
Abstract
Background
Cement-augmentation pedicle screws have been widely used in spinal internal fixation surgery combined with osteoporosis in recent years, which can significantly improve the fixation strength, but compared with conventional methods, whether it has more advantages is still inconclusive of evidencebased medicine. To systematically evaluate the efficacy and safety of cement-augmented pedicle screw in the treatment of thoracolumbar degenerative diseases with osteoporosis.
Methods
We searched PubMed, Embase, and Cochrane Library for studies published from the establishment of the database up until June 2023. We included studies that concerning the cement-augmented pedicle screw and the traditional pedicle screw placement for thoracolumbar degenerative diseases with osteoporosis. We excluded repeated publication, researches without full text, incomplete information or inability to conduct data extraction and animal experiments, case report, reviews and systematic reviews. STATA 15.1 software was used to analyze the data.
Results
A total of 12 studies were included in this meta-analysis. The sample size of patients were totally 881, of which, 492 patients in cement-augmented screw group and 389 patients in conventional screw group. Meta-analysis results showed that Japanese Orthopaedic Association (JOA) score (WMD = 1.69, 95% CI 1.15 to 2.22), intervertebral space height (WMD = 1.66, 95% CI 1.03 to 2.29) and post-operation fusion rate (OR = 2.80, 95% CI 1.49 to 5.25) were higher in the cement-augmented screw group than those in the conventional screw group. Operation time was longer in the cement-augmented screw group than that in the conventional screw group (WMD = 15.47, 95% CI 1.25 to 29.70). Screw loosening rate was lower in the cement-augmented screw group than those in the conventional screw group (OR = 0.13, 95% CI 0.07 to 0.22). However, hospitalization time, intraoperative blood loss and Visual analog scale (VAS) score were not significantly different between the two groups (P > 0.05).
Conclusion
Compared with conventional pedicle screw placement, cement-augmented pedicle screw is more effective in the treatment of osteoporotic thoracolumbar degenerative disease by improving fusion rate and interbody height, reducing the incidence of screw loosening, and elevating long-term efficacy.
Similar content being viewed by others

Introduction
Thoracolumbar degenerative diseases are common diseases in middle-aged and elderly people, which often cause patients with low back pain, lower extremity pain and limited movement. Finally, the pedicle screw system is required for internal fixation to improve spinal stability and alleviate symptoms, which brings serious mental and economic burden to patients [1, 2] With the development of modern medicine, the average life expectancy of residents in the world continues to increase, the aging population is increasing, and the population suffering from osteoporosis is becoming more and more common, and people in this age group are often accompanied by serious thoracic and lumbar degenerative diseases [3, 4]. When the traditional pedicle screw is inserted in patients with osteoporosis, the screw is often easy to loosen due to the poor bone mineral density, resulting in the failure of internal fixation [5]. Therefore, how to effectively use pedicle screws to reconstruct the spine of patients with thoracolumbar degenerative diseases, column stability, and avoid the failure of internal fixation due to nail loosening, nail extraction and other problems has been a research focus of spinal surgeons.
With the development of science and technology, spinal surgery techniques have been continuously improved, among which methods to improve the stability of pedicle screws have also been increasing. At present, three methods are mainly used: (1) Using bone cement to strengthen pedicle screws [6]; (2) Increase the contact area between screws and bone cortex, such as cortical bone screws and double-threaded screws [7]; (3) Modify the screws themselves, such as expansion screws with increased diameters and hydroxy-phosphate-lime coated screws [8, 9].
Cement-augmented pedicle screw technology is one of the common techniques to improve the stability of internal fixation of pedicle screw. Compared with traditional pedicle screw fixation, this technique can effectively improve the success and rate of internal fixation. However, the comparison of the clinical efficacy of the treatment of osteoporotic thoracic and lumbar degenerative diseases is still lack of evidence-based medical conclusion [10]. In this study, a clinical comparative study of bone cement-strengthened pedicle screw fixation and traditional pedicle screw fixation in the treatment of thoracolumbar degenerative diseases was collected, and a meta-analysis was conducted after strict screening, in order to provide reference for the fusion fixation of thoracolumbar degenerative diseases in clinic.
Methods
Literature inclusion and exclusion criteria
Inclusion criteria: the study type is retrospective or prospective study; studies that reports the cement-augmented pedicle screw and the traditional pedicle screw placement for thoracolumbar degenerative diseases with osteoporosis; the language is limited to English.
Exclusion criteria: repeated publication; studies without full text, incomplete information or inability to conduct data extraction; animal experiments; case report; reviews and systematic reviews.
Search strategy
In this meta-analysis, we searched Pubmed, Embase, Cochrane Library from establishment of the database to June, 2023. The search terms are as follows: (“osteoporosis”) AND (“pedicle screw” OR “fixation”) AND (“cement” OR “polymethyl methacrylate” OR “PMMA” OR “augmentation”).
Literature screening and data extraction
Two researchers independently carried out literature search, screening and information extraction. When a question or dispute arises, a decision is made after discussion or negotiation with a third person. The data extraction included the author, publication year of articles, study design, sample size, age, sex and outcomes including hospitalization time (day), operation time (minute), intraoperative blood loss (ml), Japanese Orthopaedic Association (JOA) score, Visual analog scale (VAS) score, intervertebral space height, fusion rate and screw loosening rate.
Literature quality assessment
The Newcastle–Ottawa Scale (NOS) for evaluating the quality of published literature is carried out separately by two academics [11], and it was used to evaluate the quality of 16 cohort studies, NOS includes 4 items (4 points) for “Research Subject Selection”, 1 item (2 points) for “Comparability between Groups” and 3 items (3 points) for “Result Measurement”, with a full score of 9 points and ≥ 7 is regarded as High-quality literature, < 7 is divided into lower-quality literature.
Data synthesis and statistical analysis
All data analyzed by STATA 15.1 (Stata Crop LP, College Station, TX) [12]. Weighted mean difference (WMD) (90%CI) is used to evaluate continuity variables. I2 and Q test were used to evaluate heterogeneity. If the heterogeneity test is P ≥ 0.1 and I2 ≤ 50%, it indicates that there is homogeneity between studies, and the fixed effects model is used for combined analysis; if P < 0.1 or I2 > 50%, it indicates that there is heterogeneity and sensitivity analysis was used to find the source of heterogeneity. If the heterogeneity is still large, use the random effects model or give up the combination of results and use descriptive analysis. Funnel plot was used to assess the publication bias.
Results
The results of literature search
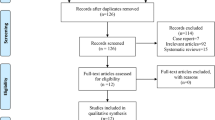
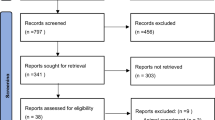
In this meta-analysis, a total of 763 studies were retrieved from the database including Pubmed, Embase and Cochrane Library. After eliminating duplicate studies, 394 were obtained. After browsing titles and abstracts, 123 studies were obtained. Finally, 6 articles were included in the meta-analysis (Fig. 1).

Flow diagram for selection of studies
Baseline characteristics and quality assessment of the included studies
A total of 12 studies were included in this meta-analysis. The sample size of patients were totally 881, of which, 492 patients in cement-augmented screw group and 389 patients in conventional screw group. The average age in cement-augmented screw group ranged from 49.0 to 76.0, while the conventional screw group ranged from 48.0 to 75.0. Average bone density ranged from − 2.5 to − 3.3 in cement-augmented screw group and − 2.5 to − 3.2 in conventional screw group. NOS scores were all above 8 points, indicating the literature included is of moderate or high quality (Table 1).
Results of the meta-analysis
Hospitalization time (day)
Three articles reported hospitalization time between cement augmented screw group and conventional screw group. Since there was heterogeneity in the study, the random-effect model was used to combine the effect sizes (I2 = 60.6%, P = 0.079). The pooled results showed that the difference in hospitalization time between the cementaugmented screw group and the conventional screw group was not statistically significant (WMD = 0.42, 95% CI − 2.14 to 2.99; P = 0.745) (Fig. 2).

Forest plot of hospitalization time between cement augmented screw group and conventional screw group
Operation time (minute)
Six articles reported operation time between cement augmented screw group and conventional screw group. Since there was heterogeneity in the study, the random-effect model was used to combine the effect sizes (I2 = 50.7%, P = 0.071). The pooled results show that the operation time of the cement augmented screw group was significantly longer than that of the conventional screw group (WMD = 15.47, 95% CI 1.25 to 29.70; P = 0.033) (Fig. 3).

Forest plot of operation time between cement augmented screw group and conventional screw group
Intraoperative blood loss
Seven articles reported intraoperative blood loss between cement augmented screw group and conventional screw group. Since there was significant heterogeneity in the study, the random-effect model was used to combine the effect sizes (I2 = 82.6%, P = 0.000). The pooled results showed that the difference in intraoperative blood loss between the cement augmented screw group and the conventional screw group was not statistically significant (WMD = − 46.36, 95% CI − 102.41 to 9.68; P = 0.105) (Fig. 4).

Forest plot of intraoperative blood loss between cement augmented screw group and conventional screw group
JOA score
Three articles reported JOA score between cement augmented screw group and conventional screw group. Since there was no heterogeneity in the study, the fixed-effect model was used to combine the effect sizes (I2 = 0.0%, P = 0.654). The pooled results show that the JOA score of the cement augmented screw group was significantly higher than that of the conventional screw group (WMD = 1.69, 95% CI 1.15 to 2.22; P = 0.000) (Fig. 5).

Forest plot of JOA score between cement augmented screw group and conventional screw group
VAS score
Five articles reported VAS score between cement augmented screw group and conventional screw group. Since there was no heterogeneity in the study, the fixed-effect model was used to combine the effect sizes (I2 = 0.0%, P = 0.553). The pooled results showed that the difference in VAS score between the cement augmented screw group and the conventional screw group was not statistically significant (WMD = − 0.08, 95% CI − 0.28 to 0.12; P = 0.427) (Fig. 6).

Forest plot of VAS score between cement augmented screw group and conventional screw group
Intervertebral space height
Two articles reported intervertebral space height between cement augmented screw group and conventional screw group. Since there was no heterogeneity in the study, the fixed-effect model was used to combine the effect sizes (I2 = 0.0%, P = 0.480). The pooled results show that the intervertebral space height of the cement augmented screw group was significantly higher than that of the conventional screw group (WMD = 1.66, 95% CI 1.03 to 2.29; P = 0.000) (Fig. 7).

Forest plot of intervertebral space height between cement augmented screw group and conventional screw group
Post-operation fusion rate
Eight articles reported post-operation fusion rate between cement augmented screw group and conventional screw group. Since there was no heterogeneity in the study, the fixed-effect model was used to combine the effect sizes (I2 = 0.0%, P = 0.480). The pooled results show that the post-operation fusion rate of the cement augmented screw group was significantly higher than that of the conventional screw group (OR = 2.80, 95% CI 1.49 to 5.25; P = 0.001) (Fig. 8).

Forest plot of post-operation fusion rate between cement augmented screw group and conventional screw group
Screw loosening rate
Six articles reported screw loosening rate between cement augmented screw group and conventional screw group. Since there was no heterogeneity in the study, the fixed-effect model was used to combine the effect sizes (I2 = 19.8%, P = 0.284). The pooled results show that the screw loosening rate of the cement augmented screw group was significantly lower than that of the conventional screw group (OR = 0.13, 95% CI 0.07 to 0.22; P = 0.000) (Fig. 9).

Forest plot of screw loosening rate between cement augmented screw group and conventional screw group
Subgroup analysis
We further performed subgroup analyses based on cement strengthening methods.
JOA score
The pooled results showed that the difference between cement treatment with conventional pedicle screws and conventional screw treatment in JOA was not statistically significant (WMD = 1.20, 95% CI − 0.47 to 2.87; P = 0.159), while the JOA after cement treatment with fenestrated pedicle screws was significantly higher than that of conventional screw treatment (WMD = 1.74, 95% CI 1.18 to 2.30; P = 0.000) (Fig. 10).

Differences between different cement strengthening modalities and conventional screw therapy in JOA core
VAS
The pooled results showed that the difference between cement treatment with conventional pedicle screws (WMD = − 0.10, 95% CI − 0.38 to 0.18; P = 0.476), or fenestrated pedicle screws (WMD = − 0.06, 95% CI − 0.34 to 0.22; P = 0.680) and conventional screw treatment in JOA were all not statistically significant (Fig. 11).

Differences between different cement strengthening modalities and conventional screw therapy in VAS
Fusion rate
The poole results showed that the fusion rate after bone cement treatment with conventional pedicle screws (OR = 2.32, 95% CI 1.14 to 4.69; P = 0.02) or fenestrated pedicle screws (OR = 5.26, 95% CI 1.16 to 23.83; P = 0.031) were all significantly higher than that of conventional screw treatment (Fig. 12).

Differences between different cement strengthening modalities and conventional screw therapy in fusion rate
Sensitivity analysis
The remaining investigations were subjected to a summative analysis to see whether any of the included studies had a disproportionate influence on the meta-overall analysis's results, which was accomplished using sensitivity analyses that eliminated each included research one at a time. According to the meta-analysis, no research had a substantial influence on its results, suggesting that the findings were steady and credible (Additional file 1: Figs. S1–S7).
Publication bias
The funnel plot of this study is shown in Fig. 13. It can be seen that the funnel plot was symmetrical, and the P value of Egger’s test was 0.242, respective, indicating that there is no obvious publication bias in this study.

Funnel plot used to assess publication bias
Discussion
The development of medical technology has led to the continuous aging of the population, and the lack of calcium supplements, sedentary and smoking, and the increasing number of the elderly population, leading to the increasing number of people suffering from osteoporosis. In osteoporosis patients with lumbar disc herniation, spinal stenosis, lumbar spondylolisthesis instability and scoliosis, and other degenerative diseases, spinal fusion and fixation with pedicle screw system is one of the main treatment methods [25]. However, patients with osteoporosis are prone to use conventional pedicle screws in the early stage, with pedicle and vertebral fractures, and the late stage may lead to progressive, junction kyphosis, pseudarthrosis formation and degeneration of adjacent vertebral segments, and the most common complication is screw loosening [26]. Studies have shown that spinal fixation stability is only 60% [27] compared to spines with good bone quality (> 120 mg/cm3) and below 0.6 g/cm2 for early screw loosening [28].
At present, many scholars use a variety of ways and technology efforts to improve the stability of spinal fixation, such as some scholars in the original fixed, on the basis of supplementary anterior fixation, laminar hook and install transverse connector, and more scholars to enhance pedicle screw, pull force, reduce pine, nail and other related complications risk, constantly improve technology [29]. Bone cement has the advantages of short setting time and high curing stability, and is widely used in the treatment of osteoporosis related diseases [30]. The study of ERDEM et al. [31] found that the pull-out force of pedicle screws increased significantly when using bone cement strengthening fixation, with an increase of 96–262%, while the lateral bending stiffness of pedicle screws increased by 153%, so this technique was gradually applied by spinologists to the surgical treatment of patients with degenerative diseases of the thoracolumbar spine [31].
A total of 12 articles were included in this study, and the results of meta-analysis showed that the operation time of the bone cement-strengthened pedicle screw group was more than that of the traditional pedicle screw group, and considering the cement-reinforced pedicle screw group increased the cement injection link, the number of fluoroscopy required also increased significantly, which in turn increased the operation time to a certain extent. There was no difference between the two groups in terms of intraoperative blood loss, hospital stay and postoperative drainage, considering that spinal canal decompression was basically concentrated in spinal canal decompression with spinal surgery bleeding and greater damage to patients, while surgical bleeding and injury were closely related to postoperative recovery, so the recent postoperative recovery speed of the two was similar, resulting in the same length of hospital stay [32].
JOA and VAS are common criteria for evaluating the efficacy of spinal surgery [33]. In this study, the JOA of the cement-enhanced pedicle screw group was better than that of the conventional pedicle screw group, and the follow-up time of the two groups was basically more than 1 year, indicating that the long-term efficacy of the cement-enhanced pedicle screw group was better than that of the conventional pedicle screw, and the treatment of cement-strengthened screw could improve the long-term quality of life of patients.
In addition, in terms of maintaining the height of intervertebral space, improving the fusion rate and reducing the screw loosening rate, the cement-reinforced pedicle screw group was still better than the conventional pedicle screw group. This shows that the use of bone cement strengthening technology can effectively improve the strength of the vertebral body, reduce the risk of loosening and nail retraction, achieve strong internal fixation, reduce the collapse of the final stub, better maintain the height of the intervertebral space, and provide a good and stable mechanical environment for intervertebral fusion, improve the fusion efficiency [34], and achieve the ideal clinical effect.
Furthermore, we performed subgroup analyses based on cement strengthening methods. The summary results suggest that in the analysis of JOA and fusion rate, cement treatment with fenestrated pedicle screws had higher postoperative JOA and fusion rate than cement treatment with conventional pedicle screws, indicating that fenestrated pedicle screws may be a better treatment and could be further promoted in the future.
This meta-analysis has several limitations. First, all of the studies included in this research were cohort studies. The literature quality is lower than that of randomized controlled trials, which may lead to selection bias. In addition, the included sample size was too small, and some studies had large statistical heterogeneity, resulting in reduced the reliability of the analysis results. The conclusions obtained in this paper need to be further verified by more rigorous high-quality, large-sample clinical studies.
Conclusion
Compared with conventional pedicle screw placement, cement-augmented pedicle screw is more effective in the treatment of osteoporotic thoracolumbar degenerative disease by improving fusion rate and interbody height, reducing the incidence of screw loosening, and elevating long-term efficacy.
Availability of data and materials
The datasets are available from the corresponding author on reasonable request.
References
Tuomainen I, Pakarinen M, Aalto T, Sinikallio S, Kroger H, Viinamaki H, Airaksinen O. Depression is associated with the long-term outcome of lumbar spinal stenosis surgery: a 10-year follow-up study. Spine J. 2018;18:458–63.
Ogihara S, Yamazaki T, Shiibashi M, Chikuda H, Maruyama T, Miyoshi K, Inanami H, Oshima Y, Azuma S, Kawamura N, Yamakawa K, Hara N, Morii J, Okazaki R, Takeshita Y, Tanaka S, Saita K. Risk factors for deep surgical site infection following posterior instrumented fusion for degenerative diseases in the thoracic and/or lumbar spine: a multicenter, observational cohort study of 2913 consecutive cases. Eur Spine J. 2021;30:1756–64.
Cui J, Liu CL, Jennane R, Ai S, Dai K, Tsai TY. A highly generalized classifier for osteoporosis radiography based on multiscale fractal, lacunarity, and entropy distributions. Front Bioeng Biotechnol. 2023;11:1054991.
Young JJ, Jensen RK, Hartvigsen J, Roos EM, Ammendolia C, Juhl CB. Prevalence of multimorbid degenerative lumbar spinal stenosis with knee or hip osteoarthritis: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2022;23:177.
Marie-Hardy L, Pascal-Moussellard H, Barnaba A, Bonaccorsi R, Scemama C. Screw loosening in posterior spine fusion: prevalence and risk factors. Glob Spine J. 2020;10:598–602.
Tandon V, Franke J, Kalidindi KKV. Advancements in osteoporotic spine fixation. J Clin Orthop Trauma. 2020;11:778–85.
Sakaura H, Ikegami D, Fujimori T, Sugiura T, Mukai Y, Hosono N, Fuji T. Early cephalad adjacent segment degeneration after posterior lumbar interbody fusion: a comparative study between cortical bone trajectory screw fixation and traditional trajectory screw fixation. J Neurosurg Spine. 2019;32:155–9.
Gazzeri R, Panagiotopoulos K, Galarza M, Bolognini A, Callovini G. Minimally invasive spinal fixation in an aging population with osteoporosis: clinical and radiological outcomes and safety of expandable screws versus fenestrated screws augmented with polymethylmethacrylate. Neurosurg Focus. 2020;49:E14.
Jang SH, Lee JH, Cho JY, Lee HY, Lee SH. The efficacy of hydroxyapatite for screw augmentation in osteoporotic patients. Neurol Med Chir. 2013;53:875–81.
Hoppe S, Keel MJ. Pedicle screw augmentation in osteoporotic spine: indications, limitations and technical aspects. Eur J Trauma Emerg Surg. 2017;43:3–8.
Cook DA, Reed DA. Appraising the quality of medical education research methods: the medical education research study quality instrument and the Newcastle-Ottawa scale-education. Acad Med. 2015;90:1067–76.
Zhu J, Jiang S, Jiang X, Luo K, Huang X, Hua F. Association of blood lipocalin-2 levels with gestational diabetes mellitus: a systematic review and meta-analysis. Horm Metab Res. 2022;54:677–85.
Kim KH, Lee SH, Lee DY, Shim CS, Maeng DH. Anterior bone cement augmentation in anterior lumbar interbody fusion and percutaneous pedicle screw fixation in patients with osteoporosis. J Neurosurg Spine. 2010;12:525–32.
Xie Y, Fu Q, Chen ZQ, Shi ZC, Zhu XD, Wang CF, Li M. Comparison between two pedicle screw augmentation instrumentations in adult degenerative scoliosis with osteoporosis. BMC Musculoskelet Disord. 2011;12:286.
Sawakami K, Yamazaki A, Ishikawa S, Ito T, Watanabe K, Endo N. Polymethylmethacrylate augmentation of pedicle screws increases the initial fixation in osteoporotic spine patients. J Spinal Disord Tech. 2012;25:E28-35.
Seo JH, Ju CI, Kim SW, Kim JK, Shin H. Clinical efficacy of bone cement augmented screw fixation for the severe osteoporotic spine, Korean. J Spine. 2012;9:79–84.
El Saman A, Meier S, Sander A, Kelm A, Marzi I, Laurer H. Reduced loosening rate and loss of correction following posterior stabilization with or without PMMA augmentation of pedicle screws in vertebral fractures in the elderly. Eur J Trauma Emerg Surg. 2013;39:455–60.
Sun HL, Li CD, Yang ZC, Yi XD, Liu H, Lu HL, Li H, Wang Y. Polymethylmethacrylate augmentation of bone cement-injectable cannulated pedicle screws for the treatment of degenerative lumbar diseases with osteoporosis. Beijing Da Xue Xue Bao Yi Xue Ban. 2016;48:1019–25.
Sun HL, Li CD, Li XW, Yi XD, Liu H, Lu HL, Li H, Yu ZR, Wang Y. Polymethylmethacrylate augmentation of bone cement injectable cannulated pedicle screws was used to treat degenerative lumbar scoliosis with osteoporosis. Beijing Da Xue Xue Bao Yi Xue Ban. 2017;49:256–61.
Cao Y, Liang Y, Wan S, Jiang C, Jiang X, Chen Z. Pedicle screw with cement augmentation in unilateral transforaminal lumbar interbody fusion: a 2-year follow-up study. World Neurosurg. 2018;118:e288–95.
Wang W, Liu C, Li J, Li H, Wu J, Liu H, Li C, Zhou Y. Comparison of the fenestrated pedicle screw and conventional pedicle screw in minimally percutaneous fixation for the treatment of spondylolisthesis with osteoporotic spine. Clin Neurol Neurosurg. 2019;183: 105377.
Mo GY, Guo HZ, Guo DQ, Tang YC, Li YX, Yuan K, Luo PJ, Zhou TP, Zhang SC, Liang D. Augmented pedicle trajectory applied on the osteoporotic spine with lumbar degenerative disease: mid-term outcome. J Orthop Surg Res. 2019;14:170.
Kim JH, Ahn DK, Shin WS, Kim MJ, Lee HY, Go YR. Clinical effects and complications of pedicle screw augmentation with bone cement: comparison of fenestrated screw augmentation and vertebroplasty augmentation. Clin Orthop Surg. 2020;12:194–9.
Tang YC, Guo HZ, Guo DQ, Luo PJ, Li YX, Mo GY, Ma YH, Peng JC, Liang D, Zhang SC. Effect and potential risks of using multilevel cement-augmented pedicle screw fixation in osteoporotic spine with lumbar degenerative disease. BMC Musculoskelet Disord. 2020;21:274.
Chin DK, Park JY, Yoon YS, Kuh SU, Jin BH, Kim KS, Cho YE. Prevalence of osteoporosis in patients requiring spine surgery: incidence and significance of osteoporosis in spine disease. Osteoporos Int. 2007;18:1219–24.
Yamada K, Satoh S, Hashizume H, Yoshimura N, Kagotani R, Ishimoto Y, Abe Y, Toyoda H, Terai H, Masuda T, Muraki S, Nakamura H, Yoshida M. Diffuse idiopathic skeletal hyperostosis is associated with lumbar spinal stenosis requiring surgery. J Bone Miner Metab. 2019;37:118–24.
Weiser L, Sehmisch S, Lehmann W, Viezens L. Techniques to increase pedicle screw stability in osteoporotic vertebrae. Oper Orthop Traumatol. 2019;31:284–92.
Zhuang XM, Yu BS, Zheng ZM, Zhang JF, Lu WW. Effect of the degree of osteoporosis on the biomechanical anchoring strength of the sacral pedicle screws: an in vitro comparison between unaugmented bicortical screws and polymethylmethacrylate augmented unicortical screws. Spine. 2010;35(19):E925–31.
Sayed D, Amirdelfan K, Hunter C, Raji OR. Posterior intra-articular fixation stabilizes both primary and secondary sacroiliac joints: a cadaveric study and comparison to lateral trans-articular fixation literature. J Orthop Surg Res. 2023;18:406.
Cai K, Jiang G, Lu B, Zhang K, Luo K. Bone cement distribution may significantly affect the efficacy of percutaneous vertebroplasty in treating symptomatic Schmorl’s nodes. BMC Musculoskelet Disord. 2023;24:473.
Erdem MN, Karaca S, Sari S, Yumrukcal F, Tanli R, Aydogan M. Application of cement on strategic vertebrae in the treatment of the osteoporotic spine. Spine J. 2017;17:328–37.
Girardo M, Cinnella P, Gargiulo G, Viglierchio P, Rava A, Aleotti S. Surgical treatment of osteoporotic thoraco-lumbar compressive fractures: the use of pedicle screw with augmentation PMMA. Eur Spine J. 2017;26:546–51.
Shi S, Zhou Z, Ni HJ, Wang CF, He ZM, Yang YH, Du JH, Wu JS, He SS. Does anxiety influence the prognosis of percutaneous transforaminal endoscopic discectomy in the treatment of lumbar disc herniation? A preliminary propensity score matching analysis. Int Orthop. 2020;44:2357–63.
Wang Y, Yang L, Li C, Sun H. The biomechanical properties of cement-augmented pedicle screws for osteoporotic spines. Glob Spine J. 2022;12:323–32.
Acknowledgements
Not applicable.
Funding
The Medical and Health Science and Technology Program of ZhejiangProvince (2021KY825). The Traditional Chinese Medicine Science and Technology Plan of ZhejiangProvince (2021ZB091).
Author information
Authors and Affiliations
Contributions
JZ conceived the manuscript, QZ wrote the manuscript, XJ participated in literature review and drawing, QZ and ZS participated in the revision of the article. ZS read and approved the final article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All of the authors are aware of and agree to the content of the paper and their being listed as a co-author of the paper.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Plots of sensitivity analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Song, Z., Zhou, Q., Jin, X. et al. Cement-augmented pedicle screw for thoracolumbar degenerative diseases with osteoporosis: a systematic review and meta-analysis. J Orthop Surg Res 18, 631 (2023). https://doi.org/10.1186/s13018-023-04077-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-023-04077-w