
Abstract
Background
A holding chamber (HC) was created to work with a vibrating mesh nebulizer (VMN) to boost the total inhalable dose for patients. In addition to the optional supply of supplemental oxygen, it facilitates intermittent and continuous nebulization. Our goal was to see how well a VMN coupled to a HC with a mouthpiece or valved facemask performed at varied oxygen flows starting at 0–6 L/min. In this study, we used a breathing simulator to simulate adults' spontaneous breathing patterns with a tidal volume of 500 mL and a 1:1 inhalation–exhalation ratio. For the combination of nebulizer and HC adapter with a valved facemask or mouthpiece, five determinations were made. Salbutamol was recovered and evaluated using high-performance liquid chromatography from the inhalation filter connected to the breathing simulator, the nebulizer reservoir chamber, and the HC.
Results
The amount of salbutamol in the nebulizer reservoir chamber and within the HC did not differ significantly when using a mouthpiece or a valved facemask. However, the supplied dose to the inhalation filter was increased until oxygen flow reached 2 and 3 L/min using the mouthpiece and valved facemask as interfaces, respectively. The supplied salbutamol was much higher at this flow than at the other oxygen flows. This was followed by a progressive reduction in the supplied salbutamol until the lowest given dose was reached at 6 L/min oxygen flow, p < 0.005.
Conclusions
The supplied doses of salbutamol to the inhalation filter were variable with the VMN connected to the HC and mouthpiece or valved facemask, with significant improvements until an oxygen flow of 2 L/min with a mouthpiece and 3 L/min with a valved facemask, followed by gradual decreases to lower values at an oxygen flow of 6 L/min. An in vivo investigation is required to further validate the findings.
Similar content being viewed by others
1 Background
The holding chamber (HC) was created to treat spontaneously breathing individuals with a vibrating mesh nebulizer (VMN) and either a mouthpiece or a valved facemask. A valved facemask has an opening and closing valve, so when the patient inhales the exhalation valve closes and the inlet valve opens to provide oxygen and nebulized aerosol medication. On exhalation, the inlet valve closes and the exhalation valve opens allowing the patient to exhale. This is just a bit clearer to the function of the valved mask. According to Aerogen Limited (Aerogen Ltd, Galway, Ireland), this HC functions as an aerosol reservoir and enables low-flow oxygen (1–6 L/min) connection. It can be utilized for both intermittent and continuous treatments in pediatric and adult patients. The HC connects to the VMN on the one side and a mouthpiece or a valved facemask on the other. The HC's valved mechanism controls aerosol flow to the patient via the aerosol chamber. The supplied oxygen gas and the air are sucked into the device through the inlet valve on the base of the HC, causing it to flow. The aerosol is removed from the chamber, and the medicine is delivered to the patient. During exhale, the inlet valve closes, while the mouthpiece valve opens. The patient can exhale through the valve on the mouthpiece while the VMN refills the aerosol chamber. The design of the device’s valved system controls flow through the aerosol chamber [1].
Ari et al. [2] reported better aerosol delivery with a VMN connected to a HC with an oxygen flow of 2 L/min compared to a jet nebulizer. However, this comparison was made between a VMN and a jet nebulizer, when only VMNs with various interfaces and oxygen flows should have been used. Furthermore, due to the VMN's higher efficiency, independent of setting, the VMN has been found to deliver more aerosol than the jet nebulizer in many studies [3,4,5,6,7,8,9,10,11,12,13].
Sarhan et al. utilized the HC with the VMN to boost aerosol delivery substantially as compared to using a T-piece [1]. They continued their research by adding oxygen at a rate of 6 L/min [14]. Within the HC, introducing oxygen at the maximum recommended flow (6 L/min) resulted in a significant reduction in aerosol distribution [14].
Our goal was to compare the performance of a VMN connected to a HC with different oxygen flows ranging from 0 to 6 L/min, as well as the effect of different interfaces (mouthpiece or facemask) when connected to a HC on the total inhaled mass of delivered nebulized salbutamol.
2 Methods
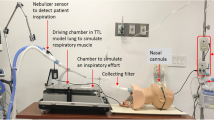
As illustrated in Fig. 1, the Aerogen Solo as a VMN (Aerogen, Galway, Ireland) was connected to the Aerogen Ultra as a HC (Aerogen, Galway, Ireland), coupled with a mouthpiece and valved facemask. In our study, we used the Solo nebulizer because of its label claim for extended use, ready availability, and use in hospital settings; Aerogen also recommended using it with the Ultra holding chamber. At varying flows of 0 to 6 L/min from a cylinder of oxygen, oxygen was delivered through an aperture in the HC at room temperature and humidity settings. The breathing simulator model (5600i, Michigan Instruments, Kentwood, Michigan) was altered to simulate a resting adult breathing pattern in European Standard EN 13544-16, which is at a tidal volume of 500 mL, with an inhalation–exhalation ratio of 1:1. (CEN methodology) [15].

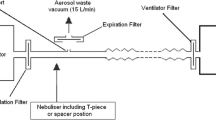
A A schematic diagram of the experimental setup for determining the amount of aerosol released (the total inhalable aerosol dose) and B a picture of the used holding chamber and the vibrating mesh nebulizer setting with the mouthpiece and the valved mask
An electrostatic filter pad encased in a filter holder (PARI, Starnberg, Germany) was coupled to the breathing simulator (inhalation filter) on the one side and the nebulizer–adapter combination on the other, as illustrated in Fig. 1. A plate with a hole in the middle was added to the experimental setup for the valved facemask interface, and the mask was sealed to it as illustrated in Fig. 1. For the determination of the inhalable mass from a nebulizer with a facemask, this plating method was previously found to have no significant differences from the facemask [16, 17]. For each determination, a different filter was used. This filter captured the entire aerosol inhaled during inspiration, allowing for a reliable estimate of the total dose inhaled (i.e., the in vitro emitted dose available for inhalation) [4, 18]. The simulator was activated just before the nebulization of a 1 mL respirable solution containing 5000 µg salbutamol (Farcolin Respirator Solution, Pharco Pharmaceuticals, Egypt).
There were five determinations taken at each oxygen flow and nebulization for dryness for each combination of nebulizer and HC coupled with a valved facemask or mouthpiece. Salbutamol deposited in the nebulizer reservoir chamber and within the HC was recovered by rinsing and sonicating with 20% acetonitrile for 3 min, and salbutamol accumulated on the filter was removed by rinsing and sonicating with 20% acetonitrile for 3 min. Using high-performance liquid chromatography with ultraviolet detection, the quantity of salbutamol was determined [19].
2.1 Statistical analysis
All data are presented as mean ± standard deviation. Using SPSS V15.0, the Kruskal–Wallis test followed by Mann–Whitney was performed to examine the effects of different flows using a mouthpiece and a valved facemask, and a t test analysis was utilized to compare the performances of the valved facemask and the mouthpiece (SPSS, Chicago, Illinois, USA).
3 Results
Table 1 and Figs. 1 and 2 summarize the results of the delivered dose of the VMN and HC connected to the mouthpiece and valved facemask with oxygen at different flows from 0 to 6 L/min expressed as mean ± SD, indicating that the delivered dose to the inhalation filter increased significantly until oxygen flows of 2 L/min and 3 L/min with the mouthpiece and valved facemask as interfaces, respectively (p < 0.05). The delivered salbutamol was much higher at the flows of 2 L/min and 3 L/min than at the other oxygen flows. As shown in Table 1 and Figs. 1 and 2, this result was followed by a gradual decline until the lowest given dose was reached at an oxygen flow of 6 L/min. All of the investigated combinations had no significant differences in the nebulizer residue left within the nebulization chamber. For the amount of salbutamol deposited in the HC, the mouthpiece and the valved facemask had means ± SD of 443.2 ± 244.9 µg and 292.2 ± 245.6 µg, respectively, at flow 0 L/min, which was the highest value with a significant difference from the rest of the oxygen flows (p < 0.005).

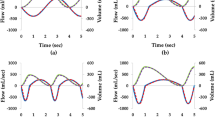
Fate of supplied doses of salbutamol (the inhalation filter, nebulizer residual, and amount deposited in holding chamber in micrograms) at different oxygen flows using a mouthpiece
Table 1 and Figs. 1 and 2 show that there were insignificant differences between the delivered inhalable doses with mouthpiece and valved facemask with oxygen at flows of 0, 1, 2, and 5 L/min (p values = 0.947, 0.94, 0.13, and 0.14, respectively), but significant differences were found at flows of 3, 4, and 6 L/min (p values = 0.001, 0).
4 Discussion
The current study compares the performance of a VMN connected to a HC using a mouthpiece and a valved facemask at various flows ranging from 0 to 6 L/min. The amount of medicine breathed is heavily influenced by the breathing pattern of the patient, the nebulizer, and the interface used for aerosol therapy [2]. We used a HC rather than a T-piece in our investigation since the HC was found to increase the supplied aerosolized dose [1]. The nebulizer is also situated next to the HC, which reduces drug particle deposition due to gravitational sedimentation [1].
Sarhan et al. [14] found that when using a VMN connected to a HC and mouthpiece without oxygen, the delivered dose was significantly higher (p < 0.05) than when using oxygen at a flow of 6 L/min, with values of 2197.7 ± 470.7 µg and 1081.5 ± 333.9 µg, respectively. Similar findings were obtained when using a valved facemask and mouthpiece; however, there was an additional effect when using varied oxygen flows. By increasing the supplied inhalable dose until flow was 2 L/min while using the mouthpiece and 3 L/min when using the valved facemask, we discovered that the flow of oxygen had a significant effect on the delivered dose. Following that, as the oxygen flow increased, the given inhalable dose gradually reduced until it reached its lowest value (1814.5 ± 162.3, and 2128.1 ± 243.1 for mouthpiece and facemask, respectively) when the oxygen flow rate was the maximum (6 L/min) that we investigated (Fig. 3).

Fate of supplied doses of salbutamol (the inhalation filter, nebulizer residual, and amount deposited in holding chamber in micrograms at different oxygen flows using a valved facemask
Bennett et al. [20] used a VMN linked to a HC with a mouthpiece and valved facemask to quantify the delivered dose using humidified air instead of oxygen at flows of 0, 2, and 6 L/min. The largest inhalable dose was found at flows of 2 L/min for both the mouthpiece and the valved facemask. However, they did not measure the oxygen flows of 1, 3, 4, and 5. Even without these four oxygen flows, their results were comparable to ours. Even though Bennett G and his colleagues [20] used Albuterol 2 mg/ml in much smaller doses, which is different from using salbutamol 5000 µg/ml in the work presented here, this would affect the comparison of the two studies. However, the benefit of the use of the VMN in the study, which allows the nebulization of almost all the nebulized solutions placed in the nebulization chamber overcome, is different [3,4,5,6,7,8,9,10,11,12,13].
Another study tested three oxygen flows (2, 4, and 6 L/min), finding that the oxygen flow of 4 L/min produced the largest inhalable dose [21]. Despite the fact that the flow found differs from ours, this investigation backs up our findings. The only difference was that they discovered a higher oxygen flow than we did. That could be due to their use of a higher tidal volume (750 mL), which is 250 mL higher than the normal tidal volume used in most in vitro studies (500 mL) but more realistic for some adult patients [22,23,24,25,26,27,28,29,30,31,32,33], as well as their use of a valved facemask only, for which we found the best oxygen flow was 3 L/min [21], implying that the higher tidal flow improved the benefit of oxygen delivered as a supplement to the aerosol within the HC.
During the exhale phase, higher oxygen flows may flush the aerosol out of the HC. The aerosol collects in the HC when there is no oxygen flow or when the flow is low and is available to the subjects on inspiration. This HC has a volume of 130 mL. The flow of 6 L/min is equivalent to 100 mL/s. Our breathing simulator was calibrated to a 500-mL tidal volume, and a 1:1 inhalation–exhalation ratio. As a result, most of the saved aerosol in the HC during exhalation would be flushed out before intake with the 2 s expiration, which is equivalent to 200 mL of oxygen. As a result, the higher the oxygen flow rate, the smaller the amount of aerosol retained by the HC between breaths. In light of this discovery, researchers compared inhaled doses across different tidal volumes and flow to see how the inhalable dose correlated. When comparing the results shown here and in Brady et al. study, the effect of tidal volume on delivered aerosol was obvious because they used different tidal volumes, with the best aerosol delivery at 3 L/min in our study using a tidal volume of 500 mL and 4 L/min in Brady et al. study using a tidal volume of 750 mL [21]. The effect of varied oxygen flows is visible in our results, but those in vivo investigations are needed to confirm the findings.
Furthermore, according to our findings, the given dose using oxygen with a valved facemask was much higher than using a mouthpiece. These findings could be related to the valved facemask's large volume of air space for aerosol retention during exhalation compared to the mouthpiece, which allows for less waste of aerosol by the oxygen flow during the exhalation phase of the respiration cycle.
The maximum deposition was reported with no oxygen flow, indicating that not much aerosol remained within the chamber while oxygen was flowing as supplemental to aerosol within the HC, supporting the theory of aerosol flushing by oxygen flow.
4.1 Limitations
A major limitation of the study was that it was in vitro, which limits the clinical relevance of the findings, so we suggest extending this work to clinical studies. Note that oxygen flow is selected for best oxygenation and not for best aerosol delivery. One should never compromise oxygenation to improve aerosol delivery. This methodology was intended to assess product quality and not to evaluate likely performance in patients with varying degrees of lung disease affecting their ability to breathe. Furthermore, the I/E ratio is too short, as values closer to 1:2 are more common, and the expiratory portion may be lengthened with therapy for severe COPD. We use the plate-setting methodology. This might not provide any information about the effect of applying force to the facemask to affect a seal on the face that could have a marked influence on medication transfer to the patient. This study was done using an adult breathing model, and future studies should evaluate the findings as they apply to pediatrics.
5 Conclusion
The effect of different oxygen flows within the HC connected to the VMN and mouthpiece or valved facemask on supplied doses of salbutamol to the inhalation filter was significantly improved until oxygen flows of 2 L/min with mouthpiece and 3 L/min with valved facemask, followed by gradual decreases to lower values at an oxygen flow of 6 L/min. An in vivo investigation is required to further validate the findings.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- HC:
-
Holding chamber
- VMN:
-
Vibrating mesh nebulizer
References
Sarhan RM, Elberry AA, Abdelwahab NS et al (2018) Effect of a nebulizer holding chamber on aerosol delivery. Respir Care 63(9):1125–1131
Ari A, de Andrade AD, Sheard M et al (2015) Performance comparisons of jet and mesh nebulizers using different interfaces in simulated spontaneously breathing adults and children. J Aerosol Med Pulm Drug Deliv 28(4):281–289
Abdelrahim ME, Chrystyn H (2009) Aerodynamic characteristics of nebulized terbutaline sulphate using the next generation impactor (NGI) and CEN method. J Aerosol Med Pulm Drug Deliv 22(1):19–28
Hassan A, Rabea H, Hussein RR et al (2016) In-vitro characterization of the aerosolized dose during non-invasive automatic continuous positive airway pressure ventilation. Pulm Ther 2:115–126
Muhammad HE, ElHansy MEB, Farid H, Chrystyn H, Maraghi SKE, Al-Kholy MB, El-Essawy AFM, Abdelrahman MM, Said ASA, Hussein RRS, Rabea H, Abdelrahim MEA (2016) In-vitro aerodynamic characteristics of aerosol delivered from different inhalation methods in mechanical ventilation. Pharm Dev Technol 22(6):844–849
ElHansy MH, Boules ME, El Essawy AFM et al (2017) Inhaled salbutamol dose delivered by jet nebulizer, vibrating mesh nebulizer and metered dose inhaler with spacer during invasive mechanical ventilation. Pulm Pharmacol Ther 45:159–163
ElHansy MHE, Boules ME, Farid H et al (2017) In vitro aerodynamic characteristics of aerosol delivered from different inhalation methods in mechanical ventilation. Pharm Dev Technol 22(6):844–849
Hassan A, Salah Eldin R, Abdelrahman MM et al (2017) In-vitro/in-vivo comparison of inhaled salbutamol dose delivered by jet nebulizer, vibrating mesh nebulizer and metered dose inhaler with spacer during non-invasive ventilation. Exp Lung Res 43(1):19–28
Madney YM, Fathy M, Elberry AA et al (2017) Nebulizers and spacers for aerosol delivery through adult nasal cannula at low oxygen flow rate: an in-vitro study. J Drug Deliv Sci Technol 39:260–265
Moustafa IO, Ali MR-A, Al Hallag M et al (2017) Lung deposition and systemic bioavailability of different aerosol devices with and without humidification in mechanically ventilated patients. Heart Lung 46(6):464–467
Moustafa IO, ElHansy MH, Al Hallag M et al (2017) Clinical outcome associated with the use of different inhalation method with and without humidification in asthmatic mechanically ventilated patients. Pulm Pharmacol Ther 45:40–46
Rabea H, Ali AM, Eldin RS et al (2017) Modelling of in-vitro and in-vivo performance of aerosol emitted from different vibrating mesh nebulisers in non-invasive ventilation circuit. Eur J Pharm Sci 97:182–191
Saeed H, Mohsen M, Fink JB et al (2017) Fill volume, humidification and heat effects on aerosol delivery and fugitive emissions during noninvasive ventilation. J Drug Deliv Sci Technol 39:372–378
Sarhan RM, Elberry AA, Abdelwahab NS et al (2019) Effect of oxygen flow on aerosol delivery from a nebulizer with a holding chamber. Respir Care 64(12):1508–1515
de Normalisation CE (2001) Respiratory therapy equipment—Part 1: nebulizing systems and their components. CEN Brussels: 13544-1
Nikander K, Berg E, Smaldone GC (2007) Jet nebulizers versus pressurized metered dose inhalers with valved holding chambers: effects of the facemask on aerosol delivery. J Aerosol Med 20(s1):S46–S58
Vecellio L, Abdelrahim ME, Montharu J et al (2011) Disposable versus reusable jet nebulizers for cystic fibrosis treatment with tobramycin. J Cyst Fibros 10(2):86–92
Abdelrahim ME (2011) Aerodynamic characteristics of nebulized terbutaline sulphate using the Andersen Cascade Impactor compared to the Next Generation Impactor. Pharm Dev Technol 16(2):137–145
Abdelrahman MM (2018) Solid-phase extraction and HPLC-DAD for determination of salbutamol in urine samples. Anal Chem Lett 8(1):35–45
Bennett G, Joyce M, Fernández EF et al (2019) Comparison of aerosol delivery across combinations of drug delivery interfaces with and without concurrent high-flow nasal therapy. Intensive Care Med Exp 7(1):1–11
Brady P, Mhurchú SN, McKenna C et al (2018) Effect of supplemental oxygen flow rate on aerosol delivery during spontaneous breathing. In: Irish Journal of Medical Science. Springer, London
Boules ME, Laz NI, Elberry AA et al (2022) Effect of pressures and type of ventilation on aerosol delivery to chronic obstructive pulmonary disease patients. Beni-Suef Univ J Basic Appl Sci 11(1):57
Madney YM, Harb HS, Porée T et al (2022) Preliminary bronchodilator dose effect on aerosol-delivery through different nebulizers in noninvasively ventilated COPD patients. Exp Lung Res 48(2):77–85
Rashad AE, Mohammad MF, Eckes M et al (2021) Performance of different add-on devices in dual limb non-invasive mechanically ventilated circuit. J Drug Deliv Sci Technol 66:102897
Boules ME, Laz NI, Elberry AA et al (2021) Aerosol delivery through high flow nasal cannula compared to biphasic positive airway pressure, at two different pressure: an in-vitro study. Beni-Suef Univ J Basic Appl Sci 10(1):81
Seif SM, Ma E, Rabea H et al (2021) Aerosol delivery of inhalation devices with different add-on connections to invasively ventilated COPD subjects: an in-vivo study. Eur J Pharm Sci 167:105988
Madney YM, Laz NI, Elberry AA et al (2021) Aerosol delivery aspects within a high-flow therapy system in COPD patients. ERJ Open Res 7(1):00422–02020
Saeed H, Harb HS, Madney YM et al (2020) Aerosol delivery via noninvasive ventilation: role of models and bioanalysis. Ann Transl Med 9(7):589
Madney YM, Laz NI, Elberry AA et al (2020) Aerosol delivery aspects within a high flow therapy system in chronic obstructive pulmonary disease patients. ERJ Open Research: 00422-2020.
Seif SM, Elnady MA, Rabea H et al (2020) Effect of different connection adapters on aerosol delivery in invasive ventilation setting; an in-vitro study. J Drug Deliv Sci Technol 66:102177
Madney YM, Ibrahim Laz N, Elberry AA et al (2021) The impact of changing patient interfaces on delivering aerosol with titrated oxygen in the high flow system. Int J Clin Pract 74(4):e13898
Saeed H, Rabea H, Abdelwahab NS et al (2020) Effects of nebulizer fill volume on the efficacy and safety of the bronchodilator. J Drug Deliv Sci Technol 66:101508
Harb HS, Elberry AA, Rabea H et al (2018) Performance of large spacer versus nebulizer T-piece in single-limb noninvasive ventilation. Respir Care 63(11):1360–1369
Acknowledgements
Not applicable.
Funding
There was no external funding for this study itself. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Author information
Authors and Affiliations
Contributions
MA contributed to conception and design. All authors contributed to administrative support, provision of study materials, and final approval of the manuscript. ME contributed to collection and assembly of data, data analysis and interpretation, and manuscript writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised to present affiliation 3 correctly.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Amin, M.A., Taha, H.K., Hussein, R.R.S. et al. Effect of oxygen flow on aerosol delivery from a vibrating mesh nebulizer with a holding chamber. Beni-Suef Univ J Basic Appl Sci 11, 154 (2022). https://doi.org/10.1186/s43088-022-00338-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43088-022-00338-5