
Abstract
Background
Mammography is currently the modality of choice for mass screening of breast cancer, although its sensitivity is low in dense breasts. Besides, higher breast density has been identified as independent risk factor so it has been conceptualized that women with dense breasts should be encouraged for supplemental screening. In this study, we aimed to estimate the distribution of volumetric breast density using fully automated Volpara software and to analyze the level of agreement between volumetric density grades and Breast Imaging Reporting and Data System (BI-RADS) density grades. We also aim to estimate the distribution of breast cancer in different VDG and to find a correlation between VDG and risk of malignancy.
Results
VDG-c was most common followed by VDG-b and BIRADS grade B was commonest followed by grade C. The density distribution was found inversely related to the age. Level of agreement between VDG and BIRADS grades was moderate (κ = 0.5890). Statistically significant correlation was noted between VDG-c and d for risk of malignancy (p < 0.001).
Conclusion
Difficulties associated with the use of BI-RADS density categories may be avoided if assessed using a fully automated volumetric method. High VDG can be considered as independent risk factor for malignancy. Thus, awareness of a woman’s breast density might be useful in determining the frequency and imaging modality for screening.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Breast cancer is the most often encountered and the most dreaded of the various pathologies that affect the breast [1]. It is the most common cancer in Indian women [2]. During 2012–2016, breast cancer was the leading cause of death among women aged 20–49 [3, 4]. The risk factors for breast cancer in western populations have been extensively investigated and life style related factors and reproductive factors have been found to be strongly associated with breast cancer. However, in low risk populations, prevalence of these factors is low [5]. There is a constant search for other factors which may have a stronger association with an increased risk for developing breast cancer. Mammographic breast density (MBD) is one such factor, which needs more evaluation. Women with dense breasts have been found to be four to six times more likely to develop breast cancer than those with fatty breasts [6,7,8]. Extensive mammographic density may also make breast cancer more difficult to detect by mammography and thus increases the risk of the development of cancer between mammographic screening tests [9].
Breast density (BD) assessments performed using the Breast Imaging Reporting and Data System (BI-RADS) are based on subjective description, having suboptimal reproducibility [10]. Thus, several methods have been proposed for measuring mammographic density in a quantitative manner like manual planimetry and computer-assisted threshold method [11, 12]. However, limitations of these method are that the tissue thickness, radiation dose, projection angle and observer bias are not taken into account. Cumulus (University of Toronto, Canada) one of the most commonly used quantitative measurement software, estimated density based on two-dimensional mammographic images whereas BD is three-dimensional. So, this method has limited accuracy and is time consuming [13,14,15].
The fully-automated volumetric methods comprise Quantra v1.3 (Hologic, Bedford, MA, USA) which combines the information from both views to produce average estimates for each breast and Volpara v1.0 (Volpara Solutions, Matakina Technology Limited, Wellington, New Zealand), uses a relative physics model to calculate percentage of dense tissue within the breast [16, 17].
In present study, we aim-
-
1.
To estimate the distribution pattern of volumetric density grades (VDG).
-
2.
To analyze the level of agreement between VDG and BI-RADS density grades.
-
3.
To estimate the distribution of breast cancer in different VDG and to find an association between VDG and risk of malignancy.
Methods
Patient selection
This descriptive cross-sectional study was undertaken at the Breast Imaging Unit of Radiodiagnosis department of our institute between year 2019–20. This study was approved by Institution ethics committee. All women who had come for screening or diagnostic or surveillance mammography were included in the study provided they were not on Tamoxifen therapy. Pregnant or lactating women and those with large or bilateral masses were excluded as they could lead to false density computation. Thus, our study population was a hybrid of both symptomatic and disease‑free subjects. A total of 1228 women were the final sample set. Requirement for written informed consent was waived off by institute ethics committee as our study was retrospective in nature.
These patients underwent standard Digital Mammography (DM) in two views: the CC and MLO views and tomosynthesis in one view (MLO) using DM Unit (GE Healthcare Senographe Essential 54,020/CESM1/SenoClaireA.6). VBD measurements were done using fully automated software Volpara Density (Imaging software version 3.3.2, Volpara Algorithm version Number1.5.4.0, Wellington, New Zealand). Additional views were taken when required. Ultrasound was done when needed, on Supersonic AIXPLORER Multiwave Version 12.2.0808USG scanner.
Assessment of volumetric breast density (VBD)
VBD was automatically calculated in each case using Volpara software which works by using a model of the physics regarding digital mammography in order to work backwards from the pixel value in the image to the X-ray attenuation between the pixel and the X-ray source. It calculates the types of tissue that must have been present between the pixel and the X-ray source. Then, the volume of fibro glandular tissue and breast tissue in cubic centimeters, and their ratio are obtained to acquire quantitative VBD. The VDG is the VBD threshold at various levels, which can be used to obtain an approximate BI-RADS breast composition classification [18]. VBD of less than 3.5% is VDG a, 3.5–7.4% is VDG b, 7.5–15.5% is VDG c, and ≥ 15.5% to VDG d (Fig. 1).

Medio-lateral oblique views of mammograms of different patients showing volumetric density grades (VDG-A, B, C and D) with VOLPARA numerical breast density values
Qualitative BD grade was independently assigned by two radiologists (Radiologist 1 with 12 years of experience and Radiologist 2 with 5 years of experience) according to the BI-RADS 5th edition (2013) to A, B, C and D (A: the breast is almost entirely fatty, B: scattered areas of fibro glandular density, C: the breast is heterogeneously dense, and D: the breast is extremely dense) [19] (Fig. 2). Cases which showed discrepancy in BI-RADS categorization were reviewed by both the radiologists and based on mutual consensus final BI-RADS density category were assigned.

Medio-lateral oblique views of mammograms of different patients showing ACR BI-RADS categories (A, B, C and D) of breast density
Final BI-RADS assessment category was assigned to each case based on the clinical presentation, mammographic and ultrasound findings. 323 masses with suspicious morphology were identified and Trucut biopsy was performed. After pathological examination 193 cases came out to be malignant and constituted the “case” group. Women with no suspicious lesion on mammogram or ultrasound constituted the comparison or “control” group. Information about age, age at menarche, number of children, breastfeeding, strong family history and hormone replacement therapy were taken from our records and noted for women in both groups. Depending upon the age of menarche, data was recorded for presence or absence of early menarche in both groups, cut off being taken as ≤ 12 years. Similarly, based on the number of children data was recorded for presence or absence of Nulliparity in both the groups.
Statistical analysis
It was carried out on SPSS Version 21.0 statistical Analysis Software. The values were represented in number, percentage (%) and mean ± SD. Level of agreement between VDG and BI-RADS density grade was calculated by calculating weighted kappa. The kappa values were interpreted as follows: A kappa value less than 0 had less than chance agreement, between 0.001 and 0.20 indicated slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–0.99, almost perfect agreement. Chi-square test followed by post hoc test, i.e., Bonferroni correction was used to assess the association between VDG and breast malignancy with calculation of P values.
Results
Our study population had age range27-83 years, mean age 48.82 ± 10.94 years and most common age group was 41–60 years. VDG-c was most common (43.97%) pattern, followed by VDG-b (26.14%), VDG-d (24.9%) and VDG-a (4.96%). Distribution of BI-RADS density grades as determined by two radiologists independently and after mutual consensus is depicted in Table1. The inter‑observer agreement between two radiologists was substantial (Kappa value = 0.67).BI-RADS grade B (39.41%) was most common, followed by grade C (38.84%), D (15.14%) and A (6.59%). (Table 1, Fig. 3).

Bar chart shows comparison of the distribution of different volumetric density grades and BIRADS density grades in study population
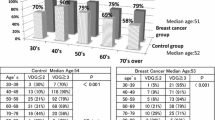
In below 40 age group (n = 42), VDG-b and d were commonest (33.33% each) followed by VDG-c (28.57%) and VDG-a (4.7%). In age group 41–50 years (n = 762), VDG-c and d were most common (47.76% and 29.13%, respectively) followed by VDG-b (19.42%) and VDG-a (3.67%). In 51–60 year group (n = 295), VDG-c (38.64%) and b (34.91%) were followed by VDG-d (21.69%) and VDG-a (4.74%). Only a small proportion of women 61–70 years, (n = 97) had VDG-d (4.1%), commonest being VDG-c (47.42%), followed by VDG-b and a (39.17% and 9.27%, respectively). In 71–80 year age group (n = 26), VDG-b was most common (61.53%) followed by VDG-a (19.23%), c (11.53%) and d (7.69%). There was no VDG-d breast in women above 80 years. (Table 2, Fig. 4).

Bar chart shows comparison of the distribution of normalcy and malignancy among different volumetric density grades (VDG) in study population
On assessing the agreement between VDG and ACR grades, similarity in grades was observed for 882 (71.8%) out of 1228 breasts. Level of agreement was found to be moderate with κ = 0.589 (Level of agreement; Moderate κ = 0.41–0.60). (Table 3).
On basis of Mammography and ultrasound findings final BI-RADS category was assigned to each patient. Out of 1228 women, 5% population fell in category 1, 50.16% in category 2 and 17.67% in category 3. Category 4, 5 and 6 were assigned to 18.07%, 8.2% and 0.81% of the subjects, respectively. Out of 61, VDG-a breasts, suspicious features (BIRADS 4, 5 and 6) were noted only in 9.8% population. Among 321 women with grade b, suspicious features were present in 16.3%. Similarly, BIRADS 4, 5 and 6 in VDG-c and d breasts were assigned to 30.85% and 35.6% of population. Thus, with increase in BD grades, increase in number of findings suspicious for malignancy was seen. (Table 4).
Biopsy was performed in a total of 323 suspicious masses (BIRADS 4 and 5) and 193 came out to be malignant. 104 cases (53.88%) of carcinoma breasts were from VDG-c and 57 from VDG-d (29.53%). Only 32 masses (2.6%) were from low density breasts (4 and 28 in VDG-a and b, respectively). Out of 61 breasts with VDG-a, malignancy was noted in 6.55%. Similarly, in VDG-b, c and d, malignancy was present in 8.72%, 19.25% and 18.62%, respectively (Fig. 5). Thus, with increase in BD grades, increase in number of malignant lesions was seen.

Bar chart shows age wise distribution of different volumetric density grades (VDG) in study population
To find out any association between different VDG and risk of malignancy, 193 cases and 247 controls were compared. All the aforementioned factors (age, age at menarche, number of children, breastfeeding, strong family history and hormone replacement therapy) were comparable in cases and controls (Table 5).
There was statistically significant difference between the VDG grades for risk of malignancy among cases and controls, as determined by Chi-square test (p value < 0.001) (Table 6) After applying Bonferroni correction, we found that VDG-a &b (p value = 0.212) and VDG-c & d (p value = 0.278) groups did not have any significant difference between them. However, VDG-a and VDG-b when individually compared to VDG-c (p value < 0.001) and VDG-d (p value < 0.001) showed significantly higher normal population. VDG-c and d when compared to VDG-a and b showed significantly higher number of malignancy (p value < 0.01 for each). (Table 7).
Discussion
Breast cancer is the second leading cause of death in women. It has been well established that the sensitivity of mammography for diagnosis is inversely related to BD but here it is important to emphasize that the association between degree of BD and risk for breast cancer cannot be explained merely by a reduction in sensitivity [20]. High MBD is one of the strongest known risk factors, regardless of age, family history or ethnic background [21, 22]. A variety of qualitative and quantitative techniques have been excogitated for measuring MBD. BI-RADS classification system is the most commonly practiced method for the same [23]. However, this method is subjective and is influenced by many factors including over/underestimation tendency, bias due to defensive practice and reading room conditions [3]. Inter- and intra-reader variabilities are also noted to be considerable in published studies [17, 23]. To conquer this problem, a range of quantitative methods have been developed for BD measurement. The advantages of a quantitative BD evaluation include faster speed, increased efficiency and having a reliable, highly reproducible calculation to report. Apart from that, objective BD measurement can help develop individualized screening protocols (like more frequent screening, screening with USG and magnetic resonance imaging) and individual breast cancer risk prediction models.
Yaffe, in 2008 [15], described several quantitative techniques to measure BD subjectively or objectively. These include two-dimensional dense area measures, Hand Delineation and semi-automated thresholding technique with Image J [22]. Alternatively, fully automated methods include 3D measurements of dense areas, yielding an aggrandized compendious computation of the volume of dense breast tissue [20, 24]. Presently, there are a number of fully automated methods to measure BD quantitatively. One of these promising software is VOLPARA, which has received Food and Drug Administration and Therapeutic Goods Administration approval, as well as the CE mark for use in mammography practices [25,26,27]. In present study, we used the same software to calculate MBD.
The study population age ranged from 27 to 83 years, which is representative of the patients age group that attended our breast imaging unit. VBD assessment showed that VDG-c was most common pattern followed by VDG-b, VDG-d and VDG-a. Daniëlle van der Waal et al. [28] found 32.5–45.7% women with heterogeneously dense breasts in various regions in Netherlands using Volpara software. Förnvik et al. [29] used LIBRA software for BD measurements and found that majority of women had heterogeneously dense breasts (category-C in 68%). Data from the Breast Cancer Surveillance Consortium (BD estimation was done using age and BMI) showed that 43.3% of the US women are considered dense [30]. Our findings well correlated with the recently published study on Asian population [31]. Although the most common pattern seen in a study performed on Indian population was also VDG-c but next in sequence were a and b followed by d [32]. The density distribution according to age is as reported previously, with density categories inversely related to age, the reason being post-menopausal involution [33,34,35]. However, it is striking to note that within VDG-c and d groups in our study population, only 6.6% were age 60 and above. But in all the females above 60 years age (n = 129) about 46.6% had high VDG (c or d). Similarly, in below 40 women (n = 42), about 38% had VDG-a or b. Hence, generalizing lower BD to higher age and vice versa, which is not always true, may lead to erroneous presumptive BD assessment. In such cases, Volpara will be advantageous in comparison to visual assessment, as age is not factored in Volpara density assessment.
The BI-RADS density categories assigned by two radiologists had shown substantial (κ = 0.67) inter-observer agreement between two radiologists. In our study, grade B density (39.41%) was most common followed by grade C (38.84%) and grade D (15.14%). It was in accordance with the recently published study on Asian population [31]. The other study performed in Indian population had also shown that grade B was commonest but next common was grade A [36]. Our data shows that most of the elderly females had low BD, i.e., grade A or B. Unexpectedly, a considerable percentage of younger women (< 40 years) were classified with either grade A or B density and elderly women (> 60 years) with grade C or D.
Our study show a moderate level of agreement between VDG and BI-RADS grade (κ value 0.41–0.60) (p < 0.001). This is consistent with the findings by Gweon et al. [12] and Seo et al. [37] that had shown moderate to significant level of agreement between the two. Tagliafico et al. [38] presented with similar findings and demonstrated that the use of the fully automated software eliminated intra- and inter-observer differences and correlated with ACR BI-RADS categories (r¼ 0.62, p < 0.01). We also observed that in general VDG scores were higher than BI-RADS scores. For instance 156 BI-RADS B categories were classified as VDG-c and 31 BI-RADSB categories were classified as VDG-d, while 96 of BI-RADSC categories were classified as VDG-d. This is in agreement to what has been observed by Gubern-Mérida et al. [39] who saw a similar trend of Volpara scoring higher than BI-RADS category.
In our study, occurrence of malignancy was significantly higher in VDG-c and d (p value < 0.01 each) as compared to VDG- a and b. However, we did not find any statistically significant difference between VDG-c and d (p value = 0.29) for risk of cancer. Our results are in accordance with previous study by Singh et al. [40] which showed statistically significant increased risk of developing carcinoma in high-density breasts (VDG-c + VDG-d) as compared with low-density breasts (VDG-a + VDG-b) in both premenopausal and postmenopausal subgroups. Study by Koshi et al. [41] showed similar results in premenopausal women but they did not found such association in post-menopausal women. In our study, we did not divide patients in pre and post-menopausal groups and so did not compare them. Duffy et al. [42] measured BD using Volpara software in the TOMMY trial and found that increased levels of density are associated with increased risk of breast cancer similar to ours. Puliti et al. [43] also saw that breast cancer incidence gradually increased with the increase in VBD: 3.7%, 5.1%, 5.4% and 9.1% in the VDG categories 1–4, respectively (p trend < 0.001) with the highest number of cancers in category 4; consistent with our results. Boyd et al. [6] reported similar results using BI-RADS assessment, with higher malignancy being detected in breasts with density > 75%. The major limitation of our study was that study subjects were a hybrid of screening and diagnostic population which is not the ideal condition for risk estimation. To overcome this issue, we took out a subset of population and constituted ‘case’ group and ‘control’ group for cancer risk estimation. Our findings just add to the existing literature of BD serving as a risk factor of breast cancer. The role of ACR- BI-RADS density in breast cancer has been established; however, our study shows that even VBD can be a useful predictor of malignancy.
While comparing the correlation of Volpara based VDG with benign vs. malignant lesions, no statistical significance was found, thus indicating that BD, while being a good individual predictor of breast cancer, cannot be used to distinguish the development of benign or malignant lesions.
Conclusion
We have demonstrated that the difficulties associated with the use of BI-RADS density categories, such as moderate to substantial inter-observer variability and broad ranges in the same category, may be avoided when mammographic density is being assessed using a fully automated volumetric method with digital mammography. We also demonstrated that high VDG is associated with high rate of malignancy. However, BD does not pick out all women who will develop breast cancer, because many cancers were found in low density breasts. Thus, awareness of a woman’s BD might be useful in determining the frequency and imaging modality for screening.
Availability of data and materials
The datasets used during the current study can be made available from the corresponding author on reasonable request.
Abbreviations
- VBD:
-
Volumetric breast density
- VDG:
-
Volumetric density grades
- BD:
-
Breast density
- ACR-BIRADS:
-
American college of radiology breast imaging reporting and data system
- k:
-
Kappa
- CC:
-
Cranio-caudal
- MLO:
-
Medio-lateral oblique
- DM:
-
Digital mammography
References
Tiwari PK, Ghosh S, Agrawal VK (2017) Diagnostic accuracy of mammography and ultrasonography in assessment of breast cancer. Int J Contemp Med Res 4:81–83
Cancer statistics. India against cancer. [Cited 2020 Jan 5]. Available from: http://cancerindia.org.in/cancer-statistics/
Brown AL, Phillips J, Slanetz PJ et al (2017) Clinical value of mammography in the evaluation of palpable breast lumps in women 30 years old and older. Am J Roentgenol 209:935–942
Annual report to the nation 2019: special topic: cancer among adults ages 20–49. SEER. [Cited 2020 Feb 9]. Available from: https://seer.cancer.gov/report_to_nation/special.html
Rao D, Ganesh B, Desai P (1994) Role of reproductive factors in breast cancer in a low-risk area: a case–control study. Br J Cancer 70:129–132
Boyd NF, Lockwood GA, Byng JW et al (1998) Mammographic densities and breast cancer risk. Cancer Epidemiol Prev Biomark 7:1133–1144
Boyd NF, Jensen HM, Cooke G et al (1992) Relationship between mammographic and histological risk factors for breast cancer. JNCI J Natl Cancer Inst 84:1170–1179
Ursin G, Ma H, Wu AH et al (2003) Mammographic density and breast cancer in three ethnic groups. Cancer Epidemiol Prev Biomark 12:332–338
Mammographic parenchymal patterns and mode of detection: implications for the breast screening programme, 1998. [Cited 2020 Jan 9]. Available from: https://journals.sagepub.com/doi/abs/https://doi.org/10.1136/jms.5.4.207
Rao AA, Feneis J, Lalonde C et al. (2016) A Pictorial Review of Changes in the BI-RADS Fifth Edition. Radio Graphics 36: 623–639
Wolfe JN, Saftlas AF, Salane M (1987) Mammographic parenchymal patterns and quantitative evaluation of mammographic densities: a caseecontrol study. Am J Roentgenol 148:1087–1092
Gweon HM, Youk JH, Kim JA et al (2013) Radiologist assessment of breast density by BI-RADS categories versus fully automated volumetric assessment. Am J Roentgenology 201:692–697
Byng JW, Boyd NF, Fishell E et al (1994) The quantitative analysis of mammographic densities. Phys Med Biol 39:1629–1638
Eng A, Gallant Z, Shepherd J et al (2014) Digital mammographic density and breast cancer risk: a case-control study of six alternative density assessment methods. Breast Cancer Res 16:439
Yaffe MJ (2008) Mammographic density. Measurement of mammographic density. Breast Cancer Res 10:209
Highnam R, Brady SM, Yaffe MJ, Karssemeijer N, Harvey J (2010) Robust breast composition measurement - VolparaTM . In: Martí J, Oliver A, Freixenet J, Martí R (eds) Digital mammography. IWDM 2010. Lecture Notes in Computer Science, vol 6136. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-13666-5_46
Ciatto S, Bernardi D, Calabrese M et al (2012) A first evaluation of breast radiological density assessment by QUANTRA software as compared to visual classification. Breast 21:503–506
DeAngelis CD, Fontanarosa PB (2010) US preventive services task force and breast cancer screening. JAMA 303:172–173
D’Orsi CJ, Sickles EA, Mendelson EB, Morris EA, et al (2013) ACR BI-RADS® Atlas, breast imaging reporting and data system. American College of Radiology, Reston, VA
Vachon CM, Gils CHV, Sellers TA et al (2007) Mammographic density, breast cancer risk and risk prediction. Breast Cancer Res 9:217
Santen RJ, Boyd NF, Chlebowski RT et al (2007) Critical assessment of new risk factors for breast cancer: considerations for development of an improved risk predictionmodel. EndocRelat Cancer 14:169–187
McCormack VA (2006) Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomark Prev 15:1159–1169
Kerlikowske K, Grady D, Barclay J et al (1998) Variability and accuracy in mammographic interpretation using the American college of radiology breast imaging reporting and data system. J Natl Cancer Inst 90:1801–1809
Shepherd JA, Kerlikowske K, Ma L et al (2011) Volume of mammographic density and risk of breast cancer. Cancer Epidemiol Biomark Prev 20:1473–1482
Alonzo-Proulx O, Mawdsley G, Patrie JT et al (2015) Reliability of automated breast density measurements. Radiology 275:366–376
Youk JH, Gweon HM, Son EJ et al (2016) Automated volumetric breast density measurements in the Era of the BI-RADS fifth edition: a comparison with visual assessment. Am J Roentgenol 206:1–7
Volpara solutions receives FDA clearance for Volpara density maps. Volpara Solutions. 2016
Van der Waal D, Emaus MJ, Bakker MF et al (2015) Geographic variation in volumetric breast density between screening regions in the Netherlands. Eur Radiol 25:3328–3337
Förnvik D, Kataoka M, Iima M et al (2018) The role of breast tomosynthesis in a predominantly dense breast population at a tertiary breast centre: breast density assessment and diagnostic performance in comparison with MRI. Eur Radiol 28:3194–3203
Sprague BL, Gangnon RE, Burt V et al (2014) Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst 106(10):dju255. https://doi.org/10.1093/jnci/dju255
Rahmat K, AbMumin N, Ramli Hamid MT et al (2020) Evaluation of automated volumetric breast densitysoftware in comparison with visual assessments in an Asian population: a retrospective observational study. Medicine 99:e22405
Singh T, Sharma M, Singla V et al (2016) Breast density estimation with fully automated volumetric method: comparison to radiologists’ assessment by BI-RADS categories. Acad Radiol 23:78–83
Carney PA, Miglioretti DL, Yankaskas BC et al (2003) Individual andcombined effects of age, breast density, and hormone replacementtherapy use on the accuracy of screening mammography. Ann Intern Med 138:168–175
Heller SL, Hudson S, Wilkinson LS (2015) Breast density across a regionalscreening population: effects of age, ethnicity and deprivation. Br J Radiol 88:20150242
Kopans D (2007) Breast Anatomy and Basic Histology, Physiology, and Pathology. In: Kopans DB Breast Imaging. 3rd Edition. Philadelphia: Lippincott Williams and Williams, pp 7–43
Singh T, Khandelwal N, Singla V et al (2018) Breast density in screening mammography in Indian population-is it different from western population? Breast J 24:365–368
Seo JM, Ko ES, Han B-K et al (2013) Automated volumetric breast density estimation: a comparison with visual assessment. Clin Radiol 68:690–695
Tagliafico A, Tagliafico G, Tosto S et al (2009) Mammographic density estimation: comparison among BI-RADS categories, a semi-automated software and a fully automated one. Breast 18:35–40
Gubern-Mérida A, Kallenberg M, Platel B et al (2014) Volumetric breast density estimation from full-field digital mammograms: a validation study. PLoS ONE 9:e85952
Singh N, Joshi P, Gupta A et al (2022) Evaluation of volumetric breast density as a risk factor for breast carcinoma in pre- and postmenopausal women, its association with hormone receptor status and breast carcinoma subtypes defined by histology and tumor markers. Egypt J Radiol Nucl Med 53:84
Koshi S, Singla V, Singh T et al (2020) Mammographic breast density and breast cancer risk: evaluation using volumetric breast density software. J Can Res Ther 16:1258–1264
Duffy SW, Morrish OWE, Allgood PC et al (2018) Mammographic density and breast cancer risk in breast screening assessment cases and women with a family history of breast cancer. Eur J Cancer 88:48–56
Puliti D, Zappa M, Giorgi Rossi P et al (2018) Volumetric breast density and risk of advanced cancers after a negative screening episode: a cohort study. Breast Cancer Res 20:95
Acknowledgements
We thank Mrs. Suchita Rai, our Mammography Technologist for her dedication and tireless efforts to get excellent quality Mammograms for patients’ and our benefit.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
NS: conceptualization and manuscript writing, PJ: data collection and image formation, DS: helped in manuscript writing and proof reading of the manuscript, SN: helped in manuscript writing, AG: data collection and helped in manuscript writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval granted by Dr Ram Manohar Lohia Institute of Medical sciences Lucknow Institute ethics committee, IEC no- 06/22. Requirement of consent to participate was waived off by the Institute Ethics Committee.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Singh, N., Joshi, P., Singh, D.K. et al. Volumetric breast density evaluation using fully automated Volpara software, its comparison with BIRADS density types and correlation with the risk of malignancy. Egypt J Radiol Nucl Med 53, 118 (2022). https://doi.org/10.1186/s43055-022-00796-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00796-y