
Abstract
Acute myeloid leukemia (AML) is a malignant blood cancer with marked cellular heterogeneity due to altered maturation and differentiation of myeloid blasts, the possible causes of which are transcriptional or epigenetic alterations, impaired apoptosis, and excessive cell proliferation. This neoplasm has a high rate of resistance to anticancer therapies and thus a high risk of relapse and mortality because of both the biological diversity of the patient and intratumoral heterogeneity due to the acquisition of new somatic changes. For more than 40 years, the old gold standard “one size fits all” treatment approach included intensive chemotherapy treatment with anthracyclines and cytarabine.
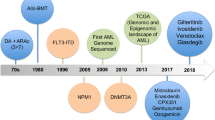
The manuscript first traces the evolution of the understanding of the pathology from the 1970s to the present. The enormous strides made in its categorization prove to be crucial for risk stratification, enabling an increasingly personalized diagnosis and treatment approach.
Subsequently, we highlight how, over the past 15 years, technological advances enabling single cell RNA sequencing and T-cell modification based on the genomic tools are affecting the classification and treatment of AML. At the dawn of the new millennium, the advent of high-throughput next-generation sequencing technologies has enabled the profiling of patients evidencing different facets of the same disease, stratifying risk, and identifying new possible therapeutic targets that have subsequently been validated. Currently, the possibility of investigating tumor heterogeneity at the single cell level, profiling the tumor at the time of diagnosis or after treatments exist. This would allow the identification of underrepresented cellular subclones or clones resistant to therapeutic approaches and thus responsible for post-treatment relapse that would otherwise be difficult to detect with bulk investigations on the tumor biopsy. Single-cell investigation will then allow even greater personalization of therapy to the genetic and transcriptional profile of the tumor, saving valuable time and dangerous side effects. The era of personalized medicine will take a huge step forward through the disclosure of each individual piece of the complex puzzle that is cancer pathology, to implement a “tailored” therapeutic approach based also on engineered CAR-T cells.
Similar content being viewed by others

Introduction
Acute myeloid leukemia (AML) is an aggressive blood cancer characterized by an accumulation of immature cells of the myeloid lineage. Although most patients initially respond to chemotherapy, about 75% relapse and succumb to the disease within 5 years after diagnosis [1]. The latter aspect of the disease highlights how important it is to better understand the underlying mechanisms that prevent the elimination of all cancer cells to develop more targeted and efficient therapies.
In the 19th century Lewis Carroll wrote “Who in the world am I? Ah, that is the great puzzle.” This sentence referring to the famous novel “Alice’s adventure in wonderland” seems to fit perfectly in our scientific context about leukemia and, more generally, the development and evolution of cancer.
We could paraphrase the question written by Carrol in “What disease am I?”. Already in the end of the 1800s, the German pathologist David Paul Von Hansemann published the first observations on the state of cells that, losing their specific characteristics, assume an undifferentiated and atypical appearance. He was in fact the first to coin the terms anaplasia and dedifferentiation referring to the nuclear and mitotic differences that characterize morphological heterogeneity within the tumor tissue [2]. In the 1970s, a major work by Peter Nowell provided to the scientific community a milestone in reference to the clonal evolutionary model on tumor growth [3]. Neoplastic development is defined by a series of mutational events. These genetic lesions occur in somatic cells and first and foremost characterize the loss of proliferation control and programmed death regulation. These genetic alterations, as in Darwinian evolution, may grant selective advantages to these clonal subpopulations, allowing survival to chemo- or radio-therapy treatments, as well as the ability to evade the immune system and acquire metastatic features [4, 5].
The complex adaptive process of cancer evolution involves genetic assortment combined with clonal selection and subsequently subclonal expansion.
Certainly cancer is a great puzzle, and although the cytogenetic heterogeneity of leukemia cells has been recognized for more than 40 years [6], the enormous molecular heterogeneity of the disease was evidenced only with the advent of new massive sequencing techniques such as Next Generation Sequencing (NGS) [7]. It has also been clarified that some genomic alterations are shared by the entire tumor, but not all cancer cells show identical genomic and cytogenetic profiles. Interestingly, the single-cell analysis, now possible thanks to advanced miniaturization techniques, has shown that cancers are characterized by enormous cellular heterogeneity presenting different markers can be used for the diagnosis and treatment.
This review will discuss risk factors associated with AML, therapies developed to contrast the progression of AML, and recent discoveries based on genomic methods and single-cell analyses that could be the basis for new therapeutic approaches.
AML: description of the pathology
AML is a biologically heterogeneous disease characterized by a broad category of overlapping hematologic aggressive neoplasms associated with rapid onset with a progressive course and often chemoresistant to cytotoxic therapies [8, 9]. Normally, the course of the disease begins in the bone marrow (BM) and then rapidly progresses to the bloodstream. It is not uncommon for leukemic cancer cells to invade other tissues and organs such as lymph nodes, liver, testes, spleen, and central nervous system (brain and spinal cord).
This blood cancer is characterized by malignant transformation of progenitor/precursor cells committed to the myeloid lineage. The blasts fate is then compromised, impairing maturation and differentiation into granulocytic, monocytic, erythroid and/or megakaryocytic elements. The result of abnormal and poor differentiation of myeloid cells is also the dangerous accumulation of high levels of immature malignant cells and the decrease of normally differentiated blood components in blood and non-blood tissues [10, 11].
Clinical manifestations of AML include symptoms and signs associated with cytopenia, for example, anemia, infections related to low white blood cell counts, as well as bleeding or ecchymosis due to thrombocytopenia. In parallel, they may be accompanied by constitutional symptoms, such as abnormalities of metabolic pathways and various complications such as fever, bone pain, shortness of breath, pale skin, lethargy, and fatigue. AML has also been called acute myeloid leukemia and acute non-lymphocytic leukemia [12, 13].
Leukemogenesis: risk factors
AML is the result of a series of mutational events that occur in hematopoietic stem cells (HSCs) that include genetic and epigenetic alterations effectively altering normal hematopoiesis. Indeed, the leukemic condition appears to be maintained by an uncommon subpopulation of leukemic cells called leukemic stem cells (LSC), also referred as leukemia-initiating cells (LIC). These cells, identified at the end of the last century, are fully transformed by driver mutations that confer typical characteristics of stem cells and therefore the ability to reconstitute the heterogeneous condition of leukemia, self-renewal ability and drug resistance [14, 15]. In most cases it is still not possible to deduce the exact event that causes AML. In any case, it is now established that the disease can develop thanks to the contribution of various aspects that identify various acquired risk factors: (a) the age and therefore the senescence of HSCs; (b) exposure to anticancer therapy with chemotherapy or ionizing radiation (the total or part loss of chromosome 5 or 7 following treatments with alkylating agents and/or radiotherapy as well as the mutagenic action of topoisomerase 2 inhibitors is well documented [16]); (c) obesity; (d) smoking [17, 18]; (e) family predisposition (Table 1). Family predisposition can be due to aneuploidy as trisomy 21, Fanconi’s anemia and some germline mutations in Tumor Protein P53 (TP53), CCAAT Enhancer Binding Protein Alpha (CEBPA), ETS Variant Transcription Factor 6 (ETV6), Ankyrin Repeat Domain Containing 26 (ANKRD26), DEAD-Box Helicase 41 (DDX41), RUNX Family Transcription Factor 1 (RUNX1), Telomerase RNA Component (TERC), GATA Binding Protein 2 (GATA2), Signal Recognition Particle 72 (SRP72), and Telomerase Reverse Transcriptase (TERT) genes [19, 20]; (f) acquired somatic genetic lesions that will examined through the process of leukemogenesis.
Leukemogenesis can certainly be defined as a multistep process (Fig. 1) characterized by the succession of the acquisition or loss of genetic alterations which will then define the heterogeneity that characterizes the disease. In fact, during life HSCs undergo some genetic insults that lead to the acquisition of mutations, called founder mutations, which however are not a sufficient condition for the development of AML but rather to a pre-leukemic condition of cells defined as preleukemic stem cell (pre-LSCs) [21, 22].
Founder mutations mostly affect genes involved in epigenetic regulation. It has in fact been documented that the first mutational events compromise the correct functionality of DNA methyltransferase 3a (DNMT3A), isocitrate dehydrogenases 1 and 2 (IDH1/2), ten-eleven translocation 2 (TET2) and ASXL transcriptional regulator 1 (ASXL1) compromising therefore the maturation of blasts and promoting the ability of self-renewal and clonal expansion [23, 24]. When a pre-LSCs unfortunately undergoes a mutational event responsible for the genesis of AML, this is defined driver mutation. De facto, these genetic lesions occur temporally following the founder mutations [25], and confer proliferative advantages to tumor cells by impairing normal apoptotic activity compromising the function of FMS-like tyrosine kinase 3 (FLT3) [10], neuroblastoma RAS viral oncogene homolog (NRAS) [26], nucleophosmin (NPM1), and TP53 [27, 28]. Leukemogenesis is hence a process that involves the deregulation of several pathways. Genes commonly mutated in AML can be grouped into 8 different categories which include 1) genes involved in signal transduction 2), tumor suppressors, 3) genes responsible for DNA methylation and 4) chromatin modifications, 5) myeloid transcription factors, 6) nucleophosmin, 7) genes related to the spliceosome complex, and 8) to the cohesine complex (Table 2).

Leukemogenesis is a multistep process in which normal hematopoiesis is impaired by the accumulation of preliminary mutational events, founder mutations, which characterize the Pre-SLC state. The SLC condition develops following mutational events defined as driver mutations which can give rise to clones resistant to anticancer treatments and therefore responsible for the relapse of the disease (figure edited with biorender.com)
How to classify AML: AML subtypes
Over the years, different classification schemes have been developed for all the various forms of acute myeloid leukemia. This because the development of new molecular biology based techniques for the leukemic cells classification: microarray gene expression, DNA and RNA sequencing. There are 3 major systems that are used to classify AML into subtypes. The French-American British classification was in use earlier and has been replaced by the newer World Health Organization classification and in parallel with the guidelines of the European Leukemia Network.
The French-American-British (FAB) classification was developed by a group of French, American, and British leukemia experts in 1976s and it has been used up to 2001 [29]. This classification included the division of AML into eight subtypes (from M0 to M7) in relation to the origin and the level of maturity of cell from which the leukemia developed. In detail, M0 to M5 subtypes comprise hematological disorders that originate from immature white blood cells. AML M6 subtype has its beginning from very immature red blood cells, while the subtype M7 originates from immature megakaryocytes [30]. Subsequently, over the years, changes have been made to the FAB classification thanks to the discovery of various genetic factors involved in the pathology (Table 3).
However, more recent classification schemes, based on molecular and prognostic scoring systems, have replaced the FAB classification.
After the advent of the World Health Organization (WHO) classification in 2001, AML were classified according to this more modern system, revised in 2008 with the 4th edition [31] and then in 2016 with the 5th edition [32].
If FAB classification has some problems because it does not take into consideration various factors that may affect the prognosis, WHO classification integrates different categorizing aspects such as clinical, morphologic, immunophenotypic, and genetic features. This approach was taken in an attempt to define clinically relevant biological entities in order to incorporate new knowledge about these disorders to gain a better patient perspective [8]. WHO then proposed a newer system to classify AML with minimum of 20% of blasts in BM or blood to diagnose AML (FAB classification requires 30% of blasts). An important distinction was to detach de novo AML, from secondary AML developing from myelodysplastic syndrome, as well as subtypes of therapy related disease.
Many of these revisions involved prognostication derived from gene expression analyses and next generation sequencing studies according whose six categories of AML were identified: (1) categories encompass AML with recurrent genetic aberrations, (2) AML with myelodysplasia related changes, (3) therapy related myeloid neoplasms, (4) AML not otherwise specified (NOS), (5) myeloid sarcoma, (6) myeloid proliferations related to Down Syndrome. Moreover, a new category, the myeloid neoplasms with germline predisposition, was added to incorporate the subgroup of familial AML associated with germline mutations (e.g., germline RUNX1, GATA2, CEBPA) (Table 3).
In 2022, the European Leukemia Network (ELN-Net) updated the 2017 recommendations for the diagnosis and management of AML in adults [9]. This revision aimed to correlate genetic abnormalities with clinical variables and prognostic impact, leading to the reclassification of risk stratification. The ELN-Net continued to group patients into three risk categories: favorable, intermediate, and adverse risk. However, certain changes were introduced to reflect new insights into AML disease biology and risk assessment [33].
One significant change in the ELN2022 classification is the categorization of CEBPA mutations as favorable risk. Now, CEBPA mutations are restricted to in-frame mutations in the basic leucine zipper (bZIP) region, whether they occur as mono- or biallelic mutations (Table 3). Additionally, the previous division based on high or low FLT3-ITD allelic ratio (AR) has been abandoned. All patients with FLT3-ITD are now placed in the ELN2022 intermediate risk group, irrespective of the presence or absence of an NPM1 mutation. NPM1 mutations continue to indicate favorable outcomes, except when co-occurring with adverse risk cytogenetics, which now places them in the ELN2022 adverse risk group. Furthermore, the definition of a complex karyotype has been updated to exclude hyperdiploid karyotypes with multiple trisomies from this group.
In the ELN2017 classification, mutations in ASXL1, RUNX1, and TP53 were introduced as new adverse risk prognostic factors. Now, in ELN2022, so-called myelodysplasia-related gene mutations in BCOR, EZH2, SF3B1, SRSF2, STAG2, U2AF1, or ZRSR2 are additional markers defining ELN2022 adverse risk, when not accompanied by favorable risk genetics. Moreover, a 10% variant allele frequency (VAF) threshold for TP53 mutations has been established to assign individuals to ELN2022 adverse risk [9].
Therapies used to contrast AML evolution
Standard therapies. In the United States, the incidence of AML is 4.3 per 100,000 people with an average age at diagnosis of 68 years and similar statistics were also found in Europe with 3.7 per 100,000 people [34]. Among all subtypes of leukemia, AML is the one with the highest percentage of poor prognosis, accounting for about 62% of cases according to SEER database [35]. Although about 50 years ago AML was considered an incurable disease, today about 35–40% of cases under the age of 60 have a favorable prognosis while unfortunately remains dismal with a cure rate of around 5–15% for geriatric patients [36]. In general, little has changed regarding the therapeutic approach to AML for decades. In fact, the treatment involves a first chemotherapy approach called induction therapy while the post-remission strategy involves consolidation therapy with intensive chemotherapy treatment as well as hematopoietic stem cell transplantation (HSCT).
Induction therapy provides the typical “7 + 3” treatment defined in this way as it involves the continuous infusion of Cytarabine (Ara-C) for 7 days combined with 3 days of Anthracycline (Idarubicin, Daunorubucin, Mitoxantrone) [37, 38]. This therapeutic approach has a fairly good response in patients younger than 60 years, reaching a complete remission between 60% and 85% of cases, however capitulating considerably in patients over 65 years where the response rate to therapy is about 50% and complete remission (CR) of approximately 10% of cases [36]. This is likely due to the fact that older patients may have collected a greater number of genetic and cytogenetic abnormalities, as well as the comorbidity of clinically significant conditions. An example is given by genetic lesions in TP53, the most important tumor suppressor protein that regulates cellular response to various stresses, which lead to greater resistance to chemotherapeutic agents with consequent tumor progression and poor prognosis [39]. It was also attempted to assist the chemotherapy action with humanized CD33 antibodies such as Gentuzumab Ozogamicin (GO), obtaining significantly improved event-free survival of newly diagnosed AML pediatric patients or whose with favorable and intermediate cytogenetic-risk disease but poor results with those with adverse-risk [40, 41].
As mentioned above, post-remission strategies involve consolidation treatment with intensive chemotherapy and allogenic HSCT.
The first gives good results in patients under the age of 60 and with more favorable ELN genetic profile with a rate cure that is between 60 and 70%. This treatment involves a variable regimen between 2 and 4 cycles of Ara-C with an intermediate dose (IDAC) between 1000 and 1500 mg/m2. Clinical studies have shown that increasing the dose of Ara-C for the treatment of AML has no clinical findings [42], although the balance with better results between the number of cycles such as the optimal dose of chemotherapy remains an open discussion. Unfortunately, as extensively treated, patients with unfavorable genetic and cytogenetic characteristics, as well as the presence of other risk factors such as age and the presence of other pathologies, do not show benefits with this type of therapy, indeed the risks tend to be greater than the benefits.
Allogenic HSCT provides the most incisive effects against cancer thanks to the immunologic anti-leukemic graft versus leukemia effect [43]; AML is in fact the most frequent indication for transplantation [44, 45]. It benefits those patients in whom, regrettably, minimal residual disease (MRD) monitoring shows incomplete remission with conventional chemotherapy approaches [46, 47]. Likewise, in this case, geriatric patients present problems in the implementation of the transplant, and in fact only a small fraction of them are eligible by carefully balancing the relationship between risks and benefits. Normally allogeneic HSCT is indicated in those patients whose risk of relapse is between 35 and 40% and is the only treatment option for patients with primary refractory disease [48] (Table 4).
Maintenance therapy is the third phae of treatments, and it is intended to reduce the risk of recurrence in patients who have achieved CR following remission with intensive chemotherapy treatment. While this treatment approach lacks a universal definition, the FDA characterizes it as an extensive but limited and less toxic treatment regimen [9]. In the past 30 years, the approach to maintenance therapy in AML has shifted from using chemotherapeutic agents to employing targeted therapies and enhancing immune system modulation [49]. When devising maintenance therapy for AML, it is crucial to consider potential additional toxicities and the patient’s quality of life. An ongoing trial at Md Anderson Cancer Center is exploring these considerations, employing a genomics-driven approach to study different combinations of oral maintenance therapy in AML (NCT05010772) [50]. This trial involves adult patients in first remission, who will receive various oral decitabine-based regimens for up to 24 cycles, based on their specific induction therapy and transplant eligibility. It is now recommended maintenance therapy for all AML patients through ongoing clinical trials. In cases of CBF-AML, parenteral decitabine is advised when designated cycles of certain regimens cannot be completed or when persistent molecular MRD is observed. For intermediate and adverse-risk AML, HSCT is preferred, followed by appropriate maintenance. For patients unable to proceed to HSCT, a combination of HMA +/- venetoclax is suggested. In patients with targetable mutations, corresponding inhibitors are continued as maintenance therapy after remission induction.
Over the past 25 years, the approach to AML maintenance has evolved from low-intensity chemotherapy to targeted therapies and immunotherapy. While high-risk AML cases generally benefit from maintenance therapy, ongoing trials will determine its potential benefits for less adverse-risk AML. It is important to consider the possibility of exacerbating genomic instability and clonal escape when designing such regimens.
New perspectives. Thanks to the advent of new broad-spectrum molecular investigation technologies such as NGS, the evidence of the heterogeneity that characterizes almost all diseases, and in particular AML, has made it possible to overcome the “one-size-fits-all” concept typical of the old chemotherapeutic approach, which led to a low response rate invalidating the restoration of normal hematopoiesis being toxic to HSCT even in AML with good prognosis.
Now, by reason of the discovery of various genetic factors characterizing the disease, it is possible to use them as therapeutic targets both with inhibitory drugs and/or immunotherapeutic treatments already present and approved for AML or other diseases. The characterization of cellular heterogeneity therefore allows the development of further drugs and cell therapies that can treat the patient more appropriately, overcoming potential side-effects.
From some years, and increasingly in the future, the focus has been on a therapy tailored to the patient according to the molecular characteristics that differentiate the same disease in different patients.
These new therapeutic targets include (a) suppressor and oncogenic proteins target therapies, (b) protein kinase inhibitors, (c) epigenetic modulators, (d) chemotherapeutic agents, (e) mitochondrial inhibitors, (f) antibodies and immuno-therapies, (g) therapies that target the microenvironment that supports the maintenance and expansion of leukemic cells.
Genetic alterations of FMS-Like Tyrosine Kinase 3 (FLT3) characterize about 25–30% of AML cases [51] as well as several solid tumors such as lung adenocarcinoma and gastrointestinal cancer [52]. 2017 and 2018 were 2 prolific years for FLT3 inhibitors since the first generation inhibitor Midostaurin, and then the next generation inhibitor Gilterinib, were approved by the US Food and Drug Administration (FDA).
Midostaurin was approved following the good results obtained from the CALGB10603 or RATIFY study published by Stone in 2017 [53,54,55] which showed a significant 7.2% increase in OS in relation to addition of Midostaurin to induction and consolidation therapy followed by a year of Midostaurin maintenance therapy. This small molecule with inhibitory activity has been shown to be effective with up-front AML targeting both AML with internal tandem duplication (FLT3-IDT) and those carrying mutations in the tyrosin kinase domain (FLT3-TKD).
Gilterinib received FDA approval at the end of 2018 when the ADMIRAL study published the results of the efficacy of this next generation inhibitor against r/r FLT3-ITD AML increasing OS by 9.3 months [56, 57]. It should also be mentioned how first generation inhibitors such as Sunitinib (SU11248), Midostaurin (PKC412), lestaurtinib (CEP-701), and Sorafenib (BAY43-9006) have initiated the development of new generation inhibitors such as Gilterinib, Crenolanib or Quizartinib[58, 59]. The inhibitory action of monoclonal antibodies such as LY3012218 [60], a novel bispecific antibody IgG-based FLT3xCD3 for the treatment of AML [61], is also studied.
Mutations in Isocitrate dehydrogenase 1 and 2 (IDH1 and IDH2) were found in approximately 7–14% and 8–19% of patients with AML respectively [62] as well as in solid tumors such as glioma, chondrosarcoma and cholangiocarcinoma [63]. Impairment of the correct function of IDH1/2 leads to the accumulation of the oncometabolite R-2-hydroxyglutarate with consequent epigenetic alterations that affect correct hematopoiesis. In 2017 and 2019 the US FDA approved Enasidenib AG-221 for IDH2 mutated AML in adult relapsed/refractory (r/r) patients, and Ivosidenib AG120 in patients with IDH1 mutations over 75 years of age or not eligible for standard chemotherapy treatment.
For both, data have been published that attest to an overall response rate (ORR) of 40% with an average increase in overall survival (OS) of 9 months [64, 65]. However, both show adverse effects associated with differentiation syndrome such as dyspnea, fever, pulmonary infiltrates and hypoxemia [64, 66].
Mutated IDH patients treated with a combinatorial regimen with Azacytidine together with Venetoclax [67] appear to have good prospects.
B-Cell Lymphoma 2
(BCL2) is a mithocondrial key regulator responsible of cell survival [68] which has proved to be a promising target in various neoplasms whose inhibition reactivates the apoptotic process [69, 70]. Venetoclax was highlighted as a promising drug for the treatment of r/r AML with an ORR of 19% [71, 72]. Further trials have then demonstrated the efficacy of the antitumor action of Venetoclax combined with other therapeutic agents. For example, in the NCT02203773 study a CR of 54% was found in AML patients treated with Venetoclax in combination with Decitabine or Azacytidine [73]. Encouraging results were also detected from the combination with low dose Ara-C (LDAC). In fact, the NCT02287233 study showed that 21% of patients over 60 years of age ineligible for classic chemotherapy [74] achieved excellent CR rates. Over the years, other combinatorial approaches have also been tried, assisting the synergistic action of different drugs. An example is a study with Trametinib, an inhibitor of the MEK tyrosine kinase, that stopped in phase 2 because data published in June of this year unfortunately did not show significant improvements in the pathological condition [75].
It is now evident how aberrant activation of Hedgehog (HH) signaling pathway is associated with a wide variety of neoplasms [76] promoting growth, migration and stemness. Furthermore, the expression of the transcription factor Glioma-associated oncogene homolog 1 (GLI) and Smoothened (SMO) are connected to the promotion of treatment resistance survival in AML [77, 78]. Current treatment strategies aim to inhibit GLI signaling by targeting SMO in cancer cells. Glasdegib is a SMO inhibitor approved by the FDA in 2018 for the treatment of AML in combination with LDAC. Data from the phase 3 study showed a significant improvement in patients over 75 years old ineligible for standard intensive chemotherapy who achieved a remission of 17% versus 2.3% and an OS of 8.3 versus 4.3 months when the treatment is done with LDAC only [79, 80].
Further in vitro research lines have revealed that synthetic Benzimidazole Mebendazole (MBZ) mediates its anti-leukemic effects via the inhibition of HSP70/90 chaperone activity and the promotion of the degradation of GLI transcription factors by the proteasome pathway [81].
Tumor Protein P53
(TP53) is a crucial tumor suppressor that maps to the short arm of chromosome 17 [82]. De novo TP53 mutation or deletions are quite rare, about 10% in newly diagnosed AML, while they are more common in secondary therapy-related AML [10]. The range of mutations is very heterogeneous and often in conjunction with other genetic alterations involved in epigenetic regulation: DNMT3A and TET2, RAS / MAPK signaling (NF1, KRAS / NRAS, PTPN11), and RNA splicing (SRSF2) [83]. These genetic alterations are responsible for the resistance to DNA damaging chemotherapy agents [84].
Significant progress has been made by restoring the functional activity of TP53 with the agent Eprenetapopt (APR-246) in combination with Azacytidine, reaching phase 3 of the NCT03072043 clinical trial yielding high rates of clinical response and molecular remissions [85].
There are also encouraging data regarding clinical trial NCT04214860 that is in phase 1. Triplet regimen with Eprenetapopt, Venetoclax and Azacytidine demonstrated highly encouraging efficacy showing CR rate of 37% [86].
Novel agents for the treatment of AML
Mouse Double Minute proteins
(MDMs) are E3 ligase that negatively regulate TP53 [87] via its proteasomal degradation. MDM2 is a potential therapeutic target investigated in the MIRROS clinical trial (NTC02545283) by administering the MDM2 antagonist molecule Idasanutlin to patients with r/r AML concomitantly with Ara-C treatment.
Published data show that the addition of Idasanutlin, despite significantly improving the ORR from 22.0 to 38.8%, proved to be ineffective in increasing the OS or CR rates in patients with r/r AML [88].
Another recently published study showed that DNMT3A-mutant samples had an overexpression of MDM4. ALRN-6924 a MDM2/4 inhibitor impairs the growth of DNMT3AWT/R882X cells by inducing cell cycle arrest through the upregulation of TP53 target genes [89].
An additional potent MDM2 inhibitor is APG-115 that is being tested for patients with solid tumors, and has shown an optimal antileukemic activity in vitro and in xenograft models, both alone and synergically with standard-of-care hypomethylating agents Azacytidine and Decitabine, or the DNA-damaging agent Ara-C [90].
Another enzyme involved in the phosphorylation of TP53 and in the assembly of the mitotic spindle is the serine-threonine Aurora Kinase whose expression levels were found to be elevated in leukemic cells [91, 92].
In vitro studies have shown an increase in apoptosis and aneuploidy following anomalies in the formation of nuclei when Aurora kinase was inhibited using the small molecule antagonist MLN8054 [93].
This enzyme has thus emerged as a hypothetical therapeutic target against which several inhibitors such as Alisertib (MLN8237), Barasertib (AZD1152) have been developed. However, clinical studies both in single therapy and in combination with other therapeutic agents such as Ara-C and idarubicin have yielded discordant results [94, 95].
Promising in vitro results have been published about the cytotoxicity of these inhibitors in leukemic cells carrying the 8;21 translocation with AML1-ETO gene fusion [96].
Polo-Like Kinase
(PLKs) is a protein found to be overexpressed in AML whose inhibition in preclinical studies has shown to promote the arrest of the cell cycle and the reactivation of the apoptotic process [97, 98].
Among the various PLK inhibitors, volasertib has been studied most extensively in the clinic. Although phase 2 results of a clinical trial demonstrated improved OS in newly-diagnosed unfit AML patients through co-administration of volasertib to LDAC, it was not possible to confirm results in a larger subsequent phase 3 trial [99].
The Phase 1 dose escalation trial of Volasertib in combination with Decitabine has instead shown to have good results with an ORR of 23% and relative tolerated side effects from patients [100].
Onvansertib (NMS-P937) is another PLK1 inhibitor. It has a shorter half-life than Volasertib, which exhibited antitumor activity in both solid and hematologic cancer models including AML xenografts. For the moment, it has been shown to have synergistic activity with Ara-C in vitro [101].
Aberrant action of the methyl transferase Disruptor of Telomeric Silencing 1-Like (DOT1L) occurs following rearrangements in the long arm of chromosome 11 which occurs in about 2–11% of AML cases [102, 103] and promotes the overexpression of some genes involved in the leukemogenesis including HOXA9 and MEIS1 [104,105,106]. It is therefore a good target candidate. In fact, inhibitory molecules have been created such as Pinometostat (EPZ-5676) and multi-kinase inhibitor Sorafenib whose combined action has been shown to have significant cytotoxic levels in vitro both in cell lines and primary cell cultures from pediatric AML patients [107].
SNDX-5613 and KO-539 are small inhibitory molecules still in the primeval phase of study (NTC04067336, NTC04065399) which appear to have promising therapeutic effects and that have been granted orphan drug designation by the FDA for treatment of r/r AML. Published data show an ORR of 55% for SNDX-5613 [108,109,110].
Recently, Heikamp and colleagues demonstrated that mouse leukemia cell lines driven by NUP98-HOXA9 and NUP98-JARID1A fusion oncoproteins are sensitive to the menin-MLL1 inhibitor VTP50469 by significantly increasing the OS of mice engrafted with cells from leukemia patients with genetic rearrangements above [111]. Table 5 summarizes possible therapeutic interventions against AML and perspectives and novel agents for the AML treatment.
Single cell analysis
NGS/single cell approaches allowed the improving of the risk classification of AML. It moved from the FAB morphological classification in favor of the molecular identity card of the ELN [51]. Compared to solid tumors, the number of mutations found in a given AML is much lower and several of them are druggable such as the FLT3 mutations as well as IDH1 and IDH2. Considering this, targeted therapies may be the ultimate weapon in the treatment of AMLs. Unfortunately, single cell approaches evidenced extreme heterogeneity of leukemic blasts that makes difficult the treatment of this pathology.
Single cell RNA/DNA sequencing approaches
While out of the purposes of this review, some information about the methods used to profile single cell expression or DNA alterations may help readers in understanding the importance of these methods in the evaluation of AML heterogeneity, development, and identification of new therapies.
Single cell analyses start from the tissue dissociation to obtain single cells that can be compartmentalized and then analyzed. Tissue dissociation methods are based on mechanical, enzymatic, or a combination of both, dissociation methods to obtain high yields of viable single cells. Dissociation problem is simpler for tissues already dissociated in single cells as the blood.
Dissociated cells are then compartmentalized in small volumes to produce the sequencing library from each cell. Most promising methods for cell compartmentalization are based on microfluidics using nanowells (BD Rhapsody), microvalves (Fluidigim), and droplets (10X Genomics) [112]. The droplet based compartmentalization furnish the best throughput (about 10–30,000 cells analyzed per sample) and is becoming the gold standard for the analysis of single cells. For a discussion of other different methods used for cell compartmentalization see [113].
Here we will explain the gold standard 10X Genomics for genomic and transcriptomic analyses at the single cell level. Droplet compartmentalization creates nanoreactors to retrotranscribe polyadenylated RNAs or to create DNA libraries using tagmentation (ATAC-seq). For the analysis of the RNA, cells are secluded with nanobeads that release within the droplet oligonucleotides composed by a stretch of thymidines to capture the mRNA and specific barcodes to recognize mRNA released from the cell within the droplet. Each oligonucleotide has a specific sequence (UMI) that is used to count the RNA. In fact, it is necessary to amplify the cDNA produced because the amount is insufficient for the next sequencing step. cDNA amplification is based on the SMART-PCR method [114] that in some cases preferentially amplify specific sequences. Therefore, if the aim of the experiment is to understand gene expression, it is important to avoid to base RNA quantification on the number of aligned reads to a specific gene. Using UMI it is possible to have a one-to-one relationship between mRNA and UMI also after the SMART-PCR because they are associated during the retrotranscription and before the PCR amplification (Fig. 2). If researchers are interested in the analysis of chromatin state, it is possible to use transposases within each droplet that target open chromatin allowing its fragmentation and insertion of sequencing primers (ATAC-seq). Finally, using antibody, it is possible to typing the cells basing on their surface proteins.
A problem of this technique is that, unfortunately, not all transcripts released from a single cell can be captured by the oligonucleotides that cover the bead within the microreactors. Therefore, to capture whole transcriptome for a specific call type it is necessary to sequence several types the same cell population and then cluster them basing on specific gene markers [115]. A key challenge in analyzing single cell RNA-sequencing data is the large number of false zeros, where genes actually expressed in a given cell are incorrectly measured as unexpressed. To overcome this problem several bioinformatics approaches were developed for data imputation [116,117,118,119] and allow following analyses (e.g. cell cluster, identification of differentially expressed genes).

Description of the experimental process for RNA sequencing in single cells. A suspension of cells (A) is used to separate each cell into individual reactors. The figure describes the approach based on the formation of microbubbles (B), which contain beads to allow the capture of RNA released by cell lysis within the reactor (C). RNA capture by the bead in the reactor is permitted by covering the beads with oligonucleotides that have a T-tail in their 3’ terminal portion (D). Each bead contains millions of these oligonucleotides that have common sequences (oligod(T) and R1), a unique sequence for each oligonucleotide (UMI) and a different sequence for each bead (cell barcode) (E). The UMIs allow for the digital counting of gene expression because different UMIs can be associated with the same RNA sequence, based on the abundance of the RNA. The cell barcode allows understanding whether the RNAs being evaluated are derived from the same bead, and therefore cell, or from different beads, and therefore different cells. Oligod(T) allows the capture of polyadenylated RNAs and their retrotranscription (F). Once retrotranscriptase (RT) reaches the 3’ terminal of RNA, due to its 3’ terminal transferase activity, it adds 3 cytosines to the cDNA (G). The overhang of C allows binding of the template switch primer (TSP) and continuation of retrotranscription of this primer (H) as well. At the end of retrotranscription, the cDNA will be characterized by having known ends given by R1 and the template switch primer (I and J). This whole process takes place within each reactor and therefore separately for each cell. Since at the end of the retrotranscription the cDNAs will be labeled with the cell barcode, it is possible to destroy the bubbles and continue the rest of the protocol in bulk. To amplify the low amount of RNA released from each individual cell, a PCR is done by exploiting primers complementary to R1 and TSP (K). This will yield a dsDNA with two known ends (L) that can be used for the sequencing of the full length by binding sequencing adapters to the ends of cDNA by using a PCR or can be fragmented and sequenced the portion corresponding to the 3’ end of RNA.
Improvements in AML comprehension thank to single cell analyses
Single cell DNA sequencing. The accumulation of somatic mutations within a tumor causes clonal diversity and is a consequence of therapeutic resistance, recurrence, and poor outcomes in cancer. A precise characterization of clonal diversity may help to move toward a personalized therapy. Single cell DNA sequencing (scDNA-seq) allows the precise discovering of clonal diversity within a tumor mass. Computational inference using variant allele fraction (VAF) data from massively parallel DNA sequencing of bulk tumor samples has been used to infer the clonal architecture of tumors [26, 120, 121]. However, the ability to infer clonal heterogeneity and tumor phylogeny from bulk sequencing data is inherently limited, because bulk sequencing techniques cannot reliably infer mutation co-occurrences and hence often fail in accurately reconstructing clonal substructure. Pellegrino and colleagues demonstrated the feasibility of scDNA-seq from AML samples taking advantage of cell compartmentalization by microfluidics [122]. The same research group profiled DNA sequences from single cells of 154 AML samples enabling them to reconstruct mutational histories [123]. The most frequently detected mutations by scDNA-seq were in NPM1, followed by FLT3 (29% with internal tandem duplication (ITD) and 18% with non-ITD mutations), DNMT3A, NRAS, IDH2, RUNX1, SRSF2, TET2, and KRAS. scDNA-seq detected substantially more FLT3 mutations than bulk-seq [123]. The authors demonstrated that using scDNA-seq it is possible to infer mutational history with a resolution not possible with bulk-seq. By simultaneous single-cell DNA and cell surface protein analysis, they illustrated both genetic and phenotypic evolution in AML. NPM1 or IDH mutations were significantly associated with lower expression of CD34 and HLA-DR, whereas TP53 mutations were associated with higher CD34 expression [123]. The simultaneous analysis of DNA and cell surface phenotypes by DAb-seq over multiple treatment time-points and disease recurrences demonstrated an extreme genotype-phenotype dynamics and the incongruity between blast cell genotype and phenotype in different clinical scenarios [124]. By analyzing samples after therapies (e.g. FLT3 inhibitor-containing or IDH2 inhibitor-containing) it is possible to evaluate changes in the tumor cell population (123). These results may sustain a continuous re-evaluation of the patient to identify alternative therapies that avoid relapse due to cell survive to the therapy. Knowing which cells are prone to survive to specific therapies by using a single cell approach, we can foresee the development of drugs to avoid relapse caused by surviving cells. ScDNA-seq can be performed also on specific portions of DNA. Targeted sequencing of mutational hotspots using 40 amplicons from 8 AML-specific genes and 16 time-points permitted to Peretz and colleagues to identify pathogenic variants not detected by clinical bulk NGS [125]. Again, the single cell approach evidenced polyclonal nature of the samples and the ability of the tumor to respond to treatments by originating new and previously undetectable mutations. Using scDNA-seq Peretz and colleagues demonstrated that RAS pathway mutations are a mechanism of clinical resistance to Quizartinib [125].
An example of the application of scDNA-seq and phenotyping of cell surface receptors was reported by Dillon and colleagues last year. The pairing of cell-surface immunophenotype with scDNA-seq genotyping allowed researchers to fully resolve the relationship between clonal hematopoiesis and AML in the three considered patients [126].
Genetic mutations associated with AML also occur in age-related clonal hematopoiesis, often in the same individual. This makes it difficult to safely assign the detected variants to malignancy. Therefore, it is important to identify functional alterations related with pathologies. In this context RNA sequencing appears to be useful.
Single cell RNA sequencing. Flow cytometry is widely used for exploring cell heterogeneity in leukemia; however, it is limited to the choice of surface markers [127]. RNA expression can be considered as a proxy of protein expression with the advantage respect to protein analysis of analyzing whole transcriptome because of the possibility of amplifying the signal using in vitro transcription [128] or SMART-PCR [114]. Single cell RNA-sequencing (scRNA-seq) is likely to become a method of increasing importance in the clinical diagnostic of hematologic malignancies [129]. Galen and colleagues used scRNA-seq to describe heterogeneity of leukemia cells [130]. They started describing normal BM-derived cells demonstrating that they can be separated in three major lineages of mature blood cells expressing established markers of hematopoietic populations (CD34 for HSC/Prog cells, CD14 for monocytes, and CD3 for T cells), as described in other manuscripts [131,132,133,134,135]. Performing the same analysis, Galen and colleagues did not distinguish normal and leukemia cells from their expression programs although they showed that cell type proportions markedly changed over the clinical course [130]. To distinguish tumor cells from normal cells the authors decided to sequence portions of transcripts that contain AML mutations from single cells and then profile their mRNAs. This method allows the identification of mutations in relation to gene expression (lower expressed genes are difficultly amplified) and in relation to the mutation positioning (those near to the 3’ end are more efficiently detected). The authors showed that mutations were not detected in healthy donors and were markedly decreased in AML patients in clinical remission meaning that cells with detected mutations were depleted from the patients. Interestingly, cells with mutations derived from myeloid axis and were classified as HSC-like, progenitor-like, GMP-like, promonocyte-like, monocyte-like, or cDC-like malignant cells.
Finally, the authors applied long reads obtained from MiniIon sequencing (Oxford Nanopore) to describe new tandem duplication and transcript fusion rearrangements demonstrating the feasibility of this approach also on single cells.
In this work the authors demonstrated that scRNA-seq data are consistent with clinical parameters but revealed more extensive malignant cell diversity than could be appreciated from a limited number of markers. Therefore, the approach provides more detailed information on AML cell types and differentiation states to deeper understand the better treatment to contrast the progression of the pathology.
The integration of scRNA-seq and scDNA-seq permitted to Petti and colleagues[136] to demonstrate that expression heterogeneity relates to subclonal genetic events: a particular expression of a cell correspond to mutationally defined somatic mutations. The same authors also stated that the data revealed transcriptional heterogeneity that occurred independently of subclonal mutations, suggesting that additional factors drive epigenetic heterogeneity. Apparently from this study resulted particularly important the integration of different omics information to better understand the heterogeneity in gene expression patterns.
Another study conducted on 40 de novo AMLs showed that cell groups were less distinct when compared with those of healthy BM with the lack of cell cluster boundaries [137]. In this study The authors showcased that a high expression levels of ribosomal proteins in AML progenitor cells is a predictor of poor prognosis providing a new perspective for the classification of AML or to evaluate the effects of the therapy.
Lefort and colleagues reported that the BMP pathway sustains a permanent pool of LSCs that express high levels of BMPR1B receptor and, upon treatment, evolve to progressively implement an autocrine loop of BMP4, leading to cells resistant to tyrosine kinase inhibitors (TKIs). RNA-Seq analysis of single TKI-resistant LSCs revealed co-activation of the Smad1/5/8 and Stat3 pathways, which could be targeted by blocking BMPR1B/Jak2 signaling. A specific inhibitor of BMPR1B impaired BMP4-mediated protection of LSCs against TKIs [138]. Targeting BMPs could eliminate leukemic cells within a protective BM microenvironment to effectively affect residual resistance or persistence of LSCs in myeloid leukemia. This work sustains the possibility of identifying specific pathways in resistant cells that can be targeted also by already used drugs to better treat patients.
It is known that tumor microenvironment plays an important role in tumor progression and response to therapy. Several studies have used scRNA-seq to investigate tumor microenvironment and immune response in AML. For example, Zhang and colleagues [139] used scRNA-seq data from 128,688 cells to reveal the microenvironment and exhaustion status of T/NK cells in AML. Specific gene expression associated with T/NK cell exhaustion was identified, providing insight into immune dysfunction in AML. Furthermore, Pan and colleagues [140] performed a comprehensive scRNA-seq study in AML samples to identify patterns of immune response to tumor microenvironment, prognosis, and immunotherapy response This study highlights the importance of of aggrephagy-related patterns in tumor microenvironment. It is a kind of selective autophagy to clear protein aggregates. Once the function of molecular chaperone and ubiquitin proteasome is limited or the clearance efficiency of misfolded proteins is lower than the production rate, protein aggregates, and the aggrephagy needs to be activated to degrade them.
Single cell RNA sequencing of bone marrow cells from AML patients allowed the identification of a novel microRNA: hsa-miR-12,462 [141]. They found that overexpression of hsa-miR-12,462 in AML cells significantly decreased their growth rate. This highlights the importance of epigenetic alterations that were discussed also by Duchmann and colleagues [142].
After medical treatments it is possible that some cancer cells remain in the body. Since they are fundamental for relapse it is important to understand if they are present. Minimal residual disease (MRD) refers to the small number of cancer cells that remain in the body after treatment. Their identification is difficult because they do not cause any physical signs or symptoms and often cannot even be detected through traditional methods such as viewing cells under a microscope and/or by tracking abnormal serum proteins in the blood.
Dillon and colleagues developed a targeted RNA-sequencing-based approach for the quantification of MRD in AML using scRNA-seq [143] that permitted to detect all newly approved European Leukemia Network molecular targets for MRD in AML, with a limit of detection as low as 1 in 100,000 cells. This result is comparable to the flow cytometry that usually bases the detection to a reduced number of surface markers. Alternatively, with PCR, it is possible to identify one cancer cell within 100,000 to one million normal cells and next generation sequencing can detect one cancer cell in one million bone marrow cells checked.
Spatial transcriptomic. Lefort and colleagues showed the importance of protective BM microenvironment against the treatment of leukemia [138]. For a review describing the BM microenvironment mechanisms in AML see [144]. Here we want to highlight the fact that the analysis of single cells is based on the loss of cellular interactions and thus the loss of information related to cell-cell relationship and communication. Latterly, the spatial transcriptomic was applied to evaluate alterations in BM. Spatial transcriptomic allows the evaluation of gene expression maintaining tissue structure. It allows RNA sequencing or highlight specific transcripts on a tissue slice [145]. Recently transcriptional map all major BM-resident cell types and their spatial allocation to distinct BM niches was described by Baccin and collaborator [146]. The authors showed that arteriolar and sinusoidal vascular scaffolds represent key sites for the production of factors required for HSC maintenance and differentiation. These sites have central hubs populated with previously unappreciated subpopulations of cells named by the authors Adipo- and Osteo-CAR cells. The model proposed by the authors sustains that the establishment of distinct niches is mediated by the differential localization of professional cytokine-producing cells.
ScRNA-seq provided an improvement in understanding the cellular ecosystem of both leukemic and residual normal hematopoietic cells not possible until a few years ago with bulk RNA sequencing [130, 147].
CAR-T and genomic tools to improve the treatment of AML
With the advent of single cell RNA sequencing it is possible to evidence subpopulation of tumor cells also after the treatment with conventional chemotherapies. This allows to identify their surface antigens that may be recognized by specific immune cells. In this context the immunotherapy techniques may take advantages for the treatment of AML. They are based on vaccine therapy, monoclonal antibodies, checkpoint inhibitors, stem cell transplantation, and Chimeric Antigen Receptor (CAR) T cell therapy. These therapies are discussed in the Winer and Stone’s review [148]. Here we will discuss how the recently advent of CAR-T cell therapy may take advantage from information retrieved from single cell RNA sequencing to avoid relapse or to ameliorate the treatment of AML. CAR-T cell therapies were approved by FDA in 2017 and transformed the treatment of blood cancers. By providing immune cells with the information they need to better recognize cancer cells as foreign and attack them, this type of targeted immunotherapy aims to boost the immune system. The production of CAR-T cells is well described in [149].
CAR-T cell therapies have made great strides against B-cell-derived leukemias and lymphomas, but have been largely ineffective against myeloid cell-derived leukemias. In fact, CAR-T can target not only cancer cells but also normal cells. This is not a judge problem with lymphoid malignancies, such as acute lymphoblastic leukemia and B-cell lymphomas, because diminished ability to produce immunoglobulins can be compensated by replacing them with transfusions. Differently, the elimination of normal myeloid cells affects the ability of the body to respond to infections. Before the study published from Leick and colleagues, CAR-T therapy of AML has been hampered by the lack of suitable antigens and by off-target effects. They identified CD70 as an antigen largely present in AML cells. In a recently published work the team demonstrated that to improve CAR-T therapy of AML condition it is necessary to combine it with drug therapy based on azacitidine. It has the ability to improve the number of CD70 antigens on the surface of cancer cells. Leick and colleagues also engineered CAR-T cells to improve the strength and durability of the tumor-killing effect by stabilizing the binding of the CAR to CD70 [150].
CD70 is not the only antigen against CAR-T cells may work in AML fighting. Table 6 summarizes different clinical trials based on CAR-T.
CD33 is a transmembrane protein of the sialic acid-binding immunoglobulin-like lectin (SIGLEC) family. CD33 is expressed in normal progenitor cells, myeloid cells, and more than 90% of AML cells and has diagnostic and therapeutic capabilities. The recombinant humanized anti-CD33 antibody conjugated to calicheamicin (gemtuzumab ozogamicin; GO) is used for the treatment of AML as the only approved drug. This supports the potential of using CD33 as a target antigen against which CAR-T cells can act. Some in vivo and in vitro studies have demonstrated the antitumor activity of CD33-CAR-T cells against AML cells [151,152,153,154,155,156].
CD38 is a type II transmembrane glycoprotein that is expressed in AML blasts but not in normal human hematopoietic stem cells. To engineer CD38-CAR-T cells against AML cells, the intensity and number of CD38 should be increased. All-trans retinoic acid (ATRA) as a therapeutic factor for the treatment of acute promyelocytic leukemia has the ability to induce CD38 expression in AML cells. It was observed that CD38-CAR-T cell combined with ATRA eliminate the tumor cells [157].
The IL-3 receptor α subunit (IL3Rα) is named CD123 and is overexpressed on leukemic stem cells (LSCs) and AML blasts with no significant expression on normal hematopoietic stem cells. This makes it as a potential therapeutic target but an anti-CD123 neutralizing monoclonal antibody demonstrated insufficient efficacy against AML [158]. CD123-CAR-T cells with ScFv composed of VL and VH from various mAbs presented the low off-tumor toxicity and lysis effect on healthy hematopoietic stem cells compared to CAR-T cells with VL and VH chains of only one mAb [159].
C-type lectin-like molecule-1 (CLL1) is a type II transmembrane glycoprotein overexpressed on differentiated myeloid cells and AML blasts in 92% of AML cases. This allowed to produce monoclonal Ab against CLL1 as well as CLL1-CAR-T cells with an effective therapeutic function against AML along with reducing tumor burden [160].
Lewis Y (LeY) is a carbohydrate tumor-associated antigen related to blood-group members. Due to LeY expression on early myeloid progenitor cells, it can be a proper targeting choice for AML treatment [161]. LeY-CAR-T demonstrated cytolytic response against LeY + tumor cells and high-level production of IFN-γ [162].
Wilms Tumor 1 (WT1) is a zinc-finger transcription factor overexpressed in various hematological disorders [163]. WT1-CAR-T cells were used against WT1+/HLA-A*02:01 + primary tumor cells or cell lines with satisfactory results [164].
CD7 is a transmembrane glycoprotein expressed by leukemic cells like AML (30%) but not by healthy myeloid cells [165]. Due to CD7 expression on T cells it is necessary to engineering CAR-T cells to avoid CD7 expression ad allow targeting of only tumor cells. Reduction of tumor burden indicated that CD7-CAR-T cell prevents systemic leukemia progression making them treatment for refractory or relapsed AML [166, 167].
Natural killer group 2D (NKG2D) is a receptor whose ligands are overexpressed in various hematological malignancies [168]. Autologous first-generation NKG2D-CD3ζ-CAR-T cells were developed by Baumeister et al. [169]. They validated CAR-T cells in AML patients evidencing in one of these a clinical response with a high level of IFN-γ production.
CAR-T cells are important weapons against tumors, but their proliferation, persistence, and anti-tumor functions may decrease encountering some challenges in hematological malignancies. Delivery methods impact on CAR-T activity with the local delivery better than systemic one [170, 171]. In vitro proliferation of CAR-T cells is another problem in the production of these therapeutic compounds also considering the small starting amount of T cells due to treatments that patients have to manage the tumor. Persistence, proliferation, and efficacy of CAR-T are features that researchers have to improve constantly. The incorporation in CAR-T structure of co-stimulatory receptor is a prosperous manner of overcoming poor persistence [172,173,174,175,176]. CAR-T cells may induce side effects like abundant production of cytokines, off target toxicity, anaphylaxis because the presence of murine ScFv, neurotoxicity, and insertional oncogenesis due to lentiviral or retroviral activity. In fact, the production of CAR-T cells is based on lentiviral or retroviral transfection to deliver the CAR gene into T cells. This cause its random insertion in the genome of the host cells potentially causing unwanted genetic side effects.
Currently CAR-T therapies have some limitations (suboptimal T cell quality when isolated from patients who have already been treated with lymphotoxic chemotherapies, poor CAR-T cell persistence, economic barriers for production, quality control of patient-derived CAR-T cells, long time to infusion of CAR-T cells which may reduce overall outcome) and researchers, to augment their efficacy and overcome limitations, have turned to gene-editing technologies such as CRISPR-Cas, transcription activator-like effector nucleases (TALENs) and meganucleaases. The discovery of meganucleases (naturally occurring restriction enzymes that can recognize 12–40 bp DNA sequences) was the initial step towards genome editing, followed by the discovery of zinc finger nucleases (ZFN) in the 1980s [177] CRISPR/Cas9 is the most recent developed robust genome-editing tool with high precision (Fig. 3A) that can substitute lenti- or retro-viruses for the genome modification of T cells [178]. Until now, it was not clinically tested CAR-T energized with CRISPR/CAS9 technique in the AML field probably because it relatively recent development (2012) in comparison with TALEN approach. In fact, phase I clinical trials (NCT01864902, NCT03190278) are ongoing for testing CAR-T cells engineered with TALEN approach [179], developed in 2010, are fusions of a transcription activator-like effector (TALE) and the catalytic domain of the restriction endonuclease FokI. Transcription activator-like effectors (TALEs) are proteins from plant pathogenic Xanthomonas bacteria. TALE proteins contain three functional domains; the key domain for their specific and programmable DNA-binding is a central repeat region composed of tandem repeats of amino acids where position 12 and 13 of each repeat define the DNA binding specificity (Fig. 3B). Endonuclease associated with TALE produces a double strand DNA (dsDNA) break that is processed as in the case of dsDNA break produced by CRISPR/CAS9 tool (Fig. 3). NCT01864902, NCT03190278 clinical trials aim at evaluating the safety and efficacy of CAR-T targeting CD123 in patients with relapsed/refractory AML. TALENS are used to disable the TCRαβ gene T cells use to recognize ’self’ to prevent them from attacking the host.
Limitations in the usage of genomic tools to manipulate the DNA of cells are associated with the frequency of induced mutation and their specificity. It has been reported levels of over 50% of mutations using the best TALEN and CRIPR/CAS9 systems [179, 180]. Several factors affect the off-target effect generated by a nuclease: (a) the frequency of the homologous sequence in the genome, (b) the level of nuclease expression, (c) the duration of nuclease exposure, (d) target site accessibility. This aspect is well discussed in [181]. There are limited paper that identified no off targets of nucleases and several depend on the approach used to identify off targets, but the development of engineered DNA cutting proteins allowed to produce limited effects on off target genomic regions.

Description of gene editing. (A) Cas9 is a protein that can induce double-stranded brakes in a target DNA (blue in the figure). Cas9 is guided at the DNA site through an RNA guide (gRNA) that has a proper 3D conformation and a complementary to a DNA sequence near a PAM motive that is different for different Cas types. (B) Architecture of TALEs. The N-terminal region of a TALE contains a type III secretion signal (T3SS) and four non-canonical repeats (NCR), the C-terminal part a transcription factor binding site (TFB), two nuclear localisation signals (NLS) and an acidic activation domain (AAD). Each TALE also contains a repeat region with a variable number of highly conserved 33-35-aa repeats arranged in tandem. The amino acid sequence of a consensus 34-aa TALE repeat is shown and the amino acids responsible for the DNA specificity of a TALE, the variable repeat di-residues (RVDs), are highlighted. The five most commonly used RVDs and the nucleotides they specify are also shown in the table. In both cases a double strand break in the target DNA sequence is induced. The cell activate repair mechanisms that cause the introduction of an insertion or a deletion at the site where the DNA was broken. If the site is in a coding sequence, the protein will not be produced because the introduction of wrong codon stops
Conclusions
Already the philosophers of Ionian Greece of the 7th century B.C. they conceived the current of thought called Atomism assuming a plurality of fundamental constituents at the origin of physical matter, which would tend to aggregate and disrupt.
In the history of medicine and biology, immense strides have been made in the understanding of the functionality and architecture of the human body. Above all in the last century the progression of science and knowledge had a sudden climb providing the world with sensational discoveries in ever shorter periods of time: in 1953 the structure of DNA [182], DNA sequencing in 1977 [183, 184] in 1984 the PCR molecular technique which completely carried out the genetic investigations [185] in 2003 the sequencing of the human genome [186], in 2008 the high throughput NGS methods [187,188,189], in the 10s of the new millennium the advent of single cell analysis techniques [112], in 2014 the innovative gene editing technology CRSPR/CAS9 [190].
It is therefore now clear how the ancient thought of the Atomists can approach the reality of the biology and pathology of the tissues of the human body. Returning to the Lewis Caroll quotation with which we started this paper, “it’s a great puzzle”, the large and complicated puzzle that represents the tumour heterogeneity that characterizes, in this case AML, can be completed thanks to the advent of the new single cell investigation techniques.
Several studies have investigated genome or transcriptome alterations of r/r AML. These analyses provided an exceptional contribution in solving the clonal evolution of the disease, characterizing its molecular patterns, thus allowing us to think about target therapy.
The next step is to exploit single-cell investigation techniques such as scRNA-seq to be able to discriminate the clonal and subclonal composition of the tumor as well as the identification of cells causing relapse after chemotherapy treatments.
The vast panorama of cell-by-cell investigations ranging from proteomics (cytofluorimetry) to genomics (scDNA-seq) and transcriptomics (scRNA-seq) has allowed, and will increasingly allow in the future, to discern the various components of the puzzle represented by the subclonal cellular components constituting the tumor.
The FAB, WHO and ELN characterization of the molecular profiles of AMLs has allowed us to stratify the risk of diagnosis and prognosis of these terrible haematological tumours. Increasingly in-depth study and the discovery of further pieces of the puzzle have made it possible to highlight therapeutic targets and therefore the possibility of creating new directed drugs by limiting side effects as much as possible and ameliorating the prognosis. The development target drugs, antibodies and CAR-T treatments is also crucial, for which there are great expectations for the future.
Technological innovation regarding the so-called omics sciences has the massive power to outline a molecular identity card of human body allowing, when necessary, to customize drug therapy or treatment following the development of diseases.
Data Availability
The data generated are included within the manuscript.
References
Pollyea DA, Jordan CT. Therapeutic targeting of acute myeloid leukemia stem cells. Blood. 2017;129:1627–35.
D. P. Hansemann. (Virchow’s Arch., 1890), vol. 119, pp. 299–326.
Nowell PC. The clonal evolution of tumor cell populations. Science. 1976;194:23–8.
Greaves M, Maley CC. Clonal evolution in cancer. Nature. 2012;481:306–13.
Swanton C. Intratumor heterogeneity: evolution through space and time. Cancer Res. 2012;72:4875–82.
Tomiyasu T, Sasaki M, Kondo K, Okada M. Chromosome banding studies in 106 cases of chronic myelogenous leukemia. Jinrui Idengaku Zasshi. 1982;27:243–58.
Bacher U, Schnittger S, Haferlach C, Haferlach T. Molecular diagnostics in acute leukemias. Clin Chem Lab Med. 2009;47:1333–41.
Arber DA, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–405.
Döhner H, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140:1345–77.
Papaemmanuil E, et al. Genomic classification and prognosis in Acute myeloid leukemia. N Engl J Med. 2016;374:2209–21.
Ding L, et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature. 2012;481:506–10.
Ferrara F, Schiffer CA. Acute myeloid leukaemia in adults. Lancet. 2013;381:484–95.
Tallman MS, et al. Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17:721–49. Acute Myeloid Leukemia.
Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3:730–7.
Lapidot T, et al. A cell initiating human acute myeloid leukaemia after transplantation into SCID mice. Nature. 1994;367:645–8.
Kayser S, et al. The impact of therapy-related acute myeloid leukemia (AML) on outcome in 2853 adult patients with newly diagnosed AML. Blood. 2011;117:2137–45.
Colamesta V, et al. Do the smoking intensity and duration, the years since quitting, the methodological quality and the year of publication of the studies affect the results of the meta-analysis on cigarette smoking and Acute Myeloid Leukemia (AML) in adults? Crit Rev Oncol Hematol. 2016;99:376–88.
Poynter JN, et al. Obesity over the life course and risk of acute myeloid leukemia and myelodysplastic syndromes. Cancer Epidemiol. 2016;40:134–40.
Godley LA. Inherited predisposition to acute myeloid leukemia. Semin Hematol. 2014;51:306–21.
Newell LF, Cook RJ. Advances in acute myeloid leukemia. BMJ. 2021;375:n2026.
Shlush LI, et al. Identification of pre-leukaemic haematopoietic stem cells in acute leukaemia. Nature. 2014;506:328–33.
Abelson S, et al. Prediction of acute myeloid leukaemia risk in healthy individuals. Nature. 2018;559:400–4.
Boila LD, Sengupta A. Evolving insights on histone methylome regulation in human acute myeloid leukemia pathogenesis and targeted therapy. Exp Hematol. 2020;92:19–31.
Pastore F, Levine RL. Epigenetic regulators and their impact on therapy in acute myeloid leukemia. Haematologica. 2016;101:269–78.
Pulikkan JA, Castilla LH. Preleukemia and Leukemia-Initiating cell activity in inv(16) Acute myeloid leukemia. Front Oncol. 2018;8:129.
Welch JS, et al. The origin and evolution of mutations in acute myeloid leukemia. Cell. 2012;150:264–78.
Badar T, et al. Detectable FLT3-ITD or RAS mutation at the time of transformation from MDS to AML predicts for very poor outcomes. Leuk Res. 2015;39:1367–74.
Daver N, Schlenk RF, Russell NH, Levis MJ. Targeting FLT3 mutations in AML: review of current knowledge and evidence. Leukemia. 2019;33:299–312.
Bennett JM, et al. Proposals for the classification of the acute leukaemias. French-american-british (FAB) co-operative group. Br J Haematol. 1976;33:451–8.
Walter RB, et al. Significance of FAB subclassification of acute myeloid leukemia, NOS in the 2008 WHO classification: analysis of 5848 newly diagnosed patients. Blood. 2013;121:2424–31.
Yin CC, Medeiros LJ, Bueso-Ramos CE. Recent advances in the diagnosis and classification of myeloid neoplasms–comments on the 2008 WHO classification. Int J Lab Hematol. 2010;32:461–76.
Khoury JD, et al. The 5th edition of the World Health Organization classification of Haematolymphoid Tumours: myeloid and Histiocytic/Dendritic neoplasms. Leukemia. 2022;36:1703–19.
Herold T, et al. Validation and refinement of the revised 2017 european LeukemiaNet genetic risk stratification of acute myeloid leukemia. Leukemia. 2020;34:3161–72.
Visser O, et al. Incidence, survival and prevalence of myeloid malignancies in Europe. Eur J Cancer. 2012;48:3257–66.
Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM. Epidemiology of acute myeloid leukemia: recent progress and enduring challenges. Blood Rev. 2019;36:70–87.
Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373:1136–52.
Fernandez HF, et al. Anthracycline dose intensification in acute myeloid leukemia. N Engl J Med. 2009;361:1249–59.
Löwenberg B. Sense and nonsense of high-dose cytarabine for acute myeloid leukemia. Blood. 2013;121:26–8.
Yan B, Claxton D, Huang S, Qiu Y. AML chemoresistance: the role of mutant TP53 subclonal expansion and therapy strategy. Exp Hematol. 2020;87:13–9.
Baron J, Wang ES. Gemtuzumab ozogamicin for the treatment of acute myeloid leukemia. Expert Rev Clin Pharmacol. 2018;11:549–59.
Pollard JA, et al. Gemtuzumab Ozogamicin improves event-free survival and reduces relapse in Pediatric. J Clin Oncol. 2021;39:3149–60.
Canaani J, et al. Reassessing the role of high dose cytarabine and mitoxantrone in relapsed/refractory acute myeloid leukemia. Oncotarget. 2020;11:2233–45.
Gupta V, Tallman MS, Weisdorf DJ. Allogeneic hematopoietic cell transplantation for adults with acute myeloid leukemia: myths, controversies, and unknowns. Blood. 2011;117:2307–18.
Gratwohl A, et al. One million haemopoietic stem-cell transplants: a retrospective observational study. Lancet Haematol. 2015;2:e91–100.
Niederwieser D, et al. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the Worldwide Network for Blood and Marrow Transplantation Group including the global survey. Bone Marrow Transplant. 2016;51:778–85.
Elsawy M, et al. Prognostic performance of the augmented hematopoietic cell transplantation-specific Comorbidity/Age index in recipients of allogeneic hematopoietic stem cell transplantation from alternative graft sources. Biol Blood Marrow Transplant. 2019;25:1045–52.
Sorror ML, et al. Comorbidity-age index: a clinical measure of biologic age before allogeneic hematopoietic cell transplantation. J Clin Oncol. 2014;32:3249–56.
Webster JA, Luznik L, Gojo I. Treatment of AML Relapse after Allo-HCT. Front Oncol. 2021;11:812207.
Senapati J, Kadia TM, Ravandi F. Maintenance therapy in acute myeloid leukemia: advances and controversies. Haematologica. 2023;108:2289–304.
Bhansali RS, Pratz KW, Lai C. Recent advances in targeted therapies in acute myeloid leukemia. J Hematol Oncol. 2023;16:29.
Döhner H, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129:424–47.
Lim SH, et al. The implication of FLT3 amplification for FLT targeted therapeutics in solid tumors. Oncotarget. 2017;8:3237–45.
Stone RM, et al. Midostaurin plus chemotherapy for Acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377:454–64.
Döhner K, et al. Impact of NPM1/FLT3-ITD genotypes defined by the 2017 european LeukemiaNet in patients with acute myeloid leukemia. Blood. 2020;135:371–80.
Larson RA, et al. Midostaurin reduces relapse in FLT3-mutant acute myeloid leukemia: the Alliance CALGB 10603/RATIFY trial. Leukemia. 2021;35:2539–51.
Perl AE, et al. Gilteritinib or Chemotherapy for Relapsed or Refractory. N Engl J Med. 2019;381:1728–40.
Numan Y, et al. Gilteritinib clinical activity in relapsed/refractory FLT3 mutated acute myeloid leukemia previously treated with FLT3 inhibitors. Am J Hematol. 2022;97:322–8.
Wu M, Li C, Zhu X. FLT3 inhibitors in acute myeloid leukemia. J Hematol Oncol. 2018;11:133.
Zhou F, Ge Z, Chen B. Quizartinib (AC220): a promising option for acute myeloid leukemia. Drug Des Devel Ther. 2019;13:1117–25.
Small S, Numan Y, Platanias LC. Innate Immune Mechanisms and Immunotherapy of Myeloid Malignancies. Biomedicines 9, (2021).
Mehta NK et al. A novel IgG-based FLT3xCD3 bispecific antibody for the treatment of AML and B-ALL. J Immunother Cancer 10, (2022).
Medeiros BC, et al. Isocitrate dehydrogenase mutations in myeloid malignancies. Leukemia. 2017;31:272–81.
Dang L, Yen K, Attar EC. IDH mutations in cancer and progress toward development of targeted therapeutics. Ann Oncol. 2016;27:599–608.
DiNardo CD, et al. Durable remissions with Ivosidenib in IDH1-Mutated relapsed or refractory AML. N Engl J Med. 2018;378:2386–98.
Stuani L et al. Mitochondrial metabolism supports resistance to IDH mutant inhibitors in acute myeloid leukemia. J Exp Med 218, (2021).
Fathi AT, et al. Differentiation syndrome Associated with Enasidenib, a selective inhibitor of mutant isocitrate dehydrogenase 2: analysis of a phase 1/2 study. JAMA Oncol. 2018;4:1106–10.
Pollyea DA, et al. Impact of Venetoclax and Azacitidine in Treatment-Naïve patients with Acute myeloid leukemia and IDH1/2 mutations. Clin Cancer Res. 2022;28:2753–61.
Ruvolo PP, Deng X, May WS. Phosphorylation of Bcl2 and regulation of apoptosis. Leukemia. 2001;15:515–22.
Ashkenazi A, Fairbrother WJ, Leverson JD, Souers AJ. From basic apoptosis discoveries to advanced selective BCL-2 family inhibitors. Nat Rev Drug Discov. 2017;16:273–84.
Hafezi S, Rahmani M. Targeting BCL-2 in Cancer: advances, Challenges, and perspectives. Cancers (Basel) 13, (2021).
Stilgenbauer S, et al. Venetoclax in relapsed or refractory chronic lymphocytic leukaemia with 17p deletion: a multicentre, open-label, phase 2 study. Lancet Oncol. 2016;17:768–78.
Guerra VA, DiNardo C, Konopleva M. Venetoclax-based therapies for acute myeloid leukemia. Best Pract Res Clin Haematol. 2019;32:145–53.
DiNardo CD, et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 2019;133:7–17.
Wei AH, et al. Venetoclax Combined with Low-Dose Cytarabine for previously untreated patients with Acute myeloid leukemia: results from a phase Ib/II study. J Clin Oncol. 2019;37:1277–84.
Desikan SP et al. A phase II study of azacitidine, Venetoclax and Trametinib in Relapsed or Refractory AML harboring RAS Pathway-Activating mutations. Acta Haematol, (2022).
Teglund S, Toftgård R. Hedgehog beyond medulloblastoma and basal cell carcinoma. Biochim Biophys Acta. 2010;1805:181–208.
Wellbrock J, et al. Expression of hedgehog pathway Mediator GLI Represents a negative prognostic marker in human acute myeloid leukemia and its inhibition exerts Antileukemic Effects. Clin Cancer Res. 2015;21:2388–98.
Latuske EM, et al. Combined inhibition of GLI and FLT3 signaling leads to effective anti-leukemic effects in human acute myeloid leukemia. Oncotarget. 2017;8:29187–201.
Cortes JE, et al. Randomized comparison of low dose cytarabine with or without glasdegib in patients with newly diagnosed acute myeloid leukemia or high-risk myelodysplastic syndrome. Leukemia. 2019;33:379–89.
Cortes JE, et al. Glasdegib plus intensive/nonintensive chemotherapy in untreated acute myeloid leukemia: BRIGHT AML 1019 Phase III trials. Future Oncol. 2019;15:3531–45.
Freisleben F et al. Mebendazole mediates proteasomal degradation of GLI transcription factors in Acute myeloid leukemia. Int J Mol Sci 22, (2021).
Hasserjian RP. Revealing the dark secrets of TP53-mutated AML. Blood. 2022;140:8–10.
Tashakori M, et al. TP53 copy number and protein expression inform mutation status across risk categories in acute myeloid leukemia. Blood. 2022;140:58–72.
Hunter AM, Sallman DA. Current status and new treatment approaches in TP53 mutated AML. Best Pract Res Clin Haematol. 2019;32:134–44.
Sallman DA, et al. Eprenetapopt (APR-246) and azacitidine in. J Clin Oncol. 2021;39:1584–94.
Garcia-Manero, Guillermo et al. (Blood, November 23 2021), vol. 138 (Supplement 1), pp. 3409.
Moll UM, Petrenko O. The MDM2-p53 interaction. Mol Cancer Res. 2003;1:1001–8.
Konopleva MY, et al. Idasanutlin plus cytarabine in relapsed or refractory acute myeloid leukemia: results of the MIRROS trial. Blood Adv. 2022;6:4147–56.
Sidorova OA et al. RNAi-Mediated screen of primary AML cells nominates MDM4 as a therapeutic target in NK-AML with. Cells 11, (2022).
Fang DD, et al. MDM2 inhibitor APG-115 exerts potent antitumor activity and synergizes with standard-of-care agents in preclinical acute myeloid leukemia models. Cell Death Discov. 2021;7:90.
Glover DM, Leibowitz MH, McLean DA, Parry H. Mutations in aurora prevent centrosome separation leading to the formation of monopolar spindles. Cell. 1995;81:95–105.
Yang J, et al. CD34+/CD38– acute myelogenous leukemia cells aberrantly express Aurora kinase A. Int J Cancer. 2013;133:2706–19.
Hoar K, et al. MLN8054, a small-molecule inhibitor of Aurora A, causes spindle pole and chromosome congression defects leading to aneuploidy. Mol Cell Biol. 2007;27:4513–25.
Goldberg SL, et al. An exploratory phase 2 study of investigational Aurora A kinase inhibitor alisertib (MLN8237) in acute myelogenous leukemia and myelodysplastic syndromes. Leuk Res Rep. 2014;3:58–61.
Löwenberg B, et al. Phase 1/2 study to assess the safety, efficacy, and pharmacokinetics of barasertib (AZD1152) in patients with advanced acute myeloid leukemia. Blood. 2011;118:6030–6.
Qi J, et al. Selective inhibition of Aurora A and B kinases effectively induces cell cycle arrest in t(8;21) acute myeloid leukemia. Biomed Pharmacother. 2019;117:109113.
Renner AG, et al. Polo-like kinase 1 is overexpressed in acute myeloid leukemia and its inhibition preferentially targets the proliferation of leukemic cells. Blood. 2009;114:659–62.
Goroshchuk O, Kolosenko I, Vidarsdottir L, Azimi A. Palm-Apergi, Polo-like kinases and acute leukemia. Oncogene. 2019;38:1–16.
Döhner H, et al. Randomized, phase 2 trial of low-dose cytarabine with or without volasertib in AML patients not suitable for induction therapy. Blood. 2014;124:1426–33.
Cortes J, et al. Phase 1 dose escalation trial of volasertib in combination with decitabine in patients with acute myeloid leukemia. Int J Hematol. 2021;113:92–9.
Casolaro A, et al. The Polo-Like kinase 1 (PLK1) inhibitor NMS-P937 is effective in a new model of disseminated primary CD56 + acute monoblastic leukaemia. PLoS ONE. 2013;8:e58424.
Schoch C, et al. AML with 11q23/MLL abnormalities as defined by the WHO classification: incidence, partner chromosomes, FAB subtype, age distribution, and prognostic impact in an unselected series of 1897 cytogenetically analyzed AML cases. Blood. 2003;102:2395–402.
Yi Y, Ge S. Targeting the histone H3 lysine 79 methyltransferase DOT1L in MLL-rearranged leukemias. J Hematol Oncol. 2022;15:35.
Nguyen AT, Taranova O, He J, Zhang Y. DOT1L, the H3K79 methyltransferase, is required for MLL-AF9-mediated leukemogenesis. Blood. 2011;117:6912–22.
Chen CW, Armstrong SA. Targeting DOT1L and HOX gene expression in MLL-rearranged leukemia and beyond. Exp Hematol. 2015;43:673–84.
Riedel SS, et al. MLL1 and DOT1L cooperate with meningioma-1 to induce acute myeloid leukemia. J Clin Invest. 2016;126:1438–50.
Lonetti A et al. Inhibition of methyltransferase DOT1L sensitizes to Sorafenib Treatment AML cells irrespective of. Cancers (Basel) 12, (2020).
Wang AJ, Petti t ES, De Botton K, Walter S, Fenaux RP, Burrows P, Tomkinson F, Martell BE, Fathi B. AT. (Blood, 2020), vol. 136(suppl_1):7–8.
Fiskus W, et al. Effective menin inhibitor-based combinations against AML with MLL rearrangement or NPM1 mutation (NPM1c). Blood Cancer J. 2022;12:5.
Bai H, et al. Menin-MLL protein-protein interaction inhibitors: a patent review (2014–2021). Expert Opin Ther Pat. 2022;32:507–22.
Heikamp EB, et al. The menin-MLL1 interaction is a molecular dependency in NUP98-rearranged AML. Blood. 2022;139:894–906.
Luo X, Chen JY, Ataei M, Lee A. Microfluidic compartmentalization platforms for single cell analysis. Biosens (Basel) 12, (2022).
Alessio E, Bonadio RS, Buson L, Chemello F, Cagnin S. A single cell but many different transcripts: a journey into the World of Long non-coding RNAs. Int J Mol Sci 21, (2020).
Hillmann A, Dunne E, Kenny D. cDNA amplification by SMART-PCR and suppression subtractive hybridization (SSH)-PCR. Methods Mol Biol. 2009;496:223–43.
Zheng GX, et al. Massively parallel digital transcriptional profiling of single cells. Nat Commun. 2017;8:14049.
Eraslan G, Simon LM, Mircea M, Mueller NS, Theis FJ. Single-cell RNA-seq denoising using a deep count autoencoder. Nat Commun. 2019;10:390.
van Dijk D, et al. Recovering gene interactions from single-cell data using data Diffusion. Cell. 2018;174:716–729e727.
Huang M, et al. SAVER: gene expression recovery for single-cell RNA sequencing. Nat Methods. 2018;15:539–42.
Li WV, Li JJ. An accurate and robust imputation method scImpute for single-cell RNA-seq data. Nat Commun. 2018;9:997.
Nik-Zainal S, et al. The life history of 21 breast cancers. Cell. 2012;149:994–1007.
Strino F, Parisi F, Micsinai M, Kluger Y. TrAp: a tree approach for fingerprinting subclonal tumor composition. Nucleic Acids Res. 2013;41:e165.
Pellegrino M, et al. High-throughput single-cell DNA sequencing of acute myeloid leukemia tumors with droplet microfluidics. Genome Res. 2018;28:1345–52.
Morita K, et al. Clonal evolution of acute myeloid leukemia revealed by high-throughput single-cell genomics. Nat Commun. 2020;11:5327.
Demaree B, et al. Joint profiling of DNA and proteins in single cells to dissect genotype-phenotype associations in leukemia. Nat Commun. 2021;12:1583.
Peretz CAC, et al. Single-cell DNA sequencing reveals complex mechanisms of resistance to quizartinib. Blood Adv. 2021;5:1437–41.
Dillon LW, et al. Personalized single-cell proteogenomics to Distinguish Acute myeloid leukemia from non-malignant clonal hematopoiesis. Blood Cancer Discov. 2021;2:319–25.
Zeijlemaker W, et al. CD34 Leuk. 2019;33:1102–12.
Baugh LR, Hill AA, Brown EL, Hunter CP. Quantitative analysis of mRNA amplification by in vitro transcription. Nucleic Acids Res. 2001;29:E29.
Pfisterer U, et al. Single-cell sequencing in translational cancer research and challenges to meet clinical diagnostic needs. Genes Chromosomes Cancer. 2021;60:504–24.
van Galen P, et al. Single-cell RNA-Seq reveals AML Hierarchies relevant to Disease Progression and Immunity. Cell. 2019;176:1265–1281e1224.
Hay SB, Ferchen K, Chetal K, Grimes HL, Salomonis N. The human cell Atlas bone marrow single-cell interactive web portal. Exp Hematol. 2018;68:51–61.
Karamitros D, et al. Single-cell analysis reveals the continuum of human lympho-myeloid progenitor cells. Nat Immunol. 2018;19:85–97.
Laurenti E, et al. The transcriptional architecture of early human hematopoiesis identifies multilevel control of lymphoid commitment. Nat Immunol. 2013;14:756–63.
Novershtern N, et al. Densely interconnected transcriptional circuits control cell states in human hematopoiesis. Cell. 2011;144:296–309.
Velten L, et al. Human haematopoietic stem cell lineage commitment is a continuous process. Nat Cell Biol. 2017;19:271–81.
Petti AA, et al. A general approach for detecting expressed mutations in AML cells using single cell RNA-sequencing. Nat Commun. 2019;10:3660.
Wu J, et al. A single-cell survey of cellular hierarchy in acute myeloid leukemia. J Hematol Oncol. 2020;13:128.
Lefort S, Maguer-Satta V. Targeting BMP signaling in the bone marrow microenvironment of myeloid leukemia. Biochem Soc Trans. 2020;48:411–8.
Zhang Z et al. Single-cell RNA-seq reveals a microenvironment and an exhaustion state of T/NK cells in acute myeloid leukemia. Cancer Sci, (2023).
Pan Y, et al. Aggrephagy-related patterns in tumor microenvironment, prognosis, and immunotherapy for acute myeloid leukemia: a comprehensive single-cell RNA sequencing analysis. Front Oncol. 2023;13:1195392.
Jia Y, et al. Roles of hsa-miR-12462 and SLC9A1 in acute myeloid leukemia. J Hematol Oncol. 2020;13:101.
Duchmann M, Laplane L, Itzykson R. Clonal Architecture and Evolutionary Dynamics in Acute Myeloid Leukemias. Cancers (Basel) 13, (2021).
Dillon LW, et al. Targeted RNA-sequencing for the quantification of measurable residual disease in acute myeloid leukemia. Haematologica. 2019;104:297–304.
Pimenta DB, et al. The bone Marrow Microenvironment Mechanisms in Acute myeloid leukemia. Front Cell Dev Biol. 2021;9:764698.
Moses L, Pachter L. Museum of spatial transcriptomics. Nat Methods. 2022;19:534–46.
Baccin C, et al. Combined single-cell and spatial transcriptomics reveal the molecular, cellular and spatial bone marrow niche organization. Nat Cell Biol. 2020;22:38–48.
Witkowski MT, et al. Extensive remodeling of the Immune Microenvironment in B Cell Acute Lymphoblastic Leukemia. Cancer Cell. 2020;37:867–882e812.
Winer ES, Stone RM. Novel therapy in Acute myeloid leukemia (AML): moving toward targeted approaches. Ther Adv Hematol. 2019;10:2040620719860645.
Marofi F, et al. Novel CAR T therapy is a ray of hope in the treatment of seriously ill AML patients. Stem Cell Res Ther. 2021;12:465.
Leick MB, et al. Non-cleavable hinge enhances avidity and expansion of CAR-T cells for acute myeloid leukemia. Cancer Cell. 2022;40:494–508e495.
Pizzitola I, et al. Chimeric antigen receptors against CD33/CD123 antigens efficiently target primary acute myeloid leukemia cells in vivo. Leukemia. 2014;28:1596–605.
Marin V, et al. Cytokine-induced killer cells for cell therapy of acute myeloid leukemia: improvement of their immune activity by expression of CD33-specific chimeric receptors. Haematologica. 2010;95:2144–52.
Wang QS, et al. Treatment of CD33-directed chimeric antigen receptor-modified T cells in one patient with relapsed and refractory acute myeloid leukemia. Mol Ther. 2015;23:184–91.
Kenderian SS, et al. CD33-specific chimeric antigen receptor T cells exhibit potent preclinical activity against human acute myeloid leukemia. Leukemia. 2015;29:1637–47.
Dutour A et al. In Vitro and In Vivo Antitumor Effect of Anti-CD33 Chimeric Receptor-Expressing EBV-CTL against CD33 Acute Myeloid Leukemia. Adv Hematol 2012, 683065 (2012).
Kim MY, et al. Genetic inactivation of CD33 in hematopoietic stem cells to enable CAR T cell immunotherapy for Acute myeloid leukemia. Cell. 2018;173:1439–1453e1419.
Yoshida T, et al. All-trans retinoic acid enhances cytotoxic effect of T cells with an anti-CD38 chimeric antigen receptor in acute myeloid leukemia. Clin Transl Immunology. 2016;5:e116.
Frankel A, Liu JS, Rizzieri D, Hogge D. Phase I clinical study of diphtheria toxin-interleukin 3 fusion protein in patients with acute myeloid leukemia and myelodysplasia. Leuk Lymphoma. 2008;49:543–53.
Thokala R, et al. Redirecting specificity of T cells using the sleeping Beauty System to Express chimeric Antigen receptors by Mix-and-matching of VL and VH Domains Targeting CD123 + tumors. PLoS ONE. 2016;11:e0159477.
van Rhenen A, et al. The novel AML stem cell associated antigen CLL-1 aids in discrimination between normal and leukemic stem cells. Blood. 2007;110:2659–66.
Peinert S, et al. Gene-modified T cells as immunotherapy for multiple myeloma and acute myeloid leukemia expressing the Lewis Y antigen. Gene Ther. 2010;17:678–86.
Neeson P, et al. Ex vivo culture of chimeric antigen receptor T cells generates functional CD8 + T cells with effector and central memory-like phenotype. Gene Ther. 2010;17:1105–16.
Sugiyama H. WT1 (Wilms’ tumor gene 1): biology and cancer immunotherapy. Jpn J Clin Oncol. 2010;40:377–87.
Rafiq S, et al. Optimized T-cell receptor-mimic chimeric antigen receptor T cells directed toward the intracellular Wilms Tumor 1 antigen. Leukemia. 2017;31:1788–97.
Saxena A, et al. Biologic and clinical significance of CD7 expression in acute myeloid leukemia. Am J Hematol. 1998;58:278–84.
Gomes-Silva D, et al. CD7 CAR T cells for the therapy of Acute myeloid leukemia. Mol Ther. 2019;27:272–80.
Gomes-Silva D, et al. CD7-edited T cells expressing a CD7-specific CAR for the therapy of T-cell malignancies. Blood. 2017;130:285–96.
Spear P, Barber A, Rynda-Apple A, Sentman CL. NKG2D CAR T-cell therapy inhibits the growth of NKG2D ligand heterogeneous tumors. Immunol Cell Biol. 2013;91:435–40.
Baumeister SH, et al. Phase I trial of autologous CAR T cells targeting NKG2D ligands in patients with AML/MDS and multiple myeloma. Cancer Immunol Res. 2019;7:100–12.
Kershaw MH, et al. A phase I study on adoptive immunotherapy using gene-modified T cells for ovarian cancer. Clin Cancer Res. 2006;12:6106–15.
Brown CE, et al. Regression of Glioblastoma after chimeric Antigen receptor T-Cell therapy. N Engl J Med. 2016;375:2561–9.
Kowolik CM, et al. CD28 costimulation provided through a CD19-specific chimeric antigen receptor enhances in vivo persistence and antitumor efficacy of adoptively transferred T cells. Cancer Res. 2006;66:10995–1004.
Long AH, et al. 4-1BB costimulation ameliorates T cell exhaustion induced by tonic signaling of chimeric antigen receptors. Nat Med. 2015;21:581–90.
Song DG, et al. CD27 costimulation augments the survival and antitumor activity of redirected human T cells in vivo. Blood. 2012;119:696–706.
Lai Y, et al. Toll-like receptor 2 costimulation potentiates the antitumor efficacy of CAR T cells. Leukemia. 2018;32:801–8.
Mata M, et al. Inducible activation of MyD88 and CD40 in CAR T cells results in controllable and potent antitumor activity in Preclinical Solid Tumor Models. Cancer Discov. 2017;7:1306–19.
Chandrasegaran S, Carroll D. Origins of Programmable Nucleases for Genome Engineering. J Mol Biol. 2016;428:963–89.
Dimitri A, Herbst F, Fraietta JA. Engineering the next-generation of CAR T-cells with CRISPR-Cas9 gene editing. Mol Cancer. 2022;21:78.
Reyon D, et al. FLASH assembly of TALENs for high-throughput genome editing. Nat Biotechnol. 2012;30:460–5.
Wang H, et al. One-step generation of mice carrying mutations in multiple genes by CRISPR/Cas-mediated genome engineering. Cell. 2013;153:910–8.
Yee JK. Off-target effects of engineered nucleases. FEBS J. 2016;283:3239–48.
WATSON JD, CRICK FH. Molecular structure of nucleic acids; a structure for deoxyribose nucleic acid. Nature. 1953;171:737–8.
Maxam AM, Gilbert W. A new method for sequencing DNA. Proc Natl Acad Sci U S A. 1977;74:560–4.
Sanger F, Nicklen S, Coulson AR. DNA sequencing with chain-terminating inhibitors. Proc Natl Acad Sci U S A. 1977;74:5463–7.
Mullis KB, Faloona FA. Specific synthesis of DNA in vitro via a polymerase-catalyzed chain reaction. Methods Enzymol. 1987;155:335–50.
Collins FS, Morgan M, Patrinos A. The Human Genome Project: lessons from large-scale biology. Science. 2003;300:286–90.
Korbel JO, et al. Paired-end mapping reveals extensive structural variation in the human genome. Science. 2007;318:420–6.
Kidd JM, et al. Mapping and sequencing of structural variation from eight human genomes. Nature. 2008;453:56–64.
Wang J, et al. The diploid genome sequence of an asian individual. Nature. 2008;456:60–5.
Doudna JA, Charpentier E. Genome editing. The new frontier of genome engineering with CRISPR-Cas9. Science. 2014;346:1258096.
Acknowledgements
None.
Funding
This research received “Ricerca Corrente” funding from the Italian Ministry of Health to cover publication costs.
Author information
Authors and Affiliations
Contributions
EP and SC wrote the manuscript, MLR and AR revised and provided important intellectual content. All authors contributed to the research and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Peroni, E., Randi, M.L., Rosato, A. et al. Acute myeloid leukemia: from NGS, through scRNA-seq, to CAR-T. dissect cancer heterogeneity and tailor the treatment. J Exp Clin Cancer Res 42, 259 (2023). https://doi.org/10.1186/s13046-023-02841-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13046-023-02841-8