
Abstract
Background
The interaction between modelers and policymakers is becoming more common due to the increase in computing speed seen in recent decades. The recent pandemic caused by the SARS-CoV-2 virus was no exception. Thus, this study aims to identify and assess epidemiological mathematical models of SARS-CoV-2 applied to real-world data, including immunization for coronavirus 2019 (COVID-19).
Methodology
PubMed, JSTOR, medRxiv, LILACS, EconLit, and other databases were searched for studies employing epidemiological mathematical models of SARS-CoV-2 applied to real-world data. We summarized the information qualitatively, and each article included was assessed for bias risk using the Joanna Briggs Institute (JBI) and PROBAST checklist tool. The PROSPERO registration number is CRD42022344542.
Findings
In total, 5646 articles were retrieved, of which 411 were included. Most of the information was published in 2021. The countries with the highest number of studies were the United States, Canada, China, and the United Kingdom; no studies were found in low-income countries. The SEIR model (susceptible, exposed, infectious, and recovered) was the most frequently used approach, followed by agent-based modeling. Moreover, the most commonly used software were R, Matlab, and Python, with the most recurring health outcomes being death and recovery. According to the JBI assessment, 61.4% of articles were considered to have a low risk of bias.
Interpretation
The utilization of mathematical models increased following the onset of the SARS-CoV-2 pandemic. Stakeholders have begun to incorporate these analytical tools more extensively into public policy, enabling the construction of various scenarios for public health. This contribution adds value to informed decision-making. Therefore, understanding their advancements, strengths, and limitations is essential.
Similar content being viewed by others


Introduction
Coronavirus 2019 (COVID-19) is a pathology caused by the SARS-CoV-2 virus. Since 2020, it has resulted in numerous cases and fatalities [1]. Its transmission primarily occurs from person to person, exhibiting high transmissibility and a variable, unpredictable course [2]. Consequently, in March 2020, the World Health Organization (WHO) classified COVID-19 as a pandemic due to its global spread.
Throughout the initial 2 years of the pandemic, cases spread swiftly across the world, albeit asynchronously, yielding heterogeneous effects among different territories. At present, there exist multiple highly effective vaccines against COVID-19, with over 12.5 billion doses administered worldwide [3]. It is important to note that the success of COVID-19 vaccination hinges on factors such as the duration of immunity conferred by vaccines, their efficacy against new SARS-CoV-2 variants, and the implementation protocols in each country [4,5,6].
The scientific community has been fervently engaged in describing and studying epidemiological phenomena through theoretical and methodological modeling. Hence, this review delves into diverse facets, including the types of epidemiological mathematical model employed, the simulation software used as well as sociodemographic, socioeconomic, clinical, and vaccination-related factors [7]. Epidemiological mathematical modeling furnishes vital information for informed decision-making in public policy. It plays a pivotal role in comprehending and managing infectious diseases, as its tools facilitate the simplification of complex and uncertain scenarios [8]. These quantitative models serve to build scenario planning, evaluate possible scenarios, and analyze them according to their potential risks based on different health outcomes.
Furthermore, the interaction between modelers and policymakers has become more prevalent due to the escalating computing speed in recent decades. This relationship is characterized by complex models that collect the reality of the epidemiological situation in detail and interventions to mitigate it [7]. The recent SARS-CoV-2 pandemic is closely intertwined with this interaction. As a result, the objective of this research is to compile and analyze the predictive models developed for studying diverse health outcomes stemming from COVID-19. This analysis adopts a mathematical epidemiological approach, involving the scrutiny of real-world data. Given the new generation of quantitative health analyses applied to the pandemic with real-world data, we wanted to review what kind of new approaches had been developed that could serve as a basis for future applications of predictive analytics.
Methodology
A systematic literature search was conducted in accordance with the rapid review format guidelines established in the Cochrane international methods [9]. This approach was complemented with the literature review methodology from software engineering [10, 11]. The PROSPERO registration number for this study is CRD42022344542. A comprehensive and generic search strategy was formulated and subsequently tailored for the diverse sources of information. Language, study type, and date restrictions were not applied. The search strategy encompassed articles available up to April 1, 2022.
The study’s target population comprised individuals who had been vaccinated against COVID-19 within the context of mathematical epidemiological models. The intervention under examination was the COVID-19 vaccine, regardless of brand name. The health outcomes sought were the number of deaths, recovered, hospitalized, infected, and susceptible due to COVID-19. Inclusion criteria therefore referred to the development of mathematical epidemiological models that had used real-world data for their analysis.
The consulted databases included PubMed, JSTOR, medRxiv, LILACS, EconLit, IEEE Transactions on Software Engineering, ACM Transactions on Software Engineering Methodology (TOSEM), Empirical Software Engineering Journal, Journal of Systems and Software, and Information and Software Technology. Google Scholar was utilized for grey literature search. These databases selection was based on the quantitative approach of the literature review and the expertise of the authors.
The search strategy, outlined in Supplement N°. 1, was also complemented with manual searches. The articles included in this review provided information on mathematical epidemiological models of the SARS-CoV-2 virus, incorporating vaccination and relying on real-world data for analysis. Mendeley software facilitated reference deduplication, and Microsoft Excel® software was employed for the screening process. Two independent groups of reviewers (OE, DR, JR, and VB, AR, CS) evaluated each title and abstract in a blinded manner, with conflicts resolved by a third evaluator (OE or LM) when necessary. Full-text screening followed a similar process. Studies included in the full-text review phase were the incorporated into the data extraction phase. Excluded studies are listed in Supplement N°. 2.
Five reviewers (VB, DR, AR, CS, JR) extracted the information, which was independently verified by two reviewers (OE and LM) using a data extraction form designed in Microsoft Excel® (Supplement N°. 3A). Variable definitions are provided in Supplement N°. 3B. The extracted characteristics were summarized descriptively. Results were categorized based on the country’s income, determined by gross national income (GNI) per capita [12], into high-income countries (USD > 12695), upper-middle income (USD 4096–12695), lower-middle income (USD 1046–4095), low-income (USD < 1046), and multi-income studies encompassing countries from different income levels.
Methodological quality was assessed by independent reviewers using two tools: initially, the Joanna Briggs Institute (JBI), classic checklist based on the methodological design [13, 14], and PROBAST, a specialized tool for assessing the risk of bias and applicability assessment in predictive modeling studies in health sciences [15]. Methodological quality assessment was carried out by an expert (LM) and, when needed, agreed upon with a second methodological expert (OE). The methodological tools are shown in Supplement N°. 4.
Results
Literature search results
A total of 5646 references were identified from indexed databases, and an additional 197 documents were located in the grey literature. Among these, 2362 (40.4%) were excluded as duplicates, leaving 3481 (59.6%) references for title and abstract screening. From these, 398 (11.43%) references proceeded to full-text evaluation, resulting in the inclusion of 202 (5.8%) articles. Furthermore, by applying a snowball strategy using the Connected Papers platform (which uses advanced textual analytics techniques) and reviewing the reference lists of the included articles, an additional 209 references were incorporated, yielding a total of 411 documents included in this review. The information flowchart is depicted in the PRISMA figure (see Supplement N°. 5), and the list of included studies is presented in Supplement N°. 6.
In terms of publication distribution, 16 [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31], 280 [32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309,310,311], and 115 [312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343,344,345,346,347,348,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400,401,402,403,404,405,406,407,408,409,410,411,412,413,414,415,416,417,418,419,420,421,422,423,424,425,426] articles were published in 2020, 2021, and 2022, respectively. The majority of these articles were concentrated in high-income countries, constituting 69.3% of the publications [16, 17, 20,21,22,23,24, 26, 29,30,31, 33, 34, 37, 39,40,41,42,43, 46,47,48,49, 51, 52, 57,58,59, 61, 62, 66, 68,69,70, 72,73,74,75,76,77, 79, 80, 82,83,84,85,86,87, 90, 92,93,94, 98,99,100,101,102, 106,107,108,109,110,111,112,113,114, 116,117,118,119,120,121,122,123,124, 126,127,128, 130,131,132,133,134,135,136,137, 140, 142, 145, 147, 150, 151, 153,154,155,156,157,158,159,160,161, 164, 165, 167, 169,170,171,172,173, 175, 178,179,180,181,182,183,184,185,186,187,188, 191,192,193,194,195, 197,198,199,200,201,202, 204, 205, 207, 209, 211, 212, 217, 220, 222, 224, 227, 232,233,234,235,236,237, 239,240,241,242,243,244,245,246,247,248,249,250,251,252, 254, 255, 257, 258, 260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283, 285, 286, 288,289,290,291,292,293,294,295,296,297,298, 300, 302,303,304, 307, 310, 314,315,316,317, 323, 324, 326,327,328, 332, 333, 335,336,337,338, 340, 342,343,344,345, 347,348,349, 351,352,353, 355, 357,358,359,360,361,362,363,364,365,366,367,368, 372,373,374, 376,377,378, 381,382,383,384,385, 387,388,389,390,391, 393, 394, 397, 400, 401, 403,404,405, 407, 410, 412, 415, 416, 418, 420, 421, 423,424,425,426]. Only 8% of the articles were for low-middle income countries [36, 38, 44, 45, 54, 56, 89, 104, 105, 115, 129, 138, 143, 144, 146, 163, 206, 218, 223, 256, 287, 299, 306, 312, 318, 319, 331, 339, 369, 380, 398, 399, 414]. The United States (USA) had the most articles related to the topic, with 106 articles (25.8%) [16, 17, 21, 24, 26, 29, 31, 34, 42, 43, 47, 49, 51, 57, 62, 74, 76, 82, 85, 87, 90, 93, 94, 107, 112, 113, 118,119,120,121,122, 131, 133, 135, 137, 142, 147, 151, 153, 155, 159, 172, 179, 180, 182,183,184, 191,192,193,194, 198, 209, 217, 220, 227, 234,235,236, 241,242,243,244,245, 248, 251, 254, 255, 263, 265,266,267, 270, 273, 281, 290, 292, 296, 310, 328, 332, 333, 335, 337, 345, 348, 349, 351, 353, 358, 363, 366, 367, 377, 382,383,384, 388, 390, 391, 400, 401, 407, 410, 415, 424]. Canada followed with 22 documents (5.4%) [22, 33, 41, 66, 77, 111, 126, 145, 154, 156, 181, 197, 200, 202, 205, 240, 269, 276, 300, 317, 357, 364], and China with 20 articles (4.9%) [25, 55, 63, 81, 88, 91, 95, 97, 174, 208, 216, 221, 225, 229, 230, 320, 329, 330, 409, 411]. No information from exclusively low-income countries was found (see Table 1).
Description of epidemiological mathematical models
The primary mathematical model employed was the SEIR (susceptible, exposed, infectious, and recovered) compartmental model, utilized in 47% [193]) of the retrieved articles [17, 19, 24,25,26,27,28, 31,32,33,34,35,36, 42, 45, 46, 57, 60, 65, 67, 69, 71, 73, 77, 80, 87, 89, 91, 92, 94, 96,97,98,99,100, 103,104,105,106,107, 109, 111,112,113, 115, 118, 122,123,124,125,126,127,128, 130, 131, 133, 135, 138,139,140,141,142,143,144,145,146, 148,149,150, 156, 157, 159,160,161,162,163,164,165, 167, 168, 174,175,176,177, 179, 180, 183, 185, 187, 188, 192, 199, 210, 212, 215, 218,219,220, 223,224,225,226,227, 233,234,235,236,237, 241, 243, 247, 251,252,253,254,255, 258, 260, 261, 264, 266, 267, 269, 271, 272, 275, 276, 279,280,281, 283, 284, 288, 289, 291, 294, 297,298,299,300,301, 304, 306, 307, 310, 312,313,314, 317,318,319, 326, 327, 331, 341, 344,345,346,347, 350, 352,353,354,355, 357, 359,360,361, 369, 371, 381, 382, 384, 390,391,392, 396, 397, 399, 401, 403, 405, 408, 412,413,414,415,416, 418, 420, 422, 423, 426]. The category “other models” encompasses less commonly models, such as Bayesian networks, Poisson models, and other compartmental models (see Table 2).
Regarding the operational characteristics and accessibility to the databases and models employed in the included studies, it was noted that only 16.3% of the references did not engage in mathematical development of the proposed model [18, 20, 30, 40, 43, 52, 59, 62, 81, 83, 90, 120, 121, 131, 137, 142, 151, 154, 157, 167, 170, 172, 173, 177, 178, 188, 189, 192, 194, 202, 205,206,207,208, 211, 215, 217, 222, 242, 245, 247,248,249,250, 254, 273, 277, 285, 295, 301, 305, 324, 332, 334, 339, 340, 351, 358, 365, 372, 385, 387, 390, 393, 404, 417, 426]. The main software utilized was R, accounting for 19.7% of cases [27, 29, 32, 33, 40, 41, 53, 60, 62, 67, 76, 82, 91, 92, 94,95,96, 106, 109, 111, 114, 117, 132, 138, 157, 164,165,166, 179, 180, 211, 218, 219, 222, 238, 244,245,246, 248, 253, 254, 261, 264, 275, 277, 279, 283, 288, 292, 295, 296, 311, 313, 319, 323, 325, 326, 328, 330, 332, 334, 336, 346, 347, 349, 355, 361, 363, 373, 378, 380, 382,383,384, 388, 389, 392, 394, 397, 407, 415]. A majority of the references, 59.9%, did not present the programming code with open access. Merely 3.6% of these references developed a dashboard [60, 74, 84, 114, 180, 250, 256, 260, 280, 295, 331, 338, 378, 380, 382] (see Table 3).
Description of sociodemographic aspects
When analyzing the sociodemographic characteristics reported in the included articles, it was observed that 252 articles (61.3%) incorporated age in their models [16,17,18, 21, 23, 25, 26, 29, 31, 33, 34, 36, 39,40,41,42, 44, 47, 48, 50, 52,53,54,55, 58,59,60, 64,65,66, 68,69,70, 72, 74, 77, 79, 80, 82,83,84,85,86,87,88, 90, 92, 95, 96, 99, 102,103,104,105,106, 108, 109, 111,112,113,114, 116,117,118,119,120,121,122,123,124,125,126, 129, 133, 134, 137, 138, 140,141,142, 144, 147,148,149,150,151, 153,154,155,156,157, 160,161,162, 164, 165, 167,168,169,170, 174, 175, 178, 179, 184, 187, 188, 192, 196, 199, 201,202,203,204,205,206, 208, 210, 211, 213, 215,216,217, 219, 221, 222, 227, 229, 234,235,236,237, 241, 242, 245,246,247,248,249, 253,254,255, 258,259,260, 262, 263, 266, 269, 271,272,273,274,275,276,277, 279, 281,282,283,284,285, 288, 290, 291, 293,294,295, 297, 298, 300,301,302,303,304, 308,309,310,311, 313, 314, 316, 319, 320, 323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343, 345, 347,348,349,350,351, 354, 355, 357,358,359, 361, 365,366,367, 370, 371, 373,374,375,376,377,378, 380, 382, 386,387,388,389,390,391, 393, 394, 397, 402, 403, 405,406,407, 410, 416,417,418, 423,424,425,426]. Among these, 13 (3.2%) were documented within lower-middle-income countries [36, 44, 54, 104, 105, 129, 138, 144, 206, 319, 331, 339, 380].
Sex-related data were incorporated into mathematical modeling in 23 articles (5.6%) [59, 68, 74, 84, 95, 165, 170, 174, 203, 227, 235, 260, 263, 285, 301, 305, 334, 336, 367, 377, 388, 397, 426]. Additionally, 6 articles (1.5%) included information related to ethnicity [59, 137, 155, 235, 367, 388], and 15 articles (3.6%) included vulnerable groups [63, 64, 71, 81, 177, 291, 331, 374, 378, 380, 382, 404, 408, 409, 412] (see Table 4).
Description of clinical and vaccine aspects
Comorbidities and reinfection
Among the included articles, 40 (9.7%) incorporated information related to comorbidities [42, 59, 64, 74, 77, 84, 85, 91, 99, 104, 108, 119,120,121, 123, 129, 137, 138, 144, 146, 155, 173, 196, 202, 203, 205, 206, 241, 253, 269, 282, 283, 300, 349, 351, 354, 366, 372, 377, 388]. Among these, 28 (6.8%) were within high-income countries. However, none of these studies provided a specific description of the identified comorbidities.
On the other hand, 117 (28.5%) references considered the reinfection variable [17, 22, 28, 32, 36,37,38, 44, 46, 59,60,61, 63, 70, 72, 77, 79, 92, 94, 103, 105, 108, 122, 125, 128, 129, 138, 140, 145, 146, 149, 153, 156, 157, 163,164,165, 168, 172, 175, 176, 178, 185, 190, 192, 198, 201, 217,218,219, 223, 226, 230, 231, 233, 241, 243, 254, 258, 264, 265, 267, 269, 276, 277, 281, 283, 285, 291, 293, 296, 299, 300, 304, 305, 308, 313,314,315, 318, 319, 328, 333,334,335, 341, 343, 344, 346, 350, 354, 358, 361, 362, 364, 373, 374, 377, 380,381,382, 389, 390, 396, 399, 402,403,404, 406, 408, 409, 411, 413, 414, 420, 421, 426]. Out of these, 90 articles (21.9%) were elaborated for high and upper-high income countries [17, 22, 28, 32, 37, 46, 59, 61, 63, 70, 72, 77, 79, 92, 94, 108, 122, 125, 128, 140, 145, 149, 153, 156, 157, 164, 165, 168, 172, 175, 176, 178, 185, 192, 198, 201, 217, 230, 233, 241, 243, 254, 258, 264, 265, 267, 269, 276, 277, 281, 283, 285, 291, 293, 296, 300, 304, 305, 308, 314, 315, 328, 333,334,335, 343, 344, 346, 354, 358, 361, 362, 364, 373, 374, 377, 381, 382, 389, 390, 403, 404, 406, 408, 409, 411, 413, 420, 421, 426].
Types of vaccines, number of vaccines, and heterologous vaccination
Although most articles indicate the use of vaccines in the modeling, many did not specify a particular vaccine. Specifically, 319 articles (77.6%) considered the use of only one type of vaccine [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32, 34, 35, 37,38,39,40,41, 43,44,45,46,47,48,49,50, 53,54,55,56,57,58, 60,61,62,63,64,65,66,67, 69,70,71, 73,74,75, 79,80,81,82,83,84,85,86, 88,89,90,91,92,93,94,95,96,97,98,99,100, 102,103,104,105, 107, 111, 112, 115, 118, 121, 122, 124,125,126, 128,129,130,131,132,133, 135, 137,138,139,140,141, 143,144,145,146,147,148,149,150,151, 154, 156, 158,159,160, 163, 165,166,167,168,169,170,171,172,173,174,175,176,177, 180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195, 197,198,199,200,201,202, 206, 208, 209, 212, 213, 215,216,217,218,219,220,221, 223,224,225,226,227,228,229,230,231,232,233,234, 236,237,238, 240,241,242,243,244,245,246,247, 249,250,251,252,253, 255, 256, 258, 259, 261, 263,264,265,266, 269, 274, 275, 277, 278, 280,281,282, 284, 286,287,288,289,290,291,292,293,294,295,296,297,298,299, 301,302,303, 306,307,308,309,310, 314,315,316,317, 321,322,323, 327, 329,330,331,332, 334, 337,338,339,340,341,342,343, 345,346,347,348, 350,351,352,353, 356,357,358, 362, 363, 366, 368,369,370,371, 373,374,375,376,377,378,379,380,381,382, 384,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400,401,402, 404,405,406,407,408,409,410,411,412,413,414,415,416,417,418,419,420,421,422,423,424,425,426]. Only two articles (0.5%) did not refer to this topic [106, 110].
Regarding the number of reported doses, 159 references (38.7%) included data from the first and second doses of the vaccines in the models [29, 39, 41, 43, 49, 53,54,55, 59, 60, 62, 63, 66, 68,69,70, 73, 78, 79, 82, 85, 90, 97, 100, 101, 103, 105, 109, 111, 114, 117, 121, 123,124,125,126, 128, 134, 136, 138, 140, 142, 144, 152, 153, 155, 156, 158,159,160,161,162,163,164,165, 167, 173, 178, 182, 184, 186,187,188, 195, 199, 202,203,204,205,206, 216, 217, 221, 224, 228,229,230, 233, 235,236,237, 239, 240, 242, 249, 260, 263, 265, 271, 273, 276, 278, 279, 287, 290, 292, 297, 298, 302,303,304,305, 307, 308, 310, 312, 313, 315, 319, 320, 323, 324, 329, 330, 332, 334, 335, 337, 340, 342, 348, 349, 351,352,353, 356, 358, 359, 361,362,363, 366, 367, 370, 372,373,374, 376,377,378, 381, 384, 387,388,389, 392,393,394, 397, 405, 407, 410, 415, 417, 418, 421, 423,424,425]. Ten (2.4%) articles reported data concerning booster doses [91, 96, 115, 122, 127, 201, 322, 333, 341, 422].
Heterogeneous vaccine was indicated for high-income countries in two (0.5%) articles [106, 382]. In 95 articles (23.1%), the difference in days between administered doses were considered; out of these, 22 articles (23.2%) considered a 21-day interval between doses [55, 60, 69, 100, 122, 133, 134, 140, 187, 216, 217, 221, 302, 303, 329, 330, 335, 342, 383, 384, 424, 425], while 22 (23.2%) considered a period of 21- to 28-day interval [42, 90, 116, 119,120,121, 136, 142, 151, 155, 184, 204, 205, 258, 260, 273, 324, 328, 351, 354, 356, 366]. Additionally, 11 (11.6%) articles considered a period equal to or greater than three months [203, 211, 222, 269, 300, 314, 317, 333, 334, 350, 361]. Four articles identified had dose intervals greater than 150 days, all in high-income countries [211, 222, 314, 333], with one having a 240-day interval for the booster dose [333].
Regarding trademarked vaccines, 12 articles reported a 28-day difference for the Moderna vaccine [42, 116, 119, 120, 142, 155, 184, 205, 258, 260, 351, 366]. For the Pfizer-BioNTech, 10 references indicated a 21-day difference between the first and second dose [69, 100, 133, 134, 217, 302, 303, 335, 342, 383], while one reference indicated a 28-day difference [173]. Different intervals were identified for the AstraZeneca vaccine: 70 days [139], 84 days [99], and 28, 56, 84, 112, and 140 days [350].
Vaccine effectiveness and difference between effectiveness
Most studies were conducted in high-income countries. Within the total references, effectiveness rates of 50%, 60%, 70%, 80%, and 100% were presented in 63, 40, 47, 52, and 33 articles, respectively. Notably, articles focused on low-middle-income countries predominantly employed an effectiveness rates of 80%. Out of the 33 articles considering an effectiveness rate of 100%, 23 (5.6%) were conducted in high-income countries.
The majority of articles did not specify the exact outcome against which the effectiveness was measured. Among those reporting a 100% effectiveness rate, two indicated effectiveness in preventing death [99, 282]. In 14 articles (3.4%), the effectiveness rates were reported to be less than 10% [23, 28, 78, 106, 112, 179, 229, 311, 319, 326, 364, 379, 391, 400]. Notably, two of these articles mentioned an effectiveness of 0%. The first dealt with the gamma variant using the CoronaVac vaccine [311], while the second addressed subsequent infection [379].
Regarding the different variants, 155 articles (37.7%) described the specific strain included in their models. Among these, the delta variant was the most frequently modeled, with a total of 41 references (10%) [43, 47, 91, 96, 105, 114, 119, 122, 124, 128, 149, 153, 218, 252, 258, 262, 278, 286, 297, 314, 318, 321, 326, 328, 329, 332, 333, 338, 340, 343, 350, 352, 357, 367, 380, 387, 401, 416, 419, 421, 425]. The alpha variant followed with 18 articles (4.4%) [60, 93, 101, 113, 156, 157, 180, 195, 199, 247,248,249, 296, 298, 303, 331, 393, 397] (see Table 5).
The articles encompassed a range of evaluated outcomes, including deceased, recovered, hospitalized (e.g., in an intensive care unit), infected, and susceptible cases. Among these, the main outcome studied, death, was reported in 313 articles (76.2%) [16,17,18,19,20,21,22, 25, 26, 28, 29, 31,32,33,34,35,36,37,38,39,40,41,42,43,44,45, 47,48,49,50, 52,53,54,55,56,57,58,59,60,61,62, 64,65,66, 68,69,70, 72,73,74, 76,77,78,79, 82,83,84,85,86,87,88,89,90,91, 93, 97,98,99,100, 102,103,104,105,106,107,108,109,110, 112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127, 129,130,131,132,133,134,135,136,137,138,139,140,141,142, 144,145,146,147,148, 150, 151, 153,154,155,156, 158, 159, 163, 164, 166,167,168,169,170, 172, 174,175,176, 178,179,180,181, 183, 184, 187,188,189, 193,194,195,196, 198, 202,203,204,205, 207, 210,211,212,213, 215, 217,218,219,220,221,222, 224,225,226,227,228,229,230,231, 235, 237, 240,241,242,243, 245,246,247,248, 250, 252,253,254,255,256, 258,259,260,261, 263,264,265,266,267, 269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288, 290,291,292,293,294, 300, 301, 305, 306, 308, 310,311,312, 314, 315, 317,318,319,320,321,322,323,324,325,326, 328,329,330,331,332,333,334,335,336,337, 339,340,341,342, 344,345,346, 348,349,350,351,352,353,354,355, 358,359,360, 362,363,364,365,366,367,368, 370, 371, 374, 375, 377, 384, 385, 387,388,389,390, 392,393,394,395, 397, 398, 400, 401, 403, 404, 406, 408,409,410,411,412,413,414,415,416,417,418,419,420,421, 423, 424]. Notably, the majority of these articles, 218 (53%), were conducted in high-income countries [16, 17, 20,21,22, 26, 29, 31, 33, 34, 37, 39,40,41,42,43, 47,48,49, 52, 57,58,59, 61, 62, 66, 68,69,70, 72,73,74, 76, 77, 79, 82,83,84,85,86,87, 90, 93, 98,99,100, 102, 106,107,108,109,110, 112,113,114, 116,117,118,119,120,121,122,123,124, 126, 127, 130,131,132,133,134,135,136,137, 140, 142, 145, 147, 150, 151, 153,154,155,156, 158, 159, 164, 167, 169, 170, 172, 175, 178,179,180,181, 183, 184, 187, 188, 193,194,195, 198, 202, 204, 205, 207, 211, 212, 217, 220, 222, 224, 227, 235, 237, 240,241,242,243, 245,246,247,248, 250, 252, 254, 255, 258, 260, 261, 263,264,265,266,267, 269,270,271,272,273,274,275,276,277,278,279,280,281,282,283, 285, 286, 288, 290,291,292,293,294, 300, 310, 314, 315, 317, 323, 324, 326, 328, 332, 333, 335,336,337, 340, 342, 344, 345, 348, 349, 351,352,353, 355, 358,359,360, 362,363,364,365,366,367,368, 374, 377, 384, 385, 387,388,389,390, 393, 394, 397, 400, 401, 403, 404, 410, 412, 415, 416, 418, 420, 421, 423, 424].
In terms of the health outcomes studied, 270 references (65.7%) included the number of recovered cases. Additionally, 189 articles (46%) reported the number of hospitalizations, while 45 articles (10.9%) incorporated the count of infected cases [30, 60, 69, 73,74,75, 81, 95, 101, 148, 152, 159, 164, 168, 172, 187, 189, 198, 200, 207,208,209, 215, 224, 226, 227, 232, 239, 251, 257, 260, 279, 284, 351, 356, 372, 373, 377, 379, 382, 386, 390, 405, 410, 415] (see Table 6).
Methodological quality of the studies
Methodological evaluation was conducted on 402 articles (97.8%) [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83, 85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109, 111,112,113,114,115,116,117,118,119,120,121, 123, 126, 128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195, 197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301, 303,304,305,306,307,308,309,310,311,312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343,344,345,346,347,348,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400, 402,403,404,405,406,407,408,409,410,411,412,413,414,415,416,417,418,419,420,421,422,423,424,425,426]. However, the checklist was not applied to nine articles (2.2%) due to their nature as letters to the editor or comments [83, 87, 106, 113, 115, 119, 188, 204, 351].
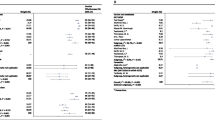
Upon using the JBI tool, it was determined that 135 articles (33.6%) were at high risk due to a lack of description regarding the studied population [16,17,18, 20, 22,23,24, 30,31,32,33, 40, 41, 43,44,45,46, 49, 57, 59, 67, 78, 82, 88, 89, 94, 97, 98, 101, 102, 107, 108, 111, 132, 137, 138, 151,152,153,154, 162, 163, 165, 166, 172, 175, 176, 178,179,180, 182, 189, 190, 194, 202, 203, 205, 207, 208, 211, 212, 214, 215, 220, 222, 224, 228, 231, 232, 234,235,236, 239, 241, 246, 248, 250, 252, 253, 255, 257, 259, 261,262,263,264, 267,268,269, 271,272,273,274,275, 279, 281, 283, 286, 289,290,291,292, 295,296,297, 300, 301, 309, 315, 316, 318, 319, 323, 332, 334, 345, 348, 351, 353, 360, 364, 365, 369, 371, 374, 377, 379, 380, 382, 384, 387, 404, 414, 418]. Conversely, 247 articles (61.4%) were deemed low risk as they met the methodological domains outlined in the quality tool. Additionally, 20 articles (5.0%) [27, 35, 109, 125, 136, 155, 160, 169, 173, 198, 247, 261, 311, 324, 344, 368, 389, 403, 405, 423] were categorized as unclear due to insufficient methodological information.
In applying the PROBAST tool, it was concluded that 65.3% of the articles presented a low risk in the bias risk domain. On the other hand, in the applicability domain, 89.8% reported a low risk. Articles classified as high risk in the bias risk domain often lacked information about the population studied. In contrast, those classified as unclear in the applicability domain lacked sufficient methodological details for evaluation. Many of these articles also lacked information on the methods used to control for third variables or analyze predictive outcomes (Supplement N°. 7).
Discussion
In this review, most models were developed in countries classified as high income, and the SEIR model was more frequently used. This research identified a considerable increase in these articles in the years 2021 (1650%) and 2022 (618.8%) compared to the initial year of the pandemic, a fact that reflects the unavailability of vaccines until the end of 2020.
High-income countries have used these strategies extensively to advise on health decision-making. In this sense, it is striking that only Singapore, the United Arab Emirates, South Korea, Japan, Italy, and Canada are among the countries that exceeded 80% of the population vaccinated [427]. The USA, where the largest number of identified models were developed, has one of the highest crude mortality rates from the disease, even after deploying vaccinations, suggesting a disconnect between the developers of the models and their actual implementation and articulation with public health.
This systematic review provided insight into the main features that have been incorporated into mathematical epidemiological models worldwide, allowing for a clear picture of the different advantages and disadvantages of the multiple analytical approaches to describe COVID-19 behavior and vaccine effectiveness. For governmental decision-making and depending on the public policy question to be answered, this research is a comprehensive compilation that provides sufficient information on the different options for scientific teams to choose from. Depending on the health outcomes to be predicted, the socio-demographic variables to be included, among other aspects, there is an amalgam of algorithms to carry out the mathematical epidemiological modeling.
One point to keep in mind during mathematical modeling in COVID-19 is that the inputs used should ideally come from reliable sources close to the context of the community in which the model is being applied. Hence the importance of an effective surveillance system in capturing cases and outcomes of the disease. Many high-income countries opted to use new technologies to analyze patterns of cases, to strengthen their surveillance system [428].
Among the main advantages of mathematical modeling in infectious diseases and in the context of public health are the multiple representations of scenarios, which can predict essential health outcomes at lower costs [429]. However, the realization of these models often implies the need to financially support multidisciplinary groups carrying out such processes. Unfortunately, not all institutions and governments can afford this. In our systematic review, this gap becomes visible in the scientific production of high-income countries compared to lower-middle and low-income countries.
One limitation of this study is that the predictive capacity of the analytical models was not reviewed, given the impossibility of measuring this characteristic homogeneously. In addition, unfortunately, most of the articles did not present their open programming codes, making it impossible to replicate and review their computational developments. Another limitation of this research was that it was not possible to take into account predictive models used (by some governments) that were useful for decision-making, because some governments considered it a national security issue and never shared these advances with society.
Although the most widely used model (SEIR, in its classic version) has limitations [430], such as the absence of a defined case model, discrepancies in the information available at the population level compared to the individual [431], a lack of incorporation of individual behavior and social influence, and the lack of flexibility to incorporate new evidence [432], it is a very useful and practical model for different purposes in environments with high uncertainty. Therefore, it is necessary to dynamically adjust the models to the reality of the evolution of the pandemic.
Based on our exhaustive compilation, we consider it good international practice for future analytical modeling of infectious diseases to (i) use as many parameters as possible from real-world evidence from the area being studied; (ii) be clear about the mathematical structure of the model being applied (annexes can provide such details of the document); (iii) show all the parameters with which the basis of the exercise is modeled; and (iv) where possible leave the programming code open or available on request to the reader.
Likewise, one of the significant challenges at present is to know the impact of vaccination (effectiveness) in the long term, whether hybrid protection (natural and vaccine immunity) is better, and what vaccination schemes (one, two, three, or four doses) or what type of heterologous schemes produce a greater response. Mathematical modeling is of great help in epidemiology and public health; however, increasing the number of parameters can make the analysis, calibration, implementation, and interpretation of results difficult.
Epidemiological mathematical models are a tool that allows us to predict the behavior of the virus, with certain limitations, providing information for decision-making on public health control measures. The development of more and better epidemiological mathematical models in public health serves as a tool to mitigate negative scenarios and to aid policymakers in navigating through uncertain contexts. It will be essential to standardize the methods used for epidemiological modeling to guarantee high-quality results. Similarly, it will be vital to ensure human and financial resources so that these models are made in the best possible way, with accurate data and in real time. Thus, health policies must be based on evidence to generate the best results in the population.
Availability of data and materials
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
References
Basavaraju S, Aswathanarayan J, Basavegowda M, Somanathan B. Coronavirus: occurrence, surveillance, and persistence in wastewater. Environ Monit Assess. 2021;193:508. https://doi.org/10.1007/s10661-021-09303-8.
Estrada J, Ospina J, Hincapié M, Gómez M. Estimación del intervalo serial y número reproductivo básico para los casos importados de COVID-19. Rev Salud Pública. 2020;22(2):194–7. https://doi.org/10.15446/rsap.V22n2.87492.
The New York Times. Covid world vaccination tracker. 2022. Cited 2022 Sep 12. Available from: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html.
Andeweg SP, de Gier B, Eggink D, van den Ende C, van Maarseveen N, Ali L, et al. Protection of COVID-19 vaccination and previous infection against Omicron BA.1, BA.2 and Delta SARS-CoV-2 infections. Nat Commun. 2022;13(1):1–9. https://doi.org/10.1038/s41467-022-31838-8.
Watson O, Barnsley G, Toor J, Hogan A, Winskill P, Ghani A. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022;22(9):1293–302. https://doi.org/10.1016/S1473-3099(22)00320-6.
Sharma K, Koirala A, Nicolopoulos K, Chiu C, Wood N, Britton P. Vaccines for COVID-19: where do we stand in 2021? Paediatr Respir Rev. 2021;39:22–31. https://doi.org/10.1016/j.prrv.2021.07.001.
Alahmadi A, Belet S, Black A, Cromer D, Flegg J, House T, et al. Influencing public health policy with data-informed mathematical models of infectious diseases: recent developments and new challenges. Epidemics. 2020;32:100393. https://doi.org/10.1016/j.epidem.2020.100393.
Wei Y, Sha F, Zhao Y, Jiang Q, Hao Y, Chen F. Better modelling of infectious diseases: lessons from covid-19 in China. BMJ. 2021;375. https://doi.org/10.1136/bmj.n2365.
Garritty C, Gartlehner G, Kamel C, King V, Nussbaumer-Streit B, Stevens A, et al. Interim guidance from the cochrane rapid reviews methods group. Cochrane Rapid Rev. 2020;2020(March):1–2. Available from: https://methods.cochrane.org/sites/methods.cochrane.org.rapidreviews/files/uploads/cochrane_rr_-_guidance-23mar2020-final.pdf.
Kitchenham B, Budgen D, Brereton P. Evidence-based software engineering and systematic reviews. Chapman and Hall/CRC; 2015. ISBN 9780367575335.
Kitchenham B, Charters S. Guidelines for performing systematic literature reviews in software engineering. Version 2.3. EBSE Technical Report EBSE-2007-01. 2007. Available from: https://legacyfileshare.elsevier.com/promis_misc/525444systematicreviewsguide.pdf.
Hamadeh N, Van Rompaey C, Metreau E. New World Bank country classifications by income level: 2021-2022. World Bank Blogs. 2021. Cited 2022 Sep 12. Available from: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2021-2022.
Munn Z, Stern C, Aromataris E, Lockwood C, Jordan Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. 2018;18(1):1–9. https://doi.org/10.1186/s12874-017-0468-4.
The Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition. 2014.
Wolff R, Moons K, Riley R, Whiting P, Westwood M, Collins G, et al. PROBAST: a tool to assess the risk of bias and applicability of prediction model studies. Ann Intern Med. 2019;170(1):51–8. https://doi.org/10.7326/M18-1376.
Babus A, Das S, Lee S. The optimal allocation of COVID-19 vaccines. medRxiv. 2020. https://doi.org/10.1101/2020.07.22.20160143.
Bartsch S, O’Shea K, Ferguson M, Bottazzi M, Wedlock P, Strych U, et al. Vaccine efficacy needed for a COVID-19 coronavirus vaccine to prevent or stop an epidemic as the sole intervention. Am J Prev Med. 2020;59(4):493–503. https://doi.org/10.1016/j.amepre.2020.06.011.
Chinazzi M, Davis J, Dean N, Mu K, Pastore y Piontti A, Xiong X, et al. Estimating the effect of cooperative versus uncooperative strategies of COVID-19 vaccine allocation: a modeling study. 2020.
Ghosh S, Ghosh S. COVID-19: risks of re-emergence, re-infection, and control measures - a long term modelling study. medRxiv. 2020. https://doi.org/10.1101/2020.09.19.20198051.
Giacopelli G. A full-scale agent-based model of Lombardy COVID-19 dynamics to explore social networks connectivity and vaccine impact on epidemic. medRxiv. 2020. https://doi.org/10.1101/2020.09.13.20193599.
Glover A, Heathcote J, Krueger D, Rios-Rull J-V. Health versus wealth: on the distributional effects of controlling a pandemic. NBER working papers SSRN. 2020;27046. https://doi.org/10.3386/w27046.
Good M, Hawkes M. The interaction of natural and vaccine-induced immunity with social distancing predicts the evolution of the COVID-19 pandemic. MBio. 2020;11(5):e02617–20. https://doi.org/10.1128/mbio.02617-20.
Guerstein S, Romeo-Aznar V, Dekel M, Miron O, Davidovitch N, Puzis R, et al. Optimal strategies for combining vaccine prioritization and social distancing to reduce hospitalizations and mitigate COVID19 progression. medRxiv. 2020. https://doi.org/10.1101/2020.12.22.20248622.
Iboi E, Ngonghala C, Gumel A. Will an imperfect vaccine curtail the COVID-19 pandemic in the U.S.? Infect Dis Model. 2020;5:510–24. https://doi.org/10.1016/j.idm.2020.07.006.
Makhoul M, Ayoub H, Chemaitelly H, Seedat S, Mumtaz G, Al-Omari S, et al. Epidemiological impact of SARS-CoV-2 vaccination: mathematical modeling analyses. Vaccines. 2020;8(4):668. https://doi.org/10.3390/vaccines8040668.
Matrajt L, Eaton J, Leung T, Brown E. Vaccine optimization for COVID-19: who to vaccinate first? Sci Adv. 2021;7(6):eabf1374. https://doi.org/10.1126/sciadv.abf1374.
Mukandavire Z, Nyabadza F, Malunguza N, Cuadros D, Shiri T, Musuka G. Quantifying early COVID-19 outbreak transmission in South Africa and exploring vaccine efficacy scenarios. PLoS One. 2020;15(7):e0236003. https://doi.org/10.1371/journal.pone.0236003.
Musa R, Ezugwu A, Mbah G. Assessment of the impacts of pharmaceutical and non-pharmaceutical intervention on COVID-19 in South Africa using mathematical model. medRxiv. 2020. https://doi.org/10.1101/2020.11.13.20231159.
Swan D, Goyal A, Bracis C, Moore M, Krantz E, Brown E, et al. Vaccines that prevent SARS-CoV-2 transmission may prevent or dampen a spring wave of COVID-19 cases and deaths in 2021. medRxiv. 2020. https://doi.org/10.1101/2020.12.13.20248120.
Braun P, Haffner S, Woodcock B. COVID-19 pandemic predictions using the modified Bateman SIZ model and observational data for Heidelberg, Germany: effect of vaccination with a SARS-CoV-2 vaccine, coronavirus testing and application of the Corona-Warn-App. Int J Clin Pharmacol Ther. 2020;58(8):417. https://doi.org/10.5414/CP203846.
Chen X, Li M, Simchi-Levi D, Zhao T. Allocation of COVID-19 vaccines under limited supply. medRxiv. 2020. https://doi.org/10.1101/2020.08.23.20179820.
Acuña-Zegarra M, Díaz-Infante S, Baca-Carrasco D, Olmos-Liceaga D. COVID-19 optimal vaccination policies: a modeling study on efficacy, natural and vaccine-induced immunity responses. Math Biosci. 2021;337:108614. https://doi.org/10.1016/j.mbs.2021.108614.
Adibi A, Mozafarihashjin M, Sadatsafavi M. Continuing COVID-19 vaccination of front-line workers in british columbia with the Astrazeneca vaccine: benefits in the face of increased risk for prothrombotic thrombocytopenia. medRxiv. 2021. https://doi.org/10.1101/2021.04.11.21255138.
Albani V, Loria J, Massad E, Zubelli J. The impact of COVID-19 vaccination delay: a data-driven modeling analysis for Chicago and New York City. Vaccine. 2021;39(41):6088–94. https://doi.org/10.1016/j.vaccine.2021.08.098.
Flores-Arguedas H, Camacho-Gutiérrez J, Saldaña F. Estimating the impact of non-pharmaceutical interventions and vaccination on the progress of the COVID-19 epidemic in Mexico: a mathematical approach. arXiv. 2021. https://doi.org/10.48550/arXiv.2102.11071.
Foy B, Wahl B, Mehta K, Shet A, Menon G, Britto C. Comparing COVID-19 vaccine allocation strategies in India: a mathematical modelling study. Int J Infect Dis. 2021;103:431–8. https://doi.org/10.1016/j.ijid.2020.12.075.
Frieswijk K, Zino L, Cao M. Modelling the effect of vaccination and human behaviour on the spread of epidemic diseases on temporal networks. arXiv. 2021. http://arxiv.org/abs/2111.05590.
Fuady A, Nuraini N, Sukandar K, Lestari B. Targeted vaccine allocation could increase the COVID-19 vaccine benefits amidst its lack of availability: a mathematical modeling study in Indonesia. Vaccines. 2021;9(5):462. https://doi.org/10.3390/vaccines9050462.
Fujii D, Nakata T. COVID-19 and output in Japan. Japanese Econ Rev. 2021;72(4):609–50. https://doi.org/10.1007/s42973-021-00098-4.
Furuse Y. Simulation of future COVID-19 epidemic by vaccination coverage scenarios in Japan. J Glob Health. 2021;11:1–11. https://doi.org/10.7189/jogh.11.05025.
Gabriele-Rivet V, Spence K, Ogden N, Fazil A, Turgeon P, Otten A, et al. Modelling the impact of age-stratified public health measures on SARS-CoV-2 transmission in Canada. R Soc Open Sci. 2021;8(11):210834. https://doi.org/10.1098/rsos.210834.
Galanti M, Pei S, Yamana T, Angulo F, Charos A, Khan F, et al. Non-pharmaceutical interventions and inoculation rate shape SARS-CoV-2 vaccination campaign success. Epidemiol Infect. 2021;149(e222,1):1–8. https://doi.org/10.1017/S095026882100217X.
Galloway S, Paul P, MacCannell D, Johansson M, Brooks J, MacNeil A, et al. Emergence of SARS-CoV-2 B.1.1.7 lineage. Morb Mortal Wkly Rep. 2021;70(3):95–9. https://doi.org/10.15585/mmwr.mm7003e2.
Ganesan S, Subramani D, Anandh T, Ghose D, Babu G. Ensemble forecast of COVID-19 for vulnerability assessment and policy interventions. 2021. https://doi.org/10.1101/2021.08.31.21262943.
Aldila D, Samiadji B, Simorangkir G, Khosnaw S, Shahzad M. Impact of early detection and vaccination strategy in COVID-19 eradication program in Jakarta Indonesia. BMC Res Notes. 2021;14(1):1–7. https://doi.org/10.1186/s13104-021-05540-9.
Di Giamberardino P, Iacoviello D. Optimal exit strategy design for COVID-19. In: International Conference on System Theory, Control and Computing. 2021:372–7. https://doi.org/10.1109/ICSTCC52150.2021.9607220.
Glover A, Heathcote J, Krueger D. Optimal age-based vaccination and economic mitigation policies for the second phase of the COVID-19. J Econ Dyn Control. 2022;140:104306. https://doi.org/10.1016/j.jedc.2022.104306.
Goldstein J, Cassidy T, Wachter K. Vaccinating the oldest against COVID-19 saves both the most lives and most years of life. Proc Natl Acad Sci. 2021;118(11):e2026322118. https://doi.org/10.1073/pnas.2026322118.
Gonzalez-Parra G. Analysis of delayed vaccination regimens: a mathematical modeling approach. Epidemiologia. 2021;2(3):271–93. https://doi.org/10.3390/epidemiologia2030021.
Gozzi N, Bajardi P, Perra N. The importance of non-pharmaceutical interventions during the COVID-19 vaccine rollout. PLoS Comput Biol. 2021;17(9):e1009346. https://doi.org/10.1371/journal.pcbi.1009346.
Gumel A, Iboi E, Ngonghala C, Ngwa G. Toward achieving a vaccine-derived herd immunity threshold for COVID-19 in the U.S. Front Public Heal. 2021;9:1–22. https://doi.org/10.3389/fpubh.2021.709369.
Guzmán-Merino M, Durán C, Marinescu MC, Delgado-Sanz C, Gomez-Barroso D, Carretero J, et al. Assessing population-sampling strategies for reducing the COVID-19 incidence. Comput Biol Med. 2021;139:1–10. https://doi.org/10.1016/j.compbiomed.2021.104938.
Hagens A, Çağkan A, Yildirak K, Sancar M, van der Schans J, Acar A, et al. COVID-19 vaccination scenarios: a cost-effectiveness analysis for Turkey. Vaccines. 2021;9(4):399. https://doi.org/10.3390/vaccines9040399.
Hammoumi A, Hmarrass H, Qesmi R. Impact of booster COVID-19 vaccine for Moroccan adults: a discrete age-structured model approach. medRxiv. 2021. https://doi.org/10.1101/2021.03.14.21253555.
Han S, Cai J, Yang J, Zhang J, Wu Q, Zheng W, et al. Time-varying optimization of COVID-19 vaccine prioritization in the context of limited vaccination capacity. Nat Commun. 2021;12(1):1–10. https://doi.org/10.1038/s41467-021-24872-5.
Almajose A, White A, Diego C, Lazaro R, Austriaco N. A 2SIR-VD model for optimizing geographical COVID-19 vaccine distribution in the Philippines. medRxiv. 2021. https://doi.org/10.1101/2021.05.20.21257556.
Hartnett G, Parker E, Gulden T, Vardavas R, Kravitz D. Modelling the impact of social distancing and targeted vaccination on the spread of COVID-19 through a real city-scale contact network. J Complex Networks. 2021;9(6):cnab042. https://doi.org/10.1093/comnet/cnab042.
Hinch R, Probert W, Nurtay A, Kendall M, Wymant C, Hall M, et al. OpenABM-Covid19-an agent-based model for non-pharmaceutical interventions against COVID-19 including contact tracing. PLoS Comput Biol. 2021;17(7):e1009146. https://doi.org/10.1371/journal.pcbi.1009146.
Hoertel N, Blachier M, Limosin F, Sánchez-Rico M, Blanco C, Olfson M, et al. Optimizing SARS-CoV-2 vaccination strategies in France: results from a stochastic agent-based model. medRxiv. 2021. https://doi.org/10.1101/2021.01.17.21249970.
Hogan A, Winskill P, Watson O, Walker P, Whittaker C, Baguelin M, et al. Within-country age-based prioritisation, global allocation, and public health impact of a vaccine against SARS-CoV-2: a mathematical modelling analysis. Vaccine. 2021;39(22):2995–3006. https://doi.org/10.1016/j.vaccine.2021.04.002.
Hohenegger S, Cacciapaglia G, Sannino F. Effective mathematical modelling of health passes during a pandemic. Sci Rep. 2022;12(1):1–13. https://doi.org/10.1038/s41598-022-10663-5.
Holmdahl I, Kahn R, Slifka K, Dooling K, Slayton R. Modeling the impact of vaccination strategies for nursing homes in the context of increased SARS-CoV-2 community transmission and variants. Clin Infect Dis. 2022;1–4. https://doi.org/10.1093/cid/ciac062.
Huang B, Wang J, Cai J, Yao S, Sheung P, Hong-Wing T, et al. Integrated vaccination and physical distancing interventions to prevent future COVID-19 waves in Chinese cities. Nat Hum Behav. 2021;5(6):695–705. https://doi.org/10.1038/s41562-021-01063-2.
Jabłońska K, Aballéa S, Toumi M. The real-life impact of vaccination on COVID-19 mortality in Europe and Israel. Public Health. 2021;198:230–7. https://doi.org/10.1016/j.puhe.2021.07.037.
Jayasundara P, Peariasamy K, Law K, Abd K, Wai S, Ghazali, Izzuna Abayawardana M, et al. Sustaining effective COVID-19 control in Malaysia through large-scale vaccination. Epidemics. 2021;37:100517. https://doi.org/10.1016/j.epidem.2021.100517.
Jentsch P, Anand M, Bauch C. Prioritising COVID-19 vaccination in changing social and epidemiological landscapes: a mathematical modelling study. Lancet Infect Dis. 2021;21(8):1097–106. https://doi.org/10.1016/S1473-3099(21)00057-8.
Amaku M, Covas D, Coutinho F, Azevedo R, Massad E. Modelling the impact of delaying vaccination against SARS-CoV-2 assuming unlimited vaccine supply. Theor Biol Med Model. 2021;18(1):1–11. https://doi.org/10.1186/s12976-021-00143-0.
Jiménez-Rodríguez P, Muñoz-Fernández G, Rodrigo-Chocano J, Seoane-Sepúlveda J, Weber A. A population structure-sensitive mathematical model assessing the effects of vaccination during the third surge of COVID-19 in Italy. J Math Anal Appl. 2021;514(2):125975. https://doi.org/10.1016/j.jmaa.2021.125975.
Karabay A, Kuzdeuov A, Ospanova S, Lewis M, Varol H. A vaccination simulator for COVID-19: effective and sterilizing immunization cases. IEEE J Biomed Heal informatics. 2021;25(12):4317–27. https://doi.org/10.1109/JBHI.2021.3114180.
Karabay A, Kuzdeuov A, Atakan H. COVID-19 vaccination strategies considering hesitancy using particle-based epidemic simulation. In: 43rd Annu Int Conf IEEE Eng Med Biol Soc; 2021: 1985–8. https://doi.org/10.1109/EMBC46164.2021.9630797.
Kassa S, Njagarah J, Terefe Y. Modelling COVID-19 mitigation and control strategies in the presence of migration and vaccination: the case of South Africa. Afrika Mat. 2021;32(7):1295–322. https://doi.org/10.1007/s13370-021-00900-x.
Keeling M, Brooks-Pollock E, Challen R, Danon L, Dyson L, Gog J, et al. Short-term projections based on early Omicron variant dynamics in England. medRxiv. 2021. https://doi.org/10.1101/2021.12.30.21268307.
Kemp F, Proverbio D, Aalto A, Mombaerts L, D’Hérouël A, Husch A, et al. Modelling COVID-19 dynamics and potential for herd immunity by vaccination in Austria. Luxembourg and Sweden J Theor Biol. 2021;530(110874):1–29. https://doi.org/10.1016/j.jtbi.2021.110874.
Kerr C, Stuart R, Mistry D, Abeysuriya R, Rosenfeld K, Hart G, et al. Covasim: an agent-based model of COVID-19 dynamics and interventions. PLoS Comput Biol. 2021;17(7):e1009149. https://doi.org/10.1371/journal.pcbi.1009149.
Khan T, Ullah R, Zaman G, El Khatib Y. Modeling the dynamics of the SARS-CoV-2 virus in a population with asymptomatic and symptomatic infected individuals and vaccination. Phys Scr. 2021;96(10):104009. https://doi.org/10.1088/1402-4896/ac0e00.
Kim D, Pekgün P, Yildirim I, Keskinocak P. Resource allocation for different types of vaccines against COVID-19: tradeoffs and synergies between efficacy and reach. Vaccine. 2021;39(47):6876–82. https://doi.org/10.1016/j.vaccine.2021.10.025.
Kirwin E, Rafferty E, Harback K, Round J, McCabe C. A net benefit approach for the optimal allocation of a COVID-19 vaccine. Pharmacoeconomics. 2021;39(9):1059–73. https://doi.org/10.1007/s40273-021-01037-2.
Amaral F, Casaca W, Oishi C, Cuminato J. Simulating immunization campaigns and vaccine protection against COVID-19 pandemic in Brazil. IEEE Access. 2021;9:126011–22. https://doi.org/10.1109/ACCESS.2021.3112036.
Kitano T, Aoki H. The incremental burden of invasive pneumococcal disease associated with a decline in childhood vaccination using a dynamic transmission model in Japan: a secondary impact of COVID-19. Comput Biol Med. 2021;133:104429. https://doi.org/10.1016/j.compbiomed.2021.104429.
Ko Y, Lee J, Seo Y, Jung E. Risk of COVID-19 transmission in heterogeneous age groups and effective vaccination strategy in Korea: a mathematical modeling study. Epidemiol Health. 2021;43:1–9. https://doi.org/10.4178/epih.e2021059.
Kou L, Wang X, Li Y, Guo X, Zhang H. A multi-scale agent-based model of infectious disease transmission to assess the impact of vaccination and non-pharmaceutical interventions: the COVID-19 case. J Saf Sci Resil. 2021;2(4):199–207. https://doi.org/10.1016/j.jnlssr.2021.08.005.
Kraay A, Gallagher M, Ge Y, Han P, Baker J, Koelle K, et al. Modeling the use of SARS-CoV-2 vaccination to safely relax non-pharmaceutical interventions. medRxiv. 2021. https://doi.org/10.1101/2021.03.12.21253481.
Latkowski R, Dunin-Keplicz B. An agent-based COVID-19 simulator: extending Covasim to the Polish context. Promedia Comput Sci. 2021;192:3607–16. https://doi.org/10.1016/j.procs.2021.09.134.
Lau C, Mayfield H, Sinclair J, Brown S, Waller M, Enjeti A, et al. Risk-benefit analysis of the AstraZeneca COVID-19 vaccine in Australia using a Bayesian network modelling framework. Vaccine. 2021;39(51):7429–40. https://doi.org/10.1016/j.vaccine.2021.10.079.
Lee E, Li Z, Liu Y, LeDuc J. Strategies for vaccine prioritization and mass dispensing. Vaccines. 2021;9(5):506–30. https://doi.org/10.3390/vaccines9050506.
Lemaitre J, Pasetto D, Zanon M, Bertuzzo E, Mari L, Miccoli S, et al. Optimizing the spatual allocation of COVID-19 vaccines: Italy as a case study. medRxiv. 2022. https://doi.org/10.1101/2021.05.06.21256732.
León T, Vargo J, Pan E, Jain S, Shete P. Nonpharmaceutical interventions remain essential to reducing coronavirus disease 2019 burden even in a well-vaccinated society: a modeling study. Open Forum Infect Dis. 2021;8(9):ofab415. https://doi.org/10.1093/ofid/ofab415.
Leung K, Wu J, Leung G. Effects of adjusting public health, travel, and social measures during the roll-out of COVID-19 vaccination: a modelling study. Lancet Public Health. 2021;6(9):e674–82. https://doi.org/10.1016/S2468-2667(21)00167-5.
Amouch M, Karim N. Modeling the dynamic of COVID-19 with different types of transmissions. Chaos Solitons Fractals. 2021;150:111188. https://doi.org/10.1016/j.chaos.2021.111188.
Li J, Giabbanelli P. Returning to a normal life via COVID-19 vaccines in the United States: a large-scale agent-based simulation study. JMIR Med informatics. 2021;9(4):e27419. https://doi.org/10.2196/27419.
Li K, Zhao Z, Wei H, Rui J, Huang J, Guo X, et al. Feasibility of booster vaccination in high-risk populations for controlling coronavirus variants - China, 2021. China CDC Wkly. 2021;3:1071–4. https://doi.org/10.46234/ccdcw2021.259.
Li R, Bjørnstad O, Stenseth N. Prioritizing vaccination by age and social activity to advance societal health benefits in Norway: a modelling study. Lancet Reg Heal Eur. 2021;10:1–7. https://doi.org/10.1016/j.lanepe.2021.100200.
Li R, Li Y, Zou Z, Liu Y, Li X, Zhuang G, et al. Evaluating the impact of SARS-CoV-2 variants on the COVID-19 epidemic and social restoration in the United States: a mathematical modelling study. Front Public Heal. 2022;2067:1–9. https://doi.org/10.3389/fpubh.2021.801763.
Li Y, Ge L, Zhou Y, Cao X, Zheng J. Toward the impact of non-pharmaceutical interventions and vaccination on the COVID-19 pandemic with time-dependent SEIR model. Front Artif Intell. 2021;4:648579. https://doi.org/10.3389/frai.2021.648579.
Li Y, Hu T, Gai X, Zhang Y, Zhou X. Transmission dynamics, heterogeneity and controllability of SARS-CoV-2: a rural-urban comparison. Int J Environ Res Public Health. 2021;18(10):5221. https://doi.org/10.3390/ijerph18105221.
Li Z, Wang J, Yang B, Li W, Xu J-G, Wang T. Impact of non-pharmacological interventions on COVID-19 boosting vaccine prioritization and vaccine-induced herd immunity: a population-stratified modelling study. medRxiv. 2021. https://doi.org/10.1101/2021.10.27.21265522.
Luo T, Cao Z, Zhao P, Zeng D, Zhang Q. Evaluating the impact of vaccination on COVID-19 pandemic used a hierarchical weighted contact network model. In: IEEE International Conference on Intelligence and Security Informatics; 2021. p. 1–6. https://doi.org/10.1109/ISI53945.2021.9624841.
Mahmoud N, Tsoungui H, Ngucho Y, Kwamou S, Kayanula L, Kamanga G, et al. The impact of COVID-19 vaccination campaigns accounting for antibody-dependent enhancement. PLoS One. 2021;16(4):e0245417. https://doi.org/10.1371/journal.pone.0245417.
Maier B, Burdinski A, Rose A, Schlosser F, Hinrichs D, Betsch C, et al. Potential benefits of delaying the second mRNA COVID-19 vaccine dose. arXiv. 2022. https://doi.org/10.48550/arXiv.2102.13600.
Antonini C, Calandrini S, Bianconi F. A modeling study on vaccination and spread of SARS-CoV-2 variants in Italy. Vaccines. 2021;9(8):915. https://doi.org/10.3390/vaccines9080915.
Mairanowski F, Below D. Functional dependence of COVID-19 growth rate on lockdown conditions and rate of vaccination. medRxiv. 2021. https://doi.org/10.1101/2021.06.06.21258425.
Mairanowski F, Below D. The age-stratified analytical model for the spread of the COVID-19 epidemic. medRxiv. 2021. https://doi.org/10.1101/2021.07.13.21260459.
Makhoul M, Chemaitelly H, Ayoub H, Seedat S, Abu-Raddad L. Epidemiological differences in the impact of COVID-19 vaccination in the United States and China. Vaccines. 2021;9(3):1–13. https://doi.org/10.3390/vaccines9030223.
Mandal S, Arinaminpathy N, Bhargava B, Panda S. India’s pragmatic vaccination strategy against COVID-19: a mathematical modelling-based analysis. BMJ Open. 2021;11(7):e048874. https://doi.org/10.1136/bmjopen-2021-048874.
Mandal S, Arinaminpathy N, Bhargava B, Panda S. Plausibility of a third wave of COVID-19 in India: a mathematical modelling based analysis. Indian Journal of Medical Research. 2021;153(5):522–32. https://doi.org/10.4103/ijmr.ijmr_1627_21.
Marín-Hernández D, Nixon D, Hupert N. Anticipated reduction in COVID-19 mortality due to population-wide BCG vaccination: evidence from Germany. Hum Vaccin Immunother. 2021;17(8):2451–3. https://doi.org/10.1080/21645515.2021.1872344.
Martínez-Rodríguez D, Gonzalez-Parra G, Villanueva R-J, Martínez-Rodríguez D, Gonzalez-Parra G, Villanueva R-J. Analysis of key factors of a SARS-CoV-2 vaccination program: a mathematical modeling approach. Epidemiologia. 2021;2(2):140–61. https://doi.org/10.1101/2021.02.19.21252095.
Marziano V, Guzzetta G, Mammone A, Riccardo F, Poletti P, Trentini F, et al. The effect of COVID-19 vaccination in Italy and perspectives for living with the virus. Nature Communications. 2021;12(1):1–8. https://doi.org/10.1038/s41467-021-27532-w.
Massonnaud C, Roux J, Colizza V, Crépey P. Evaluating COVID-19 booster vaccination strategies in a partially vaccinated population: a modeling study. Vaccines. 2021;10(3):479–92. https://doi.org/10.3390/vaccines10030479.
Mathiot J-F, Gerbaud L, Breton V. Highlighting the impact of social relationships on the propagation of respiratory viruses using percolation theory. Sci Rep. 2021;11(1):1–9. https://doi.org/10.1038/s41598-021-03812-9.
Are E, Song Y, Stockdale J, Tupper P, Colijn C. COVID-19 endgame: from pandemic to endemic? Vaccination, reopening and evolution in a well-vaccinated population. medRxiv. 2021. https://doi.org/10.1101/2021.12.18.21268002.
Matrajt L, Eaton J, Leung T, Dimitrov D, Schiffer J, Swan D, et al. Optimizing vaccine allocation for COVID-19 vaccines: potential role of single-dose vaccination. Nature Communications. 2021;12(1):1–18. https://doi.org/10.1038/s41467-021-23761-1.
Matrajt L, Janes H, Schiffer J, Dimitrov D. Quantifying the impact of lifting community nonpharmaceutical interventions for COVID-19 during vaccination rollout in the United States. Open Forum Infectious Diseases. 2021;8(7):ofab341. https://doi.org/10.1093/ofid/ofab341.
McBryde E, Meehan M, Caldwell J, Adekunle A, Ogunlade S, Kuddus M, et al. Modelling direct and herd protection effects of vaccination against the SARS-CoV-2 Delta variant in Australia. Med J Australia. 2021;215:427–32. https://doi.org/10.5694/mja2.51263.
Michael E. Projections and management of the COVID-19 emergency in India. Research Square. 2021. https://doi.org/10.21203/rs.3.rs-575258/v1.
Min K-D, Tak S. Dynamics of the COVID-19 epidemic in the post-vaccination period in Korea: a rapid assessment. Epidemiology and Health. 2021;43:e2021040. https://doi.org/10.4178/epih.e2021040.
Miura F, Leung K, Klinkenberg D, Ainslie K, Wallinga J. Optimal vaccine allocation for COVID-19 in the Netherlands: a data-driven prioritization. PLoS Computational Biology. 2021;17(12):e1009697. https://doi.org/10.1371/journal.pcbi.1009697.
Moghadas S, Fitzpatrick M, Shoukat A, Zhang K, Galvani A. Simulated identification of silent COVID-19 infections among children and estimated future infection rates with vaccination. JAMA Netw Open. 2021;4(4):e217097. https://doi.org/10.1001/jamanetworkopen.2021.7097.
Moghadas S, Sah P, Vilches T, Galvani A. Can the USA return to pre-COVID-19 normal by July 4?. Lancet Infect Dis. 2021;21(8):1073–4. https://doi.org/10.1016/S1473-3099(21)00324-8.
Moghadas S, Vilches T, Zhang K, Nourbakhsh S, Sah P, Fitzpatrick M, et al. Evaluation of COVID-19 vaccination strategies with a delayed second dose. PLoS Biology. 2021;19(4):e3001211. https://doi.org/10.1371/journal.pbio.3001211.
Moghadas S, Vilches T, Zhang K, Wells C, Shoukat A, Singer B, et al. The impact of vaccination on Coronavirus Disease 2019 (COVID-19) outbreaks in the United States. Clin Infect Dis. 2021;73(12):2257–64. https://doi.org/10.1093/cid/ciab079.
Arslan N, Morton D, Pichette J, Walkes D, Ancel L. Projections for Austin’s COVID-19 staged alert sytem, incorporating reported cases as additional indicator. 2021. Available from: https://covid-19.tacc.utexas.edu/media/filer_public/f9/58/f95850cc-1428-4966-8873-601bae0dc0e6/projections_for_austins_covid-19_staged_alert_system_incorporating_reported_cases_as_additional_indicator.pdf.
Moore S, Hill E, Dyson L, Tildesley M, Keeling M. Modelling optimal vaccination strategy for SARS-CoV-2 in the UK. PLoS Computat Biol. 2021;17(5):e1008849. https://doi.org/10.1371/journal.pcbi.1008849.
Moore S, Hill EM, Tildesley MJ, Dyson L, Keeling MJ. Vaccination and non-pharmaceutical interventions for COVID-19: a mathematical modelling study. Lancet Infect Dis. 2021;21(6):793–802. https://doi.org/10.1016/S1473-3099(21)00143-2.
Mumtaz G, El-Jardali F, Jabbour M, Harb A, Abu-Raddad L, Makhoul M. Modeling the impact of COVID-19 vaccination in Lebanon: a call to speed-up vaccine roll out. Vaccines. 2021;9(7):1–10. https://doi.org/10.3390/vaccines9070697.
Nam A, Ximenes R, Yeung M, Mishra S, Wu J, Tunis M, et al. Modelling the impact of extending dose intervals for COVID-19 vaccines in Canada. medRxiv. 2021. https://doi.org/10.1101/2021.04.07.21255094.
Nichita E, Pietrusiak M, Xie F, Schwanke P, Pandya A. Modeling COVID-19 transmission using IDSIM, an epidemiological-modelling desktop app with multi-level immunization capabilities. arXiv. 2021. https://arxiv.org/abs/2112.15252.
Nixon E, Thomas A, Stocks D, Barreaux A, Hemani G, Trickey A, et al. Impacts of vaccination and asymptomatic testing on SARS-CoV-2 transmission dynamics in a university setting. medRxiv. 2021. https://doi.org/10.1101/2021.11.22.21266565.
Nuraini N, Sukandar K, Hadisoemarto P, Susanto H, Hasan A, Sumarti N. Mathematical models for assessing vaccination scenarios in several provinces in Indonesia. Infect Dis Model. 2021;6:1236–58. https://doi.org/10.1016/j.idm.2021.09.002.
Omar O, Alnafisah Y, Elbarkouky R, Ahmed H. COVID-19 deterministic and stochastic modelling with optimized daily vaccinations in Saudi Arabia. Results Phys. 2021;28:104629. https://doi.org/10.1016/j.rinp.2021.104629.
Padula W, Malaviya S, Reid N, Cohen B, Chingcuanco F, Ballreich J, et al. Economic value of vaccines to address the COVID-19 pandemic: a U.S. cost-effectiveness and budget impact analysis. J Med Econ. 2021;24(1):1060–9. https://doi.org/10.1080/13696998.2021.1965732.
Pae B. Calibrating an SIR model for South Korea COVID-19 infections and predicting vaccination impact. medRxiv. 2021. https://doi.org/10.1101/2021.09.27.21264172.
Arslan N, Sürer Ö, Morton D, Yang H, Lachmann M, Woody S, et al. COVID-19 alert stages, healthcare projections and mortality patterns in Austin, Texas, May 2021 UT COVID-19 Modeling Consortium. 2021. Available from: https://covid-19.tacc.utexas.edu/media/filer_public/15/4d/154defa8-9217-478e-a459-8fc4144c61b5/austin_covid_alert_stage_and_mortality_trends_-_ut_-_may_2021.pdf.
Pageaud S, Ponthus N, Gauchon R, Pothier C, Rigotti C, Eyraud-Loisel A, et al. Adapting French COVID-19 vaccination campaign duration to variant dissemination. medRxiv. 2021. https://doi.org/10.1101/2021.03.17.21253739.
Paltiel A, Schwartz J. Assessing COVID-19 prevention strategies to permit the safe opening of residential colleges in fall 2021. Ann Intern Med. 2021;174(11):1563–71. https://doi.org/10.7326/m21-2965.
Parino F, Zino L, Calafiore G, Rizzo A. A model predictive control approach to optimally devise a two‐dose vaccination rollout: a case study on COVID‐19 in Italy. Int J robust nonlinear Control. 2021; 33(9):4808–23. https://doi.org/10.1002/rnc.5728.
Patel M, Rosenstrom E, Ivy J, Mayorga M, Keskinocak P, Boyce R, et al. Association of simulated COVID-19 vaccination and nonpharmaceutical interventions with infections, hospitalizations, and mortality. JAMA Netw Open. 2021;4(6):e2110782. https://doi.org/10.1001/jamanetworkopen.2021.10782.
Pearson C, Bozzani F, Procter S, Davies N, Huda M, Jensen H, et al. COVID-19 vaccination in Sindh Province, Pakistan: a modelling study of health impact and cost-effectiveness. PLoS Med. 2021;18(10):e1003815. https://doi.org/10.1371/journal.pmed.1003815.
Pérez Á, Oluyori D. An extended SEIARD model for COVID-19 vaccination in Mexico: analysis and forecast. Math Appl Sci Eng. 2021;2(4):219–309. https://doi.org/10.5206/mase/14233.
Rachaniotis N, Dasaklis T, Fotopoulos F, Tinios P. A two-phase stochastic dynamic model for COVID-19 mid-term policy recommendations in Greece: a pathway towards mass vaccination. Int J Environ Res Public Health. 2021;18(5):2497. https://doi.org/10.3390/ijerph18052497.
Rahmandad H, Lim T, Sterman J. Behavioral dynamics of COVID-19: estimating underreporting, multiple waves, and adherence fatigue across 92 nations. Syst Dyn Rev. 2021;37(1):5–31. https://doi.org/10.1002/sdr.1673.
Raina C, Costantino V, Chanmugam A. The use of face masks during vaccine roll-out in New York City and impact on epidemic control. Vaccine. 2021;39(42):6296–301. https://doi.org/10.1016/j.vaccine.2021.08.102.
Rajapaksha R, Wijesinghe M, Jayasooriya K, Gunawardana B, Weerasinghe W. An extended susceptible-exposed-infected-recovered (SEIR) model with vaccination for forecasting the COVID-19 pandemic in Sri Lanka. medRxiv. 2022. https://doi.org/10.1101/2021.06.17.21258837.
Adiga A, Athreya S, Lewis B, Marathe M, Rathod N, Sundaresan R, et al. Strategies to mitigate COVID-19 resurgence assuming immunity waning: a study for Karnataka, India. medRxiv. 2021. https://doi.org/10.1101/2021.05.26.21257836.
Aruffo E, Yuan P, Tan Y, Gatov E, Gournis E, Collier S, et al. Community structured model for vaccine strategies to control COVID-19 spread: a mathematical study. PLoS ONE. 2022;17(10):e0258648. https://doi.org/10.1371/journal.pone.0258648.
Rajput A, Sajid M, Tanvi, Shekhar C, Aggarwal R. Optimal control strategies on COVID-19 infection to bolster the efficacy of vaccination in India. Sci Rep. 2021;11(1):1–18. https://doi.org/10.1038/s41598-021-99088-0.
Rao I, Brandeau M. Optimal allocation of limited vaccine to control an infectious disease: simple analytical conditions. Math Biosci. 2021;337:108621. https://doi.org/10.1016/j.mbs.2021.108621.
Reddy K, Fitzmaurice K, Scott J, Harling G, Lessells R, Panella C, et al. Clinical outcomes and cost-effectiveness of COVID-19 vaccination in South Africa. Nat Commun. 2021;12(1):1–10. https://doi.org/10.1038/s41467-021-26557-5.
Rocha T, Moret M, Chow C, Phillips J, Cordeiro A, Scorza F, et al. A data-driven model for COVID-19 pandemic: evolution of the attack rate and prognosis for Brazil. Chaos, Solitons & Fractals. 2021;152:111359. https://doi.org/10.1016/j.chaos.2021.111359.
Rodríguez J, Patón M, Acuña J. COVID-19 vaccination rate and protection attitudes can determine the best prioritisation strategy to reduce fatalities. medRxiv. 2021. https://doi.org/10.1101/2020.10.12.20211094.
Romero-Brufau S, Chopra A, Ryu A, Gel E, Raskar R, Kremers W, et al. Public health impact of delaying second dose of BNT162b2 or mRNA-1273 covid-19 vaccine: simulation agent based modeling study. BMJ. 2021;373:n1087. https://doi.org/10.1136/bmj.n1087.
Roy D, Chakravortty D, Basu S. The efficacy of vaccines in the context of COVID-19 and its variants: role of spatio-temporal boundary. medRxiv. 2021. https://doi.org/10.1101/2021.07.19.21260758.
Roy J, Heath S, Ramkrishna D, Wang S. Modeling of COVID-19 transmission dynamics on US population: inter-transfer infection in age groups, mutant variants, and vaccination strategies. medRxiv. 2021. https://doi.org/10.1101/2021.09.25.21264118.
Sadarangani M, Abu B, Conway J, Iyaniwura S, Cardim R, Colijn C, et al. Importance of COVID-19 vaccine efficacy in older age groups. Vaccine. 2021;39(15):2020–3. https://doi.org/10.1016/j.vaccine.2021.03.020.
Sah P, Vilches T, Moghadas S, Fitzpatrick M, Singer B, Hotez P, et al. Accelerated vaccine rollout is imperative to mitigate highly transmissible COVID-19 variants. EClinicalMedicine. 2021;35:100865. https://doi.org/10.1016/j.eclinm.2021.100865.
Aruffo E, Yuan P, Tan Y, Gatov E, Moyles I, Bélair J, et al. Mathematical modeling of vaccination rollout and NPIs lifting on COVID-19 transmission with VOC: a case study in Toronto, Canada. BMC Public Health. 2022;22:1–12. https://doi.org/10.1186/s12889-022-13597-9.
Sandmann F, Davies N, Vassall A, Edmunds W, Jit M, Centre for the matematical modelling of infectious diseases COVID-19 working group. The potential health and economic value of SARS-CoV-2 vaccination alongside physical distancing in the UK: a transmission model-based future scenario analysis and economic evaluation. Lancet Infect Dis. 2021;21(7):962–74. https://doi.org/10.1016/S1473-3099%2821%2900079-7.
Scarabaggio P, Carli R, Cavone G, Epicoco N, Dotoli M. Modeling, estimation, and optimal control of anti-COVID-19 multi-dose vaccine administration. IEEE 17th International Conference on Automation Science and Engineering. 2021;990–5. https://doi.org/10.1109/CASE49439.2021.9551418.
Shen M, Zu J, Fairley C, Pagán J, An L, Du Z, et al. Projected COVID-19 epidemic in the United States in the context of the effectiveness of a potential vaccine and implications for social distancing and face mask use. Vaccine. 2021;39(16):2295–302. https://doi.org/10.1016/j.vaccine.2021.02.056.
Shim E. Optimal allocation of the limited COVID-19 vaccine supply in South Korea. J Clin Med. 2021;10(4):591. https://doi.org/10.3390/jcm10040591.
Shim E. Projecting the impact of SARS-CoV-2 variants and the vaccination program on the fourth wave of the COVID-19 pandemic in South Korea. Int J Environ Res Public Health. 2021;18(14):7578. https://doi.org/10.3390/ijerph18147578.
Silva P, Sagastizábal C, Nonato L, Struchiner C, Pereira T. Optimized delay of the second COVID-19 vaccine dose reduces ICU admissions. Proc Natl Acad Sci. 2021;118(35):e2104640118. https://doi.org/10.1073/pnas.2104640118.
Sivadas N, Panda P, Mahajan A. Control strategies for the COVID-19 infection wave in India: a mathematical model incorporating vaccine effectiveness. medRxiv. 2021. https://doi.org/10.1101/2021.12.27.21268464.
Sonabend R, Whittles L, Imai N, Perez-Guzman P, Knock E, Rawson T, et al. Non-pharmaceutical interventions, vaccination, and the SARS-CoV-2 Delta variant in England: a mathematical modelling study. Lancet. 2021;398(10313):1825–35. https://doi.org/10.1016/S0140-6736%2821%2902276-5.
Song F, Bachmann M. Vaccination against COVID-19 and society’s return to normality in England: a modelling study of impacts of different types of naturally acquired and vaccine-induced immunity. BMJ Open. 2021;11:e053507. https://doi.org/10.1136/bmjopen-2021-053507.
Song H, Fan G, Liu Y, Wang X, He D. The second wave of COVID-19 in South and Southeast Asia and the effects of vaccination. Front Med. 2021;8:1–7. https://doi.org/10.3389/fmed.2021.773110.
Ayoub H, Chemaitelly H, Makhoul M, Al Kanaani Z, Al Kuwari E, Butt A, et al. Epidemiological impact of prioritising SARS-CoV-2 vaccination by antibody status: mathematical modelling analyses. BMJ Innov. 2021;7(2):327–36. https://doi.org/10.1136/bmjinnov-2021-000677.
Stanojevic S, Ponjavic M, Stanojevic S, Stevanovic A, Radojicic S. Simulation and prediction of spread of COVID-19 in The Republic of Serbia by SEAIHRDS model of disease transmission. Microb risk Anal. 2021;18:100161. https://doi.org/10.1016/j.mran.2021.100161.
Stapelberg N, Smoll N, Randall M, Palipana D, Bui B, Macartney K, et al. A discrete-event, simulated social agent- based network transmission (DESSABNeT) model for communicable diseases: method and validation using SARS-CoV-2 data in three large Australian cities. PLoS One. 2021;16(5):e0251737. https://doi.org/10.1371/journal.pone.0251737.
Stevenson M, Metry A, Messenger M. Modelling of hypothetical SARS-CoV-2 point of care tests for routine testing in residential care homes: rapid cost-effectiveness analysis. Health Technol Assess. 2021;25(39):1–74. https://doi.org/10.3310/hta25390.
Stollenwerk N, Mar J, Van-Dierdonck J, Ibarrondo O, Estadilla C, Aguiar M. Modeling COVID-19 vaccine efficacy and coverage towards herd-immunity in the Basque Country, Spain. medRxiv. 2021. https://doi.org/10.1101/2021.07.12.21260390.
Storlie C, Pollock B, Rojas R, Demuth G, Johnson P, Wilson P, et al. Quantifying the importance of COVID-19 vaccination to our future outlook. Mayo Clin Proc. 2021;96(7):1890–5. https://doi.org/10.1016/j.mayocp.2021.04.012.
Sulis E, Terna P. An agent-based decision support for a vaccination campaign. J Med Syst. 2021;45:97. https://doi.org/10.1007/s10916-021-01772-1.
Sun X, Guan T, Xue T, Fan C, Yang M, Meng Y, et al. Analysis on action tracking reports of COVID-19 informs control strategies and vaccine delivery in post-pandemic era. medRxiv. 2021. https://doi.org/10.1101/2021.04.08.21254953.
Sunohara S, Asakura T, Kimura T, Ozawa S, Oshima S, Yamauchi D, et al. Effective vaccine allocation strategies, balancing economy with infection control against COVID-19 in Japan. PLoS One. 2021;16(9):e0257107. https://doi.org/10.1371/journal.pone.0257107.
Suphanchaimat R, Nittayasoot N, Thammawijaya P, Teekasap P, Ungchusak K. Predicted impact of vaccination and active case finding measures to control epidemic of Coronavirus Disease 2019 in a migrant-populated area in Thailand. Risk Manag Healthc Policy. 2021;14:3197–207. https://doi.org/10.2147/RMHP.S318012.
Suphanchaimat R, Tuangratananon T, Rajatanavin N, Phaiyarom M, Jaruwanno W, Uansri S. Prioritization of the target population for Coronavirus disease 2019 (COVID-19) vaccination program in Thailand. Int J Environ Res Public Health. 2021;18(20):10803. https://doi.org/10.3390/ijerph182010803.
Bablani L, Wilson T, Andrabi H, Sundararajan V, Oukarim D, Abraham P, et al. Can a vaccine-led approach end the NSW’s outbreak in 100 days, or at least substantially reduce morbidity and mortality?. medRxiv. 2021. https://doi.org/10.1101/2021.08.18.21262252.
Swan D, Bracis C, Janes H, Moore M, Matrajt L, Reeves D, et al. COVID-19 vaccines that reduce symptoms but do not block infection need higher coverage and faster rollout to achieve population impact. Sci Rep. 2021;11:15531. https://doi.org/10.1038/s41598-021-94719-y.
Swan D, Goyal A, Bracis C, Moore M, Krantz E, Brown E, et al. Mathematical modeling of vaccines that prevent SARS-CoV-2 transmission. Viruses. 2021;13(10):1921. https://doi.org/10.3390/v13101921.
Tang B, Zhang X, Li Q, Bragazzi N, Golemi-Kotra D, Wu J. The minimal COVID-19 vaccination coverage and efficacy to compensate for potential increase of transmission contacts, and increased transmission probability of the emerging strains. BMC Public Health. 2022;22:1258. https://doi.org/10.1186/s12889-022-13429-w.
Tang B, Zhou W, Wang X, Wu H, Xiao Y, Tang S. Controlling multiple COVID-19 epidemic waves: an insight from a multi-scale model linking the behavior change dynamics to the disease transmission dynamics. Bull Math Biol. 2022;84:106. https://doi.org/10.1007/s11538-022-01061-z.
Tang K, Ma Y, Yan H, Rao Y. A new prediction method of COVID-19 epidemic. 2021 4th International conference on pattern recognition and artificial intelligence. 2021;331–5. https://doi.org/10.1109/PRAI53619.2021.9551052.
Tatapudi H, Das R, Das T. Impact of vaccine prioritization strategies on mitigating COVID-19: an agent-based simulation study using an urban region in the United States. BMC Med Res Methodol. 2021;21:272. https://doi.org/10.1186/s12874-021-01458-9.
Teslya A, Rozhnova G, Pham T, van Wees D, Nunner H, Godijk N, et al. The importance of sustained compliance with physical distancing during COVID-19 vaccination rollout. Commun Med. 2022;2:146. https://doi.org/10.1038/s43856-022-00207-3.
Tetteh J, Nguyen VK, Hernández-Vargas E. Network models to evaluate vaccine strategies towards herd immunity in COVID-19. J Theor Biol. 2021;531:110894. https://doi.org/10.1016/j.jtbi.2021.110894.
Thompson J, Wattam S. Estimating the impact of interventions against COVID-19: from lockdown to vaccination. PLoS One. 2021;16(12):e0261330. https://doi.org/10.1371/journal.pone.0261330.
Tokuda Y, Kuniya T, Shibuya K. Potential impact of alternative vaccination strategies on COVID-19 cases, hospitalization, and mortality in Japan during 2021–2022. J Gen Fam Med. 2021;22(6):311–3. https://doi.org/10.1002/jgf2.493.
Badfar E, Zaferani EJ, Nikoofard A. Design a robust sliding mode controller based on the state and parameter estimation for the nonlinear epidemiological model of Covid-19. Nonlinear Dyn. 2022;109:5–18. https://doi.org/10.1007/s11071-021-07036-4.
Topîrceanu A. Immunization using a heterogeneous geo-spatial population model: a qualitative perspective on COVID-19 vaccination strategies. Procedia Comput Sci. 2021;192:2095–104. https://doi.org/10.1016/j.procs.2021.08.217.
Torku T, Khaliq A, Furati K. Deep-data-driven neural networks for COVID-19 vaccine efficacy. Epidemiologia. 2021;2(4):564–86. https://doi.org/10.3390/epidemiologia2040039.
Tran T, Wikle N, Albert E, Inam H, Strong E, Brinda K, et al. Optimal SARS-CoV-2 vaccine allocation using real-time attack-rate estimates in Rhode Island and Massachusetts. BMC Med. 2021;19:162. https://doi.org/10.1186/s12916-021-02038-w.
Truszkowska A, Thakore M, Zino L, Butail S, Caroppo E, Jiang ZP, et al. Designing the safe reopening of US towns through high-resolution agent-based modeling. Adv Theory Simul. 2021;4(9):2100157. https://doi.org/10.1002/adts.202100157.
Usherwood T, LaJoie Z, Srivastava V. A model and predictions for COVID-19 considering population behavior and vaccination. Sci Rep. 2021;11:2051. https://doi.org/10.1038/s41598-021-91514-7.
Utamura M, Koizumi M, Kirikami S. Novel deterministic epidemic model considering mass vaccination and lockdown against coronavirus disease 2019 spread in Israel: a numerical study. Biology Methods and Protocols. 2022;7(1):bpac023. https://doi.org/10.1093/biomethods/bpac023.
Van Gordon M, Mwananyanda L, Gill C, McCarthy K. Regional comparisons of COVID reporting rates, burden, and mortality age-structure using auxiliary data sources. medRxiv. 2021. https://doi.org/10.1101/2021.08.18.21262248.
Van Heusden K, Stewart G, Otto S, Dumont G. Pandemic policy design via feedback: a modelling story. medRxiv. 2021. https://doi.org/10.1101/2021.09.23.21263924.
Van Egeren D, Stoddard M, Novokhodko A, Rogers M, Joseph-McCarthy D, Zetter B, et al. Rapid relaxation of pandemic restrictions after vaccine rollout favors growth of SARS-CoV-2 variants: a model-based analysis. PLoS One. 2021;16(11):e0258997. https://doi.org/10.1371/journal.pone.0258997.
Viana J, van Dorp C, Nunes A, Gomes M, van Boven M, Kretzschmar M, et al. Controlling the pandemic during the SARS-CoV-2 vaccination rollout. Nat Commun. 2021;12:3674. https://doi.org/10.1038/s41467-021-23938-8.
Barlow M, Marshall N, Tyson R. Optimal shutdown strategies for COVID-19 with economic and mortality costs: British Columbia as a case study. R Soc Open Sci. 2021;8(9):202255. https://doi.org/10.1098/rsos.202255.
Vignals C, Dick D, Thiébaut R, Wittkop L, Prague M, Heffernan J. Barrier gesture relaxation during vaccination campaign in France: modelling impact of waning immunity. COVID. 2021;1(2):472–88. https://doi.org/10.3390/covid1020041.
Vilches T, Nourbakhsh S, Zhang K, Juden-Kelly L, Cipriano L, Langley J, et al. Multifaceted strategies for the control of COVID-19 outbreaks in long-term care facilities in Ontario, Canada. Prev Med. 2021;148:106564. https://doi.org/10.1016/j.ypmed.2021.106564.
Vilches T, Alves F, Forti R, Berg G, Castelo C, Pio C. Vaccination efforts in Brazil: scenarios and perspectives under a mathematical modeling approach. medRxiv. 2021. https://doi.org/10.1101/2021.02.22.21252208.
Vilches T, Sah P, Abdollahi E, Moghadas S, Galvani A. Importance of non-pharmaceutical interventions in the COVID-19 vaccination era: a case study of the Seychelles. J Glob Health. 2021;11:03104. https://doi.org/10.7189/jogh.11.03104.
Vilches T, Zhang K, Van Exan R, Langley J, Moghadas S. Projecting the impact of a two-dose COVID-19 vaccination campaign in Ontario Canada. Vaccine. 2021;39(17):2360–5. https://doi.org/10.1016/j.vaccine.2021.03.058.
Volodymyrovych T, Ivanovich S, Tetiana K, Yaroslavovych T. Pharmaco economics analysis of COVID-19 vaccines in Ukraine. J Pharm Res Int. 2021;33(32A):140–7. https://doi.org/10.9734/JPRI/2021/v33i32A31727.
Wang W, Fann J, Chang R-E, Jeng Y, Hsu C-Y, Chen H-H, et al. Economic evaluation for mass vaccination against COVID-19. J Formos Med Assoc. 2021;120:S95-S105. https://doi.org/10.1016/j.jfma.2021.05.020.
Wang Z, Wu P, Wang J, Lourenço J, Li B, Rader B, et al. Asymptomatic SARS-CoV-2 infection and the demography of COVID-19. J R Soc Interface. 2022;19:20220498. https://doi.org/10.1098/rsif.2022.0498.
Webb G. A COVID-19 epidemic model predicting the effectiveness of vaccination in the US. Infect Dis Rep. 2021;13(3):654–67. https://doi.org/10.3390/idr13030062.
Więcek W, Ahuja A, Kremer M, Simoes A, Snyder C, Tabarrok A, et al. Could vaccine dose stretching reduce COVID-19 deaths?. National Bureau of Economic Research. 2021. https://doi.org/10.3386/w29018.
Barnard R, Davies N, Centre for mathematical modelling of infectious disease COVID-19 working group, Mark J, Edmunds J. Modelling the medium-term dynamics of SARS-CoV-2 transmission in England in the Omicron era. Nat Commun. 2022;13:4879. https://doi.org/10.1038/s41467-022-32404-y.
Wieland J, Mercorelli P. Simulation of SARS-CoV-2 pandemic in Germany with ordinary differential equations in MATLAB. 2021 25th International conference on system theory, control and computing. 2021;564–9. https://doi.org/10.1109/ICSTCC52150.2021.9607181.
Wirtz K. Decline in mitigation readiness facilitated second waves of SARS-CoV-2. medRxiv. 2021. https://doi.org/10.1101/2021.02.10.21251523.
Wong W, Juwono F, Chua T. SIR Simulation of COVID-19 pandemic in Malaysia: Will the vaccination program be effective?. arXiv. 2021. https://arxiv.org/pdf/2101.07494.pdf.
Yang C, Yang Y, Li Y. Assessing vaccination priorities for different ages and age-specific vaccination strategies of COVID-19 using an SEIR modelling approach. PLoS One. 2021;16(2):e0261236. https://doi.org/10.1371/journal.pone.0261236.
Yang J, Marziano V, Deng X, Guzzetta G, Zhang J, Trentini F, et al. Despite vaccination, China needs non-pharmaceutical interventions to prevent widespread outbreaks of COVID-19 in 2021. Nat Hum Behav. 2021;5:1009–20. https://doi.org/10.1038/s41562-021-01155-z.
Yang W, Kandula S, Shaman J. Simulating the impact of different vaccination policies on the COVID-19 pandemic in New York City. medRxiv. 2021. https://doi.org/10.1101/2021.01.21.21250228.
Yang W, Shaman J. COVID-19 pandemic dynamics in India, the SARS-CoV-2 Delta variant, and implications for vaccination. J R Soc Interfac. 2022;19(191):20210900. https://doi.org/10.1098/rsif.2021.0900.
Yang W, Shaman J. Development of a model-inference system for estimating epidemiological characteristics of SARS-CoV-2 variants of concern. Nat Commun. 2021;12:5573. https://doi.org/10.1038/s41467-021-25913-9.
Young G, Xiao P, Newcomb K, Michael E. Interplay between COVID-19 vaccines and social measures for ending the SARS-CoV-2 pandemic. arXiv. 2021. https://doi.org/10.48550/arXiv.2103.06120.
Yu H, Han S, Cai J, Yang J, Zhang J, Wu Q, et al. Dynamic optimization of COVID-19 vaccine prioritization in the context of limited supply. Research Square. 2021. https://doi.org/10.21203/rs.3.rs-257573/v1.
Barnard R, Davies N, Pearson C, Jit M, Edmunds W. Projected epidemiological consequences of the Omicron SARS-CoV-2 variant in England, December 2021 to April 2022. medRxiv. 2021. https://doi.org/10.1101/2021.12.15.21267858.
Zhang L, Ullah S, Alwan B, Alshehri A, Sumelka W. Mathematical assessment of constant and time-dependent control measures on the dynamics of the novel coronavirus: an application of optimal control theory. Results Phys. 2021;31:104971. https://doi.org/10.1016/j.rinp.2021.104971.
Zhang S, Bi G, Wang X, Yang Y, Qi J, Li S, et al. An extended COVID-19 epidemiological model with vaccination and multiple interventions for controlling COVID-19 outbreaks in the UK. medRxiv. 2021. https://doi.org/10.1101/2021.03.10.21252748.
Zhao C, Liang X, Zhao H. Analysis of the vaccine effect on infectious diseases by system dynamics model. In The Fifth International Conference on Biological Information and Biomedical Engineering. 2021;18:1–5. https://doi.org/10.1145/3469678.3469696.
Zhao S, Sha T, Wu CI, Xue Y, Chen H. Will the large-scale vaccination succeed in containing the COVID-19 pandemic and how soon?. Quant Biol. 2021;9(3):304–16. https://doi.org/10.15302/j-qb-021-0256.
Zhao X, Tatapudi H, Corey G, Gopalappa C. Threshold analyses on combinations of testing, population size, and vaccine coverage for COVID-19 control in a university setting. PLoS One. 2021;16(8):e0255864. https://doi.org/10.1371/journal.pone.0255864.
Zhao Z, Li X, Liu F, Jin R, Ma C, Huang B, et al. Stringent nonpharmaceutical interventions are crucial for curbing COVID-19 transmission in the course of vaccination: a case study of South and Southeast Asian countries. Healthcare. 2021;9(10):1292. https://doi.org/10.3390/healthcare9101292.
Zhao Z, Niu Y, Luo L, Hu Q, Yang T, Chu M, et al. The optimal vaccination strategy to control COVID-19: a modeling study based on the transmission scenario in Wuhan city, China. Infect Dis Poverty. 2021;10:140. https://doi.org/10.1186/s40249-021-00922-4.
Zhou W, Tang B, Bai Y, Shao Y, Xiao Y, Tang S. The resurgence risk of COVID-19 in the presence of immunity waning and ADE effect: a mathematical modelling study. medRxiv. 2021. https://doi.org/10.1101/2021.08.25.21262601.
Zia K. Why a globally fair COVID-19 vaccination? An analysis based on agent-based simulation. medRxiv. 2021. https://doi.org/10.1101/2021.10.03.21264494.
Zou Z, Fairley C, Shen M, Scott N, Xu X, Li Z, et al. Critical timing and extent of public health interventions to control outbreaks dominated by SARS-CoV-2 variants in Australia: a mathematical modelling study. Int J Infect Dis. 2022;115:154–65. https://doi.org/10.1016/j.ijid.2021.11.024.
Barreiro N, Govezensky T, Ventura C, Núñez M, Bolcatto P, Barrio R. Modelling the interplay of SARS-CoV-2 variants in the United Kingdom. Sci Rep. 2021;12:12372. https://doi.org/10.1038/s41598-022-16147-w.
Bartsch S, O’Shea K, Wedlock P, Strych U, Ferguson M, Bottazzi M, et al. The benefits of vaccinating with the first available COVID-19 Coronavirus vaccine. Am J Prev Med. 2021;60(5):605–13. https://doi.org/10.1016/j.amepre.2021.01.001.
Agarwal N, Komo A, Patel C, Pathak P, Unver U. The trade-off between prioritization and vaccination speed depends on mitigation measures. medRxiv. 2021. https://doi.org/10.1101/2021.02.24.21252352.
Bartsch S, Wedlock P, O’Shea K, Cox S, Strych U, Nuzzo J, et al. Lives and costs saved by expanding and expediting Coronavirus Disease 2019 vaccination. J Infect Dis. 2021;224(6):938–48. https://doi.org/10.1093/infdis/jiab233.
Bauer S, Contreras S, Dehning J, Linden M, Iftekhar E, Mohr S, et al. Relaxing restrictions at the pace of vaccination increases freedom and guards against further COVID-19 waves in Europe. PLoS Comput Biol. 2021;17(9):e1009288. https://doi.org/10.1371/journal.pcbi.1009288.
Bautista L, Gil M, Bautista B, Alcaide A, Rodríguez G. COVID-19 immunization threshold(s): an analysis. medRxiv. 2021. https://doi.org/10.1101/2021.01.02.20248596.
Below D, Mairanowski F. The impact of vaccination on the spread patterns of the COVID epidemic. medRxiv. 2021. https://doi.org/10.1101/2021.04.29.21256322.
Berkane S, Harizi I, Tayebi A. Modeling the effect of population-wide vaccination on the evolution of COVID-19 epidemic in Canada. medRxiv. 2021. https://doi.org/10.1101/2021.02.05.21250572.
Bertsimas D, Digalakis V, Jacquillat A, Li ML, Previero A. Where to locate COVID-19 mass vaccination facilities?. Nav Res Logist. 2021;69(2):179–200. https://doi.org/10.1002/nav.22007.
Bhattacharya P, Machi D, Chen J, Hoops S, Lewis B, Mortveit H, et al. AI-driven agent-based models to study the role of vaccine acceptance in controlling COVID-9 spread in the US. 2021 IEEE International Conference on Big Data (Big Data), Orlando, FL, USA. 2021;1566–74. https://doi.org/10.1109/BigData52589.2021.9671811.
Bianchin G, Dall’Anese E, Poveda J, Buchwald A. When can we safely return to normal? A novel method for identifying safe levels of NPIs in the context of COVID-19 vaccinations. medRxiv. 2021. https://doi.org/10.1101/2021.04.20.21255350.
Bilinski A, Ciaranello A, Fitzpatrick M, Giardina J, Shah M, Salomon J, et al. Estimated transmission outcomes and costs of SARS-CoV-2 diagnostic testing, screening, and surveillance strategies among a simulated population of primary school students. JAMA Pediatr. 2022;176(7):679–89. https://doi.org/10.1001/jamapediatrics.2022.1326.
Bilinski A, Salomon J, Giardina J, Ciaranello A, Fitzpatrick M. Passing the test: a model-based analysis of safe school-reopening strategies. Ann Intern Med. 2021;174(8):1090–100. https://doi.org/10.7326/M21-0600.
Aguas R, Bharath A, White L, Gao B, Pollard A, Voysey M, et al. Potential global impacts of alternative dosing regimen and rollout options for the ChAdOx1 nCoV-19 vaccine. Nat Commun. 2021;12:6370. https://doi.org/10.1038/s41467-021-26449-8.
Booton R, Powell A, Turner K, Wood R. Modelling the effect of COVID-19 mass vaccination on acute admissions in a major English healthcare system. International Journal for Quality in Health Care. 2021;34(2):mzac031. https://doi.org/10.1093/intqhc/mzac031.
Borchering R, Viboud C, Howerton E, Smith C, Truelove S, Runge M, et al. Modeling of future COVID-19 cases, hospitalizations, and deaths, by vaccination rates and nonpharmaceutical intervention scenarios: United States, April-September 2021. Morb Mortal Wkly Rep. 2021;70(19):719–24. https://www.cdc.gov/mmwr/volumes/70/wr/mm7019e3.htm?s_cid=mm7019e3_w#suggestedcitation.
Bosetti P, Kiem CT, Andronico A, Paireau J, Bruhl L, Lina B, et al. A race between SARS-CoV-2 variants and vaccination: the case of the B.1.1.7 variant in France. 2021. https://pasteur.hal.science/pasteur-03149525.
Bowie C, Friston K. A twelve-month projection to September 2022 of the Covid-19 epidemic in the UK using a dynamic causal model. medRxiv. 2021. https://doi.org/10.1101/2021.10.04.21262827.
Brown R. A simple model for control of COVID-19 infections on an urban campus. 2021;118(36):e2105292118. https://doi.org/10.1073/pnas.2105292118.
Bu X, Gu N. Forecast of the development of COVID-19 based on the small-world network. In Proceedings of the 2021 5th International Conference on Computer Science and Artificial Intelligence (CSAI 21). Association for Computing Machinery, New York, NY, USA. 2021;175–81. https://doi.org/10.1145/3507548.3507575.
Bubar K, Reinholt K, Kissler S, Lipsitch M, Cobey S, Grad Y, et al. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science. 2021;371(6532):916–21. https://doi.org/10.1126/science.abe6959.
Buchwald A, Carlton E, Ghosh D, Samet J, Timm L, Wu E, et al. Colorado COVID-19 mathematical model documentation prepared by the colorado COVID-19 modeling group. 2021. Available from: https://agb85.github.io/covid-19/SEIR%20Documentation.pdf.
Buckner J, Chowell G, Springborn M. Dynamic prioritization of COVID-19 vaccines when social distancing is limited for essential workers. Proc Natl Acad Sci. 2021;118(16):e2025786118. https://doi.org/10.1073/pnas.2025786118.
Buhat C, Lutero D, Olave Y, Quindala K, Recreo M, Talabis D, et al. Using constrained optimization for the allocation of COVID-19 vaccines in the Philippines. Appl Health Econ Health Policy. 2021;19:699–708. https://doi.org/10.1007/s40258-021-00667-z.
Aguiar M, Van-Dierdonck J, Mar J, Stollenwerk N. The role of mild and asymptomatic infections on COVID-19 vaccines performance: a modeling study. J Adv Res. 2021;39:157-66. https://doi.org/10.1016/j.jare.2021.10.012.
Caetano C, Morgado M, Patrício P, Leite A, Machado A, Torres A, et al. Measuring the impact of COVID-19 vaccination and immunity waning: a modelling study for Portugal. Vaccine. 2022;40(49):7115–21. https://doi.org/10.1016/j.vaccine.2022.10.007.
Campos E, Cysne R, Madureira A, Mendes G. Multi-generational SIR modeling: determination of parameters, epidemiological forecasting and age-dependent vaccination policies. Infect Dis Model. 2021;6:751–65. https://doi.org/10.1016/j.idm.2021.05.003.
Català M, Li X, Prats C, Prieto-Alhambra D. The impact of prioritisation and dosing intervals on the effects of COVID-19 vaccination in Europe: an agent-based cohort model. Sci Rep. 2021;11:18812. https://doi.org/10.1038/s41598-021-98216-0.
Cazelles B, Nguyen-Van-Yen B, Champagne C, Comiskey C. Dynamics of the COVID-19 epidemic in Ireland under mitigation. BMC Infect Dis. 2021;21:735. https://doi.org/10.1186/s12879-021-06433-9.
Chang S, Cliff O, Zachreson C, Prokopenko M. Nowcasting transmission and suppression of the Delta variant of SARS-CoV-2 in Australia. Research Square. 2021. https://doi.org/10.21203/rs.3.rs-757351%2Fv1.
Chen J, Hoops S, Marathe A, Mortveit H, Lewis B, Venkatramanan S, et al. Prioritizing allocation of COVID-19 vaccines based on social contacts increases vaccination effectiveness. medRxiv. 2021. https://doi.org/10.1101/2021.02.04.21251012.
Chen J, Jin M, Wang X, Yang X, Zhang N, Liu F, et al. Fitting and predicting trend of COVID-19 by SVEPIUHDR dynamic model. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42(8):1341–6. https://doi.org/10.3760/cma.j.cn112338-20210225-00147.
Chen V, Zhou Y, Fallahi A, Viswanatha A, Yang J, Liu F, et al. An optimization framework to study the balance between expected fatalities due to COVID-19 and the reopening of U.S. communities. IEEE Trans Autom Sci Eng. 2022;19(2):586–602. https://doi.org/10.1109/TASE.2021.3119930.
Chen X, Zhu G, Zhang L, Fang Y, Guo L, Chen X. Age-stratified COVID-19 spread analysis and vaccination: a multitype random network approach. IEEE Trans Netw Sci Eng. 2021;8(2):1862–72. https://doi.org/10.1109/TNSE.2021.3075222.
Chen Y, Lin Y, Miller E, Neumann J, Mallela A, Posner R, et al. Impacts of vaccination and severe acute respiratory syndrome Coronavirus 2 variants Alpha and Delta on Coronavirus Disease 2019 transmission dynamics in the 15 most populous metropolitan statistical areas in the United States. medRxiv. 2021. https://doi.org/10.1101/2021.10.19.21265223.
Aguilar-Canto F, Ponce de León U, Avila-Vales E. SIR-based model with multiple imperfect vaccines. medRxiv. 2021. https://doi.org/10.1101/2021.05.07.21256860.
Childs L, Dick D, Feng Z, Heffernan J, Li J, Röst G. Modeling waning and boosting of COVID-19 in Canada with vaccination. Epidemics. 2021;39:100583. https://doi.org/10.1016/j.epidem.2022.100583.
Chinchilla R, Yang G, Erdal M, Costa R, Hespanha J. A tale of two doses: model identification and optimal vaccination for COVID-19. 2021 60th IEEE Conference on Decision and Control (CDC), Austin, TX, USA. 2021;3544–50. https://doi.org/10.1109/CDC45484.2021.9683311.
Choi W, Shim E. Vaccine effects on susceptibility and symptomatology can change the optimal allocation of COVID-19 vaccines: South Korea as an example. J Clin Med. 2021;10(13):2813. https://doi.org/10.3390/jcm10132813.
Choi Y, Kim J, Kim J, Choi H, Lee C. Vaccination prioritization strategies for COVID-19 in Korea: a mathematical modeling approach. Int J Environ Res Public Health. 2021;18:4240. https://doi.org/10.3390/ijerph18084240.
Chopra A, Raskar R, Subramanian J, Krishnamurthy B, Gel E, Romero-Brufau S, et al. DeepABM: scalable and efficient agent-based simulations via geometric learning frameworks: a case study for COVID-19 spread and interventions. In: 2021 Winter Simulation Conference. IEEE Press; 2021. p. 1–12. https://doi.org/10.1109/WSC52266.2021.9715507.
Chu L, Grafton Q, Kompas T. What vaccination rate(s) minimise total societal costs after “opening Up” to COVID-19? Age-structured SIRM results for the Delta variant in Australia (New South Wales, Victoria and Western Australia). PLoS Glob public Heal. 2022;2(6):e0000499. https://doi.org/10.1371/journal.pgph.0000499.
Chun J, Jeong H, Beutels P, Ohmagari N, Kim Y, Tsuzuki S. COVID-19 vaccine prioritisation in Japan and South Korea. medRxiv. 2021. https://doi.org/10.1101/2021.04.16.21255649.
Cipriano L, Haddara W, Sander B. Mitigating the 4th wave of the COVID-19 pandemic in Ontario. medRxiv. 2021. https://doi.org/10.1101/2021.09.02.21263000.
Colomer M, Margalida A, Alòs F, Oliva-Vidal P, Vilella A, Fraile L. Modelling the SARS-CoV-2 outbreak: assessing the usefulness of protective measures to reduce the pandemic at population level. Sci Total Environ. 2021;789:147816. https://doi.org/10.1016/j.scitotenv.2021.147816.
Conn H, Taylor R, Willis M, Wright A, Bramfitt V. Mechanistic model calibration and the dynamics of the COVID-19 epidemic in the UK (the past, the present and the future). medRxiv. 2021. https://doi.org/10.1101/2021.05.18.21257384.
Ainslie K, Backer J, de Boer P, van Hoek A, Klinkenberg D, Korthals H, et al. The impact of vaccinating adolescents and children on COVID-19 disease outcomes. medRxiv. 2021. https://doi.org/10.1101/2021.10.21.21265318.
Contreras S, Dehning J, Mohr S, Bauer S, Spitzner F, Priesemann V. Low case numbers enable long-term stable pandemic control without lockdowns. Sci Adv. 2021;7(41):eabg2243. https://doi.org/10.1126/sciadv.abg2243.
Contreras S, Dönges P, Wagner J, Bauer S, Mohr S, Iftekhar E, et al. The winter dilemma. ArvXiv. 2021. https://doi.org/10.48550/arXiv.2110.01554.
Cook T, Roberts. Impact of vaccination by priority group on UK deaths, hospital admissions and intensive care admissions from COVID-19. Anaesthesia. 2021;76(5):608–16. https://doi.org/10.1111/anae.15442.
Coudeville L, Jollivet O, Mahé C, Chaves S, Gomez G. Potential impact of introducing vaccines against COVID-19 under supply and uptake constraints in France: a modelling study. PLoS One. 2021;16(4):e0250797. https://doi.org/10.1371/journal.pone.0250797.
Cruz E, Maciel J, Clozato C, Serpa M, Navaux P, Meneses E, et al. Simulation-based evaluation of school reopening strategies during COVID-19: a case study of Sao Paulo Brazil. Epidemiol Infect. 2021;149(e118):1–9. https://doi.org/10.1017/S0950268821001059.
Cuesta-Lazaro C, Quera-Bofarull A, Aylett-Bullock J, Lawrence B, Fong K, Icaza-Lizaola M, et al. Vaccinations or non-pharmaceutical interventions: safe reopening of schools in England. medRxiv. 2021. https://doi.org/10.1101/2021.09.07.21263223.
Dagpunar J, Wu C. A prototype vaccination model for endemic COVID-19 under waning immunity and imperfect vaccine take-up. medRxiv. 2021. https://doi.org/10.1101/2021.11.06.21266002.
Darapaneni N, Dhua S, Khare N, Ayush K, Karthikeyan N, Ghodke S, et al. Forecasting vaccination drive in India for Herd immunity using SIR and prophet model. 2021 IEEE World AI IoT Congress, Seattle, WA, USA, 2021; p. 21–7. https://doi.org/10.1109/AIIoT52608.2021.9454186.
Davies N, Abbott S, Barnard R, Jarvis C, Kucharski A, Munday J, et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science. 2021;372(6538):eabg3055. https://doi.org/10.1126/science.abg3055.
De la Sen M, Alonso-Quesada S, Ibeas A, Nistal R. On a discrete SEIR epidemic model with two-doses delayed feedback vaccination control on the susceptible. Vaccines. 2021;9(4):398. https://doi.org/10.3390/vaccines9040398.
Alagoz O, Sethi A, Patterson B, Churpek M, Alhanaee G, Scaria E, et al. The impact of vaccination to control COVID-19 burden in the United States: a simulation modeling approach. PLoS One. 2021;16(7):e0254456. https://doi.org/10.1371/journal.pone.0254456.
De la Sen M, Ibeas A, Garrido A. On a new SEIRDE o I o epidemic model eventually initiated from outside with delayed re-susceptibility and vaccination and treatment feedback controls. Phys Scr. 2021;96(9):095002. https://doi.org/10.1088/1402-4896/ac018c.
de Lima P, Lempert R, Vardavas R, Baker L, Ringel J, Rutter C, et al. Reopening California: seeking robust, non-dominated COVID-19 exit strategies. PLoS One. 2021;16(10):1–18. https://doi.org/10.1371/journal.pone.0259166.
De Visscher A, Sutton B, Sutton T. Second-wave dynamics of COVID-19: impact of behavioral changes, immunity loss, new strains, and vaccination. 2021. https://doi.org/10.21203/rs.3.rs-195879/v1.
Debrabant K, Grønbæk L, Kronborg C. The cost-effectiveness of a COVID-19 vaccine in a Danish context. Clin Drug Investig. 2021;41(11):975–88. http://dx.doi.org/10.2139/ssrn.3773381.
De-Leon H, Aran D. What pushed Israel out of herd immunity? Modeling COVID-19 spread of Delta and waning immunity. medRxiv. 2021;1–11. https://doi.org/10.1101/2021.09.12.21263451.
DeWitt M. Rapid impact analysis of B 1.1.7 variant on the spread of SARS-CoV-2 in North Carolina. medRxiv. 2021. https://doi.org/10.1101/2021.02.07.21251291.
Di Domenico L, Sabbatini C, Pullano G, Lévy-Bruhl D, Colizza V. Impact of January 2021 curfew measures on SARS-CoV-2 B.1.1.7 circulation in France. Eurosurveillance. 2021;26:6. https://doi.org/10.2807/1560-7917.ES.2021.26.15.2100272.
Di Domenico L, Sabbatini C, Boëlle P-Y, Poletto C, Crépey P, Paireau J, et al. Adherence and sustainability of interventions informing optimal control against the COVID-19 pandemic. Commun Med. 2021;1(1):1–13. https://doi.org/10.1038/s43856-021-00057-5.
Diagne M, Rwezaura H, Tchoumi S, Tchuenche J. A mathematical model of COVID-19 with vaccination and treatment. Comput Math Methods Med. 2021;2021:1–16. https://doi.org/10.1155/2021/1250129.
Dick D, Childs L, Feng Z, Li J, Röst G, Buckeridge D, et al. Fall 2021 resurgence and COVID-19 seroprevalence in Canada: modelling waning and boosting COVID-19 immunity in Canada, a Canadian immunization research network study. medRxiv. 2021. https://doi.org/10.1101/2021.08.17.21262188.
Albani V, Loria J, Massad E, Zubelli J. COVID-19 underreporting and its impact on vaccination strategies. BMC Infect Dis. 2021;21(1):1–13. https://doi.org/10.1186/s12879-021-06780-7.
Dimeglio C, Miedougé M, Loubes J, Mansuy J, Izopet J. Estimating the impact of public health strategies on the spread of SARS-CoV-2: epidemiological modelling for Toulouse. France Rev Med Virol. 2021;31(5):1–8. https://doi.org/10.1002/rmv.2224.
Dimeglio C, Milhes M, Loubes J-M, Ranger N, Mansuy J-M, Trémeaux P, et al. Influence of SARS-CoV-2 variant B.1.1.7, vaccination, and public health measures on the spread of SARS-CoV-2. Viruses. 2021;13(5):1–10. https://doi.org/10.3390/v13050898.
Dyson L, Hill E, Moore S, Curran-Sebastian J, Tildesley M, Lythgoe K, et al. Possible future waves of SARS-CoV-2 infection generated by variants of concern with a range of characteristics. Nat Commun. 2021;12(1):1–13. https://doi.org/10.1038/s41467-021-25915-7.
España G, Cucunubá Z, Cuervo-Rojas J, Díaz H, González-Mayorga M, Ramírez J. The potential impact of Delta variant of SARS-CoV-2 in the context of limited vaccination coverage and increasing social mixing in Bogota, Colombia. medRxiv. 2021. https://doi.org/10.1101/2021.08.06.21261734.
Estadilla C, Uyheng J, de Lara-Tuprio E, Teng T, Macalalag J, Estuar M. Impact of vaccine supplies and delays on optimal control of the COVID-19 pandemic: mapping interventions for the Philippines. Infect Dis Poverty. 2021;10(4):46–59. https://doi.org/10.1186/s40249-021-00886-5.
Faranda D, Alberti T, Arutkin M, Lembo V, Lucarini V. Interrupting vaccination policies can greatly spread SARS-CoV-2 and enhance mortality from COVID-19 disease: the AstraZeneca case for France and Italy. Chaos an Interdiscip J nonlinear Sci. 2021;31(4):041105. https://doi.org/10.1063/5.0050887.
Fawaz A, Owayjan M, Achkar R. Development of a robust mathematical model to estimate COVID-19 cases in Lebanon based on SEIRDV modified model. In: International conference on advances in biomedical engineering. IEEE; 2021. p. 141–6. https://doi.org/10.1109/ICABME53305.2021.9604824.
Feng M, Tian L, Zhou C. Mechanism of optimal time-course COVID-19 vaccine prioritization based on non-Markovian steady-state prediction. medRxiv. 2021. https://doi.org/10.1101/2021.10.11.21264836.
Ferranna M, Cadarette D, Bloom D. COVID-19 vaccine allocation: modeling health outcomes and equity implications of alternative strategies. Engineering. 2021;7(7):924–35. https://doi.org/10.1016/j.eng.2021.03.014.
Ferreira L, Berga G, Borges M, Mendes L, Poloni S, Bagattini Â, et al. Modelling optimal vaccination strategies against COVID-19 in a context of Gamma variant predominance in Brazil. medRxiv. 2021. https://doi.org/10.1016/j.vaccine.2022.09.082.
Omar O, Elbarkouky R, Ahmed H. Fractional stochastic modelling of COVID-19 under wide spread of vaccinations: Egyptian case study. Alexandria Eng J. 2022;61(11):8595–609. https://doi.org/10.1016/j.aej.2022.02.002.
Chapman L, Barnard R, Russell T, Abbott S, van Zandvoort K, Davies N, et al. Unexposed populations and potential COVID-19 hospitalisations and deaths in European countries as per data up to 21 November 2021. EuroSurveillance. 2022;27(1):2101038. https://doi.org/10.2807/1560-7917.ES.2022.27.1.2101038.
Bosetti P, Kiem C, Andronico A, Paireau J, Levy-Bruhl D, Alter L, et al. Impact of booster vaccination on the control of COVID-19 Delta wave in the context of waning immunity: application to France in the winter 2021/22. Eurosurveillance. 2022;27:2101125. https://doi.org/10.2807/1560-7917.ES.2022.27.1.2101125.
Gutiérrez-Jara J, Saracini C. Risk perception influence on vaccination program on COVID-19 in Chile: a mathematical model. Int J Environ Res Public Health. 2022;19(4):1–12. https://doi.org/10.3390/ijerph19042022.
Contreras D, Colosi E, Bassignana G, Colizza V, Barrat A. Impact of the representation of contact data on the evaluation of interventions in infectious diseases simulations. medRxiv. 2022. https://doi.org/10.1101/2022.02.28.22271600.
Yuan P, Aruffo E, Tan Y, Yang L, Ogden N, Fazil A, et al. Projections of the transmission of the Omicron variant for Toronto, Ontario, and Canada using surveillance data following recent changes in testing policies. Infect Dis Model. 2022;7(2):83–93. https://doi.org/10.1016/j.idm.2022.03.004.
Nakhaeizadeh M, Chegeni M, Adhami M, Sharifi H, Gohari M, Iranpour A, et al. Estimating the number of COVID-19 cases and impact of new COVID-19 variants and vaccination on the population in Kerman, Iran: a mathematical modeling study. Comput Math Methods Med. 2022;2022:1–11. https://doi.org/10.1155/2022/6624471.
Ghafari M, Watson O, Karlinsky A, Ferretti L, Katzourakis A. A framework for reconstructing SARS-CoV-2 transmission dynamics using excess mortality data. medRxiv. 2022. https://doi.org/10.1038/s41467-022-30711-y.
Xiong X, Li J, Huang B, Tam T, Hong Y, Chong K-C, et al. Economic value of vaccines to address the COVID-19 pandemic in Hong Kong: a cost-effectiveness analysis. Vaccines. 2022;10(4):495. https://doi.org/10.3390/vaccines10040495.
Xavier C, Oliveira R, Vieira V, Rocha B, Reis R, Quintela B, et al. Timing the race of vaccination, new variants, and relaxing restrictions during COVID-19 pandemic. J Comput Sci. 2022;61:1–15. https://doi.org/10.1016/j.jocs.2022.101660.
Savinkina A, Bilinski A, Fitzpatrick M, Paltiel A, Rizvi Z, Salomon J, et al. Model-based estimates of deaths averted and cost per life saved by scaling-up mRNA COVID-19 vaccination in low and lower-middle income countries in the COVID-19 Omicron variant era. medRxiv. 2022. https://doi.org/10.1101/2022.02.08.22270465.
Hjorleifsson K, Rognvaldsson S, Jónsson H, Agustsdottir A, Andrésdóttir M, Birgisdottir K, et al. Reconstruction of a large-scale outbreak of SARS-CoV-2 infection in Iceland informs vaccination strategies. Clin Microbiol Infect. 2022;28(6):852–85. https://doi.org/10.1016/j.cmi.2022.02.012.
Olmedo C, Díez J, Expósito D, Moriña D, Aznarte J, Almagro J, et al. Predicciones de tres modelos matemáticos en relación a la estrategia de vacunación frente a la COVID-19 en España. Junio de 2021. Rev Esp Salud Publica. 2022;96(7):1–10. Available from: https://dialnet.unirioja.es/servlet/articulo?codigo=8620587.
Souto L, Canton O, da Silva R, Poloni S, Sudbrack V, Borges M, et al. Assessing the best time interval between doses in a two-dose vaccination regimen to reduce the number of deaths in an ongoing epidemic of SARS-CoV-2. PLoS Comput Biol. 2022;18(3):1–15. https://doi.org/10.1371/journal.pcbi.1009978.
Wiȩcek W, Ahuja A, Chaudhuri E, Kremer M, Gomes A, Snyder C, et al. Testing fractional doses of COVID-19 vaccines. Proc Natl Acad Sci. 2022;119(8):e2116932119. https://doi.org/10.1073/pnas.2116932119.
Brüningk S, Klatt J, Stange M, Mari A, Brunner M, Roloff T-C, et al. Determinants of SARS-CoV-2 transmission to guide vaccination strategy in an urban area. Virus Evol. 2022;8(1):veac002. https://doi.org/10.1093/ve/veac002.
Tan S, Park H, Rodríguez-Barraquer I, Rutherford G, Bibbins-Domingo K, Schechter R, et al. COVID-19 vaccination and estimated public health impact in California. JAMA Netw Open. 2022;5(4):1–14. https://doi.org/10.1001/jamanetworkopen.2022.8526.
Liu H, Zhang J, Cai J, Deng X, Peng C, Chen X, et al. Investigating vaccine-induced immunity and its effect in mitigating SARS-CoV-2 epidemics in China. BMC Med. 2022;20(1):1–12. https://doi.org/10.1186/s12916-022-02243-1.
Cai J, Yang J, Deng X, Peng C, Chen X, Wu Q, et al. Assessing the transition of COVID-19 burden towards the young population while vaccines are rolled out in China. Emerg Microbes Infect. 2022;11(1):1205–14. https://doi.org/10.1080/22221751.2022.2063073.
Moldokmatova A, Dooronbekova A, Zhumalieva C, Mukambetov A, Kubatova A, Usenbaev N, et al. Mathematical modelling of COVID-19 vaccination strategies in Kyrgyzstan. medRxiv. 2022. https://doi.org/10.1101/2021.12.21.21268200.
Borchering R, Mullany L, Howerton E, Chinazzi M, Smith C, Qin M, et al. Impact of SARS-CoV-2 vaccination of children ages 5–11 years on COVID-19 disease burden and resilience to new variants in the United States, November 2021-March 2022: a multi-model study. medRxiv. 2022. https://doi.org/10.1101/2022.03.08.22271905.
Truszkowska A, Zino L, Butail S, Caroppo E, Jiang Z, Rizzo A, et al. Predicting the effects of waning vaccine immunity against COVID-19 through high-resolution agent-based modeling. Adv Theory Simul. 2022;2100521:1–13. https://doi.org/10.1002/adts.202100521.
Cohen J, Stuart R, Panovska-Griffiths J, Mudimu E, Abeysuriya R, Kerr C, et al. The changing impact of vaccines in the COVID-19 pandemic. medRxiv. 2022. https://doi.org/10.1101/2022.03.10.22272222.
Gómez J, García Y, Schmidt A, Martínez-López B, Nuño M. Testing and vaccination to reduce the impact of COVID-19 in nursing homes: an agent-based approach. BMC Infect Dis. 2022;22(1):1–14. https://doi.org/10.1186/s12879-022-07385-4.
Robles-Fontán M, Nieves E, Cardona-Gerena I, Irizarry R. Effectiveness estimates of three COVID-19 vaccines based on observational data from Puerto Rico. Lancet Reg Heal Am. 2022;9:100212. https://doi.org/10.1016/j.lana.2022.100212.
Yang Q, Gruenbacher D, Scoglio C. Estimating data-driven Coronavirus Disease 2019 mitigation strategies for safe university reopening. J R Soc Interface. 2022;19(188):20210920. https://doi.org/10.1098/rsif.2021.0920.
Lasser J, Sorger J, Richter L, Thurner S, Schmid D, Klimek P. Assessing the impact of SARS-CoV-2 prevention measures in Austrian schools using agent-based simulations and cluster tracing data. Nat Commun. 2021;13(1):1–17. https://doi.org/10.1038/s41467-022-28170-6.
Du Z, Wang L, Pandey A, Lim W, Chinazzi M, Piontti A, et al. Modeling comparative cost-effectiveness of SARS-CoV-2 vaccine dose fractionation in India. Nat Med. 2022;28(5):934–8. https://doi.org/10.1038/s41591-022-01736-z.
Milne G, Carrivick J, Whyatt D. Mitigating the SARS-CoV-2 Delta disease burden in Australia by non-pharmaceutical interventions and vaccinating children: a modelling analysis. BMC Med. 2022;20(1):1–13. https://doi.org/10.1186/s12916-022-02241-3.
Dönges P, Wagner J, Contreras S, Iftekhar E, Bauer S, Mohr S, et al. Interplay between risk perception, behaviour, and COVID-19 spread. arXiv. 2022. https://doi.org/10.48550/arXiv.2112.12062.
Somekh I, KhudaBukhsh W, Dowling E, Keinan L, Rempala G, Simões E, et al. Quantifying the population-level effect of the COVID-19 mass vaccination campaign in Israel: a modeling study. Open Forum Infect Dis. 2022;9(5):1–8. https://doi.org/10.1093/ofid/ofac087.
Feng A, Obolski U, Stone L, He D. Modelling COVID-19 vaccine breakthrough infections in highly vaccinated Israel - the effects of waning immunity and third vaccination dose. medRxiv. 2022. https://doi.org/10.1371/journal.pgph.0001211.
Canga A, Bidegain G. Modelling the effect of the interaction between vaccination and non-pharmaceutical measures on COVID-19 incidence. Glob Heal Epidemiol Genomics. 2022:9244953. https://doi.org/10.1101/2021.11.29.21266986.
Li M, Zu J, Zhang Y, Ma L, Shen M, Li Z, et al. COVID-19 epidemic in New York City: development of an age group-specific mathematical model to predict the outcome of various vaccination strategies. Virol J. 2022;19(1):1–13. https://doi.org/10.1186/s12985-022-01771-9.
Yang W, Shaman J. COVID-19 pandemic dynamics in South Africa and epidemiological characteristics of three variants of concern (Beta, Delta, and Omicron). medRxiv. 2022. https://doi.org/10.1101/2021.12.19.21268073.
De Cellès M, Wong A, Andrea Barrero Guevara L, Rohani P. Immunological heterogeneity informs estimation of the durability of COVID-19 vaccine protection. J R Soc Interface. 2022;19(190):20220070. https://doi.org/10.1098/rsif.2022.0070.
González-Parra G, Cogollo M, Arenas A. Mathematical modeling to study optimal allocation of vaccines against COVID-19 using an age-structured population. Axioms. 2022;11(3):109. https://doi.org/10.3390/axioms11030109.
Walker J, Paul P, Dooling K, Oliver S, Prasad P, Steele M, et al. Modeling strategies for the allocation of SARS-CoV-2 vaccines in the United States. Vaccine. 2022;40(14):2134–9. https://doi.org/10.1016/j.vaccine.2022.02.015.
Liu Y, Pearson C, Sandmann F, Barnard R, Kim J, Flasche S, et al. Dosing interval strategies for two-dose COVID-19 vaccination in 13 middle-income countries of Europe: health impact modelling and benefit-risk analysis. Lancet Reg Heal Eur. 2020;17:100381. https://doi.org/10.1016/j.lanepe.2022.100381.
Vilches T, Moghadas S, Sah P, Fitzpatrick M, Shoukat A, Pandey A, et al. Estimating COVID-19 infections, hospitalizations, and deaths following the US vaccination campaigns during the pandemic. JAMA Netw Open. 2022;5(1):e2142725. https://doi.org/10.1001/jamanetworkopen.2021.42725.
Machado B, Antunes L, Caetano C, Pereira J, Nunes B, Patrício P, et al. The impact of vaccination on the evolution of COVID-19 in Portugal. Math Biosci Eng. 2022;19(1):936–52. https://doi.org/10.3934/mbe.2022043.
Avila-Ponce de León U, Avila-Vales E, Huang K. Modeling COVID-19 dynamic using a two-strain model with vaccination. Chaos Solitons Fractals. 2022;157:111927. https://doi.org/10.1016/j.chaos.2022.111927.
Morales-Zamora G, Espinosa O, Puertas E, Fernández J, Hernández J, Zakzuk V, et al. Cost-effectiveness analysis of strategies of COVID-19 vaccination in Colombia: comparison of high-risk prioritization and no prioritization strategies with the absence of a vaccination plan. Value Heal Reg Issues. 2022;31:101–10. https://doi.org/10.1016/j.vhri.2022.04.004.
Chun J, Jeong H, Kim Y. Age-varying susceptibility to the Delta variant (B16172) of SARS-CoV-2. JAMA Netw Open. 2022;5(3):e223064. https://doi.org/10.1001/jamanetworkopen.2022.3064.
Zhu S, Iboi E. Estimation of the reproduction number for COVID-19 based on latest vaccination results and the timing for herd-immunity: prospect for 2021. Fortune J Heal Sci. 2022;05(01):159–81. https://doi.org/10.26502/fjhs.051.
David J, Bragazzi N, Scarabel F, McCarthy Z, Wu J. Non-pharmaceutical intervention levels to reduce the COVID-19 attack ratio among children. R Soc Open Sci. 2022;9(3):211863. https://doi.org/10.1098/rsos.211863.
Di Fusco M, Marczell K, Deger K, Moran M, Wiemken T, Cané A, et al. Public health impact of the Pfizer-BioNTech COVID-19 vaccine (BNT162b2) in the first year of rollout in the United States. J Med Econ. 2022;25(1):605–17. https://doi.org/10.1080/13696998.2022.2071427.
Keeling M, Dyson L, Guyver-Fletcher G, Holmes A, Semple M, Tildesley M, et al. Fitting to the UK COVID-19 outbreak, short-term forecasts and estimating the reproductive number. Stat Methods Med Res. 2022;1–22. https://doi.org/10.1177/09622802211070257.
Aguilar-Canto F, Avila-Ponce de León U, Avila-Vales E. Sensitivity theorems of a model of multiple imperfect vaccines for COVID-19. Chaos Solitons Fractals. 2022;156:111844. https://doi.org/10.1016/j.chaos.2022.111844.
Barmpounakis P, Demiris N, Kontoyiannis I, Pavlakis GN, Sypsa V. Evaluating the effects of second-dose vaccine-delay policies in European countries: a simulation study based on data from Greece. PLoS One. 2022;17(4):1–13. https://doi.org/10.1371/journal.pone.0263977.
Omae Y, Kakimoto Y, Sasaki M, Toyotani J, Hara K, Gon Y, et al. SIRVVD model-based verification of the effect of first and second doses of COVID-19/SARS-CoV-2 vaccination in Japan. Math Biosci Eng. 2022;19(1):1026–40. https://doi.org/10.3934/mbe.2022047.
Wang X, Wang H, Ramazi P, Nah K, Lewis M. From policy to prediction: forecasting COVID-19 dynamics under imperfect vaccination. 2022. https://doi.org/10.1007/s11538-022-01047-x.
Layton A, Sadria M. Understanding the dynamics of SARS-CoV-2 variants of concern in Ontario, Canada: a modeling study. Sci Rep. 2022;12(1):1–16. https://doi.org/10.1038/s41598-022-06159-x.
Expósito D, Olmedo C, Limia A, Guzmán M, Carretero J. Impact of vaccination against COVID-19 in children aged 5–11 years: a mathematical model. Rev Esp Salud Publica. 2022;96:1–9.
Vilches T, Sah P, Moghadas S, Shoukat A, Fitzpatrick M, Hotez P, et al. COVID-19 hospitalizations and deaths averted under an accelerated vaccination program in northeastern and southern regions of the USA. Lancet Reg Heal - Am. 2022;6:100147. https://doi.org/10.1016/j.lana.2021.100147.
Chen X, Huang H, Ju J, Sun R, Zhang J. Impact of vaccination on the COVID-19 pandemic in U.S. states. Sci Rep. 2022;12(1):1–10. https://doi.org/10.1038/s41598-022-05498-z.
Bousquet A, Conrad W, Sadat S, Vardanyan N, Hong Y. Deep learning forecasting using time-varying parameters of the SIRD model for COVID-19. Sci Rep. 2022;12(1):1–13. | https://doi.org/10.1038/s41598-022-06992-0.
Shadi R, Fakharian A, Khaloozadeh H. Mathematical modeling of the novel coronavirus pandemic in Iran: a model with vaccination. In: 2022 8th International conference on control, instrumentation and automation. Tehran: IEEE; 2022. https://doi.org/10.1109/ICCIA54998.2022.9737192.
Gozzi N, Chinazzi M, Davis J, Mu K, Pastore y Piontti A, Vespignani A, et al. Preliminary modeling estimates of the relative transmissibility and immune escape of the Omicron SARSCoV2 variant of concern in South Africa. medRxiv. 2022. https://doi.org/10.1101/2022.01.04.22268721.
Schulenburg A, Cota W, Costa G, Ferreira S. Effects of infection fatality ratio and social contact matrices on vaccine prioritization strategies. Chaos. 2022;32(9). https://doi.org/10.1063/5.0096532.
Lasser J, Hell T, Garcia D. Assessment of the effectiveness of Omicron transmission mitigation strategies for European universities using an agent-based network model. arXiv. 2022. https://doi.org/10.1093/cid/ciac340.
Colosi E, Bassignana G, Contreras DA, Poirier C, Boëlle P-Y, Cauchemez S, et al. Screening and vaccination against COVID-19 to minimise school closure: a modelling study. Lancet Infect Dis. 2022;22(7):977–89. https://doi.org/10.1016/S1473-3099(22)00138-4.
Ko Y, May V, Mendoza R, Seo Y, Lee J, Lee J, et al. Multi-faceted analysis of COVID-19 epidemic in the Republic of Korea considering Omicron variant: mathematical modeling-based study. medRxiv. 2022. https://doi.org/10.1101/2022.04.15.22273907.
Matrajt L, Brown E, Cohen M, Dimitrov D, Janes H. Could widespread use of antiviral treatment curb the COVID-19 pandemic? A modeling study. medRxiv. 2022. https://doi.org/10.1186/s12879-022-07639-1.
Colosi E, Bassignana G, Barrat A, Lina B, Vanhems P, Bielicki J, et al. Minimizing school disruption under high incidence conditions due to the Omicron variant in early 2022. medRxiv. 2022. https://doi.org/10.1101/2022.02.04.22270473.
Hladish T, Pillai A, Longini I. Updated projections for COVID-19 Omicron wave in Florida. medRxiv. 2022. https://doi.org/10.1101/2022.01.06.22268849.
Hanly M, Churches T, Fitzgerald O, Post J, MacIntyre C, Jorm L. The impact of re-opening the international border on COVID-19 hospitalisations in Australia: a modelling study. Med J Aust. 2022;216(1):39–42. https://doi.org/10.5694/mja2.51291.
Zachreson C, Shearer F, Price D, Lydeamore M, Mcvernon J, Mccaw J, et al. COVID-19 in low-tolerance border quarantine systems: impact of the Delta variant of SARS-CoV-2. Sci Adv. 2022;3624(April):1–12. https://doi.org/10.1126/sciadv.abm3624.
Diarra M, Kebir A, Talla C, Barry A, Faye J, Louati D, et al. Non-pharmaceutical interventions and COVID-19 vaccination strategies in Senegal: a modelling study. BMJ Glob Heal. 2022;7(2):e007236. https://doi.org/10.1136/bmjgh-2021-007236.
Gomes M, Ferreira M, Corder R, King J, Souto-Maior C, Penha-Gonçalves C, et al. Individual variation in susceptibility or exposure to SARS-CoV-2 lowers the herd immunity threshold. J Theor Biol. 2022;540:111063. https://doi.org/10.1101/2020.04.27.20081893.
Hupert N, Marín-Hernández D, Gao B, Nixon D. Heterologous vaccination interventions to reduce pandemic morbidity and mortality: modeling the US winter 2020 COVID-19 wave. Proc Natl Acad Sci. 2022;119(3):e2025448119. https://doi.org/10.1073/pnas.2025448119.
Kahn R, Holmdahl I, Reddy S, Jernigan J, Mina M, Slayton R. Mathematical modeling to inform vaccination strategies and testing approaches for Coronavirus Disease 2019 (COVID-19) in nursing homes. Clin Infect Dis. 2022;74(4):597–603. https://doi.org/10.1093/cid/ciab517.
Avila-Ponce de León U, Avila-Vales E, Huang K. Modeling the transmission of the SARS-CoV-2 Delta variant in a partially vaccinated population. Viruses. 2022;14:158. https://doi.org/10.3390/v14010158.
Sanz-Leon P, Stevenson N, Stuart R, Abeysuriya R, Pang J, Lambert S, et al. Risk of sustained SARS-CoV-2 transmission in Queensland. Australia Sci Rep. 2022;12(1):1–9. https://doi.org/10.1038/s41598-022-10349-y.
Gavish N, Katriel G. Optimal vaccination at high reproductive numbers: sharp transitions and counter-intuitive allocations. 2022. https://doi.org/10.1098/rspb.2022.1525.
Gandjour A. Benefits, risks, and cost-effectiveness of COVID-19 self-tests from a consumer’s perspective. BMC Health Serv Res. 2022;22(1):1–8. https://doi.org/10.1186/s12913-021-07277-4.
Chapman L, Shukla P, Rodríguez-Barraquer I, Shete P, León T, Bibbins-Domingo K, et al. Risk factor targeting for vaccine prioritization during the COVID-19 pandemic. Sci Rep. 2022;12(1):1–12. https://doi.org/10.1038/s41598-022-06971-5.
Reyné B, Richard Q, Selinger C, Sofonea M, Djidjou-Demasse R, Alizon S. Non-markovian modelling highlights the importance of age structure on COVID-19 epidemiological dynamics. Math Model Nat Phenom. 2022;17(7). https://doi.org/10.1051/mmnp/2022008.
Bracis C, Moore M, Swan D, Matrajt L, Anderson L, Reeves D, et al. Improving vaccination coverage and offering vaccine to all school-age children allowed uninterrupted in-person schooling in King County, WA: modeling analysis. Math Biosci Eng. 2022;19(6). https://doi.org/10.3934/mbe.2022266.
Frazier P, Cashore J, Duan N, Henderson S, Janmohamed A, Liu B, et al. Modeling for COVID-19 college reopening decisions: Cornell, a case study. Proc Natl Acad Sci. 2022;119(2):e2112532119. https://doi.org/10.1073/pnas.2112532119.
Lin L, Chen B, Zhao Y, Wang W, He D. Two waves of COVID-19 in Brazilian cities and vaccination impact. SSRN. 3977464. 2021. https://doi.org/10.3934/mbe.2022216.
Gandjour A. Cost-effectiveness of future lockdown policies against the COVID-19 pandemic. Heal Serv Manag Res. 2022;09514848221080687. https://doi.org/10.1177/09514848221080687.
Hawkes M, Good M. Vaccinating children against COVID-19: commentary and mathematical modelling. MBio. 2022;13(1):e03789–21. https://doi.org/10.1128/mbio.03789-21.
Rajakaruna M, Rajakaruna H, Rajakaruna R. Dynamical regulations on mobility and vaccinations for controlling COVID-19 spread. Sci Rep. 2022;12(1):1–11. https://doi.org/10.1038/s41598-022-07371-5.
Rana P, Sharma N. The modeling and analysis of the COVID-19 pandemic with vaccination and treatment control: a case study of Maharashtra, Delhi, Uttarakhand, Sikkim, and Russia in the light of pharmaceutical and non-pharmaceutical approaches. Eur Phys J Spec Top. 2022;1–20. https://doi.org/10.1140/epjs/s11734-022-00534-5.
Berec L, Levínský R, Weiner J, Šmíd M, Neruda R, Vidnerová P, et al. Importance of vaccine action and availability and epidemic severity for delaying the second vaccine dose. Sci Rep. 2022;12(1):1–12. https://doi.org/10.1038/s41598-022-11250-4.
Zhang Y, Kapoor S. Modeling vaccinations, virus variants and lockdown: early guidance for SARS-CoV-2 health policies in India. medRxiv. 2022. https://doi.org/10.1101/2022.02.02.22270353.
Bugalia S, Tripathi J, Wang H. Mutations make pandemics worse or better: modeling SARS-CoV-2 variants and imperfect vaccination. arXiv. 2022. https://doi.org/10.48550/arXiv.2201.06285.
Demongeot J, Griette Q, Magal P, Webb G. Modeling vaccine efficacy for COVID-19 outbreak in New York city. Biology (Basel). 2022;11(3):345. https://doi.org/10.3390/biology11030345.
Mallela A, Neumann J, Miller E, Chen Y, Posner R, Lin Y, et al. Bayesian inference of state-level COVID-19 basic reproduction numbers across the United States. Viruses. 2022;14(1):157–75 . https://doi.org/10.3390/v14010157.
Saldaña J, Scoglio C. Influence of heterogeneous age - group contact patterns on critical vaccination rates for herd immunity to SARS - CoV - 2. Sci Rep. 2022;12(1):1–12. https://doi.org/10.1038/s41598-022-06477-0.
Schneider K, Tsoungui H, Adil N, Ngougoue P. Predicting the impact of COVID-19 vaccination campaigns - a flexible age-dependent, spatially-stratified predictive model, accounting for multiple viral variants and vaccines. medRxiv. 2022;1–25. https://doi.org/10.1371/journal.pone.0277505.
Castro e Silva A, Tristão A, Gonçalves E, Santana das Changas I, Dáttilo W, Barbosa A, et al. Successive pandemic waves with different virulent strains and the effects of vaccination for SARS-CoV-2. Vaccines. 2022;10(3):343. https://doi.org/10.3390/vaccines10030343.
Steyn N, Plank M, Binny R, Hendy S, Lustig A, Ridings K. A COVID-19 vaccination model for Aotearoa New Zealand. Sci Rep. 2022;12(1):1–11. https://doi.org/10.1038/s41598-022-06707-5.
Genari J, Goedert G, Lira S, Oliveira K, Barbosa A, Lima A, et al. Quantifying protocols for safe school activities. PLoS one. 2022;17(9):e0273425. https://doi.org/10.1371/journal.pone.0273425.
Giardina J, Bilinski A, Fitzpatrick M, Kendall E, Linas B, Salomon J, et al. Model-estimated association between simulated US elementary school-related SARS-CoV-2 transmission, mitigation interventions, and vaccine coverage across local incidence levels. JAMA Netw Open. 2022;5(2):e2147827. https://doi.org/10.1001/jamanetworkopen.2021.47827.
Rabiu M, Iyaniwura S. Assessing the potential impact of immunity waning on the dynamics of COVID-19 in South Africa: an endemic model of COVID-19. Nonlinear Dyn. 2022;1–21. https://doi.org/10.1007/s11071-022-07225-9.
Zou Y, Yang W, Lai J, Hou J, Lin W. Vaccination and quarantine effect on COVID-19 transmission dynamics incorporating Chinese-spring-festival travel rush: modeling and simulations. Bull Math Biol. 2022;84(2):1–19. https://doi.org/10.1007/s11538-021-00958-5.
Gavish N, Katriel G. The role of childrens’ vaccination for COVID-19 - Pareto-optimal allocations of vaccines. PLoS Comput Biol. 2022;18(2):1–30. https://doi.org/10.1371/journal.pcbi.1009872.
Pan J, Zhu W, Tian J, Liu Z, Xu A, Yao Y, et al. Vaccination as an alternative to non-drug interventions to prevent local resurgence of COVID-19. Infect Dis poverty. 2022;11(1):1–13. https://doi.org/10.1186/s40249-022-00960-6.
Buonomo B, Della Marca R, D’Onofrio A, Groppi M. A behavioural modelling approach to assess the impact of COVID-19 vaccine hesitancy. J Theor Biol. 2022;534:110973. https://doi.org/10.1016/j.jtbi.2021.110973.
Oloniiju S, Otegbeye O, Ezugwu A. Investigating the impact of vaccination and non-pharmaceutical measures in curbing COVID-19 spread:a South Africa perspective. Math Biosci Eng. 2022;19(1):1058–77. https://doi.org/10.3934/mbe.2022049.
Majumder A, Bairagi N. COVID-19 disease dynamics with vaccination: the effect of uncertainty. medRxiv. 2022;1–18. https://doi.org/10.1101/2022.01.10.22269006.
Lin L, Zhao Y, Chen B, He D. Multiple COVID-19 waves and vaccination effectiveness in the United States. Int J Environ Res public Heal. 2022;19(4):2282. https://doi.org/10.3390/ijerph19042282.
Bosetti P, Kiem C, Andronico A, Colizza V, Yazdanpanah Y, Fontanet A, et al. Epidemiology and control of SARS-CoV-2 epidemics in partially vaccinated populations: a modeling study applied to France. BMC Med. 2022;20(33):1–11. https://doi.org/10.1186/s12916-022-02235-1.
García Y, Mery G, Vásquez P, Calvo J, Barboza L, Rivas T, et al. Projecting the impact of COVID-19 variants and vaccination strategies in disease transmission using a multilayer network model in Costa Rica. Sci Rep. 2022;12(1):1–9. https://doi.org/10.1038/s41598-022-06236-1.
Tonkens S, Klaver P, Salazar M. Optimizing vaccine allocation strategies in pandemic outbreaks: an optimal control approach. arXiv. 2022. https://doi.org/10.48550/arXiv.2112.11908.
Liu F, Zhao Z, Ma C, Nie X, Wu A, Li X. Return to normal pre-COVID-19 life is delayed by inequitable vaccine allocation and SARS-CoV-2 variants. Epidemiol Infect. 2022;150:1–8. https://doi.org/10.1017/S0950268822000139.
Fierro A, Romano S, Liccardo A. Vaccination and variants: retrospective model for the evolution of COVID-19 in Italy. medRxiv. 2022. https://doi.org/10.1101/2022.02.27.22271593.
Omae Y, Sasaki M, Toyotani J, Hara K, Takahashi H. Theoretical analysis of the SIRVVD model for insights into the target rate of COVID-19/SARS-CoV-2 vaccination in Japan. IEEE Access. 2022;10:43044–54. https://doi.org/10.1109/ACCESS.2022.3168985.
Suphanchaimat R, Teekasap P, Nittayasoot N, Phaiyarom M, Cetthakrikul N. Forecasted trends of the new COVID-19 epidemic due to the Omicron variant in Thailand, 2022. bioRxiv. 2022. https://doi.org/10.3390/vaccines10071024.
Parolini N, Dede’ L, Ardenghi G, Quarteroni A. Modelling the COVID-19 epidemic and the vaccination campaign in Italy by the SUIHTER model. Infect Dis Model. 2022;7(2):45–63. https://doi.org/10.1016/j.idm.2022.03.002.
Du Z, Wang L, Bai Y, Wang X, Pandey A, Fitzpatrick M, et al. Cost-effective proactive testing strategies during COVID-19 mass vaccination: a modelling study. Lancet Reg Heal - Am. 2022;8:100182. https://doi.org/10.1016/j.lana.2021.100182.
Faucher B, Assab R, Roux J, Levy-Bruhl D, Tran C, Cauchemez S, et al. Agent-based modelling of reactive vaccination of workplaces and schools against COVID-19. Nat Commun. 2022;13(1):1–11. https://doi.org/10.1038/s41467-022-29015-y.
Ayoub H, Tomy M, Chemaitelly H, Altarawneh H, Coyle P, Tang P, et al. Estimating protection afforded by prior infection in preventing reinfection: applying the test-negative study design. medRxiv. 2022. https://doi.org/10.1101/2022.01.02.22268622.
Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hasell J, Appel C, et al. A global database of COVID-19 vaccinations. Nat Hum Behav. 2021,5:947–53. https://doi.org/10.1038/s41562-021-01122-8.
Kostkova P, Saigí-Rubió F, Eguia H, Borbolla D, Verschuuren M, Hamilton C, et al. Data and digital solutions to support surveillance strategies in the context of the COVID-19 pandemic. Front Digit Heal. 2021;3:707902. https://doi.org/10.3389/fdgth.2021.707902.
Christen P, Conteh L. How are mathematical models and results from mathematical models of vaccine-preventable diseases used, or not, by global health organisations? BMJ Glob Heal. 2021;6(9):e006827. https://doi.org/10.1136/bmjgh-2021-006827.
Chen S, Robinson P, Janies D, Dulin M. Four challenges associated with current mathematical modeling paradigm of infectious diseases and call for a shift. Open Forum Infect Dis. 2020;7(8). https://doi.org/10.1093/ofid/ofaa333.
Sauré D, O’Ryan M, Torres J, Zuniga M, Santelices E, Basso L. Dynamic IgG seropositivity after rollout of CoronaVac and BNT162b2 COVID-19 vaccines in Chile: a sentinel surveillance study. Lancet Infect Dis. 2022;22(1):56–63. https://doi.org/10.1016/S1473-3099(21)00479-5.
Liang H-Y, Wu Y, Yau V, Yin H-X, Lowe S, et al. SARS-CoV-2 variants, current vaccines and therapeutic implications for COVID-19. Vaccines. 2022;10(9):1538. https://doi.org/10.3390/vaccines10091538.
Acknowledgements
We would like to express our great appreciation to Edgar Gallo, León Nuñez, Diane Moyano, Carlos Pinto, Santiago Quevedo, Sofía Ríos, Sara Valencia, Diego Veloza, and Juan-Camilo Vargas for their valuable and constructive suggestions regarding this research work.
Funding
Pan-American Health Organization (PAHO) funded this study through the Contract CON22-00000261 with the Instituto de Evaluación Tecnológica en Salud (IETS), with the support of Koica and the District Health Secretariat of Bogotá.
The study results were independent and there was no interference from the contracting entity.
Author information
Authors and Affiliations
Contributions
OE: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, visualization, writing—original draft, and writing—review and editing. LM, JR, VB, CS, AR, DR, NB: data curation, investigation, methodology, formal analysis, visualization, writing—original draft, and writing—review and editing. CA, JC, CS, OF: validation, writing—original draft, and writing—review and editing. ARob: funding acquisition, validation and writing—review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not apply.
Consent for publication
All authors approved the final manuscript.
Competing interests
JC has a research grant from Pfizer for antimicrobial use, not related to this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Espinosa, O., Mora, L., Sanabria, C. et al. Predictive models for health outcomes due to SARS-CoV-2, including the effect of vaccination: a systematic review. Syst Rev 13, 30 (2024). https://doi.org/10.1186/s13643-023-02411-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02411-1