
Abstract
Background
Nilotinib inhibits the tyrosine kinase activities of ABL1/BCR-ABL1, KIT, and platelet-derived growth factor receptors (PDGFRs). The results of a phase III clinical trial indicated that nilotinib could not be recommended for broad use as first-line therapy for gastrointestinal stromal tumor (GIST). However, some clinical studies have reported the effectiveness of nilotinib. We report here the cases of two patients who underwent surgical resections of nilotinib-resistant lesions after long-term nilotinib administration.
Case presentation
Two Japanese female patients, aged 66 and 70 years, experienced peritoneal recurrence of intestinal GIST several years after surgery. Both were registered in the ENESTg1 trial and received nilotinib therapy. Although they continued nilotinib administration with a partial response according to the protocol, nilotinib-resistant lesions, which were diagnosed as focally progressive disease, developed and complete surgical resection was performed. Pathological examination revealed that the tumors were composed of viable KIT-positive spindle cells, and the recurrent tumors were diagnosed as nilotinib-resistant GIST. In gene mutation analysis, a secondary KIT gene mutation was detected in one case. Both patients have survived more than 5 years after the first surgery.
Conclusions
Of patients who were registered in this trial, we have encountered two patients with long-term effects after nilotinib administration. Moreover, secondary mutations in the KIT gene, similar to those involved in resistance to imatinib, might be involved in resistance to nilotinib.
Similar content being viewed by others


Background
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal neoplasms of the gastrointestinal tract [1–4]. In 2000, imatinib, a selective tyrosine kinase inhibitor (TKI), was introduced for GIST therapy [5]. Since then, the prognoses of patients with unresectable and metastatic GIST have dramatically improved [6–9]. Worldwide, imatinib is the standard first-line therapy for patients with GISTs that are metastatic, unresectable, or both. However, despite such high clinical efficacy, imatinib treatment cannot achieve complete disease control. Nearly 90% of patients undergoing imatinib therapy experience disease progression following a significant response despite treatment continuation. Various treatments are available for patients with secondary imatinib resistance. In cases with limited progression wherein there are few lesions with a limited distribution, local therapies, including surgical resection, have been effective [10–12]. Moreover, gene mutation analysis revealed that lesions acquired resistance via secondary KIT mutations in addition to primary KIT mutations. Acquired resistance to imatinib is most commonly caused by secondary KIT mutations in other exons that arise during tyrosine kinase inhibitor therapy [6, 13–17].
Nilotinib is a selective tyrosine kinase inhibitor that targets ABL1, BCR-ABL, KIT, PDGFRα and PDGFRβ, and DDR-1 and DDR-2. Nilotinib has in vitro inhibitory activity similar to that of imatinib against KIT and platelet-derived growth factor receptors (PDGFRs) [18–20]. A phase III trial (ENESTg1) was performed to clarify the efficacy and safety of nilotinib compared to imatinib as first-line therapy for patients with advanced GISTs. In these trial results, although tolerance to nilotinib was similar to that of imatinib, nilotinib treatment failed to show superiority based on the primary end point of progression free-survival [21]. Because of this, nilotinib could not replace imatinib as first-line therapy for metastatic GIST. However, we have encountered two patients who have experienced long-term effects after nilotinib administration in the ENESTg1 trial and showed focal resistance. We resected each resistant lesion and continued molecular targeting therapy.
In this report, we assessed the therapeutic strategy and mechanism of nilotinib resistance.
Case presentation
Patient 1
A 76-year-old woman was diagnosed with a small intestinal primary GIST and underwent partial jejunum resection via open surgery. The tumor stained positively for CD117 (KIT) and CD34, and it was composed of spindle cells with >5 mitoses/50 high-power fields (HPF). Gene mutation analysis revealed a Lys (AAG) 558 to Asn&Pro (AACCCG) KIT mutation in exon 11. Postoperatively, she was followed-up strictly without adjuvant therapy. Two years after operation, a 15-mm peritoneal metastasis was discovered in the mesentery (Fig. 1a). We informed her of the randomized phase III trial (ENESTg1), and she agreed to enroll in the trial. After assignment to the nilotinib arm, she was treated with nilotinib. Because of several adverse events, including grade 2 appetite loss and skin bruising, she continued this treatment for 57 months at a decreased nilotinib dose according to the protocol guidelines and achieved a partial response (Fig. 1b).

Case 1 imaging findings. a Abdominal CT at study enrollment. b Abdominal CT 3 months after start of nilotinib therapy. c Abdominal CT of the developing nilotinib-resistant tumor
Fifty-seven months after nilotinib administration, she experienced abdominal distention and vomiting. From imaging examinations, she was diagnosed with ileus due to a recurrent tumor (Fig. 1c). Since we diagnosed her with focal resistance, she underwent surgical tumor resection (Fig. 2a and b). Pathological examination revealed that the tumor was composed of viable spindle cells with 15 mitoses/50 HPF that stained positively for CD117 (KIT) and CD34 (Fig. 2c–f). From the above findings, we diagnosed the patient with recurrent nilotinib-resistant GIST. According to gene mutation analysis, the resistant GIST contained the same genetic KIT mutation in exon 11 observed in the primary GIST without any secondary mutations. After an additional surgery, nilotinib administration has been continued for 21 months, with no evidence of recurrence.

Case 1 surgical and pathological images. a, b Intraoperative photography. c Hematoxylin and eosin staining (×400). d–f Immunohistochemical staining of KIT/CD117 (d), CD34 (e), and MIB-1 (f) (×400)
Patient 2
Similar to the patient in case 1, a 66-year-old woman was diagnosed with a primary submucosal tumor in the small intestine and underwent partial jejunum resection via open surgery. The tumor stained positively for CD117 (KIT) and was composed of spindle cells with 19 mitoses/50 HPF. From the above findings, tumor was finally diagnosed as a GIST originating from the small intestine. Gene mutation analysis revealed a Del-5a.a (557-561) KIT mutation in exon 11. She received postoperative adjuvant imatinib (400 mg daily) for 1 year. As adverse events of imatinib, she experienced leukopenia (grade 3), thrombopenia (grade 2), and leg edema (grade 1). Four years after the operation, a 77-mm peritoneal metastasis was discovered (Fig. 3a). We informed her of the randomized phase III trial (ENESTg1), and she agreed to enroll. After assignment to the nilotinib arm, she was treated with nilotinib. She experienced no adverse events. She continued this treatment with a partial response for 41 months, according to the protocol guidelines (Fig. 3b).

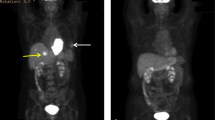
Case 2 imaging findings. a Abdominal CT at study enrollment. b Abdominal CT 3 months after start of nilotinib therapy. c Abdominal CT (C-1) and PET-CT (C-2) of the developing nilotinib-resistant tumor
Forty-one months after nilotinib administration, an abdominal computed tomography (CT) scan showed a 55-mm enhanced tumor area in the tumor margin, and fluorodeoxyglucose (FDG) accumulation was observed in the tumor margin by positron emission tomography-CT (PET-CT) (Fig. 3c). Because her tumor exhibited focal progression, she underwent surgical tumor resection (Fig. 4a and b). Pathological examination revealed a tumor composed of viable spindle cells with 34 mitoses/50 HPF and positive CD117 (KIT) staining (Fig. 4c–f). From the above findings, we diagnosed the patient with recurrent nilotinib-resistant GIST. According to gene mutation analysis, the resistant GIST contained not only the primary genetic KIT mutation in not only exon 11 but also secondary KIT mutation in exon 13 (Asn655Thr). After an additional surgery, since the nilotinib clinical trial was complete, we suggested that the patient receive imatinib therapy. However, the patient opted for observation only because of adverse events due to imatinib therapy. Sixteen months after reoperation, an abdominal CT scan showed multiple peritoneal metastases. Imatinib (300 mg daily) was administered for recurrence, and the patient now has stable disease (SD).

Case 2 surgical and pathological images. a, b Intraoperative photography. c Hematoxylin and eosin staining (×400). d–f Immunohistochemical staining of KIT/CD117 (d), CD34 (e), and MIB-1 (f) (×400).
We summarized the main characteristics of two cases with nilotinib therapy in Table 1.
Discussion
Nilotinib is a selective tyrosine kinase inhibitor that targets ABL1, BCR-ABL1, KIT, PDGFRα and PDGFRβ, and DDR-1 and DDR-2. It has in vitro inhibitory activity similar to that of imatinib against KIT and PDGFRs [18–20]. For chronic myelogenous leukemia (CML), a phase III randomized controlled trial showed the benefits of first-line nilotinib treatment compared to imatinib [22]. Currently, nilotinib is a first-line treatment for CML according to the National Comprehensive Cancer Network (NCCN) guidelines [23]. Since the same effect as CML has been expected for GIST, clinical trials comparing nilotinib with imatinib have been performed. Previously, nilotinib was reported to be efficacious in imatinib- and/or sunitinib-resistant GIST [24–27]. The randomized multi-center phase III ENESTg1 trial was performed to compare imatinib and nilotinib as first-line treatment for distant metastasis or unresectable GIST [21]. In this trial, 647 people were registered, and patients demonstrated good tolerance to nilotinib compared with imatinib. However, nilotinib did not exhibit superiority in the progression-free survival (PFS) as the primary endpoint, with a PFS of 25.9 months in the nilotinib group vs. 29.7 months in the imatinib group. In addition, in subgroup analysis, patients with exon 11 mutations had better prognosis in overall survival or PFS both imatinib and nilotinib treatment group. In the present cases, the two patients with primary GISTs who participated in the ENESTg1 trial also had KIT mutations in exon 11, suggesting that long-term control of disease progression might be possible.
For patients with imatinib-resistant GIST, although sunitinib is recommended as treatment, surgery and continued imatinib therapy have been effective against focally progressive disease [11, 12, 28, 29]. Hasegawa et al. reported that patients with imatinib-resistant GISTs that are small, have few foci, and are of gastric origin might benefit from surgery plus continued imatinib therapy, with considerable tolerance and safety [30]. Additionally, in the two cases mentioned here, since the patients had good disease control after long-term nilotinib administration and no distant metastasis, similar to the therapeutic strategy for imatinib-resistant GIST, surgical resection was a good option. From pathological examination, we noted positive KIT staining, which was also similar to that seen in imatinib-resistant GIST. Patient 1, who underwent complete surgical resection and continued nilotinib therapy, has lived for 21 months with no recurrence.
In imatinib-resistant lesions, secondary KIT mutations were usually acquired in addition to primary KIT mutations [10–12]. Nishida et al. reported that 33 out of 45 tumors (73%) harbored secondary KIT mutations in the KIT kinase domain in GIST patients treated with imatinib therapy [13]. In case 2, in which the lesion developed resistance during nilotinib administration for recurrent GIST in addition to the primary KIT mutation in exon 11, the resistant lesion had a secondary KIT mutation in exon 13. Secondary mutations may lead to nilotinib resistance, similarly to those involved in imatinib resistance.
In GISTs showing secondary resistance to imatinib, a particular Val654Ala mutation has been detected as the exon 13-type secondary c-kit gene mutation. On the other hand, Asn655Thr mutation at exon 13 of the c-kit gene was observed as a secondary mutation in case 2 with secondary resistance to nilotinib. Kinoshita et al. reported that Asn655Lys mutation at exon 13 which was observed as a primary mutation in a sporadic GIST was imatinib-sensitive [31]. Since the codon number in Asn655Thr and Asn655Lys is the same, there is a possibility that Asn655Thr mutation in the present case 2 might be nilotinib-resistant but imatinib-sensitive. However, the properties of resistance to imatinib and nilotinib might be different from each other in Asn655Thr and Asn655Lys because the substituted amino acid is different between them. Effectiveness of imatinib in Asn655Thr remains to be clarified.
Conclusions
The results of the ENESTg1 trial indicated that nilotinib cannot be recommended instead of imatinib for broad use as first-line treatment for patients with distant metastasis or unresectable GIST. Of patients who were registered in this trial, we have encountered two patients with long-term effects after nilotinib administration. Moreover, with regard to nilotinib resistance, secondary KIT mutations might be involved, similarly to those involved in imatinib resistance.
Abbreviations
- CML:
-
Chronic myelogenous leukemia
- GIST:
-
Gastrointestinal stromal tumor
- HPF:
-
High power fields
- NCCN:
-
National comprehensive cancer network
- PDGFRA:
-
Platelet-derived growth factor receptor
- PET-CT:
-
Positron emission tomography-CT
- PFS:
-
Progression-free survival
- SD:
-
Stable disease
- TKI:
-
Tyrosine kinase inhibitor
References
Miettinen M, Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med. 2006;130:1466–78.
Corless CL, Barnett CM, Heinrich MC. Gastrointestinal stromal tumours: origin and molecular oncology. Nat Rev Cancer. 2011;11:865–78.
Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science. 1998;279:577–80.
Chung JC, Kim HC, Hur SM. Limited resections for duodenal gastrointestinal stromal tumors and their oncologic outcomes. Surg Today. 2016;46:110–6.
Joensuu H, Roberts PJ, Sarlomo-Rikala M, Andersson LC, Tervahartiala P, Tuveson D, et al. Effect of the tyrosine kinase inhibitor STI571 in a patient with a metastatic gastrointestinal stromal tumor. N Engl J Med. 2001;344:1052–6.
Demetri GD, Von Mehren M, Blanke CD, Van den Abbeele AD, Eisenberg B, Roberts PJ, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347:472–80.
Blanke CD, Demetri GD, Von Mehren M, Heinrich MC, Eisenberg B, Fletcher JA, et al. Long-term results from a randomized phase II trial of standard- versus higher-dose imatinib mesylate for patients with unresectable or metastatic gastrointestinal stromal tumors expressing KIT. J Clin Oncol. 2008;26:620–5.
Kanda T, Ishikawa T, Hirota S, Yajima K, Kosugi S, Ohashi M, et al. Prospective observational study of imatinib therapy in Japanese patients with advanced gastrointestinal stromal tumors: long-term follow-up and second malignancy. Jpn J Clin Oncol. 2012;42:578–85.
Sato S, Tsujinaka T, Yamamoto K, Takahashi T, Kishi K, Imamura H, et al. Primary surgery as a frontline treatment for synchronous metastatic gastrointestinal stromal tumors: an analysis of the Kinki GIST registry. Surg Today. 2016;46:1068–75.
Rutkowski P, Nowecki Z, Nyckowski P, Dziewirski W, Grzesiakowska U, Nasierowska-Guttmejer A, et al. Surgical treatment of patients with initially inoperable and/or metastatic gastrointestinal stromal tumors (GIST) during therapy with imatinib mesylate. J Surg Oncol. 2006;93:304–11.
Raut CP, Posner M, Desai J, Morgan JA, George S, Zahrieh D, et al. Surgical management of advanced gastrointestinal stromal tumors after treatment with targeted systemic therapy using kinase inhibitors. J Clin Oncol. 2006;24:2325–31.
DeMatteo RP, Maki RG, Singer S, Gonen M, Brennan MF, Antonescu CR. Results of tyrosine kinase inhibitor therapy followed by surgical resection for metastatic gastrointestinal stromal tumor. Ann Surg. 2007;245:347–52.
Nishida T, Kanda T, Nishitani A, Takahashi T, Nakajima K, Ishikawa T, et al. Secondary mutations in the kinase domain of the KIT gene are predominant in imatinib-resistant gastrointestinal stromal tumor. Cancer Sci. 2008;99:799–804.
Corless CL. Gastrointestinal stromal tumors: what do we know now? Mod Pathol. 2014;27(Suppl):S1–S16.
Lee JH, Kim Y, Choi JW, Kim YS. Correlation of imatinib resistance with the mutational status of KIT and PDGFRA genes in gastrointestinal stromal tumors: a meta-analysis. J Gastrointestin Liver Dis. 2013;22:413–8.
Heinrich MC, Corless CL, Blanke CD, Demetri GD, Joensuu H, Roberts PJ, et al. Molecular correlates of imatinib resistance in gastrointestinal stromal tumors. J Clin Oncol. 2006;24:4764–74.
Antonescu CR, Besmer P, Guo T, Arkun K, Hom G, Koryotowski B, et al. Acquired resistance to imatinib in gastrointestinal stromal tumor occurs through secondary gene mutation. Clin Cancer Res. 2005;11:4182–90.
Manley PW, Stiefl N, Cowan-Jacob SW, Kaufman S, Mestan J, Wartmann M, et al. Structural resemblances and comparisons of the relative pharmacological properties of imatinib and nilotinib. Bioorg Med Chem. 2010;18:6977–86.
Guo T, Agaram NP, Wong GC, Hom G, D’Adamo D, Maki RG, et al. Sorafenib inhibits the imatinib-resistant KITT670I gatekeeper mutation in gastrointestinal stromal tumor. Clin Cancer Res. 2007;13:4874–81.
Manley PW, Drueckes P, Fendrich G, Furet P, Liebetanz J, Martiny-Baron G, et al. Extended kinase profile and properties of the protein kinase inhibitor nilotinib. Biochim Biophys Acta. 1804;2010:445–53.
Blay JY, Shen L, Kang YK, Rutkowski P, Qin S, Nosov D, et al. Nilotinib versus imatinib as first-line therapy for patients with unresectable or metastatic gastrointestinal stromal tumours (ENESTg1): a randomised phase 3 trial. Lancet Oncol. 2015;16:550–60.
Saglio G, Kim DW, Issaragrisil S, Le Coutre P, Etienne G, Lobo C, et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362:2251–9.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) chronic myelogenous leukemia. Version 3.2014 NCCN.org.
Sawaki A, Nishida T, Doi T, Yamada Y, Komatsu Y, Kanda T, et al. Phase 2 study of nilotinib as third-line therapy for patients with gastrointestinal stromal tumor. Cancer. 2011;117:4633–41.
Demetri GD, Casali PG, Blay JY, Von Mehren M, Morgan JA, Bertulli R, et al. A phase I study of single-agent nilotinib or in combination with imatinib in patients with imatinib-resistant gastrointestinal stromal tumors. Clin Cancer Res. 2009;15:5910–6.
Montemurro M, Schöffski P, Reichardt P, Gelderblom H, Schütte J, Hartmann JT, et al. Nilotinib in the treatment of advanced gastrointestinal stromal tumours resistant to both imatinib and sunitinib. Eur J Cancer. 2009;45:2293–7.
Pantaleo MA, Nannini M, Saponara M, Gnocchi C, Di Scioscio V, Lolli C, et al. Impressive long-term disease stabilization by nilotinib in two pretreated patients with KIT/PDGFRA wild-type metastatic gastrointestinal stromal tumours. Anti-Cancer Drugs. 2012;23:567–72.
Mussi C, Ronellenfitsch U, Jakob J, Tamborini E, Reichardt P, Casali PG, et al. Post-imatinib surgery in advanced/metastatic GIST: is it worthwhile in all patients? Ann Oncol. 2010;21:403–8.
Yeh CN, Chen TW, Tseng JH, Liu YY, Wang SY, Tsai CY, et al. Surgical management in gastrointestinal stromal tumor (GIST) patients after imatinib mesylate treatment. J Surg Oncol. 2010;102:599–603.
Hasegawa J, Kanda T, Hirota S, Fukuda M, Nishitani A, Takahashi T, et al. Surgical interventions for focal progression of advanced gastrointestinal stromal tumors during imatinib therapy. Int J Clin Oncol. 2007;12:212–7.
Kinoshita K, Hirota S, Isozaki K, Nishitani A, Tsutsui S, Watabe K, et al. Characterization of tyrosine kinase I domain c-kit gene mutation Asn655Lys newly found in primary jejunal gastrointestinal stromal tumor. Am J Gastroenterol. 2007;102:1134–6.
Funding
This work was supported by JSPS KAKENHI [Grant Number 15K10098].
Authors’ contributions
TS wrote the final manuscript and analyzed the results. TT, TI, HI, and TK participated in the care of the patients. SH carried out the pathological analysis of the specimen including gene analysis. All authors participated in data collection. TT, TI, TK, and SH participated in revising the manuscript critically. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent was obtained from the patient for the publication of this report and any accompanying images.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sugase, T., Takahashi, T., Ishikawa, T. et al. Surgical resection of recurrent gastrointestinal stromal tumor after interruption of long-term nilotinib therapy. surg case rep 2, 137 (2016). https://doi.org/10.1186/s40792-016-0266-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-016-0266-y