers et al. [27] observed that claudin-4 levels were increased in primary and metastatic prostate cancer. Claudin-8 was expressed in malignant tissues relative to normal ones, with a significant difference, according to Ashikari et al. [28]. Claudin-3 loss of expression was a prognostic marker in castration-resistant prostate cancer according to Orea et al. [29].
Analysis of CLDN18 expression was linked to lower Gleason grade score (p = 0.000). To what we know, this is the first study to evaluate this relationship, so we looked into the relationship of CLDN18 to tumor grades in additional organs. Pellino et al. [30] found similar associations in studied cases of advanced gastric and gastroesophageal junction adenocarcinomas. Analysis of CLDN18 by Kayikcioglu et al. [31] was high in lower grades of pancreatic ductal adenocarcinoma but did not reach a significant level.
Regarding the relationship of various claudins in prostatic carcinoma to the Gleason score, Landers et al. [27] reported that claudin-4 was expressed more in primary tumors with a Gleason score of 6 than higher Gleason scores. The low expression of claudin-1 was detected in Gleason scores of 7 or higher by Seo et al. [32]. Claudin-3 expression was found to be considerably lower in tissues of individuals with a Gleason score (≥ 8) by Orea et al. [29]. This runs in parallel with the hypothesis that tight junctions are destructed during tumorigenesis with disruption of cell adhesion molecules, contributing to cell invasiveness and metastases [33].
Claudin-18 expression was shown to be higher in advanced-stage tumors (p = 0.03). CLDN18 expression may play a role in tumor formation and progression. CLDN18 expression during tumor growth causes tight junctions to loosen, which may promote tumor cell motility and invasiveness [34].
To our awareness, no studies in the literature investigated this relation in prostatic carcinoma; however, studies in gastric and gastroesophageal junction adenocarcinomas by Pellino et al. [30] which matched our results, and in pancreatic ductal adenocarcinoma by Kayikcioglu et al. [31], where high CLDN18 expression was detected in advanced stages but did not reach a significant level.
The relation between claudin-4 expression and advanced stages of prostatic carcinoma was evaluated by Sheehan et al. [25] and reported a significant correlation.
Regarding the association between CLDN18 and lymph node metastasis, there was a statistically highly significant association (p = 0.000). This was compatible with Phattarataratip and Sappayatosok [35], who discovered that claudin-7 had a significant effect on oral squamous cell cancer. Claudin-7 alterations were linked to pathological grade, tumor size, and advanced TNM stage. Moreover, Wöll et al. [36] in pancreatic carcinoma detected higher CLDN18 expression in the lymph node metastasis-positive group. This observation could be beneficial in the development of novel targeted therapies for patients with lymph node metastases.
Androgen receptor plays pivotal roles in prostate cancer. AR has already been identified as the primary driver in the genesis and progression of prostate cancer [37].
In the present study, AR expression was detected in the nucleus of 96 (96%) of the studied carcinoma cases and in 18 (90%) cases of benign prostatic hyperplasia. No statistically significant difference was detected between AR expressions in both groups (p = 0.427). Similar results by Lai et al. [38] and Navaei et al. [39] were obtained. Lekshmy and Prema [40] reported AR expression in almost all prostate cancer cases as well.
Androgens greatly affect prostate cancer growth rates and development from preclinical to clinically relevant forms, which may be due to altered androgen metabolism.
We demonstrated that AR was correlated with the Gleason grade group (p = 0.03). In a study by Kwang et al. [41], the frequency of AR expression was higher in the group with the highest Gleason scores; similar results were obtained by Lai et al. [38]. Hashmi et al. [42] also found that low-grade tumors did not show strong AR expression, while patients in high-grade group showed strong AR expression. Hermien et al. [43] found high scores of AR expression, especially in the WHO grade groups III–V. Increased levels of AR may be especially important in driving tumor cell proliferation [44].
An association between AR and high stages of prostatic carcinoma (p = 0.01) was illustrated in our study. Similarly, Li et al. [45] documented that a high AR expression level was correlated with clinical stage. Heinlein and Chang [37] also found that high AR expression correlates with disease progression. In prostate cancer, the rate of proliferation exceeds that of cell death, where AR regulates the proliferation-death ratio of these cells. Therefore, the increased expression of AR is associated with the aggressiveness of prostate adenocarcinoma, including high grades and advanced stages.
The relationship between AR expression and LN metastasis was not found to be significant (p = 0.090). In a study conducted by Kwang et al. [41], the relationship was not statistically significant. On the contrary, Li et al. [45] documented that high AR expression levels were associated with the presence of LN metastasis.
We found a significant relationship between CLDN18 and AR expression (p = 0.002), indicating that CLDN18 may be regulated by AR. Meng et al. [46] showed that testosterone regulates the expression of CLDN8 in the prostate of mice, stating that castration resulted in lower levels of CLDN8 and a loss of the tight junction barrier, resulting in a loss of immunological privilege, inflammation, and an autoimmune reaction. It is generally understood that inflammatory responses and immunological processes play an important role in cancer genesis and progression. CLDN8-mediated androgen-dependent tight junction system barrier may preserve cellular homeostasis and cytoskeleton structure [46].
In addition, Ashikari et al. [28] showed that increased CLDN8 expression boosted prostate cancer cell growth and invasion and that AR regulates CLDN8. CLDN8 has been identified as an AR target gene in breast cancer cells, with AR being up-regulated following DHT therapy [47]. Zhang et al. [22] discovered a similar parallel relationship between CLDN8 and AR in breast cancer.
5 Conclusion
We demonstrated positive CLDN18 expression in 30% of the studied prostatic carcinoma cases, in contrast to benign prostatic tissue. This pattern of expression may suggest that CLDN18 could have a role in the development of prostatic carcinoma. The significant relationship between CLDN18 expression and Gleason grade group, tumor stage, and nodal metastasis suggests a possible role of CLDN18 in tumor aggressiveness and adverse patient outcomes. The significant correlation between CLDN18 and AR expression indicates that CLDN18 may be regulated by AR to enhance prostate cancer progression. CLDN18 could be a candidate therapeutic target for the treatment of prostatic carcinoma.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on request.
Abbreviations
- Claudin-18:
-
CLDN18
- AR:
-
Androgen receptor
- WHO:
-
World Health Organization
- LVI:
-
Lympho-vascular invasion
- SPSS:
-
Statistical package of social science
- LN:
-
Lymph node.
- PSA:
-
Prostatic specific antigen
References
Kind S, Büscheck F, Höflmayer D, Hube-Magg C, Kluth M, Tsourlakis MC et al (2020) Claudin-1 upregulation is associated with favorable tumor features and a reduced risk for biochemical recurrence in ERG-positive prostate cancer. World J Urol 38:2185–2196
Siegel RL, Miller KD, Wagle NS, Jemal A (2023) Cancer statistics. CA Cancer J Clin 73(1):17–48
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249
Wang L, Lu B, He M, Wang Y, Wang Z, Du L (2022) Prostate cancer incidence and mortality: global status and temporal trends in 89 countries from 2000 to 2019. Front Public Health 10:811044
Vlajnic T, Bubendorf L (2021) Molecular pathology of prostate cancer: a practical approach. Pathology 53(1):36–43
Formaggio N, Rubin MA, Theurillat JP (2021) Loss and revival of androgen receptor signaling in advanced prostate cancer. Oncogene 40(7):1205–1216
Bhat AA, Syed N, Therachiyil L, Nisar S, Hashem S, Macha MA et al (2020) Claudin-1, a double-edged sword in cancer. Int J Mol Sci 21:569
Krause G, Winkler L, Mueller SL, Haseloff RF, Piontek J, Blasig IE (2008) Structure and function of claudins. Biochim Biophys Acta 1778:631–645
Lal-Nag M, Morin PJ (2009) The claudins. Genome Biol 10:235
Morin PJ (2005) Claudin proteins in human cancer: promising new targets for diagnosis and therapy. Cancer Res 65(21):9603–9606
Niimi T, Nagashima K, Ward JM, Minoo P, Zimonjic DB, Popescu NC et al (2001) Claudin-18, a novel downstream target gene for the T/EBP/NKX21 homeodomain transcription factor, encodes lung- and stomach-specific isoforms through alternative splicing. Mol Cell Biol 21:7380–7390
Sahin U, Koslowski M, Dhaene K, Usener D, Brandenburg G, Seitz G et al (2008) Claudin-18 splice variant 2 is a pan-cancer target suitable for therapeutic antibody development. Clin Cancer Res 14(23):7624–7634
Iwaya M, Hayashi H, Nakajima T, Matsuda K, Kinugawa Y, Tobe Y et al (2021) Colitis-associated colorectal adenocarcinomas frequently express claudin 18 isoform 2: implications for claudin 182 monoclonal antibody therapy. Histopathology 79(2):227–237
Coati I, Lotz G, Fanelli GN, Brignola S, Lanza C, Cappellesso R et al (2019) Claudin-18 expression in oesophagogastric adenocarcinomas: a tissue microarray study of 523 molecularly profiled cases. Br J Cancer 121(3):257–263
Lordick F, Al-Batran SE, Ganguli A, Morlock R, Sahin U, Türeci Ö (2021) Patient-reported outcomes from the phase II FAST trial of zolbetuximab plus EOX compared to EOX alone as first-line treatment of patients with metastatic CLDN18.2+ gastroesophageal adenocarcinoma. Gastric Cancer 24(3):721–730
Sahin U, Türeci Ö, Manikhas G, Lordick F, Rusyn A, Vynnychenko I et al (2021) a randomised phase II study of zolbetuximab (IMAB362) plus EOX versus EOX alone for first-line treatment of advanced CLDN18.2-positive gastric and gastro-oesophageal adenocarcinoma. Ann Oncol 32(5):609–619
van Leenders GJ, van der Kwast TH, Grignon DJ, Evans AJ, Kristiansen G, Kweldam CF et al (2020) ISUP grading workshop panel members. the 2019 international society of urological pathology (ISUP) consensus conference on grading of prostatic carcinoma. Am J Surg Pathol 44(8):e87–e99
Amin MB, Edge SB, Greene FL, Byrd DR, Brookland RK, Washington MK et al (2017) AJCC cancer staging manual, 8th edn. New York, Springer
Rohde C, Yamaguchi R, Mukhina S, Sahin U, Itoh K, Türeci Ö (2019) Comparison of Claudin 18.2 expression in primary tumors and lymph node metastases in Japanese patients with gastric adenocarcinoma. Jpn J Clin Oncol 49(9):870–876
Nour El Hoda SI, Khairy RA, Talaat SM, Abd El-Fattah FA (2019) Immunohistochemical expression of androgen receptors (AR) in various breast cancer subtypes. Open Access Maced J Med Sci 7(8):1259
Tanaka M, Shibahara J, Fukushima N, Shinozaki A, Umeda M, Ishikawa S et al (2011) Claudin-18 is an early-stage marker of pancreatic carcinogenesis. J Histochem Cytochem 59(10):942–952
Zhang Y, Zheng A, Lu H, Jin Z, Peng Z, Jin F (2020) The expression and prognostic significance of claudin-8 and androgen receptor in breast cancer. Onco Targets Ther 13:3437
Karanjawala ZE, Illei PB, Ashfaq R, Infante JR, Murphy K, Pandey A et al (2008) New markers of pancreatic cancer identified through differential gene expression analyses: claudin 18 and annexin A8. Am J Surg Pathol 32(2):188–196
Arpa G, Fassan M, Guerini C, Quaquarini E, Grillo F, Angerilli V et al (2022) Claudin-18 expression in small bowel adenocarcinoma: a clinico-pathologic study. Virchows Arch 481(6):853–863
Sheehan GM, Kallakury BV, Sheehan CE, Fisher HA, Kaufman RP, Ross JS (2007) Loss of claudins-1 and -7 and expression of claudins-3 and -4 correlate with prognostic variables in prostatic adenocarcinomas. Hum Pathol 38(4):564–569
Vare P, Loikkanen I, Hirvikoski P, Vaarala MH, Soini Y (2008) Low claudin expression is associated with high Gleason grade in prostate adenocarcinoma. Oncol Rep 19(1):25–31
Landers KA, Samaratunga H, Teng L, Buck M, Burger MJ, Scells B et al (2008) Identification of claudin-4 as a marker highly overexpressed in both primary and metastatic prostate cancer. Br J Cancer 99(3):491–501
Ashikari D, Takayama KI, Obinata D, Takahashi S, Inoue S (2017) CLDN8, an androgen-regulated gene, promotes prostate cancer cell proliferation and migration. Cancer Sci 108(7):1386–1393
Orea MJ, Angulo JC, González-Corpas A, Echegaray D, Marvá M, Lobo MVT et al (2023) Claudin-3 loss of expression is a prognostic marker in castration-resistant prostate cancer. Int J Mol Sci 24(1):803
Pellino A, Brignola S, Riello E, Niero M, Murgioni S, Guido M et al (2021) Association of CLDN18 protein expression with clinicopathological features and prognosis in advanced gastric and gastroesophageal junction adenocarcinomas. J Pers Med 11(11):1095
Kayikcioglu E, Yüceer RO (2023) The role of claudin 18.2 and HER-2 in pancreatic cancer outcomes. Medicine 102(6):e32882
Seo KW, Kwon YK, Kim BH, Kim CI, Chang HS, Choe MS et al (2010) Correlation between claudins expression and prognostic factors in prostate cancer. Korean J Urol 51(4):239–244
Knights AJ, Funnell AP, Crossley M, Pearson RC (2012) Holding tight: cell junctions and cancer spread. Trends Cancer Res 8:61
Capaldo CT, Nusrat A (2015) Claudin switching: physiological plasticity of the tight junction. Semin Cell Dev Biol 42:22–29
Phattarataratip E, Sappayatosok K (2016) Expression of claudin-5, claudin-7 and occludin in oral squamous cell carcinoma and their clinico-pathological significance. J Clin Exp Dent 8:e299–e306
Wöll S, Schlitter AM, Dhaene K, Roller M, Esposito I, Sahin U et al (2014) Claudin 18.2 is a target for IMAB362 antibody in pancreatic neoplasms. Int J Cancer 134(3):731–739
Heinlein CA, Chang C (2004) Androgen receptor in prostate cancer. Endocr Rev 25:276–308
Lai CY, Chen CM, Hsu WH, Hsieh YH, Liu CJ (2017) Overexpression of endothelial cell-specific molecule 1 correlates with Gleason score and expression of androgen receptor in prostate carcinoma. Int J Med Sci 14(12):1263–1267
Navaei AH, Walter BA, Moreno V, Pack SD, Pinto P, Merino MJ (2017) Correlation between ERG fusion protein and androgen receptor expression by immunohistochemistry in prostate, possible role in diagnosis and therapy. J Cancer 8(13):2604–2613
Lekshmy KS, Prema NS (2019) Study of various prognostic factors in prostate cancer and its correlation with androgen receptor expression. J Evol Med Dent Sci 8(34):2687–2693
Kwang HB, Min EH, Yoon YJ, Chung HL, Tae JL, Eon SP et al (2012) Correlation of AR, EGFR, and HER2 expression levels in prostate cancer: immunohistochemical analysis and chromogenic in situ hybridization. Cancer Res Treat 44(1):50–56
Hashmi AA, Mudassir G, Irfan M, Hussain ZF, Hashmi SK, Asif H et al (2019) Prognostic significance of high androgen receptor expression in prostatic acinar adenocarcinoma. Asian Pac J Cancer Prev 20(3):893–896
Hermien H, Cangara H, Miskad UA, Zainuddin AA, Azis A, Achmad D et al (2022) The role of androgen receptor expression in prostate adenocarcinoma. Open Access Maced J Med Sci 10(A):1263–1267
Montgomery RB, Mostaghel EA, Vessella R, Hess DL, Kalhorn TF, Higano CS et al (2008) Maintenance of intratumoral androgens in metastatic prostate cancer: a mechanism for castration-resistant tumor growth. Cancer Res 68:4447–4454
Li R, Wheeler T, Dai H, Frolov A, Thompson T, Ayala G (2004) High level of androgen receptor is associated with aggressive clinicopathologic features and decreased biochemical recurrence-free survival in prostate: cancer patients treated with radical prostatectomy. Am J Surg Pathol 28(7):928–934
Meng J, Mostaghel EA, Vakar-Lopez F, Montgomery B, True L, Nelson PS (2011) Testosterone regulates tight junction proteins and influences prostatic autoimmune responses. Horm Cancer 2:145–156
Ni M, Chen Y, Fei T, Li D, Lim E, Liu XS et al (2013) Amplitude modulation of androgen signaling by c-MYC. Genes Dev 27(7):734–748
Acknowledgements
Not applicable
Funding
We declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to particpate
Approval from research ethics committee (REC) at faculty of medicine Benha university (RC1-8-2023) was obtained before starting the study.
Consent for publication
Not applicable.
Competing interests
We have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rashad, H.M., Ahmed, H., El Attar, K.A. et al. The association of claudin-18 and androgen receptor expression in prostatic carcinoma: an immunohistochemical study. Beni-Suef Univ J Basic Appl Sci 12, 112 (2023). https://doi.org/10.1186/s43088-023-00449-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-023-00449-7