
Abstract
Background
Despite decades of community-directed treatment with ivermectin (CDTI), onchocerciasis transmission persists in Cameroon and has been associated with increased risk for epilepsy in endemic communities. We investigated the onchocerciasis situation in the Ntui Health District (a known onchocerciasis focus in Cameroon where the Sanaga River constitutes the main source of black fly vectors) using parasitological, entomological and serological parameters.
Methods
In July 2021, community-based surveys were conducted in four villages (Essougli, Nachtigal, Ndjame and Ndowe). Onchocerciasis was diagnosed via microscopic examination of skin snips. Using rapid diagnostic tests, we screened children aged 3–6 years for Ov16 antibodies as a proxy for recent onchocerciasis transmission. Monthly black fly biting rates were obtained from the two riverside villages (Nachtigal and Essougli) for 12 consecutive months (July 2021 to June 2022) using the human landing catch technique. Some black flies were dissected each month to check for infection.
Results
Overall, 460 participants were recruited; mean age was 32.1 (range: 3–85) years with 248 (53.9%) being males. Among skin snipped participants (n = 425), onchocerciasis prevalence was 14.6%. Participants with epilepsy (n = 25) were more often skin snip positive (45.8% vs 12.7%; P < 0.001) and had higher microfilarial loads (9.2 ± 22.0 vs 0.7 ± 3.5 microfilariae/skin snip; P < 0.001) compared to their peers without epilepsy. Eight (6.5%) of the 123 tested children were Ov16 seropositive. The breeding sites we investigated along the Sanaga River during the current study harbored fewer vectors (annual biting rates reaching 530,322 vs 606,370 in the Mbam River) and exhibited lower black fly infection rates (annual transmission potentials reaching 1479 vs 4488 in the Mbam River) when compared to recent entomological reports in Cameroon.
Conclusion
Despite substantial biting rates, black fly infection rates (by microscopy) in the Ntui Health District were rather low resulting in overall low transmission potentials in study villages. Thanks to CDTI, O. volvulus infection in both humans and insects is on the decrease. However, there is evidence that O. volvulus is still endemic in these communities. Reducing the vector population will further accelerate onchocerciasis elimination prospects.
Graphical Abstract

Similar content being viewed by others


Background
Onchocerciasis is a neglected tropical disease which manifests clinically as skin lesions and eye disease leading to blindness (also known as river blindness) [1]. It is caused by the filarial nematode Onchocerca volvulus transmitted by black flies (Diptera: Simuliidae) [1]. The black fly vectors breed in fast-flowing fresh water bodies, where they lay their eggs and develop into adult insects. Onchocerciasis is the world's second leading cause of preventable blindness. It is estimated that 99% of the 20.9 million individuals currently infected with O. volvulus live in Africa [1]. In addition to the clinical symptoms, onchocerciasis is a stigmatizing condition, which engenders significant psychosocial stress in the affected individuals [2, 3].
Foci of onchocerciasis endemicity were documented in Cameroon as early as the 1970s [4]. Various black fly species have been identified as potent O. volvulus vectors in Cameroon, with most of them belonging to the Simulium damnosum complex (S. damnosum sensu stricto, S. sirbanum, S. yahense and S. squamosum) [5]. Black fly breeding sites had been identified during previous studies along the Sanaga and Mbam rivers of Cameroon [6], accounting for the high onchocerciasis transmission in the surrounding villages.
Onchocerciasis elimination strategies in Cameroon rely mainly on annual community-directed treatment with ivermectin (CDTI) introduced since the late 1990s/early 2000s [7]. However, despite > 15 years of CDTI, onchocerciasis transmission is still ongoing in several parts of the country [7,8,9]. Besides causing skin and eye disease, high onchocerciasis transmission has also been associated with a high prevalence of epilepsy [10]. Indeed, recent surveys found a prevalence of epilepsy in onchocerciasis-endemic villages of Cameroon ranging from 2.5% to 7.8% [8, 9]. The most compelling evidence for the onchocerciasis-epilepsy association is provided by two cohort studies conducted in the Mbam Valley of Cameroon, where being infected with onchocerciasis during childhood was strongly associated with increased risk (up to 28-fold) of developing epilepsy later in life [11, 12]. Epilepsy is also known to be a stigmatizing condition [13], and its association with onchocerciasis obviously compounds the stigma experienced by persons with both conditions [14]. Fortunately, the implementation of effective onchocerciasis control measures would significantly reduce the epilepsy prevalence and incidence in affected communities over time, particularly in the 5–15-year age group [9, 15, 16].
In a bid to investigate the onchocerciasis prevalence in some Cameroonian villages and the impact of strengthening onchocerciasis elimination efforts on the incidence of epilepsy, a prospective study was initiated in the Ntui Health District in Cameroon in 2021 [17]. In the present article, we report the baseline findings regarding the onchocerciasis situation prior to implementing novel onchocerciasis control measures in the study villages.
Methods
Study setting
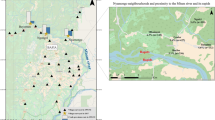
This research was conducted in rural communities of the Ntui Health District (Centre Region, Cameroon) from July 2021 to June 2022. The suburban town of Ntui is the headquarters for the Mbam et Kim division; it is located about 70 km north of the capital city Yaoundé and is surrounded by several villages. Agriculture is the main activity in the area with the production of both food and cash crops. The rural settlements located close to the Sanaga River constituted our study villages, and these included Essougli (04°23.850 N, 011°34.466 E), Nachtigal (04°22.672 N, 011°37.877 E), Ndjame (04°24.333 N, 011°38.258 E) and Ndowe (04°25.048, 011°42.835 E). Previous surveys conducted in 2009 and 2016 had confirmed that onchocerciasis was endemic in these villages, although the prevalence seemed to be decreasing with time [18, 19]. CDTI is usually conducted between June–July each year. However, due to COVID-19-related delays, the 2020 CDTI session was finally carried out in March 2021 in the Ntui Health District.
Study procedures
Prior to conducting fieldwork, the research team visited the study area to identify villages located within 10 km of the Sanaga River. We met with the local authorities (village chiefs, health officers), explained the study objectives to them and obtained their consent. We then organized meetings with the community health workers for the Ntui Health District to plan for the conduct of the research project in their respective villages. The community health workers were given a few weeks to carry out massive sensitization and mobilization in their respective communities to inform the populations about the study and its potential benefits in the fight against onchocerciasis.
Recruitment of participants and data collection
Following community engagement activities, the research team returned to the study villages and set up recruitment units in strategic locations (chief’s residence and/or primary schools). Village residents who were willing to participate came to the recruitment units where the research procedures were explained and their consent requested. Thereafter, a short questionnaire was administered to consenting participants to document their socio-demographic data (age, sex, profession, duration of stay in the village) and information about previous ivermectin use; all this information was obtained verbally from the respondents. A physical examination was conducted to assess the presence of dermatological lesions such as onchodermatitis [20]. The visual acuity of participants was measured using the tumbling E chart [21]. We also investigated a history of epilepsy among the participants using the recent operational definition of epilepsy provided by the International League Against Epilepsy (ILAE), that is, the occurrence of at least two unprovoked seizures > 24 h apart [22]. The diagnosis of epilepsy was made by the project physicians during fieldwork in the study villages.
Regarding sample collection from participants, we obtained a drop of blood by finger-pricking children aged 3–6 years to perform an Ov16 rapid diagnostic test (SD Bioline Onchocerciasis Ov16 IgG4, Standard Diagnostics, Gyeonggi-do, South Korea) for the presence of Ov16 antibodies as a proxy for onchocerciasis transmission in the community. For participants aged ≥ 5 years, two skin snips (one from each iliac crest region) were obtained using sterile 2-mm corneoscleral punches. The skin snips were placed in microtiter plates and incubated in isotonic saline for 24 h, after which they were examined under a microscope for the detection and quantification of O. volvulus microfilariae (mf) [23]. The average mf count for both skin snips from each participant was calculated. Microfilarial densities were expressed as mf/skin snip. The same experienced laboratory technician examined the skin snips from all study sites. All skin snip samples were obtained in July 2021, and Ov16 testing in children was conducted in July 2021 and March 2022. While the skin snip recruitment period in each of the villages of Essougli, Nachtigal and Ndjame lasted for at least 2 days, the research team was in Ndowe village only for 1 day because of logistical constraints; this explains why fewer participants were recruited from the latter site.
Entomological study
The Sanaga River banks (specifically the portions adjoining the two riverside villages of Nachtigal and Essougli) were prospected to identify black fly breeding sites. These two sites were chosen because of their proximity to the Sanaga River and recent confirmation of prevalent cases of onchocerciasis [18], suggesting that transmission is ongoing. The river banks were explored by an experienced entomologist, and the surfaces of various submerged substrates (leaves, grasses, sticks and rocks) were carefully examined for the presence of black fly larvae and pupae. The black fly larvae identified during this exercise were rinsed and placed in Carnoy’s fixative for future cytotaxonomic studies [5]. We obtained the GPS coordinates of the breeding sites (where black fly larvae/pupae were identified) using a Garmin GPSMAP78 device.
Once the breeding sites were identified, we proceeded to collect adult black flies and measured biting rates via the human landing catch (HLC) technique described by Walsh et al. [24]. Black fly catching sites were set up at the river banks in close proximity with the breeding sites. Adult black flies were collected between 07:00 and 18:00 for 3 consecutive days each month, beginning in July 2021. In the present article, we will present baseline biting rate data for the first 12 months from July 2021 through June 2022. Black fly catchers in each site consisted of two individuals working alternate hours, who were recruited from the nearest village and trained in standard HLC methods. Locally made tubes [5] were used to aspirate black flies into an empty container every hour, after which hourly biting rates were measured by counting the number of black flies in each container. After counting, some adult black flies were dissected in the field to determine parity rates and to detect Onchocerca spp. larvae; the remaining black flies were preserved in 95% ethanol for subsequent pool screening.
Sample size calculations
Sample size was calculated using Cochran’s formula, as follows: N = p(1-p)z2/d2 where N is the sample size, p is the prevalence of onchocerciasis in our study site (8.4% in villages of the Ntui Health District, based on a recent survey [18]), z is the decision variable at confidence of 95% (z = 1.96), and d is the sampling-related error risk (d = 0.05). The minimum sample size for the study was thus estimated at 119 participants.
Ethical and administrative considerations
Prior to the study, ethical clearance was obtained from the institutional review board of the Cameroon Baptist Convention Health Board (Ref. IRB2021-03) as well as an approval from the Centre Regional Delegation of the Ministry of Public Health of Cameroon (Ref. 1156/AP/MINSANTE/SG/DRSPC); a research permit from the Ministry of Scientific Research and Innovation (Ref. 000,144/MINRESI/B00/C00/C10/C13), an ABS-Nagoya Protocol Prior Informed Consent (Ref. Decision No. 00016/D/MINEPDED/CNA) and ABS Permit No. 00013/MINEPDED/CAN/NP-ABS/ABS-FP) from the Ministry of Environment, Protection of Nature and Sustainable Development. The consent of the village authorities was obtained for the research project. Additionally, all participants signed an individual informed consent form, and the data obtained were treated confidentially.
Data analysis
Data were analyzed in R version 4.0.2. Continuous variables were expressed as mean with standard deviation (SD) and compared across groups using the Mann-Whitney U test or the Kruskal-Wallis test as appropriate. Categorical data were expressed as percentages and compared using chi-squared tests. For multivariable analyses, we used skin snip positivity as dependent variable to investigate factors associated with O. volvulus infection in a multiple logistic regression model. In addition, we constructed a negative binomial Poisson regression model (because of the over-dispersion of the dependent variable) to investigate predictors of microfilarial density among infected participants; the superiority of this model over the ordinary Poisson regression model was confirmed by the Vuong test. For both models, covariates included participant age, sex and other variables which produced a P-value < 0.2 during univariate regression. The community microfilarial load (CMFL) for each village was calculated as the geometric mean of the individual mf load (to which the arbitrary value of 1 was added to have only non-zero values) in participants aged ≥ 20 years.
Regarding entomological data obtained from the two black fly catching points over a 12-month period, we used the biting rates for the 3 consecutive days of each month to calculate monthly biting rates as previously described [24]. Monthly transmission potentials were calculated using the method described by Walsh et al. [24], considering only data from the 1 day every month during which black flies were dissected in each village. As for annual transmission potentials, they were obtained by summing up the monthly transmission potentials for 12 consecutive months at each catching site. Similarly, annual biting rates were the sums of the monthly biting rates for each site. For all statistical analyses, two sided P-values < 0.05 were considered to be statistically significant.
Results
A total of 460 participants were recruited from our four study villages, with 248 (53.9%) being males. The mean age was 32.1 (range 3–85) years. Most participants were farmers (52.0%, mostly adults) while 33.3% were students (the younger participants). The average duration of stay of participants in the study villages was 22.6 (range: 0.5–83) years. Among participants who were skin snipped, the overall prevalence of onchocerciasis (proportion of persons with positive skin snips) was 62/425 (14.6%; 95% confidence interval: 11.4–18.4). Participants from Ndjame village were older than those from the other villages (Table 1). The CMFL was 1.35, 1.24, 1.09 and 1.07 for the participants residing in Essougli, Nachtigal, Ndjame and Ndowe, respectively. Of the 373 participants who reported to have ever taken ivermectin in all the study villages, 202 (54.2%) confirmed that they received their most recent dose during the March 2021 CDTI session.
We identified skin lesions in 48/460 (10.4%) participants. Among the latter, different skin lesions were represented as follows: papular lesions in 14 (29.2%), depigmentation in 13 (27.1%), lesions due to skin scratching in 10 (20.8%), “lizard skin” in 3 (6.3%) and desquamation in 2 (4.2%). The least common skin lesions with a single case each (frequency of 2.1%) included lymphoedema, subcutaneous nodule, vesicules, dermatomycosis, ulcerations and burn scars (in a participant who also had epilepsy). For study participants with available skin snip data (n = 425), we observed a trend: onchocerciasis prevalence increased with increasing age group; P = 0.187 (Table 2). Furthermore, when comparing O. volvulus infection among persons with epilepsy (PWE) (n = 24) and persons without epilepsy (n = 401), we found that those with epilepsy were more often skin snip positive (45.8% vs 12.7%; χ2 = 19.93, df = 1, P < 0.001) and had higher microfilarial loads (9.2 ± 22.0 vs 0.7 ± 3.5 mf/skin snip; Mann-Whitney U-test, W = 3115, P < 0.001) compared to their peers without epilepsy.
Factors associated with onchocercal infection
Among participants with skin snip data, the multiple logistic regression model revealed that having epilepsy and residing in Essougli (compared to Ndjame) were significantly associated with increased odds of being infected with O. volvulus (Table 3).
We investigated predictors of the microfilarial load in infected participants. The negative binomial Poisson regression model revealed that having epilepsy was associated with increased O. volvulus parasitic load, while there was a trend of decreasing microfilarial load with increasing level of education (Table 4).
Although the variable “number of previous ivermectin doses” was not eligible to be included in any of the multivariable models (P > 0.2 in univariate analyses), we found that the median values for the number of previous ivermectin doses received by participants varied significantly across levels of education: 0 among those without education, four among those with primary education, seven for secondary education and six for the few participants with university education (Kruskal-Wallis test, H = 20.73, df = 3, P < 0.001).
Entomological findings
Breeding sites were identified in both Essougli (coordinates: N 4°23.156, E 11°33.131) and Nachtigal (coordinates: N 4°21.146, E 11°37.953). The number of black flies caught during the 3-day HLC period each month varied from 1096 (December) to 11,247 (October) in Nachtigal and from 947 (January) to 13,906 (October) in Essougli. The median monthly biting rates were higher in Nachtigal (34,477) compared to Essougli (14,366); Mann-Whitney U test, W = 35, P = 0.033. Monthly biting rates, parity, O. volvulus infection among black flies and transmission potentials for each catching site are summarized in Table 5. There were strong positive correlations between the monthly biting rates and the monthly rainfall levels in both Nachtigal (Spearman’s correlation coefficient, rs = 0.657, P = 0.024) and Essougli (Spearman rho = 0.685, P = 0.017); see Fig. 1. The annual biting rates in our black fly catching sites along the Sanaga River were 530,322 for Nachtigal and 365,404 for Essougli.

Evolution of monthly biting rates at the two catching sites. Rainfall levels are those from the neighboring Bafia Health District, obtained from Hendy et al. [5]
Overall, 7586 black flies were dissected during the 12 months with 5 (0.07%) found to be infected with the L3 larval form of O. volvulus in their heads. These L3-infected black flies were distributed as follows: 2/4052 (0.05%) in Nachtigal and 3/3534 (0.08%) in Essougli. The annual transmission potentials in our study sites were 1479 for Nachtigal and 182 for Essougli.
Ov16 seroprevalence in children aged 3–6 years
Of the 123 children between the ages of 3 and 6 years who were tested for Ov16 antibodies, the rapid diagnostic test results were positive in 8, giving a seroprevalence of 6.5% (95% CI 3.1–12.8). There was no significant difference in Ov16 seroprevalence across villages (Fisher exact test with more than two categories, P = 0.467) or across ages (Fisher exact test with more than two categories, P = 0.540).
Discussion
Our study provides up-to-date data on the epidemiology of onchocerciasis in the Ntui Health District. A prevalence of O. volvulus infection of 14.6% was found, which is slightly higher than the 10.7% obtained in 2016 [18], which itself was a drop from a 26.4% prevalence in 2009 [19]. This sinusoidal evolution of onchocerciasis prevalence in the study area could be due to inconstant CDTI therapeutic coverage over the years. For instance, only 54% of our study participants with a history of ivermectin use had taken the drug in 2021, representing sub-optimal therapeutic coverage of ivermectin distribution. Interestingly, villages bordering the Sanaga River (Essougli and Nachtigal) had higher onchocerciasis prevalence and CMFL compared to other villages, although this was not statistically significant. This trend concurs with previous findings in Cameroon and Ethiopia [4, 25, 26], demonstrating increasing onchocerciasis burden with decreasing distance from the river.
Similar to previous reports [27], we found that the prevalence of onchocerciasis increased with age in our population although this was not statistically significant. However, none of our participants aged ≤ 5 years was infected, in contrast to the study of Nana-Djeunga et al. who found 6/169 (3.6%) of children < 5 years with positive skin snips in Mbangassina village still within the Ntui Health District [28]. This can be explained by the fact that the Mbangassina area is crisscrossed by both the Sanaga River and its tributary, the Mbam River, which probably increases the black fly population thereby increasing onchocerciasis transmission. Comparing with the Mbangassina data, we note that our study villages are not the most endemic hotspots in the district.
Contrary to what was reported by previous studies [25, 29], we did not find an inverse relationship between epilepsy prevalence and the distance of the village from the river (see Table 1). This could be due to our enrollment approach, which required that participants move to the recruitment site, which may be less efficient in detecting persons with epilepsy (PWE) compared to the gold-standard door-to-door strategy. In addition, it is likely that several PWE in the study villages were not enrolled into the study because of stigma and/or poor health conditions, which hindered them from reporting at the recruitment sites. That notwithstanding, the few PWE who did participate were more O. volvulus-infected than participants without epilepsy, supporting the existence of an association between onchocerciasis and epilepsy [10]. This hypothesis is further strengthened by the multivariable models, which showed that having O. volvulus infection and especially higher microfilarial loads was significantly associated with epilepsy, in line with previous findings from studies in Cameroon and abroad [11, 12, 25, 30].
Another notable finding from the multivariable models was the association between the educational level and microfilarial load among infected participants, in that a higher education level led to reduced infection intensity. Additionally, persons who were more educated were likely to have taken ivermectin more times in the past. Taken together, these two observations underscore the importance of educating the community to improve onchocerciasis practices, including adherence to CDTI [31, 32]. It is likely that more educated individuals adopt healthier habits regarding exposure to infected black flies. In the past, other authors have also reported an association between educational status and onchocerciasis infection [26]. Indeed, mathematical modeling studies reveal that education is a key intervention which contributes to controlling the dynamics of onchocerciasis transmission in endemic settings [33].
The annual biting rates along the Sanaga river observed in this study were a little lower compared to those in villages close to the Mbam River [5]. However, monthly observations revealed that during some months, there are more black flies along the Sanaga River than the Mbam River. In that regard, although the peak monthly biting rates for both the Sanaga and Mbam rivers were experienced during the month of October (month of maximum rainfall; see Fig. 1), the values for villages along the Sanaga river banks (in the present study: 143,695 and 116,219) were more than double those reported along the Mbam River banks (73,418 and 28,623) [5]. However, the lower biting rates in the Mbam river valley are compensated by higher black fly infection rates. A 12-month entomological study in two villages bordering the Mbam River banks showed that 17/7166 (0.2%) of the dissected black flies had infective O. volvulus L3 larvae in their heads [34], while the present study found only 5/7586 (0.07%) L3-infected black flies in the two villages on the Sanaga riverside. Therefore, the annual transmission potentials along the Mbam River (4488 and 2360) [5, 34] were higher than in the present study along the Sanaga river (1479 and 182), suggesting that more intense onchocerciasis transmission occurs in the Mbam river valley. Of note, previous entomological research already established that only the Sanaga River and its main tributary, the Mbam River, harbor black flies responsible for transmitting onchocerciasis, while their smaller tributaries are free of vectors [6]. Therefore, implementing vector control activities in these two rivers will further plummet the transmission potentials and accelerate onchocerciasis elimination prospects.
One possible explanation for the lower infection rates observed among black flies and humans during our study (compared to findings from the Mbam river) is the fact that CDTI was conducted in the study villages in March 2021, barely 4 months before the start of our survey. Following treatment with ivermectin, skin repopulation by O. volvulus mf has been shown to slowly resume within 3 to 6 months, but not reaching the initial infection intensity [35, 36]. Additionally, previous research in endemic communities in Cameroon has suggested that in villages with > 20 years of CDTI as is the case with our study sites, there is a lower mf clearance and higher repopulation rate after treatment with ivermectin [37]. One can reasonably argue that, despite the sub-optimal coverage, the ivermectin treatment had lowered the community microfilarial load in the study villages such that the probability of a black fly taking up mf during a blood meal would also be low. A prospective follow-up for O. volvulus detection in black flies and humans every month until the next CDTI session would provide more insight into these infection dynamics.
We observed that Ov16 seroprevalence among the 3–6 year olds in our study was low (6.5%) compared to 40% in a similar age group in South Sudan [38], 15–63% among children aged 6–10 years in villages of the Lekie division downstream of the Sanaga river in Cameroon (co-endemic with loiasis) [39] and 42.4–55.4% among older children aged 7–10 years in villages of the Mbam Valley in Cameroon [8, 9]. The low Ov16 seroprevalence in our study sites should be interpreted with caution as it could be influenced by the low age group we tested and our enrollment procedure at a fixed spot in the village which may have limited access for some children to participate, especially those living very close to the river. It could also be that the Ov16 antibody titers in the younger Cameroonians are relatively low, rendering the rapid diagnostic tests less sensitive in the 3–6 years age group. In summary, while O. volvulus transmission may be relatively lower in our study villages compared to other sites, our data show that the Ntui Health District is still endemic for onchocerciasis and would benefit from optimal measures to accelerate onchocerciasis elimination.
A major limitation of this work was the fact that recruitment was not done using a door-to-door approach, thereby introducing some selection bias for estimating the true prevalence of onchocerciasis and epilepsy in the study villages. However, the fact that participants from different villages took part in the study provides some perspective regarding the spread of onchocerciasis across the different communities in the Ntui Health District.
Conclusion
Our study has documented ongoing transmission of onchocerciasis in villages of the Ntui Health District alongside a sub-optimal ivermectin coverage among the village residents. Despite high biting rates, black fly infection rates (by microscopy) were rather low resulting in low transmission potentials. In addition to the reduced infection rates brought about by CDTI, interventions to reduce the high black fly biting rates could drastically limit O. volvulus transmission in these communities. Mindful of the disease burden caused by onchocerciasis and the numerous socioeconomic benefits that its elimination could bring in these communities [40], it is expedient that control strategies be strengthened to achieve the elimination goals sooner rather than later. It is to this end that the novel “Slash and Clear” vector control strategy will be deployed in the study area [17].
Availability of data and materials
The datasets for our study findings are available from the corresponding author on reasonable request.
References
Brattig NW, Cheke RA, Garms R. Onchocerciasis (river blindness)—more than a century of research and control. Acta Trop. 2021;218:105677.
Tabah EN, Yepnjio F, Njamnshi AK. Stigma in neurological diseases in the tropics. In: Bentivoglio M, Cavalheiro EA, Kristensson K, Patel NB, editors. Neglected tropical diseases and conditions of the nervous system. New York: Springer New York; 2014. p. 45–63.
Njamnshi AK, Bissek A-CZ-K, Etyale D. Onchocerciasis: neurological involvement. In: Bentivoglio M, Cavalheiro EA, Kristensson K, Patel NB, editors. Neglected tropical diseases and conditions of the nervous system. New York: Springer New York; 2014. p. 147–64.
Mendoza Aldana J, Piechulek H, Maguire J. Forest onchocerciasis in Cameroon: its distribution and implications for selection of communities for control programmes. Ann Trop Med Parasitol. 1997;91:79–86.
Hendy A, Krit M, Pfarr K, Laemmer C, De Witte J, Nwane P, et al. Onchocerca volvulus transmission in the Mbam valley of Cameroon following 16 years of annual community-directed treatment with ivermectin, and the description of a new cytotype of Simulium squamosum. Parasites Vectors. 2021;14:563.
Barbazan P, Escaffre H, Mbentengam R, Boussinesq M. Entomologic study on the transmission of onchocerciasis in a forest-savanna transition area of Cameroon. Bull Soc Pathol Exot. 1998;91:178–82.
Kamga GR, Dissak-Delon F, Nana-Djeunga HC, Biholong BD, Mbigha-Ghogomu S, Souopgui J, et al. Still mesoendemic onchocerciasis in two Cameroonian community-directed treatment with ivermectin projects despite more than 15 years of mass treatment. Parasit Vectors. 2016;9:581.
Boullé C, Njamnshi AK, Dema F, Mengnjo MK, Siewe Fodjo JN, Bissek A-CZ-K, et al. Impact of 19 years of mass drug administration with ivermectin on epilepsy burden in a hyperendemic onchocerciasis area in Cameroon. Parasites Vectors. 2019;12:114.
Siewe Fodjo JN, Tatah G, Tabah EN, Ngarka L, Nfor LN, Chokote SE, et al. Epidemiology of onchocerciasis-associated epilepsy in the Mbam and Sanaga river valleys of Cameroon: impact of more than 13 years of ivermectin. Infect Dis Poverty. 2018;7:114.
Colebunders R, Njamnshi AK, Menon S, Newton CR, Hotterbeekx A, Preux P-M, et al. Onchocerca volvulus and epilepsy: a comprehensive review using the Bradford Hill criteria for causation. PLoS Negl Trop Dis. 2021;15:e0008965.
Chesnais CB, Nana-Djeunga HC, Njamnshi AK, Lenou-Nanga CG, Boullé C, Bissek A-CZ-K, et al. The temporal relationship between onchocerciasis and epilepsy: a population-based cohort study. The Lancet Infect Dis. 2018;18:1278–86.
Chesnais CB, Bizet C, Campillo JT, Njamnshi WY, Bopda J, Nwane P, et al. A second population-based cohort study in Cameroon confirms the temporal relationship between onchocerciasis and epilepsy. Open Forum Infect Dis. 2020. https://doi.org/10.1093/ofid/ofaa206.
Njamnshi AK, Angwafor SA, Tabah EN, Jallon P, Muna WFT. General public knowledge, attitudes, and practices with respect to epilepsy in the Batibo Health District Cameroon. Epilepsy Behavior. 2009;14:83–8.
O’Neill S, Irani J, Siewe Fodjo JN, Nono D, Abbo C, Sato Y, et al. Stigma and epilepsy in onchocerciasis-endemic regions in Africa: a review and recommendations from the onchocerciasis-associated epilepsy working group. Infect Dis Poverty. 2019;8:34.
Siewe Fodjo JN, Remme JHF, Preux P-M, Colebunders R. Meta-analysis of epilepsy prevalence in West Africa and its relationship with onchocerciasis endemicity and control. Int Health. 2020;12:192–202.
Gumisiriza N, Kaiser C, Asaba G, Onen H, Mubiru F, Kisembo D, et al. Changes in epilepsy burden after onchocerciasis elimination in a hyperendemic focus of western Uganda: a comparison of two population-based, cross-sectional studies. Lancet Infect Dis. 2020;20:1315–23.
Fodjo JNS, Vieri MK, Ngarka L, Njamnshi WY, Nfor LN, Mengnjo MK, et al. Slash and clear vector control for onchocerciasis elimination and epilepsy prevention: a protocol of a cluster randomised trial in Cameroonian villages. BMJ Open. 2021;11:e050341.
Tsapi EM, Togjom FG, Gamago G-A, Pone JW, Teukeng FFD. Prevalence of onchocerciasis after seven years of continuous community-directed treatment with ivermectin in the Ntui health district Centre region Cameroon. Pan Afr Med J. 2020;1:180.
Kuete T, Mbuagbaw J, Kollo B, Kitobo E, Same-Ekobo A. Distribution des filarioses dans une zone de transition savane-forêt du Cameroun, impact sur la prise en charge: cas de l’Aire de santé de Ntui, Département du Mbam et Kim. J Cameroon Acad Sci. 2009;8:11–6.
Murdoch ME, Hay RJ, Mackenzie CD, Williams JF, Ghalib HW, Cousens S, et al. A clinical classification and grading system of the cutaneous changes in onchocerciasis. Br J Dermatol. 1993;129:260–9.
Plainis S, Kontadakis G, Feloni E, Giannakopoulou T, Tsilimbaris MK, Pallikaris IG, et al. Comparison of visual acuity charts in young adults and patients with diabetic retinopathy. Optom Vis Sci. 2013;90:174–8.
Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55:475–82.
Prost A, Prod’hon J. Le diagnostic parasitologique de l’onchocercose: revue critique des méthodes en usage. Médecine Tropicale. 1978; 38.
Walsh JF, Davies JB, Le Berre R, Garms R. Standardization of criteria for assessing the effect of Simulium control in onchocerciasis control programmes. Trans R Soc Trop Med Hyg. 1978;72:675–6.
Boussinesq M, Pion SD, Ngangue D, Kamgno J. Relationship between onchocerciasis and epilepsy: a matched case-control study in the Mbam Valley, Republic of Cameroon. Trans R Soc Trop Med Hyg. 2002;96:537–41.
Kifle B, Woldemichael K, Nigatu M. Prevalence of Onchocerciasis and Associated Factors among Adults Aged ≥ 15 Years in Semen Bench District, Bench Maji Zone, Southwest Ethiopia: community based cross-sectional study. Adv Public Health. 2019;2019:1–9.
Shintouo CM, Shey RA, Mets T, Vanhamme L, Souopgui J, Ghogomu SM, et al. Onchocerciasis fingerprints in the geriatric population: does host immunity play a role? TropicalMed. 2021;6:153.
Nana-Djeunga HC, Djune-Yemeli L, Domche A, Donfo-Azafack C, Efon-Ekangouo A, Lenou-Nanga C, et al. High infection rates for onchocerciasis and soil-transmitted helminthiasis in children under five not receiving preventive chemotherapy: a bottleneck to elimination. Infect Dis Poverty. 2022;11:47.
Colebunders R, Carter JY, Olore PC, Puok K, Bhattacharyya S, Menon S, et al. High prevalence of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan: a community-based survey. Seizure. 2018;63:93–101.
Abd-Elfarag G, Carter JY, Raimon S, Sebit W, Suliman A, Fodjo JNS, et al. Persons with onchocerciasis-associated epilepsy and nodding seizures have a more severe form of epilepsy with more cognitive impairment and higher levels of Onchocerca volvulus infection. Epileptic Disord France. 2020;22:301–8.
Shu EN, Nwadike KI, Onwujekwe EO, Ugwu OC, Okonkwo PO. Influence of health education on community participation in rapid assessment of onchocerciasis prior to distribution of ivermectin. East Afr Med J. 1999;76:320–3.
Nyagang SM, Cumber SN, Cho JF, Keka EI, Nkfusai CN, Wepngong E, et al. Prevalence of onchocerciasis, attitudes and practices and the treatment coverage after 15 years of mass drug administration with ivermectin in the Tombel Health District Cameroon. Pan Afr Med J. 2020;35:107.
Hassan A, Shaban N. Onchocerciasis dynamics: modelling the effects of treatment, education and vector control. J Biol Dyn. 2020;14:245–68.
Adam Hendy. Blackfly ecology and Onchocerca volvulus transmission in three formerly hyperendemic foci in Uganda, Tanzania and Cameroon [Internet] [PhD Thesis]. [Belgium]: Institute of Tropical Medicine; 2018. https://repository.uantwerpen.be/docman/irua/7a3e67/13135.pdf
Osei-Atweneboana MY, Eng JK, Boakye DA, Gyapong JO, Prichard RK. Prevalence and intensity of Onchocerca volvulus infection and efficacy of ivermectin in endemic communities in Ghana: a two-phase epidemiological study. The Lancet. 2007;369:2021–9.
Basáñez M-G, Pion SD, Boakes E, Filipe JA, Churcher TS, Boussinesq M. Effect of single-dose ivermectin on Onchocerca volvulus: a systematic review and meta-analysis. Lancet Infect Dis. 2008;8:310–22.
Abong RA, Amambo GN, Chounna Ndongmo PW, Njouendou AJ, Ritter M, Beng AA, et al. Differential susceptibility of Onchocerca volvulus microfilaria to ivermectin in two areas of contrasting history of mass drug administration in Cameroon: relevance of microscopy and molecular techniques for the monitoring of skin microfilarial repopulation within six months of direct observed treatment. BMC Infect Dis. 2020;20:726.
Lakwo TL, Raimon S, Tionga M, Siewe Fodjo JN, Alinda P, Sebit WJ, et al. The Role of the Maridi Dam in causing an onchocerciasis-associated epilepsy epidemic in Maridi, South Sudan: an epidemiological, sociological, and entomological study. Pathogens. 2020;9:315.
Siewe Fodjo JN, Njamnshi WY, Ngarka L, Nfor LN, Ayuk C, Mundih NN, et al. Association Between Ov16 Seropositivity and neurocognitive performance among children in Rural Cameroon: a pilot study. J Pediatr Neuropsychol. 2021;7:192–202.
Ahmed A, Elbashir A, Mohamed AA, Alim AA, Mubarak A, Abdelrahman D, et al. Socioeconomic impacts of elimination of onchocerciasis in Abu-Hamed focus, northern Sudan: lessons after elimination. BMC Res Notes. 2020;13:256.
Acknowledgements
We are grateful to various scientific collaborators who worked on the project, the population in the study villages as well as all the local authorities and volunteers for their participation.
Funding
This project is part of the EDCTP2 programme supported by the European Union (grant no. TMA2020CDF-3152-SCONE) awarded to JNSF.
Author information
Authors and Affiliations
Contributions
JNSF and AKN conceived and designed the study. JNSF, LN, WYN, PEA and AKN were involved in the fieldwork and data collection. JNSF cleaned and analyzed the data; JNSF wrote the first draft. ACZ-KB validated the de rmatological lesions and contributed to the revisios of the manuscript drafts and all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for the study was obtained from the institutional review board of the Cameroon Baptist Convention Health Board (Ref. IRB2021-03) and a research permit for the project was granted by Cameroon’s Ministry of Scientific Research and Innovation (Ref. 000144/MINRESI/B00/C00/C10/C13). Informed consent was obtained from all study participants.
Consent for publication
Written informed consent was obtained from all persons described in this paper.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Siewe Fodjo, J.N., Ngarka, L., Njamnshi, W.Y. et al. Onchocerciasis in the Ntui Health District of Cameroon: epidemiological, entomological and parasitological findings in relation to elimination prospects. Parasites Vectors 15, 444 (2022). https://doi.org/10.1186/s13071-022-05585-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13071-022-05585-0