
Abstract
Background
There is significant controversy regarding the influence of video laryngoscopy on the intubation outcomes in emergency and critical patients. This systematic review and meta-analysis was designed to determine whether video laryngoscopy could improve the intubation outcomes in emergency and critical patients.
Methods
We searched the Cochrane Central Register of Controlled Trials, PubMed, Embase, and Scopus databases from database inception until 15 February 2017. Only randomized controlled trials comparing video and direct laryngoscopy for tracheal intubation in emergency department, intensive care unit, and prehospital settings were selected. The primary outcome was the first-attempt success rate. Review Manager 5.3 software was used to perform the pooled analysis and assess the risk of bias for each eligible study. The GRADE (Grading of Recommendations Assessment, Development and Evaluation) system was used to assess the quality of evidence for all outcomes.
Results
Twelve studies (2583 patients) were included in the review for data extraction. Pooled analysis did not show an improved first-attempt success rate using video laryngoscopy (relative risk [RR], 0.93; P = 0.28; low-quality evidence). There was significant heterogeneity among studies (I 2 = 91%). Subgroup analyses showed that, in the prehospital setting, video laryngoscopy decreased the first-attempt success rate (RR, 0.57; P < 0.01; high-quality evidence) and overall success rate (RR, 0.58; 95% CI, 0.48–0.69; moderate-quality evidence) by experienced operators, whereas in the in-hospital setting, no significant difference between two devices was identified for the first-attempt success rate (RR, 1.06; P = 0.14; moderate-quality evidence), regardless of the experience of the operators or the types of video laryngoscopes used (P > 0.05), although a slightly higher overall success rate was shown (RR, 1.11; P = 0.03; moderate-quality evidence). There were no differences between devices for other outcomes (P > 0.05), except for a lower rate of esophageal intubation (P = 0.01) and a higher rate of Cormack and Lehane grade 1 (P < 0.01) when using video laryngoscopy.
Conclusions
On the basis of the results of this study, we conclude that, compared with direct laryngoscopy, video laryngoscopy does not improve intubation outcomes in emergency and critical patients. Prehospital intubation is even worsened by use of video laryngoscopy when performed by experienced operators.
Similar content being viewed by others


Background
Securing the airway with tracheal intubation (TI) is a fundamental treatment for emergency and critical care patients with respiratory dysfunction or decreased airway protection. Direct laryngoscopy (DL) is the primary method for TI, but it can be challenging when performed in emergencies because the patient often is in life-threatening condition and has the factors that make TI difficult, such as limited mouth opening, unstable cervical spine, blood or secretions in the airway, and facial trauma, and in addition the expertise of available practitioners varies [1, 2]. The first-attempt success rate of urgent TI in emergency and critical patients is relatively low [2,3,4,5], and unsuccessful or prolonged TI can be life-threatening and may result in severe complications [6,7,8,9,10,11].
Video laryngoscopy (VL) is a new device that contains a miniaturized camera at the blade tip to visualize the glottis indirectly. This method was developed at the beginning of the 21st century [12]. It has been shown that VL improves laryngeal visualization compared with DL [13, 14] and provides some advantages in surgical patients, especially those with difficult airways [15,16,17,18,19]. The use of VL in emergent and critical situations has also been tested in several observational studies, which have shown that VL can lead to better intubation outcomes [4, 5, 20, 21]. A recent meta-analysis of intensive care unit (ICU) patients demonstrated that, compared with DL, VL reduces difficult intubation and increases the first-attempt success rate [22]. Of the nine studies included in that meta-analysis, however, only three (n = 157 subjects) were randomized controlled trials (RCTs) [23,24,25]. An observational study, whether prospective, nonrandomized, or retrospective in design, does not control for the operators’ experience with each device or for patients’ conditions and thus may bias the determination of the efficacy of different airway devices.
Recently, the performance of VL and DL in patients needing emergency TI was compared in several RCTs, and some of them showed no benefit regarding success rate or intubation time with VL [24, 26,27,28,29,30,31,32]. In view of this, we performed a systematic review and meta-analysis that included only RCTs comparing the performance of VL and DL for emergency TI with respect to the intubation outcomes and complications. Our review is registered with PROSPERO (http://www.crd.york.ac.uk/PROSPERO, CRD42017054804).
Methods
Data sources
The Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Embase, and Scopus databases were searched from inception of the databases until 15 February 2017. The PubMed search strategy provided in Additional file 1 was applied to search other electronic databases. For literature without full text, the corresponding author of the study was contacted by email. The reference lists of all eligible trials and reviews were screened for additional citations. No language restriction was imposed.
Study selection
RCTs or quasi-RCTs comparing VL and DL for TI in emergency or critical care patients were included. Manikin studies, cadaveric studies, and retrospective or observational studies were excluded. Participants were nonsurgical patients needing emergent TI in the in-hospital or prehospital setting. Patients with suspected laryngeal trauma or extensive maxillofacial injury requiring an immediate surgical airway, supraglottic airway, or awake fiberoptic intubation were excluded. The primary outcome was the first-attempt success rate. The secondary outcomes were overall success rate; duration of intubation; and complications, including esophageal intubation, aspiration, severe low oxygen saturation, and in-hospital mortality. The rate of Cormack and Lehane grade 1 classification was also recorded. The definitions of the outcomes are shown in Additional file 2: Table S1.
The titles and abstracts were independently screened by two of the present review’s authors (JJ and DM). After retrieving the full texts of any potentially relevant studies, the studies’ eligibility was determined. Any disagreements between the two review authors were resolved by discussion with the other authors until a consensus was obtained. A Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flow diagram was completed to record the selection process in sufficient detail [33].
Data extraction and risk of bias assessment
The data were independently extracted by two review authors (JJ and DM). For continuous data, mean, SD, and sample size were extracted. Data such as median or CI that cannot be used directly were converted to SD by using a formula provided in the Cochrane Handbook [34]. For dichotomous variables, the number of events that had occurred and the sample size were extracted. The corresponding author of the study was contacted if the data were unavailable.
The risk of bias for each eligible study was independently assessed by two review authors (JJ and DM) using the “risk of bias” assessment tool of the Cochrane Handbook [34]. If all seven domains were assigned a low risk of bias, the study was classified as “low risk”; if one or more domains were assigned to the “unclear risk” of bias category, the study was classified as “unclear risk”; if one or more domains were assigned to a high risk of bias, the study was classified as “high risk” [34]. Furthermore, the criteria of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system (study limitations, consistency of effect, imprecision, indirectness, and publication bias) were used to assess the quality of the body of evidence associated with all outcomes [35, 36]. Then we developed a grade evidence profile table using the GRADE software (www.guidelinedevelopment.org) to rate these outcomes as being of high, moderate, low, or very low quality. If serious or very serious deficiencies in these criteria were considered, the quality of evidence was downgraded by one or two levels.
Data analysis
The weighted mean difference (WMD) and 95% CI were used for continuous data. Relative risk (RR) and 95% CI were used for dichotomous data. A P value less than 0.05 was considered statistically significant. RevMan 5.3 software (Cochrane Collaboration, London, UK) was used to perform the pooled analysis for the outcomes from more than one study. A chi-square test with the I 2 statistic was used to quantify heterogeneity. An I 2 value less than 40% was considered as low heterogeneity, and a fixed-effect model was used; otherwise, a random-effect model was used. In the presence of statistical heterogeneity (I 2 ≥ 40%) or an indication of clinical heterogeneity, subgroup analysis was planned for the primary outcomes according to the following possible heterogeneous factors: (a) different settings: in-hospital (ICU and emergency room) and prehospital; (b) operators’ experience: experienced (certified anesthesiologist, emergency medical service technician with more than 3 years of clinical experience, performed > 50 TIs, or according to the judgment of the study authors) or inexperienced; and (c) different devices: channeled, Macintosh and angulated VLs. Sensitivity analysis was conducted to explore other potential sources of heterogeneity if necessary. Reporting bias was assessed using funnel plots if the result of the primary outcome was derived from at least ten trials [37].
Results
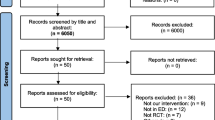
Using our search strategy, a total of 1380 papers were identified. Of them, 1313 were excluded during title and abstract screening because they were duplicates or irrelevant to our research question. Sixty-seven studies were selected for full-text assessment using our inclusion and exclusion criteria. Fifty-two further studies were removed because of having non-RCT characteristics, lacking relevant data, including surgical participants, and/or being duplicates. Authors of three studies were contacted for their full-text articles to confirm their eligibility: One [38] proved to be a meeting report that was part of another included study [24]; one was an observational study [39]; and another was qualified, but its full text could not be obtained to do the risk of bias assessment [40]. Thus, all three of these studies were excluded. One study author was contacted for additional data [41]. Eventually, 12 studies (n = 2583) were included in the review for data extraction [23,24,25,26,27,28,29,30,31,32, 41, 42]. The study selection process is shown in Fig. 1.

Search process for identified records. RCT Randomized controlled trial
Description of included studies
Characteristics of included studies are listed in Table 1. Among 12 included studies, 10 were RCTs, and the remainder were quasi-RCTs; 3 were carried out in the prehospital setting and 9 in the ICU or emergency department (in-hospital setting). Most intubations in seven studies were performed by experienced operators, and five were performed mostly by inexperienced operators. The angulated VL (GlideScope; Verathon, Seattle, WA, USA) was used in six studies, the Macintosh-type VL in four (C-MAC, Karl Storz, Tuttlingen, Germany; or McGrath MAC, Aircraft Medical, Edinburgh, Scotland), and the channeled VL in two (Pentax Airway Scope, Pentax Lifecare/Hoya, Tokyo, Japan; or Airtraq, Prodol Meditec, Las Arenas, Spain). Five in-hospital studies excluded patients with cardiac arrest, and one enrolled only patients with cardiac arrest. Rapid sequence induction (RSI) with sedatives or narcotics and neuromuscular blockades (NMBAs) were chosen for all participants or as appropriate by choice of physicians in most included studies. Three studies did not use any NMBAs [24, 26, 29].
The overall risk of bias of the included studies was relatively low. Eight of them could be classified as low-risk studies and three as high-risk studies. Detailed information regarding the risk of bias of the included studies is shown Fig. 2 and summarized in Additional file 3: Table S2. A funnel plot obtained from the primary outcome is shown in Additional file 4: Figure S1. The GRADE system showed that the quality of most evidence was low or moderate for inconsistency owing to a moderate or high level of heterogeneity. The results of the evidence of outcomes are listed in Additional file 5: Table S3.

Risk of bias summary: judgments about each risk of bias item for each included study based on quality evaluation of 12 included studies. + Low risk, − High risk, ? Unknown
First-attempt success rate
The data on the first-attempt success rate for all 12 included studies were available. Pooled analysis showed no significant difference in the first-attempt success rate between VL and DL (12 studies; RR, 0.93; 95% CI, 0.82–1.06; n = 2583; P = 0.28; low-quality evidence). There was significant heterogeneity among studies (P < 0.01; I 2 = 91%) (Additional file 6: Figure S2).
Subgroup analysis according to different settings identified a significant difference for the prehospital setting (three studies; RR, 0.57; n = 647; P < 0.01; high-quality evidence) but no significant difference for the in-hospital setting (nine studies; RR, 1.06; n = 1936; P = 0.14; moderate-quality evidence). Prehospital intubation was performed mostly by experienced operators, and two kinds of VLs (channeled [26, 41] or angulated [32] VLs) were used. Given that different settings would introduce principal heterogeneity and only three studies in the prehospital setting were included, subgroup analyses based on the experience of operators and different devices used were performed only in the in-hospital setting. No significant difference was found when TI was performed by experienced operators (four studies; RR, 1.03; n = 1108; P = 0.37) or by inexperienced operators (six studies with seven comparisons; RR, 1.16; n = 924; P = 0.05). No significant difference was found for intubation with angulated VLs (GlideScope; five studies with six comparisons; RR, 1.16; n = 1016; P = 0.04) or with Macintosh-type VLs (C-MAC/McGrath MAC; five studies; RR, 1.03; n = 1016; P = 0.43) (Fig. 3). The study by Silverberg et al. [24] had a much higher first-attempt success rate when using VL than that in other studies, and it was the only study performed in non-cardiopulmonary resuscitation (non-CPR) patients without using any NMBAs. Thus, a sensitivity analysis excluding this study in the in-hospital setting was conducted. The results were not altered; however, no evidence of heterogeneity could be found in all subgroups that originally included this study (I 2 < 40%).

VL vs. DL for first-attempt success rate based on different settings (a), experience levels of operators in in-hospital settings (b), and different types of video laryngoscopy in in-hospital settings (c). VL Video laryngoscopy, DL Direct laryngoscopy, M-H Mantel-Haenszel
Secondary outcomes
Results of secondary outcomes, including overall success rate, duration of intubation, esophageal intubation rate, in-hospital mortality, aspiration, severe low oxygen saturation, and Cormack and Lehane grade 1 classification, are summarized in Table 2 and Additional file 7: Figure S3, S4, S5, and S6.
Discussion
To our knowledge, this is the first meta-analysis and systematic review of available RCTs comparing VL and DL for TI in emergency and critical care patients, including the quality of evidence. In this analysis, the first-attempt success rate was used as the primary endpoint because multiple intubation attempts performed outside the operating room can significantly increase the risk of life-threatening complications [6, 43, 44]. Furthermore, improving the first-attempt success rate has been regarded as the main goal of emergency TI [45]. Our results show that laryngeal visualization was improved by using VL. This is consistent with findings for surgical patients in the operating room [12]. However, better visualization did not translate into an improved first-attempt success rate or other intubation outcomes or complications, except for a lower rate of esophageal intubation. Prehospital intubation outcomes were even worsened with lower first-attempt and overall success rates with VL when TI was performed by experienced operators.
Evidence derived from surgical patients shows that VL is associated with better intubation outcomes, especially for inexperienced operators and patients with difficult airways [16, 28, 46]. This is because TI in the operating room is controllable, such as with the common use of RSI and NMBAs, patients’ fasting state, and favorable oxygenation, as well as appropriate light or intubation position. For highly experienced anesthesiologists, it seems unlikely that a single device will show superiority unless a difficult airway is encountered [47,48,49,50,51], whereas for novices who have not yet received long-term DL training, visualization of the airway on a video screen can allow their supervisors to directly assist them in completing an intubation themselves, thus reducing the number of attempts and improving the safety of airway management [52]. However, emergent TI is quite another thing. Although TI in the emergency department or ICU is frequently performed by paramedics or emergency medicine physicians who do not practice TI with DL on a daily basis [53], and although the patients often have a higher risk of difficult airways [9, 54], the operators may not benefit from using VL as novices in the operating room. There are several uncontrollable factors that may explain this difference. First, critically ill patients with a poor oxygen reserve capacity are more subject to hypoxia, which makes it more likely that operators will turn to alternatives such as DL, a flexible or rigid bronchoscope, or at least further mask oxygenation. If TI is not completed within the allowed time, inexperienced operators will be replaced by more experienced operators earlier, making the first-attempt success rate much lower. Second, secretions or blood in the airway might impair laryngeal visualization with VLs [26, 28]. Third, RSI and NMBAs will be chosen with caution owing to circulation compromise, certain airway problems, operators’ experience, or accessibility of medicine. Prehospital intubation is more challenging, owing to additional risk factors such as ambient light, limited workspace, special positioning, and chest compression during CPR [55]. Under chest compression, increased intrathoracic pressure can cause reflux of gastric contents, resulting in more attempts and longer intubation time with the VL. Prolonged intubation time and subsequent hypoxemia have been identified as major reasons for increased mortality in patients undergoing prehospital intubation [56]. In addition, in prehospital care, DL is more accessible, and most operators are experienced in using it.
It must be emphasized that performance of VL is different between devices owing to various designs and shapes [57, 58]. Even a slight design modification may significantly change the success rate, intubation time, and use of adjunct maneuvers [59]. Some types of VLs have their own design-related deficiencies that may dwarf their results. For example, the A.P. Advance™ VL (Venner Medical International, St Helier, Jersey, UK), with a large video screen, shows the plastic part of the blade tip instead of the relevant airway, contributing to its poor performance [58]. Studies included in our analysis used three types of VLs (angulated, Macintosh, or channeled), including five different devices (GlideScope, C-MAC, McGrath MAC, Airwayscope, and Airtraq). In the prehospital setting, two of three included studies used channeled VL. The channeled VL, with its integrated design, might be more portable in the prehospital setting, but it is bulkier and may require other team members to maneuver the tracheal tube [58]. It should be noted that the poor performance of the VL is due mainly to the prehospital setting itself rather than to the devices chosen. We therefore did a related subgroup analysis only in the in-hospital setting. No difference was identified between VLs and DLs, regardless of the devices used. Although an angled blade design was assumed to facilitate laryngeal visualization and thus to lead to a better intubation outcome, it may afford less room for tracheal tube insertion and increase stylet use in patients with a normal airway, resulting in increased procedural difficulty and prolonged intubation time [25, 60]. In addition, pooling of results from studies evaluating different VLs may lead to intrinsic inconsistencies. An especially important issue neglected in the design of the five included studies comparing the Macintosh-type VL and DL is that the Macintosh-type VL can provide the two options of DL and VL in one device. When one attempt fails, the operators can immediately switch to another option to successfully complete the TI without having to make a second attempt [61]. This unique feature of Macintosh-type VLs is significantly different from DLs and angulated VLs, which can provide only one option. Thus, definition of laryngoscopy attempts used in these studies is desirable for DLs but not for Macintosh-type VLs [62].
The results of some studies indicate that VLs should be used with caution in critical patients because of a prolonged intubation time and subsequent possible higher incidence of severe life-threatening complications [23, 25, 30]. Our review shows that incidences of aspiration, severe low oxygen saturation, and in-hospital deaths did not differ between VLs and DLs. However, these results remain unreliable owing to the limited number of participants included. Our review shows a lower rate of esophageal intubation using VLs than that in another study [22]. This might be somewhat meaningful because “even a single episode of recognized esophageal intubation is associated with desaturation, increased risk of aspiration, and cardiac arrest” [63]. Moreover, an important and promising finding in one of our included studies and another observational study is that the use of a VL has a higher first-attempt success rate with fewer chest compression interruptions in the emergency department [29, 64].
Our study included only RCTs and quasi-RCTs. Although blinding was not adopted in most studies, we judged “no blinding” as low risk because it seems impossible to blind personnel in urgent situations at times. In the prehospital setting, moreover, there is never time for allocation concealment, and even randomization using a common method such as a random number table is impractical. Risk assessment of bias for the included studies showed that 7 of 12 studies could be classified as low-risk studies. Therefore, in general, this supports the quality of our study. The funnel plot, with its visually symmetrical distribution, qualitatively indicates a low risk of publication bias. Given that the quality of most evidence was low or moderate owing to a moderate or high level of heterogeneity, subgroup analysis and sensitivity analysis based on some potential clinical heterogeneous factors also were performed in our review.
There are some limitations of our review. First, although subgroup analyses were performed, there were still other clinical heterogeneities in subgroups, such as patients having different conditions, use of various intubation strategies, and use of any adjacent tool or maneuver. Whether patients with predicted difficult airways were enrolled was another important heterogeneous factor. However, for emergency or critical care patients, the traditional predictors of difficult airways, such as thyromental distance, Mallampati score, or neck mobility, cannot be recorded, because all intubations are performed so urgently that there is never a chance to make predictions or subsequent grouping before randomization. One observational study showed that VLs significantly increased the intubation success rate in emergency patients with difficult airways [65]. In the absence of a difficult airway, however, the use of VLs may even bring some disadvantages [25]. Whether anesthetics were used and the choice of medication can also introduce heterogeneity. RSI with sedatives, narcotics, and NMBAs has been shown to facilitate TI and decrease intubation-related complications in reasonable circumstances [66, 67]. Because most of the studies included in our review did not have strict protocols regarding medication, subgroup analysis according to medications seemed impossible. Anyway, the study by Silverberg et al. [24] demonstrated a much higher first-attempt success rate using VLs. Sensitivity analysis excluding this study did not alter the results, but the heterogeneities within the subgroups disappeared, indicating that this study may be the main factor leading to heterogeneity. The effect of the NMBAs on the result was unclear. It may be the negative influence of alternating of devices that use different configurations on the learning curve of operators with the DLs that led to a lower success rate with DLs. Second, owing to ethical considerations, some patients had to be excluded on enrollment, such as patients with low oxygen saturation [24], those with an immobilized cervical spine, and patients with predicted difficult airways, or those excluded owing to attending physicians’ discretion and unavailability of devices at the time of eligible patient arrival [25]. It is unclear whether these excluded patients would benefit from one of the interventions. Third, the classification of the operators’ qualifications and the definition of intubation time or overall success rate used in our analysis were based on previous papers or our own judgment, and this might somehow be arbitrary.
Conclusions
This review does not reveal any improvements in intubation outcomes with the use of VLs compared with DLs in emergency and critical care patients, except for a lower rate of esophageal intubation with VLs. In the prehospital setting, intubation outcomes may be worsened by the VL when intubation is performed by experienced operators. Further studies are still needed to determine whether the VL is beneficial for emergency and critical care patients with difficult airways, regardless of the operator’s experience, and should be focused more on the impact of VLs on prognostic outcomes such as severe complications, length of hospital stay, and mortality.
Abbreviations
- C&L:
-
Cormack and Lehane
- CENTRAL:
-
Cochrane Central Register of Controlled Trials
- CPR:
-
Cardiopulmonary resuscitation
- DL:
-
Direct laryngoscopy
- ED:
-
Emergency department
- EMS:
-
Emergency medical service
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- ICU:
-
Intensive care unit
- IV:
-
Inverse variation
- M-H:
-
Mantel-Haenszel
- NMBA:
-
Neuromuscular blockade
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis
- RCT:
-
Randomized controlled trial
- RR:
-
Relative risk
- RSI:
-
Rapid sequence induction
- SpO2 :
-
Oxygen saturation by pulse oximetry
- TI:
-
Tracheal intubation
- VL:
-
Video laryngoscopy
- WMD:
-
Weighted mean difference
References
Agro F, Barzoi G, Montecchia F. Tracheal intubation using a Macintosh laryngoscope or a GlideScope in 15 patients with cervical spine immobilization. Br J Anaesth. 2003;90:705–6.
Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam JJ. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34:2355–61.
Healy DW, Maties O, Hovord D, Kheterpal S. A systematic review of the role of videolaryngoscopy in successful orotracheal intubation. BMC Anesthesiol. 2012;12:32.
Kory P, Guevarra K, Mathew JP, Hegde A, Mayo PH. The impact of video laryngoscopy use during urgent endotracheal intubation in the critically ill. Anesth Analg. 2013;117:144–9.
Lakticova V, Koenig SJ, Narasimhan M, Mayo PH. Video laryngoscopy is associated with increased first pass success and decreased rate of esophageal intubations during urgent endotracheal intubation in a medical intensive care unit when compared to direct laryngoscopy. J Intensive Care Med. 2015;30:44–8.
Cook TM, Woodall N, Harper J, Benger J. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011;106:632–42.
De Jong A, Molinari N, Terzi N, Mongardon N, Arnal JM, Guitton C, Allaouchiche B, Paugam-Burtz C, Constantin JM, Lefrant JY, Leone M, Papazian L, Asehnoune K, Maziers N, Azoulay E, Pradel G, Jung B, Jaber S. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187:832–9.
Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, O’Sullivan EP, Woodall NM, Ahmad I. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015;115:827–48.
Griesdale DE, Bosma TL, Kurth T, Isac G, Chittock DR. Complications of endotracheal intubation in the critically ill. Intensive Care Med. 2008;34:1835–42.
Martin LD, Mhyre JM, Shanks AM, Tremper KK, Kheterpal S. 3,423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology. 2011;114:42–8.
Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults: a prospective investigation of 297 tracheal intubations. Anesthesiology. 1995;82:367–76.
Nouruzi-Sedeh P, Schumann M, Groeben H. Laryngoscopy via Macintosh blade versus GlideScope: success rate and time for endotracheal intubation in untrained medical personnel. Anesthesiology. 2009;110:32–7.
Parasa M, Yallapragada SV, Vemuri NN, Shaik MS. Comparison of GlideScope video laryngoscope with Macintosh laryngoscope in adult patients undergoing elective surgical procedures. Anesth Essays Res. 2016;10:245–9.
Sun Y, Lu Y, Huang Y, Jiang H. Pediatric video laryngoscope versus direct laryngoscope: a meta-analysis of randomized controlled trials. Paediatr Anaesth. 2014;24:1056–65.
Aziz MF, Dillman D, Fu R, Brambrink AM. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology. 2012;116:629–36.
Griesdale DEG, Liu D, McKinney J, Choi PT. GlideScope® video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Can J Anaesth. 2012;59:41–52.
Kelly FE, Cook TM. Seeing is believing: getting the best out of videolaryngoscopy. Br J Anaesth. 2016;117 Suppl 1:i9–13.
Niforopoulou P, Pantazopoulos I, Demestiha T, Koudouna E, Xanthos T. Video-laryngoscopes in the adult airway management: a topical review of the literature. Acta Anaesthesiol Scand. 2010;54:1050–61.
Zaouter C, Calderon J, Hemmerling TM. Videolaryngoscopy as a new standard of care. Br J Anaesth. 2015;114:181–3.
Mosier JM, Whitmore SP, Bloom JW, Snyder LS, Graham LA, Carr GE, Sakles JC. Video laryngoscopy improves intubation success and reduces esophageal intubations compared to direct laryngoscopy in the medical intensive care unit. Crit Care. 2013;17:R237.
Noppens RR, Geimer S, Eisel N, David M, Piepho T. Endotracheal intubation using the C-MAC® video laryngoscope or the Macintosh laryngoscope: a prospective, comparative study in the ICU. Crit Care. 2012;16:R103.
De Jong A, Molinari N, Conseil M, Coisel Y, Pouzeratte Y, Belafia F, Jung B, Chanques G, Jaber S. Video laryngoscopy versus direct laryngoscopy for orotracheal intubation in the intensive care unit: a systematic review and meta-analysis. Intensive Care Med. 2014;40:629–39.
Griesdale DE, Chau A, Isac G, Ayas N, Foster D, Irwin C, Choi P. Video-laryngoscopy versus direct laryngoscopy in critically ill patients: a pilot randomized trial. Can J Anaesth. 2012;59:1032–9.
Silverberg MJ, Li N, Acquah SO, Kory PD. Comparison of video laryngoscopy versus direct laryngoscopy during urgent endotracheal intubation: a randomized controlled trial. Crit Care Med. 2015;43:636–41.
Yeatts DJ, Dutton RP, Hu PF, Chang YW, Brown CH, Chen H, Grissom TE, Kufera JA, Scalea TM. Effect of video laryngoscopy on trauma patient survival: a randomized controlled trial. J Trauma Acute Care Surg. 2013;75:212–9.
Arima T, Nagata O, Miura T, Ikeda K, Mizushima T, Takahashi A, Sakaida K. Comparative analysis of airway scope and Macintosh laryngoscope for intubation primarily for cardiac arrest in prehospital setting. Am J Emerg Med. 2014;32:40–3.
Goksu E, Kilic T, Yildiz G, Unal A, Kartal M. Comparison of the C-MAC video laryngoscope to the Macintosh laryngoscope for intubation of blunt trauma patients in the ED. Turk J Emerg Med. 2016;16:53–6.
Janz DR, Semler MW, Lentz RJ, Matthews DT, Assad TR, Norman BC, Keriwala RD, Ferrell BA, Noto MJ, Shaver CM, Richmond BW, Zinggeler Berg J, Rice TW. Randomized trial of video laryngoscopy for endotracheal intubation of critically ill adults. Crit Care Med. 2016;44:1980–7.
Kim JW, Park SO, Lee KR, Hong DY, Baek KJ, Lee YH, Lee JH, Choi PC. Video laryngoscopy vs. direct laryngoscopy: which should be chosen for endotracheal intubation during cardiopulmonary resuscitation? A prospective randomized controlled study of experienced intubators. Resuscitation. 2016;105:196–202.
Lascarrou JB, Boisrame-Helms J, Bailly A, Le Thuaut A, Kamel T, Mercier E, Ricard JD, Lemiale V, Colin G, Mira JP, Meziani F, Messika J, Dequin PF, Boulain T, Azoulay E, Champigneulle B, Reignier J. Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among ICU patients: a randomized clinical trial. JAMA. 2017;317:483–93.
Sulser S, Ubmann D, Schlaepfer M, Brueesch M, Goliasch G, Seifert B, Spahn DR, Ruetzler K. C-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department: a randomised clinical trial. Eur J Anaesthesiol. 2016;33:943–8.
Trimmel H, Kreutziger J, Fitzka R, Szuts S, Derdak C, Koch E, Erwied B, Voelckel WG. Use of the GlideScope Ranger video laryngoscope for emergency intubation in the prehospital setting: a randomized control trial. Crit Care Med. 2016;44:e470–6.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647.
Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions. Version 5.1 [updated March 2011]. The Cochrane Collaboration. http://handbook-5-1.cochrane.org/. Accessed 15 Jun 2015.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S, Falck-Ytter Y, Glasziou P, DeBeer H, Jaeschke R, Rind D, Meerpohl J, Dahm P, Schunemann HJ. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–94.
Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schunemann HJ. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;336:995–8.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34.
Silverberg M, Li N, Kory P. Efficacy of video laryngoscopy vs. direct laryngoscopy during urgent endotracheal intubation: a randomized controlled trial [abstract]. Chest. 2013;144(4 Suppl):580A.
Sakles J, Mosier J, Cosentino M, Kalin L. The CMAC videolaryngoscope for difficult airway management in the emergency department [abstract 433]. Acad Emerg Med. 2012;19(4 Suppl 1):S232.
Miner JR, Moore J, Rischall M, Beste R, Maddy N, Joing S, McGill JW, Biros MH, Reardon RF. Randomized controlled trial of endotracheal intubation using the C-MAC videolaryngoscope versus standard laryngoscopy in patients undergoing emergent endotracheal intubation in the emergency department [abstract 428]. Acad Emerg Med. 2012;19(4 Suppl 1):S229.
Trimmel H, Kreutziger J, Fertsak G, Fitzka R, Dittrich M, Voelckel WG. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: a randomized control trial. Crit Care Med. 2011;39:489–93.
Driver BE, Prekker ME, Moore JC, Schick AL, Reardon RF, Miner JR. Direct versus video laryngoscopy using the C-MAC for tracheal intubation in the emergency department, a randomized controlled trial. Acad Emerg Med. 2016;23:433–9.
Bowles TM, Freshwater-Turner DA, Janssen DJ, Peden CJ. Out-of-theatre tracheal intubation: prospective multicentre study of clinical practice and adverse events. Br J Anaesth. 2011;107:687–92.
Simpson GD, Ross MJ, McKeown DW, Ray DC. Tracheal intubation in the critically ill: a multi-centre national study of practice and complications. Br J Anaesth. 2012;108:792–9.
Natt BS, Malo J, Hypes CD, Sakles JC, Mosier JM. Strategies to improve first attempt success at intubation in critically ill patients. Br J Anaesth. 2016;117 Suppl 1:i60–8.
Agro FE, Doyle DJ, Vennari M. Use of GlideScope® in adults: an overview. Minerva Anestesiol. 2015;81:342–51.
Jungbauer A, Schumann M, Brunkhorst V, Borgers A, Groeben H. Expected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients. Br J Anaesth. 2009;102:546–50.
Komasawa N, Ueki R, Nomura H, Itani M, Kaminoh Y. Comparison of tracheal intubation by the Macintosh laryngoscope and Pentax-AWS (Airway Scope) during chest compression: a manikin study. J Anesth. 2010;24:306–8.
Malik MA, Subramaniam R, Churasia S, Maharaj CH, Harte BH, Laffey JG. Tracheal intubation in patients with cervical spine immobilization: a comparison of the Airwayscope, LMA CTrach, and the Macintosh laryngoscopes. Br J Anaesth. 2009;102:654–61.
Malik MA, Subramaniam R, Maharaj CH, Harte BH, Laffey JG. Randomized controlled trial of the Pentax AWS, GlideScope, and Macintosh laryngoscopes in predicted difficult intubation. Br J Anaesth. 2009;103:761–8.
Marrel J, Blanc C, Frascarolo P, Magnusson L. Videolaryngoscopy improves intubation condition in morbidly obese patients. Eur J Anaesthesiol. 2007;24:1045–9.
Paolini JB, Donati F, Drolet P. Review article: video-laryngoscopy: another tool for difficult intubation or a new paradigm in airway management? Can J Anaesth. 2013;60:184–91.
Timmermann A, Eich C, Russo SG, Natge U, Brauer A, Rosenblatt WH, Braun U. Prehospital airway management: a prospective evaluation of anaesthesia trained emergency physicians. Resuscitation. 2006;70:179–85.
Platts-Mills TF, Campagne D, Chinnock B, Snowden B, Glickman LT, Hendey GW. A comparison of GlideScope video laryngoscopy versus direct laryngoscopy intubation in the emergency department. Acad Emerg Med. 2009;16:866–71.
Wang HE, Simeone SJ, Weaver MD, Callaway CW. Interruptions in cardiopulmonary resuscitation from paramedic endotracheal intubation. Ann Emerg Med. 2009;54:645–52.
Davis DP, Dunford JV, Poste JC, Ochs M, Holbrook T, Fortlage D, Size MJ, Kennedy F, Hoyt DB. The impact of hypoxia and hyperventilation on outcome after paramedic rapid sequence intubation of severely head-injured patients. J Trauma. 2004;57:1–10.
Kleine-Brueggeney M, Buttenberg M, Greif R, Nabecker S, Theiler L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: a randomised, controlled trial. Anaesthesia. 2017;72:370–8.
Kleine-Brueggeney M, Greif R, Schoettker P, Savoldelli GL, Nabecker S, Theiler LG. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br J Anaesth. 2016;116:670–9.
Sakles JC, Patanwala AE, Mosier J, Dicken J, Holman N. Comparison of the reusable standard GlideScope® video laryngoscope and the disposable cobalt GlideScope® video laryngoscope for tracheal intubation in an academic emergency department: a retrospective review. Acad Emerg Med. 2014;21:408–15.
van Zundert A, Pieters B, Doerges V, Gatt S. Videolaryngoscopy allows a better view of the pharynx and larynx than classic laryngoscopy. Br J Anaesth. 2012;109:1014–5.
Sakles JC, Mosier JM, Patanwala AE, Arcaris B, Dicken JM. The utility of the C-MAC as a direct laryngoscope for intubation in the emergency department. J Emerg Med. 2016;51:349–57.
Xue FS, Li HX, Liu YY, Yang GZ. Current evidence for the use of C-MAC videolaryngoscope in adult airway management: a review of the literature. Ther Clin Risk Manag. 2017;13:831–41.
Mort TC. Esophageal intubation with indirect clinical tests during emergency tracheal intubation: a report on patient morbidity. J Clin Anesth. 2005;17:255–62.
Park SO, Baek KJ, Hong DY, Kim SC, Lee KR. Feasibility of the video-laryngoscope (GlideScope®) for endotracheal intubation during uninterrupted chest compressions in actual advanced life support: a clinical observational study in an urban emergency department. Resuscitation. 2013;84:1233–7.
Ahmadi K, Ebrahimi M, Hashemian AM, Sarshar S, Rahimi-Movaghar V. GlideScope video laryngoscope for difficult intubation in emergency patients: a quasi-randomized controlled trial. Acta Med Iran. 2015;53:738–42.
Lossius HM, Roislien J, Lockey DJ. Patient safety in pre-hospital emergency tracheal intubation: a comprehensive meta-analysis of the intubation success rates of EMS providers. Crit Care. 2012;16:R24.
Wilcox SR, Bittner EA, Elmer J, Seigel TA, Nguyen NT, Dhillon A, Eikermann M, Schmidt U. Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012;40:1808–13.
Acknowledgements
The authors acknowledge the Cochrane Collaboration for guidance on implementing this review. The authors acknowledge Professor J. Salkes, Professor M. Silverberg, Professor E. Goksu, Professor H. Trimmel, and Professor D. E. Griesdale for providing additional information.
Funding
There was no special funding support provided for this work.
Availability of data and materials
JJ and FX had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Contributions
JJ and DM significantly contributed to the design and implementation of the study, as well as analysis and interpretation, and they drafted the manuscript. BL participated substantially in data acquisition and interpretation. YY contributed considerably to the conception and design of the study, supervised implementation of the study, performed data analysis and interpretation, and wrote and critically revised the manuscript. FX significantly contributed to the conception of the study, performed data analysis and interpretation, and critically revised the manuscript. All authors saw the original study data, reviewed the analysis of the data, and read and approved the final manuscript.
Corresponding authors
Ethics declarations
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare (1) receiving no support from any organization for the submitted work, (2) having no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years, and (3) having no other relationships or activities that could appear to have influenced the submitted work.
Publisher’s Note
Springer Nature remains neutral regarding jurisdictional claims in published maps and institutional affiliations
Additional files
Additional file 1:
The PubMed search strategy. (DOC 23 kb)
Additional file 2: Table S1.
Definitions of some outcomes. (DOC 28 kb)
Additional file 3: Table S2.
Description of the risk of bias for 12 included studies. (DOC 88 kb)
Additional file 4: Figure S1.
Funnel plot of comparison for the primary outcome: first-attempt success rate. (DOC 32 kb)
Additional file 5: Table S3.
GRADE evidence profile of all outcomes. (DOC 94 kb)
Additional file 6: Figure S2.
VL vs. DL for first-attempt success rate. Abbreviations: VL Video laryngoscope, DL Direct laryngoscope. (DOC 35 kb)
Additional file 7:
Figures S3, S4, S5, and S6 VL vs. DL for overall success rate. Abbreviations: VL Video laryngoscope, DL Direct laryngoscope. (DOC 97 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jiang, J., Ma, D., Li, B. et al. Video laryngoscopy does not improve the intubation outcomes in emergency and critical patients – a systematic review and meta-analysis of randomized controlled trials. Crit Care 21, 288 (2017). https://doi.org/10.1186/s13054-017-1885-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-017-1885-9