
Abstract
Background
Scaling evidence-based interventions are key to impacting population health. The National DPP lifestyle change program is one such intervention that has been scaled across the USA over the past 20 years; however, enrollment is an ongoing challenge. Furthermore, little is known about which organizations are most successful with program delivery, enrollment, and scaling. This study aims to understand more about the internal and external organization factors that impact program implementation and reach.
Methods
Between August 2020 and January 2021, data were collected through semi-structured key informant interviews with 30 National DPP delivery organization implementers. This study uses a qualitative cross-case construct rating methodology to assess which Consolidated Framework for Implementation Research (CFIR) inner and outer setting constructs contributed (both in valence and magnitude) to the organization’s current level of implementation reach (measured by average participant enrollment per year). A construct by case matrix was created with ratings for each CFIR construct by interviewee and grouped by implementation reach level.
Results
Across the 16 inner and outer setting constructs and subconstructs, the interviewees with greater enrollment per year provided stronger and more positive examples related to implementation and enrollment of the program, while the lower reach groups reported stronger and more negative examples across rated constructs. Four inner setting constructs/subconstructs (structural characteristics, compatibility, goals and feedback, and leadership engagement) were identified as “distinguishing” between enrollment reach levels based on the difference between groups by average rating, the examination of the number of extreme ratings within levels, and the thematic analysis of the content discussed. Within these constructs, factors such as organization size and administrative processes; program fit with existing organization services and programs; the presence of enrollment goals; and active leadership involvement in implementation were identified as influencing program reach.
Conclusions
Our study identified a number of influential CFIR constructs and their impact on National DPP implementation reach. These findings can be leveraged to improve efforts in recruiting and assisting delivery organizations to increase the reach and scale of the National DPP as well as other evidence-based interventions.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
According to 2020 data, the Centers for Disease Control and Prevention (CDC) has reported that 96 million adults (38% of the adult population) in the USA have prediabetes, a condition that indicates a high risk, and progression to, type 2 diabetes [1]. The National DPP lifestyle change program is an evidence-based, year-long intervention with 22 sessions led by lifestyle coaches designed to prevent the progression to diabetes in people with prediabetes [2,3,4]. Since its inception in 2010 the National DPP has made great strides in raising awareness for and accessibility to its evidence-based lifestyle change program for people with prediabetes including establishing the program as a covered benefit for Medicare and Medicaid beneficiaries [3, 5]. However, program reach, the number or proportion of individuals participating in program, is lower than hoped. Approximately 2000 organizations of various types, sizes, and settings currently deliver the program across all 50 states and US territories [6, 7], but in 2017, the CDC reported that only 0.04% of the US adults with prediabetes had been reached in the first 4 years of the National DPP implementation [8, 9]. When efficacious programs (like the National DPP) can reach a large number of individuals, population impact occurs [10,11,12,13]. However, while organizations are adopting the program and expanding financial coverage for participants, enrollment or reach remains a challenge and a key focus for stakeholders [14,15,16].
Understanding factors related to adoption, implementation, and reach of the National DPP at the organizational level is critical to scaling the program. To date, research and evaluation of the National DPP has largely focused on participant-level outcomes [5, 8, 17]. These show the vast majority of participants are female (around 80%), 45 years or older, and with a prediabetes status determined by blood-based test [8, 18]. Other research about the National DPP have posited reasons for enrollment challenges including a lack of awareness in the prediabetes population of their diagnosis and/or the program, poor and underutilized referral systems, and challenges with setting up program reimbursement as possible barriers to enrollment [14,15,16, 19]. Organization-level evaluations have explored specific implementation strategies (referrals, partner networks, adaptation of materials, etc.) and have shown that use of incentives and healthcare provider-based referrals are promising practices to increase enrollment and participation [17, 20]. However, these studies focus on limited organizational characteristics, such as type and location (e.g., state), in their analyses.
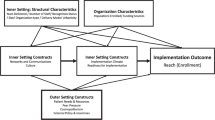
In addition to intervention characteristics and program participants, other critical contextual factors internal and external to organizations may impact implementation outcomes. Chaudoir, Dugan, and Barr refer to these as organization (internal) and structural (external) level causal factors in their “Multi-Level Framework Predicting Implementation Outcomes” [21]. Furthermore, an understanding of organization characteristics (type, size, location, etc.) and factors within and surrounding an organization that influence the delivery of programs may be useful in developing strategies for recruiting new organizations and supporting current delivery. Thus, there is a need for an in-depth and rigorous examination of internal and external organization factors and the ways they impact the implementation success of the National DPP.
This study aims to fill this gap by applying the Consolidated Framework for Implementation Research (CFIR), a metatheory comprised of constructs associated with implementation, that has been increasingly utilized in public health research to understand diverse aspects of implementation processes and outcomes [22,23,24]. Within diabetes prevention and management, researchers most commonly have used CFIR to examine facilitators and barriers to program implementation [25,26,27]. For example, Wilcox et al. (2020) used CFIR to identify predictive constructs with implementation outcomes for a cultural adaptation of the National DPP for African-American Churches in the South [28]. To our knowledge, CFIR has not been used to examine inner and outer setting factors related to enrollment and implementation in the National DPP across organizations.
Two of the five domains, the inner setting and outer setting, focus on internal and external organization factors [23]. The CFIR constructs listed in the inner setting domain aim to capture the complexity within the organization related to implementation (e.g., structural characteristics, culture, and readiness for implementation). The outer setting constructs provide insight into the greater environments and external context which constrain organizations or facilitate their ability to carry out the intervention (e.g., cosmopolitanism, peer pressure, and external policies and incentives).
To contribute to the current knowledge of the National DPP, this study will explore factors related to the internal and external organization (operationalized through the CFIR inner and outer setting constructs) to understand relationships between these constructs and program implementation and enrollment (reach). Insights gained can inform strategies to expand the capacity of delivery organizations to increase engagement in the program and scale the program up and out nationally [5, 15, 16].
Methods
In 2019, Emory Center’s Diabetes Technical Assistance and Training Center (DTTAC) was funded to study the role of Lifestyle Coaches in the implementation of the National DPP through the CDC’s Division of Diabetes Translation’s Innovations to Grow Enrollment and Retention (InGEAR) project. Over the last 10 years, DTTAC has directly trained over 5000 lifestyle coaches representing over 2000 organizations across all 50 states. The National DPP implementers included in this study participated in Emory’s DTTAC Lifestyle Coach and/or Master Trainer Select training programs and/or subscribed to the center’s resources.
This study uses a qualitative cross-case construct rating methodology to assess which CFIR constructs contributed both in valence (positive or negative influence) and magnitude (combined influence) to the organization’s current level of implementation reach (measured by average participant enrollment per year). Between August 2020 and January 2021, data were collected through semi-structured key informant interviews with 30 National DPP delivery organization implementers (see sampling for selection criteria and procedures). This study was reviewed and determined to be exempt by the Emory University Institutional Review Board (STUDY00000658).
Sampling
DTTAC provided a list of National DPP implementers (n = 239) and their basic organization characteristics (organization type, location, level of implementation, etc.) that were generated from a call for study participation via the DTTAC mailing list and newsletter. Potential participants were stratified into groups of higher (> 85 program participants), medium (26–85 program participants), and lower (≤ 25 program participants) reach organizations based on total enrollment to date. Participant enrollment data from the CDC and DTTAC’s records were used to create the higher, medium, and lower tertile ranges.
We purposively selected participants to reflect the diversity of implementers by organization type, length of program delivery, urbanicity, populations served, and size (Table 2). Due to variations in these organization characteristics, we planned to interview at least 30 participants. Thirty-nine National DPP implementers across the three organization implementation levels were selected; nine either did not respond to the invitation or declined to participate. The final sample included 30 National DPP organization key informants located in 24 states and territories. During the analysis, we found that after conducting the 30 interviews we had reached saturation or the point at which no new information relating to the CFIR constructs was identified in each of the groups. Organization staff reported a range of 5 to 600 enrolled participants to date. In the analysis, to control for length of delivery, enrollment numbers were divided by years of delivery to produce the average enrollment per year for each organization. The interviewees were re-stratified by enrolled participants per year into high (36–150), medium (17–35), and low (5–16) reach levels (Table 2).
Instruments
We developed a semi-structured interview guide with questions adapted from the CFIR guide (CFIR Research Team) and studies using similar methods [29, 30]. Open-ended question topics included interviewee training and background, program implementation success in terms of reach and sustainability, and 16 questions with suggested probes for each of the inner and outer setting CFIR constructs and sub-constructs (see Additional Table 1 for interview guide). Questions were posed in a way to encourage discussion about how each construct or subconstruct has positively or negatively impacted program implementation, particularly related to the outcome of reach (enrollment numbers). For example, the culture construct question asked, “In what ways do you think your organization's culture (general beliefs, values, assumptions that people embrace) affect the implementation of the National DPP?” The probe following asked, “How does the organization’s culture impact enrollment of participants in particular?” The interview guide was reviewed by National DPP subject matter experts and pre-tested.
Data collection
Interviewees were invited to participate in a 60-min interview using Emory’s secure Zoom videoconferencing account; verbal consent and permission to audio-record were obtained prior to initiating the interview. Interviews were conducted from August 2020 to January 2021. All recordings were transcribed by a third party, quality-checked, deidentified, and uploaded into MAXQDA 2020 [31] for coding and analysis.
Interviewee descriptive statistics
Interviewee organizations were categorized into one of five organization types: healthcare/hospitals, community-based healthcare (community health centers, federally qualified health centers, Indian Health Service, etc.) community-based organizations (YMCAs, local nonprofits, etc.), government agencies (state/local health departments), and other (health plans, insurers, worksite wellness programs, universities, private businesses). Descriptive statistics were run on organization characteristics including years delivering the National DPP, size based on the approximate number of people served across the entire organization annually, CDC Diabetes Prevention Recognition Program (DPRP) statusFootnote 1 for the National DPP (Full vs Pending/Preliminary status), location of the organization by US region, and race/ethnicity of the National DPP participant population at the organization (Table 2).
Coding interviews
A deductive codebook of CFIR constructs and interview questions was developed; in vivo (inductive) codes were added as relevant topics were identified during initial coding. The codebook was tested for clarity and relevancy and refined prior to coding. Coders (LM and OM) independently coded each transcript and conducted intercoder agreement, discussing and reaching consensus where there were discrepancies in coding. Double coding and intercoder agreement was performed on one third of the transcripts (n = 10) to ensure intercoder reliability [32, 33].
Construct rating
We used a qualitative construct rating analysis approach from Damschroder and Lowery (2013) to rate CFIR constructs related to implementation outcomes [30]. Applying this methodology, we identified distinguishing constructs among organizations with different levels of implementation reach and identified themes within those constructs that contribute to those differences.
Coded segments for each CFIR construct were exported, sorted by organization, grouped by implementation reach level, and reviewed independently by both analysts (LM and OM). All segments were assessed by construct for valence (positive or negative influence on implementation) using construct rating criteria (Table 1). Segments were scored with a − 2 to + 2, a 5-point bi-polar scale; where there was more than one segment for an interview, the analysts discussed each segment and assigned an average score. Interviews that had positive statements about a construct’s influence on implementation were scored with a 1 or 2 depending on the level of detail and impact on enrollment. Likewise, interviews with negative examples were scored with a − 1 or − 2. An equal mix of positive and negative influences received a score of zero.
Coders met weekly to discuss ratings and consensual validation was achieved through a process of deliberation and consensus. Since our sample had only one interviewee per organization, we adapted Damschroder and Lowery’s methods to remove the synthesis of findings among multiple interviewees at the organization level. Once all transcripts were rated across all 16 CFIR constructs and subconstructs (a case-oriented approach, because ratings were applied within each case), both coders examined them across cases by construct (the variable-oriented approach, since each construct is compared across cases).
Analysis and Interpretation
A construct by case matrix was created that listed the ratings for each CFIR construct by interviewee and grouped by implementation reach level (Fig. 1). This stage of the analysis focused on discerning patterns across the high, medium, and low implementation reach groups. Average rating scores were calculated for each construct by reach level to identify patterns. Interviewees within each reach level were also sorted by organization type and given a summative average rating across all of the constructs to more easily identify rating differences.

Construct rating matrix
Positive and negative extremes were discussed across all constructs and interviewees at every level. Constructs/subconstructs were identified as distinguishing based on the difference between groups by average rating (generally if the difference was over ± 0.5 between levels), the examination of the number of extreme (+ 2 or − 2) ratings within levels, and through thematic analysis based on the content discussed.
Results
Organization characteristics
Program staff from 30 unique implementing organizations were interviewed. CDC-recognized National DPP organizations designate Program Coordinators who supervise daily operations of the program, provide guidance and support to lifestyle coaches, and monitor and submit all program data to the CDC. Of these, all but one were Program Coordinators and 26 served in a combination of roles as Program Coordinators, Lifestyle Coaches, and/or Master Trainers for the National DPP.
About one third (9) of interviewees were from healthcare or hospital settings, followed by a near equal number from community-based healthcare (5, 17%), and other types of organizations (6, 20%) (Table 2). The majority of organizations were in the initial (13, 43%) or intermediate (13, 43%) phases of delivery and held Pending/Preliminary CDC DPRP status (20, 67%). There was consistent representation across the organization size categories and geographic regions. The vast majority have National DPP participants from White (80%), Black (70%), and Hispanic/Latino (63%) racial and ethnic backgrounds. Fewer organizations reported serving Alaska Native/Native American (27%) and Asian/Pacific Islander (27%) participants in their programs.
Representation across levels of implementation reach by organization type was also fairly consistent. In terms of years delivering the program, those in the higher reach group had delivered the program for the longest number of years, while the medium and lower reach groups included many organizations in the initial delivery phase (0–2 years). The higher reach group also tended to include those from larger organizations and more often with full DPRP recognition status.
CFIR construct findings
The construct rating matrix provides the CFIR ratings for each inner and outer setting construct by organization interviewee grouped by implementation reach level (Fig. 1). Overall, the majority of interviewees were net positive in terms of their implementation examples across all of the constructs (Fig. 1 interviewee average score). However, the interviewees in the higher reach group provided stronger (+ 2) and more instances of positive examples across all constructs related to implementation and enrollment, while the low reach group stronger (− 2) and more instances of negative examples across all rated constructs. Four constructs/subconstructs (incentives and rewards, learning climate, access to knowledge and information, and patient needs and resources) were not discussed in relation to implementation reach sufficiently in the interviews to conduct the construct rating and were omitted from the matrix. The following four inner setting constructs/subconstructs were identified as distinguishing: structural characteristics, compatibility, goals and feedback, and leadership engagement. No outer setting constructs were distinguishing. The following results will highlight these constructs with a discussion of the thematic analysis of the coded segments and supporting quotes.
The structural characteristics
The structural characteristics construct is comprised of many traditional measures of context and organization characteristics (organization size, type, location, etc.). Among the interviewees, Structural Characteristics often involved discussions of organization infrastructure for the program (physical space, staff size, etc.). As this construct contains a multitude of dimensions, interviewees frequently described both positive and negative examples, resulting in many mixed ratings. This construct appears to distinguish the high and medium reach level organizations from the low reach group. In the medium and high reach levels, interviewees often discussed both the benefits and challenges of implementation related to structural characteristics. For example, one interviewee commented on how the size of the organization can both help and hinder National DPP implementation (exemplary quotes provided in Table 3).
However, among the low reach group, the vast majority of the coded structural characteristics segments were rated negatively. These interviewees reported difficulties with limited infrastructure for the program, lack of staff and staff time, challenges with developing referral systems, and administrative/bureaucratic hurdles due to their organization type. For example, an interviewee from a local government agency shared many challenges involved with applying for and implementing grants due to their organization structure and bureaucracy. Across all cases, organization type and how it impacted organization reach to populations, available infrastructure/resources, administrative processes, and reputation in the community was most salient.
Compatibility
Compatibility is a subconstruct of Implementation Climate and relates to how the intervention fits within the organization and its existing workflows, systems, and services. High and medium reach groups more often yielded strong positive examples of compatibility impacting implementation, compared to those in the low reach group. Interviewees describing positive examples of the influence of compatibility on implementation often mentioned that their organization offered complementary programs to the National DPP (e.g., diabetes self-management, nutrition education, and fitness classes). This allowed them to more easily adopt and implement the National DPP. As described by one high reach organization interviewee, “it’s a nice complement and it nicely rounds out the services that we offer.”
In the strongest positive examples, interviewees shared how other programs within their organization referred program participants to the National DPP and vice versa. They also gave positive examples of how the National DPP was embedded in their workflows and systems via the electronic health records (EHR) or other referral processes, all of which support enrollment efforts. Two high reach group interviewees described challenges introducing the National DPP into their organization systems, but by taking time to educate key leaders and staff about the program, they were able to overcome those challenges and succeed with implementation. Conversely, in strong negative examples of compatibility, interviewees struggling to implement the National DPP described how it was different from the typical services and programs provided by their organization and was not embedded into their current systems, one interviewee described this as having to “force it to fit.”
Across all reach levels, there were some additional themes related to compatibility. A commonly voiced complaint was how time-consuming and burdensome the data reporting to the CDC DPRP is compared to other evidence-based interventions implemented at their organizations. Lastly, in a few cases, interviewees shared that their organization had a large number of chronic disease programs, and this created challenges for staff to remember to refer to the National DPP.
Goals and feedback
Goals and feedback is a subconstruct of Implementation Climate and refers to the degree to which goals are clearly communicated, acted upon, and fed back to staff, as well as the alignment of that feedback with goals. We asked interviewees to discuss how enrollment goals (target number of participants to recruit each year) set by them or leaders at their organization impacted their implementation efforts. Overall, interviewees did not provide many details on how enrollment goals impact implementation (hence many interviewees have an “X” on the matrix for this construct). However, while interviewees lacked examples for the construct rating, this construct was distinguishing among reach groups by some of the extreme examples in the higher reach group and the thematic analysis which found the presence or absence of enrollment goals differed by reach level. The majority of the high implementation organizations (n = 9, 82%) had formal enrollment goals set by organization leadership or the program coordinator. In comparison, only four (40%) of the medium and three (33%) low reach interviewees reported having enrollment goals.
When organizations had enrollment goals there were clear examples as to how goals facilitated enrollment. One high reach group interviewee described how goals motivate the staff to increase their referrals and enrollment, saying, “[…] it’s nice to have the number, I like numbers. Tell me what you want, I’ll go for that number.” For organizations that did not have formal enrollment goals, interviewees mentioned other goals such as achieving CDC DPRP recognition status, billing Centers for Medicare & Medicaid Services (CMS)/becoming a Medicare DPP supplier, training their staff to implement the program, general diabetes prevention in their communities, or focusing on the retention of their current cohorts first before attempting to enroll more participants. One interviewee from a medium reach organization said because their focus is on establishing a process for billing CMS, they are not concerned about enrollment and prefer a small cohort at the moment. Multiple interviewees that currently did not have enrollment goals said they were interested in setting formal enrollment goals. While the interviews focused on pre-COVID-19 implementation, a few interviewees mentioned how COVID-19 had disrupted their implementation and therefore currently enrollment goals were not a priority.
Leadership engagement
Leadership engagement is a subconstruct of Readiness for Implementation and refers to the commitment, involvement, and accountability of leaders and managers with the implementation of the program. This construct appeared numerous times throughout most interviews. While the majority of interviewees simply said they have “support” from their leadership, when asked to describe this support in terms of leadership engagement their examples varied greatly. Examples included: leadership being aware of all program activities and events, making presentations to promote the program, connecting with other organization leaders/partners for the program, facilitating internal organization processes (e.g., board approvals, system establishment) for the program, obtaining resources including adequate staffing for the program, and providing the program for free to organization employees.
Leadership engagement was a distinguishing construct as high and medium reach cases had more strong positive examples of leadership engagement compared to the low reach cases. High and medium reach interviewees also more often connected leadership engagement with positive examples of successful enrollment efforts and growing the infrastructure for the program. The lower reach group had more mixed experiences with this construct. Leadership was described as not being engaged enough; not doing enough to understand the program, and taking a “hands off” approach. The key message from all interviewees across reach levels was that leadership engagement is highly desired and appreciated when available. Leadership support and knowledge of the program was discussed as a strong facilitator in implementing and scaling the program.
Discussion
This study applied CFIR to examine the internal and external organization factors influencing National DPP implementation. The four distinguishing constructs from the inner setting (structural characteristics, compatibility, goals & feedback, and leadership engagement) indicate that there are multiple factors internal to the organization that can impact implementation and enrollment success. Our findings are consistent with other studies that have found that some of these same constructs influence successful implementation—particularly within the inner setting domains such as leadership engagement and the implementation climate subconstructs [29, 30, 34, 35].
Similar to previous research, positive leadership engagement on implementation involved going beyond surface-level support of the program and was highlighted by taking an active role in understanding the program, attending program events, promoting the program, and providing resources [29, 30, 34]. The distinguishing implementation climate subconstructs of compatibility, relative priority, and goals and feedback indicated that for organizations at higher reach levels, the National DPP fit better with existing services, health promotion programs, and systems, was prioritized by the organization leadership, and had formal enrollment goals outlined.
To date, there is a lack of evaluation of the National DPP using CFIR constructs; however, other lifestyle change programs also focused on physical activity and nourishment behaviors to achieve weight loss have been studied using CFIR [30, 36,37,38]. These studies have also found a heavy emphasis on the inner setting when exploring program implementation successes and challenges. Related the outer setting, their results described challenges with billing and program reimbursement/financing policies. Our study did not find any outer setting constructs distinguishing between reach levels; however, there were notable themes that emerged from the data around the importance of external partnerships, understanding participant needs, benefits of learning from and competing with other National DPP delivery organizations, and challenges with reimbursement programs (like Medicare DPP). Likewise, the constructs that were not rated (incentives and rewards, learning climate, access to knowledge & information, and patient needs & resources), also provided other insights into the program, such as examples of program participant barriers and challenges, however they did not talk in enough detail about these influences on implementation and enrollment to be included in this analysis.
The findings of this study have the potential to facilitate implementation of the National DPP. While the National DPP provides guidance on the standard infrastructure needed for organizations to deliver the program (structural characteristics) and the importance of partnerships (cosmopolitanism), previously there has been less of a conversation about organization compatibility, priorities, goal setting and feedback, and active leadership engagement which we identified as important in this study [39, 40]. The CDC should consider inclusion of CFIR-related constructs such as leadership engagement in the CDC DPRP Organizational Capacity Assessment, a suggested tool that delivery organizations use at the time of adoption. The assessment is primarily focused on the minimum requirements to deliver the program (e.g., classroom space, equipment, staff requirements) but does not help identify which organization characteristics may be particularly suited to reach a large number of participants and successfully scale. The current version does include about many of the CFIR constructs including the ones identified as distinguishing in our study. For example, there is no discussion of how well the program “fits” within an organization’s current programs and services or how the program would be prioritized if implemented. Inclusion of these constructs could assist with identifying key gaps in organization adoption readiness, enrollment, and scalability [41, 42].
To support low reach delivery organizations, the CDC and other National DPP technical assistance providers should consider guidance and resources to increase program compatibility, prioritization, goal setting, and leadership engagement. However, the main program implementers may not have control over these conditions. For example, a frequently mentioned challenge in the relative priority construct was limited staff and staff time dedicated to the program. Organizations may require more assistance and resources from the CDC and others to ensure adequate staff are not only hired and properly trained, but that their time is dedicated sufficiently to the National DPP. These considerations may also be applicable to other evidence-based programs as well.
Future research
More research is required to understand how internal and external organization factors influence implementation in order to continue to scale the National DPP. While this study did not identify any outer setting constructs as distinguishing, the outer setting construct, cosmopolitanism, has appeared in National DPP studies focused on referrals from providers, health systems, and other community partners [17, 20, 40]. Organizations with strong external partnerships were able to leverage this into increased referrals to their programs. Our study may not have found outer setting constructs as distinguishing because the interviewees focused more heavily on the inner setting constructs and interviewees reported mostly neutral and positive experiences regardless of reach level (Fig. 1). Additional research may be warranted to explore how the outer setting may affect the National DPP or other chronic disease programs. Likewise, future research should also include exploration of the other CFIR domains (intervention characteristics, process, and characteristics of individuals) to provide a holistic perspective on factors related to reach.
It is challenging to compare the National DPP to other programs using CFIR, as researchers have focused on different dimensions of CFIR constructs, often times based on relevant factors for the specific program. For example in the Cannon et al. 2019 study, the culture construct was operationalized as implementation of staff turnover [43], whereas in our study we focused on an organization’s general beliefs, values, and assumptions. This is a shortcoming of CFIR itself which has been criticized as very complex and multi-dimensional, and requiring more nuanced detail [44]. The developers of CFIR have developed a second version of the framework with the goal of addressing this criticism and other gaps that may be helpful to use in subsequent studies [45].
Measuring CFIR constructs quantitatively is a growing area that has great potential to assist with understanding the relationship between implementation factors and outcomes [46, 47]. Implementation science researchers have started testing quantitative measures for CFIR constructs; however, more work is needed in this area to fully understand the validity and reliability of these constructs, how they are operationalized in practice, and their associations with implementation outcomes [48,49,50,51,52]. CFIR quantitative measures have typically examined relationships between constructs and shorter-term implementation (e.g., adoption) rather than later-term outcomes like sustainability [21]. Using CFIR measures across the continuum of implementation will be critical to assess differences in key factors related to outcomes in the pre-adoption, early adoption, and maintenance phases [53].
Strengths and limitations
Strengths of this study include a priori use of CFIR constructs and instruments, highly trained qualitative researchers and coders, rigorous double coding and analysis of data, and the application of the construct rating methods employed by other researchers. However, this study had several limitations that should be considered. First, there are 2000 + organizations delivering this program nationwide, and our study included only 30 in our sample, therefore results may be limited. In addition, we recruited from Emory’s DTTAC contact list and while this population is very large and diverse, there may be implementation differences between this group and the larger National DPP population of implementers because of the training and technical assistance they receive from Emory.
Second, only one interview was conducted per organization. Other papers using this construct rating method typically include 2–3 interviewees per organization [29, 30]. However, we were able to talk with 30 different organizations which is a higher number of unique organizations than is typical for this analysis. Instead of depth within organizations, we focused on breadth across a diverse range of organizations and focused on the best possible informant to answer our questions (the Program Coordinator). In order to capture the diversity in National DPP implementation, we did not limit organizations based on a specific number of years of delivery for recruitment. Instead, we operationalized reach using the average enrollment per year of delivery. Reach numbers were self-reported by the interviewee and we did not have access to the programmatic data to confirm or examine changes in enrollment over the years of delivery. While imperfect, using the average enrollment per year helps compare implementation success across organizations.
For this study we only focused on the inner and outer setting constructs of CFIR and decidedly focused on the organization-level perspective, which limits our understanding of the other dimensions of implementation (intervention characteristics, process, and characteristics of individuals). Lastly, in early 2020 the COVID-19 pandemic disrupted the National DPP, a largely in-person program, greatly. We did try to limit our interview discussions to pre-COVID implementation and saved COVID-19 related conversations to the end of the interview. As the pandemic has been an unignorable outer setting/external factor it is hard to say how much of the discussion of these topics was impacted by implementers who found themselves in a “survival/adaptation mode” at the time of the interview. The recently released CFIR 2.0 update now includes a new outer setting construct named “critical incidents” to capture “large-scale and/or unanticipated events” that may provide useful for situations such as these [54].
Conclusions
This study found that there are a number of CFIR inner setting constructs that impact implementation reach of the National DPP. This understanding can be leveraged to improve efforts in recruiting and assisting delivery organizations to increase the reach and scale of the program. This is one of only a few studies of the National DPP at the organization level and to use the CFIR construct rating qualitative methodology to explore the national implementation of this program. More focused attention to program compatibility, prioritization, setting program goals, and leadership engagement has the potential to improve program implementation. Furthermore, these results have broader application to understand how best to assist organizations to adopt, deliver, and scale evidence-based programs.
Availability of data and materials
De-identified qualitative data is available by reasonable request to the corresponding author. Quantitative data was from DTTAC databases which are not publicly available.
Notes
The DPRP provides national quality standards to ensure organizations are delivering the program with fidelity. These standards and procedures are updated every three years based on new dietary, physical activity, self-efficacy, delivery modality, and other type 2 diabetes prevention evidence. CDC-recognized organizations work toward progressing from pending to preliminary to full recognition status.
Abbreviations
- CDC:
-
Centers for Disease Control and Prevention
- CFIR:
-
Consolidated Framework for Implementation Research
- CMS:
-
Centers for Medicare & Medicaid Services
- DPP:
-
Diabetes Prevention Program
- DPRP:
-
Diabetes Prevention Recognition Program
- DTTAC:
-
Diabetes Training and Technical Assistance Center
- EHR:
-
Electronic Health Record
- InGEAR:
-
Innovations to Grow Enrollment and Retention
- MDPP:
-
Medicare Diabetes Prevention Program
References
Centers for Disease Control and Prevention. National Diabetes Statistics Report website. 2022 01.28.2022]; Available from: https://www.cdc.gov/diabetes/data/statistics-report/index.html.
Albright A, Gregg E. Preventing type 2 diabetes in communities across the US: the National Diabetes Prevention Program. Am J Prev Med. 2013;44(4):S346–51.
Centers for Disease Control and Prevention. National Diabetes Prevention Program. 2021 [cited 17 Feb 2022]; Available from: https://www-cdc-gov.proxy.library.emory.edu/diabetes/prevention/index.html.
Knowler WC, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403.
Gruss SM, et al. Public Health Approaches to Type 2 Diabetes Prevention: the US National Diabetes Prevention Program and Beyond. Curr DiabRep. 2019;19(9):78.
Ackermann RT. From Programs to Policy and Back Again: The Push and Pull of Realizing Type 2 Diabetes Prevention on a National Scale. Diabetes Care. 2017;40(10):1298–301.
Centers for Disease Control and Prevention, Diabetes Prevention Recognition Program: Registry of All Recognized Organizations. 2022: https://dprp.cdc.gov/Registry.
Ely EK, et al. A National Effort to Prevent Type 2 Diabetes: Participant-Level Evaluation of CDC’s National Diabetes Prevention Program. Diabetes Care. 2017;40(10):1331–41.
Ritchie ND, Kaufmann P, Sauder KA, Comment on Ely, et al. A National Effort to Prevent Type 2 Diabetes: Participant-Level Evaluation of CDC’s National Diabetes Prevention Program. Diabetes Care. 2017;40:1331–41 Diabetes care, 2017. 40(11): p. e161-e162.
Wandersman A, et al. Bridging the gap between prevention research and practice: the interactive systems framework for dissemination and implementation. Am J Community Psychol. 2008;41(3–4):171–81.
Glasgow RE, et al. RE-AIM Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-Year Review. Front Public Health. 2019;7(64):1–9.
Glasgow RE, et al. The RE-AIM framework for evaluating interventions: what can it tell us about approaches to chronic illness management? Patient Educ Couns. 2001;44(2):119–27.
Cheadle A, et al. Using the concept of “population dose” in planning and evaluating community-level obesity prevention initiatives. Am J Eval. 2013;34(1):71–84.
Burd C, et al. Translating Knowledge into Action to Prevent Type 2 Diabetes: Medicare Expansion of the National Diabetes Prevention Program Lifestyle Intervention. Milbank Q. 2020;98(1):172–96.
Ackermann RT, O’Brien MJ. Evidence and challenges for translation and population impact of the diabetes prevention program. Curr DiabRep. 2020;20(3):9.
Meyer H. Medicare diabetes prevention: enrollment short of projections. Health Aff. 2021;40(11):1682–7.
Nhim K, et al. Using a RE-AIM framework to identify promising practices in National Diabetes Prevention Program implementation. Implement Sci. 2019;14(1):81.
Brunisholz KD, et al. A formative evaluation of a diabetes prevention program using the RE-AIM framework in a learning health care system, Utah, 2013–2015. Prev Chronic Dis. 2017;14:E58.
Ali MK, et al. Reach and use of diabetes prevention services in the United States, 2016–2017. JAMA Netw Open. 2019;2(5):e193160–e193160.
Mosst JT, et al. A Framework for implementing the national diabetes prevention program in Los Angeles County. Prev Chronic Dis. 2017;14:E69.
Chaudoir SR, Dugan AG, Barr CH. Measuring factors affecting implementation of health innovations: a systematic review of structural, organizational, provider, patient, and innovation level measures. Implement Sci. 2013;8(1):22.
Kirk MA, Kelley C, Yankey N, Birken SA, Abadie B, Damschroder L. A systematic review of the use of the consolidated framework for implementation research. Implementation Science. 2015;11(1):1–3.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation science. 2009;4(1):1–5.
Damschroder LJ, Reardon CM, Lowery JC. The Consolidated Framework for Implementation Research (CFIR), in Handbook on Implementation Science. UK: Edward Elgar Publishing; 2020. pp. 88–113.
Bastos De Carvalho A, et al. Evaluation of multi-level barriers and facilitators in a large diabetic retinopathy screening program in federally qualified health centers: a qualitative study. Implementation Science Communications. 2021;2(1).
VanDerBrink E, et al. Adapting the “resist diabetes” resistance training intervention for veterans. Transl J Am Coll Sport Med. 2020;5(5):39.
Kowalski CP, Veeser M, Heisler M. Formative evaluation and adaptation of pre-and early implementation of diabetes shared medical appointments to maximize sustainability and adoption. BMC Family Practice. 2018;19(1):1–23.
Wilcox S, et al. Predictors of implementation in the Faith, Activity, and Nutrition dissemination and implementation study: application of the Consolidated Framework for Implementation Research (CFIR) in a statewide initiative. Transl Behav Med. 2021;11(2):419–29.
Liang S, et al. Integrating evidence-based practices for increasing cancer screenings in safety net health systems: a multiple case study using the Consolidated Framework for Implementation Research. Implement Sci. 2015;11(1):109.
Damschroder L, Lowery JC. Evaluation of a large-scale weight management program using the consolidated framework for implementation research (CFIR). Implement Sci. 2013;8:51.
VERBI Software. MAXQDA 2020. Berlin: VERBI Software; 2019.
Malterud K. Qualitative research: standards, challenges, and guidelines. The lancet. 2001;358(9280):483–8.
Hennink, M., I. Hutter, and A. Bailey, Qualitative research methods. 2010: Sage.
Piat M, et al. Identifying and understanding the contextual factors that shaped mid-implementation outcomes during the COVID-19 pandemic in organizations implementing mental health recovery innovations into services. Implement Sci Communications. 2021;2(1):101.
Shade L, Ludden T, Dolor RJ, Halladay J, Reeves K, Rees J, Hendrickson L, Bray P, Tapp H. Using the Consolidated Framework for Implementation Research (CFIR) to evaluate implementation effectiveness of a facilitated approach to an asthma shared decision making intervention. J Asthma. 2021;58(4):554–63.
Batsis JA, McClure AC, Weintraub AB, Sette D, Rotenberg S, Stevens CJ, Gilbert-Diamond D, Kotz DF, Bartels SJ, Cook SB, Rothstein RI. Barriers and facilitators in implementing a pilot, pragmatic, telemedicine-delivered healthy lifestyle program for obesity management in a rural, academic obesity clinic. Implement Sci Comms. 2020;1(1):1–9.
Damschroder LJ, et al. Implementation evaluation of the Telephone Lifestyle Coaching (TLC) program: organizational factors associated with successful implementation. Transl Behav Med. 2016;7(2):233–41.
Makama M, et al. Reducing postpartum weight retention: a review of the implementation challenges of postpartum lifestyle interventions. J Clin Med. 2021;10(9):1891.
Centers for Disease Control and Prevention, Diabetes Prevention Recognition Program: Standards and Operating Procedures. Atlanta; 2021. https://www.cdc.gov/diabetes/prevention/pdf/dprp-standards.pdf. Retrieved May 1, 2021.
Vojta D, et al. A coordinated national model for diabetes prevention: linking health systems to an evidence-based community program. Am J Prev Med. 2013;44(4 Suppl 4):S301–6.
Weiner BJ, Amick H, Lee S-YD. Conceptualization and measurement of organizational readiness for change: a review of the literature in health services research and other fields. Med Care Res Rev. 2008;65(4):379–436.
Weiner BJ. A theory of organizational readiness for change. Implement Sci. 2009;4(1):67.
Cannon JS, et al. Influence of an Implementation Support Intervention on Barriers and Facilitators to Delivery of a Substance Use Prevention Program. Prev Sci. 2019;20(8):1200–10.
Ilott I, et al. Testing the consolidated framework for implementation research on health care innovations from South Yorkshire. J Eval Clin Pract. 2013;19(5):915–24.
Damschroder L, Smith LR. Introduction and application of version 2 of the consolidated framework for implementation research (CFIR). in 14th Annual Conference on the Science of Dissemination and Implementation. 2021. AcademyHealth.
Weiner BJ, et al. Measuring readiness for implementation: A systematic review of measures’ psychometric and pragmatic properties. Implement Res Pract. 2020;1:2633489520933896.
Miake-Lye IM, et al. Unpacking organizational readiness for change: an updated systematic review and content analysis of assessments. BMC Health Serv Res. 2020;20(1):106.
Fernandez ME, et al. Developing measures to assess constructs from the inner setting domain of the consolidated framework for implementation research. Implement Sci. 2018;13(1):52.
Dorsey CN, et al. A systematic review of measures of implementation players and processes: summarizing the dearth of psychometric evidence. Implement Res Pract. 2021;2:26334895211002470.
Wilcox S, Jake-Schoffman DE, Saunders RP, Kinnard D, Kaczynski AT, Hutto B, James KL. Predictors of implementation in the Faith, Activity, and Nutrition dissemination and implementation study: Application of the Consolidated Framework for Implementation Research (CFIR) in a statewide initiative. Transl Behav Med. 2021;11(2):419–29.
Tinc PJ, et al. Key factors for successful implementation of the National Rollover Protection Structure Rebate Program: a correlation analysis using the consolidated framework for implementation research. Scand J Work Environ Health. 2020;46(1):85–95.
McHugh S, et al. Measures of outer setting constructs for implementation research: a systematic review and analysis of psychometric quality. Implement Res Pract. 2020;1:2633489520940022.
Damschroder LJ, et al. Conceptualizing outcomes for use with the Consolidated Framework for Implementation Research (CFIR): the CFIR Outcomes Addendum. Implement Sci. 2022;17(1):1–10.
Damschroder L, et al. The Updated Consolidated Framework for Implementation Research: CFIR 2.0. 2022.
Acknowledgements
This work was made possible by the partnership between Emory’s Diabetes Training and Technical Assistance Center and The Georgia Center for Diabetes Translation Research.
Funding
This study was funded by the Centers for Disease Control and Prevention Division of Diabetes Translation Innovations to Grow Enrollment and Retention (InGEAR) project. MBW is partially supported by NIDDK P30DK111024.
Author information
Authors and Affiliations
Contributions
LM—design, conception, analysis, interpretation, and writing of the manuscript. OM—data collection, analysis, interpretation, and major contributor in writing the manuscript. MK, RH, SP, LB, MBW, CE reviewed all study protocols and instruments, assisted with interpretation of findings, and contributed in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was reviewed and provided exemption by the Emory University Institutional Review Board (STUDY00000658).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Interview Guide Questions.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Madrigal, L., Manders, O.C., Kegler, M. et al. Inner and outer setting factors that influence the implementation of the National Diabetes Prevention Program (National DPP) using the Consolidated Framework for Implementation Research (CFIR): a qualitative study. Implement Sci Commun 3, 104 (2022). https://doi.org/10.1186/s43058-022-00350-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43058-022-00350-x