
Abstract
Background
Infection with resistant Pseudomonas aeruginosa (RPA) in the intensive care unit (ICU) is known to be either endogenous or exogenous or both, but the roles of each of these contamination routes are yet to be clarified. Data regarding prevalence, risk factors, and environmental factors associated with RPA in ICU are very scanty and even when they exist, they seem to be contradictory. So, there is a strong interest in understanding both individual and environmental factors associated with RPA infection. This systematic review aims to investigate individual and environmental factors associated with the colonization and infection with RPA in ICU.
Methodology
MEDLINE (Pubmed), EMBASE (OVID), the Cochrane Library (Wiley), Web of Science, CINAHL (EBSCOHost), and LILACS (BIREME) will be searched from inception onwards. Grey literature will be identified through Google Scholar and Open Grey. Two reviewers will independently screen all citations, abstracts, and full-text articles. Potential conflicts will be resolved through discussion. Methodological quality including bias will be appraised using appropriate approaches. A narrative synthesis will describe the quality and content of the epidemiological evidence. Prevalence, odds ratio, relative risk, and hazard radio with their respective 95% confidence intervals will be calculated. A meta-analysis of data extracted from eligible studies with similar populations and RPA testing will be performed. The analysis will evaluate factors influencing the estimates. A random effect model will be used to summarize effect sizes.
Discussion
Two contrasting hypotheses on risk factors of acquisition, colonization, and infection of RPA are being debated, especially in a context where available data are scanty or exhibit high discrepancy. Indeed, most of the reviews have been focalized on hospitalized patients, and not in ICU, and few of them address the issue of environmental factors. To fill that gap, this review will combine both analyses of individual and environmental risk factors using prevalence studies in ICU and evaluation of different methodologies. These two hypotheses will be tested and challenged and could serve as a basis for a more in-depth study to fill the methodological gaps that will be identified as part of this current review.
Systematic review registration
This protocol has been submitted to the Prospective Register of Systematic Reviews (PROSPERO) and the registration number attributed was CRD42021233832 of 07 March 2021.
Similar content being viewed by others
Background
Pseudomonas aeruginosa (PA) is a ubiquitous gram-negative bacterium with minimal survival requirements in the environment.
It has a remarkable ability to colonize environmental surfaces even when they are most hostile. PA can cause infections in patients, particularly when they are immunocompromised [1]. Infections by PA are among the major pathogens involved in healthcare-associated infections in intensive care units (ICUs) [2]. The prevalence of hospital-acquired PA carriage was 15.3% in the adult French population hospitalized in ICUs [3]. Furthermore, the resistance of P. aeruginosa to various antibiotics is increasing as is the case with the global burden of antibiotics resistance [4]. A cohort study conducted in Spain reported more than 80% of isolates susceptible only to amikacin and colistin and 9% only to colistin [5]. Infections due to resistant Pseudomonas aeruginosa (RPA) has been associated with increased morbidity and mortality rates [6, 7], increased length of stay in ICU, a high number of surgeries, and invasive procedures [6,7,8]. Although existing literature demonstrates increased costs related to resistant Gram-negative infections, data focused on P. aeruginosa are limited and somewhat inconsistent [8]. Infections with PA in ICU are known to be either endogenous or exogenous or both, but the role of each of these contamination routes is yet to be clarified [9]. Endogenous transmission has been widely described [2, 10], the main source of contamination being the intestinal microbiota under antibiotic pressure [10]. Exogenous transmission occurs from hydrous environments (tap, sink...), invasive medical devices, and the patients and health personnel through their hands [11, 12]. Most studies lean towards a predominance of the endogenous source, the exogenous source being more often incriminated in outbreaks [3, 11, 13]. Moreover, the source of RPA in ICU is not well established, as well as factors associated with the carriage, colonization, and, infection [9]. Data regarding prevalence, risk factors, and environmental factors associated with RPA in ICU are very scanty and even when they do exist, they seem contradictory. For example, a systematic review performed in 2018 demonstrated that there are considerable gaps and inconsistencies in knowledge regarding risk factors associated with RPA or identifying subgroups of patients at increased risk of acquisition of RPA in hospitals [12]. Unfortunately, this systematic review did not specifically address the issue in intensive care units and was limited to endogenous risk factors [12]. There is, therefore, growing interest in understanding the individual and environmental factors associated with resistant P. aeruginosa, particularly in intensive care units where high rates of morbidity and mortality are being observed [6, 9].
The main objective of this systematic review will be to investigate individual (endogenous) and environmental (exogenous) factors associated with the colonization and infection with resistant Pseudomonas aeruginosa in intensive care units. The secondary objectives of this study will be to (i) estimate the prevalence of multidrug-resistant P. aeruginosa colonization in ICU, (ii) describe the main risk factors of acquisition and colonization with multidrug-resistant P. aeruginosa in ICU, and (iii) describe the main environmental sources of acquisition and colonization with multidrug-resistant P. aeruginosa in ICU.
Methods/design
This systematic review and meta-analysis protocol are reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) checklist provided as an additional file [14].
Eligibility criteria
Type of studies to be included
This review will be included cross-sectional studies, case-control studies (nested or not), and cohort studies (either prospective, retrospective, or ambi-directional) conducted in intensive care units (ICUs). For the meta-analysis, only articles in which risk factors of MDR Pseudomonas aeruginosa acquisition/infection could be assessed will be selected. Studies without data on MDR-PA will be excluded. For multi-disease studies, when MDR-PA data will be not available separately in isolation, these studies will be excluded.
Type of participants
Studies include all patients, admitted to an ICU, whatever the reason for admission and the origin (community, another hospital, or another unit of the same hospital) of patients. No specific definition of ICU will be applied, and all studies which authors reported as having been conducted in an ICU will be considered. We will also include studies where it will possible to identify patients with specimens collected and tested for P. aeruginosa (positivity and antimicrobial susceptibility) during hospitalization and/or samples collected from the ICU patient’s environment (including staff hands and gloves) for P. aeruginosa testing. No specific restrictions on the type of patients will be applied.
Outcomes
The primary outcome
Factors of acquisition of MDR-PA. Since the year 2000, the most common definition of MDR used for gram-positive and gram-negative bacteria is ‘resistant to three or more antimicrobial classes [15].
Secondary outcomes
-
(i)
Risk factors of carriage. The carriage was defined as positive screened specimens. These specimens could be collected from rectal swabs, nasal swabs or tracheal aspiration, or others [16].
-
(ii)
Risk factors of colonization. Colonization was defined as positive clinical specimens and infection as positive clinical specimens with clinical signs confirming infection.
Search strategy
Six databases will be searched from inception onward, namely MEDLINE (Pubmed), EMBASE (OVID), the Cochrane Library (Wiley), Web of Science, CINAHL (EBSCOHost), and LILACS (BIREME). We will also search in grey literature through.
A search strategy using medical subject headings (MeSH) and text words related to Pseudomonas aeruginosa, intensive care units, carriage, colonization, or infection will be used (Table 1). For studies that will not be found via an internet search, the authors will be directly contacted to obtain them. Also, when a full text will be not available online, the author will be asked by email or telephone to provide it.
Study selection
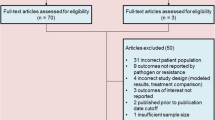
The search will be conducted by an experienced information specialist, with no language restrictions. For studies published in a language other than English, Deepl translate will be used for translation. The result of electronic searches will be uploaded to Rayyan software for duplicate identification and removal. After this phase, two reviewers will independently screen titles and abstracts of all studies yielded by the search strategy. Firstly, they will screen the studies according to the inclusion and exclusion eligibility criteria. Then, the full text of these selected studies will be retrieved for a second analysis to decide whether the study should be finally included or not. Disagreements between the two reviewers will be resolved through discussion and consensus. PRISMA-P flow diagram template will be used to describe the number of articles retrieved and screened at each step [14].
Data extraction
An online google form will be used to extract data from each included study by two independent reviewers. The following data will be extracted from each report:
-
Study characteristics: first author name, year of publication, number of recruitment centers, study design, and sampling method.
-
Participants: number of participants, region (s) and country/countries from which participants were recruited, study eligibility criteria, reasons for admission in ICU, age, gender, and duration of hospitalization.
-
P. aeruginosa carriage, colonization, or infection data: number of persons who acquired MDR-PA, number of persons who already had MDR-PA, antibiotic tested, number and type of environmental specimens.
-
Factors associated with resistant P. aeruginosa: all factors reported in studies will be collected in “authors’ own words” and with their corresponding effect estimates (odds ratios, relative risk, or hazard ratios).
Data synthesis and management
Firstly, a descriptive analysis will be performed on the characteristics of studies, persons included, and risk factors obtained. Secondly, prevalence, odds ratio, relative risk, and hazard ratio with their 95% confidence intervals will be calculated from the compiled data. Thirdly, a meta-analysis of case-control and cohort studies with a similar population, same parameters, and P. aeruginosa testing will be performed. The analysis will evaluate factors influencing the estimates. An analysis by a sub-group of endogenous factors and by subtypes of exogenous factors will be performed. A random effect model will be used to summarize effect sizes. Heterogeneity between combined studies will be tested using the standard Chi-square test with the Q statistic (p <0.10 statistically significant). The extent of heterogeneity will be quantified using the I2 statistics; I2>50% will be deemed as representing substantial inconsistency or significant statistical heterogeneity. Where statistical pooling will be not possible, results will be presented in a synthetic narrative form. All the analyses will be carried out using Stata version 15 (StataCorp, College Station, TX).
Quality of studies and evidence assessment
The methodological quality of studies will be assessed using the National Heart, Lung, and Blood Institute critical appraisal tools for each corresponding study design (cross-sectional, case-control, cohort). Potential bias in the design, conduct, and analysis of each study will be appraised by two independent reviewers. The confidence in evidence will be discussed among the authors.
Discussion
This current review will have the specificity that it will include only studies conducted in intensive care units. Another specificity of this present review is that it will focus on Pseudomonas aerugnisosa by including not only endogenous but also exogenous acquisition factors. Indeed, most of the reviews have been focalized on hospitalized patients, and not in ICU, and few of them address the issue of environmental factors. This ongoing review will combine both analyses of individual and environmental risk factors using prevalence study in ICU, assessing of risk factors, and evaluation of different methodologies. These two hypotheses will be tested and challenged and could serve as a basis for a more in-depth study to fill the methodological gaps that will be identified as part of this current review. This review will assess a great number of articles because the search will be based on open keywords. We will compare findings between this ongoing review and past reviews [8, 12].
This review will allow us to identify risk factors endogenous or exogenous of colonization or acquisition by MDR PA. This could be useful in identifying patients at high risk for MDR P. aeruginosa that may benefit from alternate empiric treatment.
The high level of heterogeneity expected between the articles to be evaluated raises concerns about the production of evidence-based and the applicability of the review results.
Availability of data and materials
The datasets used and/or analyzed during the current study will be available and could be shared with the readers.
Abbreviations
- CDBPH:
-
Centre for Development of Best Practices in Health
- CRFilMT:
-
Centre for Research on Filariasis and other Tropical Diseases
- GRADE:
-
Grading of Recommendations Assessment, Development, and Evaluation
- ICU(s):
-
Intensive care unit(s)
- PRISMA-P:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols
- PROSPERO:
-
Prospective Register of Systematic Reviews
References
Stanier RY, Palleroni NJ, Doudoroff M. The aerobic pseudomonads: a taxonomic study. J Gen Microbiol. mai. 1966;43(2):159–271.
Cohen R, Babushkin F, Cohen S, Afraimov M, Shapiro M, Uda M, et al. A prospective survey of Pseudomonas aeruginosa colonization and infection in the intensive care unit. Antimicrob Resist Infect Control. 2017;6:1–9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5225573/.
Hoang S, Georget A, Asselineau J, Venier AG, Leroyer C, Rogues AM, et al. Risk factors for colonization and infection by Pseudomonas aeruginosa in patients hospitalized in intensive care units in France. PloS One. 2018;13(3):e0193300.
Murray CJ, Ikuta KS, Sharara F, Swetschinski L, Aguilar GR, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet. 2022;399(10325):629–55.
Borgatta B, Lagunes L, Imbiscuso AT, Larrosa MN, Lujàn M, Rello J. Infections in intensive care unit adult patients harboring multidrug-resistant Pseudomonas aeruginosa: implications for prevention and therapy. Eur J Clin Microbiol Infect Dis. juill. 2017;36(7):1097–104.
Aloush V, Navon-Venezia S, Seigman-Igra Y, Cabili S, Carmeli Y. Multidrug-resistant Pseudomonas aeruginosa: risk factors and clinical impact. Antimicrob Agents Chemother. janv. 2006;50(1):43–8.
Micek ST, Lloyd AE, Ritchie DJ, Reichley RM, Fraser VJ, Kollef MH. Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment. Antimicrob Agents Chemother. 2005;49(4):1306–11.
Hirsch EB, Tam VH. Impact of multidrug-resistant Pseudomonas aeruginosa infection on patient outcomes. Expert Rev Pharmacoecon Outcomes Res. août. 2010;10(4):441–51.
Cuttelod M, Senn L, Terletskiy V, Nahimana I, Petignat C, Eggimann P, et al. Molecular epidemiology of Pseudomonas aeruginosa in intensive care units over a 10-year period (1998-2007). Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. janv. 2011;17(1):57–62.
Brzozowski M, Krukowska Ż, Galant K, Jursa-Kulesza J, Kosik-Bogacka D. Genotypic characterisation and antimicrobial resistance of Pseudomonas aeruginosa strains isolated from patients of different hospitals and medical centres in Poland. BMC Infect Dis. 2020;20(1):693.
Volling C, Thomas S, Johnstone J, Maltezou HC, Mertz D, Stuart R, et al. Development of a tool to assess evidence for causality in studies implicating sink drains as a reservoir for hospital-acquired gammaproteobacterial infection. J Hosp Infect. 2020;106(3):454–64.
Raman G, Avendano EE, Chan J, Merchant S, Puzniak L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2018;7:79.
Maatallah M, Cheriaa J, Backhrouf A, Iversen A, Grundmann H, Do T, et al. Population Structure of Pseudomonas aeruginosa from Five Mediterranean Countries: Evidence for Frequent Recombination and Epidemic Occurrence of CC235. PLoS ONE. 2011;6(10):e25617 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3184967/.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647.
Kumar VA, Khan S. Defining multidrug resistance in Gram-negative bacilli. Indian J Med Res. avr. 2015;141(4):491–2.
Bertrand X, Thouverez M, Talon D, Boillot A, Capellier G, Floriot C, et al. Endemicity, molecular diversity and colonisation routes of Pseudomonas aeruginosa in intensive care units. Intensive Care Med. août. 2001;27(8):1263–8.
Blanc DS, Francioli P, Zanetti G. Molecular Epidemiology of Pseudomonas aeruginosa in the Intensive Care Units – A Review. Open Microbiol J. 2007;1:8–11.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Med. 2009;6(7):e1000097.
Acknowledgements
The authors are grateful to Professor Joseph Kamgno, Head of the Department of Public Health of the Faculty of Medicine and Biomedical Sciences of the University of Yaoundé I and Director of the Centre for Research on Filariasis and other Tropical Diseases (CRFilMT), in Yaoundé Cameroon for his intellectual contribution to the discussions related to this study. The authors are also thankful to the staff of the Centre for Development of Best Practices in Health (CDBPH), in Yaounde Cameroon, Ecole Doctorale Galilée of the University of Sorbonne Paris Nord, and the IAME laboratory in Paris, France for their support.
Funding
This study is supported by the “Bourse du mérite” of Ecole Doctorale Galillée of the University of Sorbonne Paris Nord (Paris, France). The funding body has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Contributions
ES, HCND, GSW, and JRZ designed the study and drafted the protocol. CDE critically reviews and adjusts the search strategy. MGF, MZV, ACZ, SM, and POZ reviewed the article for intellectual content. SE and JRZ are the guarantors of this study. All the authors approved the final version of this protocol.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable as all the data will be secondary.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Eyebe, S., Nana-Djeunga, H.C., Guewo-Fokeng, M. et al. Risk factors for colonization and infection with multidrug-resistant Pseudomonas aeruginosa in intensive care unit: protocol for a systematic review and meta-analysis. Syst Rev 11, 270 (2022). https://doi.org/10.1186/s13643-022-02143-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-02143-8