
Abstract
Background
Pain is highly burdensome, affecting over 30% of long-term care (LTC) residents. Pain significantly reduces residents’ health-related quality of life (HRQoL), limits their ability to perform activities of daily living (ADLs), restricts their social activities, and can lead to hopelessness, depression, and unnecessary healthcare costs. Although pain can generally be prevented or treated, eliminating pain may not always be possible, especially when residents have multiple chronic conditions. Therefore, improving the HRQoL of LTC residents with pain is a priority goal. Understanding factors influencing HRQoL of LTC residents with pain is imperative to designing and evaluating targeted interventions that complement pain management to improve residents’ HRQoL. However, these factors are poorly understood, and we lack syntheses of available research on this topic. This systematic review protocol outlines the methods to identify, synthesize, and evaluate the available evidence on these factors.
Methods
This mixed methods review will follow the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. We will systematically search Medline, EMBASE, PsycINFO, CINAHL, Scopus, Cochrane Database of Systematic Reviews and ProQuest Dissertation and Thesis Global from database inception. We will include primary studies and systematically conducted reviews without restrictions to language, publication date, and study design. We will also include gray literature (dissertation and reports) and search relevant reviews and reference lists of all included studies. Two reviewers will independently screen articles, conduct quality appraisal, and extract data. We will synthesize results thematically and conduct meta-analyses if statistical pooling is possible. Residents and family/friend caregivers will assist with interpreting the findings.
Discussion
This proposed systematic review will address an important knowledge gap related to the available evidence on factors influencing HRQoL of LTC residents with pain. Findings will be crucial for researchers, LTC administrators, and policy makers in uncovering research needs and in planning, developing, and evaluating strategies in addition to and complementary with pain management to help improve HRQoL among LTC residents with pain.
Systematic review registration
PROSPERO CRD42023405425
Similar content being viewed by others


Background
Growth in the number of older adults is a global phenomenon [1,2,3]. Along with the population’s increasing age, the numbers of older adults with multiple chronic illnesses [4,5,6] and complex care needs are also rising, substantially increasing the need for residential long-term care (LTC) [7, 8]. LTC provides accommodation to people requiring on-site access to supervised care around the clock, including professional health care services, personal care, and services such as meals, laundry, and housekeeping [9]. More than 50% of LTC residents are 85 years and older, 70% are female, 90% are cognitively impaired, and 80% need assistance with activities of daily living (ADLs) [10, 11]. Many LTC residents suffer from multiple chronic conditions (an average of six chronic conditions) [12], including arthritis, osteoporosis, depression, hypertension, and dementia [13,14,15]. Chronic conditions increase the risk for pain in LTC residents [12, 16, 17]—a common and burdensome condition [18, 19].
Pain is “an unpleasant sensory and emotional experience associated with, or resembling that of actual or potential tissue damage” [20] (p.2). Internationally, pain prevalence estimates among LTC residents vary widely between 31 and 70% [13, 21,22,23]. Given that pain can generally be prevented or treated, these rates are unacceptably high [18, 19]. Pain severely impacts residents’ health-related quality of life (HRQoL) [24]. It impairs residents’ mobility and independence [25, 26] and contributes to hopelessness, insomnia, loneliness, depression, poor social relationships, and unnecessary health care costs [24, 27, 28]. However, even when applying best practices in pain management [29,30,31], eliminating pain is not always possible, especially when residents have multiple comorbidities [12, 32, 33]. Therefore, for residents living with pain, in addition to treating their pain as best as possible, preserving their functional abilities, and supporting their best possible HRQoL is a priority goal [34, 35]. HRQoL reflects those aspects of QoL that directly or indirectly relate to an individual’s perception of the impact a health condition, illness, or treatment has on their life [36, 37]. Recognizing that many factors influence LTC residents’ HRQoL [38,39,40], we define factors for this review as any condition influencing the HRQoL of residents experiencing pain [41]. These conditions include (1) resident characteristics [40, 42, 43], (2) socio-economic aspects [39, 44, 45], and (3) LTC facility characteristics [46,47,48]. Studies suggest that younger residents [49], female [38, 50], married [49], and financially secure [51, 52] reported better QoL. Residents who are dependent on with ADLs [40, 46], who experience pain [24, 40], have anxiety/mood disorders [49] and depression [38, 46], and who are cognitively impaired [38, 40, 50] have reduced QoL. Evidence also suggests that residents can maintain high QoL despite co-morbid health conditions, including dementia [39, 53], pain [38, 54], and diminished physical and cognitive functioning [38, 54]. Internal personal resources, such as resilience [45], meaning or purpose in life [55], sense of coherence [56, 57], and religiosity/spirituality [40, 46] effectively helped residents to cope with health and life adversities (including pain). Similarly, residents who perceived better support from family/friends and LTC staff in terms of their availability, attachment, and quality of relationship had a better HRQoL [39, 56].
Past reviews mainly focused on factors influencing the QoL of LTC residents in general or those with dementia [40, 42, 43]. However, to the best of our knowledge, no literature synthesis is available on factors that explain variation in HRQoL among LTC residents with pain. Since the best possible HRQoL is a priority goal of care for all LTC residents, especially among those whose pain cannot be removed entirely, we must understand what helps residents with pain to achieve the best possible HRQoL [58, 59]. Identifying these factors is fundamental for planning and developing targeted interventions—in addition and complementary to best practices in pain management—to support LTC residents with pain in maintaining or improving HRQoL. This systematic review protocol details the methods we will use to identify factors that influence HRQoL among LTC residents with pain. We aim to identify, evaluate, and synthesize the available research evidence on the factors that are associated with HRQoL of LTC residents experiencing pain. Our research questions are: (1) what factors associated with HRQoL of LTC residents experiencing pain do studies report? (2) What is the magnitude, direction, and strength of evidence of each factor’s association with HRQoL of LTC residents experiencing pain?
Methods/design
Review design
We will conduct a systematic mixed methods synthesis of research [60]. This paper follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) checklist (see Additional file 1) [61]. We will follow the procedures outlined in the Cochrane Handbook of Systematic Reviews [62] and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [63] for review methods and reporting of results. The protocol for this systematic review has been registered with the International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42023405425.
Inclusion and exclusion criteria for study selection
Participants
We will include studies that examined LTC residents aged 65 years and older. The average or median age of participants must be at least 65 years. Studies where participants are referred to as aged/elderly/older individuals, seniors, or residents of a continuing care institution will also be included. Studies must have included LTC residents with pain, either acute (lasting less than 3 months) or chronic pain (lasting 3 months or more) [64] assessed using a standardized clinical assessment tools (based on resident self-reports, proxy-reports or clinical assessments/observations). No further limitations on participant characteristics will be applied. Study inclusion will not be limited based on participant sex/gender, race/ethnicity, or any other social identity or demographic feature.
Outcomes
We will include studies that assessed HRQoL as a primary or secondary outcome. In particular, we will include studies if they report the association of factor(s) with the HRQoL of LTC residents who live with pain. The revised version [65] of Wilson’s & Cleary’s health-related quality of life (HRQoL) model and the Consolidated Framework for Implementation Research (CFIR) developed by Damschroder et al. [66] will inform the factors. The Zubrtisky et al. [65] model suggests that resident characteristics (physiological health, emotional health, functional status, general health perceptions, beliefs, and behaviors) and the environment where residents live (service delivery system, structure) shape their HRQoL. While this model includes the environment as one of many factors that influence resident HRQoL, it does not explicitly operationalize this important factor. Therefore, in addition to this model, we will also use the CFIR which will help further operationalize the LTC organizational context (work environment) construct. The CFIR framework defines context or environment as the “set of circumstances or unique factors that surround a particular implementation effort” [66] (p.3). For this review, we will use the CFIR dimension called inner setting to operationalize the construct of organizational context. The inner setting includes structural characteristics, networks and communication, culture, climate, and readiness, which interact with each other to influence implementation [66]. Both frameworks (HRQoL and CFIR) will inform the identification of articles that report factors of interest, theme generation during data extraction and analysis, and interpretation of results. In line with the above theoretical frameworks, factors in this review may include (a) resident factors (physical and cognitive functioning, resilience, coping strategies, optimism, purpose in life); (b) socio-economic factors (social support, social engagement, economic resource); (c) LTC factors (LTC characteristics, care practices, policies, care model, care home organizational context such as leadership, staffing, resources, work culture, evaluation, communication).
Types of studies
We will include primary empirical studies and systematically conducted reviews (i.e., reviews that included comprehensive search strategy, reported inclusion/exclusion criteria, screening process, data extraction and analysis of the included studies) without any restrictions on the language, study design, and publication date. Our study team includes members who can assess the eligibility of studies published in English, French, German, and Nepali language. For studies in other languages, we will utilize our networks of colleagues to identify persons who might be able to help with assessing eligibility, or use Google Translate to assess eligibility. We will include gray literature (dissertations, theses, and reports) identified in the database searches, but we will not systematically search gray literature. In addition to the electronic database search, we will also search the reference lists of all the included studies and relevant reviews. We will exclude non-empirical and non-systematic review studies. We will include studies conducted in LTC also referred to as nursing homes, care homes, and residential aged care facilities [9, 15, 67,68,69] (detailed inclusion and exclusion criteria in Appendix 1).
Search strategy
Assisted by a health sciences librarian (MK), we developed the search strategy (see Appendix 2 for search strategy created for various databases). Search terms were based on four major concepts and their synonyms: (1) older adults (seniors), (2) care location (LTC, nursing homes), (3) pain, and (4) quality of life. We searched the following databases: Medline, Embase, PsycINFO, CINAHL, Scopus, Cochrane Database of Systematic Reviews and ProQuest Dissertations and Theses Global from database inception till date. We will retrieve all studies without limiting language, study design, and publication date. Further we will search the reference lists of all the studies included and relevant reviews.
Data management
Records will be managed, using COVIDENCE systematic review software [70]. Reviewers will receive training on using COVIDENCE prior to screening articles. We will use COVIDENCE for de-duplication, title/abstract screening, full-text screening, and monitoring and reporting of reviewer agreement.
Study screening
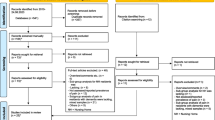
Two reviewers (SS and RD) will screen titles and abstracts of 100 papers independently, followed by a calibration meeting. If the first round demonstrates discrepancies in decisions related to publication type, setting, population, and study focus, we will do additional calibration rounds and reconcile decisions with a third reviewer (MH). Using a similar approach, we will screen the remaining titles and abstracts in batches. We will obtain full texts of all included studies and for those with inadequate information in the title/abstract screening to decide on inclusion. We will screen full texts using the same approach as for the title/abstract screening. Two reviewers (SS and RD) will independently screen reference lists of all included studies and reviews for any additional relevant studies. We will document reasons for each article’s exclusion and the selection process using a PRISMA-ScR flow diagram [61].
Data extraction
We will construct a Google form to directly abstract relevant data. To test useability of the data extraction form (Google form), we will pilot-test it using five randomly selected studies [71]. Two reviewers (SS and RD) will independently extract data from an initial 10% of the studies, followed by a consensus meeting to calibrate extraction. Reviewers will discuss discrepancies and reach a consensus before extracting data from the remaining studies. One reviewer (SS) will extract data for the remaining studies, and another (RD) will double-check the extracted data for accuracy. Data extraction will include (1) surname of the first author, (2) year of publication, (3) the title of study, (4) country of study, (5) study aim(s) or purpose(s), (6) study design, (7) setting and sample, (8) method(s) of data collection, (9) tools and measures used to assess HRQoL and pain (for quantitative studies) or phenomena assessed (qualitative studies), (10) definition of pain, (11) statistical analyses methods used, and (12) main study findings: factors influencing HRQoL of LTC residents with pain.
Risk of bias
Two reviewers will independently assess the methodological quality of all included studies. However, we will not exclude studies based on their quality. Reviewers will meet to reconcile any discrepancies. We will assess the risk of bias using validated and reliable tools depending on the study design of included studies. We will employ the validated and reliable AMSTAR 2 (Assessing the Methodological Quality of Systematic Reviews 2) tool [72, 73] for systematically conducted reviews, Quality Assessment Tool for Quantitative Studies (QATQS) [74,75,76] for quantitative studies (e.g., randomized and non-randomized, cohort and case studies); the Appraisal Tool for Cross-sectional Studies (AXIS) [77] for cross-sectional studies; Critical Appraisal Skills Program (CASP) Qualitative Research Checklist [78] for qualitative studies; and the Mixed Methods Appraisal Tool (MMAT) [79] for mixed-method studies.
We will use the scoring method developed by de Vet et al. [80] to obtain an overall quality rating for each study. de Vet et al.’s method uses the total number of checklist items that are applicable to a study as the denominator and the items that study meet as the numerator. Therefore, for each checklist and assessment, we determine the percentage of items that each study meet. Although each quality appraisal tool/checklist varies in the number of items and criteria applied, they still have in common that ideally a study should meet all required criteria and that meeting a higher number of criteria is considered better study quality. Therefore, de Vet et al.’s method is a form of standardization across checklists. Scoring will provide us with an idea about the study’s methodological quality, which is crucial in informing decision-making based on the quality of evidence [80]. We will calculate the ratio of the obtained score to the maximum possible score, which varies with the checklist used and the number of items in the checklists that apply to the respective study. The score ranges from 0 to 1. Similar to previous studies [81, 82], we will categorize the quality of studies as weak (≤ 0.50), low moderate (0.51–0.66), high moderate (0.67–0.79), or strong (≥ 0.80). In addition, we will also conduct a quality assessment on the item level for each study based on a particular quality appraisal tool.
Data analyses and synthesis
Using tables and figures, we will descriptively present the number and proportion of studies representing each category: number of studies, year of publication, countries of origin, study design, study settings, participants’ details, and quality of studies. We will conduct thematic analysis of all studies. For thematic analysis [83], two independent reviewers will familiarize and inductively code data, look for similarities and differences between the codes, and then group them into similar themes or categories. Acute (pain lasting less than 3 months) and chronic pain (pain lasting 3 months or more) [64] are different. Further, pain may be evaluated using self, proxy, or observation-based assessment tools. Accordingly, factors affecting residents’ HRQoL may be different in residents with acute and chronic pain and in residents assessed using self, proxy, or observation-based pain assessment [28]. Similarly, prior studies have shown that QoL in LTC residents may vary by sex/gender [38], race/ethnicity [49, 84], study country of origin [85], and LTC organizational context [86, 87]. Therefore, we will conduct sub-group analysis to report factors associated with HRQoL by type of pain (acute/chronic), pain assessment methods (self-report, proxy-report, observation), sex/gender, race/ethnicity, study country of origin, and LTC organizational context if we identify enough studies that allow stratification. The HRQoL [65] and CFIR [66] framework will help to categorize themes or factors influencing HRQoL of LTC residents with pain. We will resolve any discrepancies in the process by consensus. After thematic analysis, we will provide a narrative synthesis of results—a textual approach to understanding and reporting findings [88]. We will report the number of studies reporting each of the factors identified.
For qualitative results, we will conduct a content analysis [88]. In this process, we will identify key themes and assess if these key themes vary (if they are similar or different) across studies. We will then categorize themes into either resident, socio-economic, or LTC-related factors as informed by the HRQoL [65] and CFIR [66] framework. For quantitative findings, we will summarize the available quantitative evidence such as effects sizes of correlations, regression parameters, relative risks, or odd ratios. We will report the range of scores, frequency and proportion of studies reporting statistically significant positive associations, statistically significant negative associations, and statistically non-significant associations for association of factors with our study outcome based on vote counting.
If there are a sufficient number of quantitative studies reporting similar designs, settings, and outcomes, then we will statistically pool results of these studies using random effects meta-analysis [62]. Three or more studies are required to estimate measures of heterogeneity in addition to estimating pooled effects for random-effects meta-analysis [89]. For this study, we will conduct statistical pooling, if three or more studies (1) report similar factors associated with residents’ HRQoL, (2) measure HRQoL and pain in a comparable way (i.e., using a comparable measurement tool), (3) report the same resident outcome (HRQoL of LTC residents with pain), and (4) report the same type of statistical outcome. We will calculate the extent of heterogeneity using the I2 [90, 91] and H2 statistic [92] including their 95% confidence intervals [90, 91]. We will use random effects models using the statistical software SPSS (Statistical Package for Social Sciences), version 22 [93]. Random effects models are considered better than fixed-effects models in case of heterogeneity and a small number of studies [94, 95]. We will also assess if study protocols are available for the included studies (particularly randomized controlled trials) and if they were published before recruitment of patients. We will assess publication bias using funnel plots if we are able to include more than ten comparable studies because publication bias is difficult to evaluate among ten or fewer studies due to lack of power [96]. If the studies included in the review are too small in number and are heterogeneous then we will only conduct thematic analysis of the review findings as described above. We will assess the overall quality of the body of evidence using the Grading of Recommendation Assessment, Development and Evaluation guidelines (GRADE) [97]. According to GRADE, quality will be categorized as very low (any estimate of effect is very uncertain), low (further research is very likely to have a significant impact on our confidence in the estimate of effect and is likely to change the estimate), moderate (further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate), and high (further research is very unlikely to change our confidence in the estimate of effect) [97].
Stakeholder consultation
Consultation enhances a review’s relevance by integrating stakeholders’ lived experience, expertise, and perspective [98]. We plan to consult with stakeholders after synthesizing the review findings. Stakeholders will contribute meaningfully in interpreting findings in terms of whether associations reflect their experiences and reality [98]. Using our existing stakeholder networks, we will include four stakeholders as an advisory group: (a) two LTC residents with pain who can verbally express their opinion and (b) two family/friend caregivers. To recruit stakeholders, first, we will purposively select a LTC from our existing network. Second, we will contact care home administrator via email or phone and request them to identify potential stakeholders and get permission for us to contact them directly. We will then approach selected stakeholders, explain the purpose of their involvement, and obtain their verbal consent. We will conduct a semi-structured interview using recorded virtual focus group discussion (lasting about an hour). The analysis will involve theme generation, and we will integrate findings in the result section separately in a narrative form.
Discussion
Given that improving HRQoL is a priority goal in LTC residents living with pain and that there is a lack of synthesis in this topic, we aim to identify, synthesize, and evaluate available evidence on factors that are associated with HRQoL of LTC residents with pain. Identifying factors, particularly those that are modifiable and those that are positively associated with residents’ HRQoL will help us plan, develop, and evaluate tailored strategies to improve residents’ HRQoL. Further, we will be able to identify research gaps on the topic, which can inform future studies. Stakeholders’ involvement will further add credibility to the findings as they will help interpret the findings in terms of whether the associations observed reflect their experiences and reality. The findings will be crucial for researchers, LTC administrators and policymakers.
Availability of data and materials
We will include all data generated or analyzed in the published systematic review article. Upon request, other resources can be made available.
Abbreviations
- LTC:
-
Long-term care
- QoL:
-
Quality of life
- HRQoL:
-
Health-Related Quality of Life
- ADL:
-
Activities of Daily Living
- PRISMA-P:
-
Preferred reporting items for systematic review and meta-analysis protocols
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- AMSTAR 2:
-
Assessing the Methodological Quality of Systematic Reviews 2
- QATQS:
-
Quality Assessment Tool for Quantitative Studies
- AXIS:
-
Appraisal Tool for Cross-sectional Studies
- CASP:
-
Critical Appraisal Skills Program
- MMAT:
-
Mixed Methods Appraisal Tool
- GRADE:
-
Grading of Recommendation Assessment, Development and Evaluation guidelines
References
Age UK. Later life in the United Kingdom 2019 - factsheet. 2019. Available from: https://www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/later_life_uk_factsheet.pdf.
Statistics Canada. Population projections for Canada, provinces and territories. 2009–2036. 2010. Available from: https://www150.statcan.gc.ca/n1/en/pub/91-520-x/91-520-x2010001-eng.pdf?st=PYZyRoJY.
Vespa J, Medina L, Armstrong D. Demographic turning points for the United States: population projections for 2020 to 2060. Current population reports. US. Washington, DC: Census Bureau; 2020. Available from: https://census.gov/programs-surveys/popproj.html.
Rasmussen KL, Tybjarg-Hansen A, Nordestgaard BG, Frikke-Schmidt R. Absolute 10-year risk of dementia by age, sex and APOE genotype: a population-based cohort study. Can Med Assoc J. 2018;190(35):E1033–41.
GBD 2017 Disease and injury incidence and prevalence collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 Diseases and Injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–858.
Salive ME. Multimorbidity in older adults. Epidemiol Rev. 2013;35(1):75–83.
Toot S, Swinson T, Devine M, Challis D, Orrell M. Causes of nursing home placement for older people with dementia: a systematic review and meta-analysis. Int Psychogeriatr. 2017;29(2):195–208.
Kojima G. Frailty as a predictor of nursing home placement among community-dwelling older adults: a systematic review and meta-analysis. J Geriatr Phys Ther. 2018;41(1):42–8.
Government of Canada. Long-term facilities-based care. 2004. Available from: https://www.canada.ca/en/health-canada/services/home-continuing-care/long-term-facilities-based-care.html. Cited 2021 Jan 31.
Canadian Institute for Health Information. Profile of residents in residential and hospital-based continuing care, 2019–2020 – Quick stats. Ottawa; 2020. Available from: https://www.cihi.ca/en/access-data-reports/results?fs3%5B0%5D=primary_theme%3A680.
Canadian Institute for Health Information. Dementia in long-term care. 2019. Available from: https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-long-term-care. Cited 2021 Feb 10.
Moore KL, Boscardin WJ, Steinman MA, Schwartz JB. Patterns of chronic co-morbid medical conditions in older residents in U.S. nursing homes: differences between the sexes and across the agespan. J Nutr Health Aging. 2014;18(4):429–36.
Canadian Institute for Health Information (CIHI). Profile of residents in residential and hospital-based continuing care, 2020–2021. Ottawa; 2021. Available from: https://www.cihi.ca/en/access-data-reports/results?fs3%5B0%5D=primary_theme%3A680.
Gordon AL, Franklin M, Bradshaw L, Logan P, Elliott R, Gladman JRF. Health status of UK care home residents: a cohort study. Age Ageing. 2014;43(1):97–103.
Harris-Kojetin L, Sengupta M, Lendon J, Rome V, Valverde R, Caffrey C. Long-term care providers and service users in the United states, 2015-2016. National Center for Health Statistics. Vital Health Stat. Maryland; 2019. Available from: https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf.
Savvas SM, Gibson SJ. Overview of pain management in older adults. Clin Geriatr Med. 2016;32(4):635–50. https://doi.org/10.1016/j.cger.2016.06.005.
Veal F, Williams M, Bereznicki L, Cummings E, Thompson A, Peterson G, et al. Barriers to optimal pain management in aged care facilities: an Australian qualitative study. Pain Manag Nurs. 2018;19(2):177–85. https://doi.org/10.1016/j.pmn.2017.10.002.
Hoben M, Chamberlain SA, Knopp-Sihota JA, Poss JW, Thompson GN, Estabrooks CA. Impact of symptoms and care practices on nursing home residents at the end of life: a rating by front-line care providers. J Am Med Dir Assoc. 2016;17(2):155–61.
Estabrooks CA, Hoben M, Poss JW, Chamberlain SA, Thompson GN, Silvius JL, et al. Dying in a nursing home: treatable symptom burden and its link to modifiable features of work context. J Am Med Dir Assoc. 2015;16(6):515–20. https://doi.org/10.1016/j.jamda.2015.02.007.
Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. Revised definition of pain by “international association for the study of pain”: concepts, challenges and compromises. Anaesth Pain Intensive Care. 2020;00(00):1–7.
Achterberg WP, Gambassi G, Finne-Soveri H, Liperoti R, Noro A, Frijters DHM, et al. Pain in European long-term care facilities: cross-national study in Finland, Italy and the Netherlands. Pain. 2010;148(1):70–4. https://doi.org/10.1016/j.pain.2009.10.008.
Rajkumar AP, Ballard C, Fossey J, Orrell M, Moniz-Cook E, Woods RT, et al. Epidemiology of pain in people with dementia living in care homes: longitudinal course, prevalence, and treatment implications. J Am Med Dir Assoc. 2017;18:453.e1-453.e6. https://doi.org/10.1016/j.jamda.2017.01.024.
Dube CE, Morrison RA, Mack DS, Jesdale BM, Nunes AP, Liu SH, et al. Prevalence of pain on admission by level of cognitive impairment in nursing homes. J Pain Res. 2020;13:2663–72.
Brandauer A, Berger S, Freywald N, Gnass I, Osterbrink J, Seidenspinner D, et al. Quality of life in nursing home residents with pain: pain interference, depression and multiple pain-related diseases as important determinants. Qual Life Res. 2020;29:91–7.
Husebo BS, Achterberg WP, Lobbezoo F, Kunz M, Lautenbacher S, Kappesser J, et al. Pain in patients with dementia: a review of pain assessment and treatment challenges. Nor Epidemiol. 2012;22(2):243–51.
Ferretti F, Castanha AC, Padoan ER, Lutinski J, da Silva MR. Quality of life in the elderly with and without chronic pain. Braz J Pain. 2018;1(2):111–5.
Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–24. https://doi.org/10.1016/j.jpain.2012.03.009.
Cole CS, Carpenter JS, Chen CX, Blackburn J, Hickman SE. Prevalence and factors associated with pain in nursing home residents: a systematic review of the literature. J Am Med Dir Assoc. 2022;23:1916-25.e1.
Schofield P. The assessment of pain in older people: UK national guidelines. Age Ageing. 2018;47:i1-22.
Registered Nurses’ Association of Ontario (RNAO). Assessment and management of pain, third edition. Clin Best Pract Guidel. 2013;(December):97–9. Available from: http://rnao.ca/sites/rnao-ca/files/AssessAndManagementOfPain_15_WEB-_FINAL_DEC_2.pdf.
The Edith Cowan University. The PMG Kit for Aged Care. The implementation kit to accompany The Australian Pain Society’s pain in residential aged care facilities: management strategies. Sydney; 2007. Available from: https://www.apsoc.org.au/PDF/Publications/PMGKit_2007.pdf.
van Dam PH, Caljouw MAA, Slettebø DD, Achterberg WP, Husebo BS. Quality of life and pain medication use in persons with advanced dementia living in long-term care facilities. J Am Med Dir Assoc. 2019;20(11):1432–7.
Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet. 2011;377:2226–35. https://doi.org/10.1016/S0140-6736(11)60402-9.
Sheikh F, Brandt N, Vinh D, Elon RD. Management of chronic pain in nursing homes: navigating challenges to improve person-centered care. J Am Med Dir Assoc. 2021;22:1199–205. https://doi.org/10.1016/j.jamda.2020.12.029.
Hall T. Management of persistent pain in older people. J Pharm Pract Res. 2016;46(1):60–7.
Guyatt GH, Ferrans CE, Halyard MY, Revicki DA, Symonds TL, Varricchio CG, et al. Exploration of the value of health-related quality-of-life information from clinical research and into clinical practice. Mayo Clin Proc. 2007;82(10):1229–39.
Ferrans CE, Zerwic JJ, Wilbur JE, Larson JL. Conceptual model of health-related quality of life. J Nurs Scholarsh. 2005;37(4):336–42.
Abrahamson K, Lewis T, Perkins A, Clark D, Nazir A, Arling G. The influence of cognitive impairment, special care unit placement, and nursing facility characteristics on resident quality of life. J Aging Health. 2013;25(4):574–88.
O’Rourke HM, Duggleby W, Fraser KD, Jerke L. Factors that affect quality of life from the perspective of people with dementia: a metasynthesis. J Am Geriatr Soc. 2015;63(1):24–38.
Martyr A, Nelis SM, Quinn C, Wu YT, Lamont RA, Henderson C, et al. Living well with dementia: a systematic review and correlational meta-analysis of factors associated with quality of life, well-being and life satisfaction in people with dementia. Psychol Med. 2018;48:2130–3139.
Kane RA. Long-term care and a good quality of life: bringing them closer together. Gerontologist. 2001;41(3):293–304.
Beerens HC, Zwakhalen SMG, Verbeek H, Ruwaard D, Hamers JPH. Factors associated with quality of life of people with dementia in long-term care facilities: a systematic review. Int J Nurs Stud. 2013;50(9):1259–70.
Jing W, Willis R, Feng Z. Factors influencing quality of life of elderly people with dementia and care implications: a systematic review. Arch Gerontol Geriatr. 2016;66:23–41.
Degenholtz HB, Kane RA, Kane RL, Bershadsky B, Kling KC. Predicting nursing facility residents’ quality of life using external indicators. Health Serv Res. 2006;41(2):335–56.
Bradshaw SA, Playford ED, Riazi A. Living well in care homes: a systematic review of qualitative studies. Age Ageing. 2012;41(4):429–40.
Kehyayan V, Hirdes JP, Tyas SL, Stolee P. Predictors of long-term care facility residents’ self-reported quality of life with individual and facility characteristics in Canada. J Aging Health. 2016;28(3):503–29.
Johs-Artisensi JL, Hansen KE, Olson DM. Qualitative analyses of nursing home residents’ quality of life from multiple stakeholders’ perspectives. Qual Life Res. 2020;29:1229–38. https://doi.org/10.1007/s11136-019-02395-3.
Donnelly L, MacEntee MI. Care perceptions among residents of LTC facilities purporting to offer person-centred care. Can J Aging. 2016;35(2):149–60.
Shippee TP, Henning-Smith C, Kane RL, Lewis T. Resident- and facility-level predictors of quality of life in long-term care. Gerontologist. 2015;55(4):643–55.
Cordner Z, Blass DM, Rabins PV, Black BS. Quality of life in nursing home residents with advanced dementia. J Am Geriatr Soc. 2010;58(12):2394–400.
Byrne-Davis LMT, Bennett PD, Wilcock GK. How are quality of life ratings made? Toward a model of quality of life in people with dementia. Qual Life Res. 2006;15(5):855–65.
Chang HT, Liu LF, Chen CK, Hwang SJ, Chen LK, Lu FH. Correlates of institutionalized senior veterans’ quality of life in Taiwan. Health Qual Life Outcomes. 2010;8:1–9.
Farina N, King D, Burgon C, Berwald S, Bustard E, Feeney Y, et al. Disease severity accounts for minimal variance of quality of life in people with dementia and their carers: analyses of cross-sectional data from the MODEM study. BMC Geriatr. 2020;20:1–13.
Kim SJ, Park EC, Kim S, Nakagawa S, Lung J, Choi JB, et al. The association between quality of care and quality of life in long-stay nursing home residents with preserved cognition. J Am Med Dir Assoc. 2014;15(3):220–5.
Haugan G. Meaning-in-life in nursing-home patients: a valuable approach for enhancing psychological and physical well-being? J Clin Nurs. 2013;23(13–14):1830–44.
Drageset J, Eide GE, Nygaard HA, Bondevik M, Nortvedt MW, Natvig GK. The impact of social support and sense of coherence on health-related quality of life among nursing home residents-a questionnaire survey in Bergen, Norway. Int J Nurs Stud. 2009;46(1):66–76.
Drageset J, Nygaard HA, Eide GE, Bondevik M, Nortvedt MW, Natvig GK. Sense of coherence as a resource in relation to health-related quality of life among mentally intact nursing home residents - a questionnaire study. Health Qual Life Outcomes. 2008;6:1–9.
Wong EKC, Thorne T, Estabrooks C, Straus SE. Recommendations from long-term care reports, commissions, and inquiries in Canada. F1000Res. 2021;10:1–10.
Murphy K, Cooney A, Casey D. Improving the quality of life for older people in long-term care settings. J Comp Eff Res. 2014;3(3):301–15.
Harden A. Mixed-methods systematic reviews: integrating quantitative and qualitative findings. Focus (Madison). 2010;2010:1–8. Available from: https://ktdrr.org/ktlibrary/articles_pubs/ncddrwork/focus/focus25/Focus25.pdf.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1–9.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane handbook for systematic reviews of interventions version 6.3. The Cochrane Collaboration; 2022. Available from: https://training.cochrane.org/handbook/current.
Moher D, Liberrati A, Tetzlaff J, Altman DG, the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
International Association for the Study of Pain (IASP). IASP announces revised definition of pain. 2020. Available from: https://www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=10475. Cited 2020 Dec 1.
Zubritsky C, Abbott KM, Hirschman KB, Bowles KH, Foust JB, Naylor MD. Health-related quality of life: expanding a conceptual framework to include older adults who receive long-term services and supports. Gerontologist. 2013;53(2):205–10.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):1–15.
Canadian Institute for Health Information (CIHI). Access data and report. 2020. Available from: https://www.cihi.ca/en/access-data-and-reports.
Office for National Statistics. Changes in the older resident care home population between 2001 and 2011. 2014. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/changesintheolderresidentcarehomepopulationbetween2001and2011/2014-08-01.
Howe AL, Jones AE, Tilse C. What’s in a name? Similarities and differences in international terms and meanings for older peoples’ housing with services. Ageing Soc. 2013;33(4):1–32.
Cochrane Community. About covidence. 2020. Available from: https://community.cochrane.org/help/tools-and-software/covidence/about-covidence. Cited 2020 Jun 7.
Long L. Routine piloting in systematic reviews-a modified approach? Syst Rev. 2014;3(1):1–5.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:1–9.
Lorenz RC, Matthias K, Pieper D, Wegewitz U, Morche J, Nocon M, et al. A psychometric study found AMSTAR 2 to be a valid and moderately reliable appraisal tool. J Clin Epidemiol. 2019;114:133–40. https://doi.org/10.1016/j.jclinepi.2019.05.028.
Armijo-Olivo S, Craig R, Corabian P, Guo B, Souri S, Tjosvold L. Nursing staff time and care quality in long-term care facilities: a systematic review. Gerontologist. 2020;60(3):e200–17.
Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. 2004;1(3):176–84. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17163895.
Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: methodological research. J Eval Clin Pract. 2012;18(1):12–8.
Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6(12):1–7.
Critical Apprasisal Skills Programme. CASP (qualitative) checklist. Lecture notes in mechanical engineering. 2018. p. 1–6. Available from: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf.
Pluye P, Robert E, Cargo M, Bartlett G, O’Cathain A, Griffiths F, et al. Proposal: a mixed methods appraisal tool for systematic mixed studies reviews. 2011. p. 1–8. Available from: http://mixedmethodsappraisaltoolpublic.pbworks.com/f/MMAT%202011%20criteria%20and%20tutorial%202011-06-29.pdf%5Cnhttp://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Proposal:+A+mixed+methods+appraisal+tool+for+systematic+mixed+studies+reviews.#0.
de Vet HCW, De Bie RA, Van Der Heijden GJMG, Verhagen AP, Sijpkes P, Knipschild PG. Systematic reviews on the basis of methodological criteria. Physiotherapy. 1997;83(6):284–9.
Hoben M, Hu H, Xiong T, Kent A, Kobagi N, Yoon MN. Barriers and facilitators in providing oral health care to nursing home residents, from the perspective of care aides-a systematic review protocol. Syst Rev. 2016;5(1):1–7. https://doi.org/10.1186/s13643-016-0231-7.
Hoben M, Banerjee S, Beeber AS, Chamberlain SA, Hughes L, O’Rourke HM, et al. Feasibility of routine quality of life measurement for people living with dementia in long-term care. J Am Med Dir Assoc. 2022;23(7):1221-6.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:1–10.
Hayes-Larson E, Mobley TM, Gilmore-Bykovskyi A, Shaw C, Karlamangla A, Manly JJ, et al. Racial/ethnic differences in health-related quality of life in persons with and without dementia. J Am Geriatr Soc. 2021;69(3):629–36.
Rodríguez-Martínez A, De-la-Fuente-Robles YM, Martín-Cano M del C, Jiménez-Delgado JJ. Quality of life and well-being of older adults in nursing homes: systematic review. Soc Sci. 2023;12:1–22.
Hoben M, Dymchuk E, Corbett K, Devkota R, Shrestha S, Lam J, et al. Factors associated With the quality of life of nursing home residents during the COVID-19 pandemic: a cross-sectional study. J Am Med Dir Assoc. 2023;24:876–84.
Duan Y, Mueller CA, Yu F, Talley, Kristine M, Shippee TP. The relationships of nursing home culture change practices with resident quality of life and family satisfaction: toward a more nuanced understanding. Res Aging. 2022;44(2):174-85.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC Methods Programme. 2006.
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. United Kingdom: Wiley & Sons Ltd; 2009. p. 1–406.
Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(6):557–60.
Mittlbock M, Heinzl H. A simulation study comparing properties of heterogeneity measures in meta-analysis. Stat Med. 2006;25:4321–33.
IBM Corp. Released 2011. IBM SPSS statistics, Version 20.0. Armonk, New York: IBM Corp.
Brockwell SE, Gordon IR. A comparison of statistical methods for meta-analysis. Stat Med. 2001;20(6):825–40.
Kontopantelis E, Reeves D. Performance of statistical methods for meta-analysis when true study effects are non-normally distributed: a comparison between DerSimonian-Laird and restricted maximum likelihood. Stat Methods Med Res. 2012;21(6):657–9.
Kicinski M, Springate DA, Kontopantelis E. Publication bias in meta-analyses from the Cochrane Database of Systematic Reviews. Stat Med. 2015;34:2781–93.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–6.
Pollock A, Campbell P, Struthers C, Synnot A, Nunn J, Hill S, et al. Stakeholder involvement in systematic reviews: a scoping review. Syst Rev. 2018;7:1–26.
MacLeod S, Musich S, Hawkins K, Alsgaard K, Wicker ER. The impact of resilience among older adults. Geriatr Nurs (Minneap). 2016;37(4):266–72. https://doi.org/10.1016/j.gerinurse.2016.02.014.
Steptoe A, Deaton A, Stone AA. Psychological wellbeing, health and ageing. Lancet. 2015;385(9968):640–8.
Acknowledgements
We want to thank M. Kennedy, librarian at the John W. Scott Health Sciences Library, University of Alberta for her guidance and feedback in developing search strategies for databases.
Funding
The study itself is not funded. However, SS received the Nurse Endowment Award from the Faculty of Nursing, at the University of Alberta to support the stakeholder engagement activity. Funders had no role in the development of the systematic review protocol.
Author information
Authors and Affiliations
Contributions
SS developed the research question, planned, and designed the systematic review, developed the study protocol, and drafted the manuscript. GC and MH are the co-supervisor authors and guided in all aspects of the research including concept development, study planning, designing, manuscript writing, and editing. JKS is SS’s supervisory committee member and was responsible for all major areas of concept development, review planning, manuscript writing, and editing. SS developed the search strategy with the assistance of MK. RD reviewed and edited the manuscript. All authors read, provided feedback, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This review is a part of SS’s PhD project. We have obtained ethical approval from the Institutional Ethics Board of the University of Alberta (Pro00122600). We will obtain verbal consent from the stakeholders for their participation in the focus group discussion.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P 2015 Checklist.
Appendices
Appendix 1
Appendix 2
Search strategies created for various database
Database: Ovid MEDLINE(R) ALL < 1946 to August 4, 2022 > (Total searches: 715)
-
1.
(longterm care or long term care or LTC).mp.
-
2.
exp Geriatrics/ or Aged/ or Health Services for the Aged/ or Senior Centers/ or (elders or elderly or geriatric* or old age or (seniors not “high school”) or (older adj3 (adult*or person* or people or man or men or woman or women)) or centenarian* or nonagenarian* or octogenarian* or septuagenarian* or sexagenarian* or dottering or decrepit or tottering or overaged or “oldest old”).mp.
-
3.
1 and 2
-
4.
exp Nursing Homes/ or exp Homes for the Aged/ or exp Rehabilitation Centers/ or exp Skilled Nursing Facilities/ or (nursing home* or extended care* or care home*).mp. or ((senior* or continuing care or disabled or old age or geriatric* or elder care* or rehabilitat* or long term care) adj2 (lodge* or facility* or home* or residence* or centre* or center*)).mp.
-
5.
3 or 4
-
6.
exp pain/
-
7.
(pain* or discomfort* or soreness or ache* or aching or hurt*).mp.
-
8.
6 or 7
-
9.
“Quality of Life”/
-
10.
(“quality or life” or QoL or HRQoL or HQoL).mp.
-
11.
(“life satisfaction” or “life-satisfaction”).mp.
-
12.
(“wellbeing” or “well-being”).mp.
-
13.
9 or 10 or 11 or 12
-
14.
5 and 8 and 13
Database: EMBASE < 1974 to August 4, 2022 > (Total searches: 2054)
-
1.
(longterm care or long term care or LTC).mp.
-
2.
exp geriatrics/ or aged/ or aged hospital patient/ or exp elderly care/ or frail elderly/ or gerontology/ or institutionalized elderly/ or very elderly/ or (“aging in place” or elders or elderly or geriatric* or gerodontic* or old age or (seniors not “high school”) or (older adj3 (adult* or person* or people or man or men or woman or women)) or centenarian* or nonagenarian* or octogenarian* or septuagenarian* or sexagenarian* or dottering or decrepit or tottering or overaged or “oldest old”).mp.
-
3.
1 and 2
-
4.
exp nursing home/ or exp home for the aged/ or exp rehabilitation center/ or institutionalized elderly/ or (nursing home* or extended care* or care home*).mp. or ((convalescen* or senior* or continuing care or disabled or old age or geriatric* or elder care* or rehabilitat* or long term care) adj2 (lodge* or facility* or home* or residence* or centre* or center*)).mp.
-
5.
3 or 4
-
6.
exp pain/
-
7.
(pain* or discomfort* or soreness or ache* or aching or hurt*).mp.
-
8.
6 or 7
-
9.
“Quality of Life”/
-
10.
(“quality or life” or QoL or HRQoL or HQoL).mp.
-
11.
(“life satisfaction” or “life-satisfaction”).mp.
-
12.
(“wellbeing” or “well-being”).mp.
-
13.
9 or 10 or 11 or 12
-
14.
5 and 8 and 13
Database: PsychInfo < 1974 to August 4, 2022 > (Total searches: 302)
-
1.
(longterm care or long term care or LTC).mp.
-
2.
geriatrics/ or exp “aged (attitudes toward)”/ or exp aging/ or geriatric assessment/ or geriatric psychotherapy/ or gerontology/ or exp geropsychology/ or late life depression/ or exp elder care/ or elder abuse/ or (elders or elderly or geriatric* or old age or oldest age* or (seniors not “high school”) or (older adj3 (adult* or people or person or persons or man or men or woman or women)) or oldest patient* or “old old” or “very old” or centenarian* or nonagenarian* or octogenarian* or septuagenarian* or sexagenarian* or dottering or decrepit or tottering or “late* life” or overaged or “oldest old”).ti,ab,jn,jx,mh,sh.
-
3.
1 and 2
-
4.
exp Nursing Homes/
-
5.
exp Residential Care Institutions/
-
6.
exp Rehabilitation Centers/
-
7.
institutionalized elderly.mp.
-
8.
(nursing home* or extended care* or care home*).mp.
-
9.
((senior* or continuing care or disabled or old age or geriatric* or elder care* or rehabilitat* or long term care) adj2 (lodge* or facility* or home* or residence* or centre* or center*)).mp.
-
10.
4 or 5 or 6 or 7 or 8 or 9
-
11.
exp Pain/
-
12.
(pain* or discomfort* or soreness or ache* or aching or hurt*).mp.
-
13.
11 or 12
-
14.
“Quality of Life”/
-
15.
(“quality or life” or QoL or HRQoL or HQoL).mp.
-
16.
(“life satisfaction” or “life-satisfaction”).mp.
-
17.
(“wellbeing” or “well-being”).mp.
-
18.
14 or 15 or 16 or 17
-
19.
3 or 10
-
20.
13 and 18 and 19
Database: CINAHL < 1937 to August 4, 2022 > (Total searches: 1198)
-
S1
(MH “Long Term Care”) OR “(longterm care or long term care or LTC).mp.”
-
S2
(MH “Geriatrics”) or (MH “Aged, Hospitalized”) or (MH “Aged+”) or (MH “Senior Centers”) or (MH “Gerontologic Care”) or (MH “Geriatricians”) OR (MH “Gerontologic Nursing+”) OR (MH “Health Services for the Aged”) or (“aging in place” or elders or elderly or geriatric* or gerontolog* or gerodontic* or old age or (seniors not “high school”) or “senior citizen*” or (older N3 (patient* or adult* or person* or people or man or men or woman or women)) or centenarian* or nonagenarian* or octogenarian* or septuagenarian* or sexagenarian* or dottering or decrepit or tottering or overaged or “oldest old”)
-
S3
S1 and S2
-
S4
(MH “Nursing Homes + ”)
-
S5
(MH “Nursing Home Patients”)
-
S6
(MH “Rehabilitation Centers”) OR (MH “Residential facilities”) OR (MH “Housing for the Elderly”)
-
S7
((“nursing home*” or “extended care*” or “care home*”)) OR (((convalescen* or senior* or “continuing care” or disabled or “old age” or geriatric* or “elder care*” or rehabilitat* or “long term care”) N2 (lodge* or facility* or home* or residence* or centre* or center*))) 70,416
-
S8
S4 or S5 or S6 or S7
-
S9
S3 or S8
-
S10
(MH “Pain+”)
-
S11
(pain* or discomfort* or soreness or ache* or aching or hurt*)
-
S12
S10 or S11
-
S13
(MH “Quality of Life”)
-
S14
(“quality or life” or QoL or HRQoL)
-
S15
“(“life satisfaction” or “life-satisfaction”)”
-
S16
“(“wellbeing” or “well-being”)”
-
S17
S13 or S14 or S15 or S16
-
S18
S9 AND S12 AND S17
Database: SCOPUS < 1974 to August 4, 2022 > (Total searches: 145)
( ( TITLE-ABS-KEY ( elders OR elderly OR geriatric* OR old AND age OR senior* OR centenarian* OR nonagenarian* OR octogenarian* OR septuagenarian* OR sexagenarian* OR dottering OR decrepit OR tottering OR overaged OR “oldest old”)) OR ( TITLE-ABS-KEY ( older W/3 ( adult* OR person* OR people OR man OR men OR woman OR women)))) AND ( TITLE-ABS-KEY ( (“nursing home*” OR “extended care*” OR “care home*” OR ( ( senior* OR “continuing care” OR disabled OR “old age*” OR geriatric* OR “elder care*” OR rehabilitat* OR “long term care”) W/2 (lodge* OR facility* OR home* OR residence* OR centre* OR center*))))) AND ( TITLE-ABS-KEY (pain* OR discomfort* OR soreness OR ache* OR aching OR hurt*)) AND ( TITLE-ABS-KEY (“quality or life” OR qol OR hrqol OR hqol OR “life-satisfaction” OR “life satisfaction” OR “wellbeing” OR “well-being”)) AND
(LIMIT-TO ( DOCTYPE,“ar”) OR LIMIT-TO (DOCTYPE,“re”))
Database: Cochrane Library < 1993 to August 4, 2022 > (Total searches: 341)
-
1
[mh Geriatrics]
-
2
[mh Aged]
-
3
[mh “Health Services for the Aged”]
-
4
[mh “Senior Centers”]
-
5
(elders or elderly or geriatric* or old age or (seniors not “high school”)):ti,ab,kw
-
6
(older NEAR/3 (adult*or person* or people or man or men or woman or women) or centenarian* or nonagenarian* or octogenarian* or septuagenarian* or sexagenarian* or dottering or decrepit or tottering or overaged or “oldest old”):ti,ab,kw
-
7
#1 OR #2 OR #3 OR #4 OR #5 OR #6
-
8
[mh “Nursing Homes”]
-
9
[mh “Homes for the Aged”]
-
10
[mh “Rehabilitation Centers”]
-
11
[mh “Skilled Nursing Facilities”]
-
12
(nursing home* or extended care* or care home*):ti,ab,kw
-
13
((senior* or continuing care or disabled or old age or geriatric* or elder care* or rehabilitat* or long term care) NEAR/2 (lodge* or facility* or home* or residence* or centre* or center*)):ti,ab,kw
-
14
#8 OR #9 OR #10 OR #11 OR #12 OR #13
-
15
[mh pain]
-
16
(pain* or discomfort* or soreness or ache* or aching or hurt*):ti,ab,kw
-
17
#15 OR #16
-
18
[mh ^“Quality of Life”]
-
19
(“quality or life” or QoL or HRQoL or HQoL):ti,ab,kw
-
20
((life) NEAR/2 (satisfaction)):ti,ab,kw
-
21
(“wellbeing” or “well-being”):ti,ab,kw
-
22
{OR #18-#21}
-
23
#7 AND #14 AND #17 AND #22
Database: Proquest Dissertations and Theses global < 1853 to 2014 > (Total searches: 52)
-
S1
noft(elders OR elderly OR geriatric* OR “old age*”)
-
S2
noft(older NEAR/3 (adult* or person* or people or man or men or woman or women))
-
S3
S1 OR S2
-
S4
noft(“nursing home*” or “rehabilitation center*” or “skilled nursing facility*” or “care home*” or “extended care*”)
-
S5
noft((senior* or “continuing care” or disabled or “old age” or geriatric* or (“elder care”) or rehabilitat* or “long term care”) NEAR/3 (lodge* or facility* or home* or residence* or centre* or center*))
-
S6
S4 OR S5
-
S7
noft(pain* or discomfort* or soreness or ache* or aching or hurt*)
-
S8
noft(“quality of life” or QoL or HRQoL or HQoL or “life satisfaction” or “life-satisfaction” or “wellbeing” or “well-being”)
-
S9
S3 AND S6 AND S7 AND S8
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shrestha, S., Cummings, G., Knopp-Sihota, J. et al. Factors influencing health-related quality of life among long-term care residents experiencing pain: a systematic review protocol. Syst Rev 13, 49 (2024). https://doi.org/10.1186/s13643-024-02459-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02459-7