
Abstract
Background
Aneurysm of basilar perforator was rarely reported in the literature. It is difficult to treat due to its small size and deep-seated location. Excessive treatment may cause complications that resulted from ischemic events of parent perforators. Therefore, it is important to make clinical strategy for such patients to improve the prognosis.
Case presentation
One case, who presented as spontaneous subarachnoid hemorrhage, despite the negative result in computed tomography angiography firstly, was diagnosed angiographically as a ruptured aneurysm of the basilar perforator. A good clinical outcome of the case was achieved during the follow-up after conservative observation for 2 months, as well as the disappearance of previous lesion from angiography.
Conclusions
Aneurysm located at perforator of basilar trunk was rare and difficult to treat. Conservative observation for certain cases with periodic angiography follow-up was considered in order to prevent the patients from potential iatrogenic effects.
Similar content being viewed by others


Background
Aneurysms of the perforators of intracranial arteries are rare, and most of them arise from the lenticulostriate artery of middle cerebral artery (MCA) [1]. Due to the rarity of the perforator of basilar artery, the natural history and the optimal therapeutic strategy are still controversial. We report a patient who harbored a perforator aneurysm of basilar artery (PABA) presented as spontaneous subarachnoid hemorrhage (SAH) who recovered well after conservative observation.
Case presentation
A 65-year-old gentleman had the history of hypertension and diabetes mellitus, which were well controlled for several years. In the emergency room, he complained of a sudden headache and dizziness for 5 days accompanied with nausea and vomiting. There were no neurological deficits detected by physical examination except for a positive meningeal irritation sign. Emergency computed tomography (CT) of the head showed SAH surrounding the pontine (Fig. 1A), but no aneurysm or vascular malformation was noted by CT angiography (CTA) (Fig. 1B). Digital subtraction angiography (DSA) revealed a small aneurysm less than 1.5 mm in diameter of a perforator which originated from the dorsal quandrification of the basilar trunk (Fig. 1C, D). Based on the CT images, this tiny lesion was considered a ruptured aneurysm. The patient experienced conservative observation and recovered well. A follow-up DSA 2 months later found that the aneurysm disappeared spontaneously and the parent perforator remained intact (Fig. 1E, F). The modified Rankin Scale (mRS) was 0 points for this patient at that time.

Imaging data of the case. A SAH surrounding potine was confirmed by head CT after onset. B Emergency CTA did not demonstrate definite source of hemorrhage. C, D Three-dimensional rotation angiography (3DRA) revealed a small aneurysm localized at posterior perforator of rostral basilar trunk. E, F The lesion disappeared from DSA during 2 months of follow-up with preservation of parent perforator
Discussion
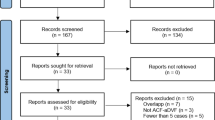
Van Gijn et al. reported a group of patients suffering from SAH in 1986 and presented the concept of “perimesencephalic nonaneurysmal subarachnoid hemorrhage (PNSH)” [2]. The similar clinical characteristics of these cases were that the location of SAH was mainly surrounding the pontine based on CT images and no definite vascular lesions could be detected by DSA. The rare pathogenic vein or capillary was considered the source of hemorrhage such as telangiectasia, tiny arteriovenous malformation, or arterial dissecting. Although the case we reported has the similar characteristic of CT images with that of PNSH, a small PABA is noted by DSA, which is definitely suggested that this is one of the causes of the so-called PNSH [3]. We retrieved the literatures from PubMed by the keywords as “basilar artery,” “perforator,” and “aneurysm.” As a result, 25 relevant literatures were selected and are listed in Table 1 after reviewing the abstracts. Due to the low morbidity of PABA, only 51 cases in 25 literatures have been published since the first case reported by Ghogawala et al. in 1996 [4]. PABA is mostly small and possibly thrombotic; therefore, it is difficult to make a definite diagnosis. For diagnosis, as the procedure of the case we reported, DSA is of choice and superior to CTA. Sometimes, shortly periodical follow-up by DSA is necessary [5].
All cases harbored PABAs reported so far were presenting as SAH instead of incidental lesions, which resulted in its undefined natural history [27]. Difficulties of endovascular catheterization, microsurgical exposure, and preservation of parent perforator complicated the determination of therapeutic strategy. On the contrary, the disappearance of aneurysm from follow-up images was found in some cases without any endo- and extravascular procedures, which resulted that a periodical DSA follow-up was considered as a preferred strategy for many authors [17]. But in 21 cases who experienced conservative observation in the literatures, rehemorrhage occurred in 6 patients (28.57%). Two of them received microsurgery, and 2 of them were treated endovascularly. Of the above 4 cases, only 1 patient recovered well, and the rest 3 patients suffered from variant neurological deficits due to the ischemic events of parent perforators. Another 2 patients, who remained under observation, recovered well. Based on the above data, the prognosis of endovascular or microsurgical strategies may not be better than conservative observation [3, 7, 12, 21, 25]. And it appears to have comparable safety and efficacy outcomes to flow-diverter (FD) treatment of other ruptured basilar artery perforator aneurysms [28]. But according to previous reports, the conservative observation cases are at high risk of rebleeding [29]; for these cases, surgical treatment may be the best strategy. However, no matter traditional surgical clipping or endovascular intervention, the therapeutic effect is still controversial.
Microsurgical clipping is not of choice for PABA. Sanchez-Mejia believed that such lesions usually had no definite neck and even were a type of blood blister-like aneurysm which should be trapped along with the parent perforator, and the control of the proximal basilar trunk was also difficult during microsurgery [7]. For our patient, we printed a three-dimensional model (Medprin Company, China, Guangzhou) to verify the feasibility of microsurgery [30]. During the simulating procedure, a more backward subtemporal approach was needed to expose the lesion, which increased the risk of injury of Labbé vein. Moreover, the aneurysm is located in the bottom of a narrow surgical corridor surrounded with critical nervous and vascular structures. In order to ensure that the clip will not obstruct the surgical view in this nearly 7 cm in-depth surgical approach, a longer straight clip is compulsory, which leads to the uncertainty of complete clipping of aneurysm and intact preserving of parent perforator (Fig. 2).

Simulating procedure on printed three dimension model. A Subtemporal keyhole approach of right side. The depth of aneurysm is 7 cm from temporal bone. B The length of visible basilar artery is 5 mm between petrosal apex and neck of aneurysm under the microsurgical corridor. C The aneurysm can be clipped by longer clip after retraction of isplateral superior cerebellar artery. D Relationship of clip and surrounding vascular structures after simulating clip application
A tiny aneurysm is prone to rupture during superselective catheterization and the parent perforator is usually too small in caliber to be preserved. Of 5 cases who experienced endovascular embolization for such aneurysms by detachable coil (3 cases) or Onyx glue (Medtronic Company, USA, California) (2 cases) in the literature, only one case with distal BAPA recovered well, and the rest of the patients suffered from hemiplegia caused by ischemic events of perforator [10, 14, 21]. Although it has been reported that the parent perforators could be compensated [31], the safety of occlusion of these arteries is still undefined.
The hemodynamics of side-wall aneurysm model revealed that the blood flow velocity and wall shear stress in the aneurysmal cavity were significantly changed when the neck was covered by a stent. Furthermore, the denser the mesh, the greater the change [32]. Accordingly, flow diverter (FD) seems to be an ideal choice, but the incidence of infarction after stenting of posterior circulation aneurysm by FD is 14% [33]. Based on 5 relevant cases treated by FD (4 by PIPELINE [Medtronic Company, CA, USA] and 1 by SILK [Balt Extrusion Company, Montmorency, France]) reported in the literature, only one patient was free of ischemic events. It is suggested that excessive change of hemoynamics may be a risk factor of perforator occlusion [16, 20, 25]. Consequently, stent-in-stent technique with conventional stents (Enterprise [Codman Neuro Company, MA, USA], Neuroform [Stryker, MI, USA], Leo [Balt Extrusion Company, Montmorency, France], etc.) was considered as a better strategy to treat more PABAs. In 10 reported patients, half of them had no definite ischemic events; the prognosis of the rest of the patients was not reported as well [13, 22, 27]. However, whether the consequent antiplatelet therapy will increase the hemorrhagic complications remains to be solved by a study with larger sample size and longer follow-up.
Jiang et al. proposed a novel endovascular strategy [24]. They reported a case with a small perforator aneurysm of proximal basilar trunk which was failed to superselective catheterization. A microguidewire (Traxcess 14 [Microvention Terumo Company, CA, USA]) was positioned into the aneurysmal cavity followed by electrocoagulation with detaching box of Solitaire system (NDS-2, Medtronic, USA). As a result, the aneurysm was occluded completely; the parent perforator was preserved as well. This approach provides us with a new concept that seems to make the endovascular procedure for PABA more convenient, safe, and cost-effective. However, the long-term durability is still unknown. On the other hand, asymptomatic ischemic events caused by thrombosis during electrocoagulation should also be considered.
Ma et al. further reported three cases treated by endovascular electrothrombosis, which failed to pass an Echelon 10 microcatheter into the aneurysm [34]. A microguidewire (Traxcess-14 [MicroVention, Tustin, CA, USA]) was placed into the sac of the aneurysms through the microcatheter and connected its proximal tip to the Solitaire stent detachment system (ev3). The first case was conducted electrothrombosis at 4.0 V and 1.0 mA current three times for 30s each; the second one was conducted electrothrombosis at 4.0 V and 1.0 mA current three times (total of 3 min); the third one use the same parameter to sustained electrothrombosis for 1.5 min. As a result, in the first and the third cases, the aneurysms were successfully occluded without treatment-related complication. The second one failed and converted to endovascular coiling using a 1.3-F microcatheter. The patient suffered from brainstem infarction and finally died of severe SAH after surgery. At 6-month follow-up, the other two patients were neurologically intact and angiography showed total occlusion of both aneurysms. The findings in this report provide a potential treatment option for ruptured PABAs to prevent re-rupture, but the risk of perforator occlusion and aneurysm re-ruptured during surgery is still unknown, and the safety of this technique remains a concern. Therefore, it needs more research to confirm its safety and efficacy.
Conclusions
Aneurysm that originated from a perforator of the basilar trunk was rare and difficult to treat. Conservative observation for certain cases with periodic angiography follow-up was considered in order to prevent the patients from potential iatrogenic effects.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- MCA:
-
Middle cerebral artery
- BAPA:
-
Basilar artery perforator aneurysm
- SAH:
-
Subarachnoid hemorrhage
- CT:
-
Computed tomography
- CTA:
-
Computed tomography angiography
- DSA:
-
Digital subtraction angiography
- mRS:
-
Modified Rankin Scale
- PNSH:
-
Perimesencephalic nonaneurysmal subarachnoid hemorrhage
- FD:
-
Flow diverter
- 3DRA:
-
Three-dimensional rotation angiography
References
Vargas J, Walsh K, Turner R, Chaudry I, Turk A, Spiotta A. Lenticulostriate aneurysms: a case series and review of the literature. J Neurointerv Surg. 2015;7(3):194–201. https://doi.org/10.1136/neurintsurg-2013-010969.
van Gijn J, van Dongen KJ, Vermeulen M, Hijdra A. Perimesencephalic hemorrhage: a nonaneurysmal and benign form of subarachnoid hemorrhage. Neurology. 1985;35(4):493–7. https://doi.org/10.1212/WNL.35.4.493.
Park SQ, Kwon OK, Kim SH, Oh CW, Han MH. Pre-mesencephalic subarachnoid hemorrhage: rupture of tiny aneurysms of the basilar artery perforator. Acta Neurochir. 2009;151(12):1639–46. https://doi.org/10.1007/s00701-009-0416-0.
Ghogawala Z, Shumacher JM, Ogilvy CS. Distal basilar perforator artery aneurysm: case report. Neurosurgery. 1996;39(2):393–6. https://doi.org/10.1097/00006123-199608000-00034.
Hamel W, Grzyska U, Westphal M, Kehler U. Surgical treatment of a basilar perforator aneurysm not accessible to endovascular treatment. Acta Neurochir. 2005;147(12):1283–6. https://doi.org/10.1007/s00701-005-0615-2.
Fiorella D, Albuquerque FC, Deshmukh VR, Woo HH, Rasmussen PA, Masaryk TJ, et al. Endovascular reconstruction with the Neuroform stent as monotherapy for the treatment of uncoilable intradural pseudoaneurysms. Neurosurgery. 2006;59(2):291–300. https://doi.org/10.1227/01.NEU.0000223650.11954.6C.
Sanchez-Mejia RO, Lawton MT. Distal aneurysms of basilar perforating and circumferential arteries. Report of three cases. J Neurosurg. 2007;107(3):654–9. https://doi.org/10.3171/JNS-07/09/0654.
Mathieson CS, Barlow P, Jenkins S, Hanzely Z. An unusual case of spontaneous subarachnoid haemorrhage - a ruptured aneurysm of a basilar perforator artery. Br J Neurosurg. 2010;24(3):291–3. https://doi.org/10.3109/02688690903572095.
Deshaies EM, Jacobsen W, Krishnamurthy S. Enterprise stent-within-stent embolization of a basilar artery perforator aneurysm. World J Neurosci. 2011;1(3):45–8. https://doi.org/10.4236/wjns.2011.13007.
Chen L, Chen E, Chotai S, Tian X. An endovascular approach to ruptured aneurysms of the circumferential branch of the basilar artery. J Clin Neurosci. 2012;19(4):527–31. https://doi.org/10.1016/j.jocn.2011.04.049.
Gross BA, Puri AS, Du R. Basilar trunk perforator artery aneurysms. Case report and literature review. Neurosurg Rev. 2013;36(1):163–8. https://doi.org/10.1007/s10143-012-0422-1.
Apok V, Tarnaris A, Brydon HL. An unusual aneurysm of a basilar perforating artery presenting with a subarachnoid haemorrhage. Br J Neurosurg. 2013;27(1):105–7. https://doi.org/10.3109/02688697.2012.717977.
Nyberg EM, Chaudry MI, Turk AS, Spiotta AM, Fiorella D, Turner RD. Report of two cases of a rare cause of subarachnoid hemorrhage including unusual presentation and an emerging and effective treatment option. J Neurointerv Surg. 2013;5(5):e30. https://doi.org/10.1136/neurintsurg-2012-010387.
Ding D, Starke RM, Jensen ME, Evans AJ, Kassell NF, Liu KC. Perforator aneurysms of the posterior circulation: case series and review of the literature. J Neurointerv Surg. 2013;5(6):546–51. https://doi.org/10.1136/neurintsurg-2012-010557.
Sivakanthan S, Carlson AP, van Loveren H, Agazzi S. Surgical clipping of a basilar perforator artery aneurysm: a case of avoiding perforator sacrifice. J Neurol Surg A Cent Eur Neurosurg. 2015;76(1):79–82. https://doi.org/10.1055/s-0033-1356488.
Chalouhi N, Jabbour P, Starke RM, Zanaty M, Tjoumakaris S, Rosenwasser RH, et al. Treatment of a basilar trunk perforator aneurysm with the pipeline embolization device: case report. Neurosurgery. 2014;74(6):E697–701. https://doi.org/10.1227/NEU.0000000000000308.
Chavent A, Lefevre PH, Thouant P, Cao C, Kazemi A, Mourier K, et al. Spontaneous resolution of perforator aneurysms of the posterior circulation. J Neurosurg. 2014;121(5):1107–11. https://doi.org/10.3171/2014.7.JNS132411.
Kim YJ, Ko JH. Sole stenting with large cell stents for very small ruptured intracranial aneurysms. Interv Neuroradiol. 2014;20(1):45–53. https://doi.org/10.15274/INR-2014-10007.
Daruwalla VJ, Syed FH, Elmokadem AH, Hurley MC, Shaibani A, Ansari SA. Large basilar perforator pseudoaneurysm: A case report. Interv Neuroradiol. 2016;22(6):662–5. https://doi.org/10.1177/1591019916659261.
Peschillo S, Caporlinqua A, Cannizzaro D, et al. Flow diverter stent treatment for ruptured basilar trunk perforator aneurysms. J Neurointerv Surg. 2016;8(2):190–6. https://doi.org/10.1136/neurintsurg-2014-011511.
Forbrig R, Eckert B, Ertl L, Patzig M, Brem C, Vollmar C, et al. Ruptured basilar artery perforator aneurysms--treatment regimen and long-term follow-up in eight cases. Neuroradiology. 2016;58(3):285–91. https://doi.org/10.1007/s00234-015-1634-1.
Satti SR, Vance AZ, Fowler D, Farmah AV, Sivapatham T. Basilar artery perforator aneurysms (BAPAs): review of the literature and classification. J Neurointerv Surg. 2017;9(7):669–73. https://doi.org/10.1136/neurintsurg-2016-012407.
Aboukais R, Zairi F, Estrade L, Quidet M, Leclerc X, Lejeune JP. A dissecting aneurysm of a basilar perforating artery. Neurochirurgie. 2016;62(5):263–5. https://doi.org/10.1016/j.neuchi.2016.03.003.
Jiang Y, Luo J, Zheng J, Li Y. Endovascular pure electrocoagulation of intracranial perforator blister-like aneurysm not accessible to microcatheter-New approach to treat small vessel hemorrhage disease. Int J Stroke. 2016;11(5):NP60–1. https://doi.org/10.1177/1747493016641953.
Finitsis S, Derelle AL, Tonnelet R, Anxionnat R, Bracard S. Basilar perforator aneurysms: presentation of 4 cases and review of the literature. World Neurosurg. 2017;97:366–73. https://doi.org/10.1016/j.wneu.2016.10.038.
Buell TJ, Ding D, Raper DMS, Chen CJ, Hixson HR, Crowley RW, et al. Posterior circulation perforator aneurysms: a proposed management algorithm. J Neurointerv Surg. 2018;10(1):55–9. https://doi.org/10.1136/neurintsurg-2016-012891.
Chau Y, Sachet M, Sédat J. Should we treat aneurysms in perforator arteries from the basilar trunk? Review of 49 cases published in the literature and presentation of three personal cases. Interv Neuroradiol. 2018;24(1):22–8. https://doi.org/10.1177/1591019917734531.
Elsheikh S, Möhlenbruch M, Seker F, et al. Flow diverter treatment of ruptured basilar artery perforator aneurysms: a multicenter experience [published online ahead of print, 2022 Jan 20]. Clin Neuroradiol. 2022. https://doi.org/10.1007/s00062-021-01133-y.
Finitsis S, Derelle AL, Tonnelet R, Anxionnat R, Bracard S. Basilar perforator aneurysms: presentation of 4 cases and review of the literature. World Neurosurg. 2017;97:366–73. https://doi.org/10.1016/j.wneu.2016.10.038.
Lan Q, Chen A, Zhang T, Li G, Zhu Q, Fan X, et al. Development of three-dimensional printed craniocerebral models for simulated neurosurgery. World Neurosurg. 2016;91:434–42. https://doi.org/10.1016/j.wneu.2016.04.069.
Marinković SV, Gibo H. The surgical anatomy of the perforating branches of the basilar artery. Neurosurgery. 1993;33(1):80–7.
Cantón G, Levy DI, Lasheras JC, Nelson PK. Flow changes caused by the sequential placement of stents across the neck of sidewall cerebral aneurysms. J Neurosurg. 2005;103(5):891–902. https://doi.org/10.3171/jns.2005.103.5.0891.
Phillips TJ, Wenderoth JD, Phatouros CC, Rice H, Singh TP, Devilliers L, et al. Safety of the pipeline embolization device in treatment of posterior circulation aneurysms. AJNR Am J Neuroradiol. 2012;33(7):1225–31. https://doi.org/10.3174/ajnr.A3166.
Ma H, Zhao R, Fang Y, Li Q, Yang P, Huang Q, et al. Endovascular electrothrombosis: a promising alternative for basilar artery perforator aneurysm treatment. Interv Neuroradiol. 2021;27(4):511–5. https://doi.org/10.1177/1591019920987913.
Acknowledgements
Not applicable.
Funding
This article was funded by Suzhou high tech zone medical & health science & technology program (2018Z014) and Suzhou science & technology development program (SYS2019067).
Author information
Authors and Affiliations
Contributions
CGD, ALC, and QZ designed this study. ZLL, TW, and DHY collected and analyzed the patient data. YW is the major contributor in writing the manuscript. QZ supervised the entire research process. All authors read and approved the final manuscript.
Authors’ information
Not applicable.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent for publication of their clinical details and clinical images was obtained from the guardian of the patient. A copy of the consent form is available for review by the editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, Y., Li, Z., Yang, D. et al. Spontaneous subarachnoid hemorrhage caused by ruptured aneurysm of basilar trunk perforator: a case report and literature review. Chin Neurosurg Jl 8, 14 (2022). https://doi.org/10.1186/s41016-022-00281-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41016-022-00281-5