
Abstract
Background
It has long been established that obesity plays a positive role against osteoporosis (OP) and low-impact fractures (Fx). However, more recent data has shown higher fracture risk in obese individuals. The aim of this study was to investigate the association between BMI, particularly obesity, OP and low-impact Fx in Brazilian women, as well as to evaluate the SAPORI (Sao Paulo Osteoporosis Risk Index) tool performance to identify low BMD according BMI category.
Methods
A total of 6182 women aged over 40 years were included in this cross-sectional analysis using data from two large Brazilian studies. All participants performed hip and spine bone mineral density (BMD) measurements and answered a detailed questionnaire about the presence of clinical risk factors (CRFs) related to low BMD and risk fractures. The World Health Organization (WHO) criteria were used to define obesity.
Results
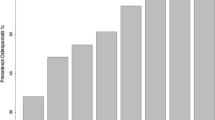
Age-adjusted osteoporosis prevalence was 20.8, 33.6, 47 and 67.1% in obese, overweight, normal and underweight category, respectively. Obesity was present in 29,6% (1.830 women) in the study population and the likelihood of osteoporosis and low-impact Fx compared to a normal BMI in this subgroup was of 0.24 (95% CI 0.20–0.28; p < 0.001) and of 1.68 (95% CI 1.35–2.11; p < 0.001), respectively. However, the hip Fx likelihood was lower in obese compared with non-obese women (OR = 0.44; 95% CI 0.20–0.97). Using an originally validated cut-off, the SAPORI tool sensitivity was significantly hampered in overweight and obese women although the accuracy had remained suitable because of increasing in specificity.
Conclusions
The osteoporosis prevalence reduced as BMI increased and obesity was associated with low-impact Fx, regardless of the BMD measurements. Moreover, the SAPORI performance was impaired in obese women.
Similar content being viewed by others

Background
Obesity and osteoporosis (OP) are two major public health problems with increasing prevalence worldwide and high impact on morbidity and mortality [1,2,3]. Osteoporosis is a silent metabolic bone disease characterized by bone loss and microarchitectural deterioration and higher susceptibility to fragility fracture. It has a relevant global burden, including almost 9,000,000 new osteoporotic fractures worldwide, as well as disability, quality of life impaired and death [1, 4]. The World Health Organization (WHO) defines obesity when the body mass index (BMI) is higher than 30 kg/ m2, with an abnormal or excessive fat accumulation and higher cardiovascular and metabolic risk [5].
According to the Brazilian Institute of Statistics and Geography over than 50% of population has been considered as overweight or obese, especially after 50 years [6]. Brazilian epidemiological studies also showed that the prevalence of osteoporosis and low-impact fractures is high [7,8,9,10,11].
BMI is an important aspect related to bone mineral density (BMD) measurements. Until recently, individuals with high BMI had some protection against fractures [12]. However, more recently epidemiological studies have shown that osteoporosis and obesity may coexist and could share complex pathophysiological mechanisms, including genetic, environmental, and hormonal factors [12, 13].
The relationship between the BMI and the fracture risk is inverse and non-linear. Patients with BMI below 20 kg/ m2 have higher risk and it is associated with low spine and hip BMD measurements. Nonetheless, only small decreases of fracture risk have been reported in individuals with BMI above 25 kg/ m2 [14]. In addition, it has been hypothesized that obese individuals have inappropriately lower BMD than expected for their body weight, increasing the fracture risk [15,16,17].
Risk factors for fracture in obese individuals appear to be similar to those in non-obese populations, except some different patterns of falling [18, 19]. Several tools have been developed to estimate the individual risk of osteoporotic fracture [20, 21]. The SAPORI (Sao Paulo Osteoporosis Risk Index) is a Brazilian validated tool for identifying women at higher risk for low bone mineral density and osteoporotic fractures to recommend some BMD measurements. [22].
The aim of this study was to investigate the BMI relationship, particularly obesity, with OP and low-impact Fx in women aged over 40 years, as well as to evaluate the SAPORI performance in predicting low BMD, according to each BMI category.
Methods
Two largest Brazilian epidemiological databases were used for this particular analysis: São Paulo Osteoporosis Study (SAPOS) and Sao Paulo Osteoporosis Risk Index (SAPORI). The first one was a population-based epidemiologic study for the assessment of risk factors for low-impact fractures and low spine or hip BMD (T-score ≤ − 2 SD) in 7533 women aged over 40 years from São Paulo, Brazil. Briefly, a total of 4332 fulfilled the eligibility criteria and a detailed questionnaire addressing clinical risk factors (CRFs) for OP and Fx, including demographic and anthropometrical data; gynecological and hormonal information; personal medical history; previous fractures; family history of femur fracture (FHHF) after 50 years of age in first-degree relatives; and details about current lifestyle habits (smoking, regular physical activity in the previous 12 months and regular intake of dairy products) [7]. Regular physical activity was defined as any physical activity performed for more than 30 min and during three or more times per week, excluding routine activities of daily living. Low-impact fracture was defined as caused by a fall from one’s own height or lower after 50 years of age. The information regarding these fractures was self-reported by the individuals [7, 22], including spine, hip and other non-vertebral fractures (humerus, distal forearm, ankle, pelvis, hands and feet). The categorization of dairy products daily intake was based on a frequency distribution of 200 mL (no serving, up to three servings, and three servings or more). All of them performed spine and hip BMD measurements by DXA (DPX NT, GE-Lunar). The height (cm) and weight (kg) were measured with the subject wearing light clothes and no shoes [7].
The second one (SAPORI) was a study that aimed to validate a new tool to identify women under risk of low BMD using variables that were associated with higher risk for OP and Fx in the previous SAPOS study: age, weight, previous fracture, white color, current smoking, physical activity and family history of hip fracture. The SAPORI tool was subsequently validated in a second cohort of 1915 women from the metropolitan area of São Paulo. In both cohorts, the protocol for BMD measurements was the same and the sampling was considered representative of the Brazilian female population older than 40 years old, based on Brazilian Institute of Statistics and Geography (IBGE) [7, 22, 23]. Thus, the SAPORI tool had suitable performance to identify women with low bone mineral density (spine and hip) and low-impact fracture, with an area under the receiving operator curve (ROC) of 0.831, 0.724, and 0.689, respectively. The index or final score was obtained through simple mathematic equations. For instance, body weight contributes to 0.04 for each increase 1 SD hip BMD. Thus, the body weight is divided by 10 and then multiplied by 4. If the woman has already had any fracture, this simple risk factor contributes with 0.48 or 5 points for each 1 SD reduction. The other risk factors are counted in this way, according to the relevance of each one of them in the final regression model. Also, when the final value is greater or equal to zero it is considered as recommended screening for low bone mineral density [7, 22].
For this study, 65 patients (1%) were excluded because missing data totalizing 6.182 women. The BMI category was defined according to the WHO classification: underweight (BMI ≤ 18.5 kg/ m2), normal weight (BMI 18.5–24.9 kg/ m2), overweight (BMI 25–29.9 kg/ m2), obesity (BMI ≥ 30 kg/ m2) [24, 25]. Also, according to the WHO classification, osteoporosis was defined when T-score (lumbar spine and/or total hip) below − 2.5 standard-deviation (SD) and osteopenia if T-score between − 1.01 and − 2.49 SD [26]. T-scores were used for all population (women aged > 40 years), following the guidelines of the Brazilian Society of Clinical Densitometry (ABRASSO) [27].
The Research Ethics Committee of the Universidade Federal de São Paulo/ Escola Paulista de Medicina approved this study (CEP- 0406/2015).
Statistical analysis
Categorical data were shown as frequency and percentages and were compared using Chi-squared or Fisher’s exact test as appropriate. Continuous data were reported as mean ± SD. Logistic regression models were used to evaluate independent predictors of low-impact Fx and osteoporosis, separately. Variables that showed some correlation (P value < 0.1, by the Chi-squared test) were entered into a forward/backward selection procedure (both with P value thresholds lesser than 0.05 to entry and retention). Variables included in the final multivariable model were: age, skin color, current smoking and physical activity, FHHF, menopausal status, hormone replacement therapy (HRT) in the last 12 months and diabetes mellitus. In this case, two final models were tested using the BMI as continuous or by WHO categories. The SAPORI tool discriminative power (accuracy) was assessed by the area under receiver-operating characteristics (ROC) curve and performed in each BMI category, separately. P value < 0.05 was set as significant. Statistical analyses were performed using SPSS (version 20.0, Chicago, USA) and R software package (version 3.2, Vienna, Austria).
Results
Population
A total of 6182 women were included in this analysis. The mean age was 60.7 ± 9.8 years, with White (76.8%) and postmenopausal (92.1%) predominance, although only 11.7% on HRT. The obesity prevalence was almost 30% (mean BMI = 34 ± 3.8 kg/m2) and only 1.2% was underweight (Table 1).
BMI and osteoporosis
The OP prevalence was 20.8, 33.6, 47 and 67.1% in obese, overweight, normal and underweight BMI category, respectively (Table 2). After adjustments for the CRFs, the higher BMI had a protective role for OP (OR = 0.89; 95%CI 0.88–0.90; p < 0.01). In obese women, the likelihood for OP was lower (OR = 0.26; 95%CI 0.23–0.31; p < 0.01) than in underweight women (OR = 2.43; 95%CI 1.35–4.61; p < 0.01), if compared to normal weight group (Fig. 1).

Multivariable logistic regression analysis for independent predictors of low-impact fractures. OR: Odds Ratio; 95% CI: 95% confidence interval; BMI: body mass index; HRT: hormone replacement therapy; FHHF: familial history of hip fracture
BMI and low-impact fracture
Low-impact fractures were self-reported by 756 women (12.2%), but there was no significant difference was observed regarding each BMI category (p = 0.81). On the other hand, there was a significant difference when the skeletal site was analyzed (p = 0.009; Fig. 2). Non-vertebral fractures were the most prevalent (distal forearm: 24.9%, metatarsus: 24.5%), followed by spine (7%) and hip (6.1%). In underweight women, there was significantly higher frequency of humerus and clavicle and the hip fracture was less common in obese women than non-obese group (7.4% vs. 3.4%; p = 0.047). Interestingly, obese and women with low-impact Fx had higher proportion of normal BMD than those with normal BMI (7.8% vs. 3.6%; p < 0.001; Fig. 3).

Low-impact fractures rate according site of fracture and BMI category

Low-impact fractures rate according the densitometric diagnosis and BMI category
After several adjustments for CRFs and BMD measurements (T-score values), it was observed that increasing BMI, the fracture risk also rises (OR = 1.03; 95%CI 1.02–1.05; p < 0.001), regardless each BMI category. This finding highlights that obese individuals had higher fracture risk than other BMI category, regardless BMD measurements. In addition, age (OR = 1.03; 95%CI 1.02–1.04; p < 0.001) and FHHF (OR = 4.18; 95%CI 3.46–5.06; p < 0.001) had high predictive power for low-impact Fx. Nonetheless, higher BMD values (OR = 0.58; 95%CI 0.53–0.63; p < 0.001) and premenopausal status (OR = 0.40; 95%CI 0.21–0.78; p < 0.007) played a positive role against low-impact fracture (Table 3). In addition, diabetes mellitus had a tendency to be associated with low-impact Fx (p = 0.06).
SAPORI tool performance
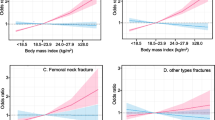
Using an originally validated cut-off (greater or equal zero) for each BMI category, the SAPORI tool performance had sensitivity hampered in overweight and obese women (Fig. 4). However, the accuracy remained suitable, due to increase of specificity (AUC ROC above 0.7 in all BMI categories) (Fig. 5).

The SAPORI tool sensibility and specificity changes according BMI category. BMI: body mass index

SAPORI accuracy for low BMD and low-impact fractures according BMI. ROC curves of the SAPORI tool for low BMD (femur or spine) and low-impact fractures according BMI category. BMD: bone mineral density; BMI: body mass index; ROC: Receiver-operating characteristic
Discussion
Our data showed that BMI played a relevant role on the prevalence of osteoporosis and caused impairment of SAPORI tool performance. On the other hand, it did not affect the prevalence of fragility fractures, suggesting that obese women are at risk for having low-impact fractures, regardless BMD measurements.
Previous studies have shown a significant relationship between BMD measurements and BMI, where higher BMI increases BMD and losing weight reduces BMD measurements values [14, 17, 28]. Although there are some patients with osteoporosis, there are a significant number of low-impact fractures in our obese women group, as reported by recent meta-analysis [29]. These new findings are a paradigm break concerning the widespread belief that obesity is protective against fractures. However, it is worthy emphasizing that high BMI has a different influence on fracture risk according to skeletal site [30, 31]. Thus, the obesity becomes a risk factor for all low-impact non-vertebral fractures, except hip fractures [18, 32]. Another thing to be considered is higher ankle and humerus fracture risk in obese women observed by the Global Longitudinal Study of Osteoporosis [18] and a Spain based-population study [31], respectively. Regarding vertebral fractures, there are conflicting data [33,34,35,36].
Several mechanisms may be involved on fracture risk in obese individuals, including site-specific BMI effects, as well as falls, reduced physical mobility, muscular weakness and postural instability. Obesity may predispose to falling backwards or side-wards rather than forwards and combined to protective reactions impairment (e.g. an outstretched hand), causes higher rate of wrist fracture. The main reason for justifying the lowest prevalence of hip fracture in obese people is associated to fat and soft tissue padding distribution [37, 38].
Obese women with high values of spine or hip BMD measurements not necessarily is associated with lower risk of fragility fractures, because other aspects seem to be involved [14, 29]. More recently, the fat-bone tissue axis has highlighted that low BMD measurements itself cannot explain higher fracture risk in obese individuals. Thus, aspects related to bone quality are pointed out as potential markers of bone strength in this scenario [38]. Considering these qualitative aspects, a similar parallel could be addressed to diabetes mellitus (DM), since is demonstrated higher spine and femur BMD measurements, but also higher non-vertebral fractures [39,40,41], where the resistance to insulin, hyperglycemia and higher advanced glycation end products levels on collagen bone fibers would cause lower bone strength and higher fracture risk. In addition, the diabetes-related complications, including poor balance and sight and peripheral neuropathy, may contribute to increased falling and fracture risk [41].
It is worthy emphasizing that although higher spine and hip BMD measurements have been observed in obese women with fractures, they may be inappropriately low for body weight, suggesting some lack of adaptive response [15, 16, 18]. Therefore, there is a growing awareness on how to identify bone fragility risk in obese individuals, considering that BMD measurements do not necessarily would cause higher fracture risk. Thus, other non-invasive methods to measure structural aspects of trabecular bone and cortical porosity, such as trabecular bone score (TBS) and high-resolution peripheral quantitative computed tomography (HR-pQCT), may have future applications for assessing the fragility fracture risk in obese individuals.
Numerous risk factors for osteoporosis and fractures have been used to develop several risk assessment tools, including the WHO Fracture Risk Assessment Tool (FRAX) algorithm, Q fracture algorithm and Garvan Fracture Risk Calculator, aiming to stratify individuals into 5- or 10-year fracture risk categories or to screen them for requesting BMD measurements. In general, the traditional CRFs for osteoporosis and fracture are similar between obese and non-obese women and it would not be necessary to individualize these indices regarding anthropometric data. Based on that, we decided to evaluate the SAPORI tool performance considering each BMI category. Interestingly, we demonstrated a significant impairment (50–60%) of its sensitivity when it was applied to obese group, suggesting that cut-off score adjustments are necessary in women with BMI above 30 kg/ m2. Although weight has been considered in several international screening tools, including OST, OSIRIS, ORAI, and SCORE, none of them was separately tested according to BMI categories, and so, their sensitivity and specificity cannot be assured in obese patients [20, 22, 42,43,44,45,46,47].
Our study has some limitations, such as a cross-sectional design, lack of information about radiographic vertebral fractures and bone turnover markers, and inherent methodological problems concerning accuracy, precision and reliability of DXA measurements in obese [48]. On the other hand, it has several strengths, including a huge pioneer study to investigate specifically the relationship among anthropometric data, BMD measurements and fragility fractures, according to each BMI category, as well as to demonstrate the poorest tool performance to screen or to measure fracture or osteoporosis risk in obese.
Conclusions
In conclusion, our data highlighted obese women have the same prevalence of non-vertebral low-impact fractures than normal weight women, regardless spine or hip BMD measurements and traditional clinical risk factors, addressing that other bone and extra-skeletal aspects may be involved with bone fragility. For the first time, we demonstrated the performance of a screening tool is hampered in obese women, suggesting the necessity of calibrating the cut-off score, according to BMI category.
References
Riggs BL, Melton LJ 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995;17(5 Suppl):505S–11S.
Stevens GA, et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul Health Metr. 2012;10(1):22–2.
Swinburn BA, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804–14.
Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–33.
WHO WHO. Obesity: Preventing and Managing the Global Epidemic; 2000.
Ence I. Antropometria e estado nutricional no Brasil :metodologia, índices e tendência secular; 2010.
Pinheiro MM, et al. Risk factors for osteoporotic fractures and low bone density in pre and postmenopausal women. Rev Saude Publica. 2010;44(3):479–85.
Pinheiro Mde M, et al. Risk factors for recurrent falls among Brazilian women and men: the Brazilian Osteoporosis Study (BRAZOS). Cad Saude Publica. 2010;26(1):89–96.
Lopes JB, et al. Osteoporotic fractures in the Brazilian community-dwelling elderly: prevalence and risk factors. J Clin Densitom. 2011;14(3):359–66.
Copes RM, et al. Obesity and Fractures in Postmenopausal Women: A Primary-care Cross-Sectional Study at Santa Maria, Brazil. J Clin Densitom. 2015;18(2):165–71.
Pinheiro MM, et al. Clinical risk factors for osteoporotic fractures in Brazilian women and men: the Brazilian Osteoporosis Study (BRAZOS). Osteoporos Int. 2009;20(3):399–408.
Felson DT, et al. Effects of weight and body mass index on bone mineral density in men and women: the Framingham study. J Bone Miner Res. 1993;8(5):567–73.
Gimble JM, et al. Playing with bone and fat. J Cell Biochem. 2006;98(2):251–66.
De Laet C, et al. Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int. 2005;16(11):1330–8.
Premaor MO, et al. Risk factors for nonvertebral fracture in obese older women. J Clin Endocrinol Metab. 2011;96(8):2414–21.
Premaor MO, et al. Obesity and fractures in postmenopausal women. J Bone Miner Res. 2010;25(2):292–7.
Gnudi S, Sitta E, Lisi L. Relationship of body mass index with main limb fragility fractures in postmenopausal women. J Bone Miner Metab. 2009;27(4):479–84.
Compston JE, et al. Obesity is not protective against fracture in postmenopausal women: GLOW. Am J Med. 2011;124(11):1043–50.
Himes CL, Reynolds SL. Effect of obesity on falls, injury, and disability. J Am Geriatr Soc. 2012;60(1):124–9.
Rubin KH, et al. Risk assessment tools to identify women with increased risk of osteoporotic fracture: complexity or simplicity? A systematic review. J Bone Miner Res. 2013;28(8):1701–17.
Rubin KH, et al. Comparison of different screening tools (FRAX(R), OST, ORAI, OSIRIS, SCORE and age alone) to identify women with increased risk of fracture. A population-based prospective study. Bone. 2013;56(1):16–22.
Pinheiro MM, et al. Development and validation of a tool for identifying women with low bone mineral density and low-impact fractures: the Sao Paulo Osteoporosis Risk Index (SAPORI). Osteoporos Int. 2012;23(4):1371–9.
Available from: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/default.shtm. Acessed 13 April, 2016.
Organization, W.H. Obesity and overweight. 2013 [cited 2013 18/08/2013].
Global Database on Body Mass Index: an interactive surveillance tool for monitoring nutrition transition. Geneva, Switzerland: WHO, 2004.; Available from: http://apps.who.int/bmi/index.jsp?introPage5intro_3.html Acessed 3 February 2014.
Kanis JA, et al. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9(8):1137–41.
Brandao. C.M., et al., [2008 official positions of the Brazilian Society for Clinical Densitometry--SBDens]. Arq Bras Endocrinol Metabol. 2009;53(1):107–12.
Saarelainen J, et al. Body mass index and bone loss among postmenopausal women: the 10-year follow-up of the OSTPRE cohort. J Bone Miner Metab. 2012;30(2):208–16.
Johansson H, et al. A meta-analysis of the association of fracture risk and body mass index in women. J Bone Miner Res. 2014;29(1):223–33.
Gonnelli S, Caffarelli C, Nuti R. Obesity and fracture risk. Clin Cases Miner Bone Metab. 2014;11(1):9–14.
Prieto-Alhambra D, et al. The association between fracture and obesity is site-dependent: a population-based study in postmenopausal women. J Bone Miner Res. 2012;27(2):294–300.
Beck TJ, et al. Does obesity really make the femur stronger? BMD, geometry, and fracture incidence in the women's health initiative-observational study. J Bone Miner Res. 2009;24(8):1369–79.
Nevitt MC, et al. Risk factors for a first-incident radiographic vertebral fracture in women > or = 65 years of age: the study of osteoporotic fractures. J Bone Miner Res. 2005;20(1):131–40.
Pirro M, et al. High weight or body mass index increase the risk of vertebral fractures in postmenopausal osteoporotic women. J Bone Miner Metab. 2010;28(1):88–93.
Laslett LL, et al. Excess body fat is associated with higher risk of vertebral deformities in older women but not in men: a cross-sectional study. Osteoporos Int. 2012;23(1):67–74.
Compston J. Obesity and bone. Curr Osteoporos Rep. 2013;11(1):30–5.
Ishii S, et al. Pleiotropic Effects of Obesity on Fracture Risk: The Study of Women's Health Across the Nation. J Bone Miner Res. 2014.
Zhao LJ, et al. Correlation of obesity and osteoporosis: effect of fat mass on the determination of osteoporosis. J Bone Miner Res. 2008;23(1):17–29.
de, L., II, et al., Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. Osteoporos Int, 2005. 16(12): p. 1713-1720.
Vashishth D, et al. Influence of nonenzymatic glycation on biomechanical properties of cortical bone. Bone. 2001;28(2):195–201.
Kurra S, Fink DA, Siris ES. Osteoporosis-associated fracture and diabetes. Endocrinol Metab Clin North Am. 2014;43(1):233–43.
Kanis JA, et al. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int. 2007;18(8):1033–46.
Hippisley-Cox J, Coupland C. Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ. 2009;339:b4229.
Cadarette SM, et al. Development and validation of the Osteoporosis Risk Assessment Instrument to facilitate selection of women for bone densitometry. CMAJ. 2000;162(9):1289–94.
Richy F, et al. Validation and comparative evaluation of the osteoporosis self-assessment tool (OST) in a Caucasian population from Belgium. QJM. 2004;97(1):39–46.
Sedrine WB, et al. Development and assessment of the Osteoporosis Index of Risk (OSIRIS) to facilitate selection of women for bone densitometry. Gynecol Endocrinol. 2002;16(3):245–50.
Lydick E, et al. Development and validation of a simple questionnaire to facilitate identification of women likely to have low bone density. Am J Manag Care. 1998;4(1):37–48.
Patel R, et al. Long-term precision of DXA scanning assessed over seven years in forty postmenopausal women. Osteoporos Int. 2000;11(1):68–75.
Acknowledgments
The authors thank to researchers of SAPOS (Sao Paulo Osteoporosis Study) and Sao Paulo Osteoporosis Index (SAPORI) for assistance and kindly have given their databases.
Funding
Not applicable.
Availability of data and materials
All data analyzed (database) in this study can be requested to authors anytime if the editors judge necessary.
Author information
Authors and Affiliations
Contributions
BANCC performed the data analysis and drafted the manuscript. VLS participated in the design of the study. ETR helped to data analysis. VM performed all statistical analysis. JS participated in the design of the study. MMP participated in the design of the study, helped with data analysis and in drafting of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Research Ethics Committee of the Universidade Federal de São Paulo/ Escola Paulista de Medicina approved the present study (CEP/UNIFESP - 0406/2015).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nunes Cavalcante Castro, B.A., Torres dos Reis Neto, E., Szejnfeld, V.L. et al. Could obesity be considered as risk factor for non-vertebral low-impact fractures?. Adv Rheumatol 58, 42 (2018). https://doi.org/10.1186/s42358-018-0044-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42358-018-0044-6