
Abstract
Background
Breaking bad news (BBN; e.g., delivering a cancer diagnosis) is perceived as one of the most demanding communication tasks in the medical field and associated with high levels of stress. Physicians’ increased stress in BBN encounters can negatively impact their communication performance, and in the long term, patient-related health outcomes. Although a growing body of literature acknowledges the stressful nature of BBN, little has been done to address this issue. Therefore, there is a need for appropriate tools to help physicians cope with their stress response, so that they can perform BBN at their best. In the present study, we implement the biopsychosocial model of challenge and threat as theoretical framework. According to this model, the balance between perceived situational demands and perceived coping resources determines whether a stressful performance situation, such as BBN, is experienced as challenge (resources > demands) or threat (resources < demands). Using two interventions, we aim to support medical students in shifting towards challenge-oriented stress responses and improved communication performance: (1) stress arousal reappraisal (SAR), which guides individuals to reinterpret their stress arousal as an adaptive and beneficial response for task performance; (2) worked examples (WE), which demonstrate how to BBN in a step-by-step manner, offering structure and promoting skill acquisition.
Methods
In a randomized controlled trial with a 2 (SAR vs. control) x 2 (WE vs. control) between-subjects design, we will determine the effects of both interventions on stress response and BBN skills performance in N = 200 third-year medical students during a simulated BBN encounter. To identify students’ stress responses, we will assess their perceived coping resources and task demands, record their cardiovascular activity, and measure salivary parameters before, during, and after BBN encounters. Three trained raters will independently score students’ BBN skills performances.
Discussion
Findings will provide unique insights into the psychophysiology of medical students who are tasked with BBN. Parameters can be understood more comprehensively from the challenge and threat perspective and linked to performance outcomes. If proven effective, the evaluated interventions could be incorporated into the curriculum of medical students and facilitate BBN skills acquisition.
Trial registration
ClinicalTrials.gov (NCT05037318), September 8, 2021.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Breaking Bad News – an important and stressful communication task
Breaking bad news (BBN) in the medical field refers to the delivery of a serious diagnosis (e.g., cancer diagnosis, stillbirth) from a physician to a patient which is associated with sudden lifechanging consequences for the patient [1, 2]. Not every diagnosis is of the same severity, and how bad news is received by the patient depends on many individual characteristics (e.g., expectations, personality traits, social support) [3]. Therefore, patients’ emotional reactions to bad news can differ greatly—from perplexity, silence, and disbelief to intense displays of anger or sadness—and are thus very difficult for the physician to predict [1, 4]. Even physicians who are frequently confronted with BBN regard it as highly demanding and stressful, and most often feel overwhelmed, uncomfortable, or insufficiently prepared [5,6,7,8,9]. Increased psychophysiological stress levels are observed in physicians during BBN encounters [6, 8]. Importantly, these increased stress levels can already be seen in medical students learning how to BBN in role-play scenarios with simulated patients (SPs) [10, 11]. Increased stress, in return, can impair educational and clinical skills performances (e.g., communication performance) of medical students in particular [12]. When being confronted with a BBN task, stressed physicians might give false hope or even avoid disclosing the bad news [3, 13]. However, it is of utter importance that bad news is delivered appropriately—with empathy while not trivializing unpleasant facts [1]. It has been shown that the way bad news is communicated can affect patient-related outcomes in the long term (e.g., treatment adherence [14,15,16], recovery [17,18,19], psychological wellbeing [18, 20]). While a growing body of literature acknowledges the highly stressful nature of BBN and investigates best-practice in BBN (see [8] for a review), further exploration of medical students’ stress responses is needed and tools to help them manage their stress in this context have been widely neglected. Although time-intensive stress management programs have helped students cope with their stress in medical training [21], integrating such programs into the already overloaded curriculum of medical students is problematic. Moreover, such extensive stress interventions can lack acceptance due to the fact that the state of ‘being stressed’ is increasingly seen as normal among medical students and that suffering from it may be viewed as a form of weakness [22]. Hence, there is a need for low-threshold approaches that allow students both to identify stress and to deal with it appropriately without being stigmatized [23].
In the current study, we aim to make a significant contribution to the advancement of research by adopting the biopsychosocial model (BPSM) of challenge and threat as organizing framework to investigate the effects of stress arousal reappraisal and worked example-based BBN learning on the psychophysiological responses and communication skills performance of medical students tasked with BBN to SPs. We first introduce the BPSM of challenge and threat, then the stress arousal reappraisal intervention, and finally, the worked example-based BBN learning.
The biopsychosocial model of challenge and threat
To understand medical students’ stress responses more holistically, we adopt the BPSM of challenge and threat as theoretical framework [24, 25]. The model builds on the premise that psychological stress states are embodied in measurable activity patterns of the cardiovascular system [26, 27]. The model is further specified to motivated performance situations, which require active (cognitive or behavioral) responses to achieve personally relevant outcomes (e.g., academic examinations, job interviews, public speaking) [24, 28, 29]. The active response and self-relevance lead to task engagement (indexed by an increased heart rate and a reduced pre-ejection period), which is a precondition for, and common across, the challenge-threat continuum [30]. Given task engagement, on the one hand, challenge emerges when individuals perceive their own resources (e.g., knowledge, abilities, familiarity) as higher than the situational demands (e.g., danger, effort, uncertainty). On the other hand, threat occurs when situational demands exceed perceived resources. The evaluation of resources and demands is an automatic and dynamic process (i.e., the evaluation can shift as the situation unfolds) [24, 25, 31, 32]. The resources-demands differential (i.e., perceived coping resources minus perceived task demands) is represented on a bipolar continuum, with challenge and threat as anchors, rather than distinct states. Therefore, relative differences in demands and resources can be interpreted as greater or lesser challenge and threat [33]. A more positive score reflects the task being evaluated as more of a challenge and less of a threat.
An important aspect of the BPSM of challenge and threat is that distinctive cardiovascular patterns manifest in challenge and threat states. Challenge states are accompanied by a lower total peripheral resistance (TPR; an index of net constriction vs. dilation in the vascular system) and increased cardiac output (CO; liters of blood pumped per minute) compared to threat states. In other words, not only does the heart pump more blood but the veins and arteries also expand to improve blood flow, resulting in a more efficient cardiovascular activity. This adaptation does not occur in threat states, meaning that the faster and stronger heart contractions during stress in fact increase TPR while not necessarily affecting CO [30, 34]. Together, the sum of CO and reverse scored TPR define the cardiovascular challenge-threat index. A higher cardiovascular challenge-threat index (higher CO, lower TPR) indicates a more adaptive challenge-oriented stress response. An advantage of the cardiovascular indices of challenge and threat is that they do not depend on an individual’s willingness or ability to accurately report on their appraisals [35, 36].
Recently, there has been increasing interest in understanding how other important physiological systems may vary along the challenge-threat continuum [28, 37]. It has been theorized that both challenge and threat states activate the sympathetic-adrenal-medullary (SAM) axis, whereas the hypothalamic-pituitary-adrenal (HPA) axis might be more responsive to threat states, in anticipation of failure and damage [30, 38,39,40].
Activation of the SAM axis increases the synthesis and release of catecholamines from the adrenal medulla—particularly epinephrine and norepinephrine—which in return trigger a multitude of cardiovascular adaptations. The main functions are to increase heart rate, reduce pre-ejection period, and constrict veins (to facilitate the return of oxygen-poor blood to the heart) [29]. Epinephrine further mediates adrenergic vasodilation (widening of blood vessels by relaxation of smooth muscles) [41]. These cardiovascular adaptations match the cardiovascular challenge pattern, which is suggested to be governed by the SAM activity. However, a downside of epinephrine and norepinephrine as indices of SAM activity is that they can only be measured reliably by blood taking. In this context, salivary alpha-amylase (sAA)—an enzyme secreted from the acinar cells of the salivary glands—has gained importance as a non-invasive marker for the activity of the locus coeruleus-norepinephrine system and peripheral SAM axis activity [42,43,44,45,46]. Previous research suggests that sAA may well indicate challenge and threat, whereby increased levels of sAA manifest in challenge states, although the authors acknowledge that this has yet to be confirmed by further research [47, 48]. The SAM axis is a fast-acting system and cardiovascular adaptations to stressors occur almost immediately.
In contrast, the main product of the HPA axis is the catabolic hormone cortisol, released from the adrenal cortex. It is theorized that cortisol dampens epinephrine-induced vasodilation, thereby increasing blood pressure when both axes are activated simultaneously [24, 39, 40]. In line with this, individuals in a cardiovascular threat state exhibited higher cortisol reactivity compared to individuals in a cardiovascular challenge state [49]. Activation of the HPA axis during acute stress also triggers the release of the anabolic hormone dehydroepiandrosterone (DHEA), which may play a protective factor during stress reaction and contribute to more favorable behavioral and emotional responses [50,51,52,53,54,55,56]. Elevated levels of DHEA compared to cortisol are further associated with resilience and thriving in stressful situations [57,58,59]. Therefore, the anabolic balance (i.e., the ratio of DHEA to cortisol) between the two hormones is of special interest, as they regulate each other and together could provide a sensitive indicator of challenge and threat [60]. While the HPA axis also responds instantly, observable adaptations and cortisol release take more time to manifest and to return to homeostasis.
To summarize, according to the BPSM of challenge and threat, an initial evaluation of personal resources and situational demands orchestrates downstream stress responses in the context of motivated performance situations (see Table 1). Crucially, previous research suggests that the resources-demands differential is amenable to interventions (e.g., [47, 61,62,63]) and, as shown in a recent meta-analysis [64], more adaptive challenge states are intertwined with increased task performance. In the present project, we propose stress arousal reappraisal and worked example-based learning interventions, that could be used to achieve more adaptive stress responses and communication performances in the BBN context.
Stress arousal reappraisal
Stress arousal reappraisal (SAR) makes use of the lay belief that stress is inherently negative. Experienced arousal (e.g., increased heart rate) during stressful situations (e.g., when giving a speech) is commonly perceived as debilitative and harmful towards task performance [39]. Consequently, a typical coping approach is to downregulate or eliminate stress arousal altogether [65]. Contrary to this misconception, SAR promotes the often-overlooked positive and adaptive aspects of stress responses and emphasizes an individuals’ agency in the emergence of said response. That is, the way people perceive stress (positive or negative) is in fact decisive to their stress responses [66]. Towards this end, SAR interventions instruct individuals to reinterpret stress arousal as a functional response, which is indeed beneficial for task performance. For instance, an increased heart rate prepares an individual for a demanding situation, by providing additional oxygen to the body and brain. The idea is that the act of defining stress arousal itself as a coping resource will cause a shift in the BPSM framework from threat towards challenge state, and ultimately promote more adaptive stress responses. It is noteworthy that task engagement is essential for reappraisal to thrive; if there is no sympathetic arousal to begin with, then there is nothing to reappraise [67]. In line with the suggested theory, previous research has demonstrated that SAR interventions lead to more efficient psychophysiological stress responses and improved task performance (e.g., [47, 48, 65, 68,69,70,71]).
Worked examples
BBN is a particularly delicate and challenging situation, and therefore devoted training is of utmost importance for physicians to optimize their BBN-performance [72, 73]. The question of how to best teach communication skills remains a core issue for medical schools worldwide [74,75,76]. We postulate that worked examples (WE) are a suitable approach to teach established BBN communication protocols (e.g., SPIKES, [1]). A worked example usually implies an initial problem (in our case how to BBN to a patient) and provides a step-by-step demonstration of its successful solution (in our case showing a physician BBN by following six steps of SPIKES). WEs are most useful for novice learners with restricted prior knowledge [77]. By breaking down an ill-defined task into individual steps, the complexity of the task, and at the same time, the cognitive load of the learner can be reduced. This allows for an easier acquisition of schemas in long-term memory, which can then be utilized to approach similar problems (e.g., communication of various diagnoses) [78]. Schemas can be retrieved as a single unit from memory despite cognitive constraints that might also occur during BBN [79]. While WE interventions have proven to be effective in well-defined domains such as mathematics and physics [80, 81], more recently, similar effects were demonstrated in ill-defined domains such as developing a medical diagnosis [82,83,84,85]. By improving the acquisition of relevant BBN-related schemas, preparatory worked example-based learning should increase the perceived coping resources of medical students tasked with BBN to an SP and should therefore promote a shifting of their stress responses from threat to challenge.
Hypotheses
The goal of this project is to determine how SAR and WE interventions influence (1) the psychophysiological stress response and (2) the communication-skills performance in medical students tasked with BBN in simulated settings. In addition, we will determine (3) if potential effects on communication performance are mediated by the psychophysiological stress response. Therefore, the study addresses following hypotheses:
H1.1 – Students receiving SAR instructions will exhibit significantly more adaptive, challenge-type psychophysiological responses (i.e., higher resources-demands differential, higher challenge-threat cardiovascular index, higher anabolic balance and higher sAA) than students receiving no SAR instructions.
H1.2 – Students receiving SAR instructions will show significantly better communication skills performance than students receiving no SAR instructions.
H2.1 – Students preparing themselves for the BBN task by learning from a BBN-related worked example will exhibit significantly more adaptive, challenge-type psychophysiological responses than students not preparatorily learning from a BBN-related worked example.
H2.2 – Students preparing themselves for the BBN task by learning from a BBN-related worked example will show significantly better communication skills performance than students not preparatorily learning from a BBN-related worked example.
H3.1 – The challenge-threat resources-demands differential and cardiovascular index are significant mediators of the effect of the SAR intervention on communication skills performance.
H3.2 – The challenge-threat resources-demands differential and cardiovascular index are significant mediators of the effect of preparatory worked example-based BBN learning on communication skills performance.
Furthermore, there are secondary, exploratory issues we want to address with this study. Theory suggests that SAR interventions might also improve mood [39]. However, research on this aspect is inconclusive [61] and the effects of WE on mood have not been investigated previously. Therefore, we treat the effects of SAR and WE on mood as an exploratory issue.
Stress mindsets are global belief systems about the nature of stress [86]. Individuals with a stress-is-enhancing mindset belief that stress is positive and promotes health and performance, whereas individuals with a stress-is-debilitating mindset belief that stress is negative and harms health and performance. By assessing stress mindsets before and after the interventions, we can check if the manipulations affected an individual’s perception of stress (e.g., [57]). This is especially interesting for medical students, since they already have a certain understanding of the functionality of stress responses presented in SAR. Pre-existing stress mindsets might be pivotal for the effectiveness of SAR interventions [67]. One previous study suggests that most cognitive benefits occur when an individual holds a stress-is-enhancing mindset and appraises a stressor as challenge [57]. However, one could also argue that instructing individuals with a stress-is-enhancing mindset to reappraise stress arousal as functional is redundant [67]. Therefore, we will (1) consider stress mindset as a control variable in the primary analysis and (2) analyze stress mindset as a secondary outcome, to evaluate if SAR interventions affect the stress mindset of medical students.
Methods
Participants
Participants will be German speaking third-year medical students from Swiss Universities, with no prior experience in BBN. They will be recruited through social media outlets, emails, and direct information in the lecture hall. Exclusion criteria are factors known to affect the psychophysiological outcomes: cardiovascular diseases, neuroendocrine conditions, use of psychotropic drugs or medication, and wearing a pacemaker. Female students additionally cannot participate if they are pregnant or lactating. Participants will be compensated with a monetary reward of 150 Swiss Francs for completing the study, and travel expenses will be reimbursed. Our goal is to collect valid data from 200 participants, to test the hypotheses with the necessary statistical power (see “Sample size calculation” for more details).
Study design
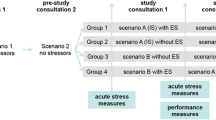
To test our hypotheses, we will conduct a randomized controlled trial applying a 2 (SAR vs. control) x 2 (WE vs. control) between-subjects design. Participants will be stratified according to gender and randomly assigned to one of four conditions: (1) SAR only, (2) WE only, (3) SAR and WE, (4) no intervention (see Fig. 1). Participants will be blinded to their condition and will not be informed about the various interventions. Raters of the BBN-skills performance will receive video recordings of the BBN situations in a random order with no information about the assigned condition. SPs interacting with the participants will only be present for the BBN situation and will not be informed about which intervention was applied before the encounter. The experimenters will not be blinded, as they are required to set up the corresponding learning modules (including interventions) for each session.

Flow of participants
Note: SAR = Stress arousal reappraisal; WE = Worked example
Study procedure
Online entry questionnaire
Interested students will be first invited to fill in an online entry questionnaire. The purpose of this questionnaire is to collect sociodemographic data as well as determine students’ eligibility. Eligible participants will then be scheduled for an individual experimental session in the research lab at the Institute for Medical Education in Bern.
Experimental session
The day before the experimental session, an email will be sent to the participants with the request to comply with the following instructions: no alcohol consumption and no intense physical activity 24 h before the session, no heavy meals and no caffeine consumption 2 h before the session, no smoking and no food consumption 1 h before the session.
The 2-hours session will start at 2pm for all participants to control for the psychophysiological effects of the circadian rhythm. The timing of each step will be identical across conditions (see Fig. 2).
Upon arrival at the lab, the experimental session, the cardiovascular measurement instruments, and the saliva sampling procedure will be explained to the participants, and written consent will be obtained from them. When explaining the experimental session, the experimenter will specifically mention that the BBN task will be video recorded, based on which participants’ performance will be rated. This information aims to increase participants’ task engagement. After these explanations, participants will have to verify their compliance with the behavioral instructions (food intake, caffeine consumption, etc.). Any violation of the behavioral instructions will be noted and considered in the statistical analysis. Participants will then be fitted with the sensors of the cardiovascular measurement devices (Finometer and VU-AMS). Next, a first saliva sample (S1) will be collected and a questionnaire (Q1; see Fig. 2 for details) answered, followed by a cardiovascular baseline measurement of 5 min (CV1). After the baseline measurement, participants will be informed about the setting of the upcoming task (i.e., BBN in prenatal setting). This will be followed by a cardiovascular recording of 2 min (CV2), a second saliva sample (S2), and a second questionnaire (Q2). During the next 40 min, participants will learn how to BBN with a web-based tool that includes a short introduction to BBN and the SPIKES protocol [1]. This protocol divides BBN into six stages (i.e., Setting, Perception, Invitation, Knowledge, Emotion, Strategy & Summary). The assigned intervention (SAR and/or WE) or control material will be part of this learning module. Immediately after the learning period, another saliva sample will be collected (S3), and a third questionnaire will be answered (Q3). Participants will then receive detailed information about a diagnosis (Trisomy 21) and be given 5 more minutes to prepare, before they have to deliver the bad news to an SP. For the BBN task, participants will be given a time limit of 12 min but will be allowed to finish earlier. Cardiovascular data will be recorded for 2 min before (CV3), during (CV4), and for 2 min after the BBN task (CV5). Next, another saliva sample will be collected (S4), and a fourth questionnaire will be answered (Q4). For the remainder of the experiment, there will be two blocks consisting in cardiovascular recording (CV6, CV7), followed by questionnaires (Q5, Q6) and saliva samples (S5, S6). During the cardiovascular recordings (excluding the BBN task), participants will be asked to sit quietly in an upright position, to not cross their legs, keep their eyes open, and their hands on the table.

Experimental Session
Note: Q1 contains the Multidimensional Mood State Questionnaire (MDMQ) and Stress Mindset Measure (SMM). Q2 contains the MDMQ, self-reported demands and resources, prior BBN experience and skills, and BBN interest and motivation. Q3 and Q4 both contain the MDMQ and self-reported demands and resources. Q5 includes the Depression, Anxiety and Stress Scale (DASS-21), Emotion Regulation Questionnaire (ERQ), SMM and MDMQ. Q6 contains the MDMQ
Measures
Online entry questionnaire measures
With the online entry questionnaire, the following sociodemographic control variables will be collected: age, gender, shift work (yes/no), and place of study. Additionally, to determine the eligibility of interested students, the following parameters will be gathered: current enrolment year, previous experiences in BBN, cardiovascular and neuroendocrine diseases, wearing a pacemaker (yes/no), use of medication and psychoactive drugs. Female participants will further provide information on the timing of their menstrual cycle and indicate whether they are pregnant, lactating, or use hormonal contraceptives.
Experimental session measures
From the measures obtained during the experimental session, we will derive primary outcomes, which will be used for hypothesis testing, and secondary outcomes, which will be used as control variables in the primary analyses or for exploratory analyses.
Cardiovascular measures
We will use two different devices to measure cardiovascular activity.
The Finometer (FMS Finapres Medical Systems, Amsterdam, The Netherlands) measures finger arterial pressure on a beat-to-beat basis by finger-cuff photoplethysmography. The finger cuff is wrapped around the middle phalanx of the left middle finger. Hydrostatic height correction of the finger with respect to the heart level will be active during the measurement. The Finometer produces waveform measurements similar to intra-arterial recordings and reconstructs brachial arterial pressure. The resulting artery pressure wave will provide systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP). Data recorded by the Finometer will be analyzed using Beatscope software. The Finometer will be paused during the learning phase, to relieve participants from prolonged pressure.
The VU Ambulatory Monitoring System (VU-AMS, Free University, Amsterdam, The Netherlands) consists of seven non-invasive electrodes, which will be applied on the participants’ thorax and back. The instrument is used to obtain impedance cardiographic and electrocardiographic data, namely, HR, PEP, left ventricular ejection time, stroke volume (SV) and CO. Data will be analyzed using the VU Data Analysis & Management Software (VU-DAMS).
The parameters derived from the two instruments are used to calculate the cardiovascular index of challenge and threat (z-scored CO-TPR), which represents a primary outcome used for hypothesis testing. CO is calculated by multiplying SV by HR (CO = SV*HR). TPR is then obtained by dividing MAP by CO (TPR = MAP/CO). In line with standard procedures in research using the BPSM of challenge and threat, HR and PEP will be analyzed to ensure that the sample as a whole was sufficiently engaged [25, 87].
A motion sensor embedded in the VU-AMS will record triaxial acceleration and angular velocity to quantify body motion, which will be used as a control variable.
Salivary measures
A passive drooling method will be used to collect saliva into low-bind polypropylene 2 mL cryovials (Salicap, IBL International, Hamburg, Germany). Before taking a sample, participants will be asked to swallow all saliva in their mouth, then accumulate saliva for 2 min, and finally transfer all saliva into the Salicap. After collection, the samples will be stored in a freezer at -30 °C. Free salivary cortisol (sC) and dehydroepiandrosterone (sDHEA) will be measured using a Cortisol and Dehydroepiandrosterone Saliva Luminescence Immunoassay kit (IBL-Tecan, Hamburg Germany), respectively. Salivary alpha amylase (sAA) activity will be measured using reagents provided by DiaSys Diagnostic Systems (Holzheim, Germany). Both the anabolic balance (sDHEA divided by sC) and sAA are primary outcomes used for hypothesis testing.
Self-reported demands and resources
Before the learning phase (Q2) and before the BBN task (Q3), we will assess perceived demands with the question “How demanding do you expect the BBN task to be?” and resources with the question “How able are you to cope with the demands of the BBN task?”. After the task (Q4), participants will report how they perceived the demands by answering the question “How demanding was the BBN task?” and their resources with the question “How able were you to cope with the demands of the BBN task?”. Participants will be asked to rate each item on a 6-point Likert scale, ranging from 1 “not at all” to 6 “extremely”. The items are adapted to the context of the BBN task from previous research [37, 88, 89]. The resources-demands differential (i.e., resource score minus demand score) represents a primary outcome used for hypothesis testing. Higher scores indicate more perceived resources compared to demands and therefore more challenge-oriented stress responses.
BBN-skills performance
Participants’ skills performances as shown during the BBN encounter will be scored by three independent raters based on video recordings. Raters will be trained on an adapted version of the SPIKES scale (see supplementary material) [90] and the ‘global Breaking Bad News Assessment Scale’ (glBAS) [91]. The adapted SPIKES scale contains one item for the steps Setting, Knowledge, Emotions, Strategy & Summary and two items for Perception and Invitation (for these two steps, the mean of the two items will be used). An additional item assesses non-verbal communication aspects. All items are rated on a bipolar five-point rating scale ranging from 1 to 5 (the higher the better). The glBAS contains 5 items [91]. Each item represents different domains of BBN and is rated on a 5-point Likert scale ranging from 1 “very good” to 5 “very poor”. We will reverse the values of the original glBAS items to match the SPIKES scale. For the SPIKES scale, the final score is the grand mean of all steps and the non-verbal communication item across the three raters. Each step as well as the non-verbal item will be weighted equally. For the glBAS, the final score will be the grand mean across the 5 items and three raters. Communication performance is a primary outcome used for hypothesis testing.
The raters’ training will be structured according to previous research [90] and given by FMS. During approximately three days of training, raters will be presented with an introduction to BBN and critical literature, and the assessment methods will be discussed. Raters will then independently score video examples covering low, mediocre, and high student BBN-related performances by using the two scales. Each evaluation run will be followed by a group discussion during which raters are requested to reach a consensus on evaluation results.
Mood
We will use the MDMQ short-scale [92, 93] to assess three dimensions of mood, following the conceptualization of Matthews et al. [94] and Schimmack et al. [95]: valence (bad/good), calmness (tense/calm), and energetic arousal (tired/awake). Valence and calmness are composed of 3 bipolar items each, whereas energetic arousal is measured by 2 items. The scale ranges from 1 to 8 with two opposing adjectives as anchors (e.g., “Right now I feel tired (1) / awake (8)”). The total score for valence and calmness ranges from 3 to 24, and for energetic arousal from 2 to 12. Half of the items are reverse scored. For the individual dimensions, higher scores represent more positive valence, higher calmness, and higher energetic arousal. Mood is a secondary outcome analyzed for exploratory purposes.
Stress mindset measure
To gauge the extent to which participants perceive stress as enhancing or debilitating, we will use a validated 4-item short version of the SMM [86]. We translated the items to German and conducted a back translation to control for quality (see supplementary material). Participants will rate each item on a 5-point scale ranging from 0 “strongly disagree” to 4 “strongly agree”. Half of the items are reversed, and the mean is calculated as index score. Higher scores correspond to a more stress-is-enhancing mindset. Stress mindset represents a control variable and secondary outcome used for exploratory analyses.
Depression, anxiety and stress
The DASS-21 [96, 97] measures the three emotional states depression, anxiety, and stress with 7 items each (total of 21 items). Participants indicate how each of the items applied to them over the past week. The scale ranges from 0 “Did not apply to me at all” to 3 “Applied to me very much or most of the time”. Scores are calculated for each of the three subscales. For each subscale, higher scores stand for a higher manifestation of the emotional state. The German version of the test possesses good psychometric properties [97]. Depression, anxiety, and stress will be treated as control variables.
Emotion regulation
We will assess participants’ habitual use of the two emotion regulation strategies expressive suppression (4 items; e.g., “I keep my emotions to myself”) and cognitive reappraisal (6 items; e.g., “When I want to feel more positive emotion (such as joy or amusement), I change what I’m thinking about”) in their daily life with the German version of the ERQ [98]. Each item is rated on a scale ranging from 1 “not at all” to 7 “completely”. The mean is calculated separately for each emotion regulation strategy. Participants’ habitual use of expressive suppression and cognitive reappraisal will be used as control variables.
Prior experience and skills in BBN
To control for possible differences in prior experience and skills in BBN, we developed a 3-item questionnaire (see supplementary material). Participants will have to state on 2 “yes/no” items if they have prior practical experience in or theoretical knowledge of BBN principles (if so, participants will need to specify in a free text field to what extend). On an additional item, participants will rate their perceived skill level in BBN from 1 “very low” to 7 “very high”.
BBN interest and motivation
Participants will report to what degree they are interested in BBN and motivated to do well at the BBN task using two 7-point scales (1 “very little interest” to 7 “very interested”; 1 “not at all motivated to perform well” to 7 “absolutely motivated to perform well”). Interest and motivation will be used as control variables.
Interventions
The interventions will be part of the learning phase and complement a written version of the SPIKES protocol, which all participants receive, regardless of their condition (see Fig. 3).
Stress arousal reappraisal
The content of the stress arousal reappraisal intervention is adapted from previous research [47, 61, 62, 69, 87, 99] and presented in the form of a 7-minute screencast using illustrations and voice-over. The screencast states that experiencing stress arousal is normal and legitimate and shows that an individual cares about a challenging situation. More specifically, participants will learn how stress arousal fulfills a vital function (e.g., an increased heart rate provides more oxygen to where it is needed) and is necessary for individuals to perform at their best. Therefore, stress arousal should be perceived as functional and beneficial for performance rather than harmful. To endorse the presented information, participants will then be asked to reflect on past and future stressful situations. Finally, right before the BBN communication task, participants will be reminded to reappraise the stress arousal they might experience in the encounter as beneficial for their BBN performance.
In the corresponding control condition, participants will be shown a 7-minute screencast about psychological and neurological learning processes (this is similar to control materials successfully used in previous studies, e.g., [87]).
Worked example
The WE will be presented in the form of a 10-minute video showing a simulated BBN encounter between a physician and a patient. The BBN encounter will be structured according to the six-step SPIKES protocol, with the physician performing each step appropriately. For instance, in the step Knowledge, the physician first announces that they have bad news, before delivering the specific diagnosis (“Unfortunately, I do not have any good news for you today”). Each of the steps is accompanied by a written hint, emphasizing which step is being displayed and why it is done in this way (in accordance with Lorch [100]). During the same period of 10 min, participants attributed to the corresponding control condition will continue working with the written SPIKES protocol.

Illustration of the learning module
Note: A general “Introduction of the BBN module” and “The six-step SPIKES framework” will be provided to participants of all groups. The worked example (“Demonstration”) and stress arousal reappraisal (“Optimizing stress arousal”) interventions will only be presented in the respective groups
Statistical analysis plan
To test the effectiveness of the interventions on communication performance (H1.2, H2.2), we will use 2 (SAR vs. no SAR) x 2 (WE vs. no WE) between-subjects ANOVAs. For the analysis of the repeated psychophysiological stress response outcomes (H1.1, H2.1), we will use linear mixed models with the participants as random effect. To test if the effects of the interventions on communication performance are mediated by the psychophysiological stress response (H3.1, H3.2), we will conduct a bootstrapping mediation analysis following state-of-the-art methodology [101]. We will follow international guidelines to derive the parameters used in the statistical analysis. For each cardiovascular measure, the mean of each 1-minute period will be calculated. For salivary measures, the area under the curve with respect to ground and increase will be computed. Where sensible, we will transform skewed variables to approach normality. We will perform sensitivity analyses with the control variables gender, age, BMI, use of hormonal contraceptives, shift work, SP, stress mindset, depression anxiety and stress, body motion, BBN-related interest & motivation, BBN-related prior experience & skills, and habitual use of emotion regulation strategies. For significance testing, an alpha level of 0.05 will be used.
Sample size calculation
An a-priori power analysis was performed to calculate the required sample size, using the G*Power 3 program [102]. We reviewed published data on psychophysiological and performance effects of our two interventions, to determine that an effect size of d = 0.40 [103] is scientifically reasonable and practically relevant. Given an alpha level of 0.05 (two-tailed) and a targeted power level of 0.80, n = 50 participants per group will be required. Thus, we will need a total of N = 200 participants with valid data to test our hypotheses. In case of device malfunctioning, dropouts, non-compliance or unusable data, additional participants will be scheduled until a total of 200 valid cases is reached.
Discussion
Implications
We anticipate the findings of the current project to have several important implications for theory and practice. Findings will provide unique insights into the psychophysiology of medical students who are tasked with BBN. Psychophysiological stress responses elicited in BBN encounters might be meaningfully mapped on to and understood from the challenge and threat perspective. In a next step, differences in stress responses can be linked to the level of communication performance. Most importantly, we propose two short interventions—stress arousal reappraisal and worked examples—that might not only improve students stress responses, but also cause cascading effects on communication performance.
If proven effective, findings may open new avenues for innovations in medical education. Not only do we provide a novel and more comprehensive understanding of BBN encounters, but we also propose low threshold interventions that could be easily incorporated into the curriculum of medical students. Further, we expect the benefits of stress arousal reappraisal to spill over to similar stress-inducing communications with patients or other motivated performance situations, which are ubiquitous in education and the medical workplace environment (e.g., [48, 68, 104]). Finally, improved communication also benefits health related outcomes of concerned patients [14,15,16,17,18,19,20].
The current project might further contribute to the advancement of the BPSM of challenge and threat. For the first time, we will assess the well-established psychophysiological indices of challenge and threat (self-reported demands and resources, cardiovascular parameters), together with less often used indices of the activity of the HPA and SAM axes (sC, sDHEA, sAA), and performance outcomes. Therefore, we hope to provide a more comprehensive understanding of individuals’ psychophysiological and behavioural stress responses. To the best of our knowledge, this project is also the first to explore and evaluate challenge and threat parameters in the unique context of BBN encounters. By doing so, we expand the framework to motivated performance situations in the medical field.
Possible pitfalls
We are aware that the present project is ambitious, which brings several possible challenges.
First, participation in the project will not be part of the regular medical study program but will rather be offered as an extracurricular learning opportunity. Although we assume that medical students have a general interest in communication training, we still rely on voluntary participation.
Second, medical students represent a distinct group of individuals compared to previous SAR-related research. In the third year, medical students already have a solid understanding of the functionality of their stress response, which is a core aspect of SAR interventions. Importantly, a person’s beliefs about stress (i.e., stress mindset) can affect their situation specific stress appraisal [67]. It remains to be seen how the SAR intervention applied in our study will affect the psychophysiology and performance of medical students specifically. We will investigate this issue by assessing participants’ stress mindset before and after the intervention and use it as control variable for primary analyses.
Third, there are more female medical students enrolled in Swiss universities than male students. Gender creates a possible confounder, given the different psychophysiology [87]. To ensure equal allocation to the experimental conditions, participants will therefore be stratified according to gender. Besides, the menstrual cycle of female participants causes monthly fluctuations of steroid hormones, which influence their psychophysiology. To control for these fluctuations, female participants will optimally be tested during the first week after menstruation. This puts restrictions on participation opportunities.
Lastly, while the BBN scenario is the same for all participants, for feasibility reasons, the SP role will be portrayed by different actors. To minimize any influence from SPs playing their role differently, a professional SP instructor of the Institute for Medical Education will provide detailed and identical training to each SP and ensure comparable acting. Further, SP will be considered as control variable in our statistical analyses. At the same time, because the BBN situation is only simulated, ecological validity could be questioned. Yet, due to the nature of the task, it is not feasible to conduct the experiment with real patients. It has been shown that communication skills performances exhibited in settings with SPs can predict performances in real clinical life [105].
Data Availability
Not applicable.
Abbreviations
- BBN:
-
Breaking bad news
- BPSM:
-
Biopsychosocial model
- CO:
-
Cardiac output
- DASS-21:
-
Depression Anxiety and Stress Scale
- DHEA:
-
Dehydroepiandrosterone
- ERQ:
-
Emotion Regulation Questionnaire
- glBAS:
-
Global Breaking Bad News Assessment Scale
- HPA:
-
Hypothalamic-pituitary-adrenal
- HR:
-
Heart rate
- MAP:
-
Mean arterial pressure
- MDMQ:
-
Multidimensional Mood State Questionnaire
- PEP:
-
Pre-ejection period
- sAA:
-
Salivary alpha-amylase
- SAM:
-
Sympathetic-adrenal-medullary
- SAR:
-
Stress arousal reappraisal
- sC:
-
Salivary cortisol
- sDHEA:
-
Salivary dehydroepiandrosterone
- SMM:
-
Stress Mindset Measure
- SP:
-
Simulated patient
- SV:
-
Stroke volume
- TPR:
-
Total peripheral resistance
- WE:
-
Worked example
References
Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES—A six-step protocol for delivering Bad News: application to the patient with Cancer. Oncologist. 2000;5(4):302–11.
Buckman R. Breaking Bad News: why is it still so difficult? British Medical Journal. (Clinical Res Edition). 1984;288(6430):1597–9.
Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. The Lancet. 2004;363(9405):312–9.
Gao Z. Delivering bad news to patients—the necessary evil. J Med Colleges Pla. 2011;26:103–8.
Brown R, Dunn S, Byrnes K, Morris R, Heinrich P, Shaw J. Doctors’ Stress Responses and Poor Communication Performance in Simulated Bad-News Consultations. Acad Med. 2009;84(11).
Francis L, Robertson N. Healthcare practitioners’ experiences of breaking bad news: a critical interpretative meta synthesis. Patient Educ Couns. 2023;107:107574.
Luz R, George A, Spitz E, Vieux R. Breaking bad news in prenatal medicine: a literature review. J Reproductive Infant Psychol. 2017;35(1):14–31.
Studer RK, Danuser B, Gomez P. Physicians’ psychophysiological stress reaction in medical communication of bad news: a critical literature review. Int J Psychophysiol. 2017;120:14–22.
Willis R, Strowd RE, Barks MC, Salas RE, Gamaldo CE, Lemmon ME. Education Research: the medical student perspective on challenging conversations. Neurology. 2020;95(5):226.
Cohen L, Baile WF, Henninger E, Agarwal SK, Kudelka AP, Lenzi R, et al. Physiological and psychological Effects of Delivering Medical News using a simulated physician–patient scenario. J Behav Med. 2003;26(5):459–71.
Hulsman RL, Pranger S, Koot S, Fabriek M, Karemaker JM, Smets EMA. How stressful is doctor–patient communication? Physiological and psychological stress of medical students in simulated history taking and bad-news consultations. Int J Psychophysiol. 2010;77(1):26–34.
Al-Ghareeb AZ, Cooper SJ, McKenna LG. Anxiety and clinical performance in simulated setting in Undergraduate Health Professionals Education: an integrative review. Clin Simul Nurs. 2017;13(10):478–91.
Maguire P. Barriers to Psychological Care of the dying. Br Med J (Clin Res Ed). 1985;291(6510):1711–3.
Haskard Zolnierek KB, DiMatteo MR. Physician Communication and Patient Adherence to Treatment: A Meta-Analysis. Med Care. 2009;47(8).
Osterberg L, Blaschke T. Adherence to Medication. N Engl J Med. 2005;353(5):487–97.
Rosenberg E, Lussier M-T, Beaudoin C. Lessons for Clinicians from Physician-Patient communication literature. Arch Fam Med. 1997;6:279–83.
Rao J, Weinberger M, Kroenke K. Visit-specific expectations and patient-centered outcomes. Arch Fam Med. 2000;9:1148–55.
Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995;152(9):1423–33.
Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician–patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301.
Ha J, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010;10:38–43.
Shapiro SL, Shapiro DE, Schwartz GER. Stress Management in Medical Education: A Review of the Literature. Acad Med. 2000;75(7).
Chew-Graham CA, Rogers A, Yassin N. I wouldn’t want it on my CV or their records’: medical students’ experiences of help-seeking for mental health problems. Med Educ. 2003;37(10):873–80.
Petko D, Egger N, Schmitz F, Totter A, Hermann T, Guttormsen S. Coping through blogging: A review of studies on the potential benefits of weblogs for stress reduction. Cyberpsychology: Journal of Psychosocial Research on Cyberspace. 2015;9.
Blascovich J. Challenge and threat. Handbook of Approach and Avoidance Motivation. Routledge; 2008.
Seery MD. Challenge or threat? Cardiovascular indexes of resilience and vulnerability to potential stress in humans. Neurosci Biobehavioral Reviews. 2011;35(7):1603–10.
Blascovich J, Mendes WB. Challenge and threat appraisals: the role of affective cues. Feeling and thinking: the role of affect in social cognition. Cambridge University Press; 2000. pp. 59–82.
Blascovich J, Tomaka J. The biopsychosocial model of arousal regulation. Advances in experimental social psychology. Volume 28. Academic Press; 1996. pp. 1–51.
Mendes W, Park J. Neurobiological concomitants of motivation. Adv motivation Sci. 2014;1:233–70.
Seery MD, Weisbuch M, Blascovich J. Something to gain, something to lose: the cardiovascular consequences of outcome framing. Int J Psychophysiol. 2009;73(3):308–12.
Johnston PR, Volkov AE, Ryan WS, Lee SWS. Planning, conducting, and analyzing a psychophysiological experiment on challenge and threat: A comprehensive tutorial. Behav Res Methods. 2022.
Quigley KS, Barrett LF, Weinstein S. Cardiovascular patterns associated with threat and challenge appraisals: a within-subjects analysis. Psychophysiology. 2002;39(3):292–302.
Weisbuch-Remington M, Mendes WB, Seery MD, Blascovich J. The nonconscious influence of religious symbols in motivated performance situations. Pers Soc Psychol Bull. 2005;31(9):1203–16.
Seery MD. The biopsychosocial model of challenge and threat: using the heart to measure the mind. Wiley-Blackwell Publishing Ltd.; 2013. pp. 637–53.
Blascovich J, Mendes WB. Social psychophysiology and embodiment. Handbook of social psychology. Volume 1, 5th ed. John Wiley & Sons, Inc.; 2010. pp. 194–227.
LeDoux JE. The emotional brain: the mysterious underpinnings of emotional life. New York, NY, US: Simon & Schuster; 1996. pp. 384–p.
Nisbett RE, Wilson TD. Telling more than we can know: verbal reports on mental processes. Psychol Rev. 1977;84:231–59.
Guyon AJAA, Studer RK, Hildebrandt H, Horsch A, Nater UM, Gomez P. Music performance anxiety from the challenge and threat perspective: psychophysiological and performance outcomes. BMC Psychol. 2020;8(1):87.
Dickerson SS, Kemeny ME. Acute stressors and cortisol responses: a theoretical integration and synthesis of Laboratory Research. Psychol Bull. 2004;130:355–91.
Jamieson JP, Crum AJ, Goyer JP, Marotta ME, Akinola M. Optimizing stress responses with reappraisal and mindset interventions: an integrated model. Anxiety Stress Coping. 2018;31(3):245–61.
Yeager DS, Lee HY, Jamieson JP. How to improve adolescent stress responses: insights from integrating implicit theories of personality and Biopsychosocial Models. Psychol Sci. 2016;27(8):1078–91.
Berntson GG, Quigley KS, Norman GJ, Lozano DL. Cardiovascular psychophysiology. In: Berntson GG, Cacioppo JT, Tassinary LG, editors. Handbook of psychophysiology. Cambridge Handbooks in psychology. 4 ed. Cambridge: Cambridge University Press; 2016. pp. 183–216.
Ali N, Nater UM. Salivary alpha-amylase as a biomarker of stress in behavioral medicine. Int J Behav Med. 2020;27(3):337–42.
Ditzen B, Ehlert U, Nater UM. Associations between salivary alpha-amylase and catecholamines – A multilevel modeling approach. Biol Psychol. 2014;103:15–8.
Nater UM, La Marca R, Florin L, Moses A, Langhans W, Koller MM, et al. Stress-induced changes in human salivary alpha-amylase activity—associations with adrenergic activity. Psychoneuroendocrinology. 2006;31(1):49–58.
Thoma MV, Kirschbaum C, Wolf JM, Rohleder N. Acute stress responses in salivary alpha-amylase predict increases of plasma norepinephrine. Biol Psychol. 2012;91(3):342–8.
Warren CM, van den Brink RL, Nieuwenhuis S, Bosch JA. Norepinephrine transporter blocker atomoxetine increases salivary alpha amylase. Psychoneuroendocrinology. 2017;78:233–6.
Beltzer ML, Nock MK, Peters BJ, Jamieson JP. Rethinking butterflies: the affective, physiological, and Performance Effects of Reappraising Arousal during Social evaluation. Emotion. 2014;14(4):761–8.
Jamieson JP, Mendes WB, Blackstock E, Schmader T. Turning the knots in your stomach into bows: reappraising arousal improves performance on the GRE. J Exp Soc Psychol. 2010;46(1):208–12.
Jamieson JP, Koslov K, Nock MK, Mendes WB. Experiencing discrimination increases risk taking. Psychol Sci. 2012;24(2):131–9.
Izawa S, Sugaya N, Shirotsuki K, Yamada KC, Ogawa N, Ouchi Y, et al. Salivary dehydroepiandrosterone secretion in response to acute psychosocial stress and its correlations with biological and psychological changes. Biol Psychol. 2008;79(3):294–8.
Melchior CL, Ritzmann RF. Dehydroepiandrosterone is an anxiolytic in mice mice on the plus maze. Pharmacol Biochem Behav. 1994;47(3):437–41.
Mendes W, Gray H, Mendoza-Denton R, Major B. Why Egalitarianism might be good for your health physiological thriving during Stressful Intergroup encounters. Psychol Sci. 2007;18:991–8.
Morgan CA III, Southwick S, Hazlett G, Rasmusson A, Hoyt G, Zimolo Z, et al. Relationships among plasma dehydroepiandrosterone sulfate and CortisolLevels, symptoms of dissociation, and objective performance in humans Exposedto Acute stress. Arch Gen Psychiatry. 2004;61(8):819–25.
Rasmusson AM, Vasek J, Lipschitz DS, Vojvoda D, Mustone ME, Shi Q, et al. An increased capacity for adrenal DHEA release is Associated with decreased avoidance and negative Mood symptoms in women with PTSD. Neuropsychopharmacology. 2004;29(8):1546–57.
Shields GS, Lam JCW, Trainor BC, Yonelinas AP. Exposure to acute stress enhances decision-making competence: evidence for the role of DHEA. Psychoneuroendocrinology. 2016;67:51–60.
Yehuda R, Brand SR, Golier JA, Yang RK. Clinical correlates of DHEA associated with post-traumatic stress disorder. Acta psychiatrica Scandinavica. 2006;114(3):187–93.
Crum AJ, Akinola M, Martin A, Fath S. The role of stress mindset in shaping cognitive, emotional, and physiological responses to challenging and threatening stress. Anxiety Stress Coping. 2017;30(4):379–95.
Epel ES, McEwen BS, Ickovics JR. Embodying psychological thriving: physical thriving in response to stress. Blackwell Publishing; 1998. pp. 301–22.
Russo S, Murrough J, Han M-H, Charney D, Nestler E. Neurobiology of Resilience. Nat Neurosci. 2012;15.
Berry Mendes W, Gray HM, Mendoza-Denton R, Major B, Epel ES. Why Egalitarianism might be good for your health: physiological thriving during Stressful Intergroup encounters. Psychol Sci. 2007;18(11):991–8.
Jamieson JP, Nock MK, Mendes WB. Mind over Matter: reappraising Arousal improves Cardiovascular and cognitive responses to stress. J EXPERIMENTAL PSYCHOLOGY-GENERAL. 2012;141(3):417–22.
Jamieson JP, Peters BJ, Greenwood EJ, Altose AJ. Reappraising stress Arousal improves performance and reduces evaluation anxiety in Classroom exam situations. Volume 7. Social Psychological and Personality Science; 2016. pp. 579–87. 6.
Sammy N, Anstiss PA, Moore LJ, Freeman P, Wilson MR, Vine SJ. The effects of arousal reappraisal on stress responses, performance and attention. Anxiety Stress Coping. 2017;30(6):619–29.
Behnke M, Kaczmarek LD. Successful performance and cardiovascular markers of challenge and threat: a meta-analysis. Int J Psychophysiol. 2018;130:73–9.
Brooks AW. Get excited: reappraising pre-performance anxiety as excitement. J Experimental Psychology-General. 2014;143(3):1144–58.
Jamieson JP, Hangen EJ, Lee HY, Yeager DS. Capitalizing on Appraisal processes to improve affective responses to social stress. Emot Rev. 2017;10(1):30–9.
Jamieson JP, Hangen EJ. Stress reappraisal interventions: Improving acute stress responses in motivated performance contexts. Handbook of wise interventions: How social psychology can help people change. 2021:239 – 58.
Brady ST, Hard BM, Gross JJ. Reappraising test anxiety increases academic performance of First-Year College Students. J Educ Psychol. 2018;110(3):395–406.
Jamieson JP, Nock MK, Mendes WB. Changing the conceptualization of stress in social anxiety disorder: affective and physiological consequences. Clin Psychol Sci. 2013;1(4):363–74.
Moore LJ, Vine SJ, Wilson MR, Freeman P. Reappraising threat: how to optimize performance under pressure. J Sport Exerc Psychol. 2015;37(3):339–43.
Rozek CS, Ramirez G, Fine RD, Beilock SL, Proceedings of the National Academy of Sciences of the United States of America. Reducing socioeconomic disparities in the STEM pipeline through student emotion regulation. 2019;116(5):1553-8.
Klein S, Tracy D, Kitchener HC, Walker LG. The effects of the participation of patients with cancer in teaching communication skills to medical undergraduates: a randomised study with follow-up after 2 years. Eur J Cancer. 1999;35(10):1448–56.
Meunier J, Merckaert I, Libert Y, Delvaux N, Etienne A-M, Liénard A, et al. The effect of communication skills training on residents’ physiological arousal in a breaking bad news simulated task. Patient Educ Couns. 2013;93(1):40–7.
Guttormsen S, Beyeler C, Bonvin R, Feller S, Schirlo C, Schnabel K, et al. The new licencing examination for human medicine: from concept to implementation. Swiss Med Wkly. 2013;143(4950):w13897.
Makoul G. The interplay between education and research about patient-provider communication. Patient Educ Couns. 2003;50:79–84.
Makoul G, Schofield T. Communication teaching and assessment in medical education: an international consensus statement. Patient Educ Couns. 1999;37(2):191–5.
Clark RC, Nguyen F, Sweller J, Baddeley M. Efficiency in learning: evidence-based guidelines to manage cognitive load. Perform Improv. 2006;45(9):46–7.
Sweller J, van Merrienboer JJG, Paas FGWC. Cognitive Architecture and Instructional Design. Educational Psychol Rev. 1998;10(3):251–96.
Chi MTH, Learning R, Development C, United States.Office of Naval R, National Institute of E, editors. : Learning Research and Development Center, University of Pittsburgh;[Pittsburgh, Pa.] 1981.
Atkinson RK, Derry SJ, Renkl A, Wortham D. Learning from examples: Instructional Principles from the worked examples Research. Rev Educ Res. 2000;70(2):181–214.
Paas F, van Gog T. Optimising worked example instruction: different ways to increase germane cognitive load. Learn Instruction. 2006;16(2):87–91.
Kopp V, Stark R, Fischer MR. Fostering diagnostic knowledge through computer-supported, case-based worked examples: effects of erroneous examples and feedback. Med Educ. 2008;42(8):823–9.
Kopp V, Stark R, Kühne-Eversmann L, Fischer MR. Do worked examples foster medical students’ diagnostic knowledge of hyperthyroidism? Med Educ. 2009;43(12):1210–7.
Schmitz FM, Schnabel KP, Stricker D, Fischer MR, Guttormsen S. Learning communication from erroneous video-based examples: a double-blind randomised controlled trial. Patient Educ Couns. 2017;100(6):1203–12.
Stark R, Kopp V, Fischer MR. Förderung der Diagnosekompetenz bei Studierenden der Medizin durch situiertes, fallbasiertes Lernen mit Lösungsbeispielen: der Einfluss von Fehlern und Feedback. Psychologie in Erziehung und Unterricht; Psychologie in Erziehung und Unterricht 2/2009 (Partnerschaft und Elternschaft (Themenreihe)). 2004.
Crum AJ. Rethinking stress: the role of mindsets in determining the stress response. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2013;73(12–BE):No–Specified.
Hangen EJ, Elliot AJ, Jamieson JP. Stress reappraisal during a mathematics competition: testing effects on cardiovascular approach-oriented states and exploring the moderating role of gender. Anxiety Stress Coping. 2019;32(1):95–108.
Moore LJ, Freeman P, Hase A, Solomon-Moore E, Arnold R. How consistent are challenge and threat evaluations? A generalizability analysis. Front Psychol. 2019;10.
Tomaka J, Blascovich J, Kelsey RM, Leitten CL. Subjective, physiological, and behavioral effects of threat and challenge appraisal. J Personal Soc Psychol. 1993;65:248–60.
Schmitz FM, Schnabel KP, Bauer D, Bachmann C, Woermann U, Guttormsen S. The learning effects of different presentations of worked examples on medical students’ breaking-bad-news skills: a randomized and blinded field trial. Patient Educ Couns. 2018;101(8):1439–51.
Schildmann J, Kupfer S, Burchardi N, Vollmann J. Teaching and evaluating breaking bad news: A pre–post evaluation study of a teaching intervention for medical students and a comparative analysis of different measurement instruments and raters. Patient Educ Couns. 2012;86(2):210–9.
Steyer R. Der mehrdimensionale Befindlichkeitsfragebogen: (MDBF); Handanweisung. Hogrefe, Verlag für Psychologie; 1997.
Wilhelm P, Schoebi D. Assessing Mood in Daily Life. Eur J Psychol Assess. 2007;23(4):258–67.
Matthews G, Jones DM, Chamberlain AG. Refining the measurement of mood: the UWIST Mood Adjective Checklist. Br J Psychol. 1990;81(1):17–42.
Schimmack U, Grob A. Dimensional models of core affect: a quantitative comparison by means of structural equation modeling. Eur J Pers. 2000;14(4):325–45.
Lovibond SH, Lovibond PF. Manual for the Depression anxiety stress scales. Psychology Foundation of Australia; 1996.
Nilges P, Essau C. Die depressions-angst-stress-skalen. Der Schmerz. 2015;29(6):649–57.
Abler B, Kessler H. Emotion regulation questionnaire – eine deutschsprachige Fassung des ERQ von Gross und John. Diagnostica. 2009;55(3):144–52.
Yeager DS, Bryan CJ, Gross JJ, Murray JS, Cobb DK, Santos PHF, et al. A synergistic mindsets intervention protects adolescents from stress. Nature. 2022;607(7919):512.
Lorch RF. Text-signaling devices and their effects on reading and memory processes. Educational Psychol Rev. 1989;1(3):209–34.
Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York, NY, US: Guilford Press; 2013.
Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91.
Cohen J. Statistical power analysis for the behavioral sciences. 2 ed. Hillsdale, NJ [u.a.]: Erlbaum; 1988.
Jamieson JP, Black AE, Pelaia LE, Gravelding H. Reappraising Stress Arousal Improves Affective, Neuroendocrine, and Academic Performance Outcomes in Community College Classrooms. J Exp Psychol Gen. 2021.
Tamblyn R, Abrahamowicz M, Dauphinee D, Wenghofer E, Jacques A, Klass D, et al. Physician scores on a National Clinical Skills Examination as Predictors of Complaints to Medical Regulatory Authorities. JAMA. 2007;298(9):993–1001.
Acknowledgements
Not applicable.
Funding
This study is funded by the Swiss National Science Foundation (subsidy number: 100019_200831). The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
MB has made substantial contributions to the conception and design of the study and has drafted the initial version of the manuscript. FS, CB, PG, SG and UN have made substantial contributions to the conception and design of the study and have substantively revised the first draft of the manuscript. All authors have approved the submitted version of the manuscript. All authors have agreed to be personally accountable for their contributions and ensured that questions related to the accuracy or integrity of any part of the work, even ones in which they were not personally involved, were appropriately investigated resolved and the resolution documented.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by the cantonal ethics commission of Bern (project-ID 2021–02098). The study will be conducted according to the World Medical Association Declaration of Helsinki, the ICH-Good Clinical Practice Guidelines, and the Swiss Federal Human Research Act. Each participant will be informed that participation in the study is voluntary and that they may withdraw from the study at any time and that withdrawal of consent will not have any consequences. The formal consent will be obtained before the participant is submitted to any study procedure. Participants will be compensated with a monetary reward of CHF 150.-, and travel expenses will be covered. Participants that do not complete the full experimental session will be compensated proportionally.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bosshard, M., Schmitz, F.M., Guttormsen, S. et al. From threat to challenge—Improving medical students’ stress response and communication skills performance through the combination of stress arousal reappraisal and preparatory worked example-based learning when breaking bad news to simulated patients: study protocol for a randomized controlled trial. BMC Psychol 11, 153 (2023). https://doi.org/10.1186/s40359-023-01167-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-023-01167-6