
Abstract
Background
In an unparalleled global response, during the COVID-19 pandemic, 90 countries asked 3.9 billion people to stay home. Yet other countries avoided lockdowns and focused on other strategies, like contact tracing. How effective and cost-effective are these strategies? We aimed to provide a comprehensive summary of the evidence on past pandemic controls, with a focus on cost-effectiveness.
Methods
Following PRISMA guidelines, MEDLINE (1946 to April week 2, 2020) and EMBASE (1974 to April 17, 2020) were searched using a range of terms related to pandemic control. Articles reporting on the effectiveness or cost-effectiveness of at least one intervention were included.
Results
We found 1653 papers; 62 were included. The effectiveness of hand-washing and face masks was supported by randomized trials. These measures were highly cost-effective. For other interventions, only observational and modelling studies were found. They suggested that (1) the most cost-effective interventions are swift contact tracing and case isolation, surveillance networks, protective equipment for healthcare workers, and early vaccination (when available); (2) home quarantines and stockpiling antivirals are less cost-effective; (3) social distancing measures like workplace and school closures are effective but costly, making them the least cost-effective options; (4) combinations are more cost-effective than single interventions; and (5) interventions are more cost-effective when adopted early. For 2009 H1N1 influenza, contact tracing was estimated to be 4363 times more cost-effective than school closure ($2260 vs. $9,860,000 per death prevented).
Conclusions and contributions
For COVID-19, a cautious interpretation suggests that (1) workplace and school closures are effective but costly, especially when adopted late, and (2) scaling up as early as possible a combination of interventions that includes hand-washing, face masks, ample protective equipment for healthcare workers, and swift contact tracing and case isolation is likely to be the most cost-effective strategy.
Similar content being viewed by others

Key points
-
Randomized trial evidence was only available to support the effectiveness of hand-washing and face masks, both highly cost-effective measures. For other interventions, only evidence from observational and modelling studies was available.
-
This lower-quality evidence suggests that overall, when timed appropriately, the following interventions are likely to be highly cost-effective: contact tracing and case isolation, protective equipment for healthcare workers, and vaccination prior to the outbreak (when available). Surveillance networks and protective equipment for healthcare workers also appear to be cost-effective.
-
The least cost-effective interventions appear to be social distancing measures, like workplace and school closures. The evidence suggests that these are more cost-effective for severe viruses and when timed early in the outbreak.
Background
On March 11, 2020, the World Health Organization (WHO) characterized COVID-19 as a pandemic. In an unparalleled global response, more than 90 countries or territories have asked about half of the world’s population to stay home [1]. During that time, over 1.5 billion (almost 90%) of the world’s students were affected by nationwide school closure [2]. Some countries focused on other interventions, such as contact tracing, which has been estimated to be 4363 times more cost-effective than school closure for H1N1 influenza ($2260 vs. $9,860,000 per death prevented) [3]. Indeed, closing school is costly—$10 to $47 billion for 4 weeks in the US alone [4]. As countries around the world are faced with the ongoing challenge of balancing public health interventions with economic, ethical, social, and legal considerations, evidence on the effectiveness and cost-effectiveness of these interventions is needed to guide policy and avoid unnecessary harm.
An earlier systematic review of non-pharmaceutical interventions to reduce influenza transmission in adults included only randomized trials, analysed 7 studies, and concluded that the evidence was lacking for most interventions [5]. While we do not dispute this conclusion when looking only at randomized trials, we would argue that as decisions of unknown cost-effectiveness are made in reaction to the COVID-19 pandemic, some evidence, even if of lower quality, is better than no evidence at all. Therefore, we turned to past pandemics and included a broad range of study designs in this review to provide a comprehensive summary of the evidence on epidemic control, with a focus on cost-effectiveness, to draw lessons applicable to COVID-19.
Methods
Following PRISMA systematic review guidelines [6], MEDLINE (1946 to April week 2, 2020) and EMBASE (1974 to April 17, 2020) were searched using the terms “non-pharmaceutical interventions”, “outbreak control”, “outbreak interventions”, “epidemic control”, “epidemic interventions”, “pandemic control”, and “pandemic interventions” (last search: April 19, 2020). Reference lists and PubMed-related articles of included studies were reviewed to find additional articles. Reviews (all types), randomized trials, observational studies, and modelling studies were included. Articles reporting on the effectiveness or cost-effectiveness of at least one intervention were included. We defined effectiveness as success in producing the desired outcome, and cost-effectiveness as doing so with minimum economic cost (in dollar value). Articles in English, French, Spanish, and Portuguese were included. Studies of sexually transmitted infections (e.g. syphilis) and mosquito-borne diseases (e.g. dengue) were not included. Abstracts, case reports, and conference proceedings were also excluded. Hand-washing and face masks were the focus of a number of reviews [5, 7, 8] and a recent meta-analysis [9, 10], so individual studies of their effectiveness were also excluded. Likewise for school closure [11,12,13,14]. Titles were screened by a single investigator. Abstracts and full texts were screened by two investigators. Discrepancies were solved by mutual agreement. Key characteristics of studies were recorded in a spreadsheet, including first author, year of publication, study design, interventions studied, and a summary of findings. Quality assessment was limited to grouping studies based on design into two categories: higher quality (randomized trials) and lower quality (other designs). Meta-analysis was not feasible due to the heterogeneous set of interventions studied, as well as substantial differences in study designs, outcomes, and effect measures. We synthesized results narratively.
Findings
Result of the systematic review
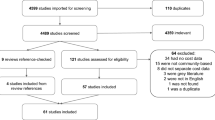
A total of 2742 papers were found. Removing duplicates left 1653. We retained 622 based on title, 137 based on abstract, and 39 based on full text. We found 23 additional studies via reference lists and PubMed-related article searches (eFigure in the Supplement). Therefore, a total of 62 studies were included (Table 1). Randomized trial evidence was only available to support the effectiveness of hand-washing and face masks [5, 7,8,9,10]. For other interventions, only lower-quality (observational and modelling) evidence was available.
Cost-effectiveness of interventions
Pasquini-Descomps et al. [15] conducted a systematic review of the cost-effectiveness of interventions in H1N1 influenza. They found 18 studies covering 12 interventions: disease surveillance networks (very cost-effective), contact tracing and case isolation (very cost-effective), face masks (very cost-effective), preventive measures in hospitals (cost-effective), antiviral treatment (cost-effective), antiviral prophylaxis (cost-effective), low efficiency vaccination (cost-effective if timed before cases peak), high efficiency vaccination (cost-effective if timed before cases peak), stockpiling antiviral medicine (cost-effective for high-income countries), quarantining confirmed cases at home (cost-effective for viruses with a case fatality rate of 1%, not cost-effective for viruses with a case fatality rate of 0.25%), self-isolation at home (cost-effective with a case fatality rate of 1%, not cost-effective with a case fatality rate of 0.25%), and school closure (not cost-effective). Based on these findings, Madhav et al. [3] estimated that for H1N1 influenza, contact tracing was 4363 times more cost-effective than school closure ($2260 vs. $9,860,000 per death prevented). Other systematic reviews found that school closures did not help control of the 2003 SARS epidemic in China, Hong Kong, and Singapore and would prevent only 2–4% of COVID-19 deaths [14]; reduced the peak of epidemics by 29.65% on average and were more effective when timed early [11]; are most effective when they cause large reductions in contact, when the basic reproduction number is below 2, and when attack rates are higher in children than in adults [12]; and appeared to be moderately effective in reducing the transmission of influenza and in delaying the peak of an epidemic, but were associated with very high costs [13]. Differences in publication date, virus transmissibility, and study selection may explain the discrepancies among these reviews.
Using data from Wang et al. [16] and Pasquini-Descomps et al. [15] found that contact tracing and case isolation was one of the most cost-effective interventions to control H1N1 in Hubei, China (less than $1000 per disability-adjusted life year). In a simulation study, Hellewell et al. [17] found that in most scenarios, highly effective contact tracing and case isolation would be enough to control a new outbreak of COVID-19 within 3 months. Transmissibility was an important factor, i.e. when Ro = 2.5, 80% of contacts needed to be traced and isolated. Timing was another important factor—with five initial cases, there was a greater than 50% chance of achieving control, even at lower contact-tracing levels. However, at 40 initial cases, control was much less likely. Similarly, any delay from symptom onset to isolation decreased the probability of control, highlighting the need for swift action. Furthermore, Armbruster and Brandeau [18] found that contact tracing is cost-effective only when population prevalence is still low (e.g. under 8% for tuberculosis). In a systematic review, Halton et al. [19] found that contact tracing and progressively earlier isolation of probable SARS cases were associated with the control of SARS outbreaks in Southeast Asia. In another review, Bell et al. [20] recommended contact tracing and case isolation at the start of an outbreak, but not in the late phase, when there is increased and sustained transmission in the general population. In a modelling study, Zhang et al. [21] found that voluntary self-isolation at symptom onset can achieve the same level of effectiveness as antiviral prophylaxis, but that this strategy had a limited effect on reducing transmission when delayed by 2 days. Young et al. [22] also found that delays could prevent case isolation from stopping incipient outbreaks. Li et al. [23] found that in the 2009 H1N1, quarantine of close contacts in Beijing reduced confirmed cases by a factor of 5.6. However, since H1N1 was mild, they concluded that this was not an economically effective measure. In another modelling study, Tuncer et al. [24] found that social distancing had the most impact on the 2014 Ebola epidemic in Liberia, followed by isolation and quarantine. Case isolation, household quarantine, and contact tracing were the most effective interventions in four other modelling studies [25,26,27,28]. Collectively, in the context of COVID-19, these studies suggest that these interventions can be effective and cost-effective, and highly so when implemented early and executed swiftly.
Saunders-Hastings et al. [9, 10] carried out a systematic review and meta-analysis of personal protective measures to reduce pandemic influenza transmission. Meta-analyses suggested that regular hand hygiene provided a significant protective effect (OR = 0.62; 95% CI 0.52–0.73). Face masks had a non-significant protective effect (OR = 0.53; 95% CI 0.16–1.71), which became significant (OR = 0.41; 95% CI 0.18–0.92) when randomized control trials and cohort studies were pooled with case–control studies (this also decreased heterogeneity). In an earlier systematic review, Jefferson et al. [7] also found a protective effect of masks. Overall, they were the best performing intervention across populations, settings, and threats. Similarly, in a narrative review, MacIntyre and Chughtai [8] drew on evidence from randomized community trials to conclude that face masks do provide protection against infection in various community settings, subject to compliance and early use. Differences in publication date, search strategy, and study selection criteria may explain the discrepancies among these reviews. Tracht et al. [29] estimated savings of $573 billion if 50% of the US population used masks in an unmitigated H1N1 epidemic. For hand-washing, Townsend et al. [30] estimated that a national behaviour change programme in India would net $5.6 billion (3.4–8.6), a 92-fold return on investment. A similar programme in China would net $2.64 billion (2.08–5.57), a 35-fold return on investment.
Preventive measures in hospitals include the use of personal protective equipment for healthcare workers in direct contact with suspected patients. Dan et al. [31] estimated that this measure was cost-effective for H1N1 ($23,600 per death prevented). However, adopting a wider set of measures (full personal protective equipment, restricting visitors, and cancelling elective procedures) was much less cost-effective ($2,500,000 per death prevented). Similarly, Lee et al. [32] found that increasing hand hygiene, use of protective apparel, and disinfection are the most cost-saving interventions to control a hospital outbreak of norovirus. If they are not adequately protected, healthcare workers can contribute disproportionately to the transmission of the infection [33].
Suphanchaimat et al. [34] found that influenza vaccination for prisoners in Thailand was cost-effective. The incremental cost-effectiveness ratio of vaccination (compared with routine outbreak control) was $1282 to $1990 per disability-adjusted life year. Shiell et al. [35] also found that vaccination (for measles) was cost-effective ($32.90 marginal cost per case prevented). Prosser et al. [36] also found that H1N1 vaccination in the US was cost-effective under many assumptions if initiated prior to the outbreak. Incremental cost-effectiveness ratios ranged from $8000 to $52,000 per quality-adjusted life year for persons aged 6 months to 64 years without high-risk conditions. The authors noted that all doses (two for some children, one for adults) should be delivered before the epidemic peak. Similarly, in a modelling study, Nguyen et al. [37] found that vaccination should be administered 5 months before to 1 week after the start of an epidemic to be cost-effective. If vaccine supplies are limited, Lee et al. [38] found that priority should be given to at-risk individuals and to children within high-risk groups. Likewise, Van Genugten et al. [39] estimated similar results from vaccinating the entire population versus only at-risk groups. Herrera-Diestra and Meyers [40] found that vaccinating based on the number of infected acquaintances is expected to prevent the most infections while requiring the fewest intervention resources. Optimal control modelling studies also suggest that early intervention and vaccination are more cost-effective and that interventions before vaccines are available need to be balanced with the potential gains of future vaccines or the potential for multiple outbreaks [41,42,43].
In another systematic review of economic evaluations, Pérez Velasco et al. [44] examined 44 studies and found that combinations of pharmaceutical and non-pharmaceutical interventions were more cost-effective than vaccines and/or antivirals alone. Reducing non-essential contacts, using pharmaceutical prophylaxis, and closing schools was the most cost-effective combination for all countries. However, quarantine for household contacts was not cost-effective, even in low- and middle-income countries. A modelling study by Day et al. [45] suggested that quarantine (of all individuals who have had contact with an infected individual) would be beneficial only when case isolation is ineffective, when there is significant asymptomatic transmission, and when the asymptomatic period is neither very long nor very short.
Perlroth et al. [46] estimated the health outcomes and costs of combinations of 4 social distancing strategies and 2 antiviral medication strategies. For a virus with a case fatality rate of 1% and a reproduction number of 2.1 or greater, school closure alone was the least cost-effective intervention and cost $32,100 per case averted. Antiviral treatment ($18,200), quarantine of infected individuals ($15,300), and adult and child social distancing ($5600) had increasing levels of cost-effectiveness. However, combining interventions was more cost-effective, and the most cost-effective combination included adult and child social distancing, school closure, and antiviral treatment and prophylaxis ($2700 per case). However, the same combination without school closure was more cost-effective for milder viruses (case fatality rate below 1%, reproduction number 1.6 or lower). If antivirals are not available, the combination of adult and child social distancing and school closure was most effective. Similarly, in another modelling study, Bolton et al. [47] found that a combination of non-pharmaceutical interventions proved as effective as the targeted use of antivirals.
In a similar study of cost-effectiveness, Saunders-Hastings et al. [10] examined a range of interventions (school closure, community-contract reduction, hand hygiene, face mask, voluntary isolation, quarantine, vaccination, antiviral prophylaxis, antiviral treatment) in response to a simulated pandemic similar to the 1957 H2N2. In a population of 1.2 million, with no intervention, 9421 life-years were lost. Vaccination plus antiviral treatment was the most cost-effective intervention (cost per life-year saved: $2581). However, it still led to 3026 life-years lost. Only 1607 life-years were lost at a marginally higher cost ($6752 per life-year) with a combination of interventions including community-contact reduction, hand hygiene, face masks, voluntary isolation, and antiviral therapy. Combining all interventions saved the most lives (only 267 life-years lost), but was very costly ($199,888 per life-year saved) due to school closure and workdays lost.
Halder et al. [48] aimed to determine the most cost-effective interventions for a pandemic similar to H1N1. They found that a combination of interventions was the most cost-effective. This combination included treatment and household prophylaxis using antiviral drugs and limited duration school closure ($632 to $777 per case prevented). If antiviral drugs are not available, limited duration school closure was significantly more cost-effective compared to continuous school closure. Other social distancing strategies, such as reduced workplace attendance, were found to be costly due to productivity losses. Closing school for 2 to 4 weeks without other interventions did not cost much more than doing nothing but gave a significant 34 to 37% reduction in cases, if optimally timed.
Studies on intervention effectiveness without cost-effectiveness analysis
Smith et al. [5] carried out a systematic review of non-pharmaceutical interventions to reduce the transmission of influenza in adults. Only randomized trials were included, and 7 studies met all selection criteria. The authors found that positive significant interventions included professional oral hygiene intervention in the elderly and hand-washing, and noted that home quarantine may be useful, but required further assessment.
Jefferson et al. [7] conducted a Cochrane systematic review of physical interventions to interrupt or reduce the spread of respiratory viruses. They found that the highest quality randomized cluster trials suggested this could be achieved by hygienic measures such as hand-washing, especially around younger children. They recommended that the following effective interventions be implemented, preferably in a combined fashion, to reduce transmission of viral respiratory disease: frequent hand-washing with or without adjunct antiseptics; barrier measures such as gloves, gowns, and masks with filtration apparatus; and suspicion diagnosis with isolation of likely cases.
Lee et al. [49] carried out a systematic review of modelling studies quantifying the effectiveness of strategies for pandemic influenza response. They found that combinations of strategies increased the effectiveness of individual strategies and could reduce their potential negative impact. Combinations delayed spread, reduced the overall number of cases, and delayed and reduced peak attack rate more than individual strategies. Similar results were found by Martinez and Das [50]. In another systematic review of 12 modelling and three epidemiological studies, Ahmed et al. [51] found that workplace social distancing reduced cumulative influenza attack rate by 23%. It also delayed and reduced the peak attack rate.
Pan et al. [52] examined associations between public health interventions and the epidemiology of COVID-19 in Wuhan, China. Traffic restrictions, cancellation of social gatherings, and home quarantines were associated with reduced transmission, but were not sufficient to prevent increases in confirmed cases. These were reduced and estimates of the effective reproduction number fell below 1 only when additional interventions were implemented. Those included hospital-based measures (designated hospitals and wards, use of personal protective equipment, increased testing capacity, accelerated reporting, and timely medical treatment) and community-based interventions (quarantine of presumptive cases and quarantine of confirmed cases of their close contacts in designated facilities).
Markel et al. [53] examined non-pharmaceutical interventions in US cities during the 1918–1919 influenza pandemic (isolation or quarantine, school closure, public gathering ban). They found that all 43 cities in the study adopted at least one of these interventions and that 15 cities applied all three. The most common combination (school closure and public gathering bans) was implemented in 34 cities (79%) for a median duration of 4 weeks and was significantly associated with reductions in weekly excess death rate. Cities that implemented interventions earlier had greater delays in reaching peak mortality (Spearman r=−0.74, P<0.001), lower peak mortality rates (Spearman r=0.31, P=.02), and lower total mortality (Spearman r=0.37, P=.008). There was a significant association between increased duration of interventions and a reduced total mortality burden (Spearman r=−0.39, P=.005). Another similar, historical study of US cities found that early intervention was associated with lower mortality (R2=0.69, P<0.01) [54].
Ishola and Phin [55] reviewed the literature on mass gatherings. They found 24 studies and cautiously concluded that there is some evidence to indicate that mass gatherings may be associated with an increased risk of influenza transmission. In a more recent systematic review, Rainey et al. [56] found that mass gathering-related respiratory disease outbreaks were relatively rare between 2005 and 2014 in the US. They concluded that this could suggest—perhaps surprisingly—low transmission at most types of gatherings, even during pandemics. Similarly, in a US survey of 50 State Health Departments and 31 large local Health Departments, Figueroa et al. [57] found that outbreaks at mass gatherings were uncommon, even during the 2009 H1N1 pandemic. In a modelling study, Shi et al. [58] found that mass gatherings that occur within 10 days before the epidemic peak can result in a 10% relative increase in peak prevalence and total attack rate. Conversely, they found that mass gatherings may have little effect when occurring more than 40 days earlier or 20 days after the infection peak (when initial Ro = 1.5). Thus, the timing of mass gatherings might explain the apparent lack of evidence in support of their ban.
Recently, Zhao et al. [59] quantified the association between domestic travel out of Wuhan, China, and the spread of SARS-CoV-2. Using location-based data, they estimated that each increase of 100 in daily new cases and daily passengers departing from Wuhan was associated with an increase of 16.25% (95% CI: 14.86–17.66%) in daily new cases outside of Wuhan. Ryu et al. [60] conducted a systematic review of international travel restrictions, screening of travellers, and border closure. They examined 15 studies and concluded that the evidence did not support entry screening as an effective measure and that travel restrictions and border closures would have limited effectiveness in controlling pandemic influenza. In another systematic review, Mateu et al. [61] concluded that the evidence did not support travel restrictions as an isolated intervention for the containment of influenza and that restrictions would be extremely limited in containing the emergence of a pandemic virus. Chong and Ying Zee [62] modelled the impact of travel restrictions on the 2009 H1N1 pandemic in Hong Kong. They estimated that restricting air travel from infected regions by 99% would have delayed the epidemic peak by up to 2 weeks. Restricting both air and land travel (from China) delayed the peak by about 3.5 weeks. However, neither 90% nor 99% travel restrictions reduced the epidemic magnitude by more than 10%, and antiviral treatment and hospitalization of infectious subjects were found to be more effective than travel restrictions. Chinazzi et al. [63] modelled the impact of travel limitations on the spread of COVID-19. They estimated that the travel quarantine of Wuhan delayed the overall epidemic progression by 3 to 5 days in mainland China and reduced international case importations by nearly 80% until mid-February. In addition, sustained 90% travel restrictions to and from China only modestly affected the epidemic trajectory, unless combined with a 50% or higher reduction of transmission in the community. Bell et al. [64] point out that screening international travellers who depart infected countries (instead of all travellers entering all countries) would be a better use of resources. Case in point: Zhang et al. [65] reported that in the 2009 H1N1, only 132 of the 600,000 travellers who underwent border entry screening in Beijing were infected (0.02%). Travel limitations may be more effective when neighbouring countries fail to implement adequate outbreak control efforts [66, 67].
We found little evidence to support the following interventions: (1) communicating health risk and promoting disease control measures in low- and middle-income countries (evidence not conclusive according to a review by [68]); (2) screening to contain spread, at the borders or locally (even under best-case assumptions, more than half of infected people would be missed, according to a modelling study by [69]).
Discussion
This systematic review aimed to provide a comprehensive summary of the evidence on pandemic control, with a focus on cost-effective interventions in the context of COVID-19. Randomized trial evidence was only available to support the effectiveness of hand-washing and face masks, both highly cost-effective measures during past pandemics. For other interventions, only evidence from observational and modelling studies was available. This lower-quality evidence suggests that overall, when timed appropriately, the following interventions were likely to be highly cost-effective: contact tracing and case isolation, protective equipment for healthcare workers, and vaccination prior to the outbreak (when available). Surveillance networks and protective equipment for healthcare workers also appeared to be cost-effective. Home quarantine for confirmed cases and stockpiling antivirals appeared less cost-effective. The least cost-effective interventions appeared to be social distancing measures like workplace and school closures. However, the evidence suggests that these could still be cost-effective when timed early in the outbreak, and when viruses were severe (with high mortality or morbidity, leading to high costs). Vaccination past the peak of infections and long-term school closure late in the outbreak appeared less cost-effective, underscoring the importance of timing.
What lessons can policymakers learn from past pandemics? Three major underlying themes stand out. First, timing and preparedness. Our findings suggest interventions are more effective when timed early. But paradoxically, some interventions may take months, or even years to prepare (e.g. establishing effective disease surveillance networks). This highlights the importance of pandemic preparedness. Learning from past pandemics, policymakers may be well advised to develop ahead of time clear, actionable pandemic response plans and to allocate the necessary human, financial, and logistical resources. Second, individual vs. population-level interventions. In general, interventions that focus on individuals appear more cost-effective (e.g. promoting hand-washing, tracing contacts, and providing personal protective equipment for healthcare workers). In contrast, interventions that apply to entire populations appear less cost-effective (e.g. closing workplaces and schools). Individual-level interventions may also be more feasible and acceptable. Indeed, infected individuals may comply with targeted interventions more readily than entire populations, in which healthy and otherwise well-functioning people may come to question the legitimacy of public health measures, especially when heavy-handed and long-lasting, thus raising ethical and legal considerations. Third, at-risk groups. In general, interventions that target individuals appear even more cost-effective when they focus on at-risk groups (e.g. prioritizing at-risk individuals for vaccination). For COVID-19, at-risk groups include older people and those with chronic diseases. Programmes like the UK’s shielding scheme have focused on these groups [70]. By definition, at-risk groups have the most potential for prevention, and they would also seem more likely to welcome interventions. Still, from a critical perspective, all the above raises important questions. How far are we willing to go to save a life? How much are we willing to spend to do so? How much are we willing to restrict freedom, and for how long? And are all lives equally worth saving? The answer to these questions should be made explicit, and policymakers in democratic countries may wish to consult the population before assuming that all lives should be saved at all cost. Finally, these findings can be further criticized for the strength of the evidence in their support, or lack thereof. Indeed, as higher-quality evidence was only available to support hand-washing and face masks, policymakers would be hard-pressed to justify the continued use of all control measures in any pandemic based on scientific evidence alone. Should policymakers wish to do so, we believe they should communicate transparently about the evidence base, and all the other factors weighing on their decision-making process.
How can these lessons from past pandemics be translated to the current COVID-19 pandemic? Key differences emerge. The incubation period is longer for COVID-19 (6.4 days) than for influenza type A (3.4 days) [71]. This poses challenges, as cases can infect others during the incubation period. Likewise, while only about 20% (95% CI: 17–25) of cases remain asymptomatic throughout infection, asymptomatic transmission does occur, albeit at a lower rate (relative risk: 0.35, 95% CI 0.10–1.27) [72]. This in turn poses substantial challenges to one of the most cost-effective measures in past pandemics, namely contact tracing. Indeed, modelling studies suggest that to stop the spread of COVID-19, public health practitioners only have 2–3 days from the time a new case develops symptoms, to isolate the case and quarantine its contacts [73]. Otherwise, cases tend to surge, and tracing efforts can become overwhelming. This may explain why many countries failed to control COVID-19 with contact tracing—the UK, for example, spent ten billion pounds on its test and trace programme, which may not have been effective [74].
Another key difference between COVID-19 and influenza is the duration of hospitalization. It is longer for COVID-19 (14 days) than for influenza (6.5–6.7 days) [71]. This may partially explain why intensive care units around the world were overburdened during the COVID-19 pandemic. Public health officials therefore aimed to “flatten the curve”. In doing so, when all other control measures fell short, they sometimes used the least cost-effective interventions of past pandemics (workplace and school closures). Past pandemics indicate that these measures are more cost-effective when timed early in the outbreak, and when caseloads are severe. That they have been used at multiple times before and during outbreaks in this pandemic, and for various durations, may explain the wide range of estimates calculated for their cost-effectiveness during the COVID-19 pandemic. These range from net benefits of $5.2 trillion [75] to costs being “at least 5–10 times” greater than benefits ([76], p.1). While their cost-effectiveness is still debated, two studies have found that less disruptive (and economical) interventions can be as effective as more restrictive (and costly) ones [77, 78]. The cost-effectiveness of interventions also depends on virus severity. For SARS-CoV-2, estimates of case fatality rates range from 1 to 7.2% [79], making it more severe than influenza and other respiratory viruses of past pandemics. To some extent, this may justify more costly measures.
Another defining characteristic of the COVID-19 pandemic is the emergence of virus variants, leading to concerns of immunity escape [80]. At the time of writing, the WHO designates four variants of concern: Alpha, Beta, Gamma, and Delta [81]. These evolve under selective pressure, are more transmissible, and may escape immunity conferred by infection or vaccination. Indeed, data suggest that some vaccines are less effective against variants B.1.351 (Beta) [82] and B.1.617.2 (Delta) [83]. Evidence from previous pandemics indicates that vaccinating past the peak of infections may not be cost-effective, yet in the current COVID-19 pandemic, as the ability to develop vaccines more rapidly has become apparent, along with multiple waves of infections, it might still be worth vaccinating past the peak, as there may be future waves once restrictions are eased. While there is no doubt that in most jurisdictions, the majority of the population has not yet been infected, some data suggest that COVID-19 can surge even in areas with high seroprevalence from past infection (e.g. 76% in Manaus, Brazil [84];) or high vaccination (e.g. 78% in Israel [85];). In this context, vaccine cost-effectiveness may be lower than hoped, especially if annual booster shots are needed [86]. Likewise, if other measures fail to prevent surges due to variants, workplace and school closures, if they are to be used again, should be timed early as daily new cases surge.
Cost-effectiveness is also shaped by cultural and behavioural responses to interventions. Culture awareness has arguably become a critical input to the successful design and implementation of effective and equitable health policies [87, 88]. Cultural and behavioural traits, while largely overlooked in the literature, are likely to play a pivotal role in shaping policy responses and assessing sanitary outcomes in the ongoing COVID-19 pandemic. Empirical evidence supports this otherwise intuitive claim, notably Erman and Medeiros’ [89] meta-study of 73 countries, accounting for ca. 93% of confirmed cases and 96% of deaths directly attributed to COVID during the first wave of the pandemic (up to September 2020), as cultural/behavioural attributes (e.g. uncertainty avoidance and long-term vs. short-term normative orientation) significantly impact public health outcomes (i.e. crude test positivity, case/infection fatality, and mortality risk). Along the same lines, a study of 1140 residents of the UK and Ireland, accounting for a culturally diverse sample across the Americas (North, Central and South), Asia and Europe, provides evidence on significant mean differences (MANCOVA) in physical and mental behaviours during the pandemic, attributable to cultural differences [90], arguably reinforcing the claim that cost-effectiveness should be assessed through cultural and behavioural lenses.
As noted, the cost-effectiveness of interventions depends on their timing and virus severity. Taking this into account, we propose a 3-stage framework for cost-effective control of COVID-19 (Fig. 1). Interventions are shown from top (most cost-effective) to bottom (least cost-effective), according to the three stages described by Madhav et al. [3] as pre-pandemic, spark, and spread (shown from left to right). A complete description is found in the Supplement.

Cost-effectiveness of interventions in COVID-19, by stage
Strengths and limitations
This review arguably has one key strength: turning to past pandemics, it included a broad range of study designs to provide a comprehensive summary of the evidence. This could also be viewed as a limitation, as the evidence for many measures is of lower quality. Lower-quality evidence should be interpreted with caution. Still, as randomized trial evidence was not available for most pandemics, and as COVID-19 forces urgent decision-making, we submit that some evidence, even if of lower quality, is better than no evidence at all. Moreover, studying these interventions during a pandemic poses substantial methodological challenges, and it may not be possible, physically or ethically, to conduct them under a trial design. In addition, this review has a number of limitations. First, as we deemed it relevant to promptly release our results, our search was limited to two databases (MEDLINE and EMBASE). Second, we did not assess the risk of bias. Third, we studied past pandemics, not COVID-19. Past pandemics have limited generalizability to COVID-19. Fourth, the COVID-19 pandemic is a rapidly evolving situation, and estimates of COVID-19 case fatality rates are subject to substantial uncertainties—especially due to variants. Should the true rate be high, all interventions would be more cost-effective. Conversely, should it be low, costly interventions such as workplace and school closures may not be cost-effective at all. Similarly, estimates of cost-effectiveness based solely on case fatality rates ignore the potential for long-term morbidity, i.e. “long COVID” [91]. To the extent that this phenomenon proves to be widespread, debilitating, and long-lasting, all interventions may become more cost-effective in hindsight. Fifth, interventions studied during past pandemics of a smaller scale may not be readily feasible during the COVID-19 pandemic, given its scale and the relative lack of preparedness of some jurisdictions—as illustrated by shortages of face masks early on in the pandemic and limited contact tracing capabilities.
Among the noteworthy, non-sanitary side-effects of the ongoing COVID-19 pandemic, the need for a broader perspective on the socio-economic costs unveiled by the disease stands out as a call for action to multiple stakeholders, particularly policymakers. Yet most of those costs remain currently hidden, as they relate to unknown morbidities subsequent to the infection, and on an aggregate note, are contingent on the resilience of the social and economic fabric of the given country or region. Hence, in order to provide a more factual assessment of cost-effectiveness, we relied on the disability-adjusted life year (DALY) as a measure of health burden, a metric extensively used in academia and policymaking.
Conclusions
Hand-washing and face masks were the only measures supported by higher-quality evidence. Other interventions were supported by lower-quality evidence. In the context of COVID-19, a cautious interpretation suggests that (1) workplace and school closures are effective but costly, especially when adopted late, and (2) scaling up as early as possible a combination of interventions that includes hand-washing, face masks, ample protective equipment for healthcare workers, and swift contact tracing and case isolation is likely to be the most cost-effective strategy.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- COVID:
-
Coronavirus disease
- EMBASE:
-
Excerpta Medica dataBASE
- H1N1:
-
Hemagglutinin type 1 and neuraminidase type 1 (influenza strain)
- H2N2:
-
Hemagglutinin type 2 and neuraminidase type 2 (influenza strain)
- ICU:
-
Intensive care unit
- MEDLINE:
-
Medical Literature Analysis and Retrieval System Online
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- SARS:
-
Severe acute respiratory syndrome
- SARS-CoV-2:
-
Severe acute respiratory syndrome coronavirus 2
- US:
-
United States of America
- WHO:
-
World Health Organization
References
Sandford A. Coronavirus: half of humanity now on lockdown as 90 countries call for confinement: Euronews; 2020. https://www.euronews.com/2020/04/02/coronavirus-in-europe-spain-s-death-toll-hits-10-000-after-record-950-new-deaths-in-24-hou. Accessed 14 June 2020
World Health Organization. Coronavirus disease 2019 (COVID-19) situation report – 77. 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200406-sitrep-77-covid-19.pdf. Accessed 14 June 2020.
Madhav N, Oppenheim B, Gallivan M, Mulembakani P, Rubin E, Wolfe N. In: Jamison DT, Gelband H, Horton S, et al., editors. Pandemics: risks, impacts, and mitigation in disease control priorities: improving health and reducing poverty. 3rd ed. Washington, DC: The International Bank for Reconstruction and Development / The World Bank; 2017.
Lempel H, Epstein JM, Hammond RA. Economic cost and health care workforce effects of school closure in the U.S. PLoS Curr. 2009;1:RRN1051.
Smith SM, Sonego S, Wallen GR, Waterer G, Cheng AC, Thompson P. Use of non-pharmaceutical interventions to reduce the transmission of influenza in adults: a systematic review. Respirology. 2015;20(6):896–903. https://doi.org/10.1111/resp.12541.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. https://doi.org/10.1136/bmj.b2535.
Jefferson T, Del Mar CB, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. 2011;(7):CD006207. https://doi.org/10.1002/14651858.CD006207.pub4.
MacIntyre CR, Chughtai AA. Facemasks for the prevention of infection in healthcare and community settings. BMJ. 2015;350:h694. https://doi.org/10.1136/bmj.h694.
Saunders-Hastings P, Crispo JAG, Sikora L, Krewski D. Effectiveness of personal protective measures in reducing pandemic influenza transmission: a systematic review and meta-analysis. Epidemics. 2017a;20:1–20. https://doi.org/10.1016/j.epidem.2017.04.003.
Saunders-Hastings P, Quinn Hayes B, Smith R, Krewski D. Modelling community-control strategies to protect hospital resources during an influenza pandemic in Ottawa, Canada. PLoS One. 2017b;12(6):e0179315. https://doi.org/10.1371/journal.pone.0179315.
Bin Nafisah S, Alamery AH, Al Nafesa A, Aleid B, Brazanji NA. School closure during novel influenza: a systematic review. J Infect Public Health. 2018;11(5):657–61. https://doi.org/10.1016/j.jiph.2018.01.003.
Jackson C, Mangtani P, Hawker J, Olowokure B, Vynnycky E. The effects of school closure on influenza outbreaks and pandemics: systematic review of simulation studies. PLoS One. 2014;9(5):e97297. https://doi.org/10.1371/journal.pone.0097297.
Rashid H, Ridda I, King C, Begun M, Tekin H, Wood JG, et al. Evidence compendium and advice on social distancing and other related measures for response to an influenza pandemic. Paediatr Respir Rev. 2015;16(2):119–26. https://doi.org/10.1016/j.prrv.2014.01.003.
Viner RM, Russell SJ, Croker H, Packer J, Ward J, Stansfield C, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. 2020. https://doi.org/10.1016/S2352-4642(20)30095-X.
Pasquini-Descomps H, Brender N, Maradan D. Value for money in H1N1 influenza: a systematic review of the cost-effectiveness of pandemic interventions. Value Health. 2017;20(6):819–27. https://doi.org/10.1016/j.jval.2016.05.005.
Wang B, Xie J, Fang P. Is a mass prevention and control program for pandemic (H1N1) 2009 good value for money? Evidence from the Chinese experience. Iran J Public Health. 2012;41(11):34–43.
Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI, Russell TW, et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health. 2020:pe488–96. https://doi.org/10.1016/S2214-109X(20)30074-7.
Armbruster B, Brandeau ML. Optimal mix of screening and contact tracing for endemic diseases. Math Biosci. 2007;209(2):386–402.
Halton K, Sarna M, Barnett A, Leonardo L, Graves N. A systematic review of community-based interventions for emerging zoonotic infectious diseases in Southeast Asia. JBI Database System Rev Implement Rep. 2013;11(2):1–235. https://doi.org/10.11124/jbisrir-2013-801 Epub 2013 Mar 12. PMCID: PMC4962925.
Bell D, Nicoll A, et al. Non-pharmaceutical interventions for pandemic influenza, national and community measures. Emerg Infect Dis. 2006;12(1):88–94. https://doi.org/10.3201/eid1201.051371.
Zhang Q, Wang D. Assessing the role of voluntary self-isolation in the control of pandemic influenza using a household epidemic model. Int J Environ Res Public Health. 2015;12(8):9750–67. https://doi.org/10.3390/ijerph120809750.
Young LS, Ruschel S, Yanchuk S, Pereira T. Consequences of delays and imperfect implementation of isolation in epidemic control. Sci Rep. 2019;9(1):3505. https://doi.org/10.1038/s41598-019-39714-0.
Li X, Geng W, Tian H, Lai D. Was mandatory quarantine necessary in China for controlling the 2009 H1N1 pandemic? Int J Environ Res Public Health. 2013;10:4690–700. https://doi.org/10.3390/ijerph10104690.
Tuncer N, Mohanakumar C, Swanson S, Martcheva M. Efficacy of control measures in the control of Ebola, Liberia 2014-2015. J Biol Dyn. 2018;12(1):913–37. https://doi.org/10.1080/17513758.2018.1535095.
Becker NG, Glass K, Li Z, Aldis GK. Controlling emerging infectious diseases like SARS. Math Biosci. 2005;193(2):205–21. https://doi.org/10.1016/j.mbs.2004.07.006.
MacIntyre CR, Costantino V, Kunasekaran MP. Health system capacity in Sydney, Australia in the event of a biological attack with smallpox. PLoS One. 2019;14(6):e0217704. https://doi.org/10.1371/journal.pone.0217704.
Sang Z, Qiu Z, Yan X, Zou Y. Assessing the effect of non-pharmaceutical interventions on containing an emerging disease. Math Biosci Eng. 2012;9(1):147–64. https://doi.org/10.3934/mbe.2012.9.147.
Chen T, Zhao B, Liu R, Zhang X, Xie Z, Chen S. Simulation of key interventions for seasonal influenza outbreak control at school in Changsha, China. J Int Med Res. 2020;48(1):300060518764268. https://doi.org/10.1177/0300060518764268.
Tracht SM, Del Valle SY, Edwards BK. Economic analysis of the use of facemasks during pandemic (H1N1) 2009. J Theor Biol. 2012;300:161–72. https://doi.org/10.1016/j.jtbi.2012.01.032.
Townsend J, Greenland K, Curtis V. Costs of diarrhea and acute respiratory infection attributable to not handwashing: the cases of India and China. Trop Med Int Health. 2017;22(1):74–81. https://doi.org/10.1111/tmi.12808.
Dan YY, Tambyah PA, Sim J, Lim J, Hsu LY, Chow WL, et al. Cost-effectiveness analysis of hospital infection control response to an epidemic respiratory virus threat. Emerg Infect Dis. 2009;15(12):1909–16. https://doi.org/10.3201/eid1512.090902.
Lee BY, Wettstein ZS, McGlone SM, Bailey RR, Umscheid CA, Smith KJ, et al. Economic value of norovirus outbreak control measures in healthcare settings. Clin Microbiol Infect. 2011;17(4):640–6. https://doi.org/10.1111/j.1469-0691.2010.03345.x.
Barnes B, Glass K, Becker NG. The role of health care workers and antiviral drugs in the control of pandemic influenza. Math Biosci. 2007;209(2):403–16. https://doi.org/10.1016/j.mbs.2007.02.008.
Suphanchaimat R, Doung-Ngern P, Ploddi K, Suthachana S, Phaiyarom M, Pachanee K, et al. Cost effectiveness and budget impact analyses of influenza vaccination for prisoners in Thailand: an application of system dynamic modelling. Int J Environ Res Public Health. 2020;17(4). https://doi.org/10.3390/ijerph17041247.
Shiell A, Jorm LR, Carruthers R, Fitzsimmons GJ. Cost-effectiveness of measles outbreak intervention strategies. Aust N Z J Public Health. 1998;22(1):126–32. https://doi.org/10.1111/j.1467-842x.1998.tb01156.x.
Prosser LA, Lavelle TA, Fiore AE, Bridges CB, Reed C, Jain S, et al. Cost-effectiveness of 2009 pandemic influenza A(H1N1) vaccination in the United States. PLoS One. 2011;6(7):e22308. https://doi.org/10.1371/journal.pone.0022308.
Nguyen VK, Mikolajczyk R, Hernandez-Vargas EA. High-resolution epidemic simulation using within-host infection and contact data. BMC Public Health. 2018;18(1):886. https://doi.org/10.1186/s12889-018-5709-x.
Lee BY, Brown ST, Korch GW, Cooley PC, Zimmerman RK, Wheaton WD, et al. A computer simulation of vaccine prioritization, allocation, and rationing during the 2009 H1N1 influenza pandemic. Vaccine. 2010;28(31):4875–9. https://doi.org/10.1016/j.vaccine.2010.05.002.
Van Genugten ML, Heijnen ML, Jager JC. Pandemic influenza and healthcare demand in the Netherlands: scenario analysis. Emerg Infect Dis. 2003;9(5):531–8. https://doi.org/10.3201/eid0905.020321.
Herrera-Diestra JL, Meyers LA. Local risk perception enhances epidemic control. PLoS One. 2019;14(12):e0225576. https://doi.org/10.1371/journal.pone.0225576.
Buonomo B, Messina E. Impact of vaccine arrival on the optimal control of a newly emerging infectious disease: a theoretical study. Math Biosci Eng. 2012;9(3):539–52. https://doi.org/10.3934/mbe.2012.9.539.
Handel A, Longini IM Jr, Antia R. What is the best control strategy for multiple infectious disease outbreaks? Proc Biol Sci. 2007;274(1611):833–7. https://doi.org/10.1098/rspb.2006.0015.
Lin F, Muthuraman K, Lawley M. An optimal control theory approach to non-pharmaceutical interventions. BMC Infect Dis. 2010;10:32. https://doi.org/10.1186/1471-2334-10-32.
Pérez Velasco R, Praditsitthikorn N, Wichmann K, Mohara A, Kotirum S, Tantivess S, et al. Systematic review of economic evaluations of preparedness strategies and interventions against influenza pandemics. PLoS One. 2012;7(2):e30333. https://doi.org/10.1371/journal.pone.0030333.
Day T, Park A, Madras N, Gumel A, Wu J. When is quarantine a useful control strategy for emerging infectious diseases? Am J Epidemiol. 2006;163(5):479–85.
Perlroth DJ, Glass RJ, Davey VJ, Cannon D, Garber AM, Owens DK. Health outcomes and costs of community mitigation strategies for an influenza pandemic in the United States. Clin Infect Dis. 2010;50(2):165–74. https://doi.org/10.1086/649867.
Bolton KJ, McCaw JM, Moss R, et al. Likely effectiveness of pharmaceutical and non-pharmaceutical interventions for mitigating influenza virus transmission in Mongolia. Bull World Health Organ. 2012;90(4):264–71. https://doi.org/10.2471/BLT.11.093419.
Halder N, Kelso JK, Milne GJ. Cost-effective strategies for mitigating a future influenza pandemic with H1N1 2009 characteristics. PLoS One. 2011;6(7):e22087. https://doi.org/10.1371/journal.pone.0022087.
Lee VJ, Lye DC, Wilder-Smith A. Combination strategies for pandemic influenza response - a systematic review of mathematical modeling studies. BMC Med. 2009;7:76. https://doi.org/10.1186/1741-7015-7-76.
Martinez DL, Das TK. Design of non-pharmaceutical intervention strategies for pandemic influenza outbreaks. BMC Public Health. 2014;14:1328. https://doi.org/10.1186/1471-2458-14-1328.
Ahmed F, Zviedrite N, Uzicanin A. Effectiveness of workplace social distancing measures in reducing influenza transmission: a systematic review. BMC Public Health. 2018;18(1). https://doi.org/10.1186/s12889-018-5446-1.
Pan A, Liu L, Wang C, Guo H, Hao X, Wang Q, et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA. 2020. https://doi.org/10.1001/jama.2020.6130.
Markel H, Lipman HB, Navarro JA, Sloan A, Michalsen JR, Stern AM, et al. Nonpharmaceutical interventions implemented by US cities during the 1918-1919 influenza pandemic. JAMA. 2007;298(6):644–54.
Bootsma MC, Ferguson NM. The effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Natl Acad Sci U S A. 2007;104(18):7588–93. https://doi.org/10.1073/pnas.0611071104.
Ishola DA, Phin N. Could influenza transmission be reduced by restricting mass gatherings? Towards an evidence-based policy framework. J Epidemiol Glob Health. 2011;1(1):33–60. https://doi.org/10.1016/j.jegh.2011.06.004.
Rainey JJ, Phelps T, Shi J. Mass gatherings and respiratory disease outbreaks in the United States - should we be worried? Results from a systematic literature review and analysis of the national outbreak reporting system. PLoS One. 2016;11(8):e0160378. https://doi.org/10.1371/journal.pone.0160378.
Figueroa A, Gulati RK, Rainey JJ. Estimating the frequency and characteristics of respiratory disease outbreaks at mass gatherings in the United States: findings from a state and local health department assessment. PLoS One. 2017;12(10):e0186730. https://doi.org/10.1371/journal.pone.0186730.
Shi P, Keskinocak P, Swann JL, Lee BY. The impact of mass gatherings and holiday traveling on the course of an influenza pandemic: a computational model. BMC Public Health. 2010;10:778. https://doi.org/10.1186/1471-2458-10-778.
Zhao S, Zhuang Z, Cao P, Ran J, Gao D, Lou Y, et al. Quantifying the association between domestic travel and the exportation of novel coronavirus (2019-nCoV) cases from Wuhan, China in 2020: a correlational analysis. J Travel Med. 2020;27(2). https://doi.org/10.1093/jtm/taaa022.
Ryu S, Gao H, Wong JY, Shiu EYC, Xiao J, Fong MW, et al. Non-pharmaceutical measures for pandemic influenza in non-healthcare settings—international travel–related measures. Emerg Infect Dis. 2020. https://doi.org/10.3201/eid2605.190993.
Mateu AL, Otete HE, Beck CR, Dolan GP, Nguyen-Van-Tam JS. Effectiveness of travel restrictions in the rapid containment of human influenza: a systematic review. Bull World Health Organ. 2014;92(12):868–880D. https://doi.org/10.2471/BLT.14.135590.
Chong KC, Ying Zee BC. Modeling the impact of air, sea, and land travel restrictions supplemented by other interventions on the emergence of a new influenza pandemic virus. BMC Infect Dis. 2012;12:309. https://doi.org/10.1186/1471-2334-12-309.
Chinazzi M, Davis JT, Ajelli M, Gioannini C, Litvinova M, Merler S, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020. https://doi.org/10.1126/science.aba9757.
Bell D, Nicoll A, et al. Non-pharmaceutical interventions for pandemic influenza, international measures. Emerg Infect Dis. 2006b;12(1):81–7. https://doi.org/10.3201/eid1201.051370.
Zhang Y, Yang P, Liyanage S, Seale H, Deng Y, Pang X, et al. The characteristics of imported cases and the effectiveness of outbreak control strategies of pandemic influenza A (H1N1) in China. Asia Pac J Public Health. 2012;24(6):932–9. https://doi.org/10.1177/1010539511408285.
Bwire G, Mwesawina M, Baluku Y, Kanyanda SS, Orach CG. Cross-border cholera outbreaks in sub-Saharan Africa, the mystery behind the silent illness: what needs to be done? PLoS One. 2016;11(6):e0156674. https://doi.org/10.1371/journal.pone.0156674.
Caley P, Becker NG, Philp DJ. The waiting time for inter-country spread of pandemic influenza. PLoS One. 2007;2(1):e143. https://doi.org/10.1371/journal.pone.0000143.
Schiavo R, May Leung M, Brown M. Communicating risk and promoting disease mitigation measures in epidemics and emerging disease settings. Pathog Glob Health. 2014;108(2):76–94. https://doi.org/10.1179/2047773214Y.0000000127.
Gostic K, Gomez AC, Mummah RO, Kucharski AJ, Lloyd-Smith JO. Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19. Elife. 2020;9:e55570. https://doi.org/10.7554/eLife.55570.
Jani BD, Ho FK, Lowe DJ, Traynor JP, MacBride-Stewart SP, Mark PB, et al. Comparison of COVID-19 outcomes among shielded and non-shielded populations. Sci Rep. 2021;11(1):15278. https://doi.org/10.1038/s41598-021-94630-6 PMID: 34315958; PMCID: PMC8316565.
Pormohammad A, Ghorbani S, Khatami A, Razizadeh MH, Alborzi E, Zarei M, et al. Comparison of influenza type A and B with COVID-19: a global systematic review and meta-analysis on clinical, laboratory and radiographic findings. Rev Med Virol. 2021;31(3):e2179. https://doi.org/10.1002/rmv.2179.
Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Hossmann S, Imeri H, Ipekci AM, et al. Occurrence and transmission potential of asymptomatic and pre-symptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis. PLoS Med. 2020;17(9):e1003346. https://doi.org/10.1371/journal.pmed.1003346.
Juneau CE, Briand AS, Pueyo T, Collazzo P, Potvin L. Effective contact tracing for COVID-19: a systematic review. MedRxiv. https://doi.org/10.1101/2020.07.23.20160234.
Iacobucci G. Covid-19: Government is criticised for “scandalous” £10bn spent on test and trace programme. BMJ. m2805. https://doi.org/10.1136/bmj.m2805.
Thunström L, Newbold S, Finnoff D, Ashworth M, Shogren J. The benefits and costs of using social distancing to flatten the curve for COVID-19. J Benefit-Cost Anal. 2020;11(2):179–95. https://doi.org/10.1017/bca.2020.12.
Joffe AR. COVID-19: rethinking the lockdown groupthink. Front Public Health. 2021;9:625778. https://doi.org/10.3389/fpubh.2021.625778.
Bendavid E, Oh C, Bhattacharya J, Ioannidis JPA. Assessing mandatory stay-at-home and business closure effects on the spread of COVID-19. Eur J Clin Invest. 2021;51(4):e13484. https://doi.org/10.1111/eci.13484.
Haug N, Geyrhofer L, Londei A, Dervic E, Desvars-Larrive A, Loreto V, et al. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat Hum Behav. 2020;4(12):1303–12. https://doi.org/10.1038/s41562-020-01009-0.
Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020. https://doi.org/10.1001/jama.2020.4683.
Tregoning JS, Flight KE, Higham SL, Wang Z, Pierce BF. Progress of the COVID-19 vaccine effort: viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat Rev Immunol. 2021:1–11. https://doi.org/10.1038/s41577-021-00592-1.
World Health Organization. Tracking SARS-CoV-2 variants. https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/. Accessed 28 Aug 2021.
Madhi SA, Baillie V, Cutland CL, Voysey M, Koen AL, Fairlie L, et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. 2021;384(20):1885–98. https://doi.org/10.1056/NEJMoa2102214.
Fowlkes A, Gaglani M, Groover K, Thiese MS, Tyner H, Ellingson K, et al. Effectiveness of COVID-19 vaccines in preventing SARS-CoV-2 infection among frontline workers before and during B.1.617.2 (Delta) variant predominance - eight U.S. locations, December 2020-August 2021. MMWR Morb Mortal Wkly Rep. 2021;70(34):1167–9. https://doi.org/10.15585/mmwr.mm7034e4.
Sabino EC, Buss LF, Carvalho MPS, Prete CA Jr, Crispim MAE, Fraiji NA, et al. Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Lancet. 2021;397(10273):452–5. https://doi.org/10.1016/S0140-6736(21)00183-5.
Wadman M. A grim warning from Israel: vaccination blunts, but does not defeat Delta. Science News; 2021. https://www.science.org/content/article/grim-warning-israel-vaccination-blunts-does-not-defeat-delta.
Mahase E. Covid-19 booster vaccines: what we know and who’s doing what. BMJ. 2021;374:n2082. https://doi.org/10.1136/bmj.n2082.
Banks J, Smith JP. International comparisons in health economics: evidence from aging studies. Annu Rev Econ. 2012;4:57–81. https://doi.org/10.1146/annurev-economics-080511-110944.
Napier AD, Depledge M, Knipper M, Lovell R, Ponarin ES, Thomas F. Using a cultural context of health approach to enhance policy-making. WHO, Regional Office for Europe; 2017. ISBN 978 92 890 5233 7. https://www.euro.who.int/en/health-topics/health-determinants/behavioural-and-cultural-insights-for-health/publications/2017/culture-matters-using-a-cultural-contexts-of-health-approach-to-enhance-policy-making-2017.
Erman A, Medeiros M. Exploring the effect of collective cultural attributes on Covid-19-related public health outcomes. Front Psychol. 2021;12:2021. https://doi.org/10.3389/fpsyg.2021.627669.
Ruiz M, Devonport T, Chen-Wilson J, Nicholls W, Cagas J, Fernandez-Montalvo J, et al. A cross-cultural exploratory study of health behaviors and wellbeing during COVID-19. Front Psychol. 2021;11:2021. https://doi.org/10.3389/fpsyg.2020.608216.
Adeloye D, Elneima O, Daines L, Poinasamy K, Quint JK, Walker S, et al. The long-term sequelae of COVID-19: an international consensus on research priorities for patients with pre-existing and new-onset airways disease. Lancet Respir Med. 2021:S2213-2600(21)00286-1. https://doi.org/10.1016/S2213-2600(21)00286-1.
Acknowledgements
Not applicable.
Funding
LP holds the Canada Research Chair in Community Approaches and Health Inequalities (CRC 950-232541). This funding source had no role in the design, conduct, or reporting of the study.
Author information
Authors and Affiliations
Contributions
CEJ, TP, and LP designed the study. CEJ, GG, MB, and PC searched and analysed the literature. CEJ, TP, and PC interpreted the findings. CEJ wrote the first draft. All authors revised drafts and approved the initial submission as well as the revised manuscript.
Authors’ information
CEJ is Doctor of Public Health (Epidemiology), serves the Canadian government (CIUSSS), and is the founder of Dr. Muscle and the COVID-19 Science Updates. TP, MB, and GG are senior members of the COVID-19 Work Group in the US, a multidisciplinary team with high-impact media publications on COVID-19. PC is Professor and Senior Researcher at Danube University in Austria, working on Health Economics and Value-Based Health Care. LP holds the Canada Research Chair in Community Approaches and Health Inequalities and is a leading researcher in the field of public health and health promotion, with extensive editorial experience, serving as Editor-in-Chief of the Canadian Journal of Public Health.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
TP, MB, PC, and LP declare that they have no competing interests. GG holds a contractual position with the Millar Group (a provider of personal protective equipment) and executive roles at Panacea Health Solutions and Angular Momentum (providers of diabetes and corporate wellness programmes). CEJ has contractual agreements with the Centre Intégré Universitaire de Santé et de Services Sociaux du Centre-Sud-de-l'Ile-de-Montreal (CIUSSS) and is founder of Dr. Muscle and the COVID-19 Science Updates (https://covid1.substack.com/).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Result of the search. Description of 3-stage framework.
Additional file 2.
PRISMA Flow Diagram.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Juneau, CE., Pueyo, T., Bell, M. et al. Lessons from past pandemics: a systematic review of evidence-based, cost-effective interventions to suppress COVID-19. Syst Rev 11, 90 (2022). https://doi.org/10.1186/s13643-022-01958-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-01958-9