
Abstract
Background
Patients with dense breasts have a higher risk factor for developing breast cancer. Digital mammography (DM) exhibits a reduced sensitivity in dense breast tissue as a result of overlapping fibro-glandular tissue. Digital breast tomosynthesis (DBT) solves this problem, so allows better characterization of masses, asymmetries, and parenchymal distortion. It is useful in screening studies for early detection of breast lesions by accurate detection and description of their margins, shape, and extent as well as surrounding structures.
Objective
We aimed to evaluate the added value of DBT in characterizing of different breast lesions in dense breasts compared to DM.
Methods
A Prospective Cohort study involved ninety female cases having dense breast parenchyma (ACR C & ACR D) having breast complaint lesions detected by DM or ultrasound or recalled from screening units, during the period from June 2021 to Jan 2023.
All patient underwent DM and DBT with correlation with the pathological finding or follow up.
Results
As regards the characterization of breast mass DBT had higher sensitivity, higher specificity (98%, 87% respectively). However, DM showed less sensitivity, less specificity (58%, 80%,) with (p < 0.0001, p = 0.0005 respectively).
Conclusions
DBT effectively visualizes overlapping tissue in dense breasts. DBT is important due to its ability to detect breast cancer earlier, characterize lesions accurately, and inspect the margins of masses precisely, along with decreasing recall rates for false-positive results.
Similar content being viewed by others

Background
Breast cancer represents the predominant type of cancer among females globally, comprising 27% of all women's cancer cases [1]. Early detection decreases mortality related to breast cancer. The survival probability within 5 years would rise to nearly 95% if the malignancies could be discovered at an earlier stage [2].
Digital mammography (DM) represents the basic imaging technique utilized for diagnosing breast cancer; however, it is linked to a few limitations as regards dense breasts [3].
Breast density is the fibrog-landular tissues’ proportion to fat so used to define how many different types of breast tissue. Women having greater breast density exhibit a four to five fold increased chance of breast cancer than those having low breast density [4, 5].
Due to decreased differentiation between the dense lesions and surrounding dense breast tissue, DM offers reduced specificity as well as sensitivity for females having dense breasts [6]. Digital breast tomosynthesis (DBT) is aimed at minimizing dense breast tissue overlap [1].
Many published studies suggest that DBT is preferable to the standard DM as DBT improves lesion description, and assessment of areas of architectural distortion and asymmetries [7, 8].
DBT is important for diagnostic settings, which lowers associated expenses, additional mammographic views [9], and biopsies [10].
DBT excludes suspicious lesions discovered during screening [11]. As it is effective in differentiating benign from malignant tumors [12].
The prognosis and treatment plans for breast cancer are determined by the initial tumor stage at the time of diagnosis. As neoadjuvant chemotherapy and breast-conservative surgeries become more common, a clear characterization of the tumor size and numbers is essential step, DBT in the preoperative local staging of breast cancer with focus on the detection of multifocal/multicentric disease in a patient population with dense breasts is a promising imaging technique [13], 14].
This work was aimed to assessing the DBT added value in characterizing different breast lesions in dense breasts compared to DM.
Methods
Study design and ethical approval
In this prospective cohort study, approved by our institutional review board of Medicine Ethical Committee, all participants were asked to fill out an informed consent after fully explaining our research to them. Privacy of all patient data is guaranteed.
Study population (eligibility criteria)
This research involved female cases with dense breasts having breast complaints during the period from 1st June 2021 to 30th Jan 2023 at our institute.
Inclusion criteria: symptomatic females with a breast lump, pain, or nipple discharge, females with lesions detected by DM or ultrasound, females recalled from screening units, females with dense breast parenchyma (ACR C & ACR D), and females below the age of 40 with positive family history.
Exclusion criteria: patients who had previous breast surgery or mastectomy, already diagnosed with breast cancer, already had breast implants and those with non-dense breast parenchyma (ACR A & ACR B) were not involved in our research.
All participants underwent DM and DBT. We carried out a complementary ultrasound to either verify or rule out mammographic findings utilizing a high-frequency probe.
The mammographic examination was performed utilizing an upgraded Hologic Healthcare Full Field Digital Mammography machine to produce 3D Digital Tomosynthesis. It possesses a dual anode (Rhodium Molybdenum) with a CsI digital detector. Standard DM views of mediolateral oblique (MLO) as well as cranio-caudal (CC) views were captured for all participants. For DBT (MLO for all patients and CC was done in 25 patients) views were also accomplished. DBT entailed obtaining twelve to fifteen 2D projection exposures utilizing a digital detector from a mammographic X-ray source, moving within a restricted arc angle. The compressed breast 3D volume was accomplished utilizing the 2D projections, resulting in a sequence of images (slices) encompassing the entire breast. Assessing these images was done on the workstation.
Image analysis and interpretation of DM and DBT
The DM along with DBT images were independently and blindly evaluated by two radiologists, one possessing eleven years of expertise while the other possessing sixteen years of expertise, If the two readers were unable to reach an agreement, a third highly skilled radiologist possessing 2 years expertise would be responsible for making the ultimate decision. The agreement level amongst observers was high.
Each participant underwent a breast density evaluation and chose a patient with dense breasts (ACR C & ACR D). Based on the ACR BIRADS lexicon 2013 [14].
All findings were assessed as regards location; type (mass, asymmetry, distortion ± calcifications) as well extension.
-
Mass lesions were assessed for margin, density, and shape.
-
Asymmetry: focal, global, or developing.
-
Parenchymal distortion: Yes, or no.
-
Calcifications: Benign or malignant.
We classified the findings in each of the two imaging techniques separately utilizing the BI-RADS lexicon 2013 classification [14], (Table 1) as indicated by the results of mammographic findings but blind to final histopathology results and complementary ultrasound.
In view of different BIRADS categories, different further recommendations have been made as follows
-
BIRADS 1 or 2: Follow up every year.
-
BIRADS 3: Follow up every 6 months for two years at least.
-
BIRADS 4 or 5: histopathological correlation (True cut biopsy, stereotactic biopsy).
These findings underwent categorization as either benign or malignant based on the mammography BI-RADS lexicon morphology descriptors [14].
In our study
-
Women diagnosed as BIRADS 4 or 5 and some cases of BIRADS3 were subjected to histopathological examination which was the gold standard reference for cancer detection.
-
Women with unbiased findings BIRADS 3 were evaluated with ultrasound and subjected to follow-up three times every 6 months.
-
Ultrasound was the golden standard for BIRADS 1 and 2 cases with annual follow-up.
-
The patient had more than one lesion on the same side of the breast we wrote the highest BIRADS for this side.
-
Cases diagnosed with multifocal/ multicenteric lesions confirmed by contrast-enhanced spectral mammogram (CESM)/ Pathology after surgery.
Statistical analysis
Data went through a process of collection, coding, revision as well as transfer to the Statistical Package for Social Science (Rstudio) version 2.3.2. The data were displayed as numbers as well as percentages regarding the qualitative data, mean, SD as well as ranges as regards the quantitative data with parametric distribution while median with interquartile range (IQR) for the quantitative data with non-parametric distribution. The chi-square test was utilized for comparing both groups with qualitative data while the Fisher exact test was utilized as a substitute for the Chi-square test when the expected count within any cell was deemed to be below 5. The receiver operating characteristic curve (ROC) is produced by plotting sensitivity (TP) on the Y axis versus 1-specificity (FP) on the X axis at different cut-off values. The area under the ROC curve indicates the test’s diagnostic performance. An area above 50% indicates acceptable performance while an area about 100% represents the ideal performance for the test. The confidence interval was established at 95% while the margin of error accepted was set at 5%.
Results
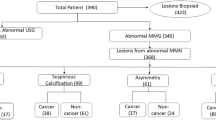
Our cohort study was carried out on one hundred and fifty (150 females) with dense breasts who had breast complains, we excluded forty (40) females who didn’t have pathology for breast lesions BIRAD 4 and 5, and twenty (20) patients missed follow-up in breast lesions BIRAD 3. Thus, statistical analysis was carried out on ninety (90) females who matched our research’s inclusion requirements.
The final cohort consisted of 90 women (whose ages range between (30 and 75) years with mean ± SD (45.7 ± 8.1) years. 52.2% ranged between (40 and 50) years, 27.7% ranged between (30 and 40) years and 15.6% ranged between (50–60) years. Among 90 females, 80% were assigned as ACR C while 20% were ACR D based on the ACR BIRADS lexicon breast density classification.
Breast lump was the most common symptom (43%) followed by breast pain (35%), and nipple discharge (24%), and (15%) were came for breast screening.
Characterization of Breast Lesions by DM: 39 lesions (43%) were defined as breast mass, 33 lesions (36%) breast asymmetry, 10 lesions (11.1%) parenchymal distortion, 31 lesions (34.3%) breast calcification, & 4 (4.4%) were normal breast (Fig. 1)

A 49-year-old female presented with a right breast lump. a Right breast craniocaudal & b mediolateral oblique DM images showed extremely dense breast parenchyma (ACR d) and right UIQ partially obscured mass lesion (Black Arrow), BIRADS 3. c Bilateral breasts mediolateral oblique DBT images showed right breast well circumscribed macrolobulated mass lesion (Yellow arrow) BIRADS 3. The lesion was categorized by DM and by DBT as BIRADS3 with better margins delineation by DBT images and follow-up by the US confirmed mass stability likely fibroadenoma and no need for biopsy
Characterization of Breast Lesions by DBT: 57 lesions (63.3%) were defined as breast mass, 17 lesions (18.8%) breast asymmetry, 27 lesions (30%) parenchymal distortion, 34 (37.7%) breast calcification & 5 (5.5%) were normal breast (Fig. 2).

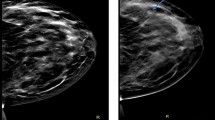
A 45-year-old female presented with a right breast lump. DM Bilateral a CC & b MLO images showed extremely dense breasts (ACR d). c Bilateral DBT CC & d left zoomed DBT images showed Left UOQ speculated mass lesion (White arrows), BIRADS4. e Right-zoomed DBT images showed right circumscribed isodense mass lesions (Yellow Arrows), BIRADS2. Proved by a biopsy to be IDC
A statistically significant variation was documented among DM and DBT about asymmetry at (p = 0.02) as shown in Table 2. DBT improved the assessment of focal asymmetry in 14 cases as it clarified that was condensed parenchyma, not a true lesion. Figure 3

A 54-year-old female came for screening. a Bilateral breasts craniocaudal & b mediolateral oblique DM images showed heterogeneously dense breasts (ACR c) and left lower quadrant asymmetry (Arrow). c Bilateral mediolateral oblique DBT images showed a left breast lower deeply seated area of focal asymmetry and were confirmed to be an area of overlapping fibro-glandular tissue with no underlying masses or distortion. The lesion was categorized by DM as BIRADS3 and BIRADS2 by DBT
A statistically significant variation was documented among DM as well as DBT regarding parenchymal distortion at (p = 0.003) as illustrated in Table 2.
As regards the association with the final diagnosis: DBT detected 27 distortions (4) were benign and (23) were malignant however DM detected only 10 distortions (4) were benign and (6) were malignant (Figs. 4 and 5).

A 40-year-old female presented with mastalgia. a Right breast craniocaudal & b mediolateral oblique DM images showed heterogeneously dense breasts (ACR c) and benign-looking calcific foci. c Bilateral breast craniocaudal & d right zoomed DBT images showed right breast UOQ subtle distortion (Arrow). The lesion was categorized by DM as BIRADS2 and BIRADS4 by DBT. Pathological data after surgery and proved ILC

A 57-year-old female presented with right nipple discharge. a Bilateral breasts craniocaudal. b mediolateral oblique DM images showed extremely dense breasts (ACR d). c Right breast craniocaudal. d Right-zoomed DBT images showed the right UOQ area of parenchymal distortion (Yellow arrows), BIRADS4. Biopsy proved IDC & DCIS
Both DM and DBT detected benign calcification (Pop-corn 2 (2.2%), Rim 3 (3.3%), Round 8 (8.9%)) and suspicious calcifications (Coarse heterogonous 3 (3.3%), Linear 3 (3.3%), Pleomorphic 8 (8.9%)) however DBT detected more Amorphous calcification 7 (7.7%)than DM 4 (4.4%), with no statistically significant association as regard of benign and suspicious calcification between DM & DBT (p = 0.99, p = 0.686 respectively).
As regards the distribution of breast lesions single lesions, multifocal or multicenteric lesions showed a statistically significant variation among DM & DBT (p = 0.004) as illustrated in Table 3 (Fig. 6).

A 63 years-old female presented with left breast sweeling (a, b) DM CC & MLO craniocaudal & b mediolateral oblique DM images showed heterogeneously dense breasts (ACR c) and LIQ focal area of asymmetry with subtle distortion. c Left breast craniocaudal & d mediolateral oblique DBT images showed left breast LIQ focal asymmetry with underling distortion and UIQ irregular mass lesion as well UOQ distortion (Arrows). e Further contrast enhanced spectral mammogram (CESM) confirmed multicentrecity. The lesion was categorized by DM as BIRADS4 and BIRADS5 by DBT. Pathological data after surgery and proved IDC
In correlation with the final diagnosis Table 4
Histopathology was done for 53 cases and revealed 45 were malignant (9 patients were done modified radical mastectomy MRM 36 cases of conservative breast surgery (CBS) and 8 were benign (4 patients did wide local excision (WLE) and 4 patients did core biopsy), Follow up with no need for biopsy for 37 cases.
The BIRADS results by DM & DBT
BY DM the most common breast lesions were categorized as BIRAD 3 (41%) Fig. 5 then BIRAD 4 (36.7%) and BIRAD 5 was the least category (2.2%) However by DBT the most common breast lesions were categorized as BIRAD 4 (45.6%) then BIRAD 2 (22.4%) and cases with BIRAD 5 category were (10%) (Fig. 7).

Distribution of breast lesions BIRADS in DM & DBT in all cases
Comparison between DM and DBT as a regard BIRADS showed a statistically high significant variation at (p < 0.001) shown in Table 5.
The DM and DBT diagnostic accuracy in characterizing of breast lesions in dense breasts showed higher sensitivity, higher specificity in DBT (98%, 87% respectively). Compared to DM sensitivity and specificity, (58%, 80% respectively) with statistically significant (p < 0.0001) illustrated on Table 6 and Fig. 8.

ROC Curve for the assessment of DM and DBT as a regard the gold standard in characterization of breast lesions
Discussion
This Study involved 90 women with dense breast. All participants went through DM& DBT, 80% were ACR C and 20% were ACR D. We evaluate the value of DBT in characterization of breast lesions compared to the DM, the DBT characterized the breast lesions more accurate than DM as in mass lesions DBT detected 57 mass (29 malignant and 28 benign) however DM detected 39 mass (18 malignant and 21 benign)So DBT detected 18 mass lesions not clearly identified in DM, in parenchymal distortion DBT detected 17 cases more than DM (1 benign and 16 malignant), In breast asymmetry DM detected 33 asymmetry, the DBT improved the result as it detected 16 /33 that were seen in DM was overlapping parenchyma and only 17 cases as asymmetry (1 benign and 16 malignant).
At our study, regarding breast lesions mammography detected 39/90 (43%) mass lesions out of them 21/39 (53.8%) and benign lesions 18/39 (46%) malignant lesions on DBT detected 57/90 (63.3%) mass lesions, out of which 28/57 (49.1%) were benign and 29/57 (50.8%) were malignant. Caumo et al. [16] comparing role of DBT and DM in cancer detection. Using 2DM alone detected 39/7294 cancers while adding DBT to the 2DM detected 59/7294 cancers. Mansour et al. [17] DBT revealed better lesions characterization and categorize masses were benign or malignant.
Regarding the parenchymal distortion, we detected better assessment by DBT compared to DM as DM detect only 10/90 (11.1%) cases while DBT detected parenchymal distortion in 27/90 (30%), DBT was of added value as it detected 17 distortions not seen by DM. as Skaane P [18]. study proved that DBT improve the detection of subtle architectural distortion especially in women with dense breasts.
Also as breast asymmetry DM detected 33/90 (36.6%) cases out of which 1/33(3%) were diffuse asymmetries, 5/33 (15%) developing asymmetry and 27/33(81%) were focal asymmetries. In DBT it verified the asymmetry in 17/90 (18.8%), 10/17 (58.8%) as malignant mass lesions and 7/17 (41.2%) as benign mass lesion. Sixteen of lesions (16/33) 48% were simply overlapping tissues and avoided unnecessary biopsy. Poplack SP etal. [19] they concluded that DBT has the potential to decrease the recall rate by 40% (37/92) when used adjunctively with digital screening mammography.
At our study, adding DBT to a conventional mammography substantially increases sensitivity for multifocal/multicentric disease from 6.2 to 34.3% (p = 0.02). Bian Tet al [20] showed higher overall detection rates using DBT compared to mammography in a study population of 631 breasts assessing benign as well as malignant lesions.
At our study, regarding calcifications by DM showed 31/90(34.4%) patients had calcification, 13/31(42%) lesions were benign calcification, 18/31(58%) lesions were malignant calcifications. While DBT showed 34/90(37.7%) patients had calcification, 13/34(38%) lesions were benign calcification, 21/37(62%) lesions were malignant calcifications. Kopans D et al. [21] after comparison the study found that DBT may display calcifications equal or even slight greater as mammography. DBT didn't add significant value to the detection nor characterization of calcification.
The diagnostic accuracy of DM and DBT in characterization of breast lesions and diagnosis of breast cancer as a regard of pathology results as a gold standard, DBT had a sensitivity of 98%, a specificity of 87%, PPV of 88%, NPV of 98% and accuracy 92%. On the other hand, DM had a sensitivity of 58%, a specificity of 80%, PPV of 74%, NPV of 65% and accuracy 69%. Mansour S [16], The sensitivity, specificity, and accuracy of DM was 60%, 20.7% and 48% respectively have significantly enhanced on applying DBT to be 94.5%, 74% and 89.7% respectively. These results are comparable to those reported by other previous studies: Tamaki K [22], Waldherr C [23], Bernardi D [24] & Hassan RM [25].
Hakim CM et al. [10] the study looked at 25 women's mammograms and wrote masses finding twice: once with the use of the extra views and once with the help of DBT and their BI-RADS. They discovered that in 50% of cases, DM and DBT (used together) were thought to be better for diagnosis. DBT showed better lesion BIRADS classification and significantly decreased the number of indeterminate/suspicious lesions, (BIRADS 3, 4). DBT changed the identified BIRADS category. It upgraded 10/31 lesions and downgraded 8/31 lesions.
In our study, after comparing DM versus DBT BIRADS scoring and different BIRADS for 40 cases (24 were upgraded and 16 were downgraded). The upgraded lesions 60% (24/40) were classified as follows, 70% (17/ 24) upgraded to BI-RADS 4 and 30% (7/24) upgraded to BI-RADS 5. Twenty-three of upgraded lesions were malignant and one was benign. The downgraded lesions 40% (16/40) more evident in lesion scored with BI-RADS 3 by 25% (10/40). All downgraded lesions were benign, this result in reduced follow-up of lesions that would not have been identified by DM alone and diminished the requirement for biopsy. Andersson I [26], Comparing one-view DM to one-view BT, 21 patients were upgraded on BIRADS classification (p < 0.01). Comparing two-view DM to one-view BT, 12 patients were upgraded on BIRADS classification (p < 0.01). The results indicate that the cancer visibility on DBT is superior to DM, which suggests that DBT may have a higher sensitivity for breast cancer detection.
Nakashima Kazuaki, [27] the misdiagnosed lesions on DBT were less than that on DM (67 false-positives and 49 false-negatives). The combined DM and DBT decreased misdiagnosed lesions (seven false-positives and two false-negatives) when compared to DM or DBT alone. At our study revealed twenty-eight of the breast lesions in this study were misdiagnosed on DM (9 false-positives and 19 false negatives). However, the misdiagnosed lesions on DBT were less than that on DM (6 false-positives and 1 false-negative).
Limits of the study was small sample size especially at females with ACR D, so further larger study for females with ACR D is recommended.
Conclusions
Digital breast tomosynthesis has a significant impact on the BI-RADS classification as it effectively visualizes overlapping tissue in dense breasts especially in breast lesion BIRAD 3 & 4, along with decreasing recall rates for false-positive results.
Availability of data and materials
Data remains available when needed by the editorial board.
Abbreviations
- 3D:
-
Three-dimensional
- CBS:
-
Conservative breast surgery
- CC:
-
Craniocaudal
- CESM:
-
Contrast-enhanced spectral mammogram
- DBT:
-
Digital breast tomosynthesis
- DM:
-
Digital mammography
- MLO:
-
Mediolateral oblique
- WLE:
-
Wide local excision
References
Basha MAA, Safwat HK, Alaa Eldin AM, Dawoud HA, Hassanin AM (2020) The added value of digital breast tomosynthesis in improving diagnostic performance of BI-RADS categorization of mammographically indeterminate breast lesions. Insights Imaging 11:26
Henderson KD, Sullivan-Halley J, Reynolds P, Horn-Ross PL, Clarke CA, Chang ET et al (2008) Incomplete pregnancy is not associated with breast cancer risk: the California Teachers Study. Contraception 77:391–396
Zeeneldin AA, Ramadan M, Gaber AA, Taha FM (2013) Clinico-pathological features of breast carcinoma in elderly Egyptian patients: a comparison with the non-elderly using population-based data. J Egypt Natl Canc Inst 25:5–11
Yaghjyan L, Colditz GA, Rosner B, Tamimi RM (2013) Mammographic breast density and subsequent risk of breast cancer in postmenopausal women according to the time since the mammogram. Cancer Epidemiol Biomarkers Prev 22:1110–1117
Bertrand KA, Tamimi RM, Scott CG, Jensen MR, Pankratz V, Visscher D et al (2013) Mammographic density and risk of breast cancer by age and tumor characteristics. Breast Cancer Res 15:R104
Fallenberg EM, Dromain C, Diekmann F, Engelken F, Krohn M, Singh JM et al (2014) Contrast-enhanced spectral mammography versus MRI: Initial results in the detection of breast cancer and assessment of tumour size. Eur Radiol 24:256–264
Kim S, Lee Y, Koo JS (2015) Differential expression of lipid metabolism-related proteins in different breast cancer subtypes. PLoS ONE 10:e0119473
Partyka L, Lourenco AP, Mainiero MB (2014) Detection of mammographically occult architectural distortion on digital breast tomosynthesis screening: initial clinical experience. AJR Am J Roentgenol 203:216–222
Sechopoulos I (2013) A review of breast tomosynthesis: part I: the image acquisition process. Med Phys 40:014301
Hakim CM, Chough DM, Ganott MA, Sumkin JH, Zuley ML, Gur D (2010) Digital breast tomosynthesis in the diagnostic environment: a subjective side-by-side review. AJR Am J Roentgenol 195:W172–W176
Gur D (2007) Tomosynthesis: potential clinical role in breast imaging. AJR Am J Roentgenol 189:614–615
Park JM, Franken EA Jr, Garg M, Fajardo LL, Niklason LT (2007) Breast tomosynthesis: present considerations and future applications. Radiographics 27(Suppl 1):S231–S240
van der Hage JA, van de Velde CJ, Julien JP, Tubiana-Hulin M, Vandervelden C, Duchateau L (2001) Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902. J Clin Oncol 19:4224–4237
Weigel S, Heindel W, Hense HW et al (2023) Breast density and breast cancer screening with digital breast tomosynthesis: a TOSYMA trial subanalysis. Radiology 306(2):e221006. https://doi.org/10.1148/radiol.221006
Radiology ACo, D'Orsi CJ, Sickles EA, Mendelson EB, Morris EA (2013) ACR BI-RADS Atlas: breast imaging reporting and data system; mammography, ultrasound, magnetic resonance imaging, follow-up and outcome monitoring, data dictionary: ACR, American College of Radiology
Caumo F, Romanucci G, Hunter K, Zorzi M, Brunelli S, Macaskill P et al (2018) Comparison of breast cancers detected in the Verona screening program following transition to digital breast tomosynthesis screening with cancers detected at digital mammography screening. Breast Cancer Res Treat 170:391–397
Mansour S, Adel L, Mokhtar O, Omar OS (2014) Comparative study between breast tomosynthesis and classic digital mammography in the evaluation of different breast lesions. Egypt J Radiol Nuclear Med 45:1053–1061
Skaane P (2012) Tomosynthesis in X-ray: proven additional value? Eur J Radiol 81(Suppl 1):S156–S157
Poplack SP, Tosteson TD, Kogel CA, Nagy HM (2007) Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screening mammography. AJR Am J Roentgenol 189:616–623
Bian T, Lin Q, Cui C, Li L, Qi C, Fei J et al (2016) Digital breast tomosynthesis: a new diagnostic method for mass-like lesions in dense breasts. Breast J 22:535–540
Kopans D, Gavenonis S, Halpern E, Moore R (2011) Calcifications in the breast and digital breast tomosynthesis. Breast J 17:638–644
Tamaki K, Tamaki N, Terukina S, Kamada Y, Uehara K, Arakaki M et al (2014) The correlation between body mass index and breast cancer risk or estrogen receptor status in Okinawan women. Tohoku J Exp Med 234:169–174
Waldherr C, Cerny P, Altermatt HJ, Berclaz G, Ciriolo M, Buser K et al (2013) Value of one-view breast tomosynthesis versus two-view mammography in diagnostic workup of women with clinical signs and symptoms and in women recalled from screening. AJR Am J Roentgenol 200:226–231
Bernardi D, Ciatto S, Pellegrini M, Tuttobene P, Fanto C, Valentini M et al (2012) Prospective study of breast tomosynthesis as a triage to assessment in screening. Breast Cancer Res Treat 133:267–271
Hassan RM, Almalki YE, Basha MAA, Alduraibi SK, Aboualkheir M, Almushayti ZA, Aldhilan AS, Aly SA, Alshamy AA (2023) the impact of adding digital breast tomosynthesis to BI-RADS categorization of mammographically equivocal breast lesions. Diagnostics (Basel) 13(8):1423. https://doi.org/10.3390/diagnostics13081423
Andersson I, Ikeda DM, Zackrisson S, Ruschin M, Svahn T, Timberg P et al (2008) Breast tomosynthesis and digital mammography: a comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur Radiol 18:2817–2825
Nakashima K, Uematsu T, Itoh T, Takahashi K, Nishimura S, Hayashi T et al (2017) Comparison of visibility of circumscribed masses on Digital Breast Tomosynthesis (DBT) and 2D mammography: are circumscribed masses better visualized and assured of being benign on DBT? Eur Radiol 27:570–577
Acknowledgements
Not applicable.
Funding
This research did not receive any funding.
Author information
Authors and Affiliations
Contributions
The research was planned and designed by WA and MR. GA The writers made equal contributions as regards data collection and analysis. The manuscript was authored by WA and MR, TR. The statistical analysis was conducted by WA, GT, MR and SA. The article has been reviewed and endorsed by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We commenced this research following the Faculty of Medicine Helwan University, Research Ethics Committee’s approval. All participants received a signed informed consent to analyze anonymized data.
Consent for publication
Not applicable.
Competing interests
The authors assert that they do not possess any conflicting interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Romeih, M., Raafat, T.A., Ahmed, G. et al. Value of digital breast tomosynthesis in characterization of breast lesions in dense breast. Egypt J Radiol Nucl Med 55, 131 (2024). https://doi.org/10.1186/s43055-024-01298-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01298-9