
Abstract
Background
Fat Free Mass (FFM) is an important and essential indicator in various sports populations, since greater muscle and bone mass generates greater strength, endurance and speed in athletes.
Objective
The purpose of the study was to validate Body Surface Area (BSA) as an anthropometric indicator to estimate FFM in young basketball players.
Methods
A descriptive cross-sectional study was carried out in 105 male basketball players of the Brazilian Basketball Confederation of Sao Paulo (Campinas), Brazil. The age range was 11 to 15 years. Weight and height were evaluated. BSA, body mass index (BMI) and maturity status (MS) were calculated. Total body scanning was performed by dual X-ray absorptiometry (DXA). The components were extracted: Fat mass (FM), Fat free mass (FFM), percentage of fat mass (%FM) and bone mass (BM). The data were analyzed using the correlation coefficient of concordance (CCC) in terms of precision and accuracy.
Results
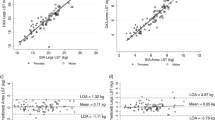
Three regression equations were generated: equation 1 had age and body weight as predictors [FFM= -30.059+(2.926*age)+(0.625*Weight)] (R2 = 92%, precision = 0.96 and accuracy = 0.99), equation 2 used age and BSA [FFM=-45.719+(1.934*age)+(39.388*BSA)] (R2 = 94%, precision = 0.97 and accuracy = 0.99) and equation 3 was based on APHV and BSA [FFM=-15.284+(1.765*APHV)+(37.610*(BSA)] (R2 = 94%, precision = 0.96 and accuracy = 0.99).
Conclusions
The results suggest the use of anthropometric equation using decimal age and BSA to estimate FFM in young basketball players. This new method developed can be used to design, evaluate and control training programs and monitor the weight status of athletes.
Similar content being viewed by others
Background
Fat-free mass (FFM) refers to the amount of non-fat body tissue, which includes muscle, bone, water and organs. It is used as an indicator of nutritional and health status in various populations [1]. It is characterized as an important indicator of body composition and health in populations of different ages and physical activity levels [2]. It is generally used to assess changes in body composition during weight loss and physical training, and has been related to various health outcomes, such as mortality, cardiovascular disease and diabetes [3]. Its assessment is often performed from direct (cadaveric analysis), indirect (chemical and physical) and doubly indirect (anthropometry and bio-impedance) methods [4, 5].
In fact, regardless of the method used, its use and application are considered essential in sports populations. Because greater muscle and bone mass generates greater strength, endurance and speed in athletes [6] and, consequently, greater physical performance. In the specific case of basketball, some studies [7,8,9], have shown that components of body composition are directly related to multiple variables of motor performance, pointing out the positive contribution of fat-free mass. The existence of a relationship has been established, where success in sports performance depends on the player’s jumping ability simultaneously with shooting or rebounding [10]. The vertical jumping performance of a player has a direct impact on his level of play, as the former is an integral part of different game movements such as rebounding, shooting at the basket, shooting at the basket, dunking and rebounding [11].
From that perspective, several studies in recent years have highlighted that anthropometric measures such as bone breadths (such as femur or humerus), body girths (arm, leg girths or thigh girths), and skinfolds (triceps and subscapular), are classic indicators that serve to estimate FFM in non-sporting populations of children, youth and adults, respectively [12,13,14].
However, to our knowledge, there is a wide variety of studies that have reported equations estimating FFM in young athletes in various sport modalities and mainly in soccer [15,16,17,18].
To date, no equations based on anthropometric measures that predict FFM in young basketball players have been identified. Thus, there is currently an urgent need to refine anthropometric methods that provide information beyond diameters, circumferences and skinfolds.
In this context, it is necessary to develop FFM prediction equations that are less time-consuming and fast in their measurements and calculations. In recent years, some studies have suggested that Body Surface Area (BSA) could be an appropriate indicator to estimate FFM in children and adolescent athletes [19] and non-athletes [20], since there is a positive relationship between both variables.
In fact, BSA has been classically defined as a measure of the extent of an individual’s skin surface área [21] and represents human dimensionality and predicts metabolic activity in clinical applications and metabolic heat production in physiology [22]. It is calculated from the height and weight of an individual, using classical mathematical formulas, such as the Dubois formula [23] or others. These equations have previously been allometrically adjusted where the geometric calculations applied normalize weight and height according to body size. The Dubois formula was used since previous studies highlight its use in athletes especially in soccer players, basketball players and volleyball players [24, 25].
Consequently, this study presupposes that BSA could be an excellent predictor of FFM in young asketball players. Since, the proposal of new predictive equations based on non-invasive methods could be a very useful alternative for clubs and professionals working in the detection and selection of sports talent. Therefore, the objective of the study was to validate the BSA as an anthropometric indicator to estimate the FFM of young Brazilian basketball players.
Materials and methods
Subjects
A descriptive cross-sectional study was carried out on 105 male basketball players of the Brazilian Basketball Confederation of Sao Paulo (Campinas), Brazil. The sample selection was non-probalistic (accidental), the youngsters belonged to 10 representative clubs, whose age range was from 11 to 15 years old.
The young people participated in the study on a voluntary basis and had 3 years of experience in the sport. Those who were within the established age range and those who were duly registered with the Brazilian basketball confederation were included in the study. Young people with any type of sports injury that prevented anthropometric evaluations and dual X-ray absorptiometry (DXA) scanning were excluded from the study. Also, children categorized as pre-pubertal (according to maturity status) were excluded of study. All parents and/or guardians of the youngsters signed the informed consent. The youth also signed the informed consent form. The study was approved by the Research Ethics Committee of the State University of Campinas UNICAMP (CAAE: 79718417.0.0000.5404). All evaluation procedures were performed in accordance with the Helsinki declaration for human subjects.
Techniques and procedures
Anthropometric measurements and DXA scanning were performed at the hospital of the faculty of medical sciences of the university. All measurements were performed in the morning period from Monday to Friday.
For the evaluation process, a team of 4 evaluators with extensive experience in anthropometric evaluations and with ISAK certification (02 evaluators) and DXA scanning (02 evaluators) was formed.
The concordance between the evaluators of anthropometric variables and DXA scanning was verified through the Kappa Coefficient. The kappa coefficient values obtained reflected an almost perfect concordance strength [26]. It was 0.93 for the anthropometrist and 0.94 for the DXA evaluators, confirming a high degree of agreement between them.
The anthropometric measurements of weight and height were evaluated without shoes and with as little clothing as possible, following the recommendations of Ross, Marfell-Jones [27]. Body weight (kg) was measured using an electronic scale (Tanita, United Kingdom) with a scale from 0 to 150 kg and with 100 g accuracy. Standing height with a portable stadiometer (Seca Gmbh & Co. KG, Hamburg, Germany) accurate to 0.1 mm, according to the Frankfurt plan.
The FFM analysis was performed using the standard method by iDXA. The equipment used was: (GE Healthcare Lunar, Madison, WI, USA) and enCore™2011 software version 13.6 (GE Healthcare Lunar). Total body measurements, including the head, were performed.
Prior to the scan, the athletes were prohibited from wearing jewelry and the presence of some types of metal on the body, which should be removed before the scan. To start the scan, the athletes were instructed to remain in the supine position with arms extended at the sides of the body and with the knees and ankles fastened with a Velcro strap (to ensure the predetermined position). One of the evaluators aligned the reference points according to the lines shown by the software. Body composition indicators [Fat free mass (FFM), Fat mass (FM), percentage of fat mass (%FM) and Bone mass (BM)] were extracted.
The maturity status of the young athletes was monitored using the anthropometric technique proposed by Moore et al. [28]. This technique uses chronological age and standing height to estimate age at maximum height velocity (APHV). The equation used was for males: APHV (years) = -7.999994 + (0.0036124 × (age × height)). This equation was used in males, whose categorization ranges in this sample were: -3APHV, -2APHV, -1APHV, 0APHV, +1APHV and + 2APHV.
The BSA (m2) was estimated by means of the DuBois equation, DuBois [23]. This equation uses weight and height and their corresponding allometric adjustments: BSA: = 0.007184*W0.425 * H0.725, where W = weight, H = standing height. Body Mass Index (BMI) was determined by the formula: BMI = weight (kg)/height2 (m).
Statistics
The normal distribution of the data was verified by the Kolmogorov-Smirnov test. The study variables were analyzed using descriptive statistics of arithmetic mean (X), standard deviation (SD) and coefficient of variation (CV). Relationships between variables were obtained using Pearson’s correlation coefficient. Three simple and multiple stepwise regression models were developed to generate FFM prediction equations. The equations were analyzed using the following criteria: R2 (coefficient of determination), standard error of estimate (SEE), Collinearity (T-tolerance and variance inflation factor FIV for each independent variable). Models with an FIV < 10 or a tolerance greater than 0.1 were considered [29, 30]. The desirable reproducibility index (DRI) according to Lin’s [31] approach was also used. This approach evaluates the degree of agreement from the concordance correlation coefficient (CCC) in terms of precision (P) and accuracy (A). Using Lin’s approach [31], the concordance correlation coefficient (CCC) was calculated and interpreted as suggested by McBride [32] (near perfect > 0.99; substantial > 0.95–0.99; moderate = 0.90–0.95; and poor < 0.90). The models created were compared by means of the t-test for related samples. The significance level for all statistical tests was < 0.05. SPSS version 16.0 (IBM Corp., Armonk, NY, USA) and MedCalc 11.1.0 were used for statistical analysis.
Results
Table 1 shows anthropometric and body composition variables aligned by decimal age and MS. The mean decimal age is 14.6 ± 1.7 years and the APHV (MS) was 14.12 ± 0.99 APHV. In both groups, it is observed that with increasing age and MS the anthropometric and body composition variables increase.
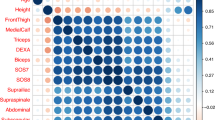
The simple linear regression values are shown in Table 2. All five variables (age, APHV, weight and BSA) evidenced positive relationships with FFM (DXA). These ranged from 0.74 to 0.96 (p < 0.001). The highest explanatory power was observed with BSA (R2 = 92%), followed by body weight (R2 = 87%). In addition, it was observed that APHV showed a better predictive percentage in relation to decimal age (R2 = 76%).
Table 3 shows the equations proposed to estimate the FFM. In general, 3 regression equations were developed. The first uses age and body weight, the second uses age and BSA and the third uses APHV and BSA. Tolerance values of 0.34 to 0.66 and FVI values of 1.52 to 2.98 were evident in all 3 equations. No collinearity was observed in the 3 equations. However, the explanatory power of equations 2 and 3 (R2 = 94%) were superior in relation to equation 1 (R2 = 92%), respectively.
Table 4 shows the comparisons between the reference DXA with the three equations and the DRI values of the proposed equations. There were no significant differences between equations 1, 2 and 3 with the reference method (p > 0.001). However, equations 2 evidences a lower CV (4.98%) in relation to the other equations. In general, the three equations present similar CCC (0.96), precision (0.96) and accuracy (0.99), respectively.
Discussion
The aim of the study was to validate the BSA as an anthropometric indicator to estimate the FFM of young basketball players. Age, body weight, MS or BSA were used as predictor variables. In fact, the results have shown that the best predictor of FFM was BSA. From these results, three regression equations estimating FFM in young basketball players were generated.
The three equations developed showed high explanatory power. For example, equation 1 using age and weight explained 92%. However, equation 2 (using age and BSA) and equation 3 (using APHV and BSA) as predictors, explained 94%. In addition, in the three cases we did not observe collinearity, since tolerance and FIV presented values within the established limits [33].
When comparing the reference DXA method with each of the equations, no significant differences were found. However, equation 2, that uses age and BSA, is the one that presents a lower SEE and CV than equations 1 and 3, respectively. Therefore, to ratify this pattern observed in the equations, we used the Desirable Reproducibility Index (DRI) proposed by Lin [31], where the CCC, precision and accuracy were similar in the three equations. In fact, these findings are relatively similar with other studies that sought similar targets in schoolchildren [34] and young athletes [18, 35, 36]. However, the results obtained here presented a higher R2 and high values of precision and accuracy.
Consequently, these results obtained in this study confirm that age and BSA are excellent predictors of FFM, so they should be included in the process of body composition assessment of young basketball players. Although the use of equation 3 using the MS (APHV) and BSA are not ruled out since the explanatory power is relatively similar to equations 1 and 2, respectively. In fact, BSA has been widely accepted as the most appropriate biometric unit to normalize physiological indices related to body metabolism in individuals of different body sizes [37]. Well, a recent study has evidenced a high positive relationship between MS determined by anthropometry with BSA in children and adolescents and its possible use as a predictor of MS [38]. Because BSA is an indicator of metabolic mass that is less affected by abnormal adipose tissue [39] due to the scaling of both weight and height.
Another recent study has verified the usefulness of the BSA to predict FFM in young 3 × 3 basketball players (determined by bio-impedance), since they have verified a better association in relation to body mass index and tri-ponderal index [40], so its use and application in young basketball players is determinant.
The estimation of FFM through BSA in young basketball players in this study can help in the evaluation, monitoring and in the design of training programs, so FFM basically intervenes in the production of force, especially during jumps, sprint and changes of rhythm [41].
Overall, FFM can provide useful information for sports scientists and coaches to improve the body composition of athletes [42]. As well as guide coaching staff decisions and assist with short-, medium-, and long-term nutritional goals.
It is widely known that basketball is characterized by evidencing high physical and physiological demands [43]. Therefore, it is necessary to ensure a favorable body composition profile (e.g., less fat mass and higher FFM), which would greatly benefit athletes in their physical performance [44].
Fat-free mass is the most important factor in the body composition of athletes, as it is involved in force production. This intervenes in many aspects of basketball, for example, in sprinting, defense and jumping [45]. This provides the basis for sport-specific technical skills and locomotor activities [46].
Therefore, players with higher FFM can jump higher than their counterparts who have higher fat mass [47, 48]. Which contributes to largely to optimize physical performance, motor ability of basketball players, prevent injuries and improve the health of athletes, especially during the stage of physical growth and biological development.
In general, this study presents some strengths that should be highlighted, for example, it is one of the first studies that considers BSA as a predictor of FFM in young basketball players. For BSA is characterized as a better indicator of metabolic mass than body weight [49]. This is often used to determine basal metabolic rate and recommended caloric intake for individuals at different stages of life and with different levels of physical activity [50]. Furthermore, the validation of equation 2 is assured, since we used a standardized protocol (standard other) such as DXA.
It must also be recognized that the study has some weaknesses. These are related to the cross-sectional design used since it does not allow cause and effect relationships. In addition, it was not possible to evaluate physical tests related to muscle strength, and it is also necessary to explore other BSA formulas. It is suggested that future studies consider these variables to obtain promising results in young basketball players.
Conclusion
In sum, this study concludes that body BSA is a better predictor of FFM in relation to body weight and MS in young basketball players. The results suggest the use of the anthropometric equation using decimal age and BSA to estimate FFM in young basketball players. This new validated method can be used to design, evaluate, and control training programs, and monitor the weight status of athletes. Its calculations can be performed at the following link: http://reidebihu.net/ffmbasketbrasil.php.
Data availability
The study data may be requested from the corresponding author, who will make the database available.
Abbreviations
- APHV:
-
Age at peak height velocity
- BM:
-
Bone mass
- BMI:
-
Body mass index
- BSA:
-
Body Surface Area (BSA)
- DXA:
-
Dual X-ray absorptiometry
- FFM:
-
Fat Free Mass
- FM:
-
Fat mass
- MS:
-
Maturity status
References
Katzmarzyk PT, Heymsfield SB, Bouchard C. Clinical utility of visceral adipose tissue for the identification of cardiometabolic risk in white and African American adults. Am J Clin Nutr. 2013;97(3):480–6. https://doi.org/10.3945/ajcn.112.047787
Pietrobelli A, Heymsfield SB. Establishing body composition in obesity. J Endocrinol Investig. 2002;25(10):884–92. https://doi.org/10.1007/BF03344052
Lee SY, Gallagher D. Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care. 2008;11(5):566–72. https://doi.org/10.1097/MCO.0b013e32830b5f23
Fosbøl MØ, Zerahn B. Contemporary methods of body composition measurement. Clin Physiol Funct Imaging. 2015;35(2):81–97. https://doi.org/10.1111/cpf.12152
Kuriyan R. Body composition techniques. Indian J Med Res. 2018;148(5):648–58. https://doi.org/10.4103/ijmr.IJMR_1777_18
Stokes T, Hector AJ, Onambélé GL. Size and strength are the key outcome measures in Sarcopenia research. J Cachexia Sarcopenia Muscle. 2015;6(3):267–76. https://doi.org/10.1002/jcsm.12040
Gaetano A, Tiziana DI, Di Tore PA. Anthropometrics characteristics and jumping ability in basketball. J Hum Sport Exerc. 2018;13:385–92. https://doi.org/10.14198/jhse.2018.13.Proc2.22
Nunes JA, Aoki MS, Altimari LR, Petroski EL, Júnior DDR, Montagner PC. Anthropometric profile and indicators of playing performance in Brazilian women s Olympic basketball teams. Revista Brasileira De Cineantropometria E Desempenho Humano. 2009;11(1):67–72. https://doi.org/10.5007/1980-0037.2009v11n1p67
Ribeiro BG, Mota HR, Sampaio-Jorge F, Morales AP, Leite TC. Correlation between body composition and the performance of vertical jumps in basketball players. J Exerc Physiol Online. 2015;18(5):69–79. https://www.asep.org/asep/asep/JEPonlineOCTOBER2015_Morales.pdf. [Google Scholar].
Kalinski M, Norkowski H, Kerner M, Tkaczuk W. Anaerobic power characteristics of elite athletes in national level team-sport games. Eur J Sport Sci. 2002;2(3):1–21. https://doi.org/10.1080/17461390200072303
Čović N, Čaušević D, Alexe CI, Rani B, Dulceanu CR, Abazović E, Lupu GS, Alexe DI. Relations between specific athleticism and morphology in young basketball players. Front Sports Act Living. 2023;5:1276953. https://doi.org/10.3389/fspor.2023.1276953
Deurenberg P, Weststrate JA, Seidell JC. Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. Br J Nutr. 1991;65(2):105–14. https://doi.org/10.1079/bjn19910073
Heyward VH, Stolarczyk LM. Applied body composition assessment. Human Kinetics; 1996. https://doi.org/10.1249/MSS.0000000000000588
Esparza-Ros F, Vaquero-Cristóbal R, Marfell-Jones M. International standards for anthropometric assessment. International Society for the Advancement of Kinanthropometry (ISAK); 2019.
Stewart AD, Hannan WJ. Prediction of fat and fat-free mass in male athletes using dual X-ray absorptiometry as the reference method. J Sports Sci. 2000;18(4):263–74. https://doi.org/10.1080/026404100365009
Koury JC, Ribeiro MA, Massarani FA, Vieira F, Marini E. Fat-free mass in adolescent athletes: accuracy of bioimpedance equations and identification of new predictive equations. Nutr (Burbank Los Angeles Cty Calif). 2019;60:59–65. https://doi.org/10.1016/j.nut.2018.09.029
Núñez FJ, Munguía-Izquierdo D, Suárez-Arrones L. Validity of field methods to estimate fat-free mass changes throughout the season in elite youth soccer players. Front Physiol. 2020;11:16. https://doi.org/10.3389/fphys.2020.00016
Gomez-Campos R, Santi-Maria T, Arruda M, Maldonado T, Albernaz A, Schiavo M, Cossio-Bolaños M. Fat-free mass and bone mineral density of young soccer players: proposal of equations based on anthropometric variables. Front Psychol. 2019;10:522. https://doi.org/10.3389/fpsyg.2019.00522
Sheikhsaraf B, Allah NH, Ali AM. Association of body surface area and body composition with heart structural characteristics of female swimmers. Int J Exerc Sci. 2010;3(3):97–101.
Teixeira PJ, Sardinha LB, Going SB, Lohman TG. Total and regional fat and serum cardiovascular disease risk factors in lean and obese children and adolescents. Obes Res. 2001;9(8):432–42. https://doi.org/10.1038/oby.2001.57
Boyd E. The growth of the surface area of the human body. Minneapolis: University of Minnesota; 1935.
Looney DP, Potter AW, Arcidiacono DM, Santee WR, Friedl KE. Body surface area equations for physically active men and women. Am J Hum Biology: Official J Hum Biology Council. 2023;35(2):e23823. https://doi.org/10.1002/ajhb.23823
Du Bois D, Du Bois EF. Clinical calorimetry: tenth paper a formula to estimate the approximate surface area if height and weight be known. Arch Intern Med. 1916;17(6–2):863–71.
Riding NR, Salah O, Sharma S, Carré F, O’Hanlon R, George KP, Hamilton B, Chalabi H, Whyte GP, Wilson MG. Do big athletes have big hearts? Impact of extreme anthropometry upon cardiac hypertrophy in professional male athletes. Br J Sports Med. 2012;46(Suppl 1Suppl1):i90–7. https://doi.org/10.1136/bjsports-2012-091258
Gaurav V, Singh E, Singh S. Anthropometric characteristics, somatotyping and body composition of volleyball and basketball players. J Phys Educ Sport. 2010;1:28–32.
Landis J, Koch G. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74.
Ross WD, Marfell-Jones MJ. Kinanthropometry. In: J. D. MacDougall, H. A. Wenger, & H. J. Geeny, editors, Physiological testing of elite athlete. London: Human Kinetics. 1991;223:308–314.
Moore SA, McKay HA, Macdonald H, Nettlefold L, Baxter-Jones AD, Cameron N, Brasher PM. Enhancing a somatic maturity prediction model. Med Sci Sports Exerc. 2015;47(8):1755–64. https://doi.org/10.1249/MSS.0000000000000588
Guo S, Chumlea WC. Statistical methods for the development and testing of predictive equations. Hum Body Composit. 1996;10:191–202.
Ndagire CT, Muyonga JH, Odur B, Nakimbugwe D. Prediction equations for body composition of children and adolescents aged 8–19 years in Uganda using deuterium dilution as the reference technique. Clin Nutr ESPEN. 2018;28:103–9. https://doi.org/10.1016/j.clnesp.2018.09.004
Lin LI. A concordance correlation coefficient to evaluate reproducibility. Biometrics. 1989;45:255–68.
Bride GB. Statistical calculators; Lin’s Concordance. 2007.
Slinker BK, Glantz SA. Multiple regression for physiological data analysis: the problem of multicollinearity. Am J Physiol. 1985;249(1 Pt 2):R1–12.
Cossio Bolaños MA, Andruske CL, de Arruda M, Sulla-Torres J, Urra-Albornoz C, Rivera-Portugal M, Luarte-Roche L, Pacheco-Carrillo J, Gomez-Campos R. Muscle mass in children and adolescents: proposed equations and reference values for assessment. Front Endocrinol. 2019;10:583. https://doi.org/10.3389/fendo.2019.00583
Giro R, Matias CN, Campa F, Santos DA, Cavaca ML, Duque P, Oliveira M, Matos N, Vicente F, Pereira P, Santos H, Subvention T, Teixeira F. Development and validation of an anthropometric equation to predict fat mass percentage in professional and semi-professional male futsal players. Nutrients. 2022;14(21):4514. https://doi.org/10.3390/nu14214514
Bonilla DA, Duque-Zuluaga LT, Muñoz-Urrego LP, Franco-Hoyos K, Agudelo-Martínez A, Kammerer-López M, Petro JL, Kreider RB. Development and validation of a novel waist Girth-based equation to estimate fat mass in young Colombian elite athletes (F20CA equation): a STROSA-based study. Nutrients. 2022;14(19):4059. https://doi.org/10.3390/nu14194059
Nwoye LO, Al-Shehri MA. A formula for the estimation of the body surface area of Saudi male adults. Saudi Med J. 2003;24(12):1341–6. PMID: 14710281.
Alvear-Vasquez F, Vidal-Espinoza R, Gomez-Campos R, et al. Body surface area is a predictor of maturity status in school children and adolescents. BMC Pediatr. 2023;23:410. https://doi.org/10.1186/s12887-023-04222-8
Kothari R, Mittal G, Gopani M, Bokariya AP, Vemparala P, Tamrakar SS. Exploring the relationship between the indices of body composition with grip strength performance and peak VO2. Cureus. 2023;15(6):e40874. https://doi.org/10.7759/cureus.40874
García-Hilares D, Vidal Espinoza R, De la Torre Choque C, Equivel Segura H, Baquerizo Sedano L, Vidal-Fernandez N, Gomez-Campos R, Cossio Bolaños M. Indicadores antropométricos como predictores de la masa libre de grasa en basquetbolistas universitarios 3 x 3. Nutr Clín Diet Hosp. 2024;44(1):137–42. https://doi.org/10.12873/441garcia
Hector AJ, McGlory C, Damas F, Mazara N, Baker SK, Phillips SM. Pronounced energy restriction with elevated protein intake results in no change in proteolysis and reductions in skeletal muscle protein synthesis that are mitigated by resistance exercise. FASEB J. 2018;32(1):265–75. https://doi.org/10.1096/fj.201700158RR
Takai Y, Nakatani M, Aoki T, Komori D, Oyamada K, Murata K, et al. Body shape indices are predictors for estimating fat-free mass in male athletes. PLoS ONE. 2018;13(1):e0189836. https://doi.org/10.1371/journal.pone.0189836
Stojanović E, Stojiljković N, Scanlan AT, Dalbo VJ, Berkelmans DM, Milanović Z. The activity demands and physiological responses encountered during basketball match-play: a systematic review. Sports medicine (Auckland, N.Z.). 2018;48(1):111–135. https://doi.org/10.1007/s40279-017-0794-z
Sansone P, Makivic B, Csapo R, Hume P, Martínez-Rodríguez A, Bauer P. Body fat of basketball players: a systematic review and meta-analysis. Sports Med– open. 2022;8(1):26. https://doi.org/10.1186/s40798-022-00418-x
Hector AJ, Phillips SM. Protein recommendations for weight loss in elite athletes: a focus on body composition and performance. Int J Sport Nutr Exerc Metab. 2018;28(2):170–7. https://doi.org/10.1123/ijsnem.2017-0273
Turnagöl HH. Body composition and bone mineral density of collegiate American football players. J Hum Kinetics. 2016;51:103–12. https://doi.org/10.1515/hukin-2015-0164
Ribeiro BG, Mota HR, Jorge FS, Morales AP. Correlation between body composition and the performance of vertical jumps in basketball players. J Exerc Physiol Online. 2015;18:69–79.
Kuo S, Dommel A, Sayer RD. Body composition changes in college basketball players over summer training. Int J Sports Exerc Med. 2022;8:232. https://doi.org/10.23937/2469-5718/1510232
Parsons S. Pharmaceutical calculations. Parsons Printing Press; 2012. Available from: http://books.google.com/books?id=EzRTAgAAQBAJ
Heymsfield SB, Waki M, Kehayias J, Lichtman S, Dilmanian FA, Kamen Y, Wang J, Pierson RN. Chemical and elemental analysis of humans in vivo using improved body composition models. Am J Physiol. 1991;261(2 Pt 1):E190–8. https://doi.org/10.1152/ajpendo.1991.261.2.E190
Acknowledgements
We would like to express our gratitude to all the young basketball participants for their tremendous support.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
M.C.B., R.G.C., A.M.M., and L.F.C contributed to the design of the research study. A.M.M., R.R.B., and E.L., collected data, contributed to the discussion, wrote the manuscript and reviewed/edited the manuscript. M.C.B., R.G.C., R.V.E., A.M.M., L.F.C., E.L., J.S.T., and R.V.E, edited, and reviewed the manuscript. M.C.B., R.G.C., A.M.M., R.R.B., L.F.C., J.S.T., and R.V.E, analyzed data and/or reviewed/edited the manuscript. M.C.B., R.G.C., and L.F.C., reviewed/edited the manuscript. All authors revised and agreed on the views expressed in the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethic Committee of of the State University of Campinas UNICAMP (CAAE: 79718417.0.0000.5404). All experiments were performed in accordance with relevant guidelines and regulations (such as the Declaration of Helsinki). Parents and guardians provided informed written consent for their children under the age of 16 participating in the study. In addition, all students under and over the age of 16 in the study provided written informed consent acknowledging their consent to participate and their understanding of the research procedures and objectives. All experiments were conducted in accordance with relevant guidelines and regulations (such as the Declaration of Helsinki). Parents and guardians gave written informed consent for their minor children to participate in the study. In addition, all students who participated in the study gave written informed consent, acknowledging their consent to participate and their understanding of the research procedures and objectives.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
de Moraes, A.M., Vidal-Espinoza, R., Bergamo, R.R. et al. Prediction of fat-free mass from body surface area in young basketball players. BMC Sports Sci Med Rehabil 16, 65 (2024). https://doi.org/10.1186/s13102-024-00857-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-024-00857-x