
Abstract
Purpose
The present three-dimensional (3D) finite element analysis (FEA) was aimed to assess the biomechanical effects and fracture risks of four different interforaminal implant-prosthodontic anchoring configurations exposed to frontal trauma.
Material and methods
A symphyseal frontal trauma of 1 MPa was applied to four dental implant models with different configurations (two unsplinted interforaminal implants [2IF-U], two splinted interforaminal implants [2IF-S], four unsplinted interforaminal implants[ 4IF-U], four splinted interforaminal implants [4IF-S]. By using a 3D-FEA analysis the effective cortical bone stress values were evaluated in four defined regions of interest (ROI) (ROI 1: symphyseal area; ROI 2: preforaminal area; ROI 3: mental foraminal area; and ROI 4: condylar neck) followed by a subsequent intermodel comparison.
Results
In all models the frontal traumatic force application revealed the highest stress values in the condylar neck region. In both models with a four-implant configuration (4IF-U, 4IF-S), the stress values in the median mandibular body (ROI 1) and in the condylar neck region (ROI 4) were significantly reduced (P <0.01) compared with the two-implant models (2IF-U, 2IF-S). However, in ROI 1, the model with four splinted implants (4IF-S) showed significantly (P < 0.01) reduced stress values compared to the unsplinted model (4IF-U). In addition, all models showed increased stress patterns in the area adjacent to the posterior implants, which is represented by increased stress values for both 2IF-U and 2IF-S in the preforaminal area (ROI 3) and for the four implant-based models (4IF-U, 4IF-S) in the mental foraminal area.
Conclusion
The configuration of four splinted interforaminal implants showed the most beneficial distribution of stress pattern representing reduced stress distribution and associated reduced fracture risk in anterior symphysis, condylar neck and preforaminal region.
Similar content being viewed by others


Introduction
According to the findings of numerous consensus statements, meta-analyses and systematic reviews the use of dental implants has emerged as a well‐accepted treatment modality for oral rehabilitation of edentulism [1,2,3,4]. Regardless of implant number, placement timing and procedures performed as well as the anchoring mechanism and the characteristics of the implant-prosthodontic anchoring used, patient satisfaction and comfort has increased significantly compared to conventional complete dentures [4,5,6,7].
In an increasingly ageing population, the associated and growing number of elderly patients requiring appropriate treatment of edentulism continues to gain importance [8,9,10]. In addition, the elderly population has also been shown to be highly physically active suggesting that this active and agile group of elderly patients may be increasingly exposed to the risk of physical maxillofacial trauma [11,12,13]. Within the field of traumatic maxillofacial lesions mandibular fractures represent the most common facial injuries predominantly related to accidents, violence and falls [14,15,16]. Moreover, epidemiologic studies have also reported fractures of the atrophic edentulous mandible occurring on account of reduced vascularity and decreased blood flow resulting in atrophy and bone weakening [17, 18].
Because the clinical use of dental implants is considered to increase as a result of significant implant‐prosthodontic advancements, oral and/or maxillofacial surgeons will also be faced with maxillofacial trauma in patients previously treated with dental implants [19,20,21]. Therefore, the aged population with previous implant-prosthodontic treatment suffering traumatic falls and/or injuries will represent a novel class of maxillofacial trauma patients [12, 17, 22]. Similar to traumatic events in patients containing osteosynthesis material dental implants are seen to alter the biomechanical bone behavior when exposed to traumatic forces [20, 23, 24].
However, only rare information is available on the evaluation of traumatic effects in patients with preceding dental implant treatment. In previous experimental studies, Kan et al. and Ayali and Bilginaylar analyzed two unsplinted implants exposed to traumatic situations using finite element analysis (FEA). Based on their findings, a more beneficial stress modulation was assumingly found for two implants placed in the lateral incisor region than for those placed in the canine region when frontal trauma was present [20, 21]. In an additional experimental study comparing the edentulous mandible without and with four interforaminal implants exposed to frontal trauma it was demonstrated that regardless of splinting or lack of splinting force absorption or transmission may shift the predominant fracture risk factor from the condylar neck to the corpus mandibulae [23].
For the oral rehabilitation of mandibular edentulism two or four interforaminal implants either with splinted bar suprastructure or unsplinted single attachments have been frequently used as a standard implant prosthodontic treatment procedure [7, 25,26,27]. According to the findings of the McGill consensus form two dental implants—splinted or non-splinted- supporting mandibular prosthesis are described as a minimum number for adequate denture stabilization and retention in the treatment of the completely edentulous mandible [27]. However, additional studies have demonstrated that the use of four implants for denture anchoring provides more rigid attachment by wide-ranging load distribution and reduced rotation than the use of two implants [28, 29]. Moreover, due to the stable anchoring design significantly higher quality of life outcome for patients has been reported for treatment concepts with four-implant splinted bar attachments [26].
In the following study two and four implant bar-connected implants with a round bar design were selected as favorable and most frequently used splinted implant configuration. Additionally, two and four single attachment configurations representing unsplinted anchoring comparing groups were included. Although these four implant-denture anchoring configurations are widely used, there is a lack of information concerning assessment and direct comparisons of traumatic response in situations of frontal trauma exposure. Based on previous literature and considering the lack of clinical data available, this topic of interest might be analyzed using finite element analysis (FEA). The use of FEA represents an appropriate and widely accepted non-invasive method providing valuable reproducible results for estimating various parameters of the complex biomechanics in the oral rehabilitation of mandibular edentulism and behavior of the mandible [20, 21, 32, 33].
The primary aim of this experimental 3-dimensional (3D) FEA study was to evaluate the biomechanical effects of two and four interforaminal implants either in a splinted or unsplinted form under a frontal facial trauma setting. As a secondary objective, the four different implant-denture anchoring configurations evaluated were compared for identifying the configuration form with the most beneficial stress pattern under simulated frontal trauma application.
Material and methods
Data acquisition
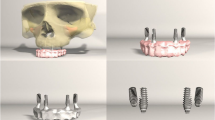
A scanned cone-beam computed tomography (CBCT) of a completely edentulous mandible of a 68-year-old male patient was used as the morphological base for the FEM models (ProMax, Planmeca, Helsinki, Finland). The selection of the image data as the anatomical template was based on the patient's medical record status with age-appropriate health and bone status, representing no morphological and mineralization variabilities. The image data with pixel conditions of 651 × 651, at 96 kV, and with increment slices of 0.2 mm in thickness was then converted to DICOM format. Using established image processing software (Amira) the acquisition of cortical and cancellous mandibular bone architecture data was achieved by semi-automatic segmentation of coronary CT layers. The reticulation of point clouds (Delauney-triangulation) to three-dimensional polygon meshes produced morphologically identical sub-models of the cortical and cancellous mandible (Fig. 1).

3-D edentulous mandible model with a two unsplinted interforaminal implants, b two splinted interforaminal implants, c four unsplinted interforaminal implants, d four splinted interforaminal implants.
CAD modeling
The generated rough polygon meshes could be converted as an DXF (drawing exchange format) to the reverse-engineering software Geomagic Wrap (Geomagic Studio, Rock Hill, SC) in order to generate a smooth computer-aided design (CAD) model of the mandible [34, 35, 35]. The design of all constructible elements of the model, such as implants, abutments, and the superstructure, could be performed virtually using established CAD tools in Inventor software (Autodesk, Munich, Germany) [23, 23, 34]. Dental implants with the dimensions of a Camlog Screw Line Promote dental implant (Camlog, Winsheim, Germany) with 3.8 mm in diameter and 13 mm in length were created based on imported Camlog CAD data [23, 23]. Detailed dimensions just as exact internal housing as well as external thread configuration were included in the detailed modelling process. In addition, the construction of corresponding abutments was performed based on imported Camlog CAD data dimensions of 13 mm in height and 3.8 mm in diameter.
Two implant configurations with two and four interforaminal implants were selected for the simulation. The anterior implant placement in the mandible was selected to be identical for both implant configurations. The horizontal implant position at the lateral incisor region was chosen for the 2-implant based configuration as well as for the anterior implants for the four-implant based configuration. Both anterior implants were placed enossally with an implant distance of 13 mm [36]. The 4IF configuration additionally included two posterior implants, which were placed in parallel to the anterior implants in the region of the first premolar about 5 mm mesial to the mental foramen [36]. The lateral implants were placed with a constant distance of 12.5 mm to the anterior implants on both sides [36]. Crestal implant placement was chosen for all implants as horizontal positioning.
The models with two and four incorporated interforaminal implants were then duplicated. Subsequently designed models of a two- and four-implant connecting suprastrucuture, representing a configuration corresponding to a fixed titanium framework similar to a bar or a fixed implant‐prosthodontic reconstruction were added to each corresponding model [37, 38]. Both implant-configuring splinting devices were constructed with identical dimensions in the area between the two anterior implants in terms of design and material thickness.
The combination of all corresponding solid models was conducted in Inventor™ software® (Autodesk GmbH) using Boolean operation method (addition and subtraction) [34, 35, 39]. The experimental study design then included four different models with two implant configurations: model 4IF-U: edentulous mandible with four unsplinted interforaminal implants; model 4IF-S: edentulous mandible with four splinted interforaminal implants; model 2IF-U, edentulous mandible with two unsplinted interforaminal implants and model 2IF-S, edentulous mandible with two splinted interforaminal implants (Fig. 1).
FEM modelling
All of the resulting CAD models (4IF-U,4IF-S,2IF-U,2IF-S) were entered into the finite element method Simulation section of Inventor software (Autodesk Inventor, Autodesk, San Rafael, USA). Then cross-linking in three dimensions was performed to build corresponding finite element method models. FEA represents an established mathematical technique that enables the reduction of complex geometries into a finite number of voxels (elements), each with a simple geometry. The element format used for the performed cross-linking was selected by the software as parabolic tetrahedrons with four nodes at each corner and one node in the center. The numbers of tetrahedrons and noduli of the four models are presented in Table 1 [34, 35, 39].
All individual structures of the FEM models were defined by specific material properties which are determined as standard values described in the current literature. In addition, the included materials were characterized as isotopic and elastic structures, respectively [40]. The ascribed values are presented in Table 2 [20, 21, 39, 41, 42]. The material properties of a titanium alloy (Ti-6Al-4V) were chosen for the implants and for both the abutments and the superstructure, as reported in previous FEA and clinical studies [43,44,45].
For the simulation a traumatic load of 1000 N was applied in perpendicular direction to the cortical bone surface of the symphysis (Fig. 2) [20, 21, 23]. A constrainment of the mandible was performed in the proximal portion of the condyles regarding the prevention of free movement in the x‐, y‐, and z‐axes during traumatic loading for simulating the presence of masticatory muscles during trauma [20, 21, 32, 33]. The contact conditions between the single model units of implants, abutments, and suprastructure were specified as constrained [20, 21]. The bone tissue/implant interfaces were considered to be fully osseointegrated [20, 21, 39, 46]. The simulation conditions regarding the force load and application as well as the boundary and contact conditions were identical for all models.

Simulation of frontal symphyseal trauma by application of 1000N.
Strain measurement
The traumatic cortical stress evaluation was conducted in detail for four defined specific regions which were selected on the basis of important areas of the mandible involved in traumatic fractures in recent literature [20, 21, 33]. The evaluated sites which were selected to be identical for all models, were defined as regions of interest (ROI) and were located as follows (Fig. 3):
-
1
ROI 1: region between the anterior implants, mandibular body
-
2
ROI 2: region between the anterior and lateral implants, preforaminal area
-
3
ROI 3: region posterior to the lateral implants, in the mental foramen area.
-
4
ROI 4: region at the condylar neck area.

Presents the analysed regions of interest (ROI) evaluated for von Mises stress values. (ROI 1 = anterior mandible; ROI 2 = preforaminal area, ROI 3 = mental foraminal region; ROI 4 = condylar neck region; homogenous distribution of the 20 pre-defined measurement points identical for all ROIs).
All regions showed a homogeneous area dimension of 10 × 6.5 mm, and the effective stress calculation in ROIs was conducted at 20 homogeneously distributed pre-defined measurement points at specific superficial cortical mandibular areas [23]. The measurement conditions represented identical inter-point distances, allocation and number of measured control points for all region of interest in all four models (Fig. 3). Therefore, an identical stress calculation of all trauma simulations could be achieved in all models. The traumatic stress evaluation was performed at these predicational survey areas according to von Mises equivalent stress dispersal.
Statistical analysis
The parameters (von Mises voltage values) of ROIs 1, 2,3 as well as 4 and models 2IF-U, 2IF-S,4IF-U and 4IF-S were tabulated as mean standard deviation. For the comparison of normally distributed continuous variables within each region, repeated analysis of variance or—in the case of non-normality (verification with the Kolmogorov- Smirnov test with Lilliefors correction)—Friedman rank analysis of variance was used. For post-hoc comparisons, Bonferroni-adjusted paired t-tests or Conover post-hoc tests were used. Type I error was set at 5% (2-sided) without adjustment for multiple testing, except for post-hoc comparisons, and P < 0.05 was considered statistically significant. Interindividual comparisons (ROI 1, 2, 3, or 4 for model 2IF-U vs ROI 1, 2, 3, or 4 for model 2IF-S vs ROI 1, 2, 3, or 4 for model 4IF-U, ROI 1, 2, 3, or 4 for model 4IF-S) were performed. For statistical analysis, the statistical software R (version 3.5.2; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org) was used.
Results
Figure 4 presents the individual finite element stress values (von Mises stress) evaluated for edentulous mandibular models with four different implant configurations (Fig. 4a: 2-unsplinted interforaminal implants [2IF-U], Fig. 4b: 2-splinted interforaminal implants [2 IF-S], Fig. 4c: 4-unsplinted interforaminal implants [4IF-U], Fig. 4d: 4-splinted interforaminal implant [4IF-S]) exposed to frontal symphyseal application of 1MPa of traumatic stress. The detailed data of the stress values generated for all models as well as for all regions of interest defined (ROI 1 [mandibular symphysis], ROI 2 [preforaminal area], ROI 3 [regio mentalis], ROI 4 [condylar neck) are presented in Table 3 (mean ± SD).

Show the Finite element stress values (von-Mises stress) for the 2IF-U model (a), 2IF-S model (b), 4IF-U model (c) as well for the 4IF-S model(d) exposed to symphyseal trauma. 2IF-U edentulous mandible model with two unsplinted interforaminal implants, 2IF-S edentulous mandible model with two splinted interforaminal implants, 4IF-U edentulous mandible model with four unsplinted interforaminal implants, 4IF-S edentulous mandible model with four splinted interforaminal implants
Figure 5a-d presents the stress values evaluated expressed as box plots for all ROIs 1—4 enabling intermodel comparisons. For the frontal symphyseal region of interest (ROI I) both models with four implants (4IF-U and 4IF-S) presented significantly (P < 0.001; P 0.043) reduced stress values as compared to models with two-implant-supported configurations (2IF-U and 2IF-S). In addition, the model with four splinted interforaminal implants (4IF-S: van Misses stress: 31.5± 9.9 MPa) also represented a significantly reduced stress level versus the edentulous mandible with four unsplinted implants (4IF-U: Van Misses stress: 42.8± 10.7 MPa; P < 0.001). In contrast, the stress values evaluated for the mandible with two splinted implants (2IF-S: Van Misses stress: 46.9± 11.7 MPa) and two unsplinted implants (2IF-U: van Misses stress: 48.5± 11.8 MPa) did not differ significantly (P 0.857, Table 3).
Van Misses stress values evaluated for ROI 2 (premental area) are presented in Fig. 5b. In ROI 2, both four-implant models (4IF-U, 4IF-S) demonstrated significantly lower stress values (P < 0.001; 0.012, 0,03) than both two-implant based configurations (2IF-U and 2IF-S). No significant differences were noted for comparisons within both 4-implant restored models (4IF-U vs 4IF-S; P > 0.129) as well for both two-implant models (2IF-U vs 2IF-S; P > 0.999, Table 3).
Figure 5c presents detailed von Mises stress values (box plots) of the ROI 3 corresponding to the mental foramen area. In the mental foraminal area (ROI 3) the stress values evaluated showed significantly (P < 0.001) lower values for both two-implant models (2IF-U, 2IF-S) as compared to both four-implant supported configurations (4IF-U, 4IF-U). However, the stress values in ROI 3 did not differ either within the four-implant or within the two-implant configuration (4IF-U vs 4IF-S P > 0.764 ; 2IF-U vs 2IF-S P = 0.999, Table 3).
By comparing all ROI within each model, the condylar neck area consistently represented the highest stress pattern (Fig. 5d, Table3). For the evaluated condylar neck area at ROI IV both four-implant restored mandibles showed significantly (P < 0.001) lower stress values than both two-implant configurations. However, the stress values in ROI 3 did not differ between the unsplinted and splinted implant models (4IF-U vs 4IF-S, P > 0 0.996; 2IF-U vs 2IF-S P = 0.999; Table3, Fig. 4c,d, Fig.5).

a-d Intermodel comparisons of stress values for ROI 1, ROI 2, ROI 3 and ROI 4 for 2IF-U model (a), 2IF-S (b), 4IF-U (c) and 4IF-S (d) with simulated frontal trauma. 2IF-U edentulous mandible model with two unsplinted interforaminal implants, 2IF-S edentulous mandible model with two splinted interforaminal implants, 4IF-U edentulous mandible model with four unsplinted interforaminal implants, 4IF-S edentulous mandible model with four splinted interforaminal implants
Discussion
According to the findings of numerous previous studies interforaminal implant placement are reported to have a weakening influence to the atrophic edentulous mandible [20, 21, 23, 47]. Different biomechanical studies could demonstrate that in case of facial trauma an osseointegrated dental implant leads to higher stress distribution and therefore a higher risk of fracture [20, 21]. Kan et al. study results show that the fracture risk increases with increasing inter-implant distance [21]. Additionally, Ayali et al. could show in their study that in case of traumatic forces higher stress levels occur where implants directly come in contact with cortical bone and subsequently a reduction of the risk of bone fracture in the mandible can be achieved by the insertion of the implant into spongious bone monocortically [20].
In addition splinted implant configuration have also been demonstrated providing reduced and beneficial stress conditions under traumatic loading [23, 23, 48, 49]. Therefore, by reducing the implant-surgical risk factors and using the prosthodontic beneficial splinted configuration it was initially hypothesized that an edentulous mandible using two splinted implants show reduced stress exposure and a lower fracture risk than four interforminal implants.
However, the according to the findings of the present experimental study this hypothesis had to be rejected. In particular, it could be shown that in a simulation of a frontal trauma the configurations with two interforaminal implants resulted in higher stress values in the anterior median mandibular area than those in models with four implants (4IF-S, 4IF-U). Regardless of whether the two interforaminal implants were used in splinted or unsplinted configuration, a frontal trauma consistently resulted in increased stress values in the area of the anterior implants and there in the periimplant cortical region, which may be attributed to the weakening of the bone by the implant insertion [20, 21, 23]. Thus, the results of the present experimental study confirm the data of Kan et al. [21] and Ayali und Bilginaylar [20] reporting that with two interforaminal implants exposure to a frontal trauma will result in increased stress values in the area of the periimplant bone as well as in the area of the implants [20, 21, 23, 24].
However, interestingly it could also be noted that in the case of a traumatic force exposure it is especially the number and the regional localization of the implants that show a significant impact on the stress distribution in the area of the anterior mandible [20, 21]. In obvious contrast to two interforaminal implants where the traumatic energy potential is immediately transmitted to the peri-implant cortical bone, exposure to a frontal traumatic force of a configuration with four implants will result in a more even distribution of the stress pattern. In particular, the comparison of four splinted interforaminal implants versus four unsplinted implants showed that the stress values were even more significantly reduced and thus associated with a favorable fracture risk in the symphysis area. This may be attributed to the fact that in the four-implant model the splinting suprastructure provides for transmission of the stress values to the splinted bar and/or the attachments and not directly to the peri-implant cortical bone as in the unsplinted model [23, 24, 50].
However, in obvious contrast to four splinted interforaminal implants the splinting device for two implants shows no significant effect on the stress and fracture behavior. This might be attributed to the reduced volume of splinting (bar length) with subsequently reduced potential of stress absorption as well as to the reduced number of implants (two vs four implants) and, consequently also to the reduced potential of stress distribution [51].
Implant splinting might be compared with the effect of a fixation providing for a positive effect on bone stress values and on fracture risk [52]. It is well known that external pin fixation represents a conventional method for stabilization of fracture segments and will also be used in certain settings in traumatology [52, 53]. A prosthetic bar or the supporting suprastructure for a fixed denture on four implants thus also represents a suitable external splinting even without an original intention and shows the potential of reducing the fracture risk in the symphysis region [23, 24].
In addition, it can be noted that the cortical stress in the preforaminal area (ROI 2) in the models with two inserted implants showed significantly higher values than in four-implant restored models. This may be explained by the fact that in a setting of anterior implant insertion and frontal trauma application the interaction of acceleration, mass inertia and deformation changes of the jawbone must be considered for increased cortical stress conditions [20, 21, 23].
In this respect, each configuration shows an increased stress pattern transmission into the distal region of the posterior implants [23, 24]. This theory of stress pattern distribution to the respective distal area of the posterior implants is also confirmed by the increased stress values in the ROI 2 with the configuration of two implants as well as by increased stress values in ROI 3 in the configuration of four implants. Strikingly, however, an additional splinting—in both implant configurations—produced no significant difference in the evaluated stress values for both the preforaminal area (ROI 2) and for the area around the mental foramen (ROI 3) concluding no influence of the suprastructure on the stress conduction into the posterior area [23, 24].
Moreover, the results of the present FEA show that upon frontal force application (symphyseal) the highest stress values—and consequently also the highest fracture risk—were invariably seen in the area of the condylar neck in all of the models [23, 24]. This obviously confirms the results of De Santos [33] for the edentulous mandible without implants and of Bilingylar and Ayali [20] for implant-treated mandibular models. According to Schwartz-Dabney and Dechow the bone relationships in the mandibular neck are narrower so that this region shows a lower bone stability which may consequently lead to an increased fracture tendency [54].
However, as a complementary finding the FEA analysis shows that the stress pattern in the condylar neck (ROI 4) in the models with two implants inserted was significantly increased versus the models with four implants. While the splinting configuration did not show any significant difference within both models. As the force load with a frontal trauma in the implant-treated mandible will be absorbed in the implant-adjacent bone regions, a reduction of the number of implants will consequently only result in a decreased reduction in the area of the condylar neck [23, 24]. Duplicating the number of implants from two to four will not only provide for stress absorption in an available implant connection (splint), but also in the peri-implant bone and will thus result in a significant stress reduction in the condylar neck and consequently provide for a reduced fracture risk in the condylar neck [23, 24].
Summary
Considering the results for all implant configurations and mandibular regions analyzed, the study was able to demonstrate that the configuration of four splinted implants provides for the most favorable stress conditions upon exposure with traumatic frontal force. This configuration shows a reduced stress distribution not only in the condylar neck, but also in the area of the symphysis and thus provides for a reduced fracture risk [21, 23, 24, 55]. Although an increased stress behavior and an increased fracture risk could be noted in the mental region with four interforaminal implants (splinted or unsplinted), this fracture region can be considered as a rather favorable site with respect to the surgical treatment options as compared to a fracture in the collum [56, 57].
Under adequate consideration of the limitations of this study, it must be noted that this study had an experimental design and only presents the changes on the objects studied [20, 21, 23]. Certainly, the risk of a mandibular fracture must be evaluated by varying degrees of mandibular atrophy and according to the bone quality of the mandible [33, 58]. The study served for exploring experimental findings which are to show a change in the fracture pattern and a relocation of potential injuries to sites providing for improved surgical access and/or facilitated treatment procedures [20, 23, 33].
Although recent literature reports have documented FEA in the mandible under traumatic conditions as reliable and accurate non-invasive method for evaluating biomechanical behavior and the anterior mandible as implantation site in our study has shown a homogenous structure, the results of this must currently be interpreted with appropriate caution [20, 21, 23, 55].
Availability of data and materials
Not applicable.
Change history
21 February 2024
A Correction to this paper has been published: https://doi.org/10.1186/s40001-024-01697-8
References
Chen K-W, Lin T-M, Liu P-R, Ramp LC, Lin H-J, Wu C-T, et al. An analysis of the implant-supported overdenture in the edentulous mandible. J Oral Rehabil. 2013;40:43–50.
Zitzmann NU, Marinello CP. A review of clinical and technical considerations for fixed and removable implant prostheses in the edentulous mandible. Int J Prosthodont. 2002;15:65–72.
Anas El-Wegoud M, Fayyad A, Kaddah A, Nabhan A. Bar versus ball attachments for implant-supported overdentures in complete edentulism: a systematic review. Clin Implant Dent Relat Res. 2018;20:243–50.
Maló P, de Araújo NM, Lopes A, Ferro A, Botto J. The All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: a longitudinal study with 10 to 18 years of follow-up. Clin Implant Dent Relat Res. 2019;21:565–77.
Emami E, Heydecke G, Rompré PH, de Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. Clin Oral Implants Res. 2009;20:533–44.
Thomason JM, Feine J, Exley C, Moynihan P, Müller F, Naert I, et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients—the York Consensus Statement. Br Dent J. 2009;207:185–6.
Melescanu Imre M, Marin M, Preoteasa E, Tancu AM, Preoteasa CT. Two implant overdenture–the first alternative treatment for patients with complete edentulous mandible. J Med Life. 2011;4:207–9.
Polzer I, Schimmel M, Müller F, Biffar R. Edentulism as part of the general health problems of elderly adults. Int Dent J. 2010;60:143–55.
Turkyilmaz I, Company AM, McGlumphy EA. Should edentulous patients be constrained to removable complete dentures? The use of dental implants to improve the quality of life for edentulous patients. Gerodontology. 2010;27:3–10.
Müller F, Srinivasan M, Krause K-H, Schimmel M. Periodontitis and peri-implantitis in elderly people experiencing institutional and hospital confinement. Periodontol 2000. 2022. https://doi.org/10.1111/prd.12454.
Bertin E, Louvrier A, Meyer C, Weber E, Barrabé A, Pons M. An epidemiologic retrospective study of maxillofacial traumatology in the elderly. J Stomatol Oral Maxillofac Surg. 2022. https://doi.org/10.1016/j.jormas.2022.05.024.
Aschkenasy MT, Rothenhaus TC. Trauma and falls in the elderly. Emerg Med Clin North Am. 2006;24(413–32):vii.
Llompart-Pou JA, Pérez-Bárcena J, Chico-Fernández M, Sánchez-Casado M, Raurich JM. Severe trauma in the geriatric population. World J Crit Care Med. 2017;6:99–106.
Wusiman P, Maimaitituerxun B, Guli null, Saimaiti A, Moming A. Epidemiology and Pattern of Oral and Maxillofacial Trauma. J Craniofac Surg. 2020;31:e517–20.
Manodh P, Prabhu Shankar D, Pradeep D, Santhosh R, Murugan A. Incidence and patterns of maxillofacial trauma-a retrospective analysis of 3611 patients-an update. Oral Maxillofac Surg. 2016;20:377–83.
Koshy JC, Feldman EM, Chike-Obi CJ, Bullocks JM. Pearls of mandibular trauma management. Semin Plast Surg. 2010;24:357–74.
Brucoli M, Boffano P, Romeo I, Corio C, Benech A, Ruslin M, et al. The epidemiology of edentulous atrophic mandibular fractures in Europe. J Craniomaxillofac Surg. 2019;47:1929–34.
Barber HD. Conservative management of the fractured atrophic edentulous mandible. J Oral Maxillofac Surg. 2001;59:789–91.
Oh W, Roumanas ED, Beumer J. Mandibular fracture in conjunction with bicortical penetration, using wide-diameter endosseous dental implants. J Prosthodont. 2010;19:625–9.
Ayali A, Bilginaylar K. Evaluating the biomechanical effects of implant diameter in case of facial trauma to an edentulous atrophic mandible: a 3D finite element analysis. Head Face Med. 2017;13:5.
Kan B, Coskunses FM, Mutlu I, Ugur L, Meral DG. Effects of inter-implant distance and implant length on the response to frontal traumatic force of two anterior implants in an atrophic mandible: three-dimensional finite element analysis. Int J Oral Maxillofac Surg. 2015;44:908–13.
Nogami S, Yamauchi K, Bottini GB, Otake Y, Sai Y, Morishima H, et al. Fall-related mandible fractures in a Japanese population: a retrospective study. Dent Traumatol. 2019;35:194–8.
Krennmair S, Winterhalder P, Hunger S, Rupperti S, Holberg C. The effects of frontal trauma on 4 interforaminal dental implants: a 3-dimensional finite element analysis comparing splinted and unsplinted implant configurations. J Oral Maxillofac Surg. 2020;78:961–72.
Krennmair S, Hunger S, Postl L, Winterhalder P, Holberg S, Malek M, et al. Edentulous mandible with four splinted interforaminal implants exposed to three different situations of trauma: a preliminary three-dimensional finite element analysis. Dent Traumatol. 2020. https://doi.org/10.1111/edt.12575.
Karbach J, Hartmann S, Jahn-Eimermacher A, Wagner W. Oral health-related quality of life in edentulous patients with two- vs four-locator-retained mandibular overdentures: a prospective, randomized, crossover study. Int J Oral Maxillofac Implants. 2015;30:1143–8.
Mumcu E, Bilhan H, Geckili O. The effect of attachment type and implant number on satisfaction and quality of life of mandibular implant-retained overdenture wearers. Gerodontology. 2012;29:e618-623.
Thomason JM, Kelly SAM, Bendkowski A, Ellis JS. Two implant retained overdentures––a review of the literature supporting the McGill and York consensus statements. J Dent. 2012;40:22–34.
Liu J, Pan S, Dong J, Mo Z, Fan Y, Feng H. Influence of implant number on the biomechanical behaviour of mandibular implant-retained/supported overdentures: a three-dimensional finite element analysis. J Dent. 2013;41:241–9.
Rosner O, Zenziper E, Heller H, Nissan J, Melamed G, Har-Ness S, et al. Long-term prosthetic aftercare of two- vs. four-ball attachment implant-supported mandibular overdentures. Appl Sci. 2021;11:8974.
de la Rosa CG, Guevara Perez SV, Arnoux P-J, Badih L, Bonnet F, Behr M. Implant-supported overdentures with different clinical configurations: mechanical resistance using a numerical approach. J Prosthet Dent. 2019;121:546.e1-546.e10.
Cakarer S, Can T, Yaltirik M, Keskin C. Complications associated with the ball, bar and Locator attachments for implant-supported overdentures. Med Oral Patol Oral Cir Bucal. 2011;16:e953-959.
Bezerra TP, Silva Junior FI, Scarparo HC, Costa FWG, Studart-Soares EC. Do erupted third molars weaken the mandibular angle after trauma to the chin region? A 3D finite element study. Int J Oral Maxillofac Surg. 2013;42:474–80.
Santos LSdM, Rossi AC, Freire AR, Matoso RI, Caria PHF, Prado FB. Finite-element analysis of 3 situations of trauma in the human edentulous mandible. J Oral Maxillofac Surg. 2015;73:683–91.
Holberg C, Winterhalder P, Holberg N, Wichelhaus A, Rudzki-Janson I. Orthodontic bracket debonding: risk of enamel fracture. Clin Oral Investig. 2014;18:327–34.
Holberg C, Winterhalder P, Wichelhaus A, Hickel R, Huth K. Fracture risk of lithium-disilicate ceramic inlays: a finite element analysis. Dent Mater. 2013;29:1244–50.
Kim K-S, Kim Y-L, Bae J-M, Cho H-W. Biomechanical comparison of axial and tilted implants for mandibular full-arch fixed prostheses. Int J Oral Maxillofac Implants. 2011;26:976–84.
Barão V, a. R, Delben JA, Lima J, Cabral T, Assunção WG. Comparison of different designs of implant-retained overdentures and fixed full-arch implant-supported prosthesis on stress distribution in edentulous mandible–a computed tomography-based three-dimensional finite element analysis. J Biomech. 2013;46:1312–20.
Idzior-Haufa M, Pilarska AA, Hędzelek W, Boniecki P, Pilarski K, Dorocka-Bobkowska B. A comparison of biomechanical properties of implant-retained overdenture based on precision attachment type. Materials. 2021;14:2598.
Holberg C, Winterhalder P, Rudzki-Janson I, Wichelhaus A. Finite element analysis of mono- and bicortical mini-implant stability. Eur J Orthod. 2014;36:550–6.
Gallas Torreira M, Fernandez JR. A three-dimensional computer model of the human mandible in two simulated standard trauma situations. J Craniomaxillofac Surg. 2004;32:303–7.
Liu X, Chen S, Tsoi JKH, Matinlinna JP. Binary titanium alloys as dental implant materials—a review. Regen Biomater. 2017;4:315–23.
Geng JP, Tan KB, Liu GR. Application of finite element analysis in implant dentistry: a review of the literature. J Prosthet Dent. 2001;85:585–98.
Pandoleon P, Bakopoulou A, Papadopoulou L, Koidis P. Evaluation of the biological behaviour of various dental implant abutment materials on attachment and viability of human gingival fibroblasts. Dent Mater. 2019;35:1053–63.
Shah FA, Trobos M, Thomsen P, Palmquist A. Commercially pure titanium (cp-Ti) versus titanium alloy (Ti6Al4V) materials as bone anchored implants—is one truly better than the other? Mater Sci Eng C Mater Biol Appl. 2016;62:960–6.
Kümbüloğlu Ö, Koyuncu B, Yerlioğlu G, Al-Haj Husain N, Özcan M. Stress distribution on various implant-retained bar overdentures. Materials. 2022;15:3248.
Osman RB, Elkhadem AH, Ma S, Swain MV. Titanium versus zirconia implants supporting maxillary overdentures: three-dimensional finite element analysis. Int J Oral Maxillofac Implants. 2013;28:e198-208.
Raghoebar GM, Stellingsma K, Batenburg RH, Vissink A. Etiology and management of mandibular fractures associated with endosteal implants in the atrophic mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:553–9.
de Faria Almeida DA, Verri FR, Lemos CAA, de Souza Batista VE, Santiago Júnior JF, Rosa CDDRD, et al. Effect of splinting of tilted external hexagon implants on 3-unit implant-supported prostheses in the posterior maxilla: a 3d finite element analysis. J Prosthodont. 2022;31:697–704.
Nissan J, Ghelfan O, Gross M, Chaushu G. Analysis of load transfer and stress distribution by splinted and unsplinted implant-supported fixed cemented restorations. J Oral Rehabil. 2010;37:658–62.
Behnaz E, Ramin M, Abbasi S, Pouya MA, Mahmood F. The effect of implant angulation and splinting on stress distribution in implant body and supporting bone: a finite element analysis. Eur J Dent. 2015;9:311–8.
Bhering CLB, Mesquita MF, Kemmoku DT, Noritomi PY, Consani RLX, Barão VAR. Comparison between all-on-four and all-on-six treatment concepts and framework material on stress distribution in atrophic maxilla: a prototyping guided 3D-FEA study. Mater Sci Eng C Mater Biol Appl. 2016;69:715–25.
Cornelius C-P, Augustin JB, Sailer L-K. External pin fixation for stabilization of the mandible–comeback of a method: historical review and first experiences with the “mandible external fixator.” Oral Maxillofac Surg. 2009;13:1–14.
Ellis E, Muniz O, Anand K. Treatment considerations for comminuted mandibular fractures. J Oral Maxillofac Surg. 2003;61:861–70.
Schwartz-Dabney CL, Dechow PC. Variations in cortical material properties throughout the human dentate mandible. Am J Phys Anthropol. 2003;120:252–77.
Liu Y, Wang R, Baur DA, Jiang X. A finite element analysis of the stress distribution to the mandible from impact forces with various orientations of third molars. J Zhejiang Univ Sci B. 2018;19:38–48.
Cortese A, Borri A, Bergaminelli M, Bergaminelli F, Claudio pp. Condylar neck and sub-condylar fractures: surgical consideration and evolution of the technique with short follow-up on five cases. Dent J. 2020;8:125.
Perez D, Ellis E. Complications of mandibular fracture repair and secondary reconstruction. Semin Plast Surg. 2020;34:225–31.
Bujtár P, Sándor GKB, Bojtos A, Szucs A, Barabás J. Finite element analysis of the human mandible at 3 different stages of life. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:301–9.
Acknowledgements
None.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors, but was supported by Johannes Kepler Open Access Publishing Fund.
Author information
Authors and Affiliations
Contributions
SK performed the evaluation and analysis and wrote the manuscript. SK and LP designed the study. All authors were involved in the data processing, the evaluation and analysis and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All the authors gave consent for the publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The given and family names of all the authors except "Philip Stähler" which were swapped inadvertently have been corrected.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Krennmair, S., Malek, M., Stehrer, R. et al. The effect of frontal trauma on the edentulous mandible with four different interforaminal implant-prosthodontic anchoring configurations. A 3D finite element analysis. Eur J Med Res 28, 608 (2023). https://doi.org/10.1186/s40001-023-01580-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01580-y