
Abstract
Purpose
The purpose of this study was to analyze the dynamic kinematics of the mobile medial pivot-type total knee arthroplasty (MMPTKA) using the three-dimensional (3D)-to-2D registration technique.
Methods
Cadaveric knees from five humans were used. Computed tomography of the lower limb and preoperative 3D planning for MMPTKA were performed. After performing TKA, passive motion of the knee was observed from a fully extended position to maximum flexion using a flat panel detector. The following parameters were determined: (1) anteroposterior (AP) translations of the medial and lateral most distal points (estimated contact point) of the femoral component, (2) rotational femoral component’s X-axis (FCX) angle, and (3) rotational insert angle. Paired t-tests were used to analyze differences in the AP translation between the medial and lateral most distal points of the femoral component as well as differences in the changes in the rotational angle between the FCX and X-axis of the insert on the tibial component’s axial plane.
Results
The AP translations of the femoral component’s medial and lateral most distal points were 8.4 ± 2.5 and 13.6 ± 3.3 mm, respectively (p = 0.001). The rotational angles of the FCX and insert were 10.7° ± 4.9° external rotation and 8.9° ± 4.1° internal rotation, respectively (p = 0.004).
Conclusions
The posterior translation of the lateral side of the femoral component was greater than that of the medial in all cases. Hence, a medial pivot pattern was identified. The femoral component exhibited external rotation throughout knee flexion in all subjects, whereas the mobile insert exhibited internal rotation (opposite pattern relative to the femoral component). This study provides valuable kinematical information of MMPTKA that has not been clear yet.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Total knee arthroplasty (TKA) is the gold standard for treating patients with end-stage knee osteoarthritis (OA), and implants of various designs have been developed to improve clinical outcomes and patient satisfaction. Mobile-bearing-type TKA (MBTKA) was designed in the late 1970s, and the reduction of polyethylene wear and a self-alignment mechanism were expected as a design concept [6, 29, 30]. Several MBTKA kinematic studies have demonstrated that the femoral component is externally rotated relative to the tibial component in the standing position and that the rotation of the femoral component is guided by the rotation of the mobile-bearing insert [7, 10, 11]. In addition, long-term clinical outcomes have been reported using MBTKA, and good long-term follow-up results over more than 15 years have been demonstrated, with 95% survival [16, 21, 28]. Medial pivot-type TKA (MPTKA) utilizes different types of implants that are designed to reproduce the medial pivot motion observed in the normal knee with a highly medially constrained insert [2, 17, 20]. Several studies on MPTKA kinematics and clinical outcomes demonstrated good results with higher sagittal stability and better patient-reported outcomes [9, 12].
In recent years, TKA, which has both a medial pivot mechanism with high medial constraint and a mobile mechanism of insert, has been developed and clinically used. However, previous studies have only described kinematics of up to less than 90° of the knee joint [3, 4] and the dynamic kinematics of this mobile medial pivot-type TKA (MMPTKA) in the deep flexion phase remains unclear. Whether MMPTKA, which employs both MBTKA and MPTKA mechanisms, can demonstrate both advantages at the same time also remains unclear. Thus, this study aimed to analyze the dynamic kinematics of MMPTKA from full extension to the deep flexion phase using the three-dimensional (3D)-to-2D registration technique.
It was hypothesized that the kinematics of MMPTKA differs from that of previously reported MBTKA and MPTKA.
Materials and methods
This cadaveric study was performed according to a protocol approved by the investigational review board of our institution (2017–0156). In this study, five human cadaveric knees from patients who had undergone thigh amputation due to lower leg gangrene without poor soft tissue conditions around the knee including skin, obvious medial and lateral collateral ligament deficiency, and without valgus deformity of the knee were used.
Preoperative planning and TKA
At first, a lower limb computed tomography (CT) scan was obtained for each subject using SOMATOM Sensation 16 (Siemens, Munich, Germany) with a 1-mm interval. Data from the CT scan were used to build a 3D digital model of the bones using the ZedView (LEXI, Tokyo, Japan) visualization and modeling software [23]. Preoperative 3D planning was performed by reading the implant computer-aided design data of Genus MB® (Adler Ortho, Milano, Italy) for all subjects. This implant has both a medial pivot mechanism with high medial constraint and a mobile mechanism of insert. Because the exact mechanical axis of an amputated limb could not be defined, the femoral components were replaced parallel to the surgical epicondylar axis both in the coronal and axial planes during preoperative planning. In the coronal plane, a few degrees of fine-tuning were sometimes performed with reference to the shapes of the femoral posterior condyles. The tibial components were replaced perpendicular to the tibial anatomical axis. Posterior slopes were parallel to the lateral tibial plateau joint surface. Rotational alignments were matched to the line connecting the posterior cruciate ligament insertion and medial border to one-third of the tibial tubercle [1]. All surgeries were performed by a single orthopedic surgeon (OT). TKA was performed using the medial parapatellar approach and the measured resection technique, and attention was paid to maintain the soft tissue balance to avoid medial instability in all ranges of motion. The posterior cruciate ligament was preserved. Regarding the mobile insert, asymmetrically designed inserts (lateral sliding version) were applied with a highly constrained surface on the medial side, and three tantalum markers were embedded into the insert. The wound was closed using 0 monofilament absorbable thread for the joint capsule and 3–0 nylon thread for the skin.
Motion analysis using a single-plane flat panel detector
The amputated limb was fixed to a special device after performing TKA. This special device was designed to apply a constant tensile force to the quadriceps and hamstring muscles via pulleys (Fig. 1). Then, passive motion of the knee was observed from a fully extended position to maximum flexion and recorded using a flat panel detector (AXIOM Artis® dTA; Siemens). Tensile forces of 4 and 2 kg were applied to the quadriceps and hamstring muscles as the bearing load, respectively. The sampling frequency was 15 Hz, with an image area of 380 × 300 mm and a resolution of 1240 × 960 pixels.

Appearance of the experimental special device. The amputated limb that underwent TKA was fixed to it. Tensile forces of 4 and 2 kg were applied to quadriceps and hamstring muscles, respectively, as the bearing load
Evaluation using the 3D-to-2D image registration technique
A series of static lateral images were digitally stored. After manually detecting the femoral and tibial component contours in these images, a 3D-to-2D technique with an automated shape-matching algorithm was employed to determine the relative 3D positions of the femoral and tibial components in each fluoroscopic image (KneeMotion®; LEXI, Tokyo, Japan) (Fig. 2). Relative motion between the femoral and tibial components was determined using this procedure for all images. Similarly, the relative 3D positions of the insert and tibial components in each fluoroscopic image were obtained by matching the tantalum markers of the insert. The root mean square errors were 0.3–0.8 mm for in-plane translation, 2.2 mm for out-of-plane translation, and 0.2°–0.6° for rotation [26, 27]. The anteroposterior (AP) locations of the femoral component’s medial and lateral most distal point (estimated contact point) of all images were evaluated as Y-values of the tibial component’s coordinate system (Fig. 3). Relative motion between the femoral and tibial components was quantified as the movement of the femoral component’s X-axis (FCX) (mediolateral axis) projected onto the axial (XY) plane of the tibial component’s coordinate system (Fig. 4). Relative motion between the insert and tibial component was also quantified as the movement of the insert’s X-axis (mediolateral axis) projected onto the axial (XY) plane of the tibial component’s coordinate system (Fig. 5).

Relative 3D positions of the femoral components and tibial components in each fluoroscopic image were obtained using the 3D-to-2D registration technique. The relative 3D positions of the inserts and tibial components in each fluoroscopic image were obtained using the same method

Anteroposterior (AP) translations of the femoral component’s medial and lateral most distal points (estimated contact point) were evaluated as Y-values of the tibial component’s coordinate system

Changes in the femoral component’s X-axis (FCX) angle on the tibial component’s axial plane (rotational angle). The FCX was projected onto the axial (XY) plane of the tibial component’s coordinate system. The rotational angle from full knee extension to maximum flexion was calculated

Changes in the angle of the insert’s X-axis on the tibial component’s axial plane (rotational angle). The insert’s X-axis was projected onto the axial (XY) plane of the tibial component’s coordinate system. The rotational angle from full knee extension to maximum flexion was calculated
The following parameters were determined: (1) AP translations of the femoral component’s medial and lateral most distal points (estimated contact point), (2) changes in the FCX angle on the tibial component’s axial plane (rotational angle), and (3) changes in the angle of the insert’s X-axis on the tibial component’s axial plane (motion pattern of the insert). AP translation was expressed as the difference between the maximum and minimum values throughout knee flexion. Changes in the FCX angle and the angle of the insert’s X-axis were expressed as the differences between the angles at full knee extension and the angles at maximum knee flexion.
Regarding the reliability of our 3D-to-2D image registration technique, intraobserver and interobserver reliabilities were examined via intra-class correlation coefficient (ICC) in a previous study. The ICCs (1, 2) of the rotational angle of the axis, AP translation of the medial end of the axis, and AP translation of the lateral end of the axis were 0.98, 0.91, and 0.85, respectively. The ICCs (2, 1) of the rotational angle of the axis, AP translation of the medial end of the axis, and AP translation of the lateral end of the axis were 0.92, 0.86, and 0.99, respectively [27].
Statistical analysis
All data are expressed as mean ± standard deviation. Shapiro–Wilk analysis was performed to test for normally distributed variables. Paired t-tests were used to analyze differences in the AP translation between the medial and lateral most distal points of the femoral component as well as differences in the changes in the rotational angle between the FCX and X-axis of the insert on the tibial component’s axial plane. A p-value of < 0.05 was considered statistically significant. Statistical analysis was performed using the Statistical Package for the Social Sciences software (IBM SPSS Statistics, Version 27.0, IBM Corp., Armonk, NY, USA).
Results
AP translations of the femoral component’s most distal points (estimated contact point)
Values in the range of the knee flexion angle (0°–120°) that could be obtained by all subjects were employed for calculations. The femoral component’s medial most distal point showed no marked AP translation until approximately 60° and then showed a gradual posterior translation (mean translation, 8.4 ± 2.5 mm; range, 4.9–11.8 mm posterior). The lateral side also demonstrated no marked AP translation until approximately 60° and then showed a gradual posterior translation (mean translation, 13.6 ± 3.3 mm; range, 9.5–17.7 mm posterior) (Fig. 6). The femoral component showed a bicondylar rollback pattern in which both medial and lateral ends moved posteriorly after 60°. A medial pivot pattern was observed in cases with a certain amount of posterior translation difference between the medial and lateral ends (medial < lateral). The amount of posterior translation of the lateral side was greater than that of the medial side in all cases. The AP translation of the femoral component’s medial most distal point was significantly smaller than that of the lateral point (p = 0.001).

AP translation of the femoral component’s medial and lateral most distal points (estimated contact point) (mean ± SD)
Changes in the FCX angle on the tibial component’s axial plane (rotational angle)
The FCX exhibited external rotation on the axial plane of the tibial component’s coordinate system throughout knee flexion in all subjects, indicating that all subjects demonstrated the internal rotation of the tibial component relative to the femoral component throughout knee flexion. The mean ± standard deviation (SD) rotational angle was 10.7° ± 4.9° external rotation (range, 5.4°–16.4° external rotation) (Table 1). The FCX angles in the knee flexion angle range (0°–120°) that could be obtained for all subjects are shown in Fig. 7.

Rotational angle of the FCX and insert’s X-axis (mean ± SD). ER: external rotation, IR: internal rotation
Changes in the angle of the insert’s X-axis on the tibial component’s axial plane (motion pattern of the insert)
The mobile insert exhibited internal rotation on the axial plane of the tibial component’s coordinate system throughout knee flexion in all subjects, indicating that all subjects demonstrated opposite patterns relative to the femoral component. In three of the five cases, the lateral side of the inserts exhibited an anterior overhang in the deep flexion phase. The mean ± SD rotational angle was 8.9° ± 4.1° internal rotation (range, 2.0°–12.0° internal rotation) (Table 1). Changes in the angle of the insert’s X-axis were significantly more internally rotated than those of the femoral component’s axis (p = 0.004). The angles of the insert’s X-axis in the knee flexion angle range (0°–120°) that could be obtained for all subjects are shown in Fig. 7.
Discussion
The important findings of the present study were that the amount of posterior translation of the lateral side of the femoral component was greater than that of the medial side in all cases. Hence, a medial pivot pattern was identified. Moreover, the femoral component exhibited external rotation throughout knee flexion in all subjects, whereas the mobile insert exhibited internal rotation (opposite pattern relative to the femoral component).
Regarding the AP translations of the femoral component in our study, no marked AP translation was observed until approximately 60°, and a gradual posterior translation was observed after 60° in the medial and lateral most distal points. A posterior translation of 8.4 mm was detected in the medial most distal point, whereas a posterior translation of 13.6 mm was detected in the lateral most distal point. A previous in vivo tibiofemoral kinematic analysis of TKA with a ball and socket joint geometry at the medial side showed similar results; this study showed less AP translation on the medial side (1.2 mm posteriorly) compared with that on the lateral side (7.3 mm posteriorly) using a 3D-to-2D image matching technique [18]. On the other hand, medial paradoxical anterior translation has been reported in posterior-stabilized (PS) and cruciate-retaining (CR) TKAs with low conformity surface [5, 8, 14]. A recent study demonstrated that paradoxical anterior translation can be reduced by increasing medial conformity of the bearing insert in PS TKA [13]. These studies combined with the results of the present study indicate that high medial conformity may contribute to the suppression of paradoxical anterior translation.
Regarding the rotation of the femoral component, a medial pivot pattern was observed in cases with a certain amount of difference in the posterior translation between the medial and lateral sides (medial < lateral). Some studies reported that TKA with highly medially constrained inserts showed a medial pivot motion [18,19,20]. Omori et al. evaluated the tibiofemoral contact kinematics of TKA with a ball and socket joint geometry at the medial side using a cadaveric knee and showed medial pivot motion [20]. Miyazaki et al. conducted in vivo tibiofemoral kinematic analysis of TKA with a ball and socket joint geometry at the medial side using a 3D-to-2D image matching technique and showed medial pivot motion [18]. Meanwhile, some studies reported that MBTKA with a flat surface insert does not show medial pivot motion [15, 31]. These results suggest that the highly constrained surface shape of the medial side of the insert is significantly related to medial pivot motion.
Regarding the rotation of the insert, some studies reported that the femoral component and insert showed the same rotation in the motion analysis of TKA with a mobile-bearing mechanism in the motion pattern of the insert [10, 33]. Futai et al. performed an in vivo kinematic analysis of MBTKA during deep-knee bending under weight-bearing conditions and showed that the amounts of external rotation of the femoral component relative to the tibial component and insert relative to the tibial component were 10.4° and 10.2°, respectively, for 0°–120° of flexion. On average, the femoral component showed slight rotation relative to the insert [10]. Yamazaki et al. also conducted an in vivo kinematic analysis of MBTKA and revealed that the femoral component rotated externally with respect to the tibial component during flexion, with an average external rotation range of 12.4°. Similarly, the mobile-bearing insert rotated externally with respect to the tibial component during flexion, with an average rotation range of 11.5°. The axial rotations of the femoral component and mobile-bearing insert with respect to the tibial component were also similar, showing no significant difference. The movement for axial rotation of the femoral component with respect to the mobile-bearing insert exhibited little rotation [33]. The mobile-bearing inserts utilized in these studies had a symmetrical medial and lateral surface. Meanwhile, motion analysis of TKA was performed in this study using mobile-bearing inserts with high medial constraint and asymmetrical medial and lateral surfaces. As a result, the femoral component and mobile-bearing insert showed opposite rotation during knee flexion.
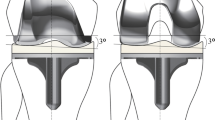
In normal knees, the amount of AP translation of the femoral condyle is lower on the medial side than that on the lateral side, and the femur exhibits external rotation relative to the tibia (medial pivot motion) and subsequent bicondylar rollback in the late flexion phase [26, 27]. Based on the superior patient-reported outcome measures for MPTKA, reproducing native kinematics is an important factor in improving patient satisfaction [9, 12, 22]. In this study, MMPTKA exhibited medial pivot motion. Moreover, the medial side of the femoral component moved posteriorly with the insert in the late flexion phase due to high conformity only on the medial side, whereas the less constrained lateral side of the femoral component moved posteriorly without being constrained by the anterior movement of the insert (Fig. 8). Thus, femoral components exhibited bicondylar rollback motion in the late flexion phase. In other words, the kinematics between the femoral component and tibial component were ideal and in line with the design concept.

Motion patterns of the femoral component and insert are shown. The femoral component exhibited external rotation throughout knee flexion. Meanwhile, the mobile insert exhibited internal rotation throughout knee flexion. These kinematics were due to the high conformity only on the medial side and less on the lateral side
All inserts in this study showed internal rotation throughout knee flexion. However, the rotational angles differed from each other. This may be due to the differences in soft-tissue tightness and component position. In addition, the lateral side of the inserts showed an overhang in the deep flexion phase, and the effect of this phenomenon remains a clinical concern. Kinematic changes in the mobile-bearing insert over time in patients are also unclear. The rotation of the mobile-bearing insert has been reported to decrease over time [32]. However, other studies have reported that the rotation of the mobile-bearing insert is maintained over time [7, 34]. Kinematic changes in the mobile-bearing insert may require further investigation, especially with the effects of soft tissue balance on in vivo motion, although these components have already been clinically used in Europe and Japan and no major complications related to the inserts in the short- and mid-term have been detected.
This study had several limitations. First, this cadaveric study had a small sample size. Although the same trends were observed in all five samples, it is better to include a larger sample size. Second, quantitative evaluations of soft tissue balancing and postoperative component positions were difficult. Therefore, in vivo studies that allow these evaluations are desirable in the future.
Regarding clinical relevance, the results of this study provide valuable kinematic information about MMPTKA that has not been clear yet and may be used as a reference for in vivo motion analyses.
Conclusions
The posterior translation of the lateral side of the femoral component was greater than that of the medial side in all cases. Hence, a medial pivot pattern was identified. The femoral component exhibited external rotation throughout knee flexion in all subjects, whereas the mobile insert exhibited internal rotation (opposite pattern relative to the femoral component). This study provides valuable kinematic information on MMPTKA that has not been clear yet.
Availability of data and materials
The datasets analyzed in this study are available from the corresponding author on reasonable request.
Abbreviations
- TKA:
-
Total knee arthroplasty
- OA:
-
Osteoarthritis
- MBTKA:
-
Mobile-bearing-type TKA
- MPTKA:
-
Medial pivot-type TKA
- MMPTKA:
-
Mobile medial pivot-type TKA
- 3D:
-
Three-dimensional
- CT:
-
Computed tomography
- AP:
-
Anteroposterior
- FCX:
-
Femoral component’s X-axis
- ICC:
-
Intra-class correlation coefficient
- SD:
-
Standard deviation
References
Akagi M, Oh M, Nonaka T, Tsujimoto H, Asano T, Hamanishi C (2004) An anteroposterior axis of the tibia for total knee arthroplasty. Clin Orthop Relat Res 420:213–219
Barnes CL, Blaha JD, DeBoer D, Stemniski P, Obert R, Carroll M (2012) Assessment of a medial pivot total knee arthroplasty design in a cadaveric knee extension test model. J Arthroplasty 27(8):1460–1468
Castellarin G, Bori E, Innocenti B (2020) Experimental and clinical analysis of the use of asymmetric vs symmetric polyethylene inserts in a mobile bearing total knee arthroplasty. J Orthop 23:25–30
Castellarin G, Pianigiani S, Innocenti B (2019) Asymmetric polyethylene inserts promote favorable kinematics and better clinical outcome compared to symmetric inserts in a mobile bearing total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 27(4):1096–1105
Cates HE, Komistek RD, Mahfouz MR, Schmidt MA, Anderle M (2008) In vivo comparison of knee kinematics for subjects having either a posterior stabilized or cruciate retaining high-flexion total knee arthroplasty. J Arthroplasty 23(7):1057–1067
Dennis DA, Komistek RD (2006) Mobile-bearing total knee arthroplasty: design factors in minimizing wear. Clin Orthop Relat Res 2006452:70–77
Dennis DA, Komistek RD, Mahfouz MR, Outten JT, Sharma A (2005) Mobile-bearing total knee arthroplasty: do the polyethylene bearings rotate? Clin Orthop Relat Res 440:88–95
Donadio J, Pelissier A, Boyer P, Massin P (2015) Control of paradoxical kinematics in posterior cruciate-retaining total knee arthroplasty by increasing posterior femoral offset. Knee Surg Sports Traumatol Arthrosc 23(6):1631–1637
Edelstein AI, Bhatt S, Wright-Chisem J, Sullivan R, Beal M, Manning DW (2020) The effect of implant design on sagittal plane stability: a randomized trial of medial- versus posterior-stabilized total knee arthroplasty. J Knee Surg 33(5):452–458
Futai K, Tomita T, Yamazaki T, Tamaki M, Yoshikawa H, Sugamoto K (2011) In vivo kinematics of mobile-bearing total knee arthroplasty during deep knee bending under weight-bearing conditions. Knee Surg Sports Traumatol Arthrosc 19(6):914–920
Hoshi K, Watanabe G, Kurose Y, Tanaka R, Fujii J, Gamada K (2020) Mobile-bearing insert used with total knee arthroplasty does not rotate on the tibial tray during a squatting activity: a cross-sectional study. J Orthop Surg Res 15(1):114
Jones CW, Jacobs H, Shumborski S, Talbot S, Redgment A, Brighton R, Walter WL (2020) Sagittal stability and implant design affect patient reported outcomes after total knee arthroplasty. J Arthroplasty 35(3):747–751
Khasian M, Meccia BA, LaCour MT, Komistek RD (2021) Effects of the medial plateau bearing insert conformity on mid-flexion paradoxical motion in a posterior-stabilized total knee arthroplasty design. J Arthroplasty 36(7):2386–2392
Khasian M, Sharma A, Fehring TK, Griffin WL, Mason JB, Komistek RD (2020) Kinematic performance of gradually variable radius posterior-stabilized primary TKA during various activities: an in vivo study using fluoroscopy. J Arthroplasty 35(4):1101–1108
Matsumoto K, Iwamoto K, Mori N, Yamasaki T, Ito Y, Takigami I, Terabayashi N, Ogawa H, Tomita T, Akiyama H (2014) In vivo kinematics of a low contact stress rotating platform total knee arthroplasty system under weight bearing and non-weight bearing condition. J Orthop Sci 19(5):750–755
Milligan DJ, O’Brien S, Doran E, Gallagher NE, Beverland DE (2019) Twenty-year survivorship of a cemented mobile bearing total knee arthroplasty. Knee 26(4):933–940
Miura K, Ohkoshi Y, Ino T, Ukishiro K, Kawakami K, Suzuki S, Suzuki K, Maeda T (2020) Kinematics and center of axial rotation during walking after medial pivot type total knee arthroplasty. J Exp Orthop 7(1):72
Miyazaki Y, Nakamura T, Kogame K, Saito M, Yamamoto K, Suguro T (2011) Analysis of the kinematics of total knee prostheses with a medial pivot design. J Arthroplasty 26(7):1038–1044
Moonot P, Mu S, Railton GT, Field RE, Banks SA (2009) Tibiofemoral kinematic analysis of knee flexion for a medial pivot knee. Knee Surg Sports Traumatol Arthrosc 17(8):927–934
Omori G, Onda N, Shimura M, Hayashi T, Sato T, Koga Y (2009) The effect of geometry of the tibial polyethylene insert on the tibiofemoral contact kinematics in advance medial pivot total knee arthroplasty. J Orthop Sci 14(6):754–760
Rassir R, Puijk R, Singh J, Sierevelt IN, Vergroesen DA, de Jong T, Nolte PA (2022) Long-term clinical performance of an uncemented, mobile bearing, anterior stabilized knee system and the impact of previous knee surgery. J Arthroplasty 37(10):2041–2048
Samy DA, Wolfstadt JI, Vaidee I, Backstein DJ (2018) A retrospective comparison of a medial pivot and posterior-stabilized total knee arthroplasty with respect to patient-reported and radiographic outcomes. J Arthroplasty 33(5):1379–1383
Sato T, Koga Y, Omori G (2004) Three-dimensional lower extremity alignment assessment system: application to evaluation of component position after total knee arthroplasty. J Arthroplasty 19(5):620–628
Solarino G, Spinarelli A, Carrozzo M, Piazzolla A, Vicenti G, Moretti B (2014) Long-term outcome of low contact stress total knee arthroplasty with different mobile bearing designs. Joints 2(3):109–114
Sugita T, Sato K, Komistek RD, Mahfouz MR, Maeda I, Sano T (2005) In vivo determination of knee kinematics for Japanese subjects having either a low contact stress rotating platform or an anteroposterior glide total knee arthroplasty. J Arthroplasty 20(2):154–161
Tanifuji O, Sato T, Kobayashi K, Mochizuki T, Koga Y, Yamagiwa H, Omori G, Endo N (2011) Three-dimensional in-vivo motion analysis of normal knees using single-plane fluoroscopy. J Orthop Sci 16(6):710–718
Tanifuji O, Sato T, Kobayashi K, Mochizuki T, Koga Y, Yamagiwa H, Omori G, Endo N (2013) Three-dimensional in-vivo motion analysis of normal knees employing transept axis as an evaluation parameter. Knee Surg Sports Traumatol Arthrosc 21(10):2301–2308
van Ooij B, de Keijzer DR, Hoornenborg D, Sierevelt IN, Haverkamp D (2022) Lower revision rates for cemented fixation in a long-term survival analysis of three different LCS designs. Knee Surg Sports Traumatol Arthrosc 30(8):2707–2713
Vertullo CJ, Easley ME, Scott WN, Insall JN (2001) Mobile bearings in primary knee arthroplasty. J Am Acad Orthop Surg 9(6):355–364
Walker PS, Komistek RD, Barrett DS, Anderson D, Dennis DA, Sampson M (2002) Motion of a mobile bearing knee allowing translation and rotation. J Arthroplasty 17(1):11–19
Wasielewski RC, Komistek RD, Zingde SM, Sheridan KC, Mahfouz MR (2008) Lack of axial rotation in mobile-bearing knee designs. Clin Orthop Relat Res 466(11):2662–2668
Wolterbeek N, Garling EH, Mertens B, Valstar ER, Nelissen RG (2009) Mobile bearing knee kinematics change over time. A fluoroscopic study in rheumatoid arthritis patients. Clin Biomech (Bristol, Avon) 24(5):441–445
Yamazaki T, Futai K, Tomita T, Sato Y, Yoshikawa H, Tamura S, Sugamoto K (2015) 3D kinematics of mobile-bearing total knee arthroplasty using X-ray fluoroscopy. Int J Comput Assist Radiol Surg 10(4):487–495
Zürcher A, van Hutten K, Harlaar J, Pöll R (2017) Mobility of the rotating platform in low contact stress knee arthroplasty is durable. Knee Surg Sports Traumatol Arthrosc 25(8):2580–2585
Acknowledgements
The authors would like to thank the entire staff of the Department of Radiology of Niigata University Medical and Dental Hospital for their technical support and cooperation.
Funding
The authors declare that they have no funding.
Author information
Authors and Affiliations
Contributions
Conception and design: Dr. OT. Collection of data and analysis: Drs. OT, TM. Interpretation of the data: Drs. OT, TM, TS, SW, GO, HK. Drafting of the article: Dr. OT. Final approval of the article: Drs. OT, TM, TS, SW, GO, HK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed according to a protocol approved by the Investigational Review Boards of our institution (Niigata University, 2017–0156).
All subjects were provided informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tanifuji, O., Mochizuki, T., Sato, T. et al. Mobile medial pivot (lateral slide) type total knee arthroplasty exhibits a medial pivot pattern: three-dimensional motion analysis using cadaveric knees. J EXP ORTOP 9, 122 (2022). https://doi.org/10.1186/s40634-022-00558-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-022-00558-9