
Abstract
Acute myeloid leukemia (AML) is the most common type of acute leukemia in adults. AML is a heterogeneous malignancy characterized by distinct genetic and epigenetic abnormalities. Recent genome-wide DNA methylation studies have highlighted an important role of dysregulated methylation signature in AML from biological and clinical standpoint. In this review, we will outline the recent advances in the methylome study of AML and overview the impacts of DNA methylation on AML diagnosis, treatment, and prognosis.
Similar content being viewed by others


Background
Acute myeloid leukemia (AML) is characterized by clonal expansion of undifferentiated myeloid precursors, resulting in impaired hematopoiesis and bone marrow failure [1]. AML is a predominantly fatal hematopoietic malignancy with high heterogeneity [2–5]. Genetic heterogeneity has been appreciated in AML since early karyotyping studies [6]. With next-generation sequencing (NGS), genome studies of somatic mutations have shown a comprehensive landscape of AML and contributed to the understanding of the pathogenesis and progression of AML [5, 7–9]. A latest study of 1540 AML patients revealed distinct molecular subgroups that reflect discrete paths in the evolution of AML, informing disease classification and prognostic stratification [5]. It is well established that genetic aberrations play a critical role on the diagnosis, treatment, and prognosis of AML, which is fully reflected in the National Comprehensive Cancer Network (NCCN) guidelines for AML. However, nearly 50% of AML samples have a normal karyotype and many patients carry no mutation [10–12]. Meanwhile, DNA methylation patterns are altered in numerous cancers and often correlate with clinically relevant information such as subtypes, prognosis, and drug response [13–15]. Indeed, aberrant DNA methylation patterns are a hallmark of AML [16–18]. Despite the recognized relationship between DNA methylation and AML, the development of methylome assessment is limited by the lack of rapid, reliable assays that provide validated information. Recently, the advance of technologies, e.g., DNA methylation microarrays and next-generation sequencing [19–25], has made methylome analysis less time-consuming, reproducible, and cost-effective [24, 26], and the genome-wide coverage has been extended to non-CpG island regions, e.g., enhancer, exon, intron, and intergenic [21, 24, 25, 27]. With high accuracy and robustness, DNA methylation analysis has been confirmed to be feasible and reliable in clinical diagnosis and precision medicine, especially for highly heterogeneous diseases such as AML [26, 28, 29]. There are now an increasing number of studies reporting aberrant DNA methylation in AML [30–34], and new methods for detecting DNA methylation on a genome-wide scale have significantly widened our knowledge about aberrant methylation patterns in AML. For example, distinct DNA methylation patterns are used to define AML subgroups and a set of aberrantly methylated genes are identified and linked to the clinical outcome [9, 30, 35]. Additionally, DNA methylation and mutation patterns may occur with distinct kinetics to affect the biological and clinical features of AML [9].
Distinct DNA methylation patterns identified in AML
AML is a highly heterogeneous disease with fewer mutations than most other adult cancers [7]. This difference suggests that other mechanisms, e.g., epigenetics or post-transcriptional regulations to play a pivotal role in determining the biological behavior of the disease. DNA methylation is the major mode of epigenetic modification [36–38], which plays an important role in carcinogenesis (Fig. 1). Aberrant DNA methylation patterns are a characteristic feature of AML [7, 17, 18]. Several studies have evaluated genome-wide methylation in AML [7, 9, 30, 39]. The Cancer Genome Atlas Research Network (TCGA) performed methylation profiling for 192 samples of AML using Illumina Infinium HumanMethylation450 BeadChip and identified significant changes in DNA methylation at 160,519 CpG loci, which accounted for 42% of sites tested, with 67% resulting in hypermethylation and 33% resulting in hypomethylation [7]. A pairwise AML cohort study examining the DNA methylation by enhanced reduced representation bisulfite sequencing (ERBBS) based on NGS platform suggested that global DNA methylation allele shifting was a universal feature of AML relative to normal bone marrow controls [9]. Another detailed study on the genomic DNA methylation landscape profiling using HpaII tiny fragment enrichment by ligation-mediated PCR (HELP) methylation microarrays revealed the existence of 16 distinct DNA methylation patterns in AML [30]. Each of these DNA methylation-defined AML subtypes displayed a unique epigenetic signature when compared with the normal bone marrow CD34+ cells. Though 11 of 16 clusters correspond to AML subtypes defined by the World Health Organization (WHO) or related to specific genetic and epigenetic lesions, 5 new clusters could not be explained based on known morphologic, cytogenetic, or molecular features. In fact, each of these AML subtypes displays a distinct DNA methylation pattern. Although this scenario was previously proposed, the findings represent an important progress made possible by the use of large-scale genome-wide DNA methylation profiling technology.

DNA methylation and deregulation of the genome in carcinogenesis. Methylation of cytosine within CpG dinucleotides is catalyzed by DNMTs. S-adenosylmethionine (SAM) donates methyl groups and is converted to S-adenosylhomocysteine (SAH). In normal cells (lower left), CpG islands are often associated with gene promoters and are resistant to DNA methylation. Gene expression can occur and is highly correlated with high levels of gene body (genic) methylation. CpG-poor regions (intergenic), except for enhancers, are typically methylated, while CpG-poor promoters are silenced by DNA methylation unless gene expression is required in specific tissue. In cancer cells (lower right), CpG islands are prone to DNA hypermethylation, which results in aberrant gene silencing (e.g., of tumor suppressor genes). Concomitant hypomethylation of intergenic regions and CpG-poor promoters contributes to genomic instability and aberrant gene expression (e.g., of oncogenes), respectively. Green circle, unmethylated CpG; purple circle, methylated CpG
Cytogenetically normal AML (CN-AML), which constitutes between 40 to 50% of all AML cases [40], is the most heterogeneous group in AML. Interestingly, a genome-wide differential methylation study in CN-AML using Illumina 450 K methylation array found that the most pronounced changes in DNA methylation occurred in non-CpG island regions, whereas hypermethylation enrichment was only represented in CpG islands [41].
It is foreseeable that future research will provide more clarity and precision to the methylome landscape of AML.
DNA methylation in diagnosis classification of AML
Recent genome-wide studies identified DNA methylation signatures unique for subtypes of AML patients [30], which could be valuable for diagnosis classification of AML [7, 9, 30]. Li et al. [9] examined the epigenetic heterogeneity by ERRBS in serial diagnosis-relapse pairwise AML samples and defined three categories of DNA methylation-shifted loci: loci unique to diagnosis, loci unique to relapse, or loci present at both diagnosis and relapse. This analysis segregated AML patients into three clusters with no significant association with age, white blood cell count (WBC), or the French–American–British (FAB) classification, suggesting that DNA methylation pattern could be an independent diagnosis classification for AML patients. Furthermore, different cytogenetic and molecular subtypes were found to exhibit highly distinct DNA methylation profiles [7, 17, 30, 39, 42], providing a new perspective for diagnosis classification of AML. For cases with t(8;21), inv(16) or t(16;16), t(15;17) or t(v;11q23) translocations, or the presence of the relevant fusion genes, unique DNA methylation signatures can define these AML subtypes [7, 17, 30, 39]. Accentuated DNA hyper- and hypomethylation were both identified in t(8;21)-AML1/ETO and inv(16)-t(16;16)-CBFB-MYH11 by Illumina 450 K, with hypomethylation being the predominant feature. However, almost equally accentuated DNA hyper- and hypomethylation was found in t(15,17)-PML-RARa. Unlike these DNA methylation patterns, a very pronounced DNA hypomethylation signature was found in t(v;11q23)-MLL translocations [7, 30, 33]. It is proposed that the underlying mechanism of aberrant DNA methylation induction in these AML was that these fusion genes might recruit DNA methyltransferases (DNMTs) to their binding site [43–45]. In addition, secondary epigenetic dysregulation might also contribute to the aberrant methylation, which includes the binding of PML-RARa to genomic regions of epigenetic modifiers such as DNMT3A and/or DNA methylation disruption of AML1-ETO target genes [46–48]. In a recent study of 60 acute promyelocytic leukemia (APL) primary samples at diagnosis, methylation of DAPK1, miR-34a and -34b/c were tumor-specific in APL [49]. Hájková et al. reported a novel hypomethylation pattern specific to CBFB-MYH11 fusion resulting from inv(16) rearrangement using targeted bisulfite sequencing in AML patients [42]. They found that average levels of DNA methylation in assigned regulatory regions of MN1, SPARC, ST18, and DHRS3 were significantly lower for inv(16) compared to non-inv(16) AML M4, other AML subtypes, and healthy controls (p < 0.0001).
Apart from translocations or the relevant fusion genes, recurrent mutations (e.g., NPM1, CEBPA, RUNX1) in AML can be defined by DNA methylation differences, especially for mutations in epigenetic regulator genes (e.g., DNMT3A, TET2, IDH1/2) [7, 30, 42]. For NPM1 mutations, four DNA methylation clusters were identified: one hypermethylated and three both hyper- and hypomethylated identified using HELP [30], the strong hypomethylation signature identified using Illumia 450 K [7], and the hypermethylation signature identified using MethylCap-seq [50]. For CEBPA double mutations, the cases could be split to two distinct subtypes with different methylation signatures: one hypermethylated and one hypomethylated identified using HELP [30], and the DNA hypermethylated signature identified using Illumina 450 K [7]. However, discrete hyper- and hypomethylation signatures were showed for RUNX1 mutations using Illumina 450 K [7].
DNMTs (DNMT1, DNMT3A, and DNMT3B) encode methyltransferases that catalyze the addition of a methyl group to the cytosine residue of CpG dinucleotide to maintain methylation status of hematopoietic stem and progenitor cells [51, 52]. DNMT3A is the essential DNA methylation regulator, was thought to have a severe impact on DNA methylation patterns [53, 54]. Mutations in DNMT3A contribute to dysregulation of DNA methylation may result in global shifts in gene expression in hematologic malignancies, which frequently leads to increased self-renewal in blood cells at the expense of normal differentiation [51, 55, 56]. DNMT3A mutations are present in preleukemic hematopoietic stem cells (HSCs), and it is considered an early event in AML [57]. Qu et al. demonstrated that DNMT3A mutations were a main genetic contributor to the global methylation pattern, and two CN-AML subtypes were generated according to the samples with or without DNMT3A mutations [41]. Additionally, Marcucci et al. noted that only DNMT3A-R882 mutations were associated with hypermethylation [50]. Furthermore, TET2 and IDH1/2 mutations resulted in genome-wide DNA hypermethylation signature, especially for IDH1/2 mutations [7, 16, 39, 50]. A meta-analysis also supported the diagnostic value of DNA methylation in leukemia with 41 case-control studies [58]. In this study, 20 genes were found to be aberrantly methylated in the leukemia patients, and CDKN2A, CDKN2B, and ID4 genes were significantly hypermethylated in AML. Though recent studies have identified the relationship between DNA methylation abnormalities and AML variability [17, 30, 39], more details remain to be revealed and many mechanisms remain unclear [17, 59]. Nevertheless, the value of DNA methylation in the diagnosis stratification of AML cannot be underappreciated.
DNA methylation in prognostic stratification of AML
Many studies have found that DNA methylation could predict clinical outcome in AML patients and aberrant DNA methylation can serve as a biomarker for risk stratification (Table 1) [9, 16, 31, 33–35]. However, the results were inconsistent due to the difference in AML cohort, genomic regions analyzed, functions of annotated methylated genes, and methods of detection and analysis. Deneberg et al. [31] reported that global and gene-specific methylation patterns were independently associated with the clinical outcome in AML patients. They analyzed the methylation of CDKN2B, E-cadherin (CDH) and hypermethylated in cancer 1 (HIC1) promoters, and global DNA methylation in 107 AML patients by the luminometric methylation assay (LUMA). They also assessed genome-wide promoter associated methylation using the Illumina HumanMethylation27 array in 20 patients. Multivariate analysis suggested that low global DNA methylation was associated with higher complete response (CR) rate, and increased genome-wide promoter associated methylation was associated with better overall survival (OS) and disease-free survival (DFS). Furthermore, P15 methylation was associated with better OS and PFS, while CDH and HIC1 methylation was not associated with clinical outcome [31].
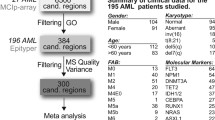
Figueroa et al. analyzed distinct DNA methylation signatures, identified new AML subtypes, and explored the potential use of aberrant DNA methylation as a predictor of important clinical features. With a three-step approach of model development and validation using a large data set, they reported a 15-gene methylation classifier predictive of OS [30]. These results suggested that DNA methylation classifier could serve as a clinically useful biomarker. Luskin et al. [35] recently reported a validated clinical measure of DNA methylation, M score, generated from expedited HpaII small fragment enrichment by ligation-mediated PCR (xMELP) assays [60, 61] that represent a binary prognostic classifier for patients with de novo AML. The M score was robustly associated with CR and OS in both univariable and multivariable models in multiple independent AML cohorts, as well as for AML patients aged ≤60 years with intermediate cytogenetics [35]. A high M score represented a shorter 2-year OS (24 vs 56%) and a lower CR rate (61 vs 84%) compared with a low M score. These findings confirmed the association of M score with clinical outcome, which has been further validated in an independent cohort of patients with APL and secondary AML [62]. Remarkably, the association of M score with clinical outcome was stronger than that of many established prognostic factors, including cytogenetics, FLT3-ITD status, and other genetic lesions. Additionally, the M score classifier also defined subgroups with significantly OS within a traditionally high-risk subgroup with intermediate cytogenetics and FLT3-ITD mutation. These results suggest that DNA methylation can be used for risk stratification, which might decrease the need for comprehensive genetic testing for risk stratification at diagnosis due to its better prognostic performance [35].
Similarly, a recent NGS study pointed out that epigenetic and genetic heterogeneity occurred with distinct kinetics in AML. The changes in DNA methylation burden were independent of the abundance of somatic mutations in patients, and relapsed AMLs showed variable changes in DNA methylation burden, which was antecedent to the genetic evolution. Furthermore, the variance of CpG methylation patterns (measured as EPM) were associated with the time to relapse, whereas the burden of somatic mutations was not. The patients with high EPM at diagnosis had a shorter time to relapse compared to the low-EPM cohort (p = 0.0396), which was most significant for EPM values assessed from promoter-annotated epigenetically shifted loci (p = 0.0077) [9]. The study also detected a specific set of 21 promoter-annotated DNA methylation shifted loci to be associated with a shorter time to relapse, which could be used as outcome biomarkers [9]. Using MethylCap-seq, Marcucci et al. identified 82 individual genes, the promoter different methylation regions (DMRs) of which were associated with OS in a set of older patients with CN-AML [50]. For 80 genes, higher DMR methylation was related to longer OS. Combined with the expression data, a novel seven-gene score for clinical prognosis was generated validated in four independent CN-AML patient sets (n = 355). In multivariable analyses, patients with low scores had a more than 80% increase in the odds of achieving CR and approximately 3.5-fold decrease in the risk of disease relapse or death compared with patients with high scores [50]. Using targeted bisulfite sequencing, Hájková et al. [42] revealed that PBX3 differential methylation could impact on prognosis of AML. They found that the hypomethylation of PBX3 regulatory region was involved in higher relapse rates and shorter relapse-free survival in AML patients with overexpressed PBX3. However, this methylation signature was not related to OS.
DNA methylation in therapeutic decision-making of AML
Variable responses to chemotherapy in AML represent a major treatment challenge, and the ability to predict therapeutic response is essential for improving the care of patients with AML. However, clinical and genetic features incompletely predict outcome, especially for CN-AML and AML with no mutation [10–12]. In general, DNA methylation might only be able to predict the response of hypomethylating agents [63–65]. For example, in a study investigating the impact of global and gene-specific DNA methylation status (promoters of 5 stem cell-related transcription factor genes SOX2, OCT4, KLF4, MYC, and NANO) in AML patients treated with decitabine [65], Zhang et al. showed that patients with a high level of 5-mC had a poor prognosis after demethylation therapy, and higher methylation status of the SOX2 and OCT4 genes was associated with differential response to demethylation therapy. This study found that relatively low methylation percentage in one or both of these two genes was also associated with longer OS after decitabine-based chemotherapy.
In fact, due to the complex epigenetic regulation mechanisms in AML, DNA methylation contributed to the overall biological and clinical features of AML and was also correlated with conventional chemotherapy [35, 66]. A decade ago, Grövdal et al. showed a significant effect of the methylation status of three genes (P15ink4b (P15), E-cadherin (CDH), and hypermethylated in cancer1 (HIC)) on the outcome of conventional chemotherapy using bisulfite-denaturing gradient gel electrophoresis (DGGE) [66]. Luskin et al., as mentioned previously, also assessed the impact of high-dose (90 mg/m2) or standard-dose (45 mg/m2) daunorubicin induction chemotherapy on a cohort AML patients by dividing the patients into low and high M score subgroups. They found that high-dose daunorubicin (90 mg/m2) was beneficial for patients with high M scores but not for those with low M scores. The different responses suggested that M score may be correlated with chemoresistance and could be used for identifying patients that might benefit from high-dose chemotherapy, which will contribute to therapeutic decision-making of AML [35].
In addition, the mutations in genes involved in DNA methylation (e.g., DNMT3A, IDH1/2, TET2) play an important role in genome-wide methylation signature in AML and contribute to the leukemogenesis and prognosis [16, 53, 67–69]. The applications of DNMTs and IDH1/2 inhibitors have been more extensive and improved the outcome of AML via reversing abnormal DNA methylation and restoring normal hematopoiesis [52, 56, 70]. Two DNMTs inhibitors, azacitidine and decitabine, have been approved for MDS and AML due to the increasing data to support the efficacy of these hypomethylating agents (HMAs) [71–76]. Especially, the particular gene mutations, such as those in DNMT3A and TET2 and methylation signatures, may predict for responsiveness to treatment with HMAs according to the studies in MDS [27, 77]. TET2 mutations and/or DNMT3A mutations were independent predictors of better response (p = 0.03) and improved PFS (p = 0.04) [77]. While a 21 selected tile regions revealing the DNA methylation differences can served as an epigenetic classifier that accurately predicted decitabine response at the time of diagnosis [27]. Following this line, it is possible that defined AML subtypes with certain changes associated DNA methylation are more responsive to HMAs than others. With DNA methylation profiling identified in AML subgroups and the evaluation of DNA methylation level with clinical outcome, extending the methylome analysis to comparable studies is of great interest as these results would have immediate implications for design of therapeutic regimens, especially dissect which AML subtypes may benefit from treatment with HMAs [16, 35, 62].
Similar to DNMT3A and TET2 mutations, IDH1/2 mutations also could predict a favorable response with a significantly higher clinical remission rate during treatment with HMAs, and the odds of achieving response with an IDH mutation was 14.2 when compared to patients without an IDH mutation (95%CI, 1.3–150.4) [78]. Furthermore, hypermethylated signature in AML with IDH mutations could be reversed via IDH inhibition [16, 79]. IDH1/2 inhibitors (e.g., IDH305, AG-220, AG-221) have been developed and are already being evaluated in clinical trials (Table 2) [70, 80]. Primary results suggest a prominent effect of these drugs in AML prognosis [81–85]. AG-120, an oral, first-in-class IDH1 inhibitor, has shown the efficacy and safety with determined IDH1 clearance as a single agent in patients with IDH1-mutant hematologic malignancies. The overall response rate (ORR) was 38.5% (30/78) [84]. A phase I study with IDH305 including 21 relapsed/refractory AML subjects enrolled reported similar results that 7 (33%) patients obtained objective responses with a favorable safety profile [83]. AG-221 is an oral first in class inhibitor of the IDH2-mutant protein. Preliminary results of a phase 1/2 study enrolled relapsed/refractory AML patients showed that AG-221 was well-tolerated and -induced responses in heavily pretreated RR-AML. Of the 138 enrolled AML patients, 128 were evaluated for efficacy and the ORR was 41% (52/128) [86]. Therefore, identification of mutations associated DNA methylation and evaluation the change of methylation signature would contribute to individual therapy of AML.
DNA methylation, genetic aberrations, and expression in AML
Genetic lesions and epigenetic abnormalities have been shown to play important roles in AML. Although the relationship of DNA methylation, genetic aberrations, and expression is unclear, it is likely that these parameters are closely related with each other [7, 30, 64, 87–89]. The TCGA study generated a genomic and epigenomic landscapes of AML, which would serve as a foundation for investigations AML pathogenesis, classification, and risk stratification [7]. A recent study by Papaemmanuil et al. identified 5234 driver mutations across 76 genes or genomic regions in 1540 patients with AML. The mutations in genes that encode DNA methylation regulators (e.g., DNMT3A, IDH1/2, TET2) were often acquired the earliest and with a high recurrence rate. Particularly, 73% of the largest class in their cohort, NPM1-mutated AML, also carried mutations in DNA methylation genes (DNMT3A, IDH1, IDH2R140, and TET2). Besides, they identified a subgroup of AML with IDH2R172 mutations [5]. Since these mutations resulted in abnormalities of genome-wide DNA methylation signature, the relationship between genetic aberrations and DNA methylation were inseparable in AML [18, 50, 89]. Furthermore, Taskesen et al. created the three different classification strategies based on gene expression and DNA methylation profiles (GEP and DMP) from 344 well-characterized AML samples [87]. They demonstrated that prediction of known cytogenetic and molecular abnormalities in AML could be further improved by integrating GEP and DMP profiles. Raj et al. also provided insight into the clinical relevance of prognostic mutations and the mutation-associated gene DNA methylation promoter and expression patterns [63]. In a mouse model that has a defined leukemia stem cell population with a characteristic transcriptional and epigenetic profile, it was confirmed that TET2 and FLT3 mutations cooperated to induce AML, and the methylation changes exhibit the cooperation of disease alleles to target multiple loci. The data also suggested that leukemic transformation by these epigenetic changes is reversible and therapies that reactivate silenced genes might improve outcomes for AML patients [88].
Conclusions
DNA methylation is a common theme in acute myelogenous leukemogenesis. With the progress of technologies in identifying DNA methylation [24–26, 28, 29], especially the milestones in data integration, sharing, and analysis strategies, such as the International Human Epigenome Consortium Data Portal (IHEC Data Portal) [90], the BLUEPRINT Data Analysis Portal (BDAP) [91], and the tool for identifying cell type-specific signal in epigenomic data (eFORGE) [92], DNA methylation will be more widely used in clinical practice and become more valuable in diagnosis classification, prognostic stratification, and therapeutic decision-making of AML. This will contribute to the development of precision medicine in AML. Besides, a further understanding of the relationship among DNA methylation, genetic aberrations, and expression might provide unprecedented insights into the pathogenesis of AML (Fig. 2).

Paradigm of integrated DNA methylation, genetic aberrations, and expression of AML leading to precise medicine. The integrated analysis of DNA methylation, genetic aberrations (gene fusions and mutations), and RNA expression (a) has revealed multiple AML subtypes, summarized into two groups (with or without recurrent genetic abnormalities) (b). Furthermore, each subtype will be characterized with distinct DNA methylation patterns (c), which play an important role in clinical implications (d), leading to precision medicine in AML. The clinical implications of DNA methylation are discussed more detail in the text
Abbreviations
- 5-mC:
-
5-Methylcytosine
- AML:
-
Acute myeloid leukemia
- AML1/ETO:
-
AML1 and eight twenty-one rearrangements
- APL:
-
Acute promyelocytic leukemia
- BDAP:
-
The BLUEPRINT Data Analysis Portal
- CBFB-MYH11:
-
Core-binding factor beta and myosin heavy chain 11 rearrangements
- CDH:
-
E-cadherin
- CDKN2A/2B:
-
Cyclin dependent kinase inhibitor 2A/2B
- CEBPA:
-
CCAAT/enhancer binding protein alpha
- CN-AML:
-
Cytogenetically normal AML
- CR:
-
Complete response
- DFS:
-
Disease-free survival
- DGGE:
-
Bisulfite-denaturing gradient gel electrophoresis
- DHRS3:
-
Dehydrogenase/reductase 3
- DMP:
-
DNA methylation profiles
- DMR:
-
Different methylation region
- DNA:
-
Deoxyribonucleic acid
- DNMT3A:
-
DNMT 3 alpha
- DNMTs:
-
DNA methyltransferases
- eFORGE:
-
The tool for identifying cell type-specific signal in epigenomic data
- EPM:
-
The global metric eloci per million loci
- ERBBS:
-
Enhanced reduced representation bisulfite sequencing
- FAB:
-
French–American–British
- FLT3-ITD:
-
Fms-related tyrosine kinase 3 internal tandem duplication
- GEP:
-
Gene expression profiles
- HELP:
-
HpaII tiny fragment enrichment by ligation-mediated PCR
- HIC1:
-
Hypermethylated in cancer 1
- HMAs:
-
Hypomethylating agents
- HSCs:
-
Hematopoietic stem cells
- ID4:
-
Inhibitor of DNA binding 4
- IDH1/2:
-
Isocitrate dehydrogenase (NADP(+)) 1/2
- IHEC:
-
Data Portal the International Human Epigenome Consortium Data Portal
- Klf4:
-
Kruppel-like factor 4
- LUMA:
-
Luminometric methylation assay
- MLL:
-
Mixed lineage leukemia
- MN1:
-
MN1 proto-oncogene, transcriptional regulator
- MYC:
-
v-Myc avian myelocytomatosis viral oncogene homolog
- NCCN:
-
National Comprehensive Cancer Network
- NGS:
-
Next-generation sequencing
- NPM1:
-
Nucleophosmin
- OCT4:
-
Organic cation/carnitine transporter4
- OS:
-
Overall survival
- PBX3:
-
PBX homeobox 3
- PML-RARa:
-
Promyelocytic leukemia and retinoic acid receptor alpha rearrangements
- RUNX1:
-
Runt related transcription factor 1
- SOX2:
-
SRY-box 2
- SPARC:
-
Secreted protein acidic and cysteine rich
- ST18:
-
ST18, C2H2C-type zinc finger
- TCGA:
-
The Cancer Genome Atlas Research Network
- TET2:
-
Tet methylcytosine dioxygenase 2
- WBC:
-
White blood cell
- WHO:
-
World Health Organization
- xMELP:
-
Expedited HpaII small fragment enrichment by ligation-mediated PCR
References
Dohner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–52.
Roboz GJ. Current treatment of acute myeloid leukemia. Curr Opin Oncol. 2012;24(6):711–9.
Grimwade D, Hills RK, Moorman AV, Walker H, Chatters S, Goldstone AH, Wheatley K, Harrison CJ, Burnett AK, National Cancer Research Institute Adult Leukaemia Working G. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council Trials. Blood. 2010;116(3):354–65.
Dohner H, Estey EH, Amadori S, Appelbaum FR, Buchner T, Burnett AK, Dombret H, Fenaux P, Grimwade D, Larson RA, Lo-Coco F, Naoe T, Niederwieser D, Ossenkoppele GJ, Sanz MA, Sierra J, Tallman MS, Lowenberg B, Bloomfield CD, European L. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453–74.
Papaemmanuil E, Gerstung M, Bullinger L, Gaidzik VI, Paschka P, Roberts ND, Potter NE, Heuser M, Thol F, Bolli N, Gundem G, Van Loo P, Martincorena I, Ganly P, Mudie L, McLaren S, O'Meara S, Raine K, Jones DR, Teague JW, Butler AP, Greaves MF, Ganser A, Dohner K, Schlenk RF, Dohner H, Campbell PJ. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374(23):2209–21.
Testa JR, Mintz U, Rowley JD, Vardiman JW, Golomb HM. Evolution of karyotypes in acute nonlymphocytic leukemia. Cancer Res. 1979;39(9):3619–27.
Cancer Genome Atlas Research N. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med. 2013;368(22):2059–74.
Welch JS, Ley TJ, Link DC, Miller CA, Larson DE, Koboldt DC, Wartman LD, Lamprecht TL, Liu F, Xia J, Kandoth C, Fulton RS, McLellan MD, Dooling DJ, Wallis JW, Chen K, Harris CC, Schmidt HK, Kalicki-Veizer JM, Lu C, Zhang Q, Lin L, O'Laughlin MD, McMichael JF, Delehaunty KD, Fulton LA, Magrini VJ, McGrath SD, Demeter RT, Vickery TL, et al. The origin and evolution of mutations in acute myeloid leukemia. Cell. 2012;150(2):264–78.
Li S, Garrett-Bakelman FE, Chung SS, Sanders MA, Hricik T, Rapaport F, Patel J, Dillon R, Vijay P, Brown AL, Perl AE, Cannon J, Bullinger L, Luger S, Becker M, Lewis ID, To LB, Delwel R, Lowenberg B, Dohner H, Dohner K, Guzman ML, Hassane DC, Roboz GJ, Grimwade D, Valk PJ, D'Andrea RJ, Carroll M, Park CY, Neuberg D, et al. Distinct evolution and dynamics of epigenetic and genetic heterogeneity in acute myeloid leukemia. Nat Med. 2016;22(7):792–9.
Bullinger L, Kronke J, Schon C, Radtke I, Urlbauer K, Botzenhardt U, Gaidzik V, Cario A, Senger C, Schlenk RF, Downing JR, Holzmann K, Dohner K, Dohner H. Identification of acquired copy number alterations and uniparental disomies in cytogenetically normal acute myeloid leukemia using high-resolution single-nucleotide polymorphism analysis. Leukemia. 2010;24(2):438–49.
Mardis ER, Ding L, Dooling DJ, Larson DE, McLellan MD, Chen K, Koboldt DC, Fulton RS, Delehaunty KD, McGrath SD, Fulton LA, Locke DP, Magrini VJ, Abbott RM, Vickery TL, Reed JS, Robinson JS, Wylie T, Smith SM, Carmichael L, Eldred JM, Harris CC, Walker J, Peck JB, Du F, Dukes AF, Sanderson GE, Brummett AM, Clark E, McMichael JF, et al. Recurring mutations found by sequencing an acute myeloid leukemia genome. N Engl J Med. 2009;361(11):1058–66.
Shen Y, Zhu YM, Fan X, Shi JY, Wang QR, Yan XJ, Gu ZH, Wang YY, Chen B, Jiang CL, Yan H, Chen FF, Chen HM, Chen Z, Jin J, Chen SJ. Gene mutation patterns and their prognostic impact in a cohort of 1185 patients with acute myeloid leukemia. Blood. 2011;118(20):5593–603.
Baylin SB, Jones PA. A decade of exploring the cancer epigenome—biological and translational implications. Nat Rev Cancer. 2011;11(10):726–34.
Ruike Y, Imanaka Y, Sato F, Shimizu K, Tsujimoto G. Genome-wide analysis of aberrant methylation in human breast cancer cells using methyl-DNA immunoprecipitation combined with high-throughput sequencing. BMC Genomics. 2010;11:137.
Glasspool RM, Teodoridis JM, Brown R. Epigenetics as a mechanism driving polygenic clinical drug resistance. Br J Cancer. 2006;94(8):1087–92.
Figueroa ME, Abdel-Wahab O, Lu C, Ward PS, Patel J, Shih A, Li Y, Bhagwat N, Vasanthakumar A, Fernandez HF, Tallman MS, Sun Z, Wolniak K, Peeters JK, Liu W, Choe SE, Fantin VR, Paietta E, Lowenberg B, Licht JD, Godley LA, Delwel R, Valk PJ, Thompson CB, Levine RL, Melnick A. Leukemic IDH1 and IDH2 mutations result in a hypermethylation phenotype, disrupt TET2 function, and impair hematopoietic differentiation. Cancer Cell. 2010;18(6):553–67.
Schoofs T, Berdel WE, Muller-Tidow C. Origins of aberrant DNA methylation in acute myeloid leukemia. Leukemia. 2014;28(1):1–14.
Gutierrez SE, Romero-Oliva FA. Epigenetic changes: a common theme in acute myelogenous leukemogenesis. J Hematol Oncol. 2013;6:57.
Bibikova M, Barnes B, Tsan C, Ho V, Klotzle B, Le JM, Delano D, Zhang L, Schroth GP, Gunderson KL, Fan JB, Shen R. High density DNA methylation array with single CpG site resolution. Genomics. 2011;98(4):288–95.
Dedeurwaerder S, Defrance M, Calonne E, Denis H, Sotiriou C, Fuks F. Evaluation of the Infinium Methylation 450 K technology. Epigenomics. 2011;3(6):771–84.
Moran S, Arribas C, Esteller M. Validation of a DNA methylation microarray for 850,000 CpG sites of the human genome enriched in enhancer sequences. Epigenomics. 2016;8(3):389–99.
Keating GM. Azacitidine: a review of its use in the management of myelodysplastic syndromes/acute myeloid leukaemia. Drugs. 2012;72(8):1111–36.
Gao F, Wang J, Ji G, Liu S, Yao Y, Wang T, Wu H, Xia Y, Gong D, Jiang H, Yang H, Zhang X. Clustering of cancer cell lines using a promoter-targeted liquid hybridization capture-based bisulfite sequencing approach. Technol Cancer Res Treat. 2015;14(4):383–94.
Allum F, Shao X, Guenard F, Simon MM, Busche S, Caron M, Lambourne J, Lessard J, Tandre K, Hedman AK, Kwan T, Ge B, Multiple Tissue Human Expression Resource Consurtium, Ronnblom L, McCarthy MI, Deloukas P, Richmond T, Burgess D, Spector TD, Tchernof A, Marceau S, Lathrop M, Vohl MC, Pastinen T, Grundberg E. Characterization of functional methylomes by next-generation capture sequencing identifies novel disease-associated variants. Nat Commun. 2015;6:7211.
Stirzaker C, Taberlay PC, Statham AL, Clark SJ. Mining cancer methylomes: prospects and challenges. Trends Genet. 2014;30(2):75–84.
consortium B. Quantitative comparison of DNA methylation assays for biomarker development and clinical applications. Nat Biotechnol. 2016;34(7):726–37.
Meldi K, Qin T, Buchi F, Droin N, Sotzen J, Micol JB, Selimoglu-Buet D, Masala E, Allione B, Gioia D, Poloni A, Lunghi M, Solary E, Abdel-Wahab O, Santini V, Figueroa ME. Specific molecular signatures predict decitabine response in chronic myelomonocytic leukemia. J Clin Invest. 2015;125(5):1857–72.
Libertini E, Heath SC, Hamoudi RA, Gut M, Ziller MJ, Herrero J, Czyz A, Ruotti V, Stunnenberg HG, Frontini M, Ouwehand WH, Meissner A, Gut IG, Beck S. Saturation analysis for whole-genome bisulfite sequencing data. Nat Biotechnol. 2016. doi:10.1038/nbt.3524.
Libertini E, Heath SC, Hamoudi RA, Gut M, Ziller MJ, Czyz A, Ruotti V, Stunnenberg HG, Frontini M, Ouwehand WH, Meissner A, Gut IG, Beck S. Information recovery from low coverage whole-genome bisulfite sequencing. Nat Commun. 2016;7:11306.
Figueroa ME, Lugthart S, Li Y, Erpelinck-Verschueren C, Deng X, Christos PJ, Schifano E, Booth J, van Putten W, Skrabanek L, Campagne F, Mazumdar M, Greally JM, Valk PJ, Lowenberg B, Delwel R, Melnick A. DNA methylation signatures identify biologically distinct subtypes in acute myeloid leukemia. Cancer Cell. 2010;17(1):13–27.
Deneberg S, Grovdal M, Karimi M, Jansson M, Nahi H, Corbacioglu A, Gaidzik V, Dohner K, Paul C, Ekstrom TJ, Hellstrom-Lindberg E, Lehmann S. Gene-specific and global methylation patterns predict outcome in patients with acute myeloid leukemia. Leukemia. 2010;24(5):932–41.
Yalcin A, Kreutz C, Pfeifer D, Abdelkarim M, Klaus G, Timmer J, Lubbert M, Hackanson B. MeDIP coupled with a promoter tiling array as a platform to investigate global DNA methylation patterns in AML cells. Leuk Res. 2013;37(1):102–11.
Bullinger L, Ehrich M, Dohner K, Schlenk RF, Dohner H, Nelson MR, van den Boom D. Quantitative DNA methylation predicts survival in adult acute myeloid leukemia. Blood. 2010;115(3):636–42.
Deneberg S, Guardiola P, Lennartsson A, Qu Y, Gaidzik V, Blanchet O, Karimi M, Bengtzen S, Nahi H, Uggla B, Tidefelt U, Hoglund M, Paul C, Ekwall K, Dohner K, Lehmann S. Prognostic DNA methylation patterns in cytogenetically normal acute myeloid leukemia are predefined by stem cell chromatin marks. Blood. 2011;118(20):5573–82.
Luskin MR, Gimotty PA, Smith C, Loren AW, Figueroa ME, Harrison J, Sun Z, Tallman MS, Paietta EM, Litzow MR, Melnick AM, Levine RL, Fernandez HF, Luger SM, Carroll M, Master SR, Wertheim GB. A clinical measure of DNA methylation predicts outcome in de novo acute myeloid leukemia. JCI insight. 2016;1(9):e87323.
Jones PA. Functions of DNA methylation: islands, start sites, gene bodies and beyond. Nat Rev Genet. 2012;13(7):484–92.
Smith ZD, Meissner A. DNA methylation: roles in mammalian development. Nat Rev Genet. 2013;14(3):204–20.
Roadmap Epigenomics Consortium, Kundaje A, Meuleman W, Ernst J, Bilenky M, Yen A, Heravi-Moussavi A, Kheradpour P, Zhang Z, Wang J, Ziller MJ, Amin V, Whitaker JW, Schultz MD, Ward LD, Sarkar A, Quon G, Sandstrom RS, Eaton ML, Wu YC, Pfenning AR, Wang X, Claussnitzer M, Liu Y, Coarfa C, Harris RA, Shoresh N, Epstein CB, Gjoneska E, Leung D, et al. Integrative analysis of 111 reference human epigenomes. Nature. 2015;518(7539):317–30.
Akalin A, Garrett-Bakelman FE, Kormaksson M, Busuttil J, Zhang L, Khrebtukova I, Milne TA, Huang Y, Biswas D, Hess JL, Allis CD, Roeder RG, Valk PJ, Lowenberg B, Delwel R, Fernandez HF, Paietta E, Tallman MS, Schroth GP, Mason CE, Melnick A, Figueroa ME. Base-pair resolution DNA methylation sequencing reveals profoundly divergent epigenetic landscapes in acute myeloid leukemia. PLoS Genet. 2012;8(6):e1002781.
Arber DA, Attilio O, Robert H, J¨urgen T, Borowitz MJ, Le Beau MM, Bloomfield CD, Mario C, Vardiman JW. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–405.
Qu Y, Lennartsson A, Gaidzik VI, Deneberg S, Karimi M, Bengtzen S, Hoglund M, Bullinger L, Dohner K, Lehmann S. Differential methylation in CN-AML preferentially targets non-CGI regions and is dictated by DNMT3A mutational status and associated with predominant hypomethylation of HOX genes. Epigenetics. 2014;9(8):1108–19.
Hajkova H, Fritz MH, Haskovec C, Schwarz J, Salek C, Markova J, Krejcik Z, Dostalova Merkerova M, Kostecka A, Vostry M, Fuchs O, Michalova K, Cetkovsky P, Benes V. CBFB-MYH11 hypomethylation signature and PBX3 differential methylation revealed by targeted bisulfite sequencing in patients with acute myeloid leukemia. J Hematol Oncol. 2014;7:66.
Di Croce L, Raker VA, Corsaro M, Fazi F, Fanelli M, Faretta M, Fuks F, Lo Coco F, Kouzarides T, Nervi C, Minucci S, Pelicci PG. Methyltransferase recruitment and DNA hypermethylation of target promoters by an oncogenic transcription factor. Science. 2002;295(5557):1079–82.
Liu S, Shen T, Huynh L, Klisovic MI, Rush LJ, Ford JL, Yu J, Becknell B, Li Y, Liu C, Vukosavljevic T, Whitman SP, Chang KS, Byrd JC, Perrotti D, Plass C, Marcucci G. Interplay of RUNX1/MTG8 and DNA methyltransferase 1 in acute myeloid leukemia. Cancer Res. 2005;65(4):1277–84.
Cole CB, Verdoni AM, Ketkar S, Leight ER, Russler-Germain DA, Lamprecht TL, Demeter RT, Magrini V, Ley TJ. PML-RARA requires DNA methyltransferase 3A to initiate acute promyelocytic leukemia. J Clin Invest. 2016;126(1):85–98.
Schoofs T, Rohde C, Hebestreit K, Klein HU, Gollner S, Schulze I, Lerdrup M, Dietrich N, Agrawal-Singh S, Witten A, Stoll M, Lengfelder E, Hofmann WK, Schlenke P, Buchner T, Hansen K, Berdel WE, Rosenbauer F, Dugas M, Muller-Tidow C. DNA methylation changes are a late event in acute promyelocytic leukemia and coincide with loss of transcription factor binding. Blood. 2013;121(1):178–87.
Martens JH, Brinkman AB, Simmer F, Francoijs KJ, Nebbioso A, Ferrara F, Altucci L, Stunnenberg HG. PML-RARalpha/RXR alters the epigenetic landscape in acute promyelocytic leukemia. Cancer Cell. 2010;17(2):173–85.
Saeed S, Logie C, Stunnenberg HG, Martens JH. Genome-wide functions of PML-RARalpha in acute promyelocytic leukaemia. Br J Cancer. 2011;104(4):554–8.
Ng HY, Wan TS, So CC, Chim CS. Epigenetic inactivation of DAPK1, p14ARF, mir-34a and -34b/c in acute promyelocytic leukaemia. J Clin Pathol. 2014;67(7):626–31.
Marcucci G, Yan P, Maharry K, Frankhouser D, Nicolet D, Metzeler KH, Kohlschmidt J, Mrozek K, Wu YZ, Bucci D, Curfman JP, Whitman SP, Eisfeld AK, Mendler JH, Schwind S, Becker H, Bar C, Carroll AJ, Baer MR, Wetzler M, Carter TH, Powell BL, Kolitz JE, Byrd JC, Plass C, Garzon R, Caligiuri MA, Stone RM, Volinia S, Bundschuh R, et al. Epigenetics meets genetics in acute myeloid leukemia: clinical impact of a novel seven-gene score. J Clin Oncol Off J Am Soc Clin Oncol. 2014;32(6):548–56.
Li KK, Luo LF, Shen Y, Xu J, Chen Z, Chen SJ. DNA methyltransferases in hematologic malignancies. Semin Hematol. 2013;50(1):48–60.
Liu X, Jia X, Yuan H, Ma K, Chen Y, Jin Y, Deng M, Pan W, Chen S, Chen Z, de The H, Zon LI, Zhou Y, Zhou J, Zhu J. DNA methyltransferase 1 functions through C/ebpa to maintain hematopoietic stem and progenitor cells in zebrafish. J Hematol Oncol. 2015;8:15.
Challen GA, Sun D, Jeong M, Luo M, Jelinek J, Berg JS, Bock C, Vasanthakumar A, Gu H, Xi Y, Liang S, Lu Y, Darlington GJ, Meissner A, Issa JP, Godley LA, Li W, Goodell MA. Dnmt3a is essential for hematopoietic stem cell differentiation. Nat Genet. 2012;44(1):23–31.
Ley TJ, Ding L, Walter MJ, McLellan MD, Lamprecht T, Larson DE, Kandoth C, Payton JE, Baty J, Welch J, Harris CC, Lichti CF, Townsend RR, Fulton RS, Dooling DJ, Koboldt DC, Schmidt H, Zhang Q, Osborne JR, Lin L, O'Laughlin M, McMichael JF, Delehaunty KD, McGrath SD, Fulton LA, Magrini VJ, Vickery TL, Hundal J, Cook LL, Conyers JJ, et al. DNMT3A mutations in acute myeloid leukemia. N Engl J Med. 2010;363(25):2424–33.
Mizuno S, Chijiwa T, Okamura T, Akashi K, Fukumaki Y, Niho Y, Sasaki H. Expression of DNA methyltransferases DNMT1, 3A, and 3B in normal hematopoiesis and in acute and chronic myelogenous leukemia. Blood. 2001;97(5):1172–9.
Deveau AP, Forrester AM, Coombs AJ, Wagner GS, Grabher C, Chute IC, Leger D, Mingay M, Alexe G, Rajan V, Liwski R, Hirst M, Steigmaier K, Lewis SM, Look AT, Berman JN. Epigenetic therapy restores normal hematopoiesis in a zebrafish model of NUP98-HOXA9-induced myeloid disease. Leukemia. 2015;29(10):2086–97.
Shlush LI, Zandi S, Mitchell A, Chen WC, Brandwein JM, Gupta V, Kennedy JA, Schimmer AD, Schuh AC, Yee KW, McLeod JL, Doedens M, Medeiros JJ, Marke R, Kim HJ, Lee K, McPherson JD, Hudson TJ, Consortium HP-LGP, Brown AM, Yousif F, Trinh QM, Stein LD, Minden MD, Wang JC, Dick JE. Identification of pre-leukaemic haematopoietic stem cells in acute leukaemia. Nature. 2014;506(7488):328–33.
Jiang D, Hong Q, Shen Y, Xu Y, Zhu H, Li Y, Xu C, Ouyang G, Duan S. The diagnostic value of DNA methylation in leukemia: a systematic review and meta-analysis. PLoS One. 2014;9(5):e96822.
Gao XN, Yan F, Lin J, Gao L, Lu XL, Wei SC, Shen N, Pang JX, Ning QY, Komeno Y, Deng AL, Xu YH, Shi JL, Li YH, Zhang DE, Nervi C, Liu SJ, Yu L. AML1/ETO cooperates with HIF1alpha to promote leukemogenesis through DNMT3a transactivation. Leukemia. 2015;29(8):1730–40.
Wertheim GB, Smith C, Figueroa ME, Kalos M, Bagg A, Carroll M, Master SR. Microsphere-based multiplex analysis of DNA methylation in acute myeloid leukemia. J Mol Diagn. 2014;16(2):207–15.
Wertheim GB, Smith C, Luskin M, Rager A, Figueroa ME, Carroll M, Master SR. Validation of DNA methylation to predict outcome in acute myeloid leukemia by use of xMELP. Clin Chem. 2015;61(1):249–58.
DiNardo CD, Luskin MR, Carroll M, Smith C, Harrison J, Pierce S, Kornblau S, Konopleva M, Kadia T, Kantarjian H, Wertheim GB, Master SR. Validation of a clinical assay of multi-locus DNA methylation for prognosis of newly diagnosed AML. Am J Hematol. 2017;92(2):E14-5.
Raj K, John A, Ho A, Chronis C, Khan S, Samuel J, Pomplun S, Thomas NS, Mufti GJ. CDKN2B methylation status and isolated chromosome 7 abnormalities predict responses to treatment with 5-azacytidine. Leukemia. 2007;21(9):1937–44.
Figueroa ME, Skrabanek L, Li Y, Jiemjit A, Fandy TE, Paietta E, Fernandez H, Tallman MS, Greally JM, Carraway H, Licht JD, Gore SD, Melnick A. MDS and secondary AML display unique patterns and abundance of aberrant DNA methylation. Blood. 2009;114(16):3448–58.
Zhang LY, Yuan YQ, Zhou DM, Wang ZY, Ju SG, Sun Y, Li J, Fu JX. Impact of global and gene-specific DNA methylation in de novo or relapsed acute myeloid leukemia patients treated with decitabine. Asian Pac J Cancer Prev. 2016;17(1):431–7.
Grovdal M, Khan R, Aggerholm A, Antunovic P, Astermark J, Bernell P, Engstrom LM, Kjeldsen L, Linder O, Nilsson L, Olsson A, Wallvik J, Tangen JM, Oberg G, Jacobsen SE, Hokland P, Porwit A, Hellstrom-Lindberg E. Negative effect of DNA hypermethylation on the outcome of intensive chemotherapy in older patients with high-risk myelodysplastic syndromes and acute myeloid leukemia following myelodysplastic syndrome. Clin Cancer Res. 2007;13(23):7107–12.
Ribeiro AF, Pratcorona M, Erpelinck-Verschueren C, Rockova V, Sanders M, Abbas S, Figueroa ME, Zeilemaker A, Melnick A, Lowenberg B, Valk PJ, Delwel R. Mutant DNMT3A: a marker of poor prognosis in acute myeloid leukemia. Blood. 2012;119(24):5824–31.
Abbas S, Lugthart S, Kavelaars FG, Schelen A, Koenders JE, Zeilemaker A, van Putten WJ, Rijneveld AW, Lowenberg B, Valk PJ. Acquired mutations in the genes encoding IDH1 and IDH2 both are recurrent aberrations in acute myeloid leukemia: prevalence and prognostic value. Blood. 2010;116(12):2122–6.
Gaidzik VI, Paschka P, Spath D, Habdank M, Kohne CH, Germing U, von Lilienfeld-Toal M, Held G, Horst HA, Haase D, Bentz M, Gotze K, Dohner H, Schlenk RF, Bullinger L, Dohner K. TET2 mutations in acute myeloid leukemia (AML): results from a comprehensive genetic and clinical analysis of the AML study group. J Clin Oncol Off J Am Soc Clin Oncol. 2012;30(12):1350–7.
Wouters BJ, Delwel R. Epigenetics and approaches to targeted epigenetic therapy in acute myeloid leukemia. Blood. 2016;127(1):42–52.
Huls G. Azacitidine in AML: a treatment option? Blood. 2015;126(3):283–4.
Chau D, Ng K, Chan TS, Cheng YY, Fong B, Tam S, Kwong YL, Tse E. Azacytidine sensitizes acute myeloid leukemia cells to arsenic trioxide by up-regulating the arsenic transporter aquaglyceroporin 9. J Hematol Oncol. 2015;8:46.
Tibes R, Al-Kali A, Oliver GR, Delman DH, Hansen N, Bhagavatula K, Mohan J, Rakhshan F, Wood T, Foran JM, Mesa RA, Bogenberger JM. The Hedgehog pathway as targetable vulnerability with 5-azacytidine in myelodysplastic syndrome and acute myeloid leukemia. J Hematol Oncol. 2015;8:114.
Nieto M, Demolis P, Behanzin E, Moreau A, Hudson I, Flores B, Stemplewski H, Salmonson T, Gisselbrecht C, Bowen D, Pignatti F. The European Medicines Agency Review of Decitabine (Dacogen) for the treatment of adult patients with acute myeloid leukemia: summary of the scientific assessment of the committee for medicinal products for human use. Oncologist. 2016;21(6):692–700.
Dombret H, Seymour JF, Butrym A, Wierzbowska A, Selleslag D, Jang JH, Kumar R, Cavenagh J, Schuh AC, Candoni A, Recher C, Sandhu I, Bernal del Castillo T, Al-Ali HK, Martinelli G, Falantes J, Noppeney R, Stone RM, Minden MD, McIntyre H, Songer S, Lucy LM, Beach CL, Dohner H. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291–9.
Han S, Kim YJ, Lee J, Jeon S, Hong T, Park GJ, Yoon JH, Yahng SA, Shin SH, Lee SE, Eom KS, Kim HJ, Min CK, Lee S, Yim DS. Model-based adaptive phase I trial design of post-transplant decitabine maintenance in myelodysplastic syndrome. J Hematol Oncol. 2015;8:118.
Traina F, Visconte V, Elson P, Tabarroki A, Jankowska AM, Hasrouni E, Sugimoto Y, Szpurka H, Makishima H, O'Keefe CL, Sekeres MA, Advani AS, Kalaycio M, Copelan EA, Saunthararajah Y, Olalla Saad ST, Maciejewski JP, Tiu RV. Impact of molecular mutations on treatment response to DNMT inhibitors in myelodysplasia and related neoplasms. Leukemia. 2014;28(1):78–87.
Emadi A, Faramand R, Carter-Cooper B, Tolu S, Ford LA, Lapidus RG, Wetzler M, Wang ES, Etemadi A, Griffiths EA. Presence of isocitrate dehydrogenase mutations may predict clinical response to hypomethylating agents in patients with acute myeloid leukemia. Am J Hematol. 2015;90(5):E77–9.
Shafer D, Grant S. Update on rational targeted therapy in AML. Blood Rev. 2016;30(4):275–83.
Stein EM. Molecular pathways: IDH2 mutations-co-opting cellular metabolism for malignant transformation. Clin Cancer Res. 2016;22(1):16–9.
IDH1 inhibitor shows promising early results. Cancer Discov. 2015;5(1):4. doi:10.1158/2159-8290.CD-NB2014-178.
Hansen E, Quivoron C, Straley K, Lemieux RM, Popovici-Muller J, Sadrzadeh H, Fathi AT, Gliser C, David M, Saada V, Micol JB, Bernard O, Dorsch M, Yang H, Su M, Agresta S, de Botton S, Lacronique VP, Yen K. AG-120, an oral, selective, first-in-Class, potent inhibitor of mutant IDH1, reduces intracellular 2HG and induces cellular differentiation in TF-1 R132H cells and primary human IDH1 mutant AML patient samples treated ex vivo. Blood. 2014;124(21):3734.
DiNardo CD, Schimmer A, Yee KWL, Hochhaus A, Kraemer A, Carvajal RD, Janku F, Bedard P, Carpio C, Wick A, Schwartz GK, Schöffski P, Wen P, van den Bent MJ, Rosenthal M, O'Keeffe J, Chen X, Pagliarini R, Schuck V, Myers A, Wei A. A phase I study of IDH305 in patients with advanced malignancies including relapsed/refractory AML and MDS that harbor IDH1R132 mutations. Blood. 2016;128(22):1073.
DiNardo CD, de Botton S, Stein EM, Roboz GJ, Swords RT, Pollyea DA, Fathi AT, Collins R, Altman JK, Flinn IW, Mannis GN, Mims AS, Foran JM, Pigneux A, Prince GT, Uy GL, Tallman MS, Kantarjian HM, Liu H, Attar EC, Sacolick J, Yen K, Hurov JB, Choe S, Wu B, Stone RM. Determination of IDH1 mutational burden and clearance via next-generation sequencing in patients with IDH1 mutation-positive hematologic malignancies receiving AG-120, a first-in-class inhibitor of mutant IDH1. Blood. 2016;128(22):1070.
Stein EM, Fathi AT, DiNardo CD, Pollyea DA, Swords RT, Roboz GJ, Collins R, Sekeres MA, Stone RM, Attar EC, Tosolini A, Xu Q, Amatangelo M, Gupta I, Knight RD, De Botton S, Tallman MS, Kantarjian HM. Enasidenib (AG-221), a potent oral inhibitor of mutant isocitrate dehydrogenase 2 (IDH2) enzyme, induces hematologic responses in patients with myelodysplastic syndromes (MDS). Blood. 2016;128(22):343.
Stein EM, DiNardo CD, Altman JK, Collins R, DeAngelo DJ, Kantarjian HM, Sekeres MA, Fathi AT, Flinn LW, Frankel AE, Levine RL, Medeiros BC, Patel MR, Pollyea DA, Roboz GJ, Stone RM, Swords RT, Tallman MS, Yen K, Attar EC, Xu Q, Tosolini A, Mei JM, Thakurta A, Knight RD, De Botton S. Safety and efficacy of AG-221, a potent inhibitor of mutant IDH2 that promotes differentiation of myeloid cells in patients with advanced hematologic malignancies: results of a phase 1/2 trial. Blood. 2015;126(23):323.
Taskesen E, Babaei S, Reinders MM, de Ridder J. Integration of gene expression and DNA-methylation profiles improves molecular subtype classification in acute myeloid leukemia. BMC Bioinf. 2015;16 Suppl 4:S5.
Shih AH, Jiang Y, Meydan C, Shank K, Pandey S, Barreyro L, Antony-Debre I, Viale A, Socci N, Sun Y, Robertson A, Cavatore M, de Stanchina E, Hricik T, Rapaport F, Woods B, Wei C, Hatlen M, Baljevic M, Nimer SD, Tallman M, Paietta E, Cimmino L, Aifantis I, Steidl U, Mason C, Melnick A, Levine RL. Mutational cooperativity linked to combinatorial epigenetic gain of function in acute myeloid leukemia. Cancer Cell. 2015;27(4):502–15.
Ohgami RS, Arber DA. The diagnostic and clinical impact of genetics and epigenetics in acute myeloid leukemia. Int J Lab Hematol. 2015;37 Suppl 1:122–32.
Bujold D, Morais DA, Gauthier C, Cote C, Caron M, Kwan T, Chen KC, Laperle J, Markovits AN, Pastinen T, Caron B, Veilleux A, Jacques PE, Bourque G. The International Human Epigenome Consortium Data Portal. Cell Syst. 2016;3(5):496–9. e492.
Fernandez JM, de la Torre V, Richardson D, Royo R, Puiggros M, Moncunill V, Fragkogianni S, Clarke L, Consortium B, Flicek P, Rico D, Torrents D, Carrillo de Santa Pau E, Valencia A. The BLUEPRINT Data Analysis Portal. Cell Syst. 2016;3(5):491–5. e495.
Breeze CE, Paul DS, van Dongen J, Butcher LM, Ambrose JC, Barrett JE, Lowe R, Rakyan VK, Iotchkova V, Frontini M, Downes K, Ouwehand WH, Laperle J, Jacques PE, Bourque G, Bergmann AK, Siebert R, Vellenga E, Saeed S, Matarese F, Martens JH, Stunnenberg HG, Teschendorff AE, Herrero J, Birney E, Dunham I, Beck S. eFORGE: a tool for identifying cell type-specific signal in epigenomic data. Cell Rep. 2016;17(8):2137–50.
Acknowledgements
The authors are grateful to Yaojie Liang for the preparation of the graphical illustrations.
Funding
This work was supported by the National Natural Science Foundation of China (8167016, 81370635, 81170518, 81270611, 81570137, 81470010, and 81400135), Capital Medical Development Scientific Research Fund (SF2001-5001-07), Beijing Natural Science Foundation (7151009), National Public Health Grant Research Foundation (No.201202017), The capital of the public health project (Z111107067311070), and Technology Innovation Nursery Foundation (13KMM01). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
This is a review article, and the specific datasets supporting the conclusions of this article were generated by other research groups. Our supporting data was obtained from the referenced publications.
Authors’ contributions
LY and YL designed this review. YL, QYX, NL, HMZ, and XLW searched literatures and contributed suggestions. YL and QYX reviewed the literatures. YL drafted the manuscript and designed the figure and table, while QYX edited and LY critically revised the manuscript. LLW, CJC, and YHL provided valuable advice and also revised the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Li, Y., Xu, Q., Lv, N. et al. Clinical implications of genome-wide DNA methylation studies in acute myeloid leukemia. J Hematol Oncol 10, 41 (2017). https://doi.org/10.1186/s13045-017-0409-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13045-017-0409-z