
Abstract
Background
Sepsis is a complex health condition, leading to long-term morbidity and mortality. Understanding the risk factors for recurrent sepsis, as well as its impact on mid- and long-term mortality among other risk factors, is essential to improve patient survival.
Methods
A risk factor analysis, based on French nationwide medico-administrative data, was conducted on a cohort of patients above 15 years old, hospitalized with an incident sepsis in metropolitan France between 1st January 2018 and 31st December 2018 and who survived their index hospitalization. Two main analyses, focusing on outcomes occurring 1-year post-discharge, were conducted: a first one to assess risk factors for recurrent sepsis and a second to assess risk factors for mortality.
Results
Of the 178017 patients surviving an incident sepsis episode in 2018 and included in this study, 22.3% died during the 1-year period from discharge and 73.8% had at least one hospital readmission in acute care, among which 18.1% were associated with recurrent sepsis. Patients aged between 56 and 75, patients with cancer and renal disease, with a long index hospital stay or with mediastinal or cardiac infection had the highest odds of recurrent sepsis. One-year mortality was higher for patients with hospital readmission for recurrent sepsis (aOR 2.93; 99% CI 2.78–3.09). Among all comorbidities, patients with cancer (aOR 4.35; 99% CI 4.19–4.52) and dementia (aOR 2.02; 99% CI 1.90–2.15) had the highest odds of 1-year mortality.
Conclusion
Hospital readmission for recurrent sepsis is one of the most important risk factors for 1-year mortality of septic patients, along with age and comorbidities. Our study suggests that recurrent sepsis, as well as modifiable or non-modifiable other risk factors identified, should be considered in order to improve patient care pathway and survival.
Similar content being viewed by others

Background
Sepsis is a complex health condition, leading to long-term morbidity, high level of mortality and substantial economic burden for the health care system [1,2,3,4]. Severe sequelae resulting from sepsis episodes can alter patients health condition, increase the risk of hospital readmission and also reduce their life expectancy [3, 5]. Sepsis is associated with a high risk of hospital readmission and recurrent sepsis is also the most common cause of hospital readmission in previous studies [1, 6, 7]. However, other causes are also reported [2, 8, 9]. Hospital readmission can be influenced by several factors such as age, specific health conditions, social background, comorbidities and acute injuries [1, 6, 10,11,12] but some of these risk factors like age or important comorbidities as well as ICU and mechanical ventilation were not significantly different between septic patients with and without recurrent sepsis [7]. More generally, risk factors for recurrent sepsis are seldomly studied. The risk of readmission is usually higher in the first weeks after the index hospitalization, but it could eventually occur after a longer period [6, 7]. Several studies focussed on 30 or 90-day readmission after the index admission for sepsis but few studies focussed specifically on hospital readmission for recurrent sepsis over a longer period and its associated risk factors [4, 7, 13].
The mortality rate for sepsis is relatively high. Studies are hardly comparable because of differences in the study population, the methods of selection for sepsis cases and changes in sepsis definition across the study periods. In recent studies, in-hospital mortality rate varied from 11.8 to 35.8%, 30-day mortality between 8.3 and 26.5% [5, 14,15,16,17,18,19] and 1-year mortality from 12.5 to almost 50% [5, 20]. The identified risk factors for mid- to short-term mortality include age, comorbidities, multiple organ failure and septic shock [14, 15, 21,22,23,24]. Short-term mortality is usually higher in the elderly. However, short-term assessment underestimate the possible sequelae of sepsis which may lead to possible hospital readmission, or other risk factors for long-term mortality in sepsis survivors [6, 7, 22, 25]. DeMerle and al. showed that 90-day mortality was higher for septic patients readmitted for sepsis [7]. However, the risk factors for long-term mortality of sepsis survivors, and in particular the association between hospital readmission for recurrent sepsis and long-term mortality, have been scarcely studied [6, 26]. To the best of our knowledge, no nationwide study was recently published in France on this specific topic.
The aim of this nationwide study was to assess the risk factors for 1-year hospital readmission for recurrent sepsis, as well as the possible impact of recurrent sepsis and other risk factors as age and comorbidities on 1-year mortality in sepsis survivors.
Methods
Data source, definitions, and study population
The study consisted of a secondary data analysis of a cohort of all patients with bacterial infections and registered in the anonymized French National Hospital Discharge Database (Programme de Médicalisation des Systèmes d'Information: PMSI) and outpatient health care consumption (Données de Consommation Inter-Régimes: DCIR) issued from the French health care database (Système National des Données de Santé: SNDS) (see Additional file 1: eMethods) [27, 28]. Therefore, only cases of sepsis of presumed bacterial etiology (referred to herein as sepsis) were considered.
Targeting to select sepsis related hospital stays, sepsis was identified as the combination of explicit sepsis and implicit sepsis [18, 29, 30]. The selection in the French medico-administrative database was based on a list of ICD-10 codes, organ dysfunction and ICU admission (see Additional file 1: eMethods and eTable 1). More details about the selection can be found in our previous study [27]. Only hospital stays in an acute-care facility (MSO: medicine surgery and obstetrics) were considered. Stays shorter than one day where the patient did not die were excluded.
The study population included all patients above 15 years old, hospitalized with an incident sepsis (index hospitalization) in metropolitan France between 1st January 2018 and 31st December 2018 and who survived their index hospitalization. Patients with an incident sepsis were identified as patients who did not experience a sepsis-related hospitalization during the previous 12 months of their first sepsis-related hospitalization in 2018. Recurrent sepsis was defined by at least one sepsis-related hospital readmission during the 12-month period following hospital discharge of the index sepsis hospitalization; 1-year mortality was defined as patient death during the same period.
Patient, infection, and hospitalization characteristics such as sex, age, Charlson index and detailed comorbidities, infection site, admission source, hospital discharge, length of stay, day of death, admission to ICU and septic shock were recorded (see Additional file 1: eTable2). One-year hospital readmissions in MSO for sepsis or other diagnoses were recorded.
Statistical analyses
Patients were categorized and described according to 1-year hospital readmissions for recurrent sepsis as well as 1-year mortality. Hospital stays and site of infections were also described for these categories as well as acute cardiac events. The mortality of sepsis survivors was estimated at 30 days, 90 days, 6 months and 1 year following discharge of the index-hospitalization and stratified according to 1-year hospital readmission for recurrent sepsis.
Firstly, patients, infection and index hospital stay characteristics were described according to the variables of interest (re-hospitalized for recurrent sepsis vs not re-hospitalized or re-hospitalized for other causes; 1-year mortality vs alive). Frequencies (percentages) were reported for discrete variables and median and interquartile range (IQR) for quantitative ones. As the data cover the national population, no confidence intervals were calculated for percentages [31, 32].
Secondly, two main analyses were conducted on the selected survivor population. The first analysis aimed at identifying risk factors for re-hospitalization with recurrent sepsis during the 1-year period from discharge of the index hospitalization. In order to improve the robustness of our results, this analysis was repeated on two subpopulations of sepsis survivors: only those experiencing hospital readmission (for sepsis or any other reason), and on sepsis survivors with explicit sepsis only. The second analysis aimed at identifying risk factors for 1-year mortality post-discharge. This analysis was also repeated on sepsis survivors with explicit sepsis only. Logistic regressions were used to identify risk factors associated with the two studied outcomes: recurrent sepsis or 1-year mortality. For the latter, a Cox regression was also used to assess hazard ratio for 1-year mortality. One-year Kaplan–Meier crude survival curve was also produced.
We conducted a univariate analysis including potential confounders and risk factors followed by a multivariate analysis. Risk factors considered are listed in Tables 1 and 2. As ICU admission and septic shock were not independent, a 4-classes variable was constructed: the absence of both, the presence of ICU admission only, the presence of septic shock only and the presence of both (see Additional file 1: eTable2). Since individual comorbidities were considered, the Charlson index, a score which combines comorbidities, was not included in the logistic regressions. The variables for which the 99% CI of the crude odd ratio or hazard ratio (cOR/cHR) did not contain 1 and with a global P-value < 0.01 were included in the multivariate analysis. As the data cover the national population, a conservative 2-tailed P-value < 0.01 in the multivariable model defined significance [31, 32].
Results
Selection of the study population
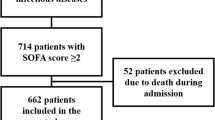
In total, 231,934 patients were admitted with incident sepsis in 2018 of which 23.3% died during the index admission (Fig. 1). Of the 178,017 patients (140,658 with explicit sepsis and 37,359 with implicit sepsis) who survived the index hospitalization, 131,364 (73.8%) had at least one hospital readmission in MSO (all causes) in the year following hospital discharge, among which 23,728 (18.1%) were associated with recurrent sepsis.

Flowchart of patient selection
Recurrent sepsis during the 1-year period following hospital discharge
Description
Patients, infections, and hospitalization characteristics recorded during the index hospitalization, according to 1-year hospital readmission for recurrent sepsis are reported in Table 3. As compared with those having no recurrence, patients with recurrent sepsis were more often men (62.6% vs 55.8%) and had more often comorbidities, especially cancer (35.7% vs 20.6%). Regarding infection sites, recurrent sepsis was more often associated with primary bacteremia (19.6% vs 15.9%), multiple sites infection (23.9% vs 21.7%) and less frequently with urinary or genital tract infections (15.2% vs 18.3%). One-year mortality was also much higher for these patients (39.8% vs 19.6%). For patients who experienced recurrent sepsis the median (range) number of recurrences in the following year was 2 (2–14). The median number of days and IQR between the index hospitalization and the first recurrence was 76 (25–178) days.
Risk factors analysis
Among potential confounders or risk factors for recurrent sepsis, only one comorbidity (paraplegia and hemiplegia) was excluded from the multivariate analysis (Table 1). After adjustment, women had a lower aOR (adjusted Odds ratio) of hospital readmission for recurrent sepsis than men, and those aged between 56 and 75 yrs had the highest aOR compared to younger patients. Among all comorbidities, cancer (aOR 1.98; 99% CI 1.90–2.07) and renal disease (aOR 1.55; 99% CI 1.47–1.63) were associated with the highest aOR while dementia had an aOR lower than 1 (aOR 0.82; 99% CI 0.74–0.90). Compared to home discharge, the risk of hospital readmission for recurrent sepsis was lower for patients discharged to long-term care (aOR 0.89; 99% CI 0.84–0.95), whereas the aOR of hospital readmission was almost twice higher for a length of stay of the index admission > 90 days compared to one < 7 days. Hospital readmission for recurrent sepsis was lower with ICU admission, only for patients without septic shock (aOR 0.82; 99% CI 0.79–0.86). Compared to urinary and genital tracts infection, heart and mediastinum infection had the highest aOR (aOR 1.47; 99% CI 1.35–1.61). The directionality of the risk factors was similar when the analysis was conducted on the subgroup of patients with explicit sepsis only (see Additional file 1: eTable 3). However, when sepsis-related readmissions were compared to hospital readmission for other causes, discharge to acute care was identified as a protective factor for sepsis-related hospital readmission (aOR 0.83; 99% CI 0.79–0.88). In the latter analysis, the length of stay and some major comorbidities (cancer, renal and liver diseases, diabetes, AIDS) remained relevant risk factors for sepsis-related hospital readmission (see Additional file 1: eTable 4).
Mortality during the 1-year period following hospital discharge
Description
Among patients who survived to their incident sepsis episode, 39,696 (22.3%) died in the year following hospital discharge of the index hospitalization. One-year mortality was much higher among patients with recurrent sepsis compared to patients which did not experience recurrent sepsis in the following year. Those who had died at 1-year were more often elderly (> 75 years), with a higher Charlson index and more often comorbidities, especially cancer (42.8% vs 16.8% among 1-year survivors). They also had more often bacteremia or multiple infections and less often urinary/genital tracts infection and a higher proportion of septic shock without ICU admission (Table 4, see Additional file 1: eTable 5).
Risk factors analysis
Among potential confounders or risk factors for 1-year mortality, two comorbidities (Rheumatologic disease and paraplegia/hemiplegia) were excluded from the multivariate analysis. Women had a lower aOR of 1-year mortality than men. As expected, mortality tended to increase with age, with the oldest age category (> 85 years) having the greatest odds of 1-year mortality (aOR 11.33; 99% CI 9.54–13.47). Among all comorbidities, cancer (aOR 4.35; 99% CI 4.19–4.52) and dementia (aOR 2.02; 99% CI 1.90–2.15) were associated with the highest aOR (Table 2). Compared to patients without hospital readmission, one-year mortality was higher for patients having sepsis-related hospital readmission (aOR 2.93; 99% CI 2.78–3.09) than for those with hospital readmission for other acute care (aOR 1.25; 99% CI 1.20–1.30). ICU admission was inversely associated with 1-year mortality, whether septic shock was present or not. Compared to patients without ICU admission and no septic shock, the aOR of patients without ICU admission and septic shock was higher (aOR 1.82; 99% CI 1.63–2.04) (see Additional file 1: eTable 6 for patients characteristics). Compared to urinary and genital tracts infection, skin and soft tissues, bacteremia, heart and mediastinum, multiple sites of infection and lower respiratory tract infection had the highest aOR. The directionality of the risk factors was similar when the analysis was restricted to explicit sepsis (see Additional file 1: eTable 7) or with the Cox regression (see Additional file 1: eTable 8). Additionally, 1-year Kaplan–Meier crude survival curve illustrates the difference in survival between patients with and without 1-year hospital readmission for recurrent sepsis (see Additional file 1: eFig. 1).
Discussion
Hospital readmission and associated mortality
Our study confirmed that hospital readmission is highly expected for most of patients hospitalized with sepsis. More than 70% of the patients who survived a first episode of sepsis experienced hospital readmission in acute care in the following year, of whom 18.1% had readmission for recurrent sepsis. One-year hospital readmission has been rarely assessed in previous studies. In previous works, 29.7 and to 42.7% of sepsis patients experienced all causes 90-days readmission and 22 to 57.4% experienced all causes readmission at 1 year [4, 7, 13, 33,34,35]. Indeed, numerous patients have comorbidities and a new admission in MSO is expected. We report a slightly higher readmission rate, but we have considered all hospital readmissions without exclusion criteria. A few studies report a high proportion (38.0 to 61.2%) of hospital readmission specifically due to infection (including sepsis) [13, 35], but there is a lack of data in the literature regarding 1-year readmission specifically due to sepsis. In line with previous studies, the mortality rate was twice higher for patients who experienced hospital readmission for recurrent sepsis compared to the patients without hospital readmission or re-hospitalized for other causes (39.8% vs 19.6%) [6, 36].
Risk factors for recurrent sepsis
Risk factors for patients with recurrent sepsis, compared to patients not re-hospitalized or re-hospitalized for other causes, were identified. In line with previous studies [1, 6, 8, 10, 10, 11, 33, 37,38,39,40,41], older patients and patients with comorbidities, especially renal disease and cancer, had the greatest odds of hospital readmission for recurrent sepsis. Indeed, immunosenescence of old patients but also cancer and associated medical procedures which impair the immune system, may increase the risk of relapse or new sepsis episode [8]. In addition, patients who had longer hospitalization or sepsis due to heart and mediastinum infection were at higher risk of hospital readmission and rehospitalization in MSO in the following 12 months for acute cardiac events were also more frequent for patients with recurrent sepsis. Indeed, longer hospitalization can act as proxy for the most serious sepsis cases or debilitated patients and infective endocarditis are frequent pathology in the elderly and associated with unfavorable outcomes [1, 6, 12, 42,43,44,45,46]. Moreover, the association between sepsis survivors and cardiovascular problem have been previously identified [47]. Hospital discharge to long-term care appeared as a protective factor in our study, possibly reflecting a limitation to acute care readmission for older and debilitated patients preferably referred to hospice care, or a larger use of follow-up care and rehabilitation contributing to better patient recovery [1, 6]. Discharge to acute care, appears to be a protective factor for readmission for recurrent sepsis compared to readmission for other causes, probably because such patients are referred post-sepsis to a unit for management of a pre-existing a primary health condition, and such patients tend to be re-hospitalized for this primary condition instead of sepsis.
Recurrent sepsis and other risk factors for 1-year mortality
Recurrent sepsis emerged as an important risk factor for 1-year mortality (~ threefold increase in 1-year mortality), along with five others important risk factors: age, cancer, dementia, septic shock and skin and soft tissues infection (> 1.5-fold increase in 1-year mortality). Indeed, readmission for sepsis was associated with higher risk of 30-days, 6-month and 2-years mortality in previous studies [6, 36]. Apart from recurrent sepsis, age, dementia and cancer, which usually result in complicated clinical scenario, represented important risk factors [23, 48,49,50]. Cancer is also an important risk factor in middle-aged patients [14, 37, 51, 52]. However, the immunosenescence in older patients might be comparable to the immune impairment of patients with cancer or receiving cancer treatment [37]. Dementia is also particularly present in older patients hospitalized with sepsis and tends to adversely influence clinical outcomes [49]. Finally, the higher odds of mortality identified for skin and soft tissues infection may be related to the most common etiologies of such infections, possibly reflecting the high frequency of Staphylococcus aureus infection, often associated with shock and mortality [45, 53]. The protective effect of ICU admission, with an increased case fatality rate for septic patients not admitted to ICU, was also noted in a previous study in France. ICU access is part of the strategy to tackle sepsis in the “surviving sepsis campaign” [54]. While admission to ICU for sepsis is usual but not mandatory, lack of admission for septic shock can be explained by several hypothesis as misdiagnosis, suboptimal care and, more probably, limitations to ICU referral of older patients [18, 54].
Preventable and non-preventable risk factors
Risk factor analysis are of interest for practitioners or decision makers when preventable risk factors can be identified, allowing subsequent intervention [9]. In previous studies, a low percentage of sepsis-related deaths were estimated preventable, at least in high income countries [55]. Moreover, medico-administrative databases, as the one used in this study, can lack of detailed information regarding these potentially preventable risks. However, some factors suggest a room for consideration and possible action. Although non-modifiable, some risk factors can act as indicators, raising awareness on specific patients in order to adapt their care pathway during their hospital stay or after their hospital discharge [9]. Because recurrent sepsis was one of main risk factor for mortality, preventing and reducing hospital readmission for recurrent sepsis could participate at reducing the mortality rate. Specific acute and post-acute care interventions could be implemented for patients at risk of recurrent sepsis, including patients with comorbidities (especially cancer), the elderly, patients with cardiac infection or more generally sepsis that have required long hospital stay. Indeed, a specific clinical pathway for sepsis according to patients profile was suggested in order to improve patients outcomes and has been already implemented for patients with cancer in Australia [3, 56]. Regarding post-acute care, discharge to long-term care appeared to be a protective factor for recurrent sepsis in our study. This suggests, as previously mentioned, fewer readmission to acute care for the most debilitated patients transferred to palliative care or, in line with previous studies, a real protective effect of post-sepsis rehabilitation [1, 6, 8, 57]. The protective effect of long-term care could suggests possible need for more transfer to long-term care or closer follow-up of some patients returning home and should be explored in additional research [8, 9]. Regarding acute care, the use of ICU appeared to be a protective factor for mortality and recurrent sepsis (in the absence of septic shock) as suggested by a previous study in France [18]. However, the higher risk of recurrent sepsis for patients with cardiac and mediastinum infection or the higher risk of mortality for skin and soft tissue infection should call for special attention or intervention, even for patients not admitted to ICU. Indeed, comorbidities might transform mild skin infection in life-threatening infection and antimicrobial resistance is relatively common in this infection sites [58, 59]. Infective endocarditis is common in the elderly due to the increasing number of cardiac procedures and the recommended therapeutic strategy can also be complicated in these patients, putting them at risk of recurrent sepsis or death [46]. Despite possible improvements, some important risk factors for recurrent sepsis or mortality can be considered as non or moderately preventable, as age or comorbidities [3, 55]. Indeed, the severity of associated illnesses at sepsis onset could make unlikely patient survival even with effective sepsis treatment [55]. However, further studies regarding the care pathway of sepsis patients and more personalized sepsis management and post-acute care according to the different typologies of patients based on age, comorbidities, sites of infection or severity of the sepsis onset could potentially improve patient outcomes, survival and cost for the health care system [8, 12, 56, 60]. General international guidelines are regularly established for sepsis management [61]. In France, the French National Authority for Health (HAS) is currently building integrated recommendations for sepsis management [62]. Based on the results of this study, specific recommendations could be beneficial for patients at high risk of recurrent sepsis.
Limitations of the study
This study is based on a secondary data analysis of medico-administrative data, without possible validation of sepsis cases based on clinical data. As a result, patients hospitalized with sepsis, based on a combination of implicit and explicit sepsis, could be slightly over or underestimated [30, 63, 64]. However, the analyses, based on explicit sepsis only, confirmed the robustness of our results. Due to administrative and regulation hurdles, a database with only sepsis with bacterial etiology was used in this analysis. However, fungus or viruses represents a small percentage of all sepsis causative pathogens [45]. Moreover, regarding recurrent sepsis, the difference between new pathogens or relapse of the initial sepsis with the same pathogens could not be made as the pathogens, potential antibiotic resistance and the connection between pathogen and infection site could not be identified. Finally, the absence of information of physical and mental impairments after discharge should be further considered in a study of the care pathway of these patients.
Conclusion
Hospital readmission and mid-term mortality of patients hospitalized with sepsis are substantial. In our study, patients with cancer and recurrent sepsis had the highest odds of 1-year mortality. Our study suggests that some risk factors, even if non modifiable, should be considered to personalize the care pathway of the most vulnerable patients. Moreover, the need for post-acute care and adequate follow-up after hospital discharge should be further considered. Changes in the care pathway to reduce sepsis related readmission could improve survival and associated economic burden for the health care system.
Availability of data and materials
The data that support the findings of this study are available from the French national health insurance information system but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
References
Gadre SK, Shah M, Mireles-Cabodevila E, Patel B, Duggal A. Epidemiology and predictors of 30-day readmission in patients with sepsis. Chest. 2019;155(3):483–90. https://doi.org/10.1016/j.chest.2018.12.008.
Hines AL, Barrett ML, Jiang HJ, Steiner CA. Conditions with the largest number of adult hospital readmissions by payer, 2011: statistical brief #172. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality (US); 2006. Accessed 1 Feb 2022. http://www.ncbi.nlm.nih.gov/books/NBK206781/.
Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet Lond Engl. 2018;392(10141):75–87. https://doi.org/10.1016/S0140-6736(18)30696-2.
Prescott HC, Langa KM, Iwashyna TJ. Readmission diagnoses after hospitalization for severe sepsis and other acute medical conditions. JAMA. 2015;313(10):1055–7. https://doi.org/10.1001/jama.2015.1410.
Farrah K, McIntyre L, Doig CJ, et al. Sepsis-associated mortality, resource use, and healthcare costs: a propensity-matched cohort study. Crit Care Med. 2021;49(2):215–27. https://doi.org/10.1097/CCM.0000000000004777.
Goodwin AJ, Rice DA, Simpson KN, Ford DW. Frequency, cost, and risk factors of readmissions among severe sepsis survivors. Crit Care Med. 2015;43(4):738–46. https://doi.org/10.1097/CCM.0000000000000859.
DeMerle KM, Royer SC, Mikkelsen ME, Prescott HC. Readmissions for recurrent sepsis: new or relapsed infection? Crit Care Med. 2017;45(10):1702–8. https://doi.org/10.1097/CCM.0000000000002626.
Jones TK, Fuchs BD, Small DS, et al. Post-acute care use and hospital readmission after sepsis. Ann Am Thorac Soc. 2015;12(6):904–13. https://doi.org/10.1513/AnnalsATS.201411-504OC.
Bowles KH, Murtaugh CM, Jordan L, et al. Sepsis survivors transitioned to home health care: characteristics and early readmission risk factors. J Am Med Dir Assoc. 2020;21(1):84. https://doi.org/10.1016/j.jamda.2019.11.001.
Ortego A, Gaieski DF, Fuchs BD, et al. Hospital-based acute care use in survivors of septic shock. Crit Care Med. 2015;43(4):729–37. https://doi.org/10.1097/CCM.0000000000000693.
Zilberberg MD, Shorr AF, Micek ST, Kollef MH. Risk factors for 30-day readmission among patients with culture-positive severe sepsis and septic shock: a retrospective cohort study. J Hosp Med. 2015;10(10):678–85. https://doi.org/10.1002/jhm.2420.
Sun A, Netzer G, Small DS, et al. Association between index hospitalization and hospital readmission in sepsis survivors. Crit Care Med. 2016;44(3):478–87. https://doi.org/10.1097/CCM.0000000000001464.
Shankar-Hari M, Saha R, Wilson J, et al. Rate and risk factors for rehospitalisation in sepsis survivors: systematic review and meta-analysis. Intensive Care Med. 2020;46(4):619–36. https://doi.org/10.1007/s00134-019-05908-3.
Wardi G, Tainter CR, Ramnath VR, et al. Age-related incidence and outcomes of sepsis in California, 2008–2015. J Crit Care. 2021;62:212–7. https://doi.org/10.1016/j.jcrc.2020.12.015.
Fay K, Sapiano MRP, Gokhale R, et al. Assessment of health care exposures and outcomes in adult patients with sepsis and septic shock. JAMA Netw Open. 2020;3(7): e206004. https://doi.org/10.1001/jamanetworkopen.2020.6004.
Rhee C, Dantes R, Epstein L, et al. Incidence and trends of sepsis in US Hospitals using clinical vs claims data, 2009–2014. JAMA. 2017;318(13):1241–9. https://doi.org/10.1001/jama.2017.13836.
Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41(5):1167–74. https://doi.org/10.1097/CCM.0b013e31827c09f8.
Dupuis C, Bouadma L, Ruckly S, et al. Sepsis and septic shock in France: incidences, outcomes and costs of care. Ann Intensive Care. 2020;10(1):145. https://doi.org/10.1186/s13613-020-00760-x.
Bauer M, Gerlach H, Vogelmann T, Preissing F, Stiefel J, Adam D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019-results from a systematic review and meta-analysis. Crit Care Lond Engl. 2020;24(1):239. https://doi.org/10.1186/s13054-020-02950-2.
Davis JS, He V, Anstey NM, Condon JR. Long term outcomes following hospital admission for sepsis using relative survival analysis: a prospective cohort study of 1092 patients with 5 year follow up. PLoS ONE. 2014;9(12): e112224. https://doi.org/10.1371/journal.pone.0112224.
Sanderson M, Chikhani M, Blyth E, et al. Predicting 30-day mortality in patients with sepsis: an exploratory analysis of process of care and patient characteristics. J Intensive Care Soc. 2018;19(4):299–304. https://doi.org/10.1177/1751143718758975.
Lee SH, Hsu TC, Lee M, Tse G, et al. Nationwide trend of sepsis: a comparison among octogenarians, elderly, and young adults. Crit Care Med. 2018;46(6):926–34. https://doi.org/10.1097/CCM.0000000000003085.
Martin S, Perez A, Aldecoa C. Sepsis and Immunosenescence in the elderly patient: a review. Front Med. 2017;4:20. https://doi.org/10.3389/fmed.2017.00020.
Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274(12):968–74.
Winters BD, Eberlein M, Leung J, Needham DM, Pronovost PJ, Sevransky JE. Long-term mortality and quality of life in sepsis: a systematic review. Crit Care Med. 2010;38(5):1276–83. https://doi.org/10.1097/CCM.0b013e3181d8cc1d.
Papanicolas I, Orav EJ, Jha AK. Is mortality readmissions bias a concern for readmission rates under the Hospital Readmissions Reduction Program? Health Serv Res. 2020;55(2):249–58. https://doi.org/10.1111/1475-6773.13268.
Pandolfi F, Guillemot D, Watier L, Brun-Buisson C. Trends in bacterial sepsis incidence and mortality in France between 2015 and 2019 based on National Health Data System (Système National des données de Santé (SNDS)): a retrospective observational study. BMJ Open. 2022;12(5): e058205. https://doi.org/10.1136/bmjopen-2021-058205.
Tuppin P, Rudant J, Constantinou P, et al. Value of a national administrative database to guide public decisions: From the système national d’information interrégimes de l’Assurance Maladie (SNIIRAM) to the système national des données de santé (SNDS) in France. Rev Epidemiol Sante Publique. 2017;65(Suppl 4):S149–67. https://doi.org/10.1016/j.respe.2017.05.004.
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–10. https://doi.org/10.1097/00003246-200107000-00002.
Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet Lond Engl. 2020;395(10219):200–11. https://doi.org/10.1016/S0140-6736(19)32989-7.
Ioannidis JPA. What have we (not) learnt from millions of scientific papers with P values? Am Stat. 2019;73(sup1):20–5. https://doi.org/10.1080/00031305.2018.1447512.
Lin M, Lucas HC Jr, Shmueli G. Too big to fail: large samples and the p-value problem. Inf Syst Res. 2013;24(4):906–17. https://doi.org/10.1287/isre.2013.0480.
Stenholt POO, Bin Abdullah SMO, Sorensen RH, Nielsen FE. Independent predictors for 90-day readmission of emergency department patients admitted with sepsis: a prospective cohort study. Bmc Infect Dis. 2021;21(1):315. https://doi.org/10.1186/s12879-021-06007-9.
Kim JS, Kim YJ, Ryoo SM, et al. Risk factors for same pathogen sepsis readmission following hospitalization for septic shock. J Clin Med. 2019;8(2):181. https://doi.org/10.3390/jcm8020181.
Liu V, Lei X, Prescott HC, Kipnis P, Iwashyna TJ, Escobar GJ. Hospital readmission and healthcare utilization following sepsis in community settings. J Hosp Med Off Publ Soc Hosp Med. 2014;9(8):502–7. https://doi.org/10.1002/jhm.2197.
Fry CH, Fluck D, Han TS. Frequent identical admission-readmission episodes are associated with increased mortality. Clin Med. 2021;21(4):E351–6. https://doi.org/10.7861/clinmed.2020-0930.
Hensley MK, Donnelly JP, Carlton EF, Prescott HC. Epidemiology and outcomes of cancer-related versus non-cancer-related sepsis hospitalizations. Crit Care Med. 2019;47(10):1310–6. https://doi.org/10.1097/CCM.0000000000003896.
Nelson JE, Cox CE, Hope AA, Carson SS. Chronic critical illness. Am J Respir Crit Care Med. 2010;182(4):446–54. https://doi.org/10.1164/rccm.201002-0210CI.
Loss SH, Nunes DSL, Franzosi OS, Salazar GS, Teixeira C, Vieira SRR. Chronic critical illness: are we saving patients or creating victims? Rev Bras Ter Intensiva. 2017;29(1):87–95. https://doi.org/10.5935/0103-507X.20170013.
Darden DB, Kelly LS, Fenner BP, Moldawer LL, Mohr AM, Efron PA. Dysregulated immunity and immunotherapy after sepsis. J Clin Med. 2021;10(8):1742. https://doi.org/10.3390/jcm10081742.
Mira JC, Gentile LF, Mathias BJ, et al. Sepsis pathophysiology, chronic critical illness and PICS. Crit Care Med. 2017;45(2):253–62. https://doi.org/10.1097/CCM.0000000000002074.
Paoli C, Reynolds M, Sinha M, Gitlin M, Crouser E. Epidemiology and costs of sepsis in the united states-an analysis based on timing of diagnosis and severity level. Crit Care Med. 2018;46:12. https://doi.org/10.1097/CCM.0000000000003342.
Liu YZ, Chu R, Lee A, et al. A surveillance method to identify patients with sepsis from electronic health records in Hong Kong: a single centre retrospective study. BMC Infect Dis. 2020;20(1):652. https://doi.org/10.1186/s12879-020-05330-x.
Krajinovic V, Ivancic S, Gezman P, Barsic B. Association between cardiac surgery and mortality among patients with infective endocarditis complicated by sepsis and septic shock. Shock. 2018;49(5):536–42. https://doi.org/10.1097/SHK.0000000000001013.
Umemura Y, Ogura H, Takuma K, et al. Current spectrum of causative pathogens in sepsis: a prospective nationwide cohort study in Japan. Int J Infect Dis. 2021;103:343–51. https://doi.org/10.1016/j.ijid.2020.11.168.
Forestier E, Fraisse T, Roubaud-Baudron C, Selton-Suty C, Pagani L. Managing infective endocarditis in the elderly: new issues for an old disease. Clin Interv Aging. 2016;11:1199–206. https://doi.org/10.2147/CIA.S101902.
Kosyakovsky LB, Angriman F, Katz E, et al. Association between sepsis survivorship and long-term cardiovascular outcomes in adults: a systematic review and meta-analysis. Intensive Care Med. 2021;47(9):931–42. https://doi.org/10.1007/s00134-021-06479-y.
Sehgal V, Bajwa SJS, Consalvo JA, Bajaj A. Clinical conundrums in management of sepsis in the elderly. J Transl Intern Med. 2015;3(3):106–12. https://doi.org/10.1515/jtim-2015-0010.
Bouza C, Martínez-Alés G, López-Cuadrado T. The impact of dementia on hospital outcomes for elderly patients with sepsis: a population-based study. PLoS ONE. 2019;14(2): e0212196. https://doi.org/10.1371/journal.pone.0212196.
Liao KM, Lin TC, Li CY, Yang YHK. Dementia increases severe sepsis and mortality in hospitalized patients with chronic obstructive pulmonary disease. Medicine (Baltimore). 2015;94(23): e967. https://doi.org/10.1097/MD.0000000000000967.
Sharma A, Nguyen P, Taha M, Soubani AO. Sepsis hospitalizations with versus without cancer: epidemiology, outcomes, and trends in nationwide analysis from 2008 to 2017. Am J Clin Oncol. 2021;44(10):505–11. https://doi.org/10.1097/COC.0000000000000859.
Prest J, Sathananthan M, Jeganathan N. Current trends in sepsis-related mortality in the United States. Crit Care Med. 2021;49(8):1276–84. https://doi.org/10.1097/CCM.0000000000005017.
Paulsen J, Mehl A, Askim Å, Solligård E, Åsvold BO, Damås JK. Epidemiology and outcome of Staphylococcus aureus bloodstream infection and sepsis in a Norwegian county 1996–2011: an observational study. BMC Infect Dis. 2015;15:116. https://doi.org/10.1186/s12879-015-0849-4.
Bennett SR. Sepsis in the intensive care unit. Surg Oxf Oxfs. 2015;33(11):565–71. https://doi.org/10.1016/j.mpsur.2015.08.002.
Rhee C, Jones TM, Hamad Y, et al. Prevalence, underlying causes, and preventability of sepsis-associated mortality in US Acute Care Hospitals. JAMA Netw Open. 2019;2(2): e187571. https://doi.org/10.1001/jamanetworkopen.2018.7571.
Thursky K, Lingaratnam S, Jayarajan J, et al. Implementation of a whole of hospital sepsis clinical pathway in a cancer hospital: impact on sepsis management, outcomes and costs. BMJ Open Qual. 2018;7(3): e000355. https://doi.org/10.1136/bmjoq-2018-000355.
Chao PW, Shih CJ, Lee YJ, et al. Association of postdischarge rehabilitation with mortality in intensive care unit survivors of sepsis. Am J Respir Crit Care Med. 2014;190(9):1003–11. https://doi.org/10.1164/rccm.201406-1170OC.
Macía-Rodríguez C, Alende-Castro V, Vazquez-Ledo L, Novo-Veleiro I, González-Quintela A. Skin and soft-tissue infections: factors associated with mortality and re-admissions. Enfermedades Infecc Microbiol Clínica. 2017;35(2):76–81. https://doi.org/10.1016/j.eimc.2016.02.030.
Ki V, Rotstein C. Bacterial skin and soft tissue infections in adults: a review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can J Infect Dis Med Microbiol. 2008;19(2):173–84.
Pesko MF, Gerber LM, Peng TR, Press MJ. Home health care: nurse-physician communication, patient severity, and hospital readmission. Health Serv Res. 2018;53(2):1008–24. https://doi.org/10.1111/1475-6773.12667.
Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11): e1063. https://doi.org/10.1097/CCM.0000000000005337.
HAS. Prise en charge du sepsis du nouveau-né, de l’enfant et de l’adulte : recommandations pour un parcours de soins intégré. Published online February 16, 2022. https://www.has-sante.fr/plugins/ModuleXitiKLEE/types/FileDocument/doXiti.jsp?id=p_3333917.
Jolley RJ, Sawka KJ, Yergens DW, Quan H, Jetté N, Doig CJ. Validity of administrative data in recording sepsis: a systematic review. Crit Care Lond Engl. 2015;19:139. https://doi.org/10.1186/s13054-015-0847-3.
Wilhelms SB, Huss FR, Granath G, Sjöberg F. Assessment of incidence of severe sepsis in Sweden using different ways of abstracting international classification of diseases codes: difficulties with methods and interpretation of results. Crit Care Med. 2010;38(6):1442–9. https://doi.org/10.1097/CCM.0b013e3181de4406.
Acknowledgements
We are grateful to DATAD department of the French National Health Insurance for providing the data.
Funding
This work was supported by award RMA19183LLA from the French Ministry of Social Affairs and Health.
Author information
Authors and Affiliations
Contributions
LW, CBB, DG and FP have designed the study. LW, CBB and FP had participated to the data collection, the data analysis and have drafted the manuscript. LW, CBB, DG and FP contributed to the critical revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study, analysis and data extraction were approved by the French Data Protection Agency (CNIL, approval DE-2016-176). Informed consent is waived for the use of these anonymised secondary data, as mentioned in the Social Security Code, Article L161-28-1. All methods were performed in accordance with CNIL regulations and with REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guideline.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. eMethods
Description of the French National Hospital Discharge Database (PMSI) and Inter-Scheme consumption data (DCIR), eTable 1 ICD-10 codes used to identify sepsis of presumed bacterial etiology according to type of selection in sepsis patients > 15 years, eTable 2 Description of the variables, eTable 3 Risk factors, recorded during the index hospitalization, for 1-year hospital readmission for recurrent sepsis for 140,658 adult patients hospitalized with explicit sepsis in metropolitan France in 2018: univariate and multivariate logistic regressions, eTable 4 Risk factors, recorded during the index hospitalization, for 1-year hospital readmission for recurrent sepsis for 131,364 adult septic patients who were rehospitalized (with sepsis or other causes) in the following year, metropolitan France, 2018: univariate and multivariate logistic regressions, eTable 5 Comorbidities and demographic, hospital stay and infection characteristics of adult patients with sepsis according to 1-year survival, metropolitan France 2018, eTable 6 Charlson index and demographic of adult patients with septic choc without ICU admission, metropolitan France 2018, eTable 7 Risk factors for 1-year mortality of the 140,658 adult patients surviving a first episode of sepsis (explicit sepsis only) in metropolitan France in 2018: univariate and multivariate logistic regression, eTable 8 Cox regression and hazard ratio for 1-year mortality of the 178,017 adult patients surviving a first episode of sepsis in metropolitan France in 2018: Multivariate analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Pandolfi, F., Brun-Buisson, C., Guillemot, D. et al. One-year hospital readmission for recurrent sepsis: associated risk factors and impact on 1-year mortality—a French nationwide study. Crit Care 26, 371 (2022). https://doi.org/10.1186/s13054-022-04212-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-022-04212-9