
Abstract
Background
Neisseria meningitidis is the leading responsible bacterium of Purpura Fulminans (PF) accounting for two thirds of PF. Skin biopsy is a simple and minimally invasive exam allowing to perform skin culture and polymerase chain reaction (PCR) to detect Neisseria meningitidis. We aimed to assess the sensitivity of skin biopsy in adult patients with meningococcal PF.
Methods
A 17-year multicenter retrospective cohort study including adult patients admitted to the ICU for a meningococcal PF in whom a skin biopsy with conventional and/or meningococcal PCR was performed.
Results
Among 306 patients admitted for PF, 195 had a meningococcal PF (64%) with a skin biopsy being performed in 68 (35%) of them. Skin biopsy was performed in median 1 day after the initiation of antibiotic therapy. Standard culture of skin biopsy was performed in 61/68 (90%) patients and grew Neisseria meningitidis in 28 (46%) of them. Neisseria meningitidis PCR on skin biopsy was performed in 51/68 (75%) patients and was positive in 50 (98%) of them. Among these 50 positive meningococcal PCR, five were performed 3 days or more after initiation of antibiotic therapy. Finally, skin biopsy was considered as contributive in 60/68 (88%) patients. Identification of the meningococcal serogroup was obtained with skin biopsy in 48/68 (71%) patients.
Conclusions
Skin biopsy with conventional culture and meningococcal PCR has a global sensitivity of 88% and should be systematically considered in case of suspected meningococcal PF even after the initiation of antimicrobial treatment.
Similar content being viewed by others


Background
Purpura fulminans (PF) is a rare infectious disease carrying a high mortality and morbidity with 41% of the patients dying in the ICU and 28% of the survivors requiring limb amputations with a median number of 3 limbs amputated [1,2,3]. Neisseria meningitidis is the leading responsible bacterium accounting for two thirds of PF [1]. Obtaining a microbiological documentation of PF is crucial for confirming the diagnosis, as well as for adjusting the antibiotic therapy. It is also of paramount importance for public health interventions and postexposure chemoprophylaxis with antibiotic therapy and vaccination of persons having close contacts with a patient with meningococcal PF.
Given the high susceptibility of Neisseria meningitidis to β-lactam antibiotics, together with the high proportion of patients empirically treated before ICU admission [1], blood cultures may be sterile in half of the patients with meningococcal PF [4]. Moreover, lumbar puncture has been shown to be of limited diagnostic value in this context [5], if not contra-indicated because of severe thrombocytopenia and coagulation disorders, which are almost constant in patients with PF [1, 4]. Given the tropism of Neisseria meningitidis for skin endothelium [3, 6], the microbiological examination of skin biopsy was previously suggested to be an interesting diagnostic tool in children with PF [7,8,9,10]. Skin biopsy is a simple and minimally invasive exam allowing to perform skin culture and polymerase chain reaction (PCR) to detect Neisseria meningitidis, even several days after the initiation of antibiotic therapy [7, 11]. Only a few studies have assessed the diagnostic yield of skin biopsy in patients with a suspected meningococcal infection [7,8,9,10]. Most of these studies were performed in children and only one assessed the rentability of meningococcal PCR on skin biopsy [7]. Our aim was to evaluate the sensitivity of skin biopsy in adult patients with meningococcal PF.
Methods
Study design
We conducted a 17-year (2000–2016) multicenter retrospective cohort study including adult patients admitted to 43 intensive care units (ICU) in France (see the participating centers in the acknowledgement section) for a meningococcal PF. This observational study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. Meningococcal PF was defined by the association of a sudden and extensive purpura together with an acute circulatory failure needing vasopressor support [2, 6] and one or more microbiological sample positive (conventional culture or PCR) for Neisseria meningitidis in the blood, the cerebrospinal fluid or in skin biopsy. Patients with a non-meningococcal PF, a noninfectious purpura and those with purpura in a context of infectious endocarditis were not included in the present study. Skin biopsy was performed at the discretion of the intensivist on a purpuric lesion by using a punch biopsy device after local anesthesia. The primary study endpoint was the rate of contributive skin biopsy. Skin biopsy was considered as contributive when culture grew Neisseria meningitidis and/or when PCR was positive for Neisseria meningitidis. All patients had blood cultures drawn upon ICU admission, and lumbar puncture was performed at the discretion of the intensivist.
Data collection
The investigator of each participating center was responsible for the identification of the patients, either from the hospital medical reports, using the function “research the files in which the word” purpura fulminans occurs of Microsoft Windows®, or through a search using the following International Classification of Diseases (Tenth Revision) codes: D65 (Disseminated intravascular coagulation), A39 (Meningococcal infection), and D65 (Disseminated intravascular coagulation). The hospital discharge reports of all identified patients were anonymized and then electronically or conventionally mailed to the main investigator (DC). Clinical charts were reviewed in order to check the inclusion criteria. Upon ICU admission and during ICU stay, data pertaining to demographics, comorbidities, clinical examinations, laboratory findings, microbiological investigations and therapeutic management were collected. Missing data were retrieved by queries to the investigators. Of note, two patients included in one of the participating centers have already been described in a previous cases series [11].
Ethics approval
This observational, non-interventional analysis of medical records was approved by the Institutional Review Board of the French Intensive Care Society in March 2016 (SRLF16-01).
Statistical analysis
Categorical variables were presented as number (percentage), and quantitative variables as mean ± standard deviation (SD) or median [interquartile range (IQR)], as appropriate. Characteristics of patients who had a skin biopsy performed or not was compared using Chi-square tests or Fisher’s exact tests, as appropriate, for categorical variables and Student t tests or Mann–Whitney tests, as appropriate, for quantitative variables. All significance tests were two-sided, and the statistical significance level was set to 5%. Missing values were not imputed. All analyses were performed with R software (version 2.4.3, The R project for Statistical Computing, Vienna, Austria).
Results
Study population
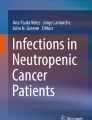
Among the 306 patients admitted for PF, 195 had a meningococcal PF (64%) with a skin biopsy being performed in 68 (35%) of them (Fig. 1).

Flowchart of patients with meningococcal purpura fulminans. A skin biopsy was performed in 35% of patients (n = 68/195). The sensitivity of standard bacterial culture and meningococcal polymerase chain reaction (PCR) is displayed. *a meningococcal PCR was not performed in all eight patients with a non-contributive skin biopsy
Comparison between patients with and without a skin biopsy is detailed in Table 1. Meningococcemia was more frequent in patients without a skin biopsy (72% vs. 47%, p = 0.001) and patients without a skin biopsy performed had more frequent lumbar puncture performed than those who underwent a skin biopsy (76% vs. 40%, p < 0.001). Culture of cerebrospinal fluid was more frequently positive in patients without a skin biopsy performed than in others (73% vs. 44%, p = 0.001) (Table 1).
Results of skin biopsy culture and PCR
Skin biopsy was performed in median 1 [0–1] day after ICU admission and 1 [0–1] day after the initiation of antibiotic therapy. Standard culture of skin biopsy was performed in 61/68 (90%) patients and grew Neisseria meningitidis in 28 (46%) of them (Fig. 1). Neisseria meningitidis PCR on skin biopsy was performed in 51/68 (75%) patients and was positive in 50 (98%) of them (Fig. 1). Among these 50 positive meningococcal PCR, five were performed 3 days or more after initiation of antibiotic therapy. Finally, skin biopsy was considered as contributive in 60/68 (88%) patients, knowing that meningococcal PCR was not performed in the 8 patients with a non-contributive skin biopsy (Table 1). Identification of the meningococcal serogroup was obtained with skin biopsy (by conventional culture or/and PCR) in 48/68 (71%) patients (serogroup B: n = 29; serogroup C: n = 15; serogroup w135: n = 2 and serogroup Y: n = 2). Skin biopsy was the only positive microbiological exam (i.e., both blood and cerebrospinal fluid cultures, when performed, were sterile) in 29/195 (15%) of the patients with meningococcal PF. No significant bleeding was reported in any of the patients who underwent skin biopsy.
Discussion
Our study indicates that only one third of the patients with meningococcal PF had a skin biopsy performed. Skin biopsy seems to be contributive in most of the patients with meningococcal PF, especially when a meningococcal PCR is performed (up to 3 days after antibiotic therapy initiation).
Our 46% high rate of positive conventional skin culture compares well with those reported in previous studies, which ranged from 56 to 64% [8,9,10] but, as opposed to our study, these studies combined Gram examination and cultures. This 46% figure is higher than the 14% rate reported by Staquet and colleagues who did not consider Gram examination. We reported on a 98% high rate of positive meningococcal PCR on skin biopsy, which is in-line with the 100% high rate previously reported by Staquet and colleagues in a smaller retrospective pediatric single-center study [7]. Overall, as previously reported [7], meningococcal PCR seems much more sensitive than conventional bacterial cultures and should be preferred in case of limited skin sample.
Given the higher rate of meningococcemia in patients without a skin biopsy obtained, one can speculate that skin biopsy was performed at day 1 because blood cultures remained sterile. Moreover, the higher rate of lumbar punctures performed in the group of patients without a skin biopsy may reflect an entrenched strategy of performing a lumbar puncture rather than a skin biopsy since coagulation disorder and Glasgow Coma Score did not differ between patients with and without a skin biopsy.
The main limitation of the study is inherent to its retrospective design. We acknowledge that a standardized protocol with a systematic realization of skin biopsy combining conventional culture and meningococcal PCR might have increased the proportion of patients with a contributive skin biopsy. The available data also did not allow us to comprehensively compute the diagnostic performances of skin biopsy. Indeed, having the total number of positive tests (standard culture and PCR) of PF patients, we could compute the sensitivity of skin biopsy, an informative parameter in this setting, but not the specificity, negative and positive predictive values, and likelihood ratios as we would have needed skin biopsy data in patients not having a meningococcal PF. Such data are currently not available, which is a limitation to our study.
Skin biopsy with conventional culture and meningococcal PCR has a global sensitivity of 88%. Given the high rentability of PCR as compared to conventional culture, meningococcal PCR on skin biopsy should be systematically considered in patients with suspected meningococcal PF in order to increase the diagnostic work-up, even several days after the initiation of antibiotic therapy.
Availability of data and materials
The dataset used and analyzed for the current study is available from the corresponding author on reasonable request.
Abbreviations
- PF:
-
Purpura fulminans
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- PCR:
-
Polymerase chain reaction
References
Contou D, Sonneville R, Canoui-Poitrine F, Colin G, Coudroy R, Pène F, et al. Clinical spectrum and short-term outcome of adult patients with purpura fulminans: a French multicenter retrospective cohort study. Intensive Care Med. 2018;44:1502–11.
Contou D, Canoui-Poitrine F, Coudroy R, Préau S, Cour M, Barbier F, et al. Long-term quality of life in adult patients surviving Purpura Fulminans: an exposed-unexposed multicenter cohort study. Clin Infect Dis. 2019;69:332–40.
Contou D, Urbina T, de Prost N. Understanding purpura fulminans in adult patients. Intensive Care Med. 2022;48:106–10.
Contou D, de Prost N, HOPEFUL Study group. Clinical phenotype and outcomes of pneumococcal versus meningococcal purpura fulminans: a multicenter retrospective cohort study. Crit Care. 2021;25:386.
Contou D, Sonneville R, Mekontso Dessap A, de Prost N, HOPEFUL Study group. Diagnostic yield of lumbar puncture in adult patients with purpura fulminans. Intensive Care Med. 2019;45:1487–9.
Lerolle N, Carlotti A, Melican K, Aubey F, Pierrot M, Diehl J-L, et al. Assessment of the interplay between blood and skin vascular abnormalities in adult purpura fulminans. Am J Respir Crit Care Med. 2013;188:684–92.
Staquet P, Lemee L, Verdier E, Bonmarchand G, Laudenbach V, Michel C, et al. Detection of Neisseria meningitidis DNA from skin lesion biopsy using real-time PCR: usefulness in the aetiological diagnosis of purpura fulminans. Intensive Care Med. 2007;33:1168–72.
Arend SM, Lavrijsen APM, Kuijken I, van der Plas RN, Kuijper EJ. Prospective controlled study of the diagnostic value of skin biopsy in patients with presumed meningococcal disease. Eur J Clin Microbiol Infect Dis. 2006;25:643–9.
Periappuram M, Taylor MR, Keane CT. Rapid detection of meningococci from petechiae in acute meningococcal infection. J Infect. 1995;31:201–3.
van Deuren M, van Dijke BJ, Koopman RJ, Horrevorts AM, Meis JF, Santman FW, et al. Rapid diagnosis of acute meningococcal infections by needle aspiration or biopsy of skin lesions. BMJ. 1993;306:1229–32.
de Risi-Pugliese T, Servy A, Decousser J-W, Nebbad B, Desroches M, Wolkenstein P, et al. Skin biopsy polymerase chain reaction for rapid microbiological diagnosis in patients with purpura fulminans. Br J Dermatol. 2017;177:e154–5.
Acknowledgements
The authors thanks all the members of the Hopeful Study group
For the HOPEFUL Study Group: Martin Cour (Lyon), Romain Sonneville and Charlotte Rabault (Bichat, AP-HP), Gaëtan Béduneau (Rouen), Sébastien Préau (Lille), Rémi Coudroy (Poitiers), Damien Roux (Louis Mourier, AP-HP), Frédéric Pène and Julien Massol (Cochin, AP-HP), Gwenhaël Colin (La Roche-sur-Yon), François Barbier and Kamel Toufik (Orléans), Antoine Marchalot (Dieppe), Quentin Quelven (Rennes), Guillaume Schnell (Le Havre), Stephan Ehrmann and Hélène Messet (Tours), Antoine Kimmoun (Nancy 1), Pascal Beuret (Roanne), Cédric Bruel (Saint-Joseph), Delphine Colling (Roubaix), Alexandre Conia (Chartres), Damien Contou (Argenteuil), Luis Ensenyat Martin and Danielle Reuter (Corbeil-Essonnes), Vincent Das and Marion Challier (Montreuil), Mathieu Jozwiak (Nice), Arnaud Galbois (Quincy sous Sénart), Mégan Fraisse (Ambroise Paré – AP-HP), Samir Jaber (Montpellier), Sébastien Jochmans (Melun), Pierre Kalfon (Chartres), Marie Conrad (Nancy 2), Alexandre Lautrette (Clermont Ferrand), Cédric Darreau (Le Mans), Nicolas Lerolle (Angers), Hugues Georges (Tourcoing), Bruno Mégarbane (Lariboisière, AP-HP), Claire Pichereau (Poissy), Tomas Urbina and Eric Maury (Saint-Antoine, AP-HP), Nicolas de Prost (Henri Mondor, AP-HP), Jean-Pierre Quenot (Dijon), Bertrand Sauneuf (Cherbourg), Matthieu Schmidt (Pitié Salpétrière, AP-HP), Xavier Valette (Caen), Lara Zafrani (Saint-Louis, AP-HP), Daniel Da Silva (Saint-Denis), Guillaume Rigault (Grenoble), Paul-Louis Woerther (Hôpital Henri Mondor, AP-HP)
Funding
None.
Author information
Authors and Affiliations
Consortia
Contributions
DC and NDP are responsible for the conception and design. All the authors were responsible for analysis and interpretation of data. All authors read, critically reviewed, and approved the final manuscript. DC takes responsibility for the paper as a whole. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This observational, non-interventional analysis of medical records was approved by the Institutional Review Board of the French Intensive Care Society in March 2016 (SRLF16-01).
Consent for publication
Not applicable.
Competing interests
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Contou, D., Béduneau, G., Rabault, C. et al. Skin biopsy in adult patients with meningococcal purpura fulminans: a multicenter retrospective cohort study. Crit Care 27, 166 (2023). https://doi.org/10.1186/s13054-023-04461-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04461-2