
Abstract
Dementia with Lewy bodies (DLB), Parkinson’s disease dementia (PDD), and Parkinson’s disease (PD) collectively known as Lewy body diseases (LBDs) are neuropathologically characterised by α-synuclein deposits (Lewy bodies and Lewy neurites). However, LBDs also exhibit pathology associated with Alzheimer’s disease (AD) (i.e. hyperphosphorylated tau and amyloid β (Aβ). Aβ can be deposited in the walls of blood vessels in the brains of individuals with AD, termed cerebral amyloid angiopathy (CAA). The aim of this study was to investigate the type and distribution of CAA in DLB, PDD, and PD and determine if this differs from AD. CAA type, severity, and topographical distribution was assessed in 94 AD, 30 DLB, 17 PDD, and 11 PD cases, and APOE genotype evaluated in a subset of cases where available. 96.3% AD cases, 70% DLB cases and 82.4% PDD cases exhibited CAA (type 1 or type 2). However only 45.5% PD cases had CAA. Type 1 CAA accounted for 37.2% of AD cases, 10% of DLB cases, and 5.9% of PDD cases, and was not observed in PD cases. There was a hierarchical topographical distribution in regions affected by CAA where AD and DLB displayed the same distribution pattern that differed from PDD and PD. APOE ε4 was associated with severity of CAA in AD cases. Topographical patterns and severity of CAA in DLB more closely resembled AD rather than PDD, and as type 1 CAA is associated with clinical dementia in AD, further investigations are warranted into whether the increased presence of type 1 CAA in DLB compared to PDD are related to the onset of cognitive symptoms and is a distinguishing factor between LBDs. Possible alignment of the the topographical distribution of CAA and microbleeds in DLB warrants further investigation. CAA in DLB more closely resembles AD rather than PDD or PD, and should be taken into consideration when stratifying patients for clinical trials or designing disease modifying therapies.
Similar content being viewed by others

Introduction
Neurodegenerative diseases of the ageing brain are defined neuropathologically by their most prevalent pathology, using internationally recognised staging criteria. However, it is rare that pathologies exist in isolation, with pure pathology only seen in 22.7% of post-mortem cases in a large neuropathological study consisting of 670 brains [40]. Although low/intermediate or indeed severe/high levels of concomitant pathology are present across numerous diseases, they are particularly evident across Lewy body diseases (LBDs) including dementia with Lewy bodies, Parkinson’s disease (PD), and Parkinson’s disease dementia (PDD), where in addition to hallmark inclusions of α-synuclein, concomitant AD related pathology (intracellular tau-immunoreactive neurofibrillary tangles and extracellular amyloid β (Aβ) plaques) is a prominent feature [17, 35, 39, 61, 62].
Cerebral amyloid angiopathy (CAA), observed in 20–100% of AD cases [20, 32, 38, 48], is defined by the deposition of Aβ (predominantly Aβ1-40) in the walls of meningeal vessels, cerebral arteries, arterioles, and less commonly in the capillaries and vein vessel walls [28, 49, 67]. It exists in two forms, the first (type 1 CAA) affects the capillaries, with or with-out involvement of cortical or leptomeningeal vessels, the second (type 2 CAA) includes Aβ deposition restricted to leptomeningeal and cortical arteries, arterioles, and rarely veins without capillary involvement [54].
The association of CAA with clinical dementia has been investigated, 87.5% of individuals with dementia have CAA, whilst only 55.6% of cognitively normally individuals exhibit CAA at post-mortem examination [4]. CAA has also been identified as a contributor to cognitive decline independent of other AD related neuropathology [7, 56]. Furthermore, type 1 CAA was found to mildly correlate with clinical dementia and AD neuropathology, whereas type 2 CAA did not [4].
Although a frequent observation in AD at post-mortem examination, CAA has also been reported in LBDs with recent studies reporting between 91 and 100% of DLB cases, 50–63% of PDD cases, and 13% of PD cases displaying CAA pathology [25, 29]. The increased presence of type 1 CAA has also been reported in LBD cases with dementia as demonstrated by a series of 88 cases including PD, PDD and DLB cases. Whilst only 25% of PD cases exhibited type 1 CAA, DLB and PDD cases exhibited higher rates of type 1 CAA deposition (90% and 85% of cases respectively) [30].
Studies suggest that neurodegenerative pathologies spread in a predictable stereotypical manner i.e. tau pathology originates in the entorhinal cortex and progresses to the neocortex [1, 8] and Aβ starts in the neocortex and advances through the limbic system and brainstem to the cerebellum [55]. α-synuclein originates in the brainstem, progresses through the limbic regions and to the neocortex in PD/PDD [9, 42], with a limbic -predominant profile being more associated with cognitive decline in DLB [58]. However, in the presence of multiple pathologies typical topographical patterns of distribution may be altered. Lewy related pathology in DLB cases with significant concomitant AD related pathology shows a different distribution to DLB cases with minimal AD related pathology, and both groups differ from PD cases [58, 61]. With respect to CAA in AD, the occipital cortex is the most commonly and severely affected brain region in AD, with frontal, parietal, and temporal lobes less affected [3, 59, 64]. However, distribution patterns of CAA have yet to be investigated in LBDs, and as DLB cases can exhibit a greater Aβ burden compared to PDD and PD cases [18, 24, 31] whether LBDs have a similar distribution of CAA is currently unknown.
Therefore, the aim of this study was to investigate differences in type, topographical distribution of CAA, and association with dementia, across the spectrum of LBDs and determine if this differs from AD cases.
Materials and methods
Study cohort
Brain tissue from 152 donors (mean age 81.39 ± 9.6 years; male: 89, female: 63) was used in this study. 94 cases fulfilled neuropathological criteria for high AD neuropathologic change according to NIA‐AA criteria [45] inclusive of Braak stage [8], Thal phase [55] and CERAD score [44], and clinically diagnosed with AD [43]. 47 cases had limbic/neocortical Lewy body disease [42] (30 clinically diagnosed as dementia with Lewy bodies (DLB) and 17 with Parkinson’s disease dementia), and 11 diagnosed with Parkinson’s disease [42]. Cases that fulfilled neuropathological criteria for mixed AD/DLB (i.e. DLB with high AD neuropathologic change) were excluded from the study. Patient demographics including neuropathological characteristics are shown in Table 1. There was no significant difference in age at death between any of the groups (p = 0.067). There was no difference between sex in the AD group (p = 0.83) or PDD group (p = 0.71), however there was significantly more males than females in the DLB and PD groups (DLB p = 0.003; PD p = 0.035). Clinical records were systematically reviewed by a board-certified Old Age Psychiatrist (AJT). Brain tissue was obtained at autopsy and stored within the Newcastle Brain Tissue Resource (NBTR) in accordance with Newcastle University Ethics Board (The Joint Ethics Committee of Newcastle and North Tyneside Health Authority, reference: 08/H0906/136). After autopsy the right hemisphere, brainstem and cerebellum were immersion fixed in 4% buffered aqueous formaldehyde solution for 6 weeks. Irrespective of clinical diagnoses, all brains underwent neuropathological assessment and were stratified by clinico-pathological consensus. APOE genotype was provided by the Newcastle Brain Tissue Resource.
Immunohistochemistry
Paraffin embedded blocks taken from the frontal (Brodmann area (BA) 9), temporal (BA 21/22), parietal (BA 40), and occipital (BA17/18) cortices were cut at 6 μm and airdried onto superfrost plus charged glass slides (Thermo Shandon, Cheshire, UK). Tissue sections then underwent immunohistochemical staining for Aβ (4G8, dilution 1:15,000, Signet Labs, Dedham, MA, USA) for the detection of Aβ deposits in vessels (CAA) and extracellular Aβ plaques. Prior to immunostaining antigen retrieval was performed by immersing slides for 1 h in 100% formic acid. Immunopositivity was detected using a MENAPATH HRP polymer detection kit (Menarini diagnostics, Berkshire, UK) with 3,3 diaminobezidine (DAB) as a chromagen and haematoxylin as counter stain. Tissue was subsequently dehydrated through a series of alcohols, cleared and mounted using DPX (CellPath, Powys, UK).
Neuropathological scoring
Each case (inclusive of frontal, temporal, parietal, and occipital lobes) was assessed for type and severity of CAA according to standardised neuropathological staging criteria described previously by Thal [54], Olichney [47] and the consensus prototcol for the assessment of CAA [36]. The agreed protocol in the consensus scores parenchymal and meningeal CAA on a 0–4 scale and capillary CAA as present/absent in the 4 cortical lobes. The semi-quantitative scoring for parenchymal and meningeal CAA was recorded as follows: 0, no Aβ present in vessel walls; 1, scant Aβ deposition; 2, some circumferential Aβ deposits; 3, widespread, circumferential Aβ positivity; 4, as for 3 with additional dyshoric changes (Fig. 1). Inter-rater reliability for CAA is high [36]. However, we are not aware of studies on the intra-rater reliability for Olichney scoring, but there will probably be some degree of intra-rater inconsistency similar to the majority of other semi-quantitative scoring methods. To calculate the overall cortical CAA score, semi-quantitative scores for each brain region (frontal, temporal, parietal, and occipital) were combined [5].

Photo micrographs demonstrating the types and semi-quantitative scoring of cerebral amyloid angiopathy (CAA). a Cortical CAA, b leptomeningeal CAA, and c capillary CAA. For this study the Olichney scoring system (41) was used and comprises of 4 grades d Olichney 1 A trace to scattered positivity in leptomeningeal or cortical vessels, e Olichney 2 —some cortical or leptomeningeal vessels circumferentially affected, f Olichney 3 A widespread circumferential CAA, and g Olichney 4— widespread circumferential CAA, with dyshoric changes surrounding the vessel. Scale bar represents 200 μm
Statistical analysis
The Statistical Package for Social Sciences software (SPSS ver. 26) was used for statistical evaluation. Variables were tested for normality using the Shapiro-Wilk test and visual inspection of variable histograms. Group effects were assessed using either non-parametric (Mann-Whitney U) or parametric (independent samples t-test) procedures. Chi-squared tests or Fisher’s exact test were used to assess differences in categorical variables. A p value of < 0.05 was considered significant.
Results
Presence of CAA and differences in CAA type
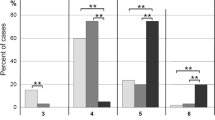
96.3% AD cases, 70% DLB cases and 82.4% PDD cases exhibited CAA (Type 1 or Type 2). However only 45.5% PD cases had any type of CAA. There was no difference in the number of PD cases that had CAA compared to those without CAA (p > 0.05) (Fig. 2). The most frequent type of CAA across all disease groups was type 2 CAA, with AD (p < 0.05), DLB and PDD (both p < 0.01) exhibiting significantly more type 2 CAA compared to type 1 CAA. Those neuropathologically categorised as type 1 CAA accounted for 37.2% of AD cases, 10% of DLB cases, and 5.9% of PDD cases. Within our cohort, type 1 CAA was not observed in any PD cases (Fig. 3).

Significantly more AD, DLB, PDD and PD cases had CAA (type 1 or type 2) compared to to those without. There were no differences in the number of PD cases with and without CAA. *p < 0.05 **p < 0.01 ***p < 0.001. Chi-square test used. Abbreviations: AD; Alzheimer’s disease, DLB; dementia with Lewy bodies, PDD; Parkinson’s disease dementia, PD; Parkinson’s disease

Prevalence of CAA subtype across each disease group. Abbreviations: AD, Alzheimer’s disease; DLB, dementia with Lewy bodies; PDD, Parkinson’s disease dementia; PD, Parkinson’s disease. Black bars represent cases with no CAA, gray bars represent cases with type 1 CAA, and white bars represent cases with type 2 CAA. *p < 0.05 **p < 0.01 ***p < 0.001 using chi-square test
Severity of CAA scores across disease groups
Further analysis investigated the severity of CAA in cortical and meningeal vessles, (this was not available for capillary CAA as criteria only stipulate presence or absence). Cases in both AD and DLB groups exhibited the highest CAA score Olichney 4 (widespread, circumferential Aβ positivity in both leptomeningeal and intercortical vessels with dyshoric changes), whilst no cases in the PDD or PD groups exceeded an Olichney score of 3 (Fig. 4). When assessing the overall cortical CAA score, AD was significantly higher than DLB (p < 0.001) and PD (p < 0.001). There were no differences between any other groups (Fig. 5). When looking at severity scores for cortical and meningeal CAA across individual brain regions AD cases had significantly increased CAA scores compared to DLB, PDD, and PD in all regions assessed (for breakdown of individual regions see Table 2). With respect to differences between the LBD groups, meningeal CAA was significantly increased in DLB compared to PD in the frontal cortex (p < 0.05), whilst in the occipital cortex both meningeal and cortical CAA was increased in PDD compared to PD (both p < 0.05).

Severity CAA scores in cases classified with type 2 CAA across disease categories. Both AD (a) and DLB (b) groups contained cases that reached the highest grading of CAA (Olichney 4), however this most severe score was not given to any case in the PDD (c) or PD (d) groups. Abbreviations: AD; Alzheimer’s disease, DLB; dementia with Lewy bodies, PDD; Parkinson’s disease dementia, PD; Parkinson’s disease

Overall mean cumulative cortical CAA scores across different groups. AD had a significantly higher mean cumulative CAA score compared to DLB (***p < 0.001), PDD (**p < 0.01), and PDD (***p < 0.001) using chi-square tests. There were no differences between any other groups
Distribution patterns of CAA between brain regions
The most commonly affected brain region across all diseases was the occipital lobe. Interestingly, the pattern of distribution was similar between AD and DLB cases with the frontal cortex being the next most commonly affected followed by the parietal and lastly the temporal cortex. This differs from the distribution pattern of CAA in PDD and PD where although the occipital cortex is the most commonly affected region the frontal cortex is the one of the least affected regions (Fig. 6).

a Scatter graph demonstrating differences in topographical distribution across the difference disease groups. Occipital lobe was affected most across all diseases, with AD and DLB groups following the same hierarchical order occipital > frontal > parietal > temporal. This differed from PDD and PD groups where frontal cortex was one of the least affected brain regions. b visual representation of graphical data
APOE genotype
APOE status was available in 96 cases (62 AD, 20 DLB, 10 PDD, and 4 PD). The most frequent genotype in AD was ε3/4 (59.7%), however in LBDs the most frequent genotype was ε3/3 (DLB 60%, PDD 70%, and PD 50%) Table 3, and CAA severity scores for each genotype is presented in Fig. 7. In the whole cohort the presence of an APOE ε4 allele was associated with CAA severity (p < 0.05), however no association was observed between CAA severity and the presence an APOE ε2 or APOE ε3 alleles. When considering individual disease groups the association between CAA severity and the presence of an APOE ε4 allele, this only remained significant in the AD group (p < 0.05). The presence of the ε4 allele was also associated with the presence of type 1 CAA (p < 0.05) in the overall cohort. No other associations were observed between APOE status and type 1 CAA.

In LBD cohort (DLB, PDD, and PD combined) the genotypes with the highest mean Olichney scores were E2/E3 and E2/E4
Effects of severe CAA on brain parenchyma
We next investigated if ischemic and haemorrhagic lesions were present in AD and DLB cases with severe CAA. Vascular pathology was present in 13/49 AD cases and 0/4 DLB cases. Both infarcts and microhaemorrhages were present in the AD cases with severe CAA (Additional file 1: Table S1, online resource).
Discussion
Mixed pathologies, in particular AD related pathology is a frequent finding in LBDs, and data from this study adds to growing evidence to suggest CAA may be a contributing pathological substrate in LBDs, in particular in DLB. Building on previous studies that have demonstrated differences in the prevalence of CAA in DLB compared to PDD [25, 29, 30], here we report differences in the severity and the topographical distribution of CAA across the LBD spectrum.
In our study we found CAA is more common in cases with clinical dementia, as significantly more AD, DLB, and PDD cases had CAA, and there was no difference in the number of PD cases with and without CAA. This is in agreement with other studies, as evidence from a longitudinal study using data from 1100 well characterised older adults suggests that CAA is associated with faster rates of decline in global cognition, perceptual speed, and episodic and semantic memory over a 19 year period [7]. Furthermore, both large population and community-based studies have reported individuals with moderate to severe CAA perform worse on cognitive tasks [2, 10]. The disease groups with the highest CAA scores (Olichney grade 4) in our study are AD and DLB, with none of the PD or PDD groups (which originally start out as motor disorders, and potentially progressing to dementia) exhibiting the highest CAA score available. When considering the LBD cases only this finding is in alignment with a study by Jellinger where only DLB cases exhibited the highest CAA score, with neither PD or PDD cases displaying the highest severity level [29]. In the current study the cumulative cortical CAA scores were significantly higher in AD compared to DLB and PD, and there was no difference observed between AD and PDD. However, in the PDD group there was one case that exhibited severe CAA in all cortical regions which could be driving this. Type 1 CAA is more common in DLB cases compared to PDD, which is interesting given the association between type 1 CAA and cognitive decline [7, 56], and not present at all in our PD cohort. The relationship between type 1 CAA, AD related pathology and dementia has been reported in a population-based study using the Vantaa 85 + cohort, where the authors found type 1 CAA was associated with severity of generalised CAA and the presence of dementia [37]. Furthermore, in agreement with a previous neuropathological study DLB and PDD cases are more likely to have type 1 CAA compared to PD without dementia [30]. Although it is difficult to neuropathologically distinguish DLB from PDD, DLB cases have been shown to exhibit increased AD related pathology compared to PDD cases [31, 62]. Therefore to investigate if the differences in CAA severity between DLB and PDD are evident in the absence of abundant amyloid plaques in the parenchyma, this study was designed to exclude all LBD cases with high AD neuropathologic change. There were no differences in Thal phase, Braak neurofibrillary tangle stage or CERAD score between DLB and PDD groups, which is also in agreement with a study by Hansen and colleagues. They found no difference in Thal phases between DLB and PDD groups, however CAA in DLB was more severe compared to PDD [25]. The relationship between parenchymal amyloid load and CAA severity has been investigated in AD [57]. No association was observed between amyloid plaque load and CAA severity in individual brain regions, and it is speculated that differing pathogenic mechanisms underpin the deposition of amyloid in plaques and blood vessels. This is not surprising considering the predominant amyloid species in plaques are mostly peptides that are 42 amino acids in length whilst amyloid deposits in CAA mainly comprise of shorter peptides of 40 amino acids.
In the current study the topographical pattern of distribution of generalised CAA in DLB is similar to AD, and this differs from the distribution pattern observed in both PD and PDD. The most commonly affected brain region across all diseases was the occipital cortex. We did not look at differences in specific Brodmann areas in the occipital cortex i.e. Brodmann areas 17 and 18, as unlike tau pathology in Braak neurofibrillary tangle staging, where this delineates Braak stages V/VI, there is no protocol for this when assessing amyloid pathology. In AD and DLB the next most commonly affected brain region is frontal cortex whilst this is the least affected brain region in PD and PDD cases. Interestingly other reports have described concomitant pathology altering the topographical distribution of pathological protein aggregates in patients with multiple pathologies. Toledo and colleagues describe different clusters patterns of pathology in patients with clinical dementia and AD and Lewy related pathology compared to PD patients without AD related pathology [58], whilst a study from our group demonstrated the spread of hyperphosphorylated tau pathology in cases with mixed AD/DLB differs to that in ‘pure ADs [61]. It has been suggested that multiple pathologies promote suitable conditions for a synergistic relationship between proteins that results in cross seeding and exacerbation of overall pathology burden and accelerating cognitive decline [6, 13, 14, 21, 27]. To our knowledge this is the first study demonstrating divergence of pathology patterns in cerebral amyloid deposition in LBDs, and could, in part, be a product of increased synergistic relationships between cortical pathologies in DLB. From a clinical perspective the finding of significant involvement of CAA in the frontal cortex of patients with AD and DLB (predominantly cognitive neurodegenerative diseases) compared to patients with PD or PD (primarily diagnosed as motor disorders) is interesting. Two previous studies have suggested the presence of CAA is associated with impairments to executive function which is controlled by the frontal cortex [12, 63]. This raises questions regarding the potential contribution of CAA to specific cognitive domains in neurodegenerative diseases.
One of the strongest genetic risk factors for increased CAA scores in AD is APOE ε4, [15, 26, 52, 66]. This has also been studied in LBD cases, as APOE ε4/4 and ε2/4 genotypes exhibit the highest general CAA scores [25]. In the current study LBD cases with ε4/4 and ε2/4 genotypes did all exhibit CAA, although this was only a small number of cases (n = 3). Although it is worth noting that we did not include LBD cases with high AD neuropathologic change (that would be neuropathologically classified as mixed DLB/AD) to avoid a masking affect from abundant amyloid β pathology. Previous studies have discussed the masking effect of abundant amyloid pathology on an association between APOE ε2 and CAA severity [66], and it has been suggested that whilst APOE ε4 promotes vascular amyloid deposition, ε2 promotes progression to severe CAA and associated vasculopathic changes [22]. Interestingly APOE ε2 has been clearly associated with CAA related haemorrhage as the frequency of the ε2 allele is high regardless of whether significant AD related pathology was present. Aditionally in the group where significant AD pathology was present the APOE ε2 frequency is 4 times higher than in patients with AD without haemorrhage [46]. The mechanisms behind the influence of APOE ε2 on increased risk of cerebral haemorrhage are still yet to be elucidated, however it has been suggested that fibrinoid necrosis caused the breakage of amyloid laden vessels though its association with APOE ε2 [41].
With regards to vascular pathology, it is well known that CAA is associated with ischaemic stroke, cerebral infarction (particularly microinfarcts) in addition to haemorrhages [11, 47, 50, 60]. With increasing severity of CAA, smooth muscle and elastic elements in the vessel walls are replaced by Aβ depositions which results in fragile vessles and subsequent brain bleeds. Another consequence of Aβ in vessel walls is impaired vasoreactivity, which can lead to vessel narrowing/occlusion and hypoperfusion which may lead to ischaemic lesions in the parenchyma. When investigating the effects of severe CAA on vascular insults in the current cohort, of the 49 AD cases with severe CAA,13 were found to have infacts and microhaemorrhages, with no significant haemorrhages seen in any of the case. Out of the 4 DLB cases that exhibited CAA there were no reported vascular lesions in the neuropathological reports.
A neuroimaging study conducted by Gungor and colleagues demonstrated cerebral microbleeds (CMBs) were predominant in the occipital and frontal regions in DLB cases [23], which is in line with the finding that occipital and frontal lobes are the most frequently affected by CAA in DLB cases in the current study. Other groups have investigated the topography of CMBs across the Lewy body disease spectrum. Yamashgiro and colleagues found deep or infratentorial microbleeds were more common than lobar microbleeds (65.5% vs 34.5% respectively) in PD [65]. Although Kim and colleagues found no differences in frequency of deep or infratentorial microbleeds in DLB compared to PDD, they did demonstrate lobar microbleeds were found more frequently in DLB compared to PDD [33]. Also the occipital lobe is the brain region most commonly affected by microbleeds in DLB [53]. Interestingly, a study comparing CMBs between AD and DLB patients found there was no significant difference in the frequency of CMBs between AD and DLB, and the presence of microbleeds in DLB was not associated with amyloid deposition [16]. This suggests other mechanisms may underly the presence of microbleeds outside of general Aβ deposition, potentially the propensity of APOE ε2 carriers to exhibit more CAA vasculopathic changes in DLB. Taken together the results are inkeeping with the hypothesis that CAA is a common finding in DLB and may contribute to other pathological lesions and the clinical phenotype observed in these cases.
When investigating the APOE status in different subtypes of CAA we found APOE ε4 carriers were more likely to have type 1 CAA in the overall cohort. This is not surprising as Thal and colleagues found the frequency of APOE ε4 carriers in type 1 CAA is 4 times higher than in type 2 CAA in AD and controls, and type 2 CAA has a higher APOE ε2 frequency compared to type 1 CAA [54]. Another study investigating the masking effect APOE ε2ss protective association with comorbid AD related pathology also ran path analysis for the presence of type 1 CAA and found no significant associations between type 1 CAA APOE ε2. However, this study excluded all participants with non-AD dementia, therefore the effects of APOE ε2 in DLB warrants further investigation.
A caveat of this study is that all of the tissue used was sampled from the right hemisphere, due to the routine protocols carried out in the Newcastle Brain Tissue Resource. Several studies have observed hemispheric asymmetry in neurodegenerative pathologies that are associated with dementia [19, 34, 51]. In terms of Aβ neuroimaging Frings and colleagues demonstrate PiB retention on average was slightly higher in the right hemisphere compared to the left [19]. Whilst neuropathological studies by King and colleagues show mild asymmetry in 3/20 AD cases (with left and right hemisphere affected differently in different cases) [34]. Stefanits and colleagues demonstrate mild vulnerability of the righ hemisphere in 5/20 AD cases and 3/15 AD/DLB cases suggesting the proportion of asymmetry between cases that have AD or AD and DLB related pathologies was similar and we assume this would be similar in our cohort. We are not aware of studies that specifically investigate asymmetry of CAA, however this would be an interesting line of research.
Conclusion
Data from the current study supports growing evidence that CAA may play an important role in the clinico-pathological phenotype of Lewy body diseases, particularly DLB. We have shown DLB cases can have more severe CAA, have an increased presence of type 1 CAA, and have a different topographical distribution of CAA, which is similar to AD, compared to PDD and PD. In conclusion data from this study suggests DLB is more aligned with AD than PDD/PD with regards to CAA severity and topographical distribution, therefore should be considered when stratifying cases for clinical trials and the design of future disease modifying therapies.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- Aβ:
-
Amyloid beta
- AD:
-
Alzheimer’s disease
- BA:
-
Brodmann area
- CAA:
-
Cerebral amyloid angiopathy
- CERAD:
-
The Consortium to Establish a Registry for Alzheimer’s Disease
- CMB:
-
Cerebral microbleed
- DAB:
-
3,3 Diaminobezidine
- DLB:
-
Dementia with Lewy bodies
- LBD:
-
Lewy body disease
- NBTR:
-
Newcastle brain tissue resource
- NIA-AA:
-
National Institute on Aging–Alzheimer’s Association
- PDD:
-
Parkinson’s disease dementia
References
Alafuzoff I, Arzberger T, Al-Sarraj S, Bodi I, Bogdanovic N, Braak H et al (2008) Staging of neurofibrillary pathology in Alzheimer’s disease: a study of the BrainNet Europe Consortium. Brain Pathol 18(4):484A496. https://doi.org/10.1111/j.1750-3639.2008.00147.x
Arvanitakis Z, Leurgans SE, Wang Z, Wilson RS, Bennett DA, Schneider JA (2011) Cerebral amyloid angiopathy pathology and cognitive domains in older persons. Ann Neurol 69(2):320A327. https://doi.org/10.1002/ana.22112
Attems J (2005) Sporadic cerebral amyloid angiopathy: pathology, clinical implications, and possible pathomechanisms. Acta Neuropathol 110(4):345A359. https://doi.org/10.1007/s00401-005-1074-9
Attems J, Jellinger KA (2004) Only cerebral capillary amyloid angiopathy correlates with Alzheimer pathologyAa pilot study. Acta Neuropathol 107(2):83A90. https://doi.org/10.1007/s00401-003-0796-9
Attems J, Jellinger KA, Lintner F (2005) Alzheimer’s disease pathology influences severity and topographical distribution of cerebral amyloid angiopathy. Acta Neuropathol 110(3):222A231. https://doi.org/10.1007/s00401-005-1064-y
Badiola N, de Oliveira RM, Herrera F, Guardia-Laguarta C, Goncalves SA, Pera M et al (2011) Tau enhances alpha-synuclein aggregation and toxicity in cellular models of synucleinopathy. PLoS ONE 6(10):e26609. https://doi.org/10.1371/journal.pone.0026609
Boyle PA, Yu L, Nag S, Leurgans S, Wilson RS, Bennett DA, Schneider JA (2015) Cerebral amyloid angiopathy and cognitive outcomes in community-based older persons. Neurology 85(22):1930A1936. https://doi.org/10.1212/WNL.0000000000002175
Braak H, Alafuzoff I, Arzberger T, Kretzschmar H, Del Tredici K (2006) Staging of Alzheimer disease-associated neurofibrillary pathology using paraffin sections and immunocytochemistry. Acta Neuropathol 112(4):389A404. https://doi.org/10.1007/s00401-006-0127-z
Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, Braak E (2003) Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging 24(2):197A211. https://doi.org/10.1016/s0197-4580(02)00065-9
Brayne C, Richardson K, Matthews FE, Fleming J, Hunter S, Xuereb JH et al (2009) Neuropathological correlates of dementia in over-80-year-old brain donors from the population-based cambridge city over-75s cohort (CC75C) study. J Alzheimer’s Dis 18:645A658. https://doi.org/10.3233/JAD-2009-1182
Cadavid D, Mena H, Koeller K, Frommelt RA (2000) Cerebral beta amyloid angiopathy is a risk factor for cerebral ischemic infarction. A case control study in human brain biopsies. J Neuropathol Exp Neurol 59(9):768A773. https://doi.org/10.1093/jnen/59.9.768
Case NF, Charlton A, Zwiers A, Batool S, McCreary CR, Hogan DB et al (2016) Cerebral amyloid angiopathy is associated with executive dysfunction and mild cognitive impairment. Stroke 47(8):2010A2016. https://doi.org/10.1161/strokeaha.116.012999
Ciaccioli G, Martins A, Rodrigues C, Vieira H, Calado P (2013) A powerful yeast model to investigate the synergistic interaction of alpha-synuclein and tau in neurodegeneration. PLoS ONE 8(2):e55848. https://doi.org/10.1371/journal.pone.0055848
Clinton LK, Blurton-Jones M, Myczek K, Trojanowski JQ, LaFerla FM (2010) Synergistic interactions between abeta, tau, and alpha-synuclein: acceleration of neuropathology and cognitive decline. J Neurosci 30(21):7281A7289. https://doi.org/10.1523/jneurosci.0490-10.2010
Corder EH, Saunders AM, Strittmatter WJ, Schmechel DE, Gaskell PC, Small GW et al (1993) Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 261(5123):921A923. https://doi.org/10.1126/science.8346443
Donaghy PC, Firbank M, Mitra D, Petrides G, Lloyd J, Barnett N et al (2020) Microbleeds in dementia with Lewy bodies. J Neurol 267(5):1491A1498. https://doi.org/10.1007/s00415-020-09736-0
Dugger BN, Adler CH, Shill HA, Caviness J, Jacobson S, Driver-Dunckley E, Beach TG (2014) Concomitant pathologies among a spectrum of parkinsonian disorders. Parkinsonism Relat Disord 20(5):525A529. https://doi.org/10.1016/j.parkreldis.2014.02.012
Edison P, Rowe CC, Rinne JO, Ng S, Ahmed I, Kemppainen N et al (2008) Amyloid load in Parkinson’s disease dementia and Lewy body dementia measured with [11C]PIB positron emission tomography. J Neurol Neurosurg Psychiatry 79(12):1331A1338. https://doi.org/10.1136/jnnp.2007.127878
Frings L, Hellwig S, Spehl TS, Bormann T, Buchert R, Vach W et al (2015) Asymmetries of amyloid-β burden and neuronal dysfunction are positively correlated in Alzheimer’s disease. Brain 138(10):3089A3099. https://doi.org/10.1093/brain/awv229
Geinisman RV, Oksova EE (1988) Morphologic diagnosis of vascular and senile dementia (the significance of Congophilic angiopathy). Zh Nevropatol Psikhiatr Im S S Korsakova 88(7):35A39
Giasson BI, Forman MS, Higuchi M, Golbe LI, Graves CL, Kotzbauer PT et al (2003) Initiation and synergistic fibrillization of tau and alpha-synuclein. Science 300(5619):636A640. https://doi.org/10.1126/science.1082324
Greenberg SM, Vonsattel JP, Segal AZ, Chiu RI, Clatworthy AE, Liao A et al (1998) Association of apolipoprotein E epsilon2 and vasculopathy in cerebral amyloid angiopathy. Neurology 50(4):961A965. https://doi.org/10.1212/wnl.50.4.961
Gungor I, Sarro L, Graff-Radford J, Zuk SM, Tosakulwong N, Przybelski SA et al (2015) Frequency and topography of cerebral microbleeds in dementia with Lewy bodies compared to Alzheimer’s disease. Parkinsonism Relat Disord 21(9):1101A1104. https://doi.org/10.1016/j.parkreldis.2015.07.008
Halliday GM, Song YJ, Harding AJ (2011) Striatal beta-amyloid in dementia with Lewy bodies but not Parkinson’s disease. J Neural Transm 118(5):713A719. https://doi.org/10.1007/s00702-011-0641-6
Hansen D, Ling H, Lashley T, Foley J, Strand C, Eid T et al (2021) Novel clinicopathological characteristics differentiate dementia with Lewy bodies from Parkinson’s disease dementia. Neuropathol Appl Neurobiol 47(1):143A156. https://doi.org/10.1111/nan.12648
Heneka MT, Carson MJ, El Khoury J, Landreth GE, Brosseron F, Feinstein DL et al (2015) Neuroinflammation in Alzheimer’s disease. Lancet Neurol 14(4):388A405. https://doi.org/10.1016/s1474-4422(15)70016-5
Irwin DJ, Grossman M, Weintraub D, Hurtig HI, Duda JE, Xie SX et al (2017) Neuropathological and genetic correlates of survival and dementia onset in synucleinopathies: a retrospective analysis. Lancet Neurol 16(1):55A65. https://doi.org/10.1016/s1474-4422(16)30291-5
Jellinger KA (2002) Alzheimer disease and cerebrovascular pathology: an update. J Neural Transm 109(5A6):813A836. https://doi.org/10.1007/s007020200068
Jellinger KA (2021) Significance of cerebral amyloid angiopathy and other co-morbidities in Lewy body diseases. J Neural Transm 128(5):687A699. https://doi.org/10.1007/s00702-021-02345-9
Jellinger KA, Attems J (2008) Cerebral amyloid angiopathy in Lewy body disease. J Neural Transm (Vienna) 115(3):473A482. https://doi.org/10.1007/s00702-007-0856-8
Jellinger KA, Attems J (2006) Does striatal pathology distinguish Parkinson disease with dementia and dementia with Lewy bodies? Acta Neuropathol 112(3):253A260. https://doi.org/10.1007/s00401-006-0088-2
Joachim CL, Morris JH, Selkoe DJ (1988) Clinically diagnosed Alzheimer’s disease: autopsy results in 150 cases. Ann Neurol 24(1):50A56. https://doi.org/10.1002/ana.410240110
Kim SW, Chung SJ, Oh YS, Yoon JH, Sunwoo MK, Hong JY et al (2015) Cerebral microbleeds in patients with dementia with lewy bodies and parkinson disease dementia. AJNR Am J Neuroradiol 36(9):1642A1647. https://doi.org/10.3174/ajnr.A4337
King A, Bodi I, Nolan M, Troakes C, Al-Sarraj S (2015) Assessment of the degree of asymmetry of pathological features in neurodegenerative diseases. What is the significance for brain banks? J Neural Transm 122(10):1499A1508. https://doi.org/10.1007/s00702-015-1410-8
Kovacs GG, Alafuzoff I, Al-Sarraj S, Arzberger T, Bogdanovic N, Capellari S et al (2008) Mixed brain pathologies in dementia: the BrainNet Europe consortium experience. Dement Geriatr Cogn Disord 26(4):343A350. https://doi.org/10.1159/000161560
Love S, Chalmers K, Ince P, Esiri M, Attems J, Jellinger K et al (2014) Development, appraisal, validation and implementation of a consensus protocol for the assessment of cerebral amyloid angiopathy in post-mortem brain tissue. Am J Neurodegener Dis 3(1):19A32
Mäkelä M, Paetau A, Polvikoski T, Myllykangas L, Tanskanen M (2016) Capillary amyloid-β protein deposition in a population-based study (Vantaa 85+). J Alzheimer’s Dis 49(1):149A157. https://doi.org/10.3233/jad-150241
Matthews FE, Brayne C, Lowe J, McKeith I, Wharton SB, Ince P (2009) Epidemiological pathology of dementia: attributable-risks at death in the medical research council cognitive function and ageing study. PLoS Med 6(11):e1000180. https://doi.org/10.1371/journal.pmed.1000180
McAleese K, Walker L, Erskine D, Johnson M, Koss D, Thomas A, Attems J (2020) Concomitant LATE-NC in Alzheimer’s disease is not associated with increased tau or amyloid-β pathological burden. Neuropathol Appl Neurobiol 46(7):722A734. https://doi.org/10.1111/nan.12664
McAleese KE, Colloby SJ, Thomas AJ, Al-Sarraj S, Ansorge O, Neal J et al (2021) Concomitant neurodegenerative pathologies contribute to the transition from mild cognitive impairment to dementia. Alzheimer’s Dement 17(7):1121A1133. https://doi.org/10.1002/alz.12291
McCarron MO, Nicoll JAR, Stewart J, Ironside JW, Mann DMA, Love S et al (1999) The apolipoprotein E ∈2 allele and the pathological features in cerebral amyloid angiopathy-related hemorrhage. J Neuropathol Exp Neurol 58(7):711A718. https://doi.org/10.1097/00005072-199907000-00005
McKeith IG, Boeve BF, Dickson DW, Halliday G, Taylor JP, Weintraub D et al (2017) Diagnosis and management of dementia with Lewy bodies: fourth consensus report of the DLB Consortium. Neurology 89(1):88A100. https://doi.org/10.1212/wnl.0000000000004058
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM (1984) Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA work group under the auspices of department of health and human services task force on Alzheimer’s disease. Neurology 34(7):939A944. https://doi.org/10.1212/wnl.34.7.939
Mirra SS, Heyman A, McKeel D, Sumi SM, Crain BJ, Brownlee LM et al (1991) The consortium to establish a registry for Alzheimer’s disease (CERAD) Part II standardization of the neuropathologic assessment of Alzheimer’s disease. Neurology 41(4):479A486. https://doi.org/10.1212/wnl.41.4.479
Montine T, Phelps C, Beach T, Bigio E, Cairns N, Dickson D et al (2012) National institute on Aging–Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease: a practical approach. Acta Neuropathol 123:1A11. https://doi.org/10.1007/s00401-011-0910-3
Nicoll JAR, Burnett C, Love S, Graham DI, Dewar D, Ironside JW et al (1997) High frequency of apolipoprotein E ϵ2 Allele in hemorrhage due to cerebral amyloid angiopathy. Ann Neurol 41(6):716A721. https://doi.org/10.1002/ana.410410607
Olichney JM, Hansen LA, Hofstetter CR, Grundman M, Katzman R, Thal LJ (1995) Cerebral infarction in Alzheimer’s disease is associated with severe amyloid angiopathy and hypertension. Arch Neurol 52(7):702A708. https://doi.org/10.1001/archneur.1995.00540310076019
Parker JC Jr, Philpot J (1985) Postmortem evaluation of Alzheimer’s disease. South Med J 78(12):1411A1413. https://doi.org/10.1097/00007611-198512000-00003
Preston SD, Steart PV, Wilkinson A, Nicoll JA, Weller RO (2003) Capillary and arterial cerebral amyloid angiopathy in Alzheimer’s disease: defining the perivascular route for the elimination of amyloid beta from the human brain. Neuropathol Appl Neurobiol 29(2):106A117. https://doi.org/10.1046/j.1365-2990.2003.00424.x
Soontornniyomkij V, Lynch MD, Mermash S, Pomakian J, Badkoobehi H, Clare R, Vinters HV (2010) Cerebral microinfarcts associated with severe cerebral beta-amyloid angiopathy. Brain Pathol 20(2):459A467. https://doi.org/10.1111/j.1750-3639.2009.00322.x
Stefanits H, Budka H, Kovacs GG (2012) Asymmetry of neurodegenerative disease-related pathologies: a cautionary note. Acta Neuropathol 123(3):449A452. https://doi.org/10.1007/s00401-011-0936-6
Strittmatter WJ, Saunders AM, Schmechel D, Pericak-Vance M, Enghild J, Salvesen GS, Roses AD (1993) Apolipoprotein E: high-avidity binding to beta-amyloid and increased frequency of type 4 allele in late-onset familial Alzheimer disease. Proc Natl Acad Sci U S A 90(5):1977A1981. https://doi.org/10.1073/pnas.90.5.1977
Takemoto M, Yamashita T, Ohta Y, Tadokoro K, Omote Y, Morihara R, Abe K (2021) Cerebral microbleeds in patients with Parkinson’s disease and dementia with lewy bodies: comparison using magnetic resonance imaging and 99 mTc-ECD SPECT subtraction imaging. J Alzheimer’s Dis 80(1):331A335. https://doi.org/10.3233/jad-201495
Thal DR, Ghebremedhin E, Rub U, Yamaguchi H, Del Tredici K, Braak H (2002) Two types of sporadic cerebral amyloid angiopathy. J Neuropathol Exp Neurol 61(3):282A293. https://doi.org/10.1093/jnen/61.3.282
Thal DR, Rub U, Orantes M, Braak H (2002) Phases of A beta-deposition in the human brain and its relevance for the development of AD. Neurology 58(12):1791A1800. https://doi.org/10.1212/WNL.58.12.1791
Thomas DX, Bajaj S, McRae-McKee K, Hadjichrysanthou C, Anderson RM, Collinge J (2020) Association of TDP-43 proteinopathy, cerebral amyloid angiopathy, and Lewy bodies with cognitive impairment in individuals with or without Alzheimer’s disease neuropathology. Sci Rep 10(1):1A9. https://doi.org/10.1038/s41598-020-71305-2
Tian J, Shi J, Bailey K, Mann DM (2003) Negative association between amyloid plaques and cerebral amyloid angiopathy in Alzheimer’s disease. Neurosci Lett 352(2):137A140. https://doi.org/10.1016/j.neulet.2003.08.048
Toledo JB, Gopal P, Raible K, Irwin DJ, Brettschneider J, Sedor S et al (2016) Pathological α-synuclein distribution in subjects with coincident Alzheimer’s and Lewy body pathology. Acta Neuropathol 131(3):393A409. https://doi.org/10.1007/s00401-015-1526-9
Vinters HV, Gilbert JJ (1983) Cerebral amyloid angiopathy: incidence and complications in the aging brain. II. The distribution of amyloid vascular changes. Stroke 14(6):924A928. https://doi.org/10.1161/01.str.14.6.924
Vonsattel JP, Myers RH, Hedley-Whyte ET, Ropper AH, Bird ED, Richardson EP Jr (1991) Cerebral amyloid angiopathy without and with cerebral hemorrhages: a comparative histological study. Ann Neurol 30(5):637A649. https://doi.org/10.1002/ana.410300503
Walker L, McAleese KE, Thomas AJ, Johnson M, Martin-Ruiz C, Parker C et al (2015) Neuropathologically mixed Alzheimer’s and Lewy body disease: burden of pathological protein aggregates differs between clinical phenotypes. Acta Neuropathol 129(5):729A748. https://doi.org/10.1007/s00401-015-1406-3
Walker L, Stefanis L, Attems J (2019) Clinical and neuropathological differences between Parkinson’s disease, Parkinson’s disease dementia and dementia with Lewy bodies current issues and future directions. J Neurochem. https://doi.org/10.1111/jnc.14698
Xiong L, Davidsdottir S, Reijmer YD, Shoamanesh A, Roongpiboonsopit D, Thanprasertsuk S et al (2016) Cognitive profile and its association with neuroimaging markers of non-demented cerebral amyloid angiopathy patients in a stroke unit. J Alzheimer’s Dis 52(1):171A178. https://doi.org/10.3233/jad-150890
Xu D, Yang C, Wang L (2003) Cerebral amyloid angiopathy in aged Chinese: a clinico-neuropathological study. Acta Neuropathol 106(1):89A91. https://doi.org/10.1007/s00401-003-0706-1
Yamashiro K, Tanaka R, Hoshino Y, Hatano T, Nishioka K, Hattori N (2015) The prevalence and risk factors of cerebral microbleeds in patients with Parkinson’s disease. Parkinsonism Relat Disord 21(9):1076A1081. https://doi.org/10.1016/j.parkreldis.2015.06.019
Yu L, Boyle PA, Nag S, Leurgans S, Buchman AS, Wilson RS et al (2015) APOE and cerebral amyloid angiopathy in community-dwelling older persons. Neurobiol Aging 36(11):2946A2953. https://doi.org/10.1016/j.neurobiolaging.2015.08.008
Zekry D, Duyckaerts C, Belmin J, Geoffre C, Moulias R, Hauw JJ (2003) Cerebral amyloid angiopathy in the elderly: vessel walls changes and relationship with dementia. Acta Neuropathol 106(4):367A373. https://doi.org/10.1007/s00401-003-0738-6
Acknowledgements
We are grateful to the individuals and their families who kindly donated their brains to the Newcastle Brain Tissue Resource. This paper presents independent research supported by the NIHR Newcastle Biomedical Research Centre. The NIHR Biomedical Research Centre (BRC) is a partnership between Newcastle Hospitals NHS Foundation Trust, Newcastle University, and Cumbria, Northumberland and Tyne and Wear NHS Foundation Trustand is funded by the National Institute for Health and Care Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
L.W is funded by Alzheimer’s Research UK (Grant Number: ARUK-RF2020A-010). Tissue for this study was provided by the Newcastle Brain Tissue Resource, which is funded in part by a grant from the UK Medical Research Council (Grant Number G0400074) and by Brains for Dementia research, a joint venture between Alzheimer’s Society and Alzheimer’s Research UK.
Author information
Authors and Affiliations
Contributions
LW conceived the study, sourced the funding, interpreted the data, and wrote the original draft of the manuscript, HS collected and interpreted the data, and edited the manuscript. AT interpreted the data and edited the manuscript. JA conceived the study, interpreted the data, and edited the manuscript. All authors read and approved the final draft of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Brain tissue was obtained at autopsy and stored within the Newcastle Brain Tissue Resource (NBTR) in accordance with Newcastle University Ethics Board (The Joint Ethics Committee of Newcastle and North Tyneside Health Authority, reference: 08/H0906/136).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file1.
Additional vascular lesions in the cohort.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Walker, L., Simpson, H., Thomas, A.J. et al. Prevalence, distribution, and severity of cerebral amyloid angiopathy differ between Lewy body diseases and Alzheimer’s disease. acta neuropathol commun 12, 28 (2024). https://doi.org/10.1186/s40478-023-01714-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40478-023-01714-7