
Abstract
Background
Maximal strength may contribute to soccer players’ performance. Several resistance training modalities offer the potential to improve maximal strength. During recent years, a large number of plyometric jump training (PJT) studies showed evidence for maximal strength improvements in soccer players. However, a comprehensive summary of the available data is lacking.
Objective
To examine the effects of PJT compared with active, passive or intervention controls on the maximal strength of soccer players, irrespective of age, sex or competitive level.
Methods
To perform a systematic review with meta-analysis following PRISMA 2020. Three electronic databases (PubMed, Web of Science, and SCOPUS) were systematically searched. Studies published from inception until March 2023 were included. A PICOS approach was used to rate studies for eligibility. The PEDro scale was used to assess risk of bias. Meta-analyses were performed using the DerSimonian and Laird random-effects model if ≥ 3 studies were available. Moderator and sensitivity analyses were performed, and meta-regression was conducted when ≥ 10 studies were available for a given comparison. We rated the certainty of evidence using GRADE.
Results
The search identified 13,029 documents, and from these 30 studies were eligible for the systematic review, and 27 for the meta-analyses. Overall, 1,274 soccer players aged 10.7–25.0 years participated in the included studies. Only one study recruited females. The PJT interventions lasted between 5 and 40 weeks (median = 8 weeks), with 1–3 weekly sessions. Compared to controls, PJT improved maximal dynamic strength (18 studies, 632 participants [7 females], aged 12.7–24.5 y; effect size [ES] = 0.43, 95% confidence interval [CI] = 0.08–0.78, p = 0.017, impact of statistical heterogeneity [I2] = 77.9%), isometric strength (7 studies; 245 participants, males, aged 11.1–22.5 y; ES = 0.58, 95% CI = 0.28–0.87, p < 0.001, I2 = 17.7%), and isokinetic peak torque (5 studies; 183 participants, males, aged 12.6–25.0 y; ES = 0.51, 95% CI = 0.22–0.80, p = 0.001, I2 = 0.0%). The PJT-induced maximal dynamic strength changes were independent of participants’ age (median = 18.0 y), weeks of intervention (median = 8 weeks), and total number of training sessions (median = 16 sessions). The certainty of evidence was considered low to very low for the main analyses.
Conclusions
Interventions involving PJT are more effective to improve maximal strength in soccer players compared to control conditions involving traditional sport-specific training.
Trial Registration The trial registration protocol was published on the Open Science Framework (OSF) platform in December 2022, with the following links to the project (https://osf.io/rpxjk) and to the registration (https://osf.io/3ruyj).
Key Points
-
Plyometric jump training is an easy-to-administer training regime that can be performed on the soccer pitch and may have the potential to improve maximal strength in soccer players.
-
Findings from this meta-analysis including 1274 soccer players indicate maximal strength improvements after plyometric jump training, with similar effects for youth and adult players, and with < 8 vs. ≥ 8 weeks or < 16 vs. ≥ 16 sessions
Similar content being viewed by others
Background
Measures of muscular fitness (i.e., muscle strength, power, local muscular endurance) have been shown to be positively related to markers of health [1,2,3,4], and athletic performance [5, 6]. For the context of this systematic review with meta-analysis, maximal strength has been defined as the ability to exert maximal force against an external resistance during a maximal voluntary contraction [7]. Maximal strength is considered a reliable measure of muscular fitness [8] and is commonly assessed through the one-repetition maximum (1-RM) method during a dynamic strength test [6], although alternative assessment techniques (e.g., isometric; isokinetic) are applied as well [9]. Maximal strength depends on factors such as intra- (motor unit recruitment and firing rate) and inter- (agonist-antagonist coordination) muscular coordination as well as muscle cross-sectional area [10]. The improvement in neural and morphological factors related to maximal strength allows athletes to have greater potential for power development [11] and sports-related skills [12]. For example, the development of maximal muscle strength is considered crucial for soccer players to respond to the multiple short-duration and maximal or near-maximal-intensity demands of a match (e.g., sprinting, acceleration, deceleration, jumping, and changes-of-direction) [13,14,15]. Further, there is evidence showing that maximal strength tests (e.g., load lifted in half squat) are related with linear sprint speed, the main action that precedes a goal in elite [16], semi-professional [14], and youth [17] soccer players. Furthermore, maximal strength (i.e., isokinetic peak torque) can be used to differentiate between soccer players of different practice levels [18].
Although the methods and loads to achieve the best results in maximal strength development have not yet been clarified [19], free weight exercises have been commonly used [7] and a meta-analysis has reported that competitive athletes experience maximal gains when training at an intensity of ~ 85% of the 1-RM [20]. However, factors such as logistical constraints (e.g., reduced access to free weight facilities), the congested schedule of professional soccer players, among others (e.g., injury or reduced performance in young soccer players), may discourage the use of high loads during training for maximal strength development [21]. In this context, plyometric jump training (PJT) presents promising advantages [12, 22] because it can be easily administered on the soccer pitch, is widely applied [23] and does not need much exercise equipment. PJT is characterized through a wide variety of different jump types (e.g., vertical, horizontal, unilateral, bilateral), leveraging body mass as resistance, and necessitating no external load [24]. Additionally, PJT involves rapid muscle eccentric actions during the braking phase immediately followed by rapid concentric actions, mimicking the specific neuromuscular needs commonly encountered in a soccer match, allowing greater transmutation [25,26,27]. Indeed, previous studies have demonstrated that integrating PJT alongside regular soccer sessions holds promise for enhancing various facets of physical fitness in players of different age, sex and competitive level [28,29,30,31,32]. There is even evidence that PJT can mitigate injury rates [33, 34].
PJT involves repeated jump actions (i.e., multi-jumps) and ground contact times during jumping are either short (i.e., < 250 ms) or long (i.e., > 250 ms), influencing the speed of the muscle–tendon stretch–shortening cycle (SSC) [35]. Muscle actions during the SSC allow an accumulation of elastic energy that facilitates greater muscle power production [36]. Therefore, the SSC stimulates the ability of the neuromuscular system to produce maximal strength and power in the shortest amount of time (i.e., increased rate of force development), with a high transfer to athletic performance [25,26,27], possibly due to improved neural activation and enhanced motor coordination [23, 37]. PJT may also increase skeletal muscle fibre contraction force and cross-sectional area [38, 39], pennation angle [40], among other neuromuscular adaptations [23], all linked to training-induced maximal strength improvements [41]. Indeed, PJT has the potential to improve maximal strength. For example, a meta-analysis [12] including 15 PJT studies showed improved maximal strength with an effect size (ES) = 0.97 vs 0.11 in trained compared to controls, respectively. The results of these analyses indicate that the PJT effects on maximal strength do not depend on the sport discipline (ES = 0.87, volleyball; ES = 0.41, basketball; ES = 0.80, body building; ES = 0.80, rowing; ES = 0.50, swimming; ES = 0.80, American football). However, no soccer-related studies were included.
Moreover, most studies investigating PJT effects in soccer involved only small sample sizes (i.e., mode n = 10) [24, 35, 42] which is a common problem in the sport science literature using highly trained athletes [43]. In an attempt to address the challenge of small sample sizes in elite sports, systematic reviews with and without meta-analyses have been conducted in adult male [44] and female players [32], as well as in young players [38, 39]. However, not all studies [28, 44] agree with the beneficial effects of PJT on measures of maximal strength in soccer. A previous systematic review showed no PJT effects on maximal strength in adult male soccer players [44], while another systematic review showed a significant effect in youth soccer players [28]. Of note, the transfer of findings from adult male to youth players (including females) appears inappropriate due to maturational processes taking place in youth such as rapid increases in stature, potential temporary disruption in motor co-ordination also known as adolescent awkwardness, large increases in fat-free mass due to hormonal changes, and changes in muscle–tendon architecture [45,46,47]. These factors may influence the muscle strength responsiveness to PJT [45, 48,49,50,51,52,53,54,55,56]. Currently, there is no study available that has contrasted youth vs. adult soccer players’ responsiveness to PJT.
To account for the previous limitations (e.g., low sample size), a meta-analysis may help practitioners to extract evidence-based information from the available literature for PJT implementation in soccer [57]. Additionally, a systematic review with meta-analysis may detect gaps and limitations in the PJT literature (e.g., lack of studies addressing the chronobiological response of maximal strength to PJT), providing valuable information for scientists and practitioners about future research avenues. Such an approach seems timely, considering that the yearly rate of PJT-related publications has increased 25-fold between 2000 and 2017 [24], with soccer-related studies at a rate of around 100 per year [58]. Therefore, the primary aim of this systematic review with meta-analysis was to examine the effects of PJT compared with active, passive or intervention controls on the maximal strength in soccer players of any age, sex or competitive level.
Methods
Procedures
A systematic review with meta-analysis was conducted following the guidelines of the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 [59]. The protocol for this systematic review with meta-analysis was published on the Open Science Framework (OSF) platform in December 2022, with the following links to the project (https://osf.io/rpxjk) and to the registration (https://osf.io/3ruyj).
Literature Search: Administration and Update
We considered recommendations from the two most comprehensive scoping reviews that previously examined the PJT literature [24, 31]. Briefly, a systematic literature search of three electronic databases (PubMed, Web of Science, and SCOPUS) was conducted. Studies published from inception and until March 2023 were included. The search strategy (code line) for each database is described in the Additional file 1: Table S1. In selecting studies for inclusion, a review of all relevant titles was conducted before the examination of the abstracts and full-texts. Two authors (RRC and JSS) independently screened the titles, abstracts, and/or full-texts of the retrieved studies. During the search and review process, potential discrepancies between the two authors regarding inclusion and exclusion criteria (e.g., intervention adequacy) were resolved through discussion with a third author (ARF)
Inclusion and Exclusion Criteria
A PICOS (participants, intervention, comparators, outcomes, and study design) approach was used to rate studies for eligibility [60]. Table 1 indicates the inclusion/exclusion criteria. Of note, the decision to determine the minimal effective PJT duration (weeks) for the improvement of maximal strength (i.e., ≥ 3 weeks) was based on the results of previous systematic reviews [12, 24, 35]. Additionally, only original studies in peer-reviewed and full-text format were eligible to be included in this meta-analysis.
We excluded books, book chapters, and congress abstracts, as well as cross-sectional studies and review papers. The following studies were excluded: retrospective studies, prospective studies (e.g., relation between bone density at the end of PJT, and at several years of follow-up), studies reported in proceedings (only abstract available), special communications, letters to the editor, invited commentaries, errata, and studies of doubtful quality or unclear peer-review process [61]. In the case of detraining studies, these were considered for inclusion if they involved a training period prior to a detraining period. When a comparator group was included in the studies, we did not consider a minimum number of participants per group as an inclusion/exclusion criterion, although case reports were excluded.
Data Item Extraction and Management
The effects of PJT compared to active (e.g., young soccer players, female soccer players), passive (e.g., soccer players non-participating in any regular training during intervention) and/or intervention (e.g., soccer players involving alternative training methods such as high-load resistance training) controls on maximal strength were assessed. Measures of maximal strength included (but were not limited to) different specific tests (e.g., squat; leg press). The 1-RM has previously shown moderate to strong levels of reliability (intra-class correlation coefficient = 0.64–0.99; coefficient of variation = 0.5–12.1%) across a range of populations [8], which is essential to ensure strong consistency between the analysed studies within a meta-analysis [60].
Pre- and post-intervention, means and standard deviations of the dependent variables were extracted from the included studies using Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA). For studies reporting values other than means and standard deviation (e.g., median, range, interquartile range, standard error values), conversion was applied as previously recommended [62,63,64]. Appropriate statistical software was used for different data formats (Comprehensive Meta-Analysis Software, Version 2, Biostat, Englewood, NJ, USA). When the required data were not clearly or completely reported, the authors of the respective studies were contacted for clarification purposes. If no response was obtained from the authors (after two attempts, with a between-attempts waiting time of 72 h) or the authors did not provide the requested data, the study outcome was excluded from further analysis. According to our registered protocol, four studies were excluded because they did not respond to our author queries and data were not sufficiently reported for the purpose of a meta-analysis, three full texts were excluded from the meta-analysis because maximal strength data were reported in combined form for both control and experimental groups (as the authors noted no difference between experimental and control groups) [65, 66] or 1-RM was measured only in the experimental group [67]. When data were displayed in a figure and no numerical data were provided by the authors, validated (r = 0.99, p < 0.001) [60] software (WebPlotDigitizer, version 4.5; https://apps.automeris.io/wpd/) was used to derive numerical data from the respective figures. One author (JSS) performed data extraction and a second author (ARF) provided confirmation, and any discrepancies between them (e.g., mean value for a given outcome) were resolved through discussion with a third author (RRC).
Risk of Bias of the Included Studies
The Physiotherapy Evidence Database (PEDro) scale was used to assess the risk of bias and methodological quality of the included studies. The validity and reliability of the PEDro scale have been established previously [68,69,70]. Moreover, the PEDro scale is the most frequently used metric in the PJT literature [35, 71, 72]. Despite being termed a “methodological quality” scale, its items mostly assess factors related to the risk of bias of studies. Accordingly, it helps to make comparisons between meta-analyses. Considering that it is not possible to satisfy all scale items in PJT interventions [73] and as outlined in previous systematic reviews in the sub-field of PJT, the overall risk of bias of PJT studies was interpreted using the following convention [31, 32, 72, 73]: ≤ 3 points was considered as “poor” quality (i.e., high risk of bias), 4–5 points was considered as “moderate” quality, while 6–7 points and 8–10 points was considered as “good” and “excellent” quality, respectively. For practical purposes and given the nature of the research field, we considered studies with ≥ 6 points to have low risk of bias. Two reviewers (JSS and ARF) independently rated/confirmed each study. Any ratings that yielded different results between two reviewers were further adjudicated by a third reviewer (RRC).
Summary Measures, Synthesis of Results, and Risk of Publication Bias
Meta-analyses can be computed with as little as two studies [74]. However, we performed our analyses if ≥ 3 studies were available considering the reduced number of participants in PJT interventions [1, 75, 76]. Means and standard deviations from pre- and post-values were taken to compute ES (i.e., Hedges' g) for maximal strength in the PJT and active, passive or intervention control groups. Data were standardised using post-intervention standard deviation values. The DerSimonian and Laird random-effects model was used to account for differences between studies that might affect the PJT effects [77, 78]. The ES values are presented with 95% confidence intervals (95% CIs). Calculated ES were interpreted using the following scale: < 0.2 trivial, 0.2–0.6 small, > 0.6–1.2 moderate, > 1.2–2.0 large, > 2.0 very large [79]. However, in strength and conditioning research studies with ES values ≥ 3.0 (improvement of ≥ 3.0 standard deviations from the mean) are unlikely after most interventions, and were considered outliers [80]. In studies including more than one intervention group, the sample size in the control group was proportionately divided to facilitate comparisons across multiple groups [81]. The impact of study heterogeneity was assessed using the I2 statistics, with values of < 25%, 25–75%, and > 75% representing low, moderate, and high levels of heterogeneity, respectively [82]. The risk of publication bias was explored for continuous variables (≥ 10 studies per outcome) [83,84,85] using the extended Egger’s test [84]. All analyses were carried out using the Comprehensive Meta-Analysis Software (Version 2, Biostat, Englewood, NJ, USA). Statistical significance was set at p ≤ 0.05.
Additional Analyses
Subgroup Analyses
As adaptive responses to PJT programs may be affected by the individual’s age and sex [56, 86, 87], these potential sources of heterogeneity are likely to influence the effects of training and were therefore selected a priori.
Single Training Factor Analyses
Single training factor analyses were computed for the programming parameters duration (intervention duration and total number of training sessions) [88] and training frequency (number of weekly exercise sessions) [12], based on the reported impact of these variables on adaptations following PJT.
When appropriate, subgroup analyses and single training factor analyses were analysed using the median split technique [87, 89, 90]. The median was calculated if at least three studies provided data for a potential moderator. Of note, when two experimental groups (with the same information for a given moderator) were included in a study, only one of the groups was considered to avoid an augmented influence of the study on the median calculation. In addition, instead of using a global median value for a given moderator (e.g., median age, derived from all included studies), median values were calculated considering only those studies that provided data for the analysed outcome. When the median split technique was found not to be appropriate, a logically defensible rationale was used for subgroup analysis.
Sensitivity Analyses
We performed sensitivity analyses to assess the robustness of the summary estimates (e.g., p-value, ES, I2). To examine the effects of each result from each study on the overall findings, results were analysed with each study deleted from the model (automated leave-one-out analysis).
Meta-regression
A multivariate DerSimonian and Laird random-effects model meta-regression was conducted to verify if any of the training variables (frequency, duration, and total number of sessions) explained the effects of PJT on the maximal strength. The computation of meta-regression was performed with at least 10 studies per covariate [91].
Certainty of Evidence
Two authors (JA and RRC) rated the certainty of evidence (i.e., high; moderate; low; very low) using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) [92,93,94]. The evidence started at a high level of certainty (per outcome), but was downgraded based on the following criteria: (i) Risk of bias in studies: judgments were downgraded by one level if the median PEDro scores were moderate (< 6) or by two levels if they were poor (< 4); (ii) Indirectness: low risk of indirectness was attributed by default due to the specificity of populations, interventions, comparators and outcomes being guaranteed by the eligibility criteria; (iii) Risk of publication bias: downgraded by one level if there was suspected publication bias; (iv) Inconsistency: judgments were downgraded by one level when I2 was high (> 75%); (v) Imprecision: one level of downgrading occurred whenever < 800 participants were available for a comparison [95] and/or if there was no clear direction of the effects. When both were observed, certainty was downgraded by two levels.
Adverse Effects
Considering the potential adverse health effects derived from the inadequate implementation of PJT interventions, a qualitative analysis of such potential effects was included.
Results
Study Selection
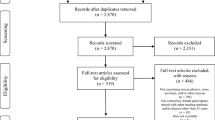
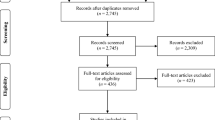
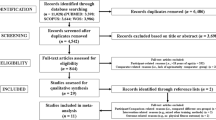
The search process in the databases identified 13,029 studies. Figure 1 provides a flow chart illustrating the study selection process. Duplicate studies were removed (n = 7644). After study titles and abstracts were screened, 4226 studies were removed and 1159 full texts were screened. Finally, 30 studies (all written in English) were considered eligible to be included in this systematic review [65,66,67, 96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122]. Three full texts were excluded from the meta-analysis because maximal strength data were reported in combined form for both control and experimental groups (as the authors noted no difference between experimental and control groups) [65, 66] or 1-RM was measured only in the experimental group [67].

Study inclusion and exclusion selection process
Risk of Bias of the Included Studies
According to the PEDro checklist results (Table 2), the median (i.e., non-parametric) score was 5 (some risk of bias-moderate quality), with 17 studies attaining 4–5 points (some risk of bias-moderate quality) and 13 studies attaining 6–7 points (low risk of bias-high quality). For studies that analyzed the effects of PJT on dynamic maximal strength, the median score was 6 (low risk of bias-high quality), with six studies attaining 4–5 points (some risk of bias-moderate quality) and seven studies attaining 6–7 points (low risk of bias-high quality). For the studies that analyzed the effect of PJT on maximal voluntary isometric strength, the median score was 5 (some risk of bias-moderate quality), with four studies attaining 4–5 points (some risk of bias-moderate quality) and three studies attaining 6–7 points (low risk of bias-high quality). The studies that analyzed the effects of PJT on peak isokinetic torque obtained a median score of 5 (some risk of bias-moderate quality), with three studies attaining 5 points (some risk of bias-moderate quality) and two studies attaining 6–7 points (low risk of bias-high quality).
Study Characteristics
The participant characteristics and the PJT programs of the included studies are detailed in Table 3. In the 30 studies included in the systematic review 1,274 soccer players were included (624 in the intervention groups; 650 in control groups), with an age range of 10.7–25.0 years (14 studies recruited participants < 18 years). Intervention control groups (e.g., involving alternative training methods such as high-load resistance training) were considered a priori for moderator analyses [97, 102, 103, 109,110,111,112, 114, 118, 123]. However, study heterogeneity (e.g., moderate-load RT; high-load RT; weightlifting; resisted sprinting; free sprinting; functional training) precluded such analyses.
The testing procedures for maximal strength among studies are described in Table 4. Broadly, testing procedures were categorized as maximal dynamic, maximal isometric, and peak isokinetic torque tests. Briefly, most (n = 20) studies included dynamic 1-RM to 5-RM squat tests, isometric tests (n = 7), isokinetic tests (n = 6), or included a combination of ≥ 2 types of the mentioned maximal strength test categories.
Results from the Meta-analysis
Maximal Dynamic Strength
Eighteen studies were used to meta-analyze the PJT effects on dynamic maximal strength, examining a total of 632 participants, 342 included in the intervention groups (22 groups) and 290 in the control groups (18 groups). Regarding the 18 control groups, 13 groups were involved in regular soccer training (active control group), five groups were involved in strength training (intervention control group) and one group was classified as passive control since the study was carried out during the off-season [98]. Seventeen studies involved male soccer players and one study used male and female soccer players [118], aged < 18 years in 9 studies (9 studies recruited participants 18–25 years). Training duration in the intervention and control groups ranged from 6 to 40 weeks, with a median value of 8 weeks. The frequency of weekly training sessions ranged from 1 to 3, although most studies (15 studies) applied 2 training sessions per week. Results (Fig. 2) showed a significant effect for the PJT groups compared to the control groups: ES = 0.61, 95% CI = 0.22 to 1.00, p = 0.002. However, after two outlier study-groups were removed [101, 109], the results changed to ES = 0.43, 95% CI = 0.08 to 0.78, p = 0.017, I2 = 77.9%, Egger test two-tailed = 0.457. In both cases, despite an effect favouring the PJT groups, the large 95% CIs suggested heterogeneous results. After the sensitivity analyses (automated leave-one-out analysis), the robustness of the summary estimates (e.g., p-value, ES) was confirmed.

Forest plot illustrating plyometric jump training (PJT)-related improvements of maximal dynamic strength (e.g., 1-RM) in comparison to active and passive controls groups. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. White rhomboid: summary value. a and b denote different experimental groups used in the same study
Maximal Voluntary Isometric Strength
Seven studies were considered to analyze the effect of PJT on isometric maximal strength, including a total of 245 participants, with 142 included in the intervention groups (9 groups) and 103 in the control groups (7 groups). Six control groups performed regular soccer training (active control group) and one passive group performed no training (unclear if this was done during the off-season) [118]. All participants were male soccer players aged 11.1–22.5 years (3 studies recruited participants < 18 years). Training duration in the intervention and control groups ranged from 6 to 8 weeks, with a frequency of weekly training sessions ranging from 1 to 3. Results (Fig. 3) showed a significant effect for the PJT groups compared to the control groups: ES = 0.58, 95% CI = 0.28–0.87, p < 0.001, I2 = 17.7%. After the sensitivity analyses (automated leave-one-out analysis), the robustness of the summary estimates (e.g., p-value, ES) was confirmed.

Forest plot illustrating plyometric jump training (PJT)-related improvements of maximal voluntary isometric strength (e.g., N) in comparison to active and passive controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. White rhomboid: summary value. a and b denote different experimental groups used in the same study
Peak Isokinetic Torque
The effects of PJT on peak isokinetic torque were analyzed in 5 studies, involving 183 participants, with 102 participants from the intervention groups (7 groups) and 81 from the control groups (5 groups). Of the control groups, 3 groups performed regular soccer training (active control group), one group did not perform any training because the study was conducted during the off-season period (passive control group) [92], and one group performed high-resistance training (intervention control group) [119]. All studies involved male soccer players, aged 12.6–25.0 years (2 studies recruited participants < 18 years). Training duration in the intervention and control groups ranged from 5 to 9 weeks, with a median value of 8 weeks. The frequency of weekly training sessions ranged from 1 to 3. Results (Fig. 4) showed a significant effect for the PJT groups compared to the control groups: ES = 0.51, 95% CI = 0.22 to 0.80, p = 0.001, I2 = 0.0%. After the sensitivity analyses (automated leave-one-out analysis), the robustness of the summary estimates (e.g., p-value, ES) was confirmed.

Forest plot illustrating plyometric jump training (PJT)-related improvements of peak isokinetic torque (e.g., N.m-1) in comparison to active, passive and intervention controls. Forest plot values are shown as effect sizes (Hedges’ g) with 95% confidence intervals (CI). Black squares: individual studies. The size represents the relative weight. White rhomboid: summary value. a and b denote different experimental groups used in the same study
Moderator Analyses
Regarding participants’ age (median age = 18.0 y), PJT-induced maximal dynamic strength changes were similar for adults (8 groups; ES = 0.49, 95% CI = 0.07–0.91; p = 0.021; I2 = 46.0%) compared to younger participants (9 groups; ES = 0.37, 95% CI = 0.04–0.69; p = 0.026; I2 = 46.1%), with a between-moderator category p = 0.650.
Regarding PJT weeks of intervention (median duration = 8 weeks), PJT-induced maximal dynamic strength changes were similar for longer (5 groups ≥ 8 weeks; ES = 0.57, 95% CI = −0.01 to 1.14; p = 0.053; I2 = 63.4%) compared to shorter interventions (12 groups < 8 weeks; ES = 0.35, 95% CI = 0.08–0.62; p = 0.011; I2 = 30.0%), with a between-moderator category p = 0.503.
Regarding total number of PJT sessions (median = 16 sessions), PJT-induced maximal dynamic strength changes were similar after interventions involving higher (6 groups ≥ 16 sessions; ES = 0.43, 95% CI = −0.12 to 0.98; p = 0.125; I2 = 65.9%) compared to lower number of sessions (11 groups < 16 sessions; ES = 0.40, 95% CI = 0.13–0.67; p = 0.003; I2 = 24.7%), with a between-moderator category p = 0.932.
Other moderator analyses were precluded due to a reduced number of studies (n < 3) available for each of the moderator categories.
Meta-regression
The meta-regression analysis (17 groups) was computed for maximal dynamic strength (e.g., 1-RM) including as potential effect modifiers the i) participants' chronological age (years), ii) PJT total duration (weeks), and iii) PJT total sessions (n). None of the variables in the model explained the effects of PJT on maximal dynamic strength (p = 0.299–0.744).
Certainty of Evidence
According to the GRADE assessment (Table 5), the certainty of evidence was considered low to very low for the main analyses.
Adverse Effects
Six studies indicated that 36 players (2.8% of total participants) did not complete the intervention studies due to adverse health events (e.g., injury; illness) [65, 66, 99, 100, 111, 115] without better clarification if events occurred during interventions. The remaining studies did not report soreness, pain, fatigue, injury, damage, or related adverse health events.
Discussion
The primary aim of this systematic review with meta-analysis was to examine the effects of PJT compared with active, passive or intervention controls on the maximal strength (i.e., dynamic, isometric, and isokinetic) in soccer players, irrespective of age, sex or competitive level. A discussion of the main results follows.
Compared to controls, PJT interventions improved maximal strength, including dynamic (ES = 0.43, Fig. 1), isometric (ES = 0.58, Fig. 2), and isokinetic (ES = 0.51, Fig. 3) maximal strength/torque measures. These results confirm the positive effects of PJT on maximal strength that were reported in previous studies [12, 124]. PJT-related maximal strength improvement was accompanied by (but not limited to) increased electromyographic activity (e.g., increased recruitment of motor units) [37], muscle activation strategies (e.g., improved intermuscular coordination) [23], single-fiber functioning (e.g., increased force) [39], muscle–tendon architecture (e.g., increased muscle pennation angle) [40], and increased muscle mass [125]. Maximal strength is related to sprint and jump performance [16, 126], common actions before scoring a goal in soccer [127] and associated with team positioning in the league [128]. Further, more competitive players exhibit greater maximal strength levels compared to less competitive players [129]. Therefore, improved maximal strength after PJT might contribute to soccer players' on-field performance. Performance enhancement through PJT interventions has proven effective and safe (with few reported injuries in the scientific PJT literature). In addition, PJT is an easy-to-administer training modality that can be conducted on the pitch and needs little equipment [24]. However, according to the GRADE assessment (Table 5), the certainty of evidence was considered low to very low for the main analyses. Moreover, the observed results were mainly assessed in male soccer players, as females represent a minor portion of the total soccer population. Therefore, a robust recommendation regarding the use of PJT to improve maximal strength in female soccer players is currently precluded. Although some limitations are difficult to address, future studies should provide stronger evidence by including larger samples in randomized-controlled trials.
The moderator analyses and the meta-regression analysis were available for maximal dynamic strength only. No moderator or meta-regression effect was noted for participants’ age (i.e., adults vs. youth). Participants were aged up to 25.0 years. Of note, a relatively greater number of studies reported the assessment of maximal strength indices for adult compared to youth players. For example, dynamic, isometric, and isokinetic maximal strength/torque was assessed in 9:9, 3:7, and 2:5 studies in youth:adult players, respectively. This contrasts with the considerably greater number of studies that reported athletic indices such as jumping and sprinting in youth compared to adult soccer players [29]. The reason why maximal strength was relatively unexplored in studies conducted in youth is unclear, but may include logistical reasons. For example, it may be difficult and time-consuming to perform safe and reliable maximal strength tests in youth players without experience in such procedures [130]. Indeed, when describing the training practices of academy soccer players, it has been noted that only 7–14% of their weekly training load is attributed to work in a gym [131]. Another reason might include fear of injury, or difficulty accessing sophisticated measurement equipment (e.g., isokinetic device) [132]. Irrespective of the potential reasons, future studies should include maximal strength assessment, given the potential of PJT to improve this outcome, and its relevance for soccer performance [14, 16]. Indeed, strength and PJT have been suggested to be important in youth soccer, due to associations with both physical performance [133,134,135,136] and injury prevention [33, 34, 137].
The moderator analyses and the meta-regression analyses for maximal dynamic strength also showed no moderator effect for total PJT programming duration (i.e., < 8 vs. ≥ 8 weeks) or total number of PJT sessions (i.e., < 16 vs. ≥ 16 sessions). The lack of differences in the PJT effects on maximal dynamic strength after longer compared to shorter interventions (e.g., < 8 vs. ≥ 8 weeks; < 16 vs. ≥ 16 sessions) are somewhat unexpected. As our moderator analysis involved cut-off values (categorical analysis), this may have affected the results. In a secondary analysis, we performed comparisons between study duration and total sessions using a continuous analysis approach. However, again, no significant differences were found. Considering the high heterogeneity for the maximal dynamic strength results noted after PJT (i.e., I2 = 77.9%), this may mean that interventions between studies varied not only in duration and total sessions, but in other potentially relevant PJT prescription variables, including exercise intensity (poorly reported among the included studies). However, currently there is no robust evidence to suggest a minimal effective duration or total number of sessions of PJT for the improvement of maximal dynamic strength in soccer players [29]. Alternatively, maximal strength response adaptation to PJT may be different from that of other physical fitness outcomes such as jump height and linear sprint speed [12, 88, 138]. Indeed, a correlation between PJT duration, sprint and jump performance improvement has been reported, although not for maximal strength [12, 88, 138].
Recently, there has been a proliferation of published studies on the effects of PJT in male soccer players [29]. However, there have been relatively few studies conducted with female soccer players [67, 121] and, according to the authors’ knowledge, none in master athletes. Indeed, of the included studies in the meta-analyses, only one study reported maximal strength data for females, in a mixed sample of male and female soccer players [121]. Furthermore, among the included studies in our meta-analyses, no youth female player data were available. This contrasts with the relatively greater number of studies conducted in youth males (i.e., 13 of a total of 27 meta-analysed studies). Therefore, the typical (not justified) sex imbalance in sport science publications [35, 139,140,141,142,143,144,145,146] is also noted in the context of this systematic review. The reason why females are less involved in PJT research and maximal strength measurements is probably multifactorial. A discussion of the (societal) biases that may underlie this phenomenon is beyond the scope of our review, and has been previously addressed [140]. Briefly, likely reasons could be (i) the lower incorporation of females in professional sports (e.g., soccer), (ii) cultural and/or religious reasons, and (iii) reduced research in females, retarding the transference to practice, as the potential PJT benefits could be less recognised by coaches (i.e., it might take up to 17 years until research findings are translated into practice) [147]. Soccer is a very popular sport around the world, with nearly 270 million people actively playing and a 50% increase in the number of female players observed between 2000 and 2006, with a stated aim for the sport to reach 60 million female players by 2026 [148]. With the increased participation of females in sports, research is required to enhance knowledge with regards to PJT programming for maximal strength optimization for female athletes.
Although six studies reported adverse health events (e.g., injury, illness) [65, 66, 99, 100, 111, 115] these were not directly linked to the PJT interventions. Thus, PJT seems a safe training method for soccer players aiming to improve maximal strength performance. Strength adaptations related to reduced injury risk were noted in some studies. In youth males (age, ~ 17 years) [122], the ratio of dominant leg/non-dominant leg peak torque for the knee extensors and flexors improved (~ 10%) after five weeks of training. Among adult males (age, ~ 21 years), eight weeks of training improved the hamstring eccentric:quadriceps concentric ratio, although only after unloaded jump training (7%) compared to loaded jumps (1%) [98]. Another study with adult males (age, ~ 23 years) [115], after seven weeks of training, noted significant improvements (5–10%) in hamstring/quadriceps peak concentric torque ratio in the dominant and non-dominant leg, and in the hamstring eccentric:quadriceps concentric peak torque ratio in the dominant and non-dominant leg. Reduced injuries are related to team success (e.g., position of the team in the league) [128]. However, among the studies (n = 24) that did not report soreness, pain, fatigue, injury, damage, or related adverse health effects, it is unclear if the lack of reporting was due to a true absence of adverse effects or merely due to the omission (i.e., non-deliberate) of such information in the reporting of the study methods. Moreover, some studies did not include in the methods section a description of instruments and protocols aimed to measure health effects (e.g., visual analogue pain scales; rating of perceived effort). Finally, these are surrogate outcomes and not direct measures of injury risk, and so they require careful interpretation. Future studies should elucidate the safety of PJT in soccer players by including robust measurement protocols and reporting methods.
Limitations
A study limitation is the reduced number of studies available to perform moderator analyses regarding PJT programming variables, players’ sex, and players’ competitive level.
Conclusions
Interventions involving PJT are more effective to improve maximal strength in soccer players compared to active, passive or intervention controls conditions involving traditional sport-specific training. This conclusion is derived from 27 studies with low-to-some risk of bias, low-to-high study heterogeneity, and low-to-very low certainty of evidence (GRADE rating), comprising 1,274 participants. The observed PJT-related maximal dynamic strength changes were similar for youth and adult players, and after shorter compared to longer interventions (i.e., < 8 vs. ≥ 8 weeks or < 16 vs. ≥ 16 sessions). Of the included studies, it seems that a minimal initial effective PJT dosage may involve one weekly training session for at least 5 weeks, involving ~ 70 jumps per session (usually at maximal intensity). However, the low-to-very low confidence in the available body of evidence precludes a robust recommendation for the implementation of PJT to improve maximal strength in soccer players.
Availability of Data and Materials
All data generated or analysed during this study are included in the article as Table(s), Figure(s), and/or Electronic Supplementary Material(s). Any other data requirement can be directed to the corresponding author upon reasonable request.
Abbreviations
- CI:
-
Confidence interval
- ES:
-
Effect size
- GRADE:
-
Grading of Recommendations, Assessment, Development and Evaluation
- I2 :
-
Impact of statistical heterogeneity
- 1-RM:
-
One-repetition maximum
- OSF:
-
Open Science Framework
- PICOS:
-
Participants, intervention, comparators, outcomes, and study design
- PEDro:
-
Physiotherapy Evidence Database
- PJT:
-
Plyometric jump training
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- SCC:
-
Stretch–shortening cycle
References
García-Hermoso A, Ramírez-Campillo R, Izquierdo M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019;49:1079–94. https://doi.org/10.1007/s40279-019-01098-6.
Metter EJ, Talbot LA, Schrager M, Conwit RA. Arm-cranking muscle power and arm isometric muscle strength are independent predictors of all-cause mortality in men. J Appl Physiol. 2004;96:814–21. https://doi.org/10.1152/japplphysiol.00370.2003.
McGrath R, Tomkinson GR, LaRoche DP, Vincent BM, Bond CW, Hackney KJ. Handgrip strength asymmetry and weakness may accelerate time to mortality in aging Americans. J Am Med Dir Assoc. 2020;21:2003–7. https://doi.org/10.1016/j.jamda.2020.04.030.
López-Bueno R, Andersen LL, Koyanagi A, Núñez-Cortés R, Calatayud J, Casaña J, et al. Thresholds of handgrip strength for all-cause, cancer, and cardiovascular mortality: a systematic review with dose-response meta-analysis. Ageing Res Rev. 2022;82:101778. https://doi.org/10.1016/j.arr.2022.101778.
Suchomel TJ, Nimphius S, Stone MH. The importance of muscular strength in athletic performance. Sports Med. 2016;46:1419–49. https://doi.org/10.1007/s40279-016-0486-0.
Williams TD, Tolusso DV, Fedewa MV, Esco MR. Comparison of periodized and non-periodized resistance training on maximal strength: a meta-analysis. Sports Med. 2017;47:2083–100. https://doi.org/10.1007/s40279-017-0734-y.
Thompson SW, Rogerson D, Ruddock A, Barnes A. The effectiveness of two methods of prescribing load on maximal strength development: a systematic review. Sports Med. 2020;50:919–38. https://doi.org/10.1007/s40279-019-01241-3.
Grgic J, Lazinica B, Schoenfeld BJ, Pedisic Z. Test-retest reliability of the one-repetition maximum (1RM) strength assessment: a systematic review. Sports Med Open. 2020;6:1–16. https://doi.org/10.1186/s40798-020-00260-z.
McMaster DT, Gill N, Cronin J, McGuigan M. A brief review of strength and ballistic assessment methodologies in sport. Sports Med. 2014;44:603–23. https://doi.org/10.1007/s40279-014-0145-2.
Rhea MR, Alvar BA, Burkett LN, Ball SD. A meta-analysis to determine the dose response for strength development. Med Sci Sports Exerc. 2003;35:456–64. https://doi.org/10.1249/01.MSS.0000053727.63505.D4.
Cormie P, McGuigan MR, Newton RU. Influence of strength on magnitude and mechanisms of adaptation to power training. Med Sci Sports Exerc. 2010;42:1566–81. https://doi.org/10.1249/MSS.0b013e3181cf818d.
Saéz-Sáez de Villarreal E, Requena B, Newton RU. Does plyometric training improve strength performance? A meta-analysis. J Sci Med Sport. 2010;13:513–22. https://doi.org/10.1016/j.jsams.2009.08.005.
Taber C, Bellon C, Abbott H, Bingham GE. Roles of maximal strength and rate of force development in maximizing muscular power. Strength Cond J. 2016;38:71–8. https://doi.org/10.1519/SSC.0000000000000193.
Requena B, González-Badillo JJ, Saez E, Ereline J, García I, Gapeyeva H, et al. Functional performance, maximal strength, and power characteristics in isometric and dynamic actions of lower extremities in soccer players. J Strength Cond Res. 2009;25:1391–401. https://doi.org/10.1519/JSC.0b013e3181a4e88e.
Heggelund J, Fimland MS, Helgerud J, Hoff J. Maximal strength training improves work economy, rate of force development and maximal strength more than conventional strength training. Eur J Appl Physiol. 2013;113:1565–73. https://doi.org/10.1007/s00421-013-2586-y.
Wisloff U, Castagna C, Helgerud J, Jones R, Hoff J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br J Sports Med. 2004;38:285–8. https://doi.org/10.1136/bjsm.2002.002071.
Keiner M, Sander German Bobsled A, Association L, Hartmann H, Sander A, Wirth K, et al. Correlations between maximal strength tests at different squat depths and sprint performance in adolescent soccer players. Am J Sports Med. 2014;2:1–7.
Kalapotharakos VI, Strimpakos N, Vithoulka I, Karvounidis C, Diamantopoulos K, Kapreli E. Physiological characteristics of elite professional soccer teams of different ranking. J Sports Med Phys Fitness. 2006;46:515–9.
Barjaste A, Mirzaei B. The periodization of resistance training in soccer players: Changes in maximal strength, lower extremity power, body composition and muscle volume. J Sports Med Phys Fitness. 2018;58:1218–25. https://doi.org/10.23736/S0022-4707.17.07129-8.
Peterson MD, Rhea MR, Alvar BA. Maximizing strength development in athletes: a meta-analysis to determine the dose-response relationship. J Strength Cond Res. 2004;18:377–82.
Weldon A, Duncan MJ, Turner A, Laplaca D, Sampaio J, Christie CJ. Practices of strength and conditioning coaches: a snapshot from different sports, countries, and expertise levels. J Strength Cond Res. 2022;36:1335–44. https://doi.org/10.1519/JSC.0000000000003773.
Sáez de Villarreal E, Requena B, Izquierdo M, Gonzalez-Badillo JJ. Enhancing sprint and strength performance: Combined versus maximal power, traditional heavy-resistance and plyometric training. J Sci Med Sport. 2013;16:146–50. https://doi.org/10.1016/j.jsams.2012.05.007
Markovic G, Mikulic P. Neuro-musculoskeletal and performance adaptations to lower-extremity plyometric training. Sports Med. 2010;40:859–95. https://doi.org/10.2165/11318370-000000000-00000.
Ramirez-Campillo R, Álvarez C, García-Hermoso A, Ramírez-Vélez R, Gentil P, Asid A, et al. Methodological characteristics and future directions for plyometric jump training research: a scoping review. Sports Med. 2018;48:1059–81. https://doi.org/10.1007/s40279-018-0870-z.
Loturco I, Pereira LA, Kobal R, Zanetti V, Kitamura K, Abad CCC, et al. Transference effect of vertical and horizontal plyometrics on sprint performance of high-level U-20 soccer players. J Sports Sci. 2015;33:2182–91. https://doi.org/10.1080/02640414.2015.1081394.
Loturco I, Tricoli V, Roschel H, Nakamura FY, Abad CCC, Kobal R, et al. Transference of traditional versus complex strength and power training to sprint performance. J Hum Kinet. 2014;41:265–73. https://doi.org/10.2478/hukin-2014-0054.
Seitz LB, Reyes A, Tran TT, de Villarreal ES, Haff GG. Increases in lower-body strength transfer positively to sprint performance: a systematic review with meta-analysis. Sports Med. 2014;44:1693–702. https://doi.org/10.1007/s40279-014-0227-1.
Oliver JL, Ramachandran AK, Singh U, Ramirez-Campillo R, Lloyd RS. The effects of strength, plyometric and combined training on strength, power and speed characteristics in high-level, highly trained male youth soccer players: a systematic review and meta-analysis. Sports Med. 2024;54:623–43. https://doi.org/10.1007/s40279-023-01944-8.
Ramirez-Campillo R, Moran J, Oliver JL, Pedley JS, Lloyd RS, Granacher U. Programming plyometric-jump training in soccer: a review. Sports. 2022;10:94. https://doi.org/10.3390/sports10060094.
Sánchez M, Sanchez-Sanchez J, Nakamura FY, Clemente FM, Romero-Moraleda B, Ramirez-Campillo R. Effects of plyometric jump training in female soccer player’s physical fitness: a systematic review with meta-analysis. Int J Environ Res Public Health. 2020;17:8911. https://doi.org/10.3390/ijerph17238911.
Ramirez-Campillo R, Castillo D, Raya-González J, Moran J, de Villarreal ES, Lloyd RS. Effects of plyometric jump training on jump and sprint performance in young male soccer players: a systematic review and meta-analysis. Sports Med. 2020;50:2125–43. https://doi.org/10.1007/s40279-020-01337-1.
Ramirez-Campillo R, Sanchez-Sanchez J, Romero-Moraleda B, Yanci J, García-Hermoso A, Clemente FM. Effects of plyometric jump training in female soccer player’s vertical jump height: a systematic review with meta-analysis. J Sports Sci. 2020;38:1475–87. https://doi.org/10.1080/02640414.2020.1745503.
Zouita S, Zouita ABM, Kebsi W, Dupont G, Ben Abderrahman A, Ben Salah FZ, et al. Strength training reduces injury rate in elite young soccer players during one season. J Strength Cond Res. 2016;30:1295–307. https://doi.org/10.1519/JSC.0000000000000920.
Owoeye OBA, VanderWey MJ, Pike I. Reducing injuries in soccer (football): an umbrella review of best evidence across the epidemiological framework for prevention. Sports Med Open. 2020. https://doi.org/10.1186/s40798-020-00274-7.
Ramirez-Campillo R, Moran J, Chaabene H, Granacher U, Behm DG, García-Hermoso A, et al. Methodological characteristics and future directions for plyometric jump training research: a scoping review update. Scand J Med Sci Sports. 2020;30:983–97. https://doi.org/10.1111/sms.13633.
Sole S, Ramírez-Campillo R, Andrade DC, Sanchez-Sanchez J. Plyometric jump training effects on the physical fitness of individual-sport athletes: A systematic review with meta-analysis. PeerJ. 2021;9:1–25. https://doi.org/10.7717/peerj.11004.
Ramirez-Campillo R, Garcia-Pinillos F, Chaabene H, Moran J, Behm DG, Granacher U. Effects of plyometric jump training on electromyographic activity and its relationship to strength and jump performance in healthy trained and untrained populations: a systematic review of randomized controlled trials. J Strength Cond Res. 2021;35:2053–65. https://doi.org/10.1519/JSC.0000000000004056.
Malisoux L, Francaux M, Theisen D. What do single-fiber studies tell us about exercise training? Med Sci Sports Exerc. 2007;39:1051–60.
Malisoux L, Francaux M, Nielens H, Renard P, Lebacq J, Theisen D. Calcium sensitivity of human single muscle fibers following plyometric training. Med Sci Sports Exerc. 2006;38:1901–8.
Ramirez-Campillo R, García-Pinillos F, Nikolaidis PT, Clemente F, Gentil P, García-Hermoso A. Body composition adaptations to lower-body plyometric training: a systematic review and meta-analysis. Biol Sport. 2022;39(2):273–87. https://doi.org/10.5114/biolsport.2022.104916.
Komi PV. Physiological and biomechanical correlates of muscle function: effects of muscle structure and stretch-shortening cycle on force and speed. Exerc Sport Sci Rev. 1984;12:81–121.
Ramirez-Campillo R, Miñano J, Sanchez-Sanchez J. Efecto del entrenamiento pliométrico sobre el rendimiento del futbolista. Revista de Preparacion Fisica en el Futbol. 2019;25:1–10.
Abt G, Boreham C, Davison G, Jackson R, Nevill A, Wallace E, et al. Power, precision, and sample size estimation in sport and exercise science research. J Sports Sci. 2020;38:1933–5. https://doi.org/10.1080/02640414.2020.1776002.
van de Hoef PA, Brauers JJ, van Smeden M, Backx FJ, Brink MS. The effectos of lower extremity plyometric training on soccer-specific outcomes in adult male soccer players: a systematic review and meta-analysis. Int J Sports Physiol Perform. 2020;15:3–17. https://doi.org/10.1123/ijspp.2019-0565.
Hirtz P, Starosta W. Co-ordination development and its. Education. 2002;7:19–28.
Radnor JM, Oliver JL, Waugh CM, Myer GD, Moore IS, Lloyd RS. The influence of growth and maturation on stretch-shortening cycle function in youth. Sports Med. 2018;48:57–71. https://doi.org/10.1007/s40279-017-0785-0.
Malina RM, Bouchard C, Bar-Or O. Growth, maturation, and physical activity: Human kinetics; 2004.
Ratel S, Duche P, Williams CA. Muscle fatigue during high-intensity exercise in children. Sports med. 2006;36:1031–65. https://doi.org/10.2165/00007256-200636120-00004.
Sacks D. Age limits and adolescents. Paediatr Child Health. 2003;8:577–677. https://doi.org/10.1093/pch/8.9.577.
Marginson V, Eston R. The relationship between torque and joint angle during knee extension in boys and men. J Sports Sci. 2001;19:875–80. https://doi.org/10.1080/026404101753113822.
Marginson V, Rowlands AV, Gleeson N, Eston RG. Comparison of the symptoms of exercise-induced muscle damage after an initial and repeated bout of plyometric exercise in men and boys. J Appl Physiol. 2005;99:1174–81. https://doi.org/10.1152/japplphysiol.01193.20042004.
Mersmann F, Bohm S, Arampatzis A. Imbalances in the development of muscle and tendon as risk factor for tendinopathies in youth athletes: a review of current evidence and concepts of prevention. Front Physiol. 2017;8:987. https://doi.org/10.3389/fphys.2017.00987.
Mersmann F, Bohm S, Schroll A, Boeth H, Duda G, Arampatzis A. Evidence of imbalanced adaptation between muscle and tendon in adolescent athletes. Scand J Med Sci Sports. 2014;24:e283–9. https://doi.org/10.1111/sms.12166.
Mersmann F, Bohm S, Schroll A, Boeth H, Duda GN, Arampatzis A. Muscle and tendon adaptation in adolescent athletes: a longitudinal study. Scand J Med Sci Sports. 2017;27:75–82. https://doi.org/10.1111/sms.12631.
Moran J, Liew B, Ramirez-Campillo R, Granacher U, Negra Y, Chaabene H. The effects of plyometric jump training on lower-limb stiffness in healthy individuals: a meta-analytical comparison. J Sport Health Sci. 2021;12:236–45. https://doi.org/10.1016/j.jshs.2021.05.005.
Moran J, Sandercock GRH, Ramírez-Campillo R, Meylan CMP, Collison JA, Parry DA. Age-related variation in male youth athletes’ countermovement jump after plyometric training: a meta-analysis of controlled trials. J Strength Cond Res. 2017;31:552–65. https://doi.org/10.1519/JSC.0000000000001444.
Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid. Evid Based Med. 2016;21:125–7. https://doi.org/10.1136/ebmed-2016-110401.
PubMed-NTNCfB. Jump training. https://www.ncbi.nlm.nih.gov/pubmed. 2020.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. https://doi.org/10.1136/bmj.n71.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151:w65. https://doi.org/10.1136/bmj.b2700.
Grudniewicz A, Moher D, Cobey KD, Bryson GL, Cukier S, Allen K, et al. Predatory journals:no definition, no defence. Nature. 2019;576:210–2.
Higgins JP, Deeks JJ. Selecting studies and collecting data. In: Higgins JPT GS, edis. Cochrane Handbook for Systematic Reviews of Interventions Version 510. 2008:168–82.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:13. https://doi.org/10.1186/1471-2288-14-135.
Lee DK, In J, Lee S. Standard deviation and standard error of the mean. Korean J Anesthesiol. 2015;68:220. https://doi.org/10.4097/kjae.2015.68.3.220.
Gauffin H, Ekstrand J, Arnesson L, Tropp H. Vertical jump performance in soccer players. A comparative study of two training programmes. J Hum Mov Stud. 1989;16:215–24.
Gauffin H, Ekstrand J, Tropp H. Improvement of vertical jump performance in soccer players after specific training. J Hum Mov Stud. 1988;15:185–90.
Siegler J, Gaskill S, Ruby B. Changes evaluated in soccer-specific power endurance either with or without a 10-week, in-season, intermittent, high-intensity training protocol. J Strength Cond Res. 2003;17:379–87.
de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55:129–33. https://doi.org/10.1016/S0004-9514(09)70043-1.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–21. https://doi.org/10.1093/ptj/83.8.713.
Yamato TP, Maher C, Koes B, Moseley A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J Clin Epidemiol. 2017;86:176–81. https://doi.org/10.1016/j.jclinepi.2017.03.002.
Asadi A, Arazi H, Young WB, de Villarreal ES. The effects of plyometric training on change-of-direction ability: a meta-analysis. Int J Sports Physiol Perform. 2016;11:563–73. https://doi.org/10.1123/ijspp.2015-0694.
Stojanović E, Ristić V, McMaster DT, Milanović Z. Effect of plyometric training on vertical jump performance in female athletes: a systematic review and meta-analysis. Sports Med. 2017;47:975–86. https://doi.org/10.1007/s40279-016-0634-6.
Cashin AG, McAuley JH. Clinimetrics: physiotherapy evidence database (PEDro) scale. J Physiother. 2020;66:59. https://doi.org/10.1016/j.jphys.2019.08.005.
Valentine JC, Pigott TD, Rothstein HR. How many studies do you need? J Educ Behav Stat. 2010;35:215–47. https://doi.org/10.3102/1076998609346961.
Moran J, Ramirez-Campillo R, Granacher U. Effects of jumping exercise on muscular power in older adults: a meta-analysis. Sports Med. 2018;48:2843–57. https://doi.org/10.1007/s40279-018-1002-5.
Jackson D, Turner R. Power analysis for random-effects meta-analysis. Res Synth Methods. 2017;8:290–302. https://doi.org/10.1002/jrsm.1240.
Deeks JJ, Higgins JP, Altman DG. Analysing data and undertaking meta-analyses. In: Deeks JJ, Higgins JP, edis. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration. 2008:243–96.
Kontopantelis E, Springate DA, Reeves D. A re-analysis of the cochrane library data: the dangers of unobserved heterogeneity in meta-analyses. PLoS ONE. 2013;8:e69930. https://doi.org/10.1371/journal.pone.0069930.
Hopkins WG, Marshall SW, Batterham AM, Hanin J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. 2009;41:3–13. https://doi.org/10.1249/MSS.0b013e31818cb278.
Kadlec D, Sainani KL, Nimphius S. With great power comes great responsibility: common errors in meta-analyses and meta-regressions in strength & conditioning research. Sport med. 2023;53:313–25. https://doi.org/10.1007/s40279-022-01766-0.
Higgins JP, Deeks JJ, Altman DG. Special topics in statistics. In: Higgins JP, Deeks JJ, edis. Cochrane handbook for systematic reviews of interventions. The Cochrane Collaboration, 2008:481–529.
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58. https://doi.org/10.1002/sim.1186.
Page MJ, Higgins JPT, Sterne JAC. Assessing risk of bias due to missing results in a synthesis. In: Cochrane handbook for systematic reviews of interventions. New York: Wiley; 2019. p. 349–74.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. https://doi.org/10.1136/bmj.315.7109.629.
Sterne JAC, Sutton AJ, Ioannidis JPA, Terrin N, Jones DR, Lau J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:4002–12. https://doi.org/10.1136/bmj.d4002.
Asadi A, Arazi H, Ramirez-Campillo R, Moran J, Izquierdo M. Influence of maturation stage on agility performance gains after plyometric training: a systematic review and meta-analysis. J Strength Cond Res. 2017;31:2609–17. https://doi.org/10.1519/JSC.0000000000001994.
Moran J, Clark CCT, Ramirez-Campillo R, Davies MJ, Drury B. A meta-analysis of plyometric training in female youth: its efficacy and shortcomings in the literature. J Strength Cond Res. 2019;33:1996–2008. https://doi.org/10.1519/JSC.0000000000002768.
Sáez-Sáez de Villarreal E, Kellis E, Kraemer WJ, Izquierdo M. Determining variables of plyometric training for improving vertical jump height performance: a meta-analysis. J Strength Cond Res. 2009;23:495–506. https://doi.org/10.1519/JSC.0b013e318196b7c6.
Moran J, Sandercock G, Ramirez-Campillo R, Clark CCT, Fernandes JFT, Drury B. A meta-analysis of resistance training in female youth: its effects on muscular strength, and shortcomings in the literature. Sports Med. 2018;48:1661–71. https://doi.org/10.1519/JSC.0000000000002768.
Moran J, Sandercock GRH, Ramírez-Campillo R, Meylan C, Collison J, Parry DA. A meta-analysis of maturation-related variation in adolescent boy athletes’ adaptations to short-term resistance training. J Sports Sci. 2017;35:1041–51. https://doi.org/10.1080/02640414.2016.1209306.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T. Cochrane handbook for systematic reviews of interventions. 2019.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–94. https://doi.org/10.1016/j.jclinepi.2010.04.026.
Zhang Y, Alonso-Coello P, Guyatt GH, Yepes-Nuñez JJ, Akl EA, Hazlewood G, et al. GRADE Guidelines: 19. Assessing the certainty of evidence in the importance of outcomes or values and preferences—Risk of bias and indirectness. J Clin Epidemiol. 2019;111:94–104. https://doi.org/10.1016/j.jclinepi.2018.01.013.
Zhang Y, Coello PA, Guyatt GH, Yepes-Nuñez JJ, Akl EA, Hazlewood G, et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences—inconsistency, imprecision, and other domains. J Clin Epidemiol. 2019;111:83–93. https://doi.org/10.1016/j.jclinepi.2018.05.011.
Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. Corrigendum to GRADE guidelines 6. Rating the quality of evidence-imprecision. J Clin Epidemiol. 2011;64:1283–93. https://doi.org/10.1016/j.jclinepi.2021.04.014.
Al Ameer A. The effects of plyometric and resistance training on selected fitness variables among university soccer-playing adults. Ann Appl Sport Sci. 2020. https://doi.org/10.29252/AASSJOURNAL.817.
Brito J, Vasconcellos F, Oliveira J, Krustrup P, Rebelo A. Short-term performance effects of three different low-volume strength-training Programmes in college male soccer players. J Hum Kinet. 2014;40:121–8. https://doi.org/10.2478/hukin-2014-0014.
Coratella G, Beato M, Milanese C, Longo S, Limonta E, Rampichini S, et al. Specific adaptations in performance and muscle architecture after weighted jumpsquat vs. body mass squat jump training in recreational soccer players. J Strength Cond Res. 2018;32:921–9. https://doi.org/10.1519/JSC.0000000000002463.
Faude O, Roth R, Di Giovine D, Zahner L, Donath L. Combined strength and power training in high-level amateur football during the competitive season: a randomised-controlled trial. J Sports Sci. 2013;31:1460–7. https://doi.org/10.1080/02640414.2013.796065.
Franco-Márquez F, Rodríguez-Rosell D, González-Suárez JM, Pareja-Blanco F, Mora-Custodio R, Yañez-García JM, et al. Effects of combined resistance training and plyometrics on physical performance in young soccer players. Int J Sports Med. 2015;36:906–14. https://doi.org/10.1055/s-0035-1548890.
Hammami M, Gaamouri N, Shephard RJ, Chelly MS. Effects of contrast strength vs. plyometric training on lower limb explosive performance, ability to change direction and neuromuscular adaptation in soccer players. J Strength Cond Res. 2019;33:2094–103. https://doi.org/10.1519/JSC.0000000000002425.
Hammami M, Negra Y, Shephard RJ, Chelly MS. The effect of standard strength vs. contrast strength training on the development of sprint, agility, repeated change of direction, and jump in junior male soccer players. J Strength Cond Res. 2017;31:901–12. https://doi.org/10.1519/JSC.0000000000001815.
Keiner M, Kadlubowski B, Sander A, Hartmann H, Wirth K. Effects of 10 months of speed, functional, and traditional strength training on strength, linear sprint, change of direction, and jump performance in trained adolescent soccer players. J Strength Condition Res. 2022;36(8):2236–46. https://doi.org/10.1519/JSC.0000000000003807.
Makhlouf I, Chaouachi A, Chaouachi M, Ben OA, Granacher U, Behm DG. Combination of agility and plyometric training provides similar training benefits as combined balance and plyometric training in young soccer players. Front Physiol. 2018;9:1611. https://doi.org/10.3389/fphys.2018.01611.
Zghal F, Colson SS, Blain G, Behm DG, Granacher U, Chaouachi A. Combined resistance and plyometric training is more effective than plyometric training alone for improving physical fitness of pubertal soccer players. Front Physiol. 2019;10:1611. https://doi.org/10.3389/fphys.2019.01026.
Rædergård HG, Falch HN, Van Den TR. Effects of strength vs. plyometric training on change of direction performance in experienced soccer players. Sports. 2020;8:144. https://doi.org/10.3390/sports8110144.
Vera-Assaoka T, Ramirez-Campillo R, Alvarez C, Garcia-Pinillos F, Moran J, Gentil P, et al. Effects of maturation on physical fitness adaptations to plyometric drop jump training in male youth soccer players. J Strength Cond Res. 2019;34:2760–8. https://doi.org/10.1519/JSC.0000000000003151.
Váczi M, Tollár J, Meszler B, Juhász I, Karsai I. Short-term high intensity plyometric training program improves strength, power and agility in male soccer players. J Hum Kinet. 2013;36:17–26. https://doi.org/10.2478/hukin-2013-0002.
Ronnestad BR, Kvamme NH, Sunde A, Raastad T. Short-term effects of strength and plyometric training on sprint and jump performance in professional soccer players. J Strength Cond Res. 2008;22:773–80.
Rodríguez-Rosell D, Torres-Torrelo J, Franco-Márquez F, González-Suárez JM, González-Badillo JJ. Effects of light-load maximal lifting velocity weight training vs. combined weight training and plyometrics on sprint, vertical jump and strength performance in adult soccer players. J Sci Med Sport. 2017;20:695–9. https://doi.org/10.1016/j.jsams.2016.11.010.
Rodríguez-Rosell D, Franco-Márquez F, Pareja-Blanco F, Mora-Custodio R, Yáñez-García JM, González-Suárez JM, et al. Effects of 6 weeks resistance training combined with plyometric and speed exercises on physical performance of pre-peak-height-velocity soccer players. Int J Sports Physiol Perform. 2016;11:240–6. https://doi.org/10.1123/ijspp.2015-0176.
Negra Y, Chaabene H, Stöggl T, Hammami M, Chelly MS, Hachana Y. Effectiveness and time-course adaptation of resistance training vs. plyometric training in prepubertal soccer players. J Sport Health Sci. 2020;9:620–7. https://doi.org/10.1016/j.jshs.2016.07.008.
Michailidis Y, Fatouros IG, Primpa E, Michailidis C, Avloniti A, Chatzinikolaou A, et al. Plyometrics’ trainability in preadolescent soccer athletes. J Strength Cond Res. 2013;27:38–49.
Mckinlay BJ, Wallace P, Dotan R, Long D, Tokuno C, Gabriel DA, et al. Effects of plyometric and resistance training on muscle strength, explosiveness, and neuromuscular function in young adolescent soccer players. J Strength Cond Res. 2018;32:3039–50. https://doi.org/10.1519/JSC.0b013e3182541ec6.
Mendiguchia J, Martinez-Ruiz E, Morin JB, Samozino P, Edouard P, Alcaraz PE, et al. Effects of hamstring-emphasized neuromuscular training on strength and sprinting mechanics in football players. Scand J Med Sci Sports. 2015;25:e621–9. https://doi.org/10.1111/sms.12388.
Lockie RG, Murphy AJ, Schultz AB, Knight TJ, De Jonge XAKJ. The effects of different speed training protocols on sprint acceleration kinematics and muscle strength and power in field sport athletes. J Strength Cond Res. 2012;26:1539–50. https://doi.org/10.1519/JSC.0b013e318234e8a0.
Ita S, Guntoro TS. The effect of plyometric and resistance training on muscle power, strength, and speed in young adolescent soccer players. Indian J Public Health Res Dev. 2018;9:1450–5. https://doi.org/10.5958/0976-5506.2018.00936.1.
Hasan S, Kandasamy G, Alyahya D, Alonazi A, Jamal A, Unnikrishnan R, et al. Effect of resisted sprint and plyometric training on lower limb functional performance in collegiate male football players: a randomised control trial. Int J Environ Res Public Health. 2021;18:6702. https://doi.org/10.3390/ijerph18136702.
Ramirez-Campillo R, Alvarez C, García-Pinillos F, Sanchez-Sanchez J, Yanci J, Castillo D, et al. Optimal reactive strength index. J Strength Cond Res. 2018;32:885–93. https://doi.org/10.1519/JSC.0000000000002467.
Spineti J, Figueiredo T, Bastos de Oliveira V, Assis M, Fernandes de Oliveira L, Miranda H, et al. Comparison between traditional strength training and complex contrast training on repeated sprint ability and muscle architecture in elite soccer players. J Sports Med Phys Fitness. 2016;56:1269–78.
Moore EW, Hickey MS, Reiser RF. Comparison of two twelve week off-season combined training programs on entry level collegiate soccer players’ performance. J Strength Cond Res. 2005;19:791–8.
Lehnert M, Psotta R, Botek Z. The effects of high-resistance and plyometric training on adolescent soccer players: a comparative study. Gazz Med Ital. 2012;171:1–10.
Lockie RG, Murphy AJ, Schultz AB, Knight TJ, de Jonge XAJ. The effects of different speed training protocols on sprint acceleration kinematics and muscle strength and power in field sport athletes. J Strength Condition Res. 2012;26(6):1539–50. https://doi.org/10.1519/JSC.0b013e318234e8a0.
Ramirez-Campillo R, Andrade DC, Izquierdo M. Effects of plyometric training volume and training surface on explosive strength. J Strength Cond Res. 2013;27:2714–22. https://doi.org/10.1519/JSC.0b013e318280c9e9.
Arntz F, Mkaouer B, Markov A, Schoenfeld BJ, Moran J, Ramirez-Campillo R, et al. Effect of plyometric jump training on skeletal muscle hypertrophy in healthy individuals: a systematic review with multilevel meta-analysis. Front Physiol. 2022;13:1–17. https://doi.org/10.3389/fphys.2022.888464.
Comfort P, Stewart A, Bloom L, Clarkson B. Relationships between strength, sprint, and jump performance in well-trained youth soccer players. J Strength Cond Res. 2014;28:173–7. https://doi.org/10.1519/JSC.0b013e318291b8c7.
Faude O, Koch T, Meyer T. Straight sprinting is the most frequent action in goal situations in professional football. J Sports Sci. 2012;30:625–31. https://doi.org/10.1080/02640414.2012.665940.
Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Physical fitness, injuries, and team performance in soccer. Med Sci Sports Exerc. 2004;36:278–85. https://doi.org/10.1249/01.MSS.0000113478.92945.CA.
Slimani M, Nikolaidis PT. Anthropometric and physiological characteristics of male soccer players according to their competitive level, playing position and age group: a systematic review. J Sports Med Phys Fitness. 2017;59:141–63. https://doi.org/10.23736/S0022-4707.17.07950-6.
Bompa T, Buzzichelli C. Periodization: theory and methodology of training. In Champaign: Human Kinetics, 2019.
Wrigley R, Drust B, Stratton G, Atkinson G, Gregson W. Long-term soccer-specific training enhances the rate of physical development of academy soccer players independent of maturation status. Int J Sports Med. 2014;35:1090–4. https://doi.org/10.1055/s-0034-1375616.
González-Badillo JJ, Sánchez-Medina L, Ribas-Serna J, Rodríguez-Rosell D. Toward a new paradigm in resistance training by means of velocity monitoring: a critical and challenging narrative. Sports Med Open. 2022;8:118. https://doi.org/10.1186/s40798-022-00513-z.
Ramirez-Campillo R, Andrade DC, Álvarez C, Henríquez-Olguín C, Martínez C, Báez-SanMartín E, et al. The effects of interday rest on adaptation to 7 weeks of explosive training in young soccer players. J Sports Sci Med. 2014;13:287–96. https://doi.org/10.1519/JSC.0000000000000283.
Matavulj D, Kukolj M, Ugarkovic D, Tihanyi J, Jaric S. Effects of plyometric training on jumping performance in junior basketball players. J Sports Med Phys Fitness. 2001;41:159–64.
Ramirez-Campillo R, Álvarez C, García-Pinillos F, García-Ramos A, Loturco I, Chaabene H, et al. Effects of combined surfaces vs. single-surface plyometric training on soccer players’ physical fitness. J Strength Cond Res. 2020;34:2644–53. https://doi.org/10.1519/JSC.0000000000002929.
Asadi A, Ramirez-Campillo R, Meylan C, Nakamura FY, Cañas-Jamett R, Izquierdo M. Effects of volume-based overload plyometric training on maximal-intensity exercise adaptations in young basketball players. J Sports Med Phys Fitness. 2017. https://doi.org/10.23736/S0022-4707.16.06640-8.
Lloyd RS, Meyers RW, Oliver JL. The natural development and trainability of plyometric ability during childhood. Strength Cond J. 2011;33:23–32. https://doi.org/10.1519/SSC.0b013e3182093a27.
Saéz-Sáez de Villarreal E, Requena B, Cronin JB. The effects of plyometric training on sprint performance: a meta-analysis. J Strength Cond Res. 2012;26:575–84. https://doi.org/10.1519/JSC.0b013e318220fd03.
Afonso J, Olivares-Jabalera J, Fernandes RJ, Clemente FM, Rocha-Rodrigues S, Claudino JG, et al. Effectiveness of conservative interventions after acute hamstrings injuries in athletes: a living systematic review. Sports Med. 2023;53:615–35. https://doi.org/10.1007/s40279-022-01783-z.
Ramirez-Campillo R, Thapa RK, Afonso J, Perez-Castilla A, Bishop C, Byrne PJ, et al. Effects of plyometric jump training on the reactive strength index in healthy individuals across the lifespan: a systematic review with meta-analysis. Sports Med. 2023;53:1029–53. https://doi.org/10.1007/s40279-023-01825-0.
Patel R, Kemp CL, Hafejee M, Peckham N, Jain V, McCann GP, et al. The underrepresentation of females in studies assessing the impact of high-dose exercise on cardiovascular outcomes: a scoping review. Sports Med Open. 2021. https://doi.org/10.1186/s40798-021-00320-y.
Cowley ES, Olenick AA, McNulty KL, Ross EZ. “Invisible Sportswomen”: the sex data gap in sport and exercise science research. Women Sport Phys Act J. 2021;29:146–51. https://doi.org/10.1123/wspaj.2021-0028.
Thorborg K, Krohn L, Bandholm T, Jacobsen JS, Rathleff MS, Klakk H, et al. ‘More Walk and Less Talk’: changing gender bias in sports medicine. Br J Sports Med. 2020;54:1380–1. https://doi.org/10.1136/bjsports-2020-102966.
Walton CC, Gwyther K, Gao CX, Purcell R, Rice SM. Evidence of gender imbalance across samples in sport and exercise psychology. Int Rev Sport Exerc Psychol. 2022;2022:1–19. https://doi.org/10.1080/1750984X.2022.2150981.
Cowan SM, Kemp JL, Ardern CL, Thornton JS, Rio EK, Bruder AM, et al. Sport and exercise medicine/physiotherapy publishing has a gender/sex equity problem: we need action now! Br J Sports Med. 2023;57:401–7. https://doi.org/10.1136/bjsports-2022-106055.
Granacher U, Lesinski M, Büsch D, Muehlbauer T, Prieske O, Puta C, et al. Effects of resistance training in youth athletes on muscular fitness and athletic performance: a conceptual model for long-term athlete development. Front Physiol. 2016;7:164. https://doi.org/10.3389/fphys.2016.00164.
Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med. 2011;104:510–20. https://doi.org/10.1258/jrsm.2011.110180.
FIFA. The FIFA big count 2006: 230 million active in football. 2007.
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
JSS and RRC conceived the idea and design for the article. JSS, ARF, JA and RRC performed the literature search, data acquisition, analysis, and/or interpretation. JSS, ARF, UG, JA and RRC drafted and/or critically revised the work. All authors have read, and approved the manuscript, and have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature. All authors read and approved the final version.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Search strategy code line for each database.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sanchez-Sanchez, J., Rodriguez-Fernandez, A., Granacher, U. et al. Plyometric Jump Training Effects on Maximal Strength in Soccer Players: A Systematic Review with Meta-analysis of Randomized-Controlled Studies. Sports Med - Open 10, 52 (2024). https://doi.org/10.1186/s40798-024-00720-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-024-00720-w