
Abstract
Background
The aim of this study is to compare the 2021–2022 bronchiolitis season to the four previous years (2017–2018, 2018–2019, 2019–2020, 2020–2021) to see if there was an anticipation of the peak, an overall increase of cases, and an increased need of intensive care.
Methods
A retrospective single-centre study in the San Gerardo Hospital Fondazione MBBM, Monza, Italy was performed. Emergency Departments (ED) visits of patients aged < 18 years and ≤ 12 months were analyzed: the incidence of bronchiolitis on total assessments, the urgency level at triage and the hospitalization rate were compared. Data of children admitted to the Pediatric Department due to bronchiolitis were analyzed in terms of need of intensive care, respiratory support (type and duration), length of hospital stay, main etiological agent, patient characteristics.
Results
During 2020–2021 (first pandemic period) an important reduction in the ED attendance for bronchiolitis was observed, while in 2021–2022 there was an increase in incidence of bronchiolitis (13% of visits in infants < 1 year) and in the rate of urgent accesses (p = 0.0002), but hospitalization rates did not differ compared to previous years. Furthermore, an anticipated peak in November 2021 was observed. In the 2021–2022 cohort of admitted children to the Pediatric Department, a statistically significative increased need of intensive care unit was detected (Odds Ratio 3.1, 95% CI 1.4–6.8 after adjustment for severity and clinical characteristics). Instead, respiratory support (type and duration) and length of hospital stay did not differ. RSV was the main etiological agent and RSV-bronchiolitis determined a more severe infection (type and duration of breathing support, intensive care need and length of hospital stay).
Conclusions
During Sars-CoV-2 lockdowns (2020–2021), there was a dramatic decrease of bronchiolitis and others respiratory infections. In the following season, 2021–2022, an overall increase of cases with an anticipated peak was observed and data analysis confirmed that patients in 2021–2022 required more intensive care than children in the four previous seasons.
Similar content being viewed by others


Background
Bronchiolitis is a major burden of the lower respiratory tract for infants and young children [1]. It is a seasonal infection, which typically presents between October and April in the northern hemisphere.
In March 2020, the World Health Organization (WHO) declared the Sars-CoV-2 outbreak a pandemic [2]. Because this virus is mainly airborne, measures such as social distancing, frequent hand washing and the usage of face-masks have been implemented worldwide. These actions influenced the transmission of other respiratory viruses [3]. A dramatic decrease of influenza and other respiratory infections, including bronchiolitis, has been globally described [4,5,6,7]. Italian Emergency Departments (ED) assisted a significant reduction of bronchiolitis admitted to the ED during the 2020–2021 cold season [8,9,10] and an overall reduction of acute respiratory tract infections [11] and hospitalized patients [12]. The second year of the pandemic has been characterized by a loosening of closure measures thanks to mass vaccination campaigns, allowing an increase in social interactions. To date, more than 90% of the Italian population over 12 years old has been vaccinated against Sars-CoV-2 [13]. Because of the increase of social interactions, a recurrence of common respiratory infections was expected. The 2021–2022 bronchiolitis surge was first described in Australian children [14], followed by intercontinental reports [15,16,17,18]. Camporesi et al. and Nenna et al. [19, 20] describe the anticipation of the bronchiolitis peak in Italy (October–November vs. mid-February), but they do not confirm an increase in overall severity. The aim of this study is to compare the 2021–2022 season to the four previous years (2017–2018, 2018–2019, 2019–2020, 2020–2021) to see if there was an anticipation of the peak, an overall increase of cases, and an increase of severity.
Materials and methods
This is a single-centre retrospective study carried out at the San Gerardo Hospital—“Fondazione Monza e Brianza per il Bambino e la sua Mamma”, Monza, Italy. No ethics committee approval is required in Italy for epidemiological studies using health care administrative databases for research purposes and with individuals identified by an anonymous patient code.
Emergency Department (ED) admissions of children aged 0–18 years between September and April of 2017–2022 were analyzed, as well as children younger than 12 months old and with the clinical diagnosis of bronchiolitis (e.g., children with rhinorrhea, cough, crackles, wheezing, dyspnea, polypnea, feeding difficulties, apnea, lethargy) [21, 22]. There is no full agreement on the upper cut-off for diagnosing bronchiolitis, despite the majority account 12 months as the upper age limit [20,21,22,23], so this cut-off was considered in this study. The etiology of bronchiolitis was determined by nose swab or by rhino pharynx aspirate analyzed by Allplex™ Respiratory Panel Assays by Seegene Inc, an assay for the detection and identification of 26 pathogens (viruses and bacteria) using one-step real-time RT-PCR, or by ID NOW™ RSV PCR by Abbott.
In the ED a stratification of severity is obtained by assignment of a colour code by triage nurses, based on nationwide criteria: red (nondeferrable emergency, life-threatening condition), yellow (urgent, but not immediate life-threatening condition), green (low urgency and priority, deferrable care), and white code (nonurgent). Infants who received a diagnosis of bronchiolitis in the ED were either discharged, admitted to the Pediatric Department according to international and Italian guidelines [24], or transferred to another hospital due to full capacity. Need of intensive care was defined as the need of intensive respiratory support such as continuous positive airway pressure (CPAP) or mechanical ventilation. Risk factors were classified as prematurity (< 37 weeks gestational age at birth) and chronic disease (e.g. Down Syndrome, inborn errors of metabolism). No patients included in the study had congenital heart disease, because such patients are referred to other hospitals in Lombardy.
Only the first episode of bronchiolitis in children with more than one throughout the same season was considered.
During the 2017–2022 period, the overall capacity of the Pediatric Department has remained the same (14–17 hospital beds available per day).
The primary outcome of the study was to determine if the 2021–2022 bronchiolitis season was more severe in terms of need of intensive care in comparison to the seasons 2017–18, 2018–19, 2019–20, 2020–21.
The secondary outcomes were to compare the need of respiratory support and hospital stay length; to define the main etiological agents throughout the five different seasons; to compare disease severity in children with RSV versus non-RSV bronchiolitis; to compare disease severity in children with RSV and no risk factors (e.g., prematurity) versus RSV and risk factors.
Our hospital is situated in Monza, Lombardy, the first and most affected region in Italy during the Sars-CoV-2 outbreak. Lockdown was instituted between March and May 2020 and between October 2020 and March 2021 [25, 26]. Primary schools (6–11 years old) were closed from March to June 2020 and from mid-February to April 2021.
We ran the statistical analysis on R (4.1.2). For categorical variables, we compared groups by using the Fisher exact test for count data (when the variable took two values) or Pearson's Chi-squared test (when the variable could take more than 2 values). None of the continuous variables appeared to follow a normal distribution, which was tested by running the Shapiro Wilk Normality test. Because of this, discrete and continuous variables were tested using the Wilcoxon rank sum test. For all tests, the null was rejected at the 5% significance level. Missing data was omitted from the analysis. In the tables, each value's count is shown for categorical variables while the median and range is shown for discrete and continuous variables.
Univariate analyses were performed to evaluate the association between the admission to intensive care unit (primary outcome) and the following variables: period (2021–22 versus 2017–2020), age (≥ 60 vs. < 60 days), presence of risk factors (yes vs. no), respiratory syncytial virus (RSV) as etiology (yes vs. no), oxygen need (HNFC/CPAP yes vs. no) and Silverman score (≥ 2 vs. < 2). The 2020–21 period was not considered in this analysis because of the limited size sample due to the pandemic. A stepwise regression analysis was performed to investigate the association between admission to ICU and the above covariates.
Results
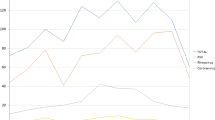
Total admissions of children and adolescents to ED during the study period decreased from 15,194 in 2017–2018 to 12,335 in 2021–2022. As described worldwide, there was a significant reduction of hospital visits during the Sars-CoV-2 pandemic (5,379 accesses between September 2020 and April 2021). Among all admissions, bronchiolitis diagnosis consisted in about 1% of all diagnosis; among children aged 0–12 months, bronchiolitis represented 7–13% of pediatric ED accesses, except for the pandemic year (1.4%). An anticipated peak was observed in November 2022, counting for 57% of all cases of the 2021–2022 season (2 bronchiolitis in September 2021, 22 in October 2021, 112 in November 2021, 39 in December 2021, 9 in January 2022, 4 in February 2022, 3 in March 2022 and 5 in April 2022) (Fig. 1).

Emergency Department (ED) diagnosis of bronchiolitis in ≤ 1 year old children
Overall, among children aged 0–12 months with a diagnosis of bronchiolitis, 15% was brought to the ED more than once, with no differences across seasons. In the 2021–2022 season there was a statistically significative difference in severity at presentation based on the colour code of assignment: 34% of bronchiolitis were given a red or yellow code in comparison to 19% of the previous years (χ2 = 18,5, p = 0.0002). Overall, 362 of 680 (53.2%) children with bronchiolitis at ED were hospitalized, 141 of whom were admitted to the Pediatric Department of San Gerardo hospital (Table 1). The hospitalization rate did not change throughout the five years (p = 0.25).
There was an increased need of intensive care in 2021–2022 in comparison to the 2017–21 period (p = 0.005). Instead, no statistically significative differences were found in terms of severity at presentation (Silverman Score and peripheral oxygen saturation, p = 0.35 and p = 1 respectively), respiratory support type and duration (p = 0.96 and p = 0.55), length of stay (p = 0.73), nasogastric feeding or intravenous hydration (p = 0.33 and p = 0.07), neither were there no differences in terms of age at presentation (63 vs 72 days, p = 0.13), weight (4.9 vs. 5.2 kg, p = 0.23), etiology (p = 1, RSV was the main viral agent) and presence of risk factors (p = 0.74).
No statistically significant difference was observed also when comparing the characteristics of 2021–2022 cohort versus 2018–19 (before the beginning of the pandemic), except for intensive care admission (p = 0.04) and need of intravenous hydration (p = 0.003). In 2021–2022 no deaths occurred, and no short-term sequelae are reported.
At the univariate analysis, the likelihood of being admitted to ICU was influenced by observation period, presence of risk factors, need of HFNC/CPAP, RSV as causal agent and Silverman Score. After adjustment of the above covariates, a greater likelihood of ICU admission was observed in 2021–22 period versus 2017–2020 (aOR 3.6; 95%,CI 1.5–8.9) (Table 2). In the analysis of the five cohorts (2017–2022), RSV was the main etiological agent (Table 2) (79% in 2017–2018, 72% in 2018–2019, 66% in 2019–2020, 0% in 2020–2021, 78% in 2021–2022). The children with RSV-bronchiolitis, throughout the entire study period (2017–2022) required more oxygen support (length and type), intensive care, and longer hospital stay in comparison to those with RSV negative bronchiolitis (Supplementary Table 1).
Finally, we compared the severity of the disease of children with RSV-bronchiolitis and risk factors (e.g. prematurity, other diseases) versus children with RSV-bronchiolitis and no risk factors between 2017 and 2022, confirming an increased need of intensive care (p = 0.001) and nose-tube feeding (p = 0.001) for children with RSV bronchiolitis and risk factors, and older age at time of presentation (p = 0.001). There were no differences between these two cohorts in terms of oxygen blood peripheral saturation (p = 0.88), Silverman score (p = 0.73), type of respiratory support (p = 0.88), length of respiratory support in days (p = 0.2), length of hospital stay (p = 0.22) and need of intravenous fluids (p = 0.81).
Discussion
During the Sars-CoV-2 pandemic, a dramatic decrease in viral infections has been described in the pediatric population [11], due to social-distancing, closure of schools, implementation of hand washing and the usage of face-masks [4, 5, 7, 27]. This phenomenon included bronchiolitis and has been described in Italy as well [8, 9], and the present findings confirm what observed between September 2020 and April 2021.
During the summer of 2021, alerts were released concerning an outbreak of an abnormal bronchiolitis season in terms of overall numbers and distribution. It was initially anticipated by pediatricians in the Southern Hemisphere [18], followed by worldwide studies, which reported an increase in overall incidence and an anticipation of the usual peak [6, 15,16,17]. In our results, after a disappearance of bronchiolitis during the first lockdown, an increase in overall incidence during September 2021 and April 2022 was observed. Moreover, this study confirms the anticipated peak and shorter duration of the season described by other Italian reports [19, 20] (Fig. 1).
In the 2021–2022 season, there was a double increase in severity at presentation based on the colour of assignment from triage nurses at admission in ED. Even so, the admission rate did not change throughout the five years.
Guitart et al. [16] describe a more severe 2021 bronchiolitis season in comparison to the previous ten years in terms of length of stay and need of pediatric intensive care unit. Whereas, in Italy, Camporesi et al. [19] do not confirm an unusual disease severity. In our sample, a three time increase after adjustment was observed in intensive care admission during 2021–2022 season in agreement with Guitart et al. findings [16]. It is not possible to completely exclude that the increase in ICU admission in 2021/22 may be due to different criteria adopted by health professionals, but in our opinion it is unlikely, since the availability of beds was scant.
In our study RSV was the main etiological agent as reported in literature [1, 21, 22], except for 2020–2021. Bronchiolitis due to RSV resulted more severe in terms of respiratory support, intensive care and length of hospital stay in comparison to those with RSV negative bronchiolitis. In literature, there is no consensus whether this is true or not [20, 22, 28, 29]. An increase of intensive care accesses and nose-tube feeding, and older age at time of presentation was observed in children with RSV-bronchiolitis and risk factors (e.g. prematurity, other diseases), in accordance with previously reported data [24, 30, 31].
The abnormal bronchiolitis peak may be explained by a global loosening of Sars-CoV-2 prevention measures and an increase in social interactions, in association to a waned herd immunity to other viruses and an increase in RSV-naïve patients. In fact, children affected by bronchiolitis during 2021–2022 were born during the Sars-CoV-2 pandemic, with an immune system that was less stimulated by external agents (bacteria, virus and others) due to all the Sars-CoV2 restrictions; even their mothers were not exposed to infections and did not develop antibodies. Furthermore, Nenna et al. described an opposite hospital admission trend between RSV and Sars-CoV-2 during their study period (2021–2022) confirming a close relationship between these two viruses [20]. A hypothesis which has been addressed is that of “viral interference”: if a person is co-infected by two viruses at the same time, the immune responses toward one of them reduces the possibility to replicate of the other [16, 32, 33]. Another hypothesis that should be considered is that during the Sars-CoV-2 pandemic there may have been a genetic lineage shift in RSV, as previously observed [34]. Finally, an association with weather and air pollution has been hypothesized: climate factors could possibly influence RSV spread, as Nenna et al. [35] suggest on a ten-year study on Italian infants with RSV bronchiolitis before Sars-CoV2 outbreak. Manti et. al [36] argue this hypothesis as well during the 2020 lockdown, during which a 60% decrease of air pollutants was observed, as well as a reduction of RSV bronchiolitis. Further studies are needed.
Analysis of future seasons will allow a better understanding of the impact of Sars-CoV-2 on respiratory infections. Recent reports from the Southern Hemisphere and the United Kingdom describe abnormal Influenza and RSV seasons in terms of incidence and distribution of cases [37,38,39,40].
The limitations of this study are that it is a retrospective single centre study with a limited sample size. The diagnosis of bronchiolitis is clinical; few patients did not have a defined etiological agent. In those without an identified germ, extensive viral testing was not performed. However, the etiological agent, according to Italian and international guidelines, does not affect treatment.
Conclusions
During Sars-CoV-2 lockdowns (2020–2021), there was a dramatic decrease of ED assessments and a dramatic decrease of clinical diagnosis of bronchiolitis, followed by an anticipated and significantly increased peak of bronchiolitis during the 2021–2022 season. Children with bronchiolitis assessed in the ED were triaged with more urgent codes, but hospitalization rates did not change. However, admissions to the Intensive Care Unit were higher than in the four previous investigated seasons. Clinicians should prepare for abnormal RSV seasons, in terms of incidence, distribution and severity.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ED:
-
Emergency Departments
- Sars-CoV-2:
-
Severe Acute Respiratory Syndrome Coronavirus—2
- BPD:
-
Bronchopulmonary Dysplasia
- RSV:
-
Respiratory Syncytial Virus
- HFNC:
-
High Flow Oxygen on Nasal Cannulae
- CPAP:
-
Continuous Positive Airway Pressure
- RT-PCR:
-
Reverse Transcriptase-Polymerase Chain Reaction
References
Florin TA, Plint AC, Zorc JJ. Viral bronchiolitis. Lancet. 2017;389(10065):211–24. https://doi.org/10.1016/S0140-6736(16)30951-5.
World Health Organization. "Novel Coronavirus (2019-nCoV) Situation Report". 2020. Retrieved from https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200125-sitrep-5-2019-ncov.pdf?sfvrsn=429b143d_8%22.
Fricke LM, Glöckner S, Dreier M, Lange B. Impact of non-pharmaceutical interventions targeted at COVID-19 pandemic on influenza burden – a systematic review. J Infect. 2021;82(1):1–35. https://doi.org/10.1016/j.jinf.2020.11.039.
Yeoh DK, Foley DA, Minney-Smith CA, et al. Impact of Coronavirus disease 2019 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin Infect Dis. 2021;72(12):2199–202. https://doi.org/10.1093/cid/ciaa1475.
Kadambari S, Goldacre R, Morris E, Goldacre MJ, Pollard AJ. Indirect effects of the covid-19 pandemic on childhood infection in England: population based observational study. BMJ. 2022;376:1–10. https://doi.org/10.1136/bmj-2021-067519.
Willis Z, De St MA. Covid-19 control measures and common paediatric infections. BMJ. 2022;376:1–2. https://doi.org/10.1136/bmj.n3093.
Trenholme A, Webb R, Lawrence S, et al. COVID-19 and infant hospitalizations for seasonal respiratory virus infections, New Zealand, 2020. Emerg Infect Dis. 2021;27(2):641–3. https://doi.org/10.3201/eid2702.204041.
Stera G, Pierantoni L, Masetti R, et al. Impact of sars-cov-2 pandemic on bronchiolitis hospitalizations: the experience of an italian tertiary center. Children. 2021;8(7):4–9. https://doi.org/10.3390/children8070556.
Curatola A, Lazzareschi I, Bersani G, Covino M, Gatto A, Chiaretti A. Impact of COVID-19 outbreak in acute bronchiolitis: Lesson from a tertiary Italian emergency department. Pediatr Pulmonol. 2021;56(8):2484–8. https://doi.org/10.1002/ppul.25442.
Clavenna A, Nardelli S, Sala D, Fontana M, Biondi A, Bonati M. Impact of COVID-19 on the pattern of access to a pediatric emergency department in the Lombardy Region. Italy Pediatr Emerg Care. 2020;36(10):e597–8. https://doi.org/10.1097/PEC.0000000000002232.
Nenna R, Matera L, Pierangeli A, Oliveto G, Viscido A, Petrarca L, La Regina DP, Mancino E, Di Mattia G, Villani A, Midulla F. First COVID-19 lockdown resulted in most respiratory viruses disappearing among hospitalised children, with the exception of rhinoviruses. Acta Paediatr. 2022;111(7):1399–403. https://doi.org/10.1111/apa.16326. (Epub 2022 Mar 16. PMID: 35266576; PMCID: PMC9111239).
Vitello AS, Clavenna A, Cartabia M, Sala D, Biondi A, Bonati M. Evaluation of the pattern of use of a pediatric emergency department in Italy. Pediatr Emerg Care. 2021;37(12):E1494–8. https://doi.org/10.1097/PEC.0000000000002091.
Ministero della Salute. "Report Vaccinazioni Anti COVID-19". 2023. Retrieved from https://www.governo.it/it/cscovid19/report-vaccini/.
Foley DA, Yeoh DK, Minney-Smith CA, et al. The interseasonal resurgence of respiratory syncytial virus in Australian children following the reduction of Coronavirus disease 2019-related public health measures. Clin Infect Dis. 2021;73(9):E2829–30. https://doi.org/10.1093/cid/ciaa1906.
Weinberger Opek M, Yeshayahu Y, Glatman-Freedman A, Kaufman Z, Sorek N, Brosh-Nissimov T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. Euro Surveill. 2021;26(29):2017–21. https://doi.org/10.2807/1560-7917.ES.2021.26.29.2100706.
Guitart C, Bobillo-Perez S, Alejandre C, et al. Bronchiolitis, epidemiological changes during the SARS-CoV-2 pandemic. BMC Infect Dis. 2022;22(1):84. https://doi.org/10.1186/s12879-022-07041-x.
Agha R, Avner JR. Delayed seasonal RSV surge observed during the COVID-19 pandemic. Pediatrics. 2021;148(3):2019–21. https://doi.org/10.1542/peds.2021-052089.
Hussain F, Kotecha S, Edwards MO. RSV bronchiolitis season 2021 has arrived, so be prepared! Arch Dis Child. 2021;106(12):e51–e51. https://doi.org/10.1136/archdischild-2021-322835.
Camporesi A, Morello R, Ferro V, et al. Epidemiology, microbiology and severity of bronchiolitis in the first post-lockdown cold season in three different geographical areas in Italy: a prospective, observational study. Children (Basel). 2022;9(4):491. https://doi.org/10.3390/children9040491.
Nenna R, Matera L, Licari A, Manti S, Di Bella G, Pierangeli A, Palamara AT, Nosetti L, Leonardi S, Marseglia GL, Midulla F, ICHRIS Group. An Italian multicenter study on the epidemiology of respiratory SyncytiaYl virus during SARS-CoV-2 pandemic in hospitalized children. Front Pediatr. 2022;10:930281. https://doi.org/10.3389/fped.2022.930281. (PMID: 35911833; PMCID: PMC9329524).
Meissner HC. Viral bronchiolitis in children. N Engl J Med. 2016;374(1):62–72. https://doi.org/10.1056/NEJMra1413456.
Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474–502. https://doi.org/10.1542/peds.2014-2742.
Korppi M. Virus-induced wheezing in infants aged 12–24 months and bronchiolitis in infants under 6 months are different clinical entities. Acta Paediatr Int J Paediatr. 2015;104(12):e539. https://doi.org/10.1111/apa.13107.
Baraldi E, Lanari M, Manzoni P, et al. Inter-society consensus document on treatment and prevention of bronchiolitis in newborns and infants. Ital J Pediatr. 2014;40:65. https://doi.org/10.1186/1824-7288-40-65.
Regione Lombardia. "Ulteriori misure urgenti per il contenimento dell’epidemia da Covid". 2022. Retrieved from https://www.regione.lombardia.it/wps/portal/istituzionale/HP/DettaglioRedazionale/servizi-e-informazioni/cittadini/salute-e-prevenzione/prevenzione-e-benessere/red-coronavirusnuoviaggiornamenti.
Governo Italiano Presidenza del Consiglio dei Ministri. "Coronavirus, le misure adottate dal Governo". 2022. Retrieved from https://www.governo.it/it/coronavirus-misure-del-governo.
Nascimento MS, Baggio DM, Fascina LP, do Prado C. Impact of social isolation due to COVID-19 on the seasonality of pediatric respiratory diseases. PLoS One. 2020;15(12):1–10. https://doi.org/10.1371/journal.pone.0243694.
Hussain F, Delgado Thompson M, Vick D, West J, Edwards M. Clinical severity of RSV bronchiolitis. Heal Sci Reports. 2022;5(2):e543. https://doi.org/10.1002/hsr2.543.
Bennett BL, Garofalo RP, Cron SG, et al. Immunopathogenesis of respiratory syncytial virus bronchiolitis. J Infect Dis. 2007;195(10):1532–40. https://doi.org/10.1086/515575.
Meissner HC. Selected populations at increased risk from respiratory syncytial virus infection. Pediatr Infect Dis J. 2003;22(2 Suppl):S40-4. https://doi.org/10.1097/01.inf.0000053884.21238.13. (discussion S44-5).
Stevens TP, Sinkin RA, Hall CB, Maniscalco WM, McConnochie KM. Respiratory syncytial virus and premature infants born at 32 weeks’ gestation or earlier: Hospitalization and economic implications of prophylaxis. Arch Pediatr Adolesc Med. 2000;154(1):55–61.
Martin ET, Kuypers J, Wald A, Englund JA. Multiple versus single virus respiratory infections: viral load and clinical disease severity in hospitalized children. Influenza Other Respir Viruses. 2012;6(1):71–7. https://doi.org/10.1111/j.1750-2659.2011.00265.x.
Wu A, Mihaylova VT, Landry ML, Foxman EF. Interference between rhinovirus and influenza A virus: a clinical data analysis and experimental infection study. The Lancet Microbe. 2020;1(6):e254–62. https://doi.org/10.1016/S2666-5247(20)30114-2.
Thielen BK, Bye E, Wang X, et al. Summer outbreak of severe RSV-B disease, Minnesota, 2017 associated with emergence of a genetically distinct viral lineage. J Infect Dis. 2020;222(2):288–97. https://doi.org/10.1093/infdis/jiaa075.
Nenna R, Evangelisti M, Frassanito A, Scagnolari C, Pierangeli A, Antonelli G, Nicolai A, Arima S, Moretti C, Papoff P, et al. Respiratory syncytial virus bronchiolitis, weather conditions and air pollution in an Italian urban area: An observational study. Environ Res. 2017;158:188–93. https://doi.org/10.1016/j.envres.2017.06.014.
Manti S, Giallongo A, Parisi GF, Papale M, Presti S, Lo Bianco M, Spicuzza L, Leonardi S. Impact of COVID-19 pandemic and lockdown on the epidemiology of RSV-mediated bronchiolitis: experience from our centre. Children (Basel). 2022;9(11):1723. https://doi.org/10.3390/children9111723.
Pérez-López A, Al Mana H, Iqbal M, Suleiman M, Hasan MR, Tang P. Resurgence of influenza A infections in children after the relaxation of COVID-19-related social distancing measures and normalization of international travel in Qatar. J Travel Med. 2022;29:taac107. https://doi.org/10.1093/jtm/taac107. (Epub ahead of print. PMID: 36150023).
NHS Department of Health and Social Care. "Commencement of a Palivizumab Passive Immunisation Programme Against Respiratory Syncytial Virus (RSV) in at risk infants in England, Scotland and Wales". 2022. Retrieved from https://www.cas.mhra.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=103210.
NHS Department of Health and Social Care. "Weekly national Influenza and COVID-19 surveillance report Week 40 report (up to week 39 data) 6 October 2022". 2022. Retrieved from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1109546/Weekly_Flu_and_COVID-19_report_w40.pdf.
New South Wales Health. "Respiratory surveillance reports - COVID-19 and influenza, summary of epidemiological week 39 ending 1 October 2022". 2022. Retrieved from https://www.health.nsw.gov.au/Infectious/covid-19/Pages/weekly-reports.aspx.
Acknowledgements
We thank A.J.O. Faraguna for all his help and precious time.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
Conceptualization, M.C.F., I.L., C.V.; methodology, M.B., A.Cl.; investigation, M.C.F. and I.L.; resources and data curation, M.C.F., I.L., C.V., D.S. M.L.M.; writing—original draft preparation, M.C.F. and I.L.; writing—review and editing, M.B., A.Cl., A.Ca., A.B., visualization, M.C.F., I.L., C.V., M.L.M., D.S., A.Cl., M.B., A.Ca., A.B., supervision, A.B.; project administration, M.B., A.Cl., A.B. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
No ethics committee approval is required in Italy for epidemiological studies using health care administrative databases for research purposes and with individuals identified by an anonymous patient code. All methods were carried out in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Comparison between the RSV-bronchiolitis and non-RSV bronchiolitis in the 2017-2022 study period.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Faraguna, M.C., Lepri, I., Clavenna, A. et al. The bronchiolitis epidemic in 2021–2022 during the SARS-CoV-2 pandemic: experience of a third level centre in Northern Italy. Ital J Pediatr 49, 26 (2023). https://doi.org/10.1186/s13052-023-01425-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-023-01425-8