
Abstract
Background
Among youth, plyometric-jump training (PJT) may provide a safe, accessible, and time-efficient training method. Less is known on PJT effectiveness according to the maturity status.
Objective
This systematic review with meta-analysis set out to analyse the body of peer-reviewed articles assessing the effects of PJT on measures of physical fitness [i.e., maximal dynamic strength; change of direction (COD) speed; linear sprint speed; horizontal and vertical jump performance; reactive strength index] and sport-specific performance (i.e., soccer ball kicking and dribbling velocity) according to the participants’ maturity status.
Methods
Systematic searches were conducted in three electronic databases using the following inclusion criteria: (i) Population: healthy participants aged < 18 years; (ii) Intervention: PJT program including unilateral and/or bilateral jumps; (iii) Comparator: groups of different maturity status with control groups; (iv) Outcomes: at least one measure of physical fitness and/or sport-specific performance before and after PJT; (v) experimental design with an active or passive control group, and two or more maturity groups exposed to the same PJT. The DerSimonian and Laird random-effects models were used to compute the meta-analysis. The methodological quality of the studies was assessed using the PEDro checklist. GRADE was applied to assess certainty of evidence.
Results
From 11,028 initially identified studies across three electronic databases, 11 studies were finally eligible to be meta-analysed (n total = 744; seven studies recruited males; four studies recruited females). Three studies were rated as high quality (6 points), and eight studies were of moderate quality (5 points). Seven studies reported the maturity status using age at peak height velocity (PHV; pre-PHV values up to − 2.3; post-PHV up to 2.5). Another four studies used Tanner staging (from Tanner I to V). The training programmes ranged from 4 to 36 weeks, using 1–3 weekly training sessions. When compared to controls, pre-PHV and post-PHV participants obtained small-to-moderate improvements (ES = 0.35 − 0.80, all p < 0.05) in most outcomes (i.e., sport-specific performance; maximal dynamic strength; linear sprint; horizontal jump; reactive strength index) after PJT. The contrast of pre-PHV with post-PHV youth revealed that PJT was similarly effective in both maturity groups, in most outcome measures except for COD speed (in favour of pre-PHV). PJT induces similar physical fitness and sport-specific performance benefits in males and females, with a minimal exercise dosage of 4 weeks (8 intervention sessions), and 92 weekly jumps. Results of this meta-analysis are based on low study heterogeneity, and low to very low certainty of evidence (GRADE analysis) for all outcomes.
Conclusion
Compared to control participants, PJT resulted in improved maximal dynamic strength, linear sprint speed, horizontal jump performance, reactive strength index, and sport-specific performance (i.e., soccer ball kicking and dribbling velocity). These effects seem to occur independently of the maturity status, as both pre-PHV and post-PHV participants achieved similar improvements after PJT interventions for most outcomes. However, several methodological issues (e.g., low sample sizes and the pooling of maturity categories) preclude the attainment of more robust recommendations at the current time. To address this issue, consistency in maturity status reporting strategies must be improved in future studies with the general youth population and youth athletes.
Similar content being viewed by others
Key Points
-
Plyometric jump training is an effective intervention to improve physical fitness of youth participants, including maximal dynamic strength, linear sprint speed, horizontal jump performance, reactive strength index, and sport-specific performance (e.g., soccer ball kicking velocity).
-
Plyometric jump training induces similar physical fitness and sport-specific performance benefits in males and females, with a minimal exercise dosage of 4 weeks (8 intervention sessions), and 92 weekly jumps.
-
Plyometric jump training is similarly effective in pre- and post-PHV youth in most outcomes, except for COD speed (in favour of pre-PHV).
-
Results of this meta-analysis are based on a total of 744 participants, from 11 articles with moderate to high methodological quality, low study heterogeneity, and low to very low certainty of evidence (GRADE analysis) for all outcomes.
Introduction
Physical fitness is correlated to current and future health outcomes [1,2,3]. There is additional evidence from original research that improvements in muscle power result in increased bone mass in school-aged participants [4]. Moreover, high levels of physical fitness appear to facilitate motor skill learning [5,6,7,8] in youths and adults and help to reduce the risk of sustaining musculoskeletal injuries [9,10,11,12]. Schools or sport clubs can provide excellent opportunities to deliver exercise interventions to improve physical fitness and sport-specific performance (SSP) because youth can be reached irrespective of their socio-economic background. Intervention programs implemented in schools or sport clubs should be easy to administer and afford little extra equipment [13, 14]. Accordingly, safe, effective and joyful training programs are needed that require little equipment and occupy large groups of individuals [15, 16], such as plyometric jump training (PJT).
Intervention programs involving PJT may provide an exercise mode that can be adapted for populations according to their age, sex, health, physical fitness and/or SSP level [17,18,19,20]. Indeed, PJT emphasises the use of jumping drills, such as hops, depth jumps, bouncing, or skipping exercises. Moreover, using limited or no equipment, it is possible to promote a wide range of exercises and intensities through the modification of variables such as drop height, ground contact time, direction (e.g., vertical vs. horizontal), type of surface (e.g., stiff- or soft-surfaces; horizontal vs. incline), landing type (e.g., bilateral vs. unilateral), or loading parameter (e.g., external load vs. unloaded; assisted vs. resisted). The implementation of PJT in schools or sports clubs may enhance physical fitness and additionally improve students’ perception of physical activity [21, 22]. Interventions using PJT have proven to be effective to promote markers of health such as bone mineral content [17, 23], measures of physical fitness (e.g., linear sprint speed) [8, 24,25,26,27,28] and SSP in a time-efficient manner e.g. two to four 5-min training sessions per week [20]. Further, PJT may induce improvements in neuromuscular, cardiovascular and body composition-related measures of physical fitness and SSP [20, 29,30,31,32,33]. Moreover, PJT is safe for youths and a key element of injury prevention programs [34].
However, most PJT studies have been conducted with adults, with comparatively fewer studies in youths [35, 36]. The transfer of findings from adults to youths appears inappropriate considering that during the youths’ maturation process a cascade of biological events leads to e.g., rapid increases in stature, potential temporary disruption in motor co-ordination, large increases in fat-free mass, changes in muscle–tendon architecture [37,38,39], all of which may influence the physical fitness and SSP responsiveness to PJT [37, 40,41,42,43,44,45,46,47,48]. More specifically, the way maturation influences the PJT response on physical fitness and SSP remains unresolved [37, 48,49,50,51,52,53,54]. Those PJT studies that reported information on maturity have used different methods to estimate participants’ maturity status (e.g., age at peak height velocity [PHV]; Tanner stages) [35, 36]. This makes a comparison between studies difficult. Although there is evidence on the effects of PJT on physical fitness and SSP in athletes aged 10–18 years [48, 51, 52, 54], comparisons across these age groups are scarce. For example, Asadi et al. [51] noted in their meta-analysis, which included 16 PJT studies with athletes aged 10–18 years, that none of the studies included two or more maturity groups. Due to this limitation, the aforementioned review study [51] compared the results between the 16 PJT studies according to chronological age but not maturity status. Greater performance gains were found for PJT studies with 13.0–18.0 years participants (ES = 0.95 − 0.99) compared to their younger peers (10.0–12.9 years; ES = 0.68) [51]. This analysis however could be confounded due to differences in the applied PJT protocols (e.g., duration; intensity) which may affect the results of PJT studies [51]. Further, chronological age-based comparisons fail to account for the variation in maturity status within the age groups. Moreover, another systematic review [54] compared the effects of PJT in different maturity groups (estimated using the reported chronological age) and, in contrast to Asadi and colleagues [51], found greater performance gains for younger compared with older participants. It must be noted though that Asadi and colleagues [51] focused their analysis on change-of-direction (COD) speed, while Peitz and colleagues [54] examined a broader spectrum of physical fitness and SSP outcomes. Further, Peitz and colleagues [54] did not provide a meta-analysis but a systematic review with comparative studies. Therefore, there is a need for a meta-analysis to compute outcome-specific results according to the maturity status of the participants involved in PJT.
A systematic review of the currently available literature could be valuable because it may shed light on the effectiveness of PJT on physical fitness and SSP as per the participants’ maturity status, with implications also for health [55, 56]. Additionally, most studies have included relatively small sample sizes (i.e., N < 10) [35, 36], which is a common issue in the sport-science literature [57]. Moreover, most studies related to the effectiveness of PJT on physical fitness and SSP in participants according to their maturity status have not addressed the potential role of moderators such as total volume (i.e., minimal effective training dosage), or participants’ sex (i.e., included only males) [35, 36, 51]. Therefore, this systematic review with meta-analysis set out to analyse the body of peer-reviewed articles assessing the effects of PJT on measures of physical fitness and SSP according to the participants’ maturity status.
Methods
Procedures
A systematic review was conducted according to international standards [58], and adapted a posteriori according to the updated PRISMA 2020 guidelines [59] and related advances in the field [35, 36, 60,61,62,63,64,65] (adaptations described in the Additional file 4: Table S1).
Literature Search: Administration and Update
With no time-frame restrictions, we performed electronic searches in the following databases PubMed, Web of Science, and SCOPUS. A detailed description of our search can be found in the Additional file 4: Table S1. Studies were eligible to be included from inception up to January 2022. One author (RRC) conducted the initial search and removed duplicates.
In accordance with the a priori defined study eligibility criteria (Table 1), two authors (RRC and FMC) independently screened and confirmed, the retrieved studies based on titles, abstracts, and full texts. A third author (UG) was consulted in case of disagreement between RRC and FMC. The respective case was discussed until we reached a unanimous decision. Potentially relevant studies were also searched for in the reference lists of the included studies.
Included studies and selection criteria were sent to three experts related to the research area PJT to help identify additional relevant articles (the experts did not receive the search strategy). Thereafter, included studies were assessed for errata or retraction.
Inclusion and Exclusion Criteria
Selection of studies was based on the PICOS approach [58]. Although most PJT studies are published in English [35], we included studies written in English, Spanish, Portuguese, and German (i.e., authors’ native languages). Only original full-text peer-reviewed articles were included, excluding other documents (e.g., books, book chapters, congress abstracts).
Regarding the comparison between groups of different maturity status, various methods were identified that estimate the individual’s maturity status such as Tanner stages [66], anthropometric characteristics to estimate PHV or similar somatic maturity prediction models [67,68,69], X-ray methods [70], or related methods (e.g., pre- and post-menarche) [71]. Nonetheless, it is difficult to compare all identified methods to estimate the maturity status. Although we did not exclude studies a priori that used different methods to determine the maturity status, we preferred those approaches that are easy-to-administer for practitioners (e.g., PHV through anthropometric characteristics). In addition, previous PJT studies indicated that PHV and Tanner stages are the two most common methods used by researchers and practitioners [35, 36]. Studies reporting only chronological age or competitive age categories were excluded.
Data Extraction
In this study, we evaluated the effects of PJT (compared to maturity-matched controls and between maturity groups) on different measures of physical fitness and SSP (see below), as these may reflect different physiological and biomechanical markers related to the health status, the injury risk, and sport-related long-term effective participation [2, 72,73,74,75]. Tests that assess physical fitness attributes such as jump performance (e.g., countermovement jump [CMJ] height), linear sprint speed (e.g., 20-m sprint time), balance (e.g., one-legged stance time), endurance (e.g., 20-m shuttle run test), and muscle strength (one-repetition maximum of leg extensors) show very high test–retest reliability with an intraclass correlation coefficient of > 0.9 [76,77,78,79,80,81], which is essential to ensure strong consistency between the analysed studies within a meta-analysis [58].
If one study included two or more tests related to the same outcome category (e.g., 20-m shuttle run test for endurance, and Yo-Yo test for endurance), we included the test that is most representative of the respective outcome variable under consideration. This was based on the following logical hierarchical rationale: (i) greater representativeness compared to other study tests [e.g., if three studies reported the 20-m shuttle run test for endurance, and one additional study reported both the 20-m shuttle run test for endurance, and the Yo-Yo test for endurance, the 20-m shuttle run test was selected]; (ii) greater specificity to the group of participants being compared [e.g., for soccer players, the Yo-Yo test for endurance would be preferred over the 20-m shuttle run test for endurance]; (iii) greater reliability. Further, only data from the final period was included if one study included two or more post-intervention test periods (e.g., 6-week, 12-week). However, if the post-intervention period involved a detraining period, this was not included. Relatedly, if one study included two or more measures from a single test (e.g., vertical jump height and ground contact time from the drop jump test), the above-mentioned logical hierarchical rationale was applied. In addition, in the context of this study, performance measures (e.g., vertical jump height) were of greater interest compared with biomechanical variables (e.g., joint angle at contact with the ground).
The means and standard deviations of dependent variables were extracted as previously reported [171], using specialised software when studies reported data only in figures [82]. Four authors were independently involved in the process (RRC, FMC, JA, UG).
Methodological Quality of the Included Studies
The studies’ methodological quality was assessed as previously described [171], using a valid and reliable tool which is the PEDro scale [83,84,85], frequently used in the PJT literature [36, 80, 86]. However, it is not possible to satisfy all scale items in PJT studies [87]. Specifically, for the present systematic review, (i) for PEDro scale item number 2, a point was awarded when participants were divided according to age/maturity, (ii) for PEDro scale item number 3 concealed allocation was precluded, as participants were allocated to groups according to their age/maturity; therefore, this item was not considered in the final classification of the study quality; (iii) for PEDro scale item number 4, baseline differences were expected due to differences in age/maturity [71]; therefore, this item was not considered in the final classification of the study quality. Therefore, PJT studies were assessed as previously recommended [26, 86, 88]: “poor”, “moderate”, and “high” quality for ≤ 3 points, 4–5 points, and 6–10 points, respectively. Two authors applied the PEDro scale for each included study independently (RRC and FMC). In cases when an author encountered studies of which he was a co-author, his assessment was not considered, and any discrepancies between authors were resolved via consensus or with the assistance of a third author (UG). We did not exclude studies if they had low methodological quality; however, moderator analyses according to the studies’ methodological quality were planned (see below, “Moderator analyses” section).
Summary Measures, Synthesis of Results, and Publication Bias
According to Valentine and colleagues, two studies are needed to aggregate and meta-analyse results [89]. However, low sample sizes are common in the field of PJT [17, 35, 36, 57, 90]. Therefore, we performed meta-analyses when ≥ 3 studies were available [2, 91]. The ES (i.e., Hedges’ g, with 95% confidence intervals [95% CIs]) for each physical fitness and SSP attribute in the compared groups (i.e., maturity-matched PJT group vs. control group; PJT group vs. PJT group with different maturity) was calculated using the DerSimonian and Laird inverse random-effects model for meta-analyses. Calculated ES were interpreted as trivial, small, moderate, large, very large, and extremely large for values < 0.2, 0.2–0.6, > 0.6–1.2, > 1.2–2.0, > 2.0–4.0, and > 4.0, respectively [92]. The I2 statistic values of < 25%, 25 − 75%, and > 75% represented low, moderate, and high levels of heterogeneity, respectively [93]. The Comprehensive Meta-Analysis software (version 2, Biostat, Englewood, NJ, USA) was used for statistical analyses (significance set at p ≤ 0.05).
Assessment of Maturity Status
Most included PJT studies reported the maturity status according to years from PHV [35, 36]. Although PHV is not the gold standard, it is valid and logistically convenient for practitioners [56, 71, 94]. Therefore, we used a proxy of PHV as a basis to pool maturity judged by different methods. To avoid the exclusion of potentially relevant studies which reported pubertal staging (i.e., Tanner stages), PHV was obtained from sex-specific equations due to its relationship to the aforementioned maturity-age markers [95]. We dichotomised PHV categorization, as previously suggested [67]. Therefore, any negative maturity offset (e.g., PHV − 0.5) classified the group mean as pre-PHV and any positive maturity offset as post-PHV. For dichotomization of groups in studies that reported the maturity status according to the Tanner method, stages I–III for boys and I–II for girls were considered as pre-PHV (i.e., < 50% of the corresponding sex-group achieved PHV for the respective Tanner stage). Stages IV–V for boys and III–V for girls were deemed as post-PHV (i.e., > 50% of the corresponding sex-group achieved PHV for the respective Tanner stage) [95]. However, when authors self-reported dichotomization (e.g., pre-, and post-menarche), this was used for further analysis. Of note, a priori, we considered maturity categorization for comparisons as pre-PHV (i.e., < − 1.0 y PHV), mid-PHV (i.e., -1.0 to 1.0 y PHV), and post-PHV (i.e., > 1.0 y PHV) [48, 51, 67]. However, a posteriori, the insufficient number of studies per outcome and maturity category precluded the categorization.
Moderator Analyses
Subgroup Analyses
The participant’s sex was considered a potential moderator variable because, in addition to the well-known sex-related differences in maturation-related biological processes [66], physical fitness and SSP adaptive responses to PJT programmes may be affected by the participant’s sex [96].
Single Training Factor Analysis
Single training factor analyses were computed for the programme duration (number of weeks and total number of training sessions) [96] and training frequency (number of sessions per week) [97], based on the reported influence of these variables on physical fitness and SSP adaptations following PJT. Additional moderators such as total number of jumps, and type of jump (i.e., unilateral, bilateral, mixed) were also considered if the studies provided such data. Further, as combined training (e.g., PJT combined with traditional controlled-velocity resistance training) may induce different outcomes in comparison to PJT or traditional resistance training in isolation in youth, particularly at different stages of maturity [98], moderator analyses were performed to compare results from studies that delivered PJT only or in conjunction with other training interventions. Given the challenges of determining/quantifying PJT intensity (and the poor reporting of this factor in the literature), this was not considered for the single training factor analysis.
The median split technique was applied as previously recommended and described [99,100,101] for moderator analyses.
Study Methodological Quality
Comparisons of results between studies with ≤ 3 points, 4–5 points, and 6–10 points on the PEDro scale were planned.
Additional Analyses
Certainty of Evidence
The GRADE rating system was applied by two authors (JA and RRC), according to previously published criteria [102,103,104,105,106].
Results
Study Selection
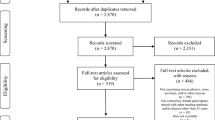
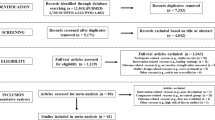
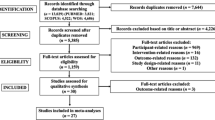
Twenty-nine studies were eligible for qualitative synthesis. Two additional studies were identified through reference list screening [107, 108]. Another 20 studies were discarded (for reasons detailed, see Additional file 5: Table S2). Finally, eleven studies were included in this meta-analysis [109,110,111,112,113,114,115,116,117,118,119] Fig. 1 illustrates the search process and study selection).

Flow chart illustrating the study selection process
Methodological Appraisal of the Included Studies
The eleven included studies had a median (i.e., nonparametric) PEDro score of 5 points. More details can be found in Table 2.
Study Characteristics
Tables 3 and 4 provide a description of the study participant characteristics and PJT interventions. More information on the control groups and whether active or passive can be found in Additional file 2.
Briefly, participants involved in PJT totalled 367 (28 groups), and control participants totalled 377 (28 groups). Seven studies recruited male participants and four studies recruited female participants (Table 3). Seven studies reported maturity using PHV and four studies using Tanner staging (Table 3). Between one and three weekly exercise sessions were applied in the PJT interventions. The exercise programmes lasted between 4 and 36 weeks. Most studies (n = 10) had an exercise period of no more than 8 weeks, with a median duration of ~ 7 weeks. The PJT intensity (Table 4) was reported in eight studies, through different indices (e.g., reactive strength index [RSI]; height/distance; jump technique [e.g., from two-leg to one-leg; landing technique]).
Meta-analyses
Table 5 and Fig. 2 summarise the main values derived from the meta-analyses. A detailed presentation of the meta-analyses per outcome, including figures, 95% CI values, I2 statistics, and other results, is provided in the Additional file 1: Figures S1-S24.

Upper figure: changes in physical fitness and sport-specific performance outcomes after PJT compared to controls in both pre-PHV and post-PHV participants. Lower figure: changes in outcomes after PJT in pre-PHV compared to post-PHV participants. CMJ: countermovement jump. COD: change of direction speed time. PHV: peak height velocity. PJT: plyometric jump training. RSI: reactive strength index
When compared to controls, both pre-PHV and post-PHV participants obtained small-moderate improvements (ES = 0.35 − 0.80) in most outcomes (i.e., SSP [soccer ball kicking velocity/distance; soccer ball dribbling velocity]; maximal dynamic strength; linear sprint; horizontal jump; RSI) after PJT. However, COD speed (ES = 0.51 − 0.62, p = 0.149–0.075) and CMJ height (ES = 0.36 − 0.50, p = 0.088 − 0.061) were not significantly improved in both pre-PHV and post-PHV participants after PJT when compared to controls. The SJ height improved after PJT to a small magnitude in both pre-PHV and post-PHV participants compared to controls (ES = 0.46 − 0.20, respectively), although only significantly in the former.
When pre-PHV and post-PHV participants involved in PJT were compared, no significant differences were noted between maturity groups regarding changes in most physical fitness and SSP outcomes, except COD speed (small ES = -0.42, favouring pre-PHV participants).
Meta-analyses According to Moderators
The Additional file 3 provides a full description of meta-analyses according to moderators. Briefly, no significant effects were noted for any moderator, including participants’ sex, PJT programme duration (number of weeks and total number of training sessions), PJT programme total number of jumps, and studies' methodological quality.
Certainty of Evidence
The GRADE analyses are provided in Table 6. According to the GRADE assessments, the certainty of evidence was considered low to very low across outcomes and groups comparisons.
Discussion
This systematic review with meta-analysis set out to analyse the body of peer-reviewed articles assessing the effects of PJT on physical fitness and SSP outcomes according to participants’ maturity status. Overall, the between-maturity group comparisons were non-significant, except for COD. A discussion is provided regarding current findings, including the potential role of incidental, casual, and statistical artefacts, as well as potential deeper mechanisms that should be explored in future studies, and the role of potential moderators. Indeed, the non-significant role of maturity on physical fitness and SSP adaptation after PJT is somewhat surprising. Indeed, most of the original studies included in our systematic review [109,110,111,112,113,114,115,116,117,118,119] and comparative studies [37, 48, 50,51,52, 54] found that maturity moderated PJT effects. Moreover, it is worth noting that the range of improvement for the different physical fitness and SSP outcomes after PJT in the pre-PHV group was relatively reduced with ES values from 0.35 (maximal dynamic strength) to 0.61 (COD speed time). In comparison, the post-PHV group achieved a wider range of ES values from 0.20 (squat jump height) to 0.82 (SSP). A discussion of the main findings is provided in the following sections.
Maximal Dynamic Strength
In relation to maximal dynamic strength, small significant improvements (ES = 0.35 − 0.46, all p < 0.05) were noted in pre-PHV and post-PHV participants after PJT, as compared to control groups. Furthermore, such improvements were similar for both the pre-PHV and post-PHV participants. These observations remained after meta-analyses of relevant moderators of the main effect which included the participants’ sex, the PJT programme duration (number of weeks and total number of training sessions), the total number of jumps in the programme and methodological quality of the studies. It was unsurprising that only small improvements were seen in both the pre-PHV and post-PHV groups when one considers the principle of specific adaptation to imposed demands in relation to training. It is likely that for larger increases in maximal dynamic strength to occur, the study participants would need to have been exposed to more appropriate exercises to achieve that outcome such as traditional resistance training with higher external loads. Indeed, a previous meta-analysis [120] reported a trivial effect (ES = 0.16) and a large effect (ES = 1.14) for lower body strength in youth participants after power training and strength training, respectively.
Although muscular strength might improve in line with advancing age and maturity, the specific effects of puberty may not always be noticed in the short-term. This could occur because there is a mismatch between the meaningful rate of physical changes and the time that the neural system requires to adapt to them [38, 66, 71]. Further, most studies in our meta-analyses had a duration of < 12 weeks. During such a short timeframe, physiological adaptations can most likely be attributed to neuromuscular improvements (e.g., motor unit recruitment and firing rate) [25, 121]. However, longer-term training interventions (> 12 weeks) may increase the relative contribution of muscle hypertrophy to training-related adaptations [121], thus inducing greater strength gains over longer training periods [122]. Older youths may exhibit a better hormonal milieu (e.g., higher testosterone levels) for muscle hypertrophy to occur as compared to younger youths who lack this characteristic [38]. As PJT can exert a considerable hypertrophic effect [123, 124], greater strength improvements, as a result of a higher potential for muscular hypertrophy, in post-PHV as compared to pre-PHV participants might be expected in the longer-term (e.g., > 12 weeks). Despite this, amongst the studies we meta-analysed, one PJT intervention of 36 weeks [111] produced no significant differences in the maximal dynamic strength of the leg extensors between pre-PHV and post-PHV participants. The cited study [111] included female participants only, a population which may be less likely to exhibit hypertrophic responses to training [101]. Accordingly, it remains unclear whether PJT can induce greater strength improvements (via greater hypertrophy) in post-PHV as compared to pre-PHV male youths. Future studies must incorporate more robust analyses particularly considering the low to very low certainty of evidence (Table 6) for maximal strength changes after PJT in both pre-PHV and post-PHV participants.
Jump-Related Performance
In relation to jump-related measures, when compared to their maturity-matched control group counterparts, pre-PHV participants had larger gains in RSI than post-PHV participants, particularly in males (ES = moderate vs. small; albeit non-significant). This appears to match with the synergistic adaptation theory which suggests that training adaptations are amplified in line with the similar physiological changes that occur in the body during growth and maturation [37, 112, 125]. Of particular importance is muscular fitness, which is an umbrella term for muscle strength, muscle power and muscle endurance [126]. Indeed, youths in pre-PHV can experience an accelerated development of explosive strength (e.g., rate of force development) and muscular power during a period that may be optimal for increasing muscular fitness through training [48, 127]. The horizontal jump movement requires greater absolute force production for execution and likely targets a different expression of the stretch–shortening cycle (SSC) when compared to the RSI, which might favour the nature of the type of adaptations experienced by post-PHV participants exposed to PJT [37, 112, 125]. Indeed, albeit a non-significant difference was noted for the effect of PJT on the horizontal jump performance change in male post-PHV compared to pre-PHV youths (ES = 0.20; p = 0.285), male post-PHV youths attained a greater (ES = 0.59) horizontal jump improvement when compared to their pre-PHV counterparts (ES = 0.32).
Of note, the SJ improved significantly when compared to control subjects only in pre-PHV group (ES = 0.46), a result that might be related to the low specificity between PJT exercises (i.e., involving the SSC) and SJ (i.e., shortening muscle action). Although this is true for both pre-PHV and post-PHV groups, the low training specificity (e.g., type of jump; reduced inter-set recovery) may affect post-PHV participants’ muscular fitness to a larger extent [37, 43, 115]. For example, pre-PHV participants may obtain a greater concentric stimulus from PJT than post-PHV participants because of differences in muscle activation patterns [128]. Indeed, post-PHV participants can exhibit a more excitatory muscle activation pattern during PJT activities, and thus more activity will arise from pre-activation and stretch reflexes, meaning greater contribution from eccentric activation [128]. Pre-PHV participants will have a more inhibitory response of the aforementioned mechanisms, and thus be more reliant on muscle activation during the propulsive/concentric phase [128]. Indeed, among the analysed outcomes in our meta-analyses, the SJ showed the lowest magnitude in terms of performance improvement after PJT in post-PHV participants while it was the fifth lowest for the pre-PHV participants. However, the extent to which youth participants (and most particularly those in post-PHV) are sensitive to the transference effect [27, 129,130,131,132,133,134] of PJT activities to a given testing exercise (e.g., concentric-only vs. SSC-based; vertical vs. horizontal; unilateral vs. bilateral), remains to be elucidated. From a practical point of view, although specificity of training is a key element of adaptation [120], a combination with non-specific PJT exercises may offer greater adaptations [27, 134, 135], particularly for athletes already performing specific jumps in the main training session. Indeed, merely replicating those jumps would repeat the same training stimulus, potentially contributing to overuse injuries [136,137,138].
For CMJ, the magnitude of change was in favour of the PJT groups compared with controls in pre-PHV (ES = 0.50, p = 0.088) and post-PHV participants (ES = 0.36, p = 0.061). However, neither result achieved the level of statistical significance. Whether the experimental groups were exposed to insufficient PJT doses is unclear, as the minimal effective dose has not been clarified in the literature. However, our moderator analyses revealed no effect of dose, in the form of PJT number of weeks, PJT number of training sessions, or PJT programme total number of jumps. Another possible explanation for the lack of significant differences between PJT participants and their controls is the training level of the controls. The included studies used school-based physical education (n = 3) as well as sport-specific activity (n = 4) as control conditions. Both control conditions involve habitual engagement in play activities, exercise drills and sports-related activities that mimic the nature of PJT exercises, such as jumps, sprints, and quick changes of direction. Such active-control conditions may have induced physiological adaptations favouring jump performance. At the same time, expected PJT effects compared with these active controls might be diminished. Another potential reason may be related to the sex of the participants. Previous meta-analyses reported a lower magnitude of CMJ performance improvement in females (ES = 0.57) [52] compared to males (ES = 0.73) [48] after PJT interventions. Indeed, in our meta-analyses the PJT-control comparisons indicated that males involved in PJT achieved small-moderate CMJ height improvements (ES = 0.51 − 0.87) compared to their maturity-matched controls. In contrast, the PJT-control comparison for the females involved in PJT revealed a trivial CMJ height improvement (ES = 0.12 − 0.16) compared to their maturity-matched controls. However, the moderator analysis according to participants’ sex indicated that pre-PHV and post-PHV participants responded similarly to PJT in relation to the outcome of CMJ height.
Sprinting and Sport-Specific Performance
Maximal-intensity short-duration linear and COD running movements frequently occur in youth male and female basketball (every 1–2 s), soccer (every 3–6 s), and handball (every 5–6 s) matches [139, 140], and are common before scoring actions in sports, such as soccer [141]. Muscular strength and power (e.g., jumping), speed, rate of force development, cognitive and technical skills correlate well with linear and COD running performance across sex, age, and sports disciplines [80, 81, 142,143,144,145,146,147,148,149,150,151,152,153,154,155,156]. Indeed, linear and COD running performance markers may reflect physiological and biomechanical indicators relevant to reducing injury risk and improving SSP [51, 74, 75, 143,144,145,146]. Different training methods with the potential to improve linear and COD running performance (e.g., complex training, sprint training) have been reported in the scientific literature [148, 157,158,159,160,161,162]. However, PJT appears to be one of the most effective exercise types, requiring fast and powerful movements that utilise the SSC. Indeed, PJT has previously resulted in favourable effects on linear and COD running performance [80, 163] and repeated sprint ability with and without COD [35, 36, 164, 165], in line with improvements in the physiological [25, 166] determinants of linear and COD running performance and associated muscular fitness components such as maximal dynamic strength [97] and jumping capability [167]. Our meta-analyses indicate that linear and COD running performance attained up to moderate magnitude of improvement (ES = 0.38 − 0.62) after PJT in both pre-PHV and post-PHV participants, even when control participants were recreationally active or engaged in sport-specific activity. Of note, linear sprinting improved after PJT compared to controls in both pre-PHV and post-PHV. However, COD running performance achieved magnitudes of improvement of 0.62 and 0.51 for pre-PHV and post-PHV participants respectively following PJT compared to controls, but without statistical significance. When compared to control subjects, these groups were involved in three school-based physical education control groups, and one soccer-specific active control group. Therefore, the fact that control participants were active (school-based physical education; sport-specific active) may partially explain the non-significant COD findings in the pre-PHV and post-PHV participants. Alternative explanatory hypotheses, such as the different proportion of studies conducted on males and females for linear sprinting speed time (5:1, respectively) compared to COD speed time (1:3, respectively), or whether (or not) the dosage of PJT applied was sufficient compared to active controls (moderator analysis precluded due to insufficient studies), warrant future assessment.
In relation to maturity status, pre-PHV participants exposed to PJT improved COD significantly more than post-PHV participants. Thus, the early incorporation of PJT into youth training schedules may offer significant advantages. Of note, all studies included in the meta-analysis assessed pre-programmed COD (i.e., movement with a pre-determined course that was known to the participant). However, the effects of PJT on COD with an unpredictable, reactive, and unplanned component should be considered in future studies. Post-PHV athletes, when compared to pre-PHV participants, might be faster in performing reactive-decisional based COD, as they will likely tend to have greater playing experience in line with cognitive development. However, this is speculative, further highlighting the need for additional investigation in the area. The underlying mechanisms for the greater improvement in COD after PJT in pre-PHV as compared to post-PHV participants are unclear, though they could potentially be related to decreases in relative strength owing to increases in the body mass of the more mature participants [168]. On the other hand, some COD tasks incorporate a cognitive element in performance and due to the heightened neural plasticity that can be experienced in pre-PHV participants, this group may be particularly sensitive to the effects of PJT, particularly considering its meaningful effects on the neuromuscular system [25, 169, 170]. It would be relevant to elucidate changes between pre- and post-PHV participants in maximal concentric and eccentric strength and the relationship of these changes with the change in different phases (e.g., acceleration; deceleration; turns to the right-left; joint and trunk angles during COD and risk of injury) of linear and COD running movements, as well as in COD deficit [171]. During growth and maturation, a cascade of biological events lead to rapid increases in stature, potential temporary disruption to motor co-ordination, large increases in fat-free mass and changes to muscle–tendon architecture [37,38,39], all of which may influence an individual’s responsiveness to PJT. More specifically, the maturity-related effects of PJT on linear and COD running performance and the underlying mechanisms of adaptations require further investigation.
The largest improvement among the meta-analysed outcomes in the post-PHV group was noted for SSP (ES = 0.82) and the third highest in the pre-PHV group (ES = 0.55). Because participants were taking part in PJT while also taking part in their normal sports training (i.e., they were training both PJT and sport specific skills), this partially supports the hypothesis related to the meaningful transference of PJT-related adaptive effects to athletic performance [27, 129,130,131,132,133,134, 172], particularly in post-PHV participants. Most of the studies that assessed SSP tested ball kicking velocity/distance with the one exception evaluating dribbling velocity [51]. However, when removed from the analysis, the results remained consistent across comparisons (details in Additional file 1: Fig. S1, S9 and S17). Of note, SSP data could be derived only from male soccer players. Therefore, it is unclear how PJT and maturity might interact to impact on tests that are specific to other sports or amongst female youths.
Meta-analyses According to Moderators
Sex
In a previous study, similar physical fitness and SSP improvements were noted after PJT in adult male and female participants [173]. However, the findings in adult populations appear inapplicable to youths because the adaptive potential in the latter is different due to the timing and tempo of maturational changes that occur during puberty [37, 41,42,43,44,45,46,47,48]. Indeed, when CMJ was assessed, males attained an ES of 0.87 (pre-PHV) and 0.51 (post-PHV) as compared to their maturity-matched controls, while females attained ES values of just 0.12 and 0.16, respectively. Further, it is notable that the main number of total jumps performed by females among the studies that assessed CMJ was 2,435, while for males it was only 874. This may suggest a diminished PJT efficiency in females calling into question their relative trainability in comparison to males. Alternatively, it is possible that the intensity of type of jumps prescribed were not the most appropriate. Regrettably, moderator analyses were precluded for certain dosing variables of PJT, due to the low number of studies per moderator category, including type of jump. If sex differences are related to the menstrual cycle, this is unclear at present, although the menstrual cycle would not affect athletic performance proxies such as sprint, jump, and force–velocity profile [174,175,176], especially with trained athletes, who are already used to coping with training under the menstrual cycle-related fluctuations.
Nonetheless, our meta-analysis moderated by the sex of the participants indicated non-significant differences between males and females. For the comparison between pre-PHV and post-PHV groups involved in PJT, no significant difference was found between the sexes. Further, for pre-PHV and post-PHV groups compared to controls, no significant differences were found between males and females. Moreover, results among all eight outcome measures included in the meta-analyses (Table 5) remained consistent for ES and p-values when a sex-based sensitivity analysis was performed. Overall, recommendations regarding the role of sex in adaptive responses to PJT in youth populations are rather limited. Indeed, in our meta-analysis, a comparison of results between studies that included males and females was conducted although only for CMJ, as the number of studies available for analysis for other outcomes was insufficient.
Programme Duration (Number of Weeks and Total Number of Training Sessions)
A comparison of results between studies with different programme durations was conducted, although this was only done for RSI and CMJ. We observed no significant effect for programme duration. In relation to RSI, pre-PHV and post-PHV provided data from seven and three groups in studies conducted over periods of ≤ 6 weeks and > 6 weeks respectively. Although the results were not significantly different (p = 0.106) between the ≤ 6 weeks (ES = 0.06) and > 6 weeks (ES = − 0.35) subgroups, four of seven groups involved in ≤ 6 weeks of PJT demonstrated a favourable effect in post-PHV. This resulted in a mean improvement of 4.9% over the pre-PHV participants. In contrast, all three groups involved in training for > 6 weeks showed a favourable effect in pre-PHV, with a mean improvement of 23.6% over the post-PHV participants. These results could suggest that over longer periods of PJT (i.e., > 6 weeks), pre-PHV participants may develop greater RSI improvements compared to their post-PHV counterparts. However, considering the potentially greater effects of power-strength training on physical fitness (i.e., jump, sprint) of untrained compared to trained youth [120], and since the participants’ experience with PJT before interventions was rarely well documented, it is difficult to determine if a greater RSI adaptive response to PJT may be moderated by previous exposure to this type of training (i.e., training history) compared to maturity. Relatedly, it is difficult to attribute these observations to optimal progressive overload during PJT. Firstly, this is because there is a lack of studies addressing optimization strategies for progressive overload in PJT [35, 36]. Secondly, amongst the studies that applied PJT for different durations, relatively similar progressive overload strategies were utilised through the manipulation of volume, technique, or a combination of both (Table 4). Accordingly, further studies are needed to elucidate optimal PJT progressions and to determine how these might interact with maturity to help youth athletes to avoid reaching stagnation following initial adaptation.
Certainty of Evidence (GRADE)
For most outcomes, we would provide a weak recommendation in favour of PJT compared to controls (involving both sport-specific active controls and active controls involved in physical education classes), while for very low certainty cases, no recommendation would be advisable. For all comparisons not analysed meta-analytically, a very low certainty of evidence is suggested. Overall, low to very low certainty of evidence is currently apparent for PJT versus control studies and very low in relation to pre-PHV versus post-PHV participants exposed to PJT.
Limitations and Recommendations for Future Research
Firstly, a relatively small number of available studies (n = 11) were included. Although a considerable number of PJT studies were found (Fig. 1), most of these were excluded at the eligibility stage because they did not report participants’ maturity status. Future studies are encouraged to report participants’ maturity status so that more accurate inferences on the adaptability of youths to exercise can be established. Secondly, a priori we considered maturity categories of ‘pre-PHV’ (i.e., < − 1.0 y PHV), ‘mid-PHV’ (i.e., − 1.0 to 1.0 y PHV), and ‘post-PHV’ (i.e., > 1.0 y PHV) [48, 51, 67] (for the full planned procedures, see the Registration section). However, a posteriori, there was an insufficient number of studies per outcome and maturity category, and this precluded the use of the ‘pre-PHV’, ‘mid-PHV’, and ‘post-PHV’ categories. Thirdly, moderator analyses were planned. However, only RSI and/or CMJ were available for such an evaluation. Further, some moderator analyses were precluded for certain dosing variables of PJT, due to the low number of studies per moderator category, including training frequency, type of jump, and studies that delivered PJT only or in conjunction with other training interventions. Fourthly, due to the limited number of studies, the analysis of the effects of PJT on outcomes such as body composition [29, 123, 124], cardiovascular fitness and health-related outcomes [177, 178] was precluded. Fifthly, the analysis for a potential ceiling effect was precluded, since most studies provided no report of participants’ previous experience with/exposure to PJT training (and training in general). Future studies should compare pre-PHV and post-PHV participants considering the amount of previous exposition to a certain intervention, including PJT.
Implications of the Findings for Sport Practice
Evidence-based practical recommendations for PJT programming to improve the physical fitness of youths is provided in Table 7. However, an evidence-based proposal for optimal PJT programming according to maturity was precluded, due to the limitations of the currently available literature (previously exposed in this systematic review). Nonetheless, the information provided in Table 7 may provide a general framework for PJT programming that would allow safe and effective interventions for physical fitness improvements (compared to maturity-matched controls), irrespective of the maturity status of male and female participants.
An effective dose of PJT would involve ≥ 4 weeks of intervention, 1–2 sessions per week, incorporating multi-type or single-type [e.g., drop jump]) jump exercises. It is recommended to start with a reduced number of jumps per week (e.g., 92) and then progressively increase this number (e.g., by 10% per week). Of note, a total minimal dose of 600–1,000 jumps seems effective to improve most physical fitness outcomes. A progression-variation of jump type-techniques is also advised, particularly for long-term interventions. Regarding the intensity of PJT exercises, a sound technique of jump execution is advised to be attained before reaching high-maximal jump efforts. An inter-set rest of ≤ 120 s seems adequate, and shorter inter-set rest periods may also be effective and would allow reduction of the total duration of training sessions. For jump exercises requiring an inter-repetition rest-pause (e.g., drop jumps), 3–15 s seem adequate. For inter-session recovery, ≥ 48 h may be advised. Surfaces such as grass, wood, parquet, or a combination of surfaces, seem safe and effective to perform jump exercises. Current evidence suggests that PJT is effective either introduced as an additional load or to replace standard training (or if a taper approach is applied). However, practitioners are advised to take such a decision depending on the fitness characteristics of the participants and their current level of training and competition. It is advised that PJT be incorporated into a comprehensive multicomponent training approach for youths, with long-term training and performance development aims [75, 179, 180].
Conclusion
Compared to control participants, pre- and post-PHV youths performing PJT experienced improved maximal dynamic strength, linear sprint speed, horizontal jump distance, RSI, and SSP (i.e., soccer ball kicking and dribbling velocity). These effects seem to occur independently of maturity status, as both pre-PHV and post-PHV participants achieved similar improvements following PJT interventions for most outcomes. However, several methodological issues (e.g., low sample sizes and the pooling of maturity categories) preclude the attainment of more robust recommendations at the current time. To address this issue in future studies with youth and youth athletes, the measurement of maturity status through skeletal age, Tanner stages, or anthropometric assessment methods is key and should be systematically reported in future studies with youth and youth athletes.
Registration
The protocol for this systematic review with meta-analysis was published in the Open Science platform (OSF) on March 8, 2022. Link to project: https://osf.io/nd6w7/. Link to registration: https://osf.io/8dybe.
Availability of Data and Materials
All data generated or analysed during this study are included in the article as Table(s), Figure(s), and/or Electronic Supplementary Material(s). Any other data requirement can be directed to the corresponding author upon reasonable request.
Abbreviations
- CI:
-
Confidence interval
- CMJ:
-
Countermovement jump
- COD:
-
Change of direction
- ES:
-
Effect size
- GRADE:
-
Grading of recommendations assessment, development, and evaluation
- OSF:
-
Open Science platform
- PEDro:
-
Physiotherapy evidence database
- PHV:
-
Age at peak height velocity
- PICOS:
-
Participants, intervention, comparators, outcomes, and study design
- PJT:
-
Plyometric jump training
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RSI:
-
Reactive strength index
- SJ:
-
Squat jump
- SSC:
-
Stretch–shortening cycle
- SSP:
-
Sport-specific performance
References
Cadenas-Sanchez C, Mena-Molina A, Torres-Lopez LV, Migueles JH, Rodriguez-Ayllon M, Lubans DR, et al. Healthier minds in fitter bodies: a systematic review and meta-analysis of the association between physical fitness and mental health in youth. Sports Med. 2021;51(12):2571–605.
Garcia-Hermoso A, Ramirez-Campillo R, Izquierdo M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019;49(7):1079–94.
Orsso CE, Tibaes JRB, Oliveira CLP, Rubin DA, Field CJ, Heymsfield SB, et al. Low muscle mass and strength in pediatrics patients: Why should we care? Clinical Nutr (Edinburgh, Scotland). 2019;38(5):2002–15.
McKay HA, MacLean L, Petit M, MacKelvie-O’Brien K, Janssen P, Beck T, et al. “Bounce at the Bell”: a novel program of short bouts of exercise improves proximal femur bone mass in early pubertal children. Brit J Sports Med. 2005;39(8):521.
Li H-Q, Spitzer NC. Exercise enhances motor skill learning by neurotransmitter switching in the adult midbrain. Nature Commun. 2020;11(1):2195.
Behringer M, Vom Heede A, Matthews M, Mester J. Effects of strength training on motor performance skills in children and adolescents: a meta-analysis. Pediatr Exerc Sci. 2011;23(2):186–206.
Duncan MJ, Eyre ELJ, Oxford SW. The effects of 10-week integrated neuromuscular training on fundamental movement skills and physical self-efficacy in 6-7-year-old children. J Strength Cond Res. 2018;32(12):3348–56.
Sortwell A, Newton M, Marinho DA, Ferraz R, Perlman D. The effects of an eight week plyometric-based program on motor performance skills and muscular power in 7–8-year-old primary school students. Int J Kinesiol Sports Sci. 2021;9(4):1–12.
Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Physical fitness, injuries, and team performance in soccer. Med Sci Sports Exerc. 2004;36(2):278–85.
Lisman PJ, de la Motte SJ, Gribbin TC, Jaffin DP, Murphy K, Deuster PA. A systematic review of the association between physical fitness and musculoskeletal injury risk: part 1-cardiorespiratory endurance. J Strength Cond Res. 2017;31(6):1744–57.
de la Motte SJ, Gribbin TC, Lisman P, Murphy K, Deuster PA. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 2-muscular endurance and muscular strength. J Strength Cond Res. 2017;31(11):3218–34.
de la Motte SJ, Lisman P, Gribbin TC, Murphy K, Deuster PA. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 3-flexibility, power, speed, balance, and agility. J Strength Cond Res. 2019;33(6):1723–35.
Blažević I, Benassi L, Šterpin A. Material working conditions in teaching physical education. Econ Res. 2020;33(1):1240–54.
Osborne R, Belmont RS, Peixoto RP. Obstacles for physical education teachers in public schools: an unsustainable situation. Motriz Rev Educ Fis. 2016;22(4):310–8.
Ward P, Hodges N, Williams AM. The road excellence in soccer: Deliberate practice and the development of expertise. High Abil Stud. 2007;18(2):119–53.
Aagaard M. Rope jumping fitness: The complete guide to jump rope fitness. Kobehavn: Denmark. 2012.
Arnett MG, Lutz B. Effects of rope-jump training on the os calcis stiffness index of postpubescent girls. Med Sci Sports Exerc. 2002;34(12):1913–9.
Ache-Dias J, Dellagrana RA, Teixeira AS, Dal Pupo J, Moro AR. Effect of jumping interval training on neuromuscular and physiological parameters: a randomized controlled study. Appl Physiol Nutr Metab. 2016;41(1):20–5.
Chen L. The impact of rope jumping exercise on physical fitness of visually impaired students. Res Develop Disabil. 2011;32(1):25–9.
Garcia-Pinillos F, Lago-Fuentes C, Latorre-Roman PA, Pantoja-Vallejo A, Ramirez-Campillo R. Jump-rope training: improved 3-km time-trial performance in endurance runners via enhanced lower-limb reactivity and foot-arch stiffness. Int J Sports Physiol Perform. 2020;15(7):927–33.
Ha A, Sum R, Chan C, Ng JYY. Promoting rope skipping at Hong Kong schools with low and mid socioeconomic statuses: an ecological perspective. Int Rev Soc Sci. 2014;2:104–15.
Faigenbaum AD, Lloyd RS, MacDonald J, Myer GD. Citius, Altius, Fortius: beneficial effects of resistance training for young athletes: Narrative review. Br J Sports Med. 2016;50(1):3–7.
Kontulainen SA, Kannus PA, Pasanen ME, Sievanen HT, Heinonen AO, Oja P, et al. Does previous participation in high-impact training result in residual bone gain in growing girls? One year follow-up of a 9-month jumping intervention. Int J Sports Med. 2002;23(8):575–81.
Markovic G, Mikulic P. Plyometric training effects on muscle function and rapid movement performance: a review. Adv Strength Cond Res; 2009. p. 157–88.
Markovic G, Mikulic P. Neuro-musculoskeletal and performance adaptations to lower-extremity plyometric training. Sports Med. 2010;40(10):859–95.
Ramirez-Campillo R, Castillo D, Raya-González J, Moran J, de Villarreal ES, Lloyd RS. Effects of plyometric jump training on jump and sprint performance in young male soccer players: a systematic review and meta-analysis. Sports Med. 2020.
Ramirez-Campillo R, Gallardo F, Henriquez-Olguin C, Meylan CM, Martinez C, Alvarez C, et al. Effect of vertical, horizontal, and combined plyometric training on explosive, balance, and endurance performance of young soccer players. J Strength Cond Res. 2015;29(7):1784–95.
Sortwell A, Newton M, Marinho DA, Knijnik J, Ramirez-Campillo R. Potential role of plyometric training in the development of motor performance skills: a narrative review. Kinesiol Rev. 2022;11(2):158–70.
Ramirez-Campillo R, García-Pinillos F, T. Nikolaidis P, Clemente F, Gentil P, García-Hermoso A. Body composition adaptations to lower-body plyometric training: a systematic review and meta-analysis. Biol Sport. 2021:273–87.
Kramer A, Poppendieker T, Gruber M. Suitability of jumps as a form of high-intensity interval training: effect of rest duration on oxygen uptake, heart rate and blood lactate. Eur J Appl Physiol. 2019;119(5):1149–56.
Ducrocq GP, Hureau TJ, Meste O, Blain GM. Similar cardioventilatory but greater neuromuscular stimuli with interval drop jump than with interval running. Int J Sports Physiol Perform. 2019;17:1–10.
Racil G, Zouhal H, Elmontassar W, Abderrahmane AB, De Sousa MV, Chamari K, et al. Plyometric exercise combined with high-intensity interval training improves metabolic abnormalities in young obese females more so than interval training alone. Appl Physiol, Nut Metabolism. 2015;41(1):103–9.
Arazi H, Jalali-Fard A, Abdinejad H. A comparison of two aerobic training methods (running vs rope jumping) on health-related physical fitness in 10 to 12 years old boy. Phys Act Rev. 2016;4:9–17.
Faigenbaum AD, Kraemer WJ, Blimkie CJ, Jeffreys I, Micheli LJ, Nitka M, et al. Youth resistance training: updated position statement paper from the national strength and conditioning association. J Strength Cond Res. 2009;23(5 Suppl):S60-79.
Ramirez-Campillo R, Alvarez C, Garcia-Hermoso A, Ramirez-Velez R, Gentil P, Asadi A, et al. Methodological characteristics and future directions for plyometric jump training research: a scoping review. Sports Med. 2018;48(5):1059–81.
Ramirez-Campillo R, Moran J, Chaabene H, Granacher U, Behm DG, Garcia-Hermoso A, et al. Methodological characteristics and future directions for plyometric jump training research: a scoping review update. Scand J Med Sci Sports. 2020;30(6):983–97.
Radnor JM, Oliver JL, Waugh CM, Myer GD, Moore IS, Lloyd RS. The influence of growth and maturation on stretch-shortening cycle function in youth. Sports Med. 2018;48(1):57–71.
Malina RM, Bouchard C, Bar-Or O. Growth, Maturation, and Physical Activity. IL, Chapaing: Human Kinetics; 2004.
Hirtz P, Starosta W. Sensitive and critical periods of motor co-ordination development and its relation to motor learning. J Hum Kinet. 2002;7:19–28.
Society CP. Age limits and adolescents. Paediatr Child Health. 2003;8(9):577–8.
Marginson V, Eston R. The relationship between torque and joint angle during knee extension in boys and men. J Sports Sci. 2001;19(11):875–80.
Marginson V, Rowlands AV, Gleeson NP, Eston RG. Comparison of the symptoms of exercise-induced muscle damage after an initial and repeated bout of plyometric exercise in men and boys. J Appl Physiol. 2005;99(3):1174–81.
Ratel S, Duche P, Williams CA. Muscle fatigue during high-intensity exercise in children. Sports Med. 2006;36(12):1031–65.
Mersmann F, Bohm S, Arampatzis A. Imbalances in the development of muscle and tendon as risk factor for tendinopathies in youth athletes: a review of current evidence and concepts of prevention. Front Physiol. 2017;8:987.
Mersmann F, Bohm S, Schroll A, Boeth H, Duda G, Arampatzis A. Evidence of imbalanced adaptation between muscle and tendon in adolescent athletes. Scand J Med Sci Sports. 2014;24(4):e283–9.
Mersmann F, Bohm S, Schroll A, Boeth H, Duda GN, Arampatzis A. Muscle and tendon adaptation in adolescent athletes: a longitudinal study. Scand J Med Sci Sports. 2017;27(1):75–82.
Moran J, Liew B, Ramirez-Campillo R, Granacher U, Negra Y, Chaabene H. The effects of plyometric jump training on lower-limb stiffness in healthy individuals: a meta-analytical comparison. J Sport Health Sci. 2021. https://doi.org/10.1016/j.jshs.2021.05.005.
Moran J, Sandercock G, Ramírez-Campillo R, Meylan C, Collison J, Parry D. Age-related variation in male youth athletes’ countermovement jump after plyometric training: A meta-analysis of controlled trials. J Strength Cond Res. 2017;31(2):552–65.
Lloyd RS, Oliver JL, Hughes MG, Williams CA. The influence of chronological age on periods of accelerated adaptation of stretch-shortening cycle performance in pre and postpubescent boys. J Strength Cond Res. 2011;25(7):1889–97.
Meylan C, Cronin J, Oliver J, Hughes M, Manson S. An evidence-based model of power development in youth soccer. Int J Sports Sci Coach. 2014;9(5):1241–64.
Asadi A, Arazi H, Ramirez-Campillo R, Moran J, Izquierdo M. Influence of maturation stage on agility performance gains after plyometric training: a systematic review and meta-analysis. J Strength Cond Res. 2017;31(9):2609–17.
Moran J, Clark CCT, Ramirez-Campillo R, Davies MJ, Drury B. A meta-analysis of plyometric training in female youth: its efficacy and shortcomings in the literature. J Strength Cond Res. 2019;33(7):1996–2008.
McNarry MA, Lloyd RS, Buchheit M, Williams CA, Oliver JL. The bases expert statement on trainability during childhood and adolescence. Sport Exerc Scientist. 2014;41:22–3.
Peitz M, Behringer M, Granacher U. A systematic review on the effects of resistance and plyometric training on physical fitness in youth—What do comparative studies tell us? PLoS ONE. 2018. https://doi.org/10.1371/journal.pone.0205525.
Jayanthi N, Schley S, Cumming SP, Myer GD, Saffel H, Hartwig T, et al. Developmental training model for the sport specialized youth athlete: a dynamic strategy for individualizing load-response during maturation. Sports health. 2022;14(1):142–53.
Cumming SP, Lloyd RS, Oliver JL, Eisenmann JC, Malina RM. Bio-banding in sport: applications to competition, talent identification, and strength and conditioning of youth athletes. Strength Cond J. 2017;39(2):34–47.
Abt G, Boreham C, Davison G, Jackson R, Nevill A, Wallace E, et al. Power, precision, and sample size estimation in sport and exercise science research. J Sports Sci. 2020;38(17):1933–5.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339: b2700.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29(372): n71.
Brooker J, Synnot A, McDonald S, Elliott J, Turner T. Guidance for the production and publication of Cochrane living systematic reviews: Cochrane Reviews in living mode. Cochranne resources: https://communitycochraneorg/review-production/production-resources/living-systematic-reviews. 2019.
Vergara-Merino L, Verdejo C, Carrasco C, Vargas-Peirano M. Living systematic review: new inputs and challenges. Medwave. 2020;20(11): e8092.
Elliott JH, Synnot A, Turner T, Simmonds M, Akl EA, McDonald S, et al. Living systematic review: 1. Introduction-the why, what, when, and how. J Clin Epidemiol. 2017;91:23–30.
van der Vlist AC, Winters M, Weir A, Ardern CL, Welton NJ, Caldwell DM, et al. Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. Br J Sports Med. 2021;55(5):249–56.
Ardern CL, Büttner F, Andrade R, Weir A, Ashe MC, Holden S, et al. Implementing the 27 PRISMA 2020 Statement items for systematic reviews in the sport and exercise medicine, musculoskeletal rehabilitation and sports science fields: the PERSiST (implementing Prisma in Exercise, Rehabilitation, Sport medicine and SporTs science) guidance. Br J Sports Med. 2022;56(4):175–95.
Elliott JH, Turner T, Clavisi O, Thomas J, Higgins JP, Mavergames C, et al. Living systematic reviews: an emerging opportunity to narrow the evidence-practice gap. PLoS Med. 2014;11(2): e1001603.
Tanner J. Growth of Adolescents. Oxford, UK: Blackwell Scientific Publications; 1962.
Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP. An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc. 2002;34(4):689–94.
Moore SA, McKay HA, Macdonald H, Nettlefold L, Baxter-Jones AD, Cameron N, et al. Enhancing a somatic maturity prediction model. Med Sci Sports Exerc. 2015;47(8):1755–64.
Khamis HJ, Roche AF. Predicting adult stature without using skeletal age: the Khamis-Roche method. Pediatrics. 1994;94(4 Pt 1):504–7.
Chumela WC, Roche AF, Thissen D. The FELS method of assessing the skeletal maturity of the hand-wrist. Amer J Human Biol. 1989;1(2):175–83.
Malina RM, Rogol AD, Cumming SP, Coelho e Silva MJ, Figueiredo AJ. Biological maturation of youth athletes: assessment and implications. Br J Sports Med. 2015;49(13):852–9.
García-Hermoso A, Alonso-Martínez AM, Ramírez-Vélez R, Pérez-Sousa M, Ramírez-Campillo R, Izquierdo M. Association of physical education with improvement of health-related physical fitness outcomes and fundamental motor skills among youths: a systematic review and meta-analysis. JAMA Pediatr. 2020;174(6): e200223.
Garcia-Hermoso A, Ramirez-Velez R, Ramirez-Campillo R, Peterson MD, Martinez-Vizcaino V. Concurrent aerobic plus resistance exercise versus aerobic exercise alone to improve health outcomes in paediatric obesity: a systematic review and meta-analysis. Br J Sports Med. 2018;52(3):161–6.
Reilly T, Bangsbo J, Franks A. Anthropometric and physiological predispositions for elite soccer. J Sports Sci. 2000;18(9):669–83.
Lloyd RS, Cronin JB, Faigenbaum AD, Haff GG, Howard R, Kraemer WJ, et al. National strength and conditioning association position statement on long-term athletic development. J Strength Cond Res. 2016;30(6):1491–509.
Slinde F, Suber C, Suber L, Edwen CE, Svantesson U. Test-retest reliability of three different countermovement jumping tests. J Strength Cond Res. 2008;22(2):640–4.
Altmann S, Ringhof S, Neumann R, Woll A, Rumpf MC. Validity and reliability of speed tests used in soccer: a systematic review. PLoS ONE. 2019;14(8): e0220982.
Grgic J, Lazinica B, Schoenfeld BJ, Pedisic Z. Test-retest reliability of the one-repetition maximum (1RM) strength testassessment: a systematic review. Sports Med Open. 2020;In press.
Bangsbo J, Iaia FM, Krustrup P. The Yo-Yo intermittent recovery test: a useful tool for evaluation of physical performance in intermittent sports. Sports Med. 2008;38(1):37–51.
Asadi A, Arazi H, Young WB, Saez de Villarreal E. The effects of plyometric training on change-of-direction ability: a meta-analysis. Int J Sports Physiol Perform. 2016;11(5):563–73.
Sheppard JM, Young WB. Agility literature review: classifications, training and testing. J Sports Sci. 2006;24(9):919–32.
Drevon D, Fursa SR, Malcolm AL. Intercoder reliability and validity of WebPlotDigitizer in extracting graphed data. Behav Modif. 2016;41(2):323–39.
de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Australian Journal of Physiotherapy. 2009;55(2):129–33.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–21.
Yamato TP, Maher C, Koes B, Moseley A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J Clin Epidemiol. 2017;86:176–81.
Stojanović E, Ristić V, McMaster DT, Milanović Z. Effect of plyometric training on vertical jump performance in female athletes: a systematic review and meta-analysis. Sports Med. 2017;47(5):975–86.
Cashin AG, McAuley JH. Clinimetrics: physiotherapy evidence database (PEDro) Scale. J Physiother. 2020;66(1):59.
Ramirez-Campillo R, Sanchez-Sanchez J, Romero-Moraleda B, Yanci J, Garcia-Hermoso A, Manuel CF. Effects of plyometric jump training in female soccer player’s vertical jump height: a systematic review with meta-analysis. J Sports Sci. 2020;38(13):1475–87.
Valentine JC, Pigott TD, Rothstein HR. How many studies do you need?: A primer on statistical power for meta-analysis. J Ed Behavioral Stat. 2010;35(2):215–47.
Pigott T. Advances in meta-analysis. Springer-Verlag New York; 2012.
Moran J, Ramirez-Campillo R, Granacher U. Effects of jumping exercise on muscular power in older adults: a meta-analysis. Sports Med. 2018;48(12):2843–57.
Hopkins WG, Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. 2009;41(1):3–13.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Muller L, Muller E, Hildebrandt C, Kapelari K, Raschner C. The assessment of biological maturation for talent selection—Which method can be used? Sportverletz Sportschaden. 2015;29(1):56–63.
Granados A, Gebremariam A, Lee JM. Relationship between timing of peak height velocity and pubertal staging in boys and girls. J Clin Res Pediatr Endocrinol. 2015;7(3):235–7.
Sáez de Villarreal E, Kellis E, Kraemer WJ, Izquierdo M. Determining variables of plyometric training for improving vertical jump height performance: a meta-analysis. J Strength Cond Res. 2009;23(2):495–506.
Sáez de Villarreal E, Requena B, Newton RU. Does plyometric training improve strength performance? A meta-analysis. J Sci Med Sport. 2010;13(5):513–22.
Radnor JM, Lloyd RS, Oliver JL. Individual response to different forms of resistance training in school-aged boys. J Strength Cond Res. 2017;31(3):787–97.
Moran J, Clark CCT, Ramirez-Campillo R, Davies MJ, Drury B. A meta-analysis of plyometric training in female youth: its efficacy and shortcomings in the literature. J Strength Cond Res. In Press.
Moran J, Sandercock G, Ramirez-Campillo R, Clark CCT, Fernandes JFT, Drury B. A meta-analysis of resistance training in female youth: its effect on muscular strength, and shortcomings in the literature. Sports Med. 2018;48:1661–71.
Moran J, Sandercock GR, Ramirez-Campillo R, Meylan C, Collison J, Parry DA. A meta-analysis of maturation-related variation in adolescent boy athletes’ adaptations to short-term resistance training. J Sports Sci. 2017;35(11):1041–51.
Guyatt GH, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Zhang Y, Alonso-Coello P, Guyatt GH, Yepes-Nuñez JJ, Akl EA, Hazlewood G, et al. GRADE Guidelines: 19. Assessing the certainty of evidence in the importance of outcomes or values and preferences—risk of bias and indirectness. J Clin Epidemiol. 2019;111:94–104.
Zhang Y, Coello PA, Guyatt GH, Yepes-Nuñez JJ, Akl EA, Hazlewood G, et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences—inconsistency, imprecision, and other domains. J Clin Epidemiol. 2019;111:83–93.
Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. Corrigendum to GRADE guidelines 6. Rating the quality of evidence-imprecision. J Clin Epidemiol. 2011;64:1283–93.
Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. Corrigendum to GRADE guidelines 6. Rating the quality of evidence-imprecision. J Clinic Epidemiol. 2021;137:265.
Marta CC, Marinho DA, Izquierdo M, Marques MC. Differentiating maturational influence on training-induced strength and endurance adaptations in prepubescent children. Am J Hum Biol Off J Hum Biol Counc. 2014;26(4):469–75.
Pena-Gonzalez I, Fernandez-Fernandez J, Cervello E, Moya-Ramon M. Effect of biological maturation on strength-related adaptations in young soccer players. PLoS ONE. 2019;14(7):e0219355.
Asadi A, Ramirez-Campillo R, Arazi H, Saez de Villarreal E. The effects of maturation on jumping ability and sprint adaptations to plyometric training in youth soccer players. J Sports Sci. 2018;36(21):2405–11.
Davies MJ, Drury B, Ramirez-Campillo R, Chaabane H, Moran J. Effect of plyometric training and biological maturation on jump and change of direction ability in female youth. J Strength Cond Res. 2021;35(10):2690–7.
Heinonen A, Sievänen H, Kannus P, Oja P, Pasanen M, Vuori I. High-impact exercise and bones of growing girls: a 9-month controlled trial. Osteoporos Int J Establ Res Coop Between Eur Found Osteoporos Natl Osteoporos Found USA. 2000;11(12):1010–7.
Lloyd RS, Radnor JM, De Ste Croix MBA, Cronin JB, Oliver JL. Changes in sprint and jump performances after traditional, plyometric, and combined resistance training in male youth pre- and post-peak height velocity. J Strength Cond Res. 2016;30(5):1239–47.
Lloyd RS, Oliver JL, Hughes MG, Williams CA. The effects of 4-weeks of plyometric training on reactive strength index and leg stiffness in male youths. J Strength Cond Res. 2012;26(10):2812–9.
Moran J, Sandercock GRH, Ramírez-Campillo R, Todd O, Collison J, Parry DA. Maturation-related effect of low-dose plyometric training on performance in youth hockey players. Pediatr Exerc Sci. 2017;29(2):194–202.
Ramirez-Campillo R, Alvarez C, Sanchez-Sanchez J, Slimani M, Gentil P, Chelly MS, et al. Effects of plyometric jump training on the physical fitness of young male soccer players: modulation of response by inter-set recovery interval and maturation status. J Sport Sci. 2019;37(23):2645–52.
Romero C, Ramirez-Campillo R, Alvarez C, Moran J, Slimani M, Gonzalez J, et al. Effects of maturation on physical fitness adaptations to plyometric jump training in youth females. J Strength Cond Res. 2021;35(10):2870–7.
Uzelac-Sciran T, Sarabon N, Mikulic P. Effects of 8-week jump training program on sprint and jump performance and leg strength in pre- and post-peak height velocity aged boys. J Sports Sci Med. 2020;19(3):547–55.
Vera-Assaoka T, Ramirez-Campillo R, Alvarez C, Garcia-Pinillos F, Moran J, Gentil P, et al. Effects of maturation on physical fitness adaptations to plyometric drop jump training in male youth soccer players. J Strength Cond Res. 2020;34(10):2760–8.
Vilela G, Caniuqueo-Vargas A, Ramirez-Campillo R, Hernandez-Mosqueira C, da Silva SF. Effects of plyometric training on explosive strength in pubescent girls volleyball players. Retos. 2021;40:41–6.
Behm DG, Young JD, Whitten JHD, Reid JC, Quigley PJ, Low J, et al. Effectiveness of traditional strength versus power training on muscle strength, power and speed with youth: a systematic review and meta-analysis. Front Physiol. 2017. https://doi.org/10.3389/fphys.2017.00423.
Sale DG. Neural adaptation to resistance training. Med Sci Sports Exerc. 1988;20(5 Suppl):S135–45.
Behringer M, Vom Heede A, Yue Z, Mester J. Effects of resistance training in children and adolescents: a meta-analysis. Pediatrics. 2010;126(5):e1199–210.
Arntz F, Mkaouer B, Markov A, Schoenfeld BJ, Moran J, Ramirez-Campillo R, et al. Effect of plyometric jump training on skeletal muscle hypertrophy in healthy individuals: a systematic review with multilevel meta-analysis. Front Physiol. 2022;13: 888464.
Grgic J, Schoenfeld BJ, Mikulic P. Effects of plyometric versus resistance training on skeletal muscle hypertrophy: a review. J Sport Health Sci. 2020.
Rhodri SL, John MR, Sylvia M, Robert WM, Paul JR, Jon LO. Applying strength and conditioning practices to young athletes. Routledge handbook of strength and conditioning: Routledge; 2018
Granacher U, Lesinski M, Büsch D, Muehlbauer T, Prieske O, Puta C, et al. Effects of resistance training in youth athletes on muscular fitness and athletic performance: a conceptual model for long-term athlete development. Frontiers in physiology. 2016;7
Viru A, Loko J, Volver A, Laaneots L, Karelson K, Viru M. Age periods of accelerated improvement of muscle strength, power, speed and endurance in the age interval 6–18 years. Biol Sport. 1998;1998:211–27.
Lloyd RS, Oliver JL, Hughes MG, Williams CA. Age-related differences in the neural regulation of stretch–shortening cycle activities in male youths during maximal and sub-maximal hopping. J Electromyogr Kinesiol. 2012;22(1):37–43.
Loturco I, Pereira LA, Kobal R, Zanetti V, Kitamura K, Abad CCC, et al. Transference effect of vertical and horizontal plyometrics on sprint performance of high-level U-20 soccer players. J Sports Sci. 2015;33(20):2182–91.
Loturco I, Tricoli V, Roschel H, Nakamura FY, Cal Abad CC, Kobal R, et al. Transference of traditional versus complex strength and power training to sprint performance. J Hum Kinet. 2014;28(41):265–73.
Randell AD, Cronin JB, Keogh JW, Gill ND. Transference of strength and power adaptation to sports performance-horizontal and vertical force production. Strength Cond J. 2010;32(4):100–6.
Rutherford OM, Greig CA, Sargeant AJ, Jones DA. Strength training and power output: transference effects in the human quadriceps muscle. J Sports Sci. 1986;4(2):101–7.
Ramirez-Campillo R, Alvarez C, Garcia-Pinillos F, Gentil P, Moran J, Pereira LA, et al. Effects of plyometric training on physical performance of young male soccer players: potential effects of different drop jump heights. Pediatr Exerc Sci. 2019;31(3):306–13.
Ramirez-Campillo R, Burgos CH, Henriquez-Olguin C, Andrade DC, Martinez C, Alvarez C, et al. Effect of unilateral, bilateral, and combined plyometric training on explosive and endurance performance of young soccer players. J Strength Cond Res. 2015;29(5):1317–28.
Ramirez-Campillo R, Alvarez C, Garcia-Pinillos F, Garcia-Ramos A, Loturco I, Chaabene H, et al. Effects of combined surfaces versus single-surface plyometric training on soccer players’ physical fitness. J Strength Cond Res. 2020;34(9):2644–53.
Brumitt J, Heiderscheit BC, Manske RC, Niemuth P, Mattocks A, Rauh MJ. The lower-extremity functional test and lower-quadrant injury in ncaa division iii athletes: a descriptive and epidemiologic report. J Sport Rehabil. 2016;25(3):219–26.
Brumitt J, Mattocks A, Engilis A, Sikkema J, Loew J. Off-season training habits and BMI, not preseason jump measures, are associated with time-loss injury in female collegiate soccer players. Sports (Basel, Switzerland). 2020. https://doi.org/10.3390/sports8030036.
Brumitt J, Wilson V, Ellis N, Petersen J, Zita CJ, Reyes J. Preseason lower extremity functional test scores are not associated with lower quadrant injury—a validation study with normative data on 395 division III athletes. Int J Sports Phys Ther. 2018;13(3):410–21.
Taylor JB, Wright AA, Dischiavi SL, Townsend MA, Marmon AR. Activity demands during multi-directional team sports: a systematic review. Sports Med. 2017;47(12):2533–51.
Mohr M, Krustrup P, Bangsbo J. Match performance of high-standard soccer players with special reference to development of fatigue. J Sports Sci. 2003;21(7):519–28.
Faude O, Koch T, Meyer T. Straight sprinting is the most frequent action in goal situations in professional football. J Sports Sci. 2012;30(7):625–31.
Asadi A. Relationship between jumping ability, agility and sprint performance of elite young basketball players: a field-test approach. Rev Bras Cineantrop Desemp Hum. 2016;18:177–86.
Young WB, Dawson B, Henry GJ. Agility and change-of-direction speed are independent skills: implications for training for agility in invasion sports. Int J Sports Sci Coach. 2015;10(1):159–69.
Young W, Farrow D. A review of agility: practical applications for strength and conditioning. Strength Cond J. 2006;28(5):24–9.
Young WB, James R, Montgomery I. Is muscle power related to running speed with changes of direction? J Sports Med Phys Fitness. 2002;42(3):282–8.
Young WB, McDowell MH, Scarlett BJ. Specificity of sprint and agility training methods. J Strength Cond Res. 2001;15(3):315–9.
Spiteri T, Newton RU, Binetti M, Hart NH, Sheppard JM, Nimphius S. Mechanical determinants of faster change of direction and agility performance in female basketball athletes. J Strength Cond Res. 2015;29(8):2205–14.
Brughelli M, Cronin J, Levin G, Chaouachi A. Understanding change of direction ability in sport: a review of resistance training studies. Sports Med. 2008;38(12):1045–63.
Chaabene H, Prieske O, Negra Y, Granacher U. Change of direction speed: toward a strength training approach with accentuated eccentric muscle actions. Sports Med. 2018;48(8):1773–9.
De Hoyo M, De La Torre A, Pradas F, Sañudo B, Carrasco L, Mateo-Cortes J, et al. Effects of eccentric overload bout on change of direction and performance in soccer players. Int J Sports Med. 2015;36(4):308–14.
Dos’Santos T, Thomas C, Jones PA, Comfort P. Mechanical determinants of faster change of direction speed performance in male athletes. J Strength Cond Res. 2017;31(3):696–705.
Fiorilli G, Iuliano E, Mitrotasios M, Pistone EM, Aquino G, Calcagno G, et al. Are change of direction speed and reactive agility useful for determining the optimal field position for young soccer players? J Sports Sci Med. 2017;16(2):247–53.
Gabbett TJ, Kelly JN, Sheppard JM. Speed, change of direction speed, and reactive agility of rugby league players. J Strength Cond Res. 2008;22(1):174–81.
Maloney SJ, Richards J, Nixon DG, Harvey LJ, Fletcher IM. Do stiffness and asymmetries predict change of direction performance? J Sports Sci. 2017;35(6):547–56.
Marshall BM, Franklyn-Miller AD, King EA, Moran KA, Strike SC, Falvey EC. Biomechanical factors associated with time to complete a change of direction cutting maneuver. J Strength Cond Res. 2014;28(10):2845–51.
Pereira LA, Nimphius S, Kobal R, Kitamura K, Turisco LAL, Orsi RC, et al. Relationship between change of direction, speed, and power in male and female national olympic team handball athletes. J Strength Cond Res. 2018;32(10):2987–94.
Thapa RK, Lum D, Moran J, Ramirez-Campillo R. Effects of complex training on sprint, jump and change of direction ability of soccer players: a systematic review and meta-analysis. Front Psychol. 2021;11:627869.
Pardos-Mainer E, Lozano D, Torrontegui-Duarte M, Carton-Llorente A, Roso-Moliner A. Effects of strength versus plyometric training programs on vertical jumping, linear sprint and change of direction speed performance in female soccer players: a systematic review and meta-analysis. Int J Environ Res Public Health. 2012;18(2):401.
Nygaard Falch H, Guldteig Raedergard H, van den Tillaar R. Effect of different physical training forms on change of direction ability: a systematic review and meta-analysis. Sports Med Open. 2019;5(1):53.
Dos’Santos T, Thomas C, Comfort P, Jones PA. The effect of training interventions on change of direction biomechanics associated with increased anterior cruciate ligament loading: a scoping review. Sports Med. 2019;49(12):1837–59.
Chaabene H, Prieske O, Moran J, Negra Y, Attia A, Granacher U. Effects of resistance training on change-of-direction speed in youth and young physically active and athletic adults: a systematic review with meta-analysis. Sports Med. 2020;50(8):1483–99.
Raya-González J, Castillo D, de Keijzer KL, Beato M. The effect of a weekly flywheel resistance training session on elite U-16 soccer players’ physical performance during the competitive season. A randomized controlled trial. Res Sports Med. 2021;29(6):571–85.
Sáez de Villarreal E, Requena B, Cronin JB. The effects of plyometric training on sprint performance: a meta-analysis. J Strength Cond Res. 2012;26(2):575–84.
Ramirez-Campillo R, Miñano J, Sanchez-Sanchez J. Efecto del entrenamiento pliométrico sobre el rendimiento del futbolista. Rev de Prep Física en el Fútbol. 2019;25(30):1–10.
Ramirez-Campillo R, Gentil P, Negra Y, Grgic J, Girard O. Effects of plyometric jump training on repeated sprint ability in athletes: a systematic review and meta-analysis. Sports Med. 2021;51(10):2165–79.
Mero A, Komi PV, Gregor RJ. Biomechanics of sprint running. A review. Sports Med. 1992;13(6):376–92.
Sáez de Villarreal E, Ramirez-Campillo R. Resistance training for the maximisation of the vertical force production: jumps. In: Muñoz-López A, Taiar R, Sañudo B, editors. Resistance training methods: from theory to practice. Cham: Springer International Publishing; 2022. p. 83–100.
Moran J, Sandercock G, Rumpf MC, Parry DA. Variation in responses to sprint training in male youth athletes: a meta-analysis. Int J Sports Med. 2017;38(1):1–11.
Ramirez-Campillo R, Garcia-Pinillos F, Chaabene H, Moran J, Behm DG, Granacher U. Effects of plyometric jump training on electromyographic activity and its relationship to strength and jump performance in healthy trained and untrained populations: a systematic review of randomized controlled trials. J Strength Cond Res. 2021;35(7):2053–65.
Taube W, Leukel C, Gollhofer A. How neurons make us jump: the neural control of stretch-shortening cycle movements. Exerc Sport Sci Rev. 2012;40(2):106–15.
Ramirez-Campillo R, Gentil P, Moran J, Dalbo VJ, Scanlan AT. Dribble deficit enables measurement of dribbling speed independent of sprinting speed in collegiate, male, basketball players. J Strength Cond Res. 2021;31(7):2040–5.
Ramirez-Campillo R, Perez-Castilla A, Thapa RK, Afonso J, Clemente FM, Colado JC, et al. Effects of plyometric jump training on measures of physical fitness and sport-specific performance of water sports athletes: a systematic review with meta-analysis. Sports Med Open. 2022;8(1):108.
Ramirez-Campillo R, Vergara-Pedreros M, Henriquez-Olguin C, Martinez-Salazar C, Alvarez C, Nakamura FY, et al. Effects of plyometric training on maximal-intensity exercise and endurance in male and female soccer players. J Sports Sci. 2016;34(8):687–93.
García-Pinillos F, Bujalance-Moreno P, Lago-Fuentes C, Ruiz-Alias SA, Domínguez-Azpíroz I, Mecías-Calvo M, et al. Effects of the menstrual cycle on jumping, sprinting and force-velocity profiling in resistance-trained women: a preliminary study. Int J Environ Res Public Health. 2021;18(9):4830.
Sánchez M, Rodríguez-Fernández A, Villa-Del Bosque M, Bermejo-Martín L, Sánchez-Sánchez J, Ramírez-Campillo R, et al. Effects of the menstrual phase on the performance and well-being of female young soccer players. Cult Cienc Deporte. 2022;17(51):113–29.
Rocha-Rodrigues S, Sousa M, Lourenço Reis P, Leão C, Cardoso-Marinho B, Massada M, et al. Bidirectional interactions between the menstrual cycle, exercise training, and macronutrient intake in women: a review. Nutrients. 2021;13(2):438.
Ramirez-Campillo R, Andrade DC, García-Pinillos F, Negra Y, Boullosa D, Moran J. Effects of jump training on physical fitness and athletic performance in endurance runners: a meta-analysis. J Sports Sci. 2021;39(18):2030–50.
Singh U, Ramachandran AK, Ramirez-Campillo R, Perez-Castilla A, Afonso A, Clemente FM, et al. Jump rope training effects on health- and sport-related physical fitness in young participants: A systematic review with meta-analysis. J Sports Sci. 2022. https://doi.org/10.1080/02640414.2022.2099161.
Lloyd RS, Meyers RW, Oliver JL. The natural development and trainability of plyometric ability during childhood. Strength Cond J. 2011;33(2):23–32.
Lloyd RS, Oliver JL. The youth physical development model: a new approach to long-term athletic development. Strength Cond J. 2012;34(3):61–72.
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. No financial support was received for the conduct of this study. The authors acknowledge the support of the Deutsche Forschungsgemeinschaft (DFG) and Open Access Publishing Fund of the University of Freiburg, Germany. This review article is part of the research project “Resistance Training in Youth Athletes” that was funded by the German Federal Institute of Sport Science (ZMVI1-081901 14-18 and ZMVI4-081901/20-23).
Author information
Authors and Affiliations
Contributions
RRC, AS, JM, and UG conceived the idea and design for the article. RRC, AS, JA, FMC, and UG performed the literature search, data acquisition, analysis, and/or interpretation. RRC, AS, JM, JA, FMC, RSL, JLO, JP, and UG drafted and/or critically revised the work. All authors have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing interests
Rodrigo Ramirez-Campillo, Andrew Sortwell, Jason Moran, José Afonso, Filipe Manuel Clemente, Rhodri S. Lloyd, Jon L. Oliver, Jason Pedley, and Urs Granacher declare that they have no conflicts of interest relevant to the content of this review.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Figures S1 to S24, with meta-analyses for participants pre-PHV (PJT vs controls), post-PHV (PJT vs controls), and PJT (pre-PHV vs post-PHV).
Additional file 2
. Characterization of activities performed by the control groups during the intervention period.
Additional file 3
. Meta-analyses according to moderators: participants’ sex, PJT programme duration (number of weeks and total number of training sessions), total number of jumps, and studies methodological quality.
Additional file 4. Table S1
. Search strategies (code line) for each database and background of search history.
Additional file 5. Table S2
. Exclusion reasons for studies included in the preliminary qualitative synthesis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ramirez-Campillo, R., Sortwell, A., Moran, J. et al. Plyometric-Jump Training Effects on Physical Fitness and Sport-Specific Performance According to Maturity: A Systematic Review with Meta-analysis. Sports Med - Open 9, 23 (2023). https://doi.org/10.1186/s40798-023-00568-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-023-00568-6