
Abstract
Background and objective
The diagnosis and treatment of benign tumors of the gallbladder and bile ducts are difficult due to their anatomical relationships with neighboring vital organs. Hemangiomas are non-epithelial benign tumors of the gallbladder. The gallbladder is an extremely rare localization for cavernous hemangiomas. To date, 7 cases of cavernous gallbladder hemangioma have been reported in the literature. Although it is seen very rarely, the main problem is that it mimics malignant lesions. Pre-operative diagnosis of gallbladder hemangiomas is difficult. Ultrasound (US), computed tomography (CT) magnetic resonance imaging(MRI), endoscopic ultrasound (EUS), and angiography are helpful in differential diagnosis.
Here, we aimed to present our case, which is the first case of cavernous gallbladder hemangioma and obstructive jaundice in the literature.
Case presentation
A 49-year-old female patient was admitted with the complaint of pain in the right upper quadrant of her abdomen. Bilirubin levels were high due to obstructive jaundice. Abdominal CT and MRI showed an appearance in favor of hemangioma in the gallbladder. There was an increase in bile duct wall thickness on MRCP, and it was evaluated as suspicious for malignant neoplasia. The patient was operated on, and extrahepatic bile duct resection + Roux-en-Y hepaticojejunostomy procedure was performed. As a result of histopathology, hemangioma was detected in the gallbladder. There was no malignancy in the bile ducts.
Conclusion
It should be kept in mind that the mass detected in the gallbladder in a patient with jaundice who is suspected of having a bile duct tumor may also be a hemangioma.
Similar content being viewed by others


Introduction
Diagnosis and treatment of benign tumors of the gallbladder and bile ducts reveal difficulties due to their anatomical relations with neighboring vital organs. Benign gallbladder tumors can mimic neoplasms developing in this area. Thus, it is important to know the characteristics of benign gallbladder lesions for differential diagnosis and treatment [1, 2]. Since hemangioma of the gallbladder is very rare, a rate related to its incidence has not been determined in the literature. Seven cases have been reported in the literature so far.
Here, a case of hemangioma of the gallbladder fundus, together with the obstructive jaundice clinical picture, which is an extremely rare association is presented.
Case
Patient information
A 49-year-old female patient, who was admitted to the emergency department with complaints of obstructive jaundice and intermittent abdominal pain for 4 months. The hypertensive patient had no previous operation history.
Clinical findings
Physical examination revealed tenderness in the right upper quadrant and epigastric region. The patient’s sclera was icteric. There was a 5% weight loss in the last 6 months.
Lab tests
Her liver function tests were high (total bilirubin 7.85, direct bilirubin 5.05, ALP 350). CA 19–9 levels were at the upper limit of normal and within the range of reference values.
Imaging studies
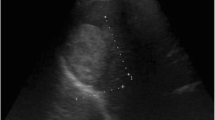
In the abdominal US, a mass with a diameter of 50 × 30 mm was observed in the gallbladder fundus. There were no pathological findings on the patient’s chest CT. Subsequently, the mass with the size of 52 × 30 mm showing lateral extension on IV contrast-enhanced abdominal CT and MRI were evaluated in favor of gallbladder hemangioma (Fig. 1). MRCP showed dilatation in the intrahepatic bile ducts up to the hilus level, wall thickening, and focal diffusion restriction in the segment less than 1 cm at the common duct level were evaluated as suspicious for malignant neoplasia.

Abdominal CT axial (A) and abdominal MR coronal (B) sections
Surgical intervention
The patient was operated with the pre-diagnosis of Klatskin tumor + gallbladder hemangioma. Extrahepatic biliary tract resection + Roux-en-Y hepaticojejunostomy procedure was performed.
Postoperative results
Gross pathology showed a well-defined cystic mass inseparable from the gallbladder fundus, 5 × 3 cm in size (Fig. 2). Microscopically, the tumor comprised of closely aggregated vessels lined by a single layer of flattened epithelium with no atypia. Immunohistochemically, the epithelium was positive for CD31 and CD34 and negative for cytokeratin (AE1/AE3), which favored the diagnosis of gallbladder hemangioma (Fig. 2). The extrahepatic biliary duct wall showed mild fibrosis and chronic inflammation, and there was no atypia in the epithelium, which were all against the suspicion of Klatskin tumor. The patient was discharged on the fifth postoperative day and has been followed up for 4 months without any problem.

Surgery picture of the gallbladder hemangioma (A). The picture of the specimen (B, C). Hemangioma located in the serosal aspect of gallbladder wall, hematoxylin–eosin × 2 (D)
Discussion
The majority (88%) of gall bladder tumors are benign lesions. Most of them are adenomyomatosis, cholesterol polyps, and inflammatory polyps. Adenomymatosis is most commonly located in the fundus and may be confused with malignant lesions of the gallbladder [2, 3].
Cavernous hemangiomas are most detected in the skin and liver. They constitute 73% of benign liver tumors. It is observed with a frequency of 0.4–7.3% in autopsy series [4]. Hemangiomas are non-epithelial benign tumors of the gallbladder [1]. The gallbladder is an extremely rare localization for cavernous hemangiomas. There is very little data in the literature regarding gallbladder hemangiomas. To date, 7 cases of cavernous gallbladder hemangioma have been reported in the literature. Although it is rare, the most critical problem is that it can be confused with malignant lesions. Differential diagnosis is vital in this regard. Gallbladder polyps can also become involved in diseases such as gallbladder tumors and xanthogranulomatous cholecystitis by thickening the gallbladder wall [3].
Histopathologically, hemangiomas are divided into 3 subtypes: capillary, cavernous, and arteriovenous. Within this classification, cavernous hemangiomas are aggressively growing tumors that do not tend to regress. Although they are benign, they may cause compression symptoms and rarely mortal hemorrhage, depending on their size [5].
Benign gallbladder lesions are usually asymptomatic. Although the cavernous hemangioma of our case originating from the gallbladder fundus reached 5 × 4 cm in size, there was no compression symptoms. Nevertheless, they may become symptomatic, depending on the size and location of the lesion. They may also present with acute biliary colic, epigastric pain, jaundice, and fever. They show similar symptoms to cholecystitis, choledocholithiasis, and gallbladder tumors and may be confused preoperatively with these diseases. A case of gallbladder hemangioma that was operated with the pre-diagnosis of a giant mesenteric cyst has been reported in the literature [6].
US is the first-line imaging technique of choice in the evaluation of gallbladder lesions. Considering its rapid rise in clinical practice, CT has also become the mainstay in evaluating the gallbladder diseases. At the same time, MRI and EUS are also generally accepted as a problem-solving tool [7]. Despite the advances in endoscopic transpapillary biliary drainage, endoscopic biliary drainage, and cytology studies, there is no ideal radiological diagnostic method to distinguish benign and malignant lesions of the gallbladder. Angiography can also be used for differential diagnosis [8].
We found that the cases of cavernous gallbladder hemangioma reported in the literature were operated with the pre-diagnoses of gallbladder carcinoma, mesenteric cyst, cholecystitis, and hepatic angioma [5, 9]. No pre-operative correct diagnosis was made in any of these cases.
In our case, pre-diagnosis of gallbladder hemangioma was made during the abdominal CT and MRI examinations performed while investigating the etiology of jaundice, our hemangioma diagnosis was confirmed with laparotomy and postoperative histopathological examination. None of the gallbladder capillary hemangioma cases reported in the literature had gallstones. The patients most frequently applied with complaints of pain. Four patients had accompanying angiomatous changes such as vocal cord hemangioma, liver hemangioma, and intestinal hemangioma. Cholecystectomy or extended cholecystectomy operation was performed on all gallbladder hemangioma patients [5, 9]. In our patient, cholecystectomy and extrahepatic resection of the bile ducts were performed due to the presence of wall thickening, diffusion restriction, and malignancy suspicion in the common hepatic canal on MRI.
Conclusion
Gallbladder hemangioma is a rare entity, and USG, CT, MRI, EUS, and angiography are helpful in the diagnosis. Laparoscopic cholecystectomy should be the first option in cases if there is only hemangioma. The gallbladder should be removed in the endobag. If there is a risk of bleeding, suspicion of malignancy, or inability to reveal the anatomy, surgical exploration with laparotomy should be performed. It should be kept in mind that gallbladder hemangioma may be associated with obstructive jaundice as in our case.
References
Levy AD, Murakata LA, Abbott RM et al (2002) From the archives of the AFIP. Benign tumors and tumorlike lesions of the gallbladder and extrahepatic bile ducts: radiologic-pathologic correlation. Armed Forces Institute of Pathology. Radiographics. 22(2):387–413
Kwon W, Jang JY, Lee SE et al (2009) Clinicopathologic features of polypoid lesions of the gallbladder and risk factors of gallbladder cancer. J Korean Med Sci 24(3):481–487
Dilek ON, Karasu S, Dilek FH (2019) Diagnosis and treatment of gallbladder polyps: current perspectives. Euroasian J Hepatogastroenterol 9(1):40–48
Toro A, Mahfouz AE, Ardiri A et al (2014) What is changing in indications and treatment of hepatic hemangiomas. A review. Ann Hepatol 13(4):327–339
Crucitti A, La Greca A, Antinori A et al (2005) Cavernous hemangioma of the gallbladder. Case report and review of the literature. Tumori 91(5):432–435
Mayorga M, Hernando M, Val-Bernal JF (1997) Diffuse expansive cavernous hemangioma of the gallbladder. Gen Diagn Pathol 142(3–4):211–215
Catalano OA, Sahani DV, Kalva SP et al (2008) MR imaging of the gallbladder: a pictorial essay. Radiographics 28(1):135–324
Patkar S, Shinde RS, Kurunkar SR et al (2017) Radiological diagnosis alone risks overtreatment of benign disease in suspected gallbladder cancer: a word of caution in an era of radical surgery. Indian J Cancer 54(4):681–684
Funamizu N, Nakabayashi Y (2019) Cavernous hemangioma of the gallbladder masquerading as a carcinoma. Case Rep Gastroenterol 13(1):219–224
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
F. Karahan: Concept, design and writing. A. Atay: Acquisition of data. N. Ekinci: Critical revision for important intellectual content. O. N. Dilek: Drafting of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Karahan, F., Atay, A., Ekinci, N. et al. A case of gallbladder hemangioma detected in a patient with jaundice and suspected Klatskin tumor: case report and review of the literature. Egypt Liver Journal 14, 48 (2024). https://doi.org/10.1186/s43066-024-00356-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-024-00356-1