
Abstract
Background
Malnutrition is the main cause of illness and death in children under the age of five. It affects millions of children worldwide, putting their health and future in jeopardy. Therefore, this study aimed to identify and estimate the effects of important determinants of anthropometric indicators by taking into account their association and cluster effects.
Method
The study was carried out in 10 countries in East Africa: Burundi, Ethiopia, Comoros, Uganda, Rwanda, Tanzania, Zimbabwe, Kenya, Zambia, and Malawi. A weighted total sample of 53,322 children under the age of five was included. Given the impact of other predictors such as maternal, child, and socioeconomic variables, a multilevel multivariate binary logistic regression model was employed to analyze the relationship between stunting, wasting, and underweight.
Result
The study included 53,322 children, and 34.7%, 14.8%, and 5.1% were stunted, underweight, and wasted, respectively. Almost half of the children (49.8%) were female, and 22.0% lived in urban areas. The estimated odds of children from secondary and higher education mothers being stunted and wasted were 0.987; 95% CI: 0.979 – 0.994 and 0.999; 95% CI: 0.995 – 0.999, respectively, times the estimated odds of children from no education mothers. Children from middle-class families were less likely to be underweight than children from poorer families.
Conclusion
The prevalence of stunting was higher than in the sub-Saharan Africa region, but the prevalence of wasting and underweight was lower. According to the study's findings, undernourishment among young children under the age of five continues to be a significant public health issue in the East African region. Governmental and non-governmental organizations should therefore plan public health participation focusing on paternal education and the poorest households in order to improve the undernutrition status of children under five. Additionally, improving the delivery of healthcare at health facilities, places of residence, children's health education, and drinking water sources are essential for lowering child undernutrition indicators.
Similar content being viewed by others
Introduction
Malnutrition is the main cause of illness and death in children under the age of five [1]. It affects millions of children worldwide, putting their health and future in jeopardy [2]. Even though the decline has not been consistent worldwide, its prevalence has decreased. In middle- and low-income countries, notably in Sub-Saharan Africa, child malnutrition is still an issue, and many children still suffer from chronic malnutrition [3, 4]. The most common symptom of chronic undernutrition in children is an inadequate intake of the nutrients and energy needed for growth and development [5]. Three anthropometric indices of malnutrition, stunting, underweight, and wasting, are used to evaluate nutritional deficiency or imbalance, the underlying causes of a number of children's health problems [6,7,8]. The three are well-known indicators of the severity of child malnutrition [9]. In poor countries, malnutrition contributes to more than half of under-five mortality. Sub-Saharan Africa has a very high proportion of under-five malnourished children, and daily death rates are rising [7].
Indicators of child malnutrition include stunting, wasting, and underweight, which refer to children who are, respectively, too short for their age (low height-for-age), too thin for their height (low weight-for-height), and too thin for their age (low weight-for-age). Height-for-age, weight-for-height, and weight-for-age z-scores are generated using the 2006 WHO child growth standards. Children who have a weight-for-height z-score (WHZ), a height-for-age z-score (HAZ), or a weight-for-age z-score (WAZ) below two are referred to as stunting, wasting, and underweight, respectively [6]. According to UNICEF, environmental, social, and economic factors all have a major impact on childhood malnutrition [8].
Each year, more than half of all children under the age of five die from malnutrition and its complications [10]. It has been established that undernourishment has a major negative impact on young children's growth and development [11]. The negative effects of childhood malnutrition are both short-term and long-term [12]. Long-term effects of undernutrition include poor educational practices [13], early mortality [11], and an increased risk of chronic illnesses like diabetes mellitus (DM), hypertension (HTN), and heart disease [14, 15]. Short-term effects of undernutrition include increased severity of illnesses [16], a delayed recovery period from disease [17], and delayed physical and mental development in children [18]. Additionally, undernutrition has a detrimental effect on female adolescents' reproductive health [19, 20]. Due to how frequently it occurs, undernutrition not only has detrimental impacts on a person's health but also negatively affects the economy. Through both direct production reduction owing to physical infirmity and indirect cognitive dysfunction and educational impairments, this condition limits economic growth and perpetuates poverty. In addition, a poor diet raises the cost of medical care [21].
In 2020, undernutrition was a factor in about half of the cases of childhood mortality [22]. In the same year, 12.6% of children under the age of five are underweight, 6.7% are wasted, and 22% are stunted [22]. Around 149.2 million children under the age of five were affected by stunting in 2020, with 53% of these children residing in Asia and 30.7% in Africa [22]. 45.4 million Children under the age of five perished because of waste. More than two-thirds of all wasted children are located in Asia, and more than a quarter are found in Africa [22]. Stunting occurs more frequently in Eastern Africa (32.6%) than in Western Africa (30.9%), Northern Africa (21.4%), or Southern Africa (23.3%), according to a more thorough analysis of the distribution of undernutrition on the African continent [22].
Numerous factors contribute to childhood stunting, wasting, and being underweight. The collective causes reported by several studies include the age of the child in a month [23,24,25,26], the gender of the child [27, 28], the birth size of children [29, 30], the birth order of the child [31, 32], age of mother at first birth and the maternal education [32, 33], household wealth index [23, 31, 34], the source of drinking water [24, 34], the family size [27], the place of residence [27], the husband’s education level [31, 34], breastfeeding [35, 36], diarrhea [36, 37], fever [35] and cough [36, 38] in the last two weeks prior to the survey, the birth type of child [24, 32], number of children aged under-five [30] have been identified as some of the factors of childhood undernutrition status in East Africa.
Numerous studies on stunting, underweight, and wasting were carried out in East Africa. However, they paid little attention to their relationship and were unable to identify the associated determinants of anthropometric indicators among East African children under the age of five. In a study carried out in Ethiopia, India, and Malawi [9, 39, 40], the link between undernutrition indices was examined. The association was determined without taking into account the impact of additional factors linked to stunting, underweight, and wasting. Other East African and international researchers examined each indicator of undernutrition separately and determined the corresponding factors [32, 41,42,43,44]. However, it was noted that there is a dearth of research available or undertaken in East Africa that identifies and estimates the drivers of undernutrition indicators in children under the age of five, such as stunting, underweight, and wasting, by taking into account the relationships between them. Furthermore, despite the fact that the population of East Africa is not uniform in terms of its culture, language, and other characteristics, the cluster effect receives little consideration. When there is a chance that the outcomes of patients in comparable groups may correlate, clustering effects may develop, which may lead to a loss of observational independence [45]. Children from the same nation are more likely to have similar undernutrition status than children from different countries; therefore, when the cluster effect is ignored, the key determinants of a child's undernutrition status within and between countries (cluster) are inadequately taken into account. As a result, the aim of this study was to identify and estimate the influence of significant factors on indicators of undernutrition.
Method
Data from the Demographic and Health Survey (DHS), which was conducted using a cross-sectional study methodology, were used in this investigation. For this particular study, we used Kids Record (KR) files, which include data on moms and children. We predict that children in the same cluster will be more similar than children across the country because the DHS data had a hierarchical structure and children were nested within clusters. The heterogeneity between clusters should therefore be taken into consideration using sophisticated models. A mixed-effect logistic regression model was therefore built (with both fixed and random effects).
Data source and sampling method
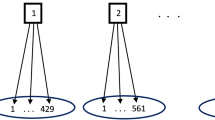
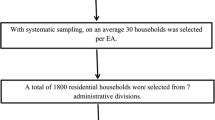
The current study is based on data from the most recent Demographic and Health Surveys (DHS) conducted in ten East African countries (Burundi, Ethiopia, Comoros, Uganda, Rwanda, Tanzania, Zimbabwe, Kenya, Zambia, and Malawi). All datasets were combined to determine the region's pooled prevalence and related causes of undernutrition indicators among children aged under-five. The DHS survey employed stratified, two-stage cluster sampling. The data was obtained from the Measure DHS website, which can be found at https://dhsprogram.com/Data/terms-of-use.cfm. Variables in this study (both dependents and independents) were taken from the Kid Record (KR file) data set after approval was granted via an online request stating the objective of this study. The current study used a weighted total sample of 53,322 children under the age of five.
Inclusion/exclusion criteria
Children under the age of five who completed relevant forms about personal information and clinical signs met the inclusion criteria. As a result, children who had not completed all relevant information (questionaries’) or who were over the age of five were excluded.
Study variables
Response variables
Once the \({Z}_{i}\) for each child is calculated, the undernutrition indices were recoded into dichotomies variables as:
-
stunted \((0 = No\,if\,HAZ \ge - 2\,and\,1 = Yes\,if\,HAZ < - 2)\),
-
wasted \((0 = No\,if\,WHZ \ge - 2\,and\,1 = Yes\,if\,WHZ < - 2)\), and
-
underweight \((0 = No\,if\,WAZ \ge - 2\,and\,1 = Yes\,if\,WAZ < - 2)\)
The outcome variables were measured using WHO 2006 child growth standards [46].
Independent variables
The independent variables were chosen based on previous research on factors influencing children's undernutrition status [47,48,49]. These variables are created by combining naturally continuous and discrete variables into categories. Table 3 lists the independent variables associated with the three-undernutrition indicators and reflected in this study. Face-to-face interviews with mothers and caregivers were used to collect the characteristics listed in Table 3.
Data management and analysis
The variables were extracted from the literature, and then we integrated the DHS data from the 10 East African nations. Before performing any statistical analysis, the data were weighted to restore survey representativeness and take into consideration the sample design for generating standard errors and trustworthy estimates. This was done using sampling weight, a primary sampling unit, and strata. R 4.2.2 was employed for the cross-tabulations and summary statistics. In order to find relevant factors connected to undernutrition indicators, a multilevel, multivariate logistic model was utilized. Adjusted odds ratios (AOR) with a 95% confidence interval (CI) and a p-value less than or equal to 0.05 were used.
In present study, let \({Y}_{1i}, {Y}_{2i} and {Y}_{3i}\) are the dichotomies outcome of stunting, underweight, and wasting of the \({i}^{th}\) under-five years children, respectively. For dichotomies outcome \({Y}_{ji}\) and a vector of independent variables X, multivariate binary logistic regression model is given by [50]:
Where \({\pi }_{j(X)}=P({Y}_{ji}={}^{1}\!\left/ \!{}_{X}\right.)\), the probability of the \({i}^{th}\) children aged under-five being stunted (\({Y}_{1i}\)), underweight (\({Y}_{2i}\)), and wasting (\({Y}_{3i}\)) given other predictors X. Regularly, the logit (log odds) that marked linear association with independent variables can be stated as:
The odds ratio is the best method that is used to measure the relationship between categorical variables in the logistic regression model. It is the proportion of odds defined as:
Multilevel multivariate logistic regression
Separate evaluations of anthropomorphic indicators, including underweight, stunting, and wasting, in children under the age of five were carried out in several studies [6, 25, 27, 29, 30, 51]. In this instance, logistic regression analysis is sufficient for determining the covariate's impact on the dependent variable. The relationship between the anthropomorphic indicators, however, would not be taken into account in a separate analysis. It is more logical to account for the relationship between estimates of covariate effects and anthropometric indices using a multivariate logistic regression model [49]. It is used to simultaneously model several interesting categorical outcomes and analyze how they relate to other factors [47, 52].
To quantify the impact of variables on anthropometric measures in a nation with a varied population, like East Africa, a multivariate logistic regression model is insufficient. According to DHS data gathered from children living in different nations in East Africa, there is a very high probability of a clustering effect. If there is a clustering effect in the dataset, the results will be disorganized. The intraclass correlation coefficient (ICC) [47, 53] and median odds ratio (MOR) [54] were used to assess the clustering effect. The ICC can be calculated using the formula shown below:
where \({\widehat{\sigma }}_{r}^{2}\) and \({\widehat{\sigma }}^{2}\) are the estimated cluster variance (regarding to country) and residual variance, respectively [47, 53]. The \(MOR\) is defined as: \(MOR=exp\left[0.6745\sqrt{2{\widehat{\sigma }}_{r}^{2}}\right]\) [47, 52]. After arranging the data in SPSS 26, the statistical analysis was carried out using R software, VGAM, and the GLMER package.
Prior to fitting the model, it is necessary to assess the model's suitability or goodness of fit. The evaluated model's forecasting ability may help to understand this. In a multivariate logistic regression model, the concordance proportion is frequently used to assess or identify the predictive power. The concordance value calculates the likelihood that the predictions and results are in agreement, or whether the anticipated outcome matches the actual outcome [50]. In order to assess how well the projected model approximates the data, the concordance proportion was evaluated in this study.
Results
Characteristics of the outcome variables
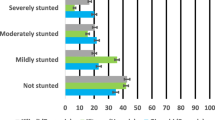
This study included a weighted total of 53,322 children aged under-five, with 34.7% (18,527), 14.8% (7894), and 5.1% (2743) suffering from stunting, underweight, and wasting, respectively (Table 1). The prevalence of stunting, underweight, and wasting was different across countries. The prevalence of stunting, wasting, and underweight was lowest in Zimbabwe (25.3%), Rwanda (2.3%), and Zimbabwe (7.5%), respectively, whereas the prevalence of stunting, wasting, and underweight was highest in Burundi (55.3%), the Comoros (11.0%), and Burundi (286.6%), respectively (Table 2).
Characteristics of the Independent variables
The result of Table 3 revealed that more than half (50.2%) of children aged under-five were males, and 79.2% of them were in the age group of 12 to 59 months. More than half of the mothers (57.5%) had their first child when they were under the age of 20. 45.4% of children aged under-five were born into poor households. More than three-fourths of (78.0%) householders were rural settlers. The overall prevalence of stunting, underweight, and wasting among children aged under-five in the region was 34.7, 14.6, and 5.1%, respectively.
The results in Tables 4 and 5 indicated that children under five were affected by more than one of the three undernutrition indicators; as a result, consideration is essential in empathetically treating the total number of malnourished children. For example, 5689 (10.67%) of the children were both stunted and underweight. For more detail, see the results in Tables 4 and 5.
The whole prevalence of indicators of undernourishment was measured by the composite index of anthropometric failure (CIAF) [55]. Accordingly, children aged under-five can be grouped into eight categories: no failure; stunted only; underweight only; wasted only; stunted and underweight; underweight and wasted; and stunted, underweight, and wasted. According to the composite index of failure, approximately 39.15% = (22.48 + 0.86 + 10.67 + 1.68 + 0.60) % of children aged under-five were diagnosed with malnutrition, whereas 60.85% of the children sampled in East Africa were not diagnosed with malnutrition. The result indicates that 39.15% of children were stunted, underweight, or wasted. This suggests that the occurrence of overall undernourishment in children is about 39.15% in the region.
Table 6 shows all of the possible pairwise relationships between stunting, underweight, and wasting using odds ratios (OR). The odds ratios for the dependency among stunting and underweight, stunting and wasting, and underweight and wasting were 3.566, 1,121, and 2.941, respectively. The result is different from unity. This indicates a dependency between the three anthropometric indicators, and hence fitting a multivariate logistic model for the three dependents is suitable to include their dependency and estimate the effects of the predictors.
Table 7 shows the bivariate analysis of the relationship between independent variables and each of the undernourishment indicators and the distribution of scores below five at each level of the independent variables. Place of residence, education level of mother, source of drinking water, family size, number of children aged under-five, wealth index, age of mother at first birth, education level of husband, birth order of children, birth type of children, sex of children, place of delivery, and size of children at birth were independent variables that were independently associated (p-value 0.05) with the three undernourishment indicators.
Parameter estimation
Random effect model
The calculated ICCs for stunting, underweight, and wasting were 59.1%, 55.87%, and 56.61%, respectively, which is a high value. This strongly suggests that there is a clustering effect and that there is between-group variability that would benefit from a cluster effect due to country. A high ICC, in this sense, indicates a high degree of similarity among children from the same country who have undernutrition indicators. On the other hand, the estimated clustering variance on stunting (\({\widehat{\sigma }}_{rs}^{2}\)), underweight (\({\widehat{\sigma }}_{ru}^{2}\)) and wasting (\({\widehat{\sigma }}_{rw}^{2}\)) found to be significant (p-value 0.05) in the model indicates that there is a country effect in the model. Stunting (MOR = 1.593), underweight (MOR = 1.492), and wasting (MOR = 1.515) have different MOR values. This indicates that there is significant clustering variation. To take into account the cluster effect because of country, a multilevel multivariate logistic regression model was applied because the traditional model cannot remove the cluster effect because the traditional model cannot remove the cluster effect (see Table 8).
Fixed effect model
The independent variables that were included in the current study were: the education level of the mother, place of delivery, birth size of children, age of children, and the husband's education level. These common predictors were significantly associated with the three undernourishment indices. Fever and diarrhea in the two weeks prior to the survey, gender of children, birth type of children, wealth status of the household, number of children aged under-five in the household, source of drinking water, and place of residence were common determinants that were significantly associated with both stunting and underweight. Where family size and birth order of children were predictors that were significantly associated with stunting (Table 8).
A multilevel multivariate binary logistic regression model for estimation of undernourishment indicators was used to calculate concordant and discordant indices. 79.8% of children under the age of five with undernourishment indicators such as stunting, underweight, and waste would have a good chance of estimating their stunting, underweight, and waste levels. In this respect, the concordant index was very high. Indicating that the model's ability to explain the association between the indicators was very decent and fit the data well.
Discussion
In this study, the impacts of the independent variables were assessed using data from a recent demographic health survey in east Africa to examine the association between undernutrition indicators such as stunting, underweight, and wasting in children under the age of five. This research discovered a strong link between stunting, wasting, and underweight status. Furthermore, it was discovered that underweight is a composite measure of stunting and wasting when the relationship between the three indicators is looked at, even when the impacts of other independent variables are not taken into consideration. Previous studies from Ethiopia, India, and Malawi [9, 39, 40] support this conclusion.
In this study, the prevalence of stunting, underweight, and wasting were 34.7, 14.8, and 5.1%, respectively. The prevalence of wasting and underweight were lower than the study reported in sub-Saharan Africa [3], but higher than the study reported in India [39], whereas the prevalence of stunting was higher than the study reported in sub-Saharan Africa [3]. This is due to the fact that the region is clearly affected by food scarcities, harsh climatic conditions, and drought situations, as well as inadequate access to land for farming purposes [56]. These dynamics extremely challenge progress toward improving farming efficiency, nutrition security, and child nutrition in east Africa.
The mother's education level, the location of the delivery, the size at birth and age of the children, as well as the husband's education level, were found to be the common predictors that were significantly linked to the three undernourishment indices. This is in line with earlier research in Sub-Saharan Africa and Ethiopia [24, 43]. The likelihood of children being stunted, underweight, or wasted decreased as father education increased, which was consistent with research conducted in Ethiopia [57]. Children born in medical institutions had a lower chance of being stunted, underweight, or wasted. Which agreed with the results of a study conducted in Sub-Saharan Africa [46]. A child with a small birth size has a higher risk of developing malnutrition than a child with an average birth size. Which was in line with the research in Ethiopia and Sub-Saharan Africa [46, 57]. According to a recent study, a child's nutritional indicators were highly correlated with the child's age. This result is in line with research conducted in Burkina Faso, Ethiopia, and Bangladesh [26, 58,59,60], which discovered that a child's risk of malnutrition rose with age. The late introduction of supplemental foods with poor nutritional value is one potential cause [61].
Common determinants that were significantly associated with stunting and underweight included fever and diarrhea in the two weeks prior to the survey, the gender of the children, their birth type, the wealth status of the household, the number of children under the age of five living in the household, the source of drinking water, and their place of residence, which is consistent with the findings in Ethiopia [24]. According to results from research in Gahanna and Pakistan [36, 37], children who had a fever two weeks prior to the survey period had a higher risk of stunting and underweight than children who had no fever at the time. Children who experienced diarrhea two weeks before the survey were more likely to be stunted and underweight than those who did not. This outcome is congruent with what was discovered in Ethiopia throughout the study [34]. The supplementary study showed that stunting and underweight were more common in males than females among east African children. This is consistent with the earlier Burkina Faso study [58]. One possible explanation is that, even after accounting for gestational phase and body size, boys still experience more complex childhood illnesses than females [62]. Children from mothers who had multiple births were more likely to have stunting and be underweight compared to singleton children at birth, which is similar to the Ethiopian research [24]. This finding further demonstrates the correlation between the wealth index and stunting and underweight. In line with the findings of an earlier study conducted in Bangladesh [33], a child from a low-wealth index household is more likely to be stunted and underweight. Increased revenue may be the cause, which boosts nutritional variety [63] and, in turn, boosts nutrient intake and nutritional status. This finding suggests that the risk that a kid would be stunted and underweight increases with the number of children under the age of five living in a household. This finding is consistent with the earlier research in Ghana [36]. Stunting and underweight were significantly influenced by the source of drinking water. Those from families without an improved source of water were more likely to have stunting and be underweight when compared to those who do. This study supports the conclusions of a prior investigation conducted in Ethiopia [34].
Conclusion
The mother's education level, place of delivery, the size at birth, the age of the children, and the husband's education level were identified to be the common predictors that were significantly linked to the three undernourishment indices in this study. Common factors that were significantly associated with stunting and underweight included fever and diarrhea in the two weeks prior to the survey, the gender of the children, the type of birth the children had, the wealth status of the household, the number of children under the age of five in the household, the source of drinking water, and the location of residence. Family size and child birth order, however, were the only variables that were strongly linked with stunting. According to the study's findings, undernourishment among young children under the age of five continues to be a significant public health issue in the East African region. Governmental and non-governmental organizations should therefore plan public health engagement focusing on maternity and child mothers' husbands' education and the poorest households in order to improve children under the age of five's undernutrition status. Additionally, improving the delivery of healthcare at health facilities, places of residence, children's health education, and drinking water sources is essential for lowering child undernutrition indicators.
Availability of data and materials
The data used in this study are from the Measure DHS program https://dhsprogram.com/Data/terms-of-use.cfm, and can be accessed following the protocol outlined in the Methods section. Further documentations on ethical issues relating to the surveys are available at http://dhsprogram.com.
Abbreviations
- DHS:
-
Demographic health survey
- EAs:
-
Enumeration areas
- GDHS:
-
Gambian demographic and health survey
- Ref.:
-
Reference Category
- HAZ:
-
Height for age standardized score
- ICF:
-
International Coaching Federation
- WAZ:
-
Weight for age standardized score
- WHZ:
-
Weight for height standardized score
- OR:
-
Odds ratio
- UNDP:
-
Untied Nation Development Program
References
Organisation mondiale de la santé. World Health Statistics 2018: Monitoring Health for the SDGs Sustainable Development Goals. World health organization. 2018.
Seboka BT, et al. Spatial variations and determinants of acute malnutrition among under-five children in Ethiopia: evidence from 2019 Ethiopian Demographic Health Survey. Ann Glob Health. 2021;87(1).
Akombi BJ, et al. Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006–2016). PLoS ONE. 2017;12(5): e0177338.
Saaka M, Galaa SZ. Relationships between wasting and stunting and their concurrent occurrence in Ghanaian preschool children. J Nutr Metab. 2016.
Carlsen L, Bruggemann R. The 17 United Nations’ sustainable development goals: A status by 2020. Int J Sustain Dev World Ecol. 2022; 29(3):219-29.
Khan S, Zaheer S, Safdar NF. Determinants of stunting, underweight and wasting among children< 5 years of age: evidence from 2012–2013 Pakistan demographic and health survey. BMC Public Health. 2019;19(1):1–15.
Babatunde RO, et al. Prevalence and determinants of malnutrition among under-five children of farming households in Kwara State, Nigeria. J Agric Sci. 2011;3(3):173–81.
Duru CB, et al. Prevalence and sociodemographic determinants of malnutrition among under-five children in rural communities in Imo State. Nigeria Am J Public Health Res. 2015;3(6):199–206.
Kassie GW, Workie DL. Exploring the association of anthropometric indicators for under-five children in Ethiopia. BMC Public Health. 2019;19(1):1–6.
Rao V, et al. Undernutrition & childhood morbidities among tribal preschool children. Indian J Med Res. 2005;122(1):43.
Dewey KG, Begum K. Long-term consequences of stunting in early life. Matern Child Nutr. 2011;7:5–18.
Reinhardt K, Fanzo J. Addressing chronic malnutrition through multi-sectoral, sustainable approaches: a review of the causes and consequences. Front Nutr. 2014;1:13.
Haile D, et al. Height for age z score and cognitive function are associated with Academic performance among school children aged 8–11 years old. Archives of Public Health. 2016;74(1):1–7.
Uauy R, et al. Nutrition, child growth, and chronic disease prevention. Ann Med. 2008;40(1):11–20.
Sawaya AL, et al. Association between chronic undernutrition and hypertension. Matern Child Nutr. 2005;1(3):155–63.
Nove A, et al. Maternal mortality in adolescents compared with women of other ages: evidence from 144 countries. Lancet Glob Health. 2014;2(3):e155–64.
Saunders J, Smith T. Malnutrition: causes and consequences. Clin Med. 2010;10(6):624.
Branca F, Ferrari M. Impact of micronutrient deficiencies on growth: the stunting syndrome. Ann Nutr Metab. 2002;46(Suppl. 1):8–17.
Konje JC, Ladipo OA. Nutrition and obstructed labor. Am J Clin Nutr. 2000;72(1):291S-297S.
Kruger H. Maternal anthropometry and pregnancy outcomes: a proposal for the monitoring of pregnancy weight gain in outpatient clinics in South Africa. Curationis. 2005;28(4):40–9.
Martins VJ, et al. Long-lasting effects of undernutrition. Int J Environ Res Public Health. 2011;8(6):1817–46.
World Health Organization. Levels and trends in child malnutrition. UNICEF; 2021.
Woldeamanuel BT, Tesfaye TT. Risk factors associated with under-five stunting, wasting, and underweight based on Ethiopian demographic health survey datasets in Tigray region, Ethiopia. J Nutr Metab. 2019.
Kassie GW, Workie DL. Determinants of under-nutrition among children under five years of age in Ethiopia. BMC Public Health. 2020;20(1):1–11.
Habaasa G. An investigation on factors associated with malnutrition among underfive children in Nakaseke and Nakasongola districts. Uganda BMC pediatrics. 2015;15(1):1–7.
Ahmadi D, et al. Determinants of child anthropometric indicators in Ethiopia. BMC Public Health. 2018;18(1):1–9.
Tekile AK, Woya AA, Basha GW. Prevalence of malnutrition and associated factors among under-five children in Ethiopia: evidence from the 2016 Ethiopia Demographic and Health Survey. BMC Res Notes. 2019;12(1):1–6.
Gebru KF, et al. Determinants of stunting among under-five children in Ethiopia: a multilevel mixed-effects analysis of 2016 Ethiopian demographic and health survey data. BMC Pediatr. 2019;19(1):1–13.
Nshimyiryo A, et al. Risk factors for stunting among children under five years: a cross-sectional population-based study in Rwanda using the 2015 Demographic and Health Survey. BMC Public Health. 2019;19(1):1–10.
Sultana P, Rahman Md M, Akter J. Correlates of stunting among under-five children in Bangladesh: a multilevel approach. BMC nutr. 2019;5:41.
Pravana NK, et al. Determinants of severe acute malnutrition among children under 5 years of age in Nepal: a community-based case–control study. BMJ Open. 2017;7(8): e017084.
Tesema GA, et al. Pooled prevalence and associated factors of chronic undernutrition among under-five children in East Africa: a multilevel analysis. PLoS ONE. 2021;16(3): e0248637.
Talukder A. Factors associated with malnutrition among under-five children: illustration using Bangladesh demographic and health survey, 2014 data. Children. 2017;4(10):88.
Mohammed S, Asfaw ZG. Bayesian Gaussian regression analysis of malnutrition for children under five years of age in Ethiopia, EMDHS 2014. Archives of Public Health. 2018;76(1):1–11.
Dapi Nzefa L, Monebenimp F, Äng C. Undernutrition among children under five in the Bandja village of Cameroon. Africa South African J Clin Nutr. 2019;32(2):46–50.
Miah R, Apanga P, Abdul-Haq Z. Risk factors for undernutrition in children under five years old: evidence from the 2011 Ghana multiple indicator cluster Survey. J AIDS Clin Res. 2016;7(585):2.
Khan GN, et al. Prevalence and associated factors of malnutrition among children under-five years in Sindh, Pakistan: a cross-sectional study. BMC nutrition. 2016;2(1):1–7.
Akombi BJ, et al. Multilevel analysis of factors associated with wasting and underweight among children under-five years in Nigeria. Nutrients. 2017;9(1):44.
Gupta AK, Borkotoky K. Exploring the multidimensional nature of anthropometric indicators for under-five children in India. Indian J Public Health. 2016;60(1):68.
Ngwira A, Munthali EC, Vwalika KD. Analysis on the association among stunting, wasting and underweight in Malawi: an application of a log-linear model for the three-way table. J Public Health Africa. 2017;8(1).
Quamme SH, Iversen PO. Prevalence of child stunting in Sub-Saharan Africa and its risk factors. Clin Nutr Open Sci. 2022;42:49-61.
Amadu I, et al. Risk factors associated with the coexistence of stunting, underweight, and wasting in children under 5 from 31 sub-Saharan African countries. BMJ Open. 2021;11(12): e052267.
Adedokun ST, Yaya S. Factors associated with adverse nutritional status of children in sub-Saharan Africa: Evidence from the Demographic and Health Surveys from 31 countries. Matern Child Nutr. 2021;17(3): e13198.
Panigrahi A, Das SC. Undernutrition and its correlates among children of 3–9 years of age residing in slum areas of Bhubaneswar, India. Sci World J. 2014.
Oltean H, Gagnier JJ. Use of clustering analysis in randomized controlled trials in orthopaedic surgery. BMC Med Res Methodol. 2015;15(1):1–8.
Rutstein SO, Rojas G. Guide to DHS statistics, vol. 38. Calverton: ORC Macro; 2006. p. 78.
Tesfaw LM, Dessie ZG. Multilevel multivariate analysis on the anthropometric indicators of under-five children in Ethiopia: EMDHS 2019. BMC Pediatr. 2022;22(1):1–13.
Tesfaw LM, Fenta HM. Multivariate logistic regression analysis on the association between anthropometric indicators of under-five children in Nigeria: NDHS 2018. BMC Pediatr. 2021;21(1):1–13.
Asmare AA, Agmas YA. Determinants of coexistence of stunting, wasting, and underweight among children under five years in the Gambia; evidence from 2019/20 Gambian demographic health survey: application of multivariate binary logistic regression model. BMC Public Health. 2022;22(1):1621.
Agresti A. An introduction to categorical data analysis. 2018;39–42.
Kejo D, et al. Prevalence and predictors of undernutrition among underfive children in Arusha District. Tanzania Food science & nutrition. 2018;6(8):2264–72.
Alamolhoda M, et al. A multivariate multilevel analysis of the risk factors associated with anthropometric indices in Iranian mid-adolescents. BMC Pediatr. 2020;20:1–9.
Ene M, Leighton EA, Blue GL Bell BA. Multilevel models for categorical data using SAS® PROC GLIMMIX: The basics. In SAS Global Forum. 2015. p. 3430-2015.
Islam MA, et al. Prevalence and factors associated with early initiation of breastfeeding among Bangladeshi mothers: a nationwide cross-sectional study. PLoS ONE. 2019;14(4): e0215733.
Al-Sadeeq AH, Bukair AZ, Al-Saqladi AWM. Assessment of undernutrition using Composite Index of Anthropo-metric Failure among children aged< 5 years in rural Yemen. East Mediterr Health J. 2018;24(12):1119-26.
Salami A, Kamara AB, Brixiova Z. Smallholder agriculture in East Africa: Trends, constraints and opportunities. Tunisia: African Development Bank Tunis; 2010.
Muche A, et al. Using geographically weighted regression analysis to cluster under-nutrition and its predictors among under-five children in Ethiopia: Evidence from demographic and health survey. PLoS ONE. 2021;16(5): e0248156.
Poda GG, Hsu C-Y, Chao JC-J. Factors associated with malnutrition among children< 5 years old in Burkina Faso: evidence from the Demographic and Health Surveys IV 2010. Int J Qual Health Care. 2017;29(7):901–8.
Endris N, Asefa H, Dube L. Prevalence of malnutrition and associated factors among children in rural Ethiopia. BioMed Res Int. 2017.
Das S, Gulshan J. Different forms of malnutrition among under five children in Bangladesh: a cross sectional study on prevalence and determinants. BMC Nutrition. 2017;3(1):1–12.
Dasgupta A, et al. Assessment of under nutrition with composite index of anthropometric failure (CIAF) among under-five children in a rural area of West Bengal. Indian J Community Health. 2014;26(2):132–8.
Haile D, et al. Exploring spatial variations and factors associated with childhood stunting in Ethiopia: spatial and multilevel analysis. BMC Pediatr. 2016;16(1):1–14.
Doan D. Does income growth improve diet diversity in China? 2014.
Acknowledgements
The authors are grateful to the measure of DHS program for giving us permission to use the data for our purpose.
Funding
The authors have no support or funding to report.
Author information
Authors and Affiliations
Contributions
AA wrote the proposal, analyzed the data and manuscript writing. YA accredited the proposal with revisions, analysis the data and manuscript writing. Both YA and AA read and approved the very last manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current study was built on the analysis of openly accessible secondary data with all identifier information were removed. The Institutional Review Board (IRB) of ICF Macro at Fairfax, Virginia in the USA reviewed and approved the MEASURE DHS Project Phase three. The 2010–2018 DHS’s are considered under that approval. The IRB of ICF Macro complied with the United States Department of Health and Human Services requirements for the “Protection of Human Subjects” (45 CFR 46). The IRB approved procedures for DHS public use datasets do not in any way allow respondents, households, or sample communities to be identified. There are no names of individuals or household addresses in the data files. The geographic identifiers only go down to the regional level (where regions are typically very large geographical areas encompassing several states/provinces). Each enumeration area (Primary Sampling Unit) has a PSU number in the data file, but the PSU numbers do not have any labels to indicate their names or locations. In surveys that collect GIS coordinates in the field, the coordinates are only for the enumeration area (EA) as a whole, and not for individual households, and the measured coordinates are randomly displaced within a large geographic area so that specific enumeration areas cannot be identified. In addition, written informed consent was obtained from a parent or guardian for participants under 16 years old. DHS Program has remained consistent with confidentiality and informed consent over the years. We obtained express approval to use the data from ICF Macro. No further approval was required for this study.
The data owners can be contacted at https://dhsprogram.com/Data/terms-of-use.cfm and data can be found at https://www.dhsprogram.com/data/dataset_admin/login_main.cfm. Further documentations on ethical issues relating to the surveys are available at http://dhsprogram.com. We confirm that all methods were carried out in accordance with the relevant guidelines and regulation.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Asmare, A.A., Agmas, Y.A. Multilevel multivariate modeling on the association between undernutrition indices of under-five children in East Africa countries: evidence from recent demographic health survey (DHS) data. BMC Nutr 9, 82 (2023). https://doi.org/10.1186/s40795-023-00741-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40795-023-00741-w