
Abstract
Background
Antimicrobial resistance (AMR) is widely acknowledged as a global health problem, yet its extent is not well evaluated, especially in low-middle income countries. It is challenging to promote policies without focusing on healthcare systems at a local level, therefore a baseline assessment of the AMR occurrence is a priority. This study aimed to look at published papers relating to the availability of AMR data in Zambia as a means of establishing an overview of the situation, to help inform future decisions.
Methods
PubMed, Cochrane Libraries, Medical Journal of Zambia and African Journals Online databases were searched from inception to April 2021 for articles published in English in accordance with the PRISMA guidelines. Retrieval and screening of article was done using a structured search protocol with strict inclusion/exclusion criteria.
Results
A total of 716 articles were retrieved, of which 25 articles met inclusion criteria for final analysis. AMR data was not available for six of the ten provinces of Zambia. Twenty-one different isolates from the human health, animal health and environmental health sectors were tested against 36 antimicrobial agents, across 13 classes of antibiotics. All the studies showed a degree of resistance to more than one class of antimicrobials. Majority of the studies focused on antibiotics, with only three studies (12%) highlighting antiretroviral resistance. Antitubercular drugs were addressed in only five studies (20%). No studies focused on antifungals. The most common organisms tested, across all three sectors, were Staphylococcus aureus, with a diverse range of resistance patterns found; followed by Escherichia coli with a high resistance rate found to cephalosporins (24–100%) and fluoroquinolones (20–100%).
Conclusions
This review highlights three important findings. Firstly, AMR is understudied in Zambia. Secondly, the level of resistance to commonly prescribed antibiotics is significant across the human, animal, and environmental sectors. Thirdly, this review suggests that improved standardization of antimicrobial susceptibility testing in Zambia could help to better delineate AMR patterns, allow comparisons across different locations and tracking of AMR evolution over time.
Similar content being viewed by others

Background
The SARS-COV-2 pandemic has highlighted the importance of implementing working systems at a local level to mitigate and prevent spread of infectious diseases. Antimicrobial resistance (AMR) has been highlighted by the World Health Organization (WHO) as a prominent threat to global health [1]. There is specific concern of low-middle income countries (LMICs) where there is poor surveillance, poor diagnosis measure and a lack of guidelines indicating therapy procedures [2]. A regional and national understanding of AMR is needed to improve human health, animal health and agricultural productivity per country [3]. A 2022 study highlights that bacterial AMR is the most prevalent cause of death related to drug resistance [4]. Given the global importance of bacterial AMR, there is an urgent need to highlight the clinically relevant resistance related to bacteria, especially in LMICs [4]. LMICs have unique socioeconomic and cultural settings that challenge the strategies from policy makers on the world stage [5], as a result of this, antimicrobial stewardship strategies must be tailored specifically from the ground level. In many LMICs, the use of antimicrobials for treatment remain undocumented and unregulated [6].
The One Health Approach is the ‘collaborative effort of multiple disciplines – working locally, nationally, and globally – to attain optimal health for people, animals and our environment…’ [7] and recognizes that there is a link between these three domains. The WHO has stated that the One Health approach is critical to addressing health threats across all three interfaces [8]. The concept focuses on the consequences, responses and actions across the human-animal-environment sectors highlighting the importance of balance and interconnectedness. A solo approach only focusing on health education will not lead to effective results because these three sources are interrelated. AMR understanding and control should be approached ideally from a One Health perspective since resistance can arise in the human, animal or the environment and spread from one to another [9].
A report was developed by the Zambian National Public Health Institute (ZNHPI) and the Centre for Science and Environment (CSE) India highlighting the need to prepare a surveillance system for Zambia [10]. This report mentions the need for interventions, however, does not reflect the rate of AMR data and studies in Zambia to date. Zambia faces a generalized HIV epidemic, with most deaths resulting from opportunistic infections. Malaria is considered to be the main cause for hospitalization, and the biggest contributor to morbidity and mortality rates [10, 11]. There have also been outbreaks of cholera, meningococcal meningitis, pneumonia, and typhoid in Zambia [10]. Standard infections are becoming increasingly difficult to treat with standard first-line antibiotics because of AMR, leading to the necessary use of newer, more targeted, but also more expensive antibiotics [12, 13].
A consolidated approach is needed to address the complexity and scale of the problem which includes incorporating the various fields of governance and policy makers [14]. When an overview of antimicrobial practice is known, more tailored implementations and control measures can be planned; and understood. Unique insight into antibiotic prescribing, ideas about AMR, and insights into use of antimicrobials in the animal and agriculture sectors. We conducted a systematic review assessing the prevalence of AMR in Zambia as a means of establishing an overview of the situation, to help inform future decisions as there are currently no guidelines in place to monitor the use of antimicrobials, nor is there standardized testing procedures in place, to date. This review will assist in creating a more tailored approach in implementing interventions by highlighting the levels of resistance and lack of data that need to be addressed across all sectors.
Methods
Search strategy
A systematic review was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines (Fig. 1) [15]. The search terms [(multiresistant OR multi-drug resistant OR antimicrobial resistance OR drug resistance OR bacterial resistance) AND (Zambia)] were used to identify relevant literature from Cochrane Libraries, PubMed, Medical Journal of Zambia and African Journals Online databases. Various spellings of the search terms were considered. A total of 994 articles were identified from the four databases that were searched using Boolean search strategies to obtain English articles relating to AMR and Zambia. No limitation on publication dates were set. Literature search began in March 2021, with an update on April 30, 2021. Reference list of relevant articles were checked for additional titles for inclusion in the review. No limitation was set on the bacteria in animal and human health sectors.

PRISMA flow-chart illustrating the study selection process on antimicrobial resistance in Zambia
Inclusion and exclusion criteria
Full-text articles on the prevalence of antibiotic resistance among clinical pathogenic bacteria isolated from humans (inpatients, outpatients, healthy volunteers), animals (avian, cattle, sheep, swine, and fish) and environment (non-healthcare: water, markets, outbreak studies; and healthcare: hospital surfaces, health care tools,) in Zambia were used for the review. Publications were initially screened independently by three reviewers (AAN, NNT, OYM) to determine eligibility. Articles were reviewed by at least two reviewers and disagreements were resolved by a third author. Studies related to human sector included both adult and pediatric populations, inpatients and outpatients, and healthy volunteers in institutions such as prisons and schools. There were no limitations on the disease or microorganism tested. Publications identified through the literature search that reported AMR in human, animal, and environment but that did not report prevalence data were not included; specific site of genetic mutations resulting in AMR were not included. Studies that mentioned insecticide resistance, assessed the quality of the drug (drug composition, generic compounds and imported medications compared to local medications) were excluded as the studies did not mention resistance rates. Studies that tested the most appropriate diagnostic testing tools were excluded. Studies that made mention of compliance of chronic medicines such as in HIV, and treatment failures were rejected. Any publication that did not report data on AMR were considered not relevant and were excluded.
Data extraction
Data was extracted from each study using a database developed by AAN for the purpose of this review using Microsoft Office 365: Excel. The data extraction was independently done by AAN and verified by co-authors NNT and OYM. Articles that met the inclusion criteria and reported prevalence data for AMR were included in the systematic review.
Information extracted included article information (first author, year of publication, duration of study, location, and specific sites), and study design (samples size, cross-sectional design, or longitudinal study). The specific information extracted for the human sector considered: category of patients (in- or out-patients, healthy persons and reason admitted if inpatient), and type of samples extracted (pus, blood, throat swabs, stool, nasal swabs, urine, vaginal or wound swabs). Regarding the animal sector: species, number of sites (including farms, sanctuaries, and veterinary sites), number of animals sampled in analysis, sample type (feces, meat, milk, blood), sampling point (farm, slaughterhouse, or retail market) were extracted. The environmental/agricultural sector included information of interest such as water, outbreak studies, vegetables, markets, clinic/hospital surfaces and medical tools were considered. Articles that studied more than one sector were classified as a One Health paper and extracted to the subsections mentioned above. The type of organism, organism numbers, antibiotics tested, and interpretation of the findings was extracted into each of the abovementioned category. The samples that were studied had to have undergone a laboratory procedure in which the type of microorganism was identified, and prevalence of antibiotic-resistant bacteria was taken into consideration for the human, animal, and environment articles. Specific site of genetic mutations was noted, highlighting the degree of resistance a microorganism has, however the specific sites were not included in this systematic review.
Data analysis
Articles were characterized based on Zambia as a geographic location (including the region and specific site if this information was available; if the study included other countries, specific information regarding Zambia was extracted if available), the type of antimicrobial resistance described in the study (antibacterial, antiviral, antifungal or antimalarial), context of the study (human, animal or environmental; or a combination of any of the sectors i.e. One Health), study design, and outcome of the studies (specifically prevalence rate of antimicrobial resistance). Meta-analysis was not conducted due to the diversity of the study types and identified data, and therefore present descriptive findings. Visualizations were performed using Microsoft Office 365.
Results
Data
The initial search of the online databases identified a total of 994 publications (PubMed (n = 234), Cochrane Libraries (n = 376), African Journals Online (AJOL) (n = 377) and Medical Journal of Zambia (MJZ) (n = 7)) from inception of database to April 2021. A total of 5 duplicates were removed. Additional 4 records were retrieved after screening references. The African Journals Online identified 377 studies, of which only 100 articles were accessible from the database due to an internal error within AJOLs system. A total of 716 studies were screened for eligibility based on the title and abstract contents. Overall, 614 articles were excluded for non-relevance to this systematic review. 102 full-text articles were assessed for eligibility with 25 articles meeting the inclusion criteria for the study (Fig. 1). Table 1 summarizes the characteristics of the analyzed articles; a full list of the included articles and breakdown of findings is provided in Table 2 and further details of specific antimicrobial results is found in Additional file 1/Supplementary Data.
Study characteristics
A total of 18 studies reported on the outcome of AMR in humans, two reported on the outcome of AMR in animals and two on the environment (Table 1a). Three studies used a One Health approach; with one study reporting outcomes of AMR in both human and animal sectors, while one study reporting on the outcome of AMR in animals and environmental sectors, one study reflected on the outcomes of AMR within the human and environmental sector (Table 1a and Table 2). Across the sectors, 21 (84%) of studies were focused on antibacterial, with 5 studies specific for antitubercular drugs, and 3 studies focused on antiretrovirals. The antimicrobials that underwent surveillance were antibiotics (antibiotic classes were aminoglycosides, cephalosporins, penicillin, sulfonamides, fluoroquinolones, macrolides, tetracyclines, chloramphenicol and glycopeptides), antivirals (nucleoside reverse transcriptase inhibitors (NRTI), non-nucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs). Only one paper reported data on antimalarials. No antifungals were surveilled. All the studies relayed information about surveillance, highlighting zero studies on policy making.
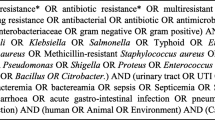
The largest number of studies originated from Lusaka Province (n = 12), followed by Copperbelt Province (n = 6), Western Province (n = 2), Southern Province (n = 1), Eastern Province (n = 1), while three studies mentioned multiple sites within the regions of the country (Fig. 2.) however, it was noted that several provinces had no studies conducted. From these studies, there were multiple samples taken, and multiple microorganisms sampled and tested (Table 2). These studies investigated isolates from diarrheal diseases (2; 10%), breast abscesses (1; 5%), chronic supportive otitis media (1; 5%), hospital acquired infections (1; 5%), malaria (1; 5%), neonatal sepsis (1; 5%), typhoid (1; 5%), HIV (4; 20%), and tuberculosis (4, 25%) (Table 1b). Overall, 27 samples were reported from the human and animal studies, the most abundant being blood (7; 26%) followed by sputum samples (5; 19%), stool samples (4; 15%), wound swabs (4; 15%), nasal swabs (2; 7%), aspirates (1; 4%), rectal swabs (1; 4%), urine samples (1; 4%) and oral swabs (2; 7%) (Table 1c) Two animal studies did not provide the source of samples for culture. Samples from the environmental sector were obtained from fish markets, veterinary hospital surfaces, healthcare white coats and the hydrotherapy bathtub of the burns unit at the Department of Surgery (Table 2). Twenty-one types of pathogens across all sectors were isolated from samples with the most common organisms isolated being Staphylococcus aureus (13; 17%) followed by Escherichia coli (11; 14%), Klebsiella species (7; 9%), Mycobacterium tuberculosis (5; 7%), Proteus species (4; 5%), Streptococcus species (4; 5%), Pseudomonas species (4, 5%), Enterobacter species (4; 5%), Coliform (3; 4%), Shigella species (3; 4%), coagulase negative Staphylococci (3; 4%), HIV (3; 4%), Vibrio cholerae (2; 3%), Salmonella Typhi (2; 3%), Salmonella paratyphi B (1; 1%), Non-Typhoidal Salmonella (NTS) (1; 1%), Citrobacter species (1; 1%), Yersinia species (1; 1%), Plasmodium falciparum (1; 1%), Campylobacter jejuni (1; 1%) and Staphylococcus pseudointermedius (2; 3%) as summarized in Fig. 3 and detailed in Table 2. The susceptibility of these isolates towards 36 antimicrobial agents across 13 classes of antibiotics was tested.

Map of Zambia showing study sites and number of articles used in the review

Microorganisms isolated across human, animal, and environmental sectors in Zambia
The animal, environmental and One Health studies focused on bacterial pathogens and resistance patterns. The most found pathogens isolated were E. coli and S. aureus. Salmonella was only studied in the human sector. The 25 included studies focused on resistance profiles of microbes. No articles included described the process or outcomes of AMR stewardship programs at a local level or focused on policy aspects of AMR prevention or management. No studies were conducted that relayed information about antifungal resistance.
Discussion
Antimicrobial Resistance has been highlighted by the World Health Organization (WHO) as a global health threat that needs urgent intervention [13, 41]. Zambia has a National Action Plan (NAP), aimed to have been implemented by 2020 [10], however the effects of these interventions may be inaccurate without a baseline investigation. As an LMIC, there are multiple challenges Zambia must overcome, such as the unavailability of diagnostic tests, lack of microbiologists at teaching hospitals, lack of reagents or inadequate equipment within hospitals and laboratories. Availability of routine and research data on antimicrobial resistance is an important step in the development of local strategies to curb the global AMR crisis [42]. The One Health approach is a progressive development of multi-disciplinary action across the human health sector with animal and environmental health [43]. A report was developed by the ZNHPI and the CSE India highlighting the need to prepare a surveillance system for Zambia [10]. An integrated baseline using information collected from secondary research was developed with the hope to accurately implement a NAP. The report mentions commonly used antimicrobials, disease burdens and estimates the trends of AMR from secondary studies conducted in Zambia [10].
This current review describes published data on antimicrobial drug resistance from Zambia, revealing a high rate of resistance of microorganisms isolated in hospital settings, animal health and environment against typical antibiotics used in Zambia. Lusaka province had majority of the studies, with various provinces having no data on AMR, indicative that more AMR data is needed for several provinces to have a more complete understanding of the status of AMR in the country. A possible explanation for why studies are conducted in Lusaka could be because Lusaka has the highest population density, with the biggest of the teaching hospitals in Zambia located in this province. There are more resources, more sites, and greater ease to collaborate in a One Health approach in Lusaka, compared to the smaller, distanced cities in Zambia. A couple of articles mentioned Zambia in a multi-country study, however in these cases, the specific region or location of the study or sample collection was rarely mentioned, resulting in limitations of the study in findings specific to the Zambian context. A 2017 systematic review reported that about 42% of African countries do not have published studies on AMR [44], and the lack of information available in Zambia is evident. Many LMICs, such as Zambia, are resource limited. The allocation of resources is crucial hence an up-to-date baseline is needed to develop, coordinate and apply surveillance systems at all levels [10].
Many studies in sub-Saharan Africa focus on antibacterial resistance with few studies on antivirals and antifungals. Countries with high prevalence of HIV, TB and malaria had high numbers of studies on these diseases [10]; this does not align with our observations from Zambia. Despite Zambia having an HIV epidemic, only four studies made mention of HIV, with one study testing the resistance to opportunistic infections in HIV patients: S. pneumoniae. HIV prevalence in Zambia was estimated 11.3% among adults ages 15 to 49 as of 2018 [45]. This represents a substantial burden of disease, and it was surprising to identify only three studies focusing on prevalence to antiretroviral resistance in Zambia: particularly because of the emerging resistance to antiretroviral regimens across Africa [46]. Zambia has a high prevalence of tuberculosis with 455/100,000 cases recorded in a study in 2019 [47]. Despite the tuberculosis epidemic, only five studies showed specific resistance to antitubercular drugs. The detection of M. bovis in Zambia and LMICs is limited due to poor laboratory facilities and lack of trained personnel [47]. Bovine tuberculosis (BTB) has been reported in traditional cattle in Zambia, with a high prevalence of 49.8% within the Kafue basin region; while abattoirs in Namwala district found that 16.8% of cattle slaughtered were infected with BTB [47]. The spill-over effect from the animal sector to the human sector has not yet been established in Zambia. A recent study found that there is a need for routine laboratory surveillance and better case managements to prevent and limit multidrug resistant TB in Zamia [48]. In Copperbelt Province, Zambia, Monde et al. [48] shows that there is emergence of Mycobacterium tuberculosis complex which are resistant to one or more anti-tuberculosis drugs.
Most studies on AMR in Zambia focused on resistance in the human sector, with a handful of studies in the animal and environmental sectors, despite the known importance of the interconnectedness of all three sectors and the vital role they play in preventing and mitigating AMR. The One Health approach should assist and encourage future researchers to consider the methodologies that explicitly look at the interlink across human-animal-environment frameworks, specifically focusing on the zoonotic diseases that have the high potential of resulting in resistance to antimicrobials. With only three studies focusing on multiple sectors, yet these studies are on microorganisms that are not epidemiological microorganisms, it was noted that there are not enough studies using the ‘One Health’ approach in Zambia. More studies highlighting the spill-over effect will be needed to establish a better overview and a better way to combat AMR in Zambia. Understanding these elements and addressing them from the ground-level is necessary to change the modifiable interactions to reduce or interrupt the spread of resistance from the environment into clinical, and animal settings; and vice versa (Fig. 4). Figure 4 shows the relationship between the sectors, and the importance of recognizing this collaboration.

One Health approach to antimicrobial resistance
Numerous studies found resistance of more than 50% suggesting high resistance or possible sampling/testing errors. It was observed that studies are diverse in samples type, study design and identified data and no standardized tool was used across the studies. Antibiograms were not found in the systematic review, and the most recent antibiogram found in a ZNHPI report was from 2016 for only one hospital [10]. Recent communication with the laboratory mentioned a shortage of reagents hence the main third level hospital cannot conduct yearly antibiograms, as recommended by the Clinical and Laboratory Standards Institute (CLSI) [49].
Several studies showed a 100% resistance to commonly prescribed drugs in Zambia, as well as multidrug resistance amongst clinical isolates. This review highlights concerns relating to the use of common antimicrobials as the choice for optimal therapy of common pathogens in Zambia. Our study highlights concern regarding second-line treatment options, such as azithromycin for cholera, in the country have also been highlighted by this study. However, the high rate of antimicrobial resistance does bring into question the testing methods and accuracy of the testing in Zambia as there may have been sample contaminations at certain studies since there were a variety of contradicting results, as seen with penicillin, cephalosporins, monobactams, and carbapenems use for S. aureus ranging from 0% resistance to 100% resistance for second line antibiotics (gentamicin, ceftazidime, nalidixic acid and norfloxacin). Similarly, it was noted that resistance has emerged and been detected for K. pneumonia and E. coli. The results vary widely, however majority shows resistance greater than 50% for both these organisms. These findings demonstrate antibiotic resistance, regardless of testing method, site, year and region, to new and extended spectrum, more efficacious antibiotics.
The most common pathogen identified across the human-animal-environmental sectors was S. aureus. S. aureus is frequently found on the human skin and is recognized as the main contributor of infections in humans [50]. There are high rates of AMR to gentamycin, ceftazidime, amoxicillin-clavulanic acid, cotrimoxazole, nalidixic acid, norfloxacin and oxacillin found in this study. Gentamycin, ceftazidime (third generation cephalosporin) and the fluoroquinolones (nalidixic acid and norfloxacin) are considered second line for Staphylococcus spp. This finding is a serious concern as we see a prominent resistance rate across multiple studies.
Special consideration needs to be addressed in Zambia regarding the surveillance techniques across the several regions. It is imperative to include rural and urban informal settlements, as well as community studies. To prevent an AMR pandemic, it is important to establish surveillance systems that also address and incorporate investigations into the knowledge, attitudes and practices across the human, animal and environmental sectors. It is also recommended to establish systems to map antimicrobial use, resistance profiles and genetics. No known system to address AMR mapping is in place in Zambia at the time of this review. Studies on antifungals, a group that is neglected, should be considered a field of interest. Researchers should be encouraged to collaborate within the human-animal-environmental sectors and conduct studies from a One Health perspective; as well as establish appropriate means to ensure a system can be in place to potentiate future studies on AMR in Zambia.
Our research is one of the first systematic reviews to assess antimicrobial resistance in Zambia. Our results provide critical information that can be used towards policy development and patient management. The different sectors should be more involved and share information to ensure that there is a holistic approach when it comes to combatting AMR.
Conclusion
To safeguard our current collection of antibiotics it is imperative to address the gaps in AMR diagnostic standardization and reporting; and improve surveillance, stewardship, infection control, and implementations of updated treatment guidelines and monitoring. Overall, this review suggests that improved standardization of antimicrobial susceptibility testing in Zambia could help to better delineate AMR patterns and allow comparisons across different locations and allow tracking of AMR evolution over time.
The findings further emphasize the need to address and implement effective AMR surveillance through continued data sharing, multidisciplinary collaborations, and coordination of all stakeholders—using the One Health Approach. This is essential to understand and manage the AMR national burden especially in Zambia.
Availability of data and materials
The data and materials of the study will be available from the corresponding author on reasonable request.
Abbreviations
- AJOL:
-
African Journals Online
- AMR:
-
Antimicrobial Resistance
- BTB:
-
Bovine tuberculosis
- CLSI:
-
Clinical and Laboratory Standards Institute
- CSE:
-
Centre for Science and Environment
- LMIC:
-
Low-middle income countries
- MJZ:
-
Medical Journal of Zambia
- NAP:
-
National Action Plan
- NRTI:
-
Nucleoside reverse transcriptase inhibitors
- NNRTI:
-
Non-nucleoside reverse transcriptase inhibitors
- PI:
-
Protease inhibitors
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analysis
- WHO:
-
World Health Organization
- ZNHPI:
-
Zambian National Public Health Institute
References
WHO. AMR and Covid-19. World Health Organization. 2020 [cited 2021 Feb 28]. Available from: https://www.euro.who.int/__data/assets/pdf_file/0004/441751/COVID-19-AMR.pdf.
Iskandar K, Molinier L, Hallit S, Sartelli M, Hardcastle TC, Haque M, et al. Surveillance of antimicrobial resistance in low- and middle-income countries: a scattered picture. Antimicrob Resist Infect Control. 2021;10(1):1–19. https://doi.org/10.1186/s13756-021-00931-w.
Caudell MA, Dorado-Garcia A, Eckford S, Creese C, Byarugaba DK, Afakye K, et al. Towards a bottom-up understanding of antimicrobial use and resistance on the farm: a knowledge, attitudes, and practices survey across livestock systems in five African countries. PLoS ONE. 2020;15(1):e0220274. https://doi.org/10.1371/journal.pone.0220274.
Murray CJ, Ikuta KS, Sharara F, Swetschinski L, Robles Aguilar G, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–55.
Haque M, Rahman NAA, McKimm J, Sartelli M, Kibria GM, Islam MZ, et al. Antibiotic use: a cross-sectional study evaluating the understanding, usage and perspectives of medical students and pathfinders of a public defence university in Malaysia. Antibiotics. 2019;8(3):154. https://doi.org/10.3390/antibiotics8030154
Gilbert M, Pullano G, Pinotti F, Valdano E, Poletto C, Boëlle PY, et al. Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. Lancet. 2020;395(10227):871–7.
Mackenzie JS, Jeggo M. The One Health approach—Why is it so important? Trop Med Infect Dis. 2019;4(2). Available from: /pmc/articles/PMC6630404/.
McEwen SA, Collignon PJ. Antimicrobial Resistance: a One Health perspective. In: Antimicrobial resistance in bacteria from livestock and companion animals [Internet]. American Society of Microbiology; 2018 [cited 2021 Jun 26]. pp. 521–47. Available from: https://pubmed.ncbi.nlm.nih.gov/29600770/.
WHO. WHO, FAO, and OIE Unite in the Fight Antimicrobial Resistance. 2021. Available from: https://www.who.int/foodsafety/areas_work/antimicrobial-resistance/amr_tripartite_flyer.pdf?ua=1.
Zambia National Public Health Institute. Baseline information for integrated antimicrobial resistance surveillance in Zambia; 2020.
Zamstats. Zambia 2020 Census. 2020. Available from: https://census.zamstats.gov.zm/.
Pearson M, Doble H-R, Nabila S, Reynolds C, Chandler C. Antibiotic prescribing and resistance: views from low-and middle-income prescribing and dispensing professionals Report to the World Health Organization, researched and compiled by students and staff of the Antimicrobial Resistance Centre at the London Sc [Internet]. London; 2017 [cited 2021 Mar 3]. Available from: http://www.who.int/antimicrobial-resistance/LSHTM-.
WHO. WHO|Global action plan on antimicrobial resistance. WHO [Internet]. 2017 [cited 2021 Feb 28]; Available from: http://www.who.int/antimicrobial-resistance/publications/global-action-plan/en/
Borek AJ, Wanat M, Sallis A, Ashiru-Oredope D, Atkins L, Beech E, et al. How can national antimicrobial stewardship interventions in primary care be improved? A stakeholder consultation. Antibiotics. 2019;8(4):207.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11. https://doi.org/10.1186/s13643-021-01626-4.
Kapatamoyo B, Andrews B, Bowa K. Association of HIV with breast abscess and altered microbial susceptibility patterns. Med J Zambia. 2010;37:58–63.
Mwape K, Kwenda G, Kalonda A, et al. Characterisation of Vibrio cholerae isolates from the 2009, 2010 and 2016 cholera outbreaks in Lusaka province, Zambia. Pan Afr Med J. 2020;35:1–10.
Matundwelo N, Mwansasu CS. Bacteriology of chronic suppurative otitis media among children at the arthur davidson children’s hospital, Ndola, Zambia. Med J Zambia. 2016;43(1):36–40.
Mainda G, Bessell PR, Muma JB, et al. Prevalence and patterns of antimicrobial resistance among Escherichia coli isolated from Zambian dairy cattle across difference production systems. Nature. 2015. https://doi.org/10.1038/srep12439.
Mainda G, Lupolova N, Sikakwa L, et al. Whole Genome sequence analysis reveals lower diversity and frequency of acquired antimicrobial resistance (AMR) genes in E. coli from dairy hers compared with human isolates from the same Region of Central Zambia. Front Microbiol 2019;1–10.36.
Chiyangi H, Muma JB, Malama S, et al. Identification and antimicrobial resistance patterns of bacterial enteropathogens from children aged 0–59 months at the University Teaching Hospital, Lusaka, Zambia: a prospective cross sectional study. BMC Infect Dis. 2017;17:1–9.
Gill CJ, Mwanakasale V, Fox MP, Chilengi R, Tembo M, Nsofwa M, et al. Effect of presumptive co-trimoxazole prophylaxis on pneumococcal colonization rates, seroepidemiology and antibiotic resistance in Zambian infants: a longitudinal cohort study. Bull World Health Organ. 2008;86(12):929–38.
Bennett SJ, Chunda-Liyoka C, Poppe LK, et al. High nonnucleoside reverse transcriptase inhibitor resistance levels in HIV-1-infected Zambian mother-infant pairs. AIDS. 2020;34:1833–42.
Inzaule SC, Jordan MR, Cournil A, et al. Tenofovir resistance in early and long-term treated patients on first-line antiretroviral therapy in eight low-income and middle-income countries. AIDS. 2020;34:1965–9.
Miti S, Handema R, Mulenga L, et al. Prevalence and characteristics of HIV drug resistance among antiretroviral treatment (ART) experienced adolescents and young adults living with HIV in Ndola, Zambia. PLoS ONE. 2020;15:1–15.
Chanda W, Manyepa M, Chikwanda E, et al. Evaluation of antibiotic susceptibility patterns of pathogens isolated from routine laboratory specimens at Ndola Teaching Hospital: a retrospective study. PLoS ONE. 2019;14(12):1–14.
Bijl HM, Koetsier DW, van der Werf TS. Chloroquine- and sulfadoxine-pyrimethamine-resistant falciparum malaria in vivo– a pilot study in rural Zambia. Trop Med Int Heal. 2000;5:692–5.
Kabwe M, Tembo J, Chilukutu L, Chilufya M, Ngulube F, Lukwesa C, Kapasa M, Enne V, Wexner H, Mwananyanda L, Hamer DH, Sinyangwe S, Ahmed Y, Klein N, Maeurer M, Zumla A, Bates M. Etiology antibiotic resistance and risk factors for neonatal sepsis in a large referral center in zambia. Pediatr Infect Dis J. 2016;35(7):e191–8. https://doi.org/10.1097/INF.0000000000001154.
Ziwa M, Jovic G, Ngwisha CLT, et al. Common hydrotherapy practices and the prevalence of burn wound bacterial colonisation at the University Teaching Hospital in Lusaka, Zambia. Burns. 2019;45:983–9.
Nagelkerke MMB, Sikwewa K, Makowa D, et al. Prevalence of antimicrobial drug resistant bacteria carried by in- and outpatients attending a secondary care hospital in Zambia. BMC Res Notes. 2017;10:1–6.
Mulenga C, Chonde A, Bwalya IC, et al. Low occurrence of tuberculosis drug resistance among pulmonary tuberculosis patients from an urban setting, with a long-running DOTS program in Zambia. Tuberc Res Treat. 2010;2010:1–6.
Habeenzu C, Mitarai S, Lubasi D, et al. Tuberculosis and multidrug resistance in Zambian prisons, 2000–2001. Int J Tuberc Lung Dis. 2007;11:1216–20.
Kapata N, Chanda-Kapata P, Bates M, et al. Multidrug-resistant TB in Zambia: review of national data from 2000 to 2011. Trop Med Int Health. 2013;18:1386–91.
Kapata N, Mbulo G, Cobelens F, et al. The second Zambian national tuberculosis drug resistance survey - a comparison of conventional and molecular methods. Trop Med Int Health. 2015;20(11):1492–500.
Masenga SK, Mubila H, Hamooya BM. Rifampicin resistance in mycobacterium tuberculosis patients using GeneXpert at Livingstone Central Hospital for the year 2015: a cross sectional explorative study. BMC Infect Dis 2017;640.
Hendriksen RS, Leekitcharoenphon P, Lukjancenko O, et al. Genomic signature of multidrug-resistant salmonella enterica serovar Typhi isolates related to a massive outbreak in Zambia between 2010 and 2012. J Clin Microbiol. 2015;53:262–72.
Youn JH, Park YH, Hang’ombe B, et al. Prevalence and characterization of Staphylococcus aureus and Staphylococcus pseudintermedius isolated from companion animals and environment in the veterinary teaching hospital in Zambia, Africa. Comp Immunol Microbiol Infect Dis. 2014;37:123–30.
Songe MM, Hang’ombe B, Knight-Jones TJD, et al. Antimicrobial resistant enteropathogenic Escherichia coli and Salmonella spp. in houseflies infesting fish in food markets in Zambia. Int J Environ Res Public Health. 2016. https://doi.org/10.3390/ijerph14010021.
Mwamungule S, Chimana HM, Malama S, et al. Contamination of health care workers’ coats at the University Teaching Hospital in Lusaka, Zambia: the nosocomial risk. J Occup Med Toxicol. 2015;10:1–7.
Schaumburg F, Mugisha L, Peck B, et al. Drug-resistant human staphylococcus aureus in sanctuary apes pose a threat to endangered wild ape populations. Am J Primatol. 2012;74:1071–5.
Mayor S. First WHO antimicrobial surveillance data reveal high levels of resistance globally. BMJ. 2018;360:k462.
Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309.
Collignon PJ, McEwen SA. One Health-its importance in helping to better control antimicrobial resistance. Trop Med Infect Dis [Internet]. 2019 Jan 29 [cited 2021 Jun 26];4(1). Available from: http://www.ncbi.nlm.nih.gov/pubmed/30700019.
Tadesse BT, Ashley EA, Ongarello S, Havumaki J, Wijegoonewardena M, González IJ, et al. Antimicrobial resistance in Africa: a systematic review. BMC Infect Dis. 2017;17(1):1–17.
UNICEF. UNICEF Zambia Statistics [Internet]. UNICEF. 2018 [cited 2021 Jul 7]. Available from: https://www.unicef.org/zambia/hivaids.
Moreno M, Caballero E, Mateus RM, Samba F, Gil E, Falcó V. HIV drug resistance in Africa: an emerging problem that deserves urgent attention. AIDS. 2017;31(11):1637–9.
Mutembo S, Mutanga JN, Musokotwane K, Kanene C, Dobbin K, Yao X, et al. Urban-rural disparities in treatment outcomes among recurrent TB cases in Southern Province, Zambia. BMC Infect Dis. 2019;19(1):1–8. https://doi.org/10.1186/s12879-019-4709-5.
Monde N, Zulu M, Tembo M, Handema R, Munyeme M, Malama S. Drug resistant tuberculosis in the Northern Region of Zambia: a retrospective study. Front Trop Dis. 2021;3:36.
Joshi S. Hospital antibiogram: a necessity. Indian J Med Microbiol. 2010;28(4):277–80.
Otto M. Staphylococcus colonization of the skin and antimicrobial peptides. Expert Rev Dermatol. 2010;5(2):183.
Acknowledgements
The authors would like to thank Dr Seth Bloom for critical review at work in progress meetings. The Pan-African Organization for Health, Education and Research (POHER) for the support for the duration of the study.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
AAN, AWA and LRS conceived the idea. AAN prepared the systematic review protocol and was involved in the literature search, screening, extraction of data, data analysis and developed the drafts of the manuscript. OYM and NNT performed the screening, extraction of data and developed the first draft of the manuscript. LRS and AWA provided critical review of the manuscript and contributed to the final version. All the authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1:
Detailed findings of antimicrobial resistance rates across the studies included.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nowbuth, A.A., Asombang, A.W., Tazinkeng, N.N. et al. Antimicrobial resistance from a One Health perspective in Zambia: a systematic review. Antimicrob Resist Infect Control 12, 15 (2023). https://doi.org/10.1186/s13756-023-01224-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13756-023-01224-0