
Abstract
Background
The utilization of video laryngoscopy (VL) has demonstrated superiority over direct laryngoscopy (DL) for intubation in surgical settings. However, its effectiveness in the intensive care unit and emergency department settings remains uncertain.
Methods
We systematically searched PubMed, Embase, Cochrane, and ClinicalTrials.gov databases for randomized controlled trials (RCTs) comparing VL versus DL in critically ill patients. Critical setting was defined as emergency department and intensive care unit. This systematic review and meta-analysis followed Cochrane and PRISMA recommendations. R version 4.3.1 was used for statistical analysis and heterogeneity was examined with I2 statistics. All outcomes were submitted to random-effect models.
Results
Our meta-analysis of 14 RCTs, compromising 3981 patients assigned to VL (n = 2002) or DL (n = 1979). Compared with DL, VL significantly increased successful intubations on the first attempt (RR 1.12; 95% CI 1.04–1.20; p < 0.01; I2 = 82%). Regarding adverse events, VL reduced the number of esophageal intubations (RR 0.44; 95% CI 0.24–0.80; p < 0.01; I2 = 0%) and incidence of aspiration episodes (RR 0.63; 95% CI 0.41–0.96; p = 0.03; I2 = 0%) compared to DL.
Conclusion
VL is a more effective and safer strategy compared with DL for increasing successful intubations on the first attempt and reducing esophageal intubations in critically ill patients. Our findings support the routine use of VL in critically ill patients.
Registration CRD42023439685 https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023439685. Registered 6 July 2023.
Similar content being viewed by others


Background
Tracheal intubation plays a crucial role in the management of critically ill patients’ airways. Approximately, 1.6 millions of patients undergo orotracheal intubations yearly in the US [1]. The number of direct laryngoscopy attempts during intubation has been associated with poor outcomes, including airway complications and hemodynamic instability [2]. Notably, initial intubation attempts fail in approximately 20% in emergency department (ED) and intensive care unit (ICU). [3,4,5,6]
The video laryngoscope (VL) has emerged as a promising alternative, offering enhanced visualization of airway structures. VL demonstrated superiority over the gold standard, direct laryngoscope (DL), in surgical scenarios [7]. Meanwhile, approximately 80% of the intubations performed in the ED and ICU worldwide are performed with a DL [2]. However, DL could be challenging due to several factors. These include limited mouth aperture and potential instability of cervical spine [8,9,10]. Despite this, there is an ongoing debate on the efficacy and safety of VL in critically ill patients [11, 12].
Previous meta-analyses showed no significant difference in successful intubation on the first attempt in critically ill patients [7, 13]. However, several randomized controlled trials (RCTs) have been published recently, including the Direct versus Video Laryngoscope (DEVICE) trial, the largest to date, showing promising results [12, 14, 15]. To shed light on this controversy, we performed an updated systematic review and meta-analysis of RCTs comparing VL versus DL in critically ill patients.
Methods
The systematic review and meta-analysis were performed and reported following the Cochrane Collaboration Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines (Additional file 1: Supplemental Methods 1, 2).[16, 17] The prospective meta-analysis protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO; CRD42023439685) on the 6 July 2023.
Data source and search strategy
We systematically searched PubMed, Embase, Cochrane Library, and ClinicalTrials.gov from inception to June 23, 2023. The search terms used included ‘video’, ‘intubation’, and ‘laryngoscope’. The complete search strategy is provided in Additional 1: Supplemental Methods 3. Two authors (B.A. and S.L.) independently screened titles and abstracts and evaluated the articles in full for eligibility based on prespecified criteria. Discrepancies were resolved in a panel discussion with a third author (A.R.). Moreover, we used backward snowballing (i.e., review of references) to identify relevant texts from articles identified in the original search.
Eligibility criteria
We considered studies eligible for inclusion if they (1) were RCTs; (2) directly compared VL versus DL; (3) enrolled critically ill patients (admitted to ED or ICU); (4) included adult patients; and (5) presented data regarding any of the prespecified efficacy and safety endpoints. The exclusion criteria were non-randomized studies, quasi-RCTs, cluster RCTs, studies that included patients younger than 16 years old or pregnant patients, studies centered on surgical scenarios, or conference abstracts.
Data extraction
Four authors (B.A., S.M., P.C., and M.S.) independently extracted the data for each study using a standardized study form to determine: authors, clinical trial registration, enrollment period, study publication year, main exclusion criteria (Additional file 1: Supplemental Methods 4), sample size, follow-up period, endpoint definition, baseline patient characteristics, and operator’s characteristics. Any discrepancies were settled through a panel discussion with a fifth author (A.R.).
The definition of operators' experiences slightly varied among studies. To allow subgroup analysis based on this characteristic, we classified operators into two groups, experienced and inexperienced, following specific criteria outlined in Additional file 1: Supplemental Methods 5. Moreover, the Additional file 1: Supplemental Methods 6 highlights how each study selected the device for the second intubation attempt. The classification of a difficult airway was made in accordance with either the study’s definition or the Mallampati 3/4 classification.
Endpoints
Our primary efficacy endpoint was (1) successful intubation on the first attempt, as defined by each individual study. Other efficacy endpoints were (2) successful intubation on the second attempt, (3) Cormack Lehane (CL) laryngeal view grade I, and (4) CL laryngeal view grade I/II. Safety endpoints were (5) incidence of aspiration, (6) esophageal intubation, (7) cardiac arrest, (8) severe hypoxemia, (9) dental injury, and (10) all-cause mortality. Additional file 1: Supplemental Methods 7 describes the endpoint definition of some outcomes.
We conducted prespecified subgroup analyses for the primary outcome. Studies were grouped based on the (1) VL brands and (2) operators’ experience. A sensitivity analysis of the subgroup analysis evaluating the operator’s experience was performed changing the threshold of from 50 to 100 prior intubations to be considered experienced. Subgroup analyses were performed if two or more studies were available in the group.
Quality assessment
Two independent authors (B.A. and R.A.) assessed the risk of bias in the included RCTs using Cochrane’s Collaboration tool for assessing the risk of bias in randomized trials (RoB 2) [18]. Any disagreements were resolved through consensus between authors. We explored the potential for publication bias by visual inspection of the comparison-adjusted funnel plots and Egger’s test for the primary endpoint.
Statistical analysis
We used the random-effects model for all outcomes. We employed risk ratios (RRs) and 95% confidence intervals (CIs) as the measure of effect size for binary endpoints. For continuous endpoints, we utilized weighted mean differences (MDs). Restricted maximum likelihood estimator was used to calculate heterogeneity variance t2. We assessed heterogeneity with Cochrane’s Q statistic and Higgins and Thompson’s I2 statistic, with p ≤ 0.10 indicating statistical significance. We determined the consistency of the studies based on I2 values of 0%, ≤ 25%, ≤ 50%, and > 50%, indicating no observed, low, moderate, and substantial heterogeneity, respectively. All tests were two-tailed, and a p value of < 0.05 was considered statistically significant. If necessary, means and standard deviations were estimated [19]. We conducted a trial sequential analysis (TSA) using random-effects model for the primary outcome, we used a statistical significance level of 5% and a beta of 80%. We used TSA version 0.9.5.10 beta (Copenhagen Trial Unit, Centre for Clinical Intervention Research, Rigshospitalet, Copenhagen, Denmark). We used R version 4.3.1 and the extension packages "meta," "metafor", "dmetar", "ggplot2", and "forestplot" for all calculations and graphics [20,21,22,23]. An in-depth description of the statistical analyses is available in Additional 1: Supplemental Methods 8.
Results
Study selection and characteristics
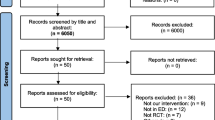
Our systematic search yielded 4278 potential articles (Fig. 1). After removing duplicates, 72 articles were retrieved and reviewed in full for possible inclusion. Of these, 14 RCTs met all inclusion criteria and were included in the primary analysis [11, 12, 14, 15, 24,25,26,27,28,29,30,31,32]. We included a total of 3981 patients, of whom 2002 (50.3%) patients were assigned to VL and 1979 (49.7%) were assigned to DL. The mean age of patients in individual studies ranged from 37 to 69 years, and the proportion of males was 63.7%. Table 1 summarizes the main characteristics of the included studies.

PRISMA flow diagram of study screening and selection. Abbreviations: RCT, randomized controlled trial
Efficacy endpoints
Compared with DL, VL significantly increased the number of successful intubations on the first attempt (RR 1.12; 95% CI 1.04–1.20; p < 0.01; I2 = 82%; Fig. 2A), the proportion of CL grade I (RR 1.73; 95% CI 1.41–2.12; p < 0.01; I2 = 71%; Fig. 2B), and grade I/II (RR 1.12; 95% CI 1.04–1.19; p < 0.01; I 2 = 91%; Additional 1: Supplemental Fig. 1). However, no statistically significant difference was observed between the groups in terms of success on the second attempt (RR 1.04; 95% CI 0.94–1.15; p = 0.49; I2 = 83%; Supplemental Fig. 2). Regarding TSA, the cumulative Z-curve crossed the required information size obtained with the 3032 subjects, indicating a low chance of type 1 error for successful intubation on the first attempt (Fig. 3).

Meta-analysis of the efficacy endpoints in critically ill patients undergoing intubation with VL. Caption: Forest plots presenting the risk ratio (RR) and 95% confidence interval (CI) for each strategy on A successful intubation on the first attempt and B Cormack Lehane (CL) Grade I. Abbreviations: CI, confidence interval; MH, Mantel–Haenszel; DL, direct laryngoscope; VL, video laryngoscope; RR, risk ratio; CL, Cormack Lehane

Trial sequential analysis of successful intubation on the first attempt with VL. Abbreviations: DL, direct laryngoscope; VL, video laryngoscope
Safety endpoints
VL substantially reduced the number of esophageal intubations (RR 0.44; 95% CI 0.24–0.80; p < 0.01; I2 = 0%; Fig. 4A) and aspirations (RR 0.63; 95% CI 0.41–0.96; p = 0.03; I2 = 0%; Fig. 4B) compared to DL. However, there were similar incidences of dental injury (RR 0.67; 95% CI 0.20–2.24; p = 0.51; I2 = 0%; Additional 1: Supplemental Fig. 3A), cardiac arrest (RR 1.66; 95% CI 0.52–5.30; p = 0.39; I2 = 0%; Additional 1: Supplemental Fig. 3B), all-cause mortality (RR 1.00; 95% CI 0.87–1.16; p = 0.95; I2 = 0%; Additional 1: Supplemental Fig. 3C), and severe hypoxemia (RR 0.98; 95% CI 0.74–1.29; p = 0.87; I2 = 22%; Additional 1: Supplemental Fig. 3D).

Meta-analysis of safety endpoints in critically ill patients undergoing intubation with VL. Caption: Forest plots presenting the risk ratio (RR) and 95% confidence interval (CI) for each strategy on A esophageal intubation and B aspiration. Abbreviations: CI, confidence interval; MH, Mantel–Haenszel; DL, direct laryngoscope; VL, video laryngoscope; RR, risk ratio
Subgroup and sensitivity analysis
There was a significant subgroup interaction among the brands of VL employed (p = 0.03; Additional 1: Supplemental Fig. 4A). C-MAC and GlideScope performed similarly, but with McGrath MAC, there was no significant difference between VL and DL (RR 0.99; 95% CI 0.96–1.02; p = 0.43; I2 = 11%). Furthermore, there were no significant subgroup interactions when analyzing subgroups stratified by settings (ICU versus ED) (p = 0.48; Additional 1: Supplemental Fig. 4B) or operators’ experience (p = 0.42; Fig. 5). In sensitivity analysis changing the threshold from 50 to 100 prior intubations to be considered experienced, there was no significant subgroup interaction (p = 0.53; Additional 1: Supplemental Fig. 5).

Subgroup analysis of primary outcome by operator's experience in intubating critically ill patients with VL. Abbreviations: CI, confidence interval; MH, Mantel–Haenszel; DL, direct laryngoscope; VL, video laryngoscope; RR, risk ratio
Addressing heterogeneity
We conducted a Graphic Display of Heterogeneity (GOSH) analysis to investigate the moderate to high heterogeneity in our findings. Our results were consistent across multiple simulations and remained stable after random exclusion of studies. We identified one study as the main outlier [25]. A comprehensive explanation of statistical protocols used to explore heterogeneity is available in Additional 1: Supplemental Results 1 and Additional 1: Supplemental Figs. 6–8, 11, and 12.
Risk of bias assessment
Individual RCT appraisal can be found in Additional 1: Supplemental Fig. 9. Regarding the primary outcome, thirteen studies carried high risk of bias due to unblinding of outcome adjudicators due to the nature of intervention, however the DEVICE trial was scored at a low risk of bias due to the presence of an independent observer keeping track of the number of intubation attempts [12]. Moreover, seven studies had some concerns of bias due to the inexistence of protocols [14, 15, 24,25,26,27, 33]. Funnel plot and Egger’s test (p = 0.048) suggested publication bias in the primary outcome, as represented in Additional 1: Supplemental Fig. 10.
Discussion
This meta-analysis of 14 RCTs, encompassing 3981 patients, compared the efficacy and safety of VL in critically ill patients. Our main findings were as follows: (1) VL resulted in higher rates of successful intubations on first attempt; (2) VL led to improved glottic visualization; and (3) VL reduced the incidence of esophageal intubations.
Comprehensive guidelines for managing the intubation of critically ill adults have acknowledged the advantages of VL and recommended its ready availability, considering it the preferred option for all intubations of critically ill patients [34,35,36]. In contrast, these recommendations were not based on previous meta-analyses of RCTs, in which there was no statistically significant benefit of VL over DL in terms of successful intubation on the first attempt [7].
Notably, the performance of VL could be different between brands owing to various designs and shapes [37, 38]. In our analysis, we included three VL blade design (hyperangulated, standard geometry, or channeled), including six different brands (GlideScope, C-MAC, McGrath MAC, UEScope, KingVision, and Airtraq). Interestingly, in the subgroup analysis comparing different VL brands, we found a potential interaction between the VL manufacturer and treatment effect. The benefit of VL over DL tended to be higher with GlideScope and C-MAC. Future head-to-head comparison studies are warranted for conclusive evidence between VL manufacturers.
Our study showed a substantially lower incidence of esophageal intubation and aspiration during tracheal intubation when utilizing VL. Despite of the substantial increase in the rates of successful intubations on the first attempt, it is noteworthy that this did not lead to significant reduction in all-cause mortality, severe hypoxemia, or cardiac arrest.
Regarding operators’ experience among providers, there were different definitions of experience among studies, which we addressed by classifying them through specific criteria (Additional 1: Supplemental Methods 5). To assess the impact of this important variable, we performed two subgroup analyses, in which there was no statistically significant subgroup interaction with a threshold of mean 50 prior intubations (p = 0.42) or 100 prior intubations to be considered experienced (p = 0.53); however, limitations must be acknowledged. One study was unclearly defined as per our criteria, limiting the complete evaluation of this analysis [27].
The choice of sedatives and analgesics for induction could also add heterogeneity to our findings. Rapid sequence induction with sedatives and neuromuscular blocking agents has been shown to facilitate tracheal intubation and decrease intubation-related complications in reasonable circumstances [39]. Due to the lack of strict protocols regarding medication in most of the studies included in this review, subgroup analysis based on medications was not feasible.
Although there is a previous meta-analysis on this issue, our study has some advantages. First, we included 7 additional RCTs compared to the previous study [13]. Second, to minimize potential confounders, we excluded quasi-RCT studies. Third, we restricted our inclusion criteria to patients who potentially derive the most benefit from VL (in the ICU and ED settings). Fourth, key findings were revealed: VL led to higher success rate of intubation on the first attempt compared with DL; and VL reduced the incidence of esophageal intubations.
Study limitations
This meta-analysis has some limitations. First, there was a substantial heterogeneity in the primary outcome. However, we meticulously addressed this heterogeneity by exploring the potential study-level characteristics, as reported in the Additional 1: Supplementary Appendix. Second, our analysis indicated the presence of publication bias concerning the primary outcome. Third, we identified an elevated risk of bias due to the outcome adjudication of the primary outcome, primarily because blinding was impossible due to its inherent nature. Fourth, aspiration relied on operator-reported data, which may be subject to reporting bias. Fifth, only one of included studies reported the presence of secretion as a reason of intubation failure. Therefore, it was not possible to analyze this important variable. Sixth, the subgroup analysis on different VL brands used by individual studies should be interpreted cautiously, as different manufacturers could provide both standard geometry and hyperangulated blades, which impact could not be analyzed. Finally, the absence of patient-level data precluded a more granular assessment of factors potentially related to the relative efficacy of VL vs. DL, such as the operators’ experience and proportion of patients with difficult airways.
Conclusion
In this meta-analysis of RCTs, in critically ill patients, VL led to a higher number of successful intubations on the first attempt, improved visualization through CL grading, and reduced esophageal intubations compared with DL. Our findings support the routine use of VL in critically ill patients.
Data availability statement
All data generated or analyzed during this study are included within the published article and its additional files.
Abbreviations
- CI:
-
Confidence interval
- CL:
-
Cormack Lehane
- DEVICE:
-
Direct versus Video Laryngoscope Trial
- DL:
-
Direct laryngoscope
- ED:
-
Emergency department
- ICU:
-
Intensive care unit
- MD:
-
Mean difference
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- RCT:
-
Randomized controlled trial
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- RR:
-
Risk ratio
- TSA:
-
Trial sequential analysis
- VL:
-
Video laryngoscope
References
Pfuntner A, Wier LM, Stocks C. Most Frequent Procedures Performed in U.S. Hospitals, 2011. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 [cited 2023 Aug 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK174682/
Russotto V, Myatra SN, Laffey JG. What’s new in airway management of the critically ill. Intensive Care Med. 2019;45:1615–8.
Martin LD, Mhyre JM, Shanks AM, Tremper KK, Kheterpal S. 3,423 Emergency tracheal intubations at a university hospital. Anesthesiology. 2011;114:42–8.
Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg. 2004;99:607–13, table of contents.
Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. Anesthesiology. 1995;82:367–76.
Bernhard M, Becker TK, Gries A, Knapp J, Wenzel V. The first shot is often the best shot: first-pass intubation success in emergency airway management. Anesth Analg. 2015;121:1389–93.
Hansel J, Rogers AM, Lewis SR, Cook TM, Smith AF. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst Rev. 2022;4:CD011136.
Jaber S, Amraoui J, Lefrant J-Y, Arich C, Cohendy R, Landreau L, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study*. Crit Care Med. 2006;34:2355–61.
Agrò F, Barzoi G, Montecchia F. Tracheal intubation using a Macintosh laryngoscope or a GlideScope ® in 15 patients with cervical spine immobilization. Br J Anaesth. 2003;90:705–6.
Stauffer JL, Olson DE, Petty TL. Complications and consequences of endotracheal intubation and tracheotomy. Am J Med. 1981;70:65–76.
Lascarrou JB, Boisrame-Helms J, Bailly A, Le Thuaut A, Kamel T, Mercier E, et al. Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among ICU patients: a randomized clinical trial. JAMA. 2017;317:483.
Prekker ME, Driver BE, Trent SA, Resnick-Ault D, Seitz KP, Russell DW, et al. Video versus direct laryngoscopy for tracheal intubation of critically ill adults. N Engl J Med. 2023;389:418–29.
Jiang J, Ma D, Li B, Yue Y, Xue F. Video laryngoscopy does not improve the intubation outcomes in emergency and critical patients—A systematic review and meta-analysis of randomized controlled trials. Crit Care. 2017;21:288.
Ajith P, Bandyopadhyay A, Meena SC, Jain K, Aggarwal S, Gupta SK. Direct laryngoscope versus McGRATH video-laryngoscope for tracheal intubation in trauma emergency: a randomised control trial. Am J Emerg Med. 2022;56:353–5.
Dharanindra MJ, Iyer S, Kulkarni SS, Dharanindra M, Jedge PP, Patil VC, et al. Endotracheal Intubation with King Vision Video Laryngoscope vs Macintosh Direct Laryngoscope in ICU: A Comparative Evaluation of Performance and Outcomes. Indian J Crit Care Med. 2023;27:101–6.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane handbook for systematic reviews of interventions. 2nd Edition. 2nd Edition. Chichester (UK): Wiley; 2019.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, The PRISMA, et al. statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021: n71.
Higgins JP, Savović J, Page MJ, Elbers RG, Sterne JA. Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions [Internet]. 1st ed. Wiley; 2019 [cited 2023 Apr 22]. p. 205–28. DOI: https://doi.org/10.1002/9781119536604.ch8
McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A, the DEPRESsion Screening Data (DEPRESSD) Collaboration, et al. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020;29:2520–37.
Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Mental Health. 2019;22:153–60.
Harrer M, CP, FT, EDD. dmetar: Companion R Package For The Guide “Doing Meta-Analysis in R” [Internet]. Available from: http://dmetar.protectlab.org/.
Wickham H. ggplot2: Elegant graphics for data analysis. New York, NY: Springer New York; 2016.
Viechtbauer W. Conducting Meta-Analyses in R with the metafor Package. J Stat Soft [Internet]. 2010 [cited 2023 Apr 22];36. Available from: http://www.jstatsoft.org/v36/i03/
Sanguanwit P, Yuksen C, Laowattana N. Direct Versus Video Laryngoscopy in Emergency Intubation: A Randomized Control Trial Study. Bull Emerge Trauma [Internet]. 2021 [cited 2023 Aug 5];9. Available from: https://doi.org/10.30476/beat.2021.89922.1240
Dey S, Pradhan D, Saikia P, Bhattacharyya P, Khandelwal H, Adarsha KN. Intubation in the Intensive Care Unit: C-MAC video laryngoscope versus Macintosh laryngoscope. Med Intensiva (Engl Ed). 2020;44:135–41.
Abdelgalel EF, Mowafy SMS. Comparison between Glidescope, Airtraq and Macintosh laryngoscopy for emergency endotracheal intubation in intensive care unit: randomized controlled trial. Egypt J Anaesthesia. 2018;34:123–8.
Gao Y-X, Song Y-B, Gu Z-J, Zhang J-S, Chen X-F, Sun H, et al. Video versus direct laryngoscopy on successful first-pass endotracheal intubation in ICU patients. World J Emerg Med. 2018;9:99–104.
Driver BE, Prekker ME, Moore JC, Schick AL, Reardon RF, Miner JR. Direct versus video laryngoscopy using the C-MAC for tracheal intubation in the emergency department, a randomized controlled trial. Acad Emerg Med. 2016;23:433–9.
Janz DR, Semler MW, Lentz RJ, Matthews DT, Assad TR, Norman BC, et al. Randomized trial of video laryngoscopy for endotracheal intubation of critically ill adults*. Crit Care Med. 2016;44:1980–7.
Sulser S, Ubmann D, Schlaepfer M, Brueesch M, Goliasch G, Seifert B, et al. C-MAC videolaryngoscope compared with direct laryngoscopy for rapid sequence intubation in an emergency department: a randomised clinical trial. Eur J Anaesthesiol. 2016;33:943–8.
Yeatts DJ, Dutton RP, Hu PF, Chang Y-WW, Brown CH, Chen H, et al. Effect of video laryngoscopy on trauma patient survival: a randomized controlled trial. J Trauma Acute Care Surg. 2013;75:212–9.
Griesdale DEG, Liu D, McKinney J, Choi PT. Glidescope® video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Can J Anesth/J Can Anesth. 2012;59:41–52.
Goksu E, Kilic T, Yildiz G, Unal A, Kartal M. Comparison of the C-MAC video laryngoscope to the Macintosh laryngoscope for intubation of blunt trauma patients in the ED. Turk J Emerg Med. 2016;16:53–6.
Quintard H, l’Her E, Pottecher J, Adnet F, Constantin J-M, De Jong A, et al. Intubation and extubation of the ICU patient. Anaesth Crit Care Pain Med. 2017;36:327–41.
Myatra S, Ahmed S, Kundra P, Garg R, Ramkumar V, Patwa A, et al. The All India Difficult Airway Association 2016 guidelines for tracheal intubation in the Intensive Care Unit. Indian J Anaesth. 2016;60:922.
Higgs A, McGrath BA, Goddard C, Rangasami J, Suntharalingam G, Gale R, et al. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018;120:323–52.
Kleine-Brueggeney M, Greif R, Schoettker P, Savoldelli GL, Nabecker S, Theiler LG. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br J Anaesth. 2016;116:670–9.
Kleine-Brueggeney M, Buttenberg M, Greif R, Nabecker S, Theiler L. Evaluation of three unchannelled videolaryngoscopes and the Macintosh laryngoscope in patients with a simulated difficult airway: a randomised, controlled trial. Anaesthesia. 2017;72:370–8.
Wilcox SR, Bittner EA, Elmer J, Seigel TA, Nguyen NTP, Dhillon A, et al. Neuromuscular blocking agent administration for emergent tracheal intubation is associated with decreased prevalence of procedure-related complications. Crit Care Med. 2012;40:1808–13.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
B.A. and A.R. contributed to conceptualization, data curation, formal analysis, investigation, methodology, project administration, and original draft preparation of the manuscript. S.M., R.A., P.C., and M.S. contributed to data curation, methodology, and formal analysis. A.G.M. provided critical revisions to the manuscript and contributed to methodology.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests. All authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. There were no external funding sources for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplementary appendix.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Araújo, B., Rivera, A., Martins, S. et al. Video versus direct laryngoscopy in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials. Crit Care 28, 1 (2024). https://doi.org/10.1186/s13054-023-04727-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04727-9