
Abstract
Background
Biomechanical characteristics of noncontinuous ACDF and noncontinuous CDA in the treatment of noncontinuous cervical degenerative disc disease were still unclear. The aim of this research is to compare the differences between these two kinds of treatment methods and to verify the effectiveness of Prodisc-C in noncontinuous CDA.
Methods
Eight FEMs of the cervical spine (C2–C7) were built based on CT images of 8 mild CDDD volunteers. In the arthroplasty group, we inserted Prodisc-C at C3/4 and C5/6. In the fusion group, CoRoent® Contour and NuVasive® Helix ACP were implanted at C3/4 and C5/6. Initial loads of 75 N were used to simulate the head weight and muscle forces. The application of 1.0 N m moment on the top on the C2 vertebra was used to create motion in all directions. Statistical analyses were performed using STATA version 14.0 (Stata Corp LP, College Station, Texas, USA). Statistical significance was set at P < 0.05.
Results
The IDPs in C2/3 (P < 0.001, P = 0.005, P < 0.001, P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) of the intact group were significantly less than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively. In addition, the IDPs in C2/3 (P < 0.001, P = 0.001, P < 0.001, P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) of the arthroplasty group were significantly less than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively. Contact forces of facet joints in C2/3 (P = 0.010) in the arthroplasty group was significantly less than that in the intact group. Contact forces of facet joints in C2/3 (P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) in the arthroplasty group was significantly less than that in the fusion group. Contact forces of facet joints in C2/3 (P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) in the intact group were significantly less than that in the fusion group.
Conclusions
Noncontinuous CDA could preserve IDP and facet joint forces at the adjacent and intermediate levels to maintain the kinematics of cervical spine near preoperative values. However, noncontinuous ACDF would increase degenerative risks at adjacent and intermediate levels. In addition, the application of Prodisc-C in noncontinuous CAD may have more advantages than that of Prestige LP.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Noncontiguous cervical degenerative disc disease (CDDD) is defined as cervical myelopathy or radiculopathy caused by two noncontiguous degenerative intervertebral discs with one normal intermediate segment (IS) [1]. Anterior cervical discectomy and fusion (ACDF) has been an accepted treatment method for degenerative cervical disc disease to alleviate cervical myelopathy or radiculopathy [2]. Previous studies indicated that the treatment effect of ACDF was excellent with over 90% of patients whose reduced movement functions were improved [3]. Long segmental anterior fusion, which included the normal intermediate segments (IS), was always used to treat noncontiguous CDDD in order to decrease the stress from fusion structures on IS and avoid the adjacent segment degeneration (ASD) in IS [4,5,6]. In general, long segmental anterior fusion was associated with high risk of pseudarthrosis, persistent postoperative dysphagia, nonunion, and ASD [4,5,6]. It has been reported that the preservation of IS could ameliorate postoperative outcomes [7]. However, most of the studies preserved the IS with noncontinuous ACDF, which would bring more additive stress from the fused levels and then cause hypermobility on IS; all of these would cause the acceleration of ASD [8].
Compared with ACDF, cervical disc arthroplasty (CDA) can preserve the motion at the operated level and theoretically alleviate ASD [9]. Previous studies reported that multilevel CDA could achieve better clinical outcomes compared with one-level CDA, even though the surgical techniques of multilevel CDA were more difficult and the inclusion criteria were stricter [10, 11]. Furthermore, Wu et al. [8] reported that noncontinuous CDA could reduce the biomechanical impact on the IS compared with noncontinuous fusion. However, they only built a standard set of models for analysis, lacking a statistical comparison of multiple patient models. In addition, most studies have discussed the effectiveness of Prestige LP in noncontinuous CDA, but the use of Prodisc-C in this kind of operation has not been fully discussed [1, 8, 12, 13]. Therefore, the aim of this research is to analyze the biomechanical characteristics of noncontinuous ACDF and noncontinuous CDA based on multiple patient models, comparing the differences between these two kinds of treatment methods, and to verify the effectiveness of Prodisc-C in noncontinuous CDA.
Methods
Geometry models
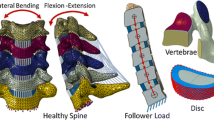
The finite element models (FEMs) of the cervical spine (C2–C7) were built according to the method reported by Rong et al. [14]. The models were constructed based on the CT images (a 0.75 mm thickness and a 0.69-mm interval, SOMATOM Definition AS+, Siemens, Germany) of 8 mild CDDD volunteers (4 male and 4 females). A commercial software Mimics 17.0 (Materialize Inc, Leuven, Belgium) was used to transform the CT images into the solid models of the C2–C7 vertebrae and output STL files. The reconstructed models were then imported into Geomagic Studio 12.0 (3D System Corporation, Rock Hill, SC, USA) to change the models into physical structures.
The devices, CoRoent® Contour (NuVasive, Inc., San Diego, CA, USA), NuVasive® Helix ACP (NuVasive, Inc. San Diego, CA, USA), and Prodisc-C (Synthes, Inc., West Chester, PA, USA ), were included in this study. CoRoent® Contour was 17 mm long, 14 mm wide, 6 mm high, and 7° lordotic. The dimensions (width, length, and thickness) of NuVasive® Helix ACP were 16 mm, 24 mm, and 2.4 mm. The diameter and length of self-tapping screws were 4.5 mm and 14 mm, respectively. Prodisc-C was 16 mm long, 15 mm wide, and 6 mm high. All the FEMs of implants were made in Solidworks 2016 (Dassault Systèmes, MA, USA).
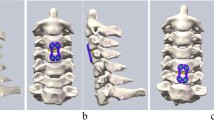
The implants and the cervical vertebra models were assembled in the software mentioned above. Considering the C3/4 and C5/6 were the most frequently discussed levels in previous studies, these two levels were chosen as the implanted levels in our study [1, 8, 12]. In the arthroplasty group, we inserted Prodisc-C at C3/4 and C5/6 after removing the anterior longitudinal ligament (ALL), the posterior longitudinal ligament (PLL), and intervertebral discs at the corresponding locations. In the fusion group, CoRoent® Contour and NuVasive® Helix ACP were implanted at C3/4 and C5/6 after removing the relevant soft tissues (Fig. 1).

FEMs of the intact group, arthroplasty group, and fusion group
Next, the high-quality FE meshes of the models were developed in Hypermesh 12.0 (Altair, Troy, MI, USA). Finally, the Models were imported into ABAQUS 6.13 (Dassault Systems Corporation, MA, USA) to set the material properties, boundary conditions, loading modes, and perform analysis.
Material properties
In these FEMs, the cortical bone and vertebral endplates were 0.4-mm thick shells [15]. The ratio of annulus fibrosus and nucleus pulposus in the intervertebral disc was 6:4; annulus fibers, which comprised 19% of the total annulus fibrosus volume, were developed with an inclination (15 to 30°) to the transverse plane [15]. The distance of the upper and lower facet articular surfaces was 0.5 mm; the facet articular surfaces were covered with articular cartilage layer; the surface to surface contact was set to nonlinear [14]. The five intervertebral ligaments, the ALL, the PLL, the ligamentum flavum (LF), the interspinous ligaments (ILs), and capsular ligaments (CLs), were modeled as tension-only truss elements and attached to the corresponding vertebrae. Table 1 showed the material properties and mesh types of FEMs.
Experimental condition
Fixed inferior surface of C7 vertebra and a tie connection between adjacent endplates and intervertebral discs were used to simulate the boundary condition in vitro experiments [16]. The cancellous bone that fills the CoRoent® Contour was set to frictionless; the simulation of the rigidly fusion between graft-vertebrae interfaces and full osseointegration between implant and vertebrae was carried out by the application of a tie constraint; the frictionless contact was applied to the implant-implant interfaces of Prodisc-C [17].
Initial loads of 75 N were used to simulate the head weight and muscle forces. The application of 1.0 N m moment on the top on the C2 vertebra was used to produce the motion of flexion, extension, lateral bending, and axial rotation. The validation of the effectiveness of our FEMs was carried out by comparing the range of motion of the segments in our FEMs with the published data. Considering the patients would attempt to move their cervical spine in a range of motion (ROM) similar to their preoperative conditions, the displacement-control test protocol was used in our subsequent evaluations.
Statistical analysis
STATA version 14.0 (Stata Corp LP, College Station, Texas, USA) was used to carry out the statistical analysis. Continuous variables were presented as mean ± standard deviations (SD). Normality of the continuous data was analyzed by Kolmogorov-Smirnov test. Normally distributed values were tested using one-way analysis of variance (ANOVA) or Student’s t test. Kruskal-Wallis test was used to analyze skew distributed values. A P value < 0.05 was statistically significant.
Results
Validation of the intact FEMs
ROMs of our FEMs in flexion-extension, lateral bending, and axial rotation were compared with the data from previous studies [8, 18,19,20]. The ROMs of the intact FEMs at C2/3, C3/4, C4/5, C5/6, and C6/7 were 4.11° ± 0.75°, 5.22° ± 1.10°, 5.74° ± 1.08°, 5.70° ± 1.11°, and 4.39° ± 0.94°, respectively, in flexion; 3.24° ± 0.79°, 4.23° ± 1.03°, 4.65° ± 1.01°, and 4.04° ± 1.03°, respectively, in extension; 5.15° ± 0.85°, 4.84° ± 1.15°, 4.73° ± 1.29°, 3.42° ± 0.77°, and 2.63° ± 0.58°, respectively, in lateral bending; and 2.04° ± 0.83°, 2.97° ± 0.79°, 3.73° ± 0.67°, 3.14° ± 0.62°, and 2.20° ± 0.93°, respectively, axial rotation (Fig. 2). The segmental ROMs of our FEMs were in good agreement with the published data.

a–d ROMs of FEMs are validated by previous studies
ROM at different levels
In comparison of ROMs at different intervertebral levels between the arthroplasty group and intact group, the results showed the ROMs in flexion of C4/5 (P = 0.032) and C6/7 (P = 0.013) in the arthroplasty group were significantly higher than that in the intact group; the ROM in lateral bending of C2/3 (P < 0.001) in the arthroplasty group was significantly less than that in the intact group; however, the ROM in lateral bending of C5/6 (P = 0.014) in the arthroplasty group was significantly more than that in the intact group. In comparison of ROMs at different intervertebral levels between the intact group and fusion group, the results showed the ROMs of C2/3 (P < 0.001, P = 0.004, P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001, P = 0.006, P = 0.002) in the intact group were significantly less than that in the fusion group in flexion, extension, and axial rotation, respectively; the ROMs of C3/4 (P < 0.001) and C5/6 (P < 0.001) in the intact group were significantly higher than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively; the ROMs in lateral bending of C4/5 (P < 0.001) and C6/7 (P = 0.002) were significantly less than that in the fusion group. In comparison of ROMs at different intervertebral levels between the arthroplasty group and fusion group, the results showed the ROMs of C2/3 (P ≤ 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001, P = 0.002, P = 0.002, P = 0.002) in the arthroplasty group were significantly less than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively; the ROMs of C3/4 (P < 0.001) and C5/6 (P < 0.001) in the arthroplasty group were significantly higher than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively. In other situations, there was no significant difference in ROMs between each of the two groups (Table 2, Fig. 3).

ROMs of FEMs under different motion states. a Flexion, b extension, c lateral bending, and d axial rotation
Intervertebral disc pressures (IDPs) at adjacent levels and in ISs
Table 3 showed that there was no significant difference in IDPs between the arthroplasty group and intact group in all situations. However, the IDPs in C2/3 (P < 0.001, P = 0.005, P < 0.001, P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) of the intact group were significantly less than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively. In addition, the IDPs in C2/3 (P < 0.001, P = 0.001, P < 0.001, P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) of the arthroplasty group were significantly less than that in the fusion group in flexion, extension, lateral bending, and axial rotation, respectively. In other situations, there was no significant difference in IDPs between each of the two groups (Fig. 4).

IDPs of FEMs under different motion states. a Flexion, b extension, c lateral bending, and d axial rotation
Contact forces of facet joints at adjacent levels and in ISs
Contact forces of facet joints in C2/3 (P = 0.010) in the arthroplasty group was significantly less than that in the intact group in extension. Contact forces of facet joints in C2/3 (P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) in the arthroplasty group was significantly less than that in the fusion group. In extension, contact forces of facet joints in C2/3 (P < 0.001), C4/5 (P < 0.001), and C6/7 (P < 0.001) in the intact group were significantly less than that in the fusion group (Table 4, Fig. 5).

The facet contact forces of FEMs at extension
Discussion
The optimal surgical treatment of multilevel CDDD is still controversial [21]. Clinical data on the surgical protocol for noncontinuous CDDD are limited [8]. ACDF is widely used to treat multilevel CDDD [22]. However, several studies reported that ACDF could result in certain complications [9, 23,24,25,26,27,28]. It has been reported that the incidences of complications in different levels of fusion are variable: the rates of internal fixation failures in one to four-level fusion are 20%, 36%, 71%, and 80%, respectively [23]; the incidences of reoperation in one to four-level fusion are 5.8%, 6.5%, 8%, and 16.8%, respectively [27]; in addition, the incidences of ASD in single-level fusion and multilevel fusion are 13.2% and 32.1%, respectively [29]. Several studies indicated that patients could benefit from CDA over ACDF in clinical scoring systems and reoperation rates in long-term follow-up [30, 31]. Meta-analysis showed that the outcomes of two-level CDA were better than the outcomes after two-level ACDF [32]. All these implied that multilevel CDA might be reasonable. Lu et al. [31] reported that there was a significant difference in diagnosis, implying that while CDA was more likely to be applied to the treatment of cervical disc herniation, it was less likely to be applied to the treatment of cervical myelopathy, cervical stenosis, and cervical spondylosis than ACDF [31]. Therefore, biomechanical studies are needed to prove the effectiveness of various surgical treatment methods.
Comparison of ROMs at different intervertebral levels between each of the two groups showed that noncontinuous CDA could significantly increase the ROM in flexion at implanted levels and lower adjacent levels. This implied that noncontinuous CDA requires high biomechanical properties of the lower adjacent intervertebral discs. Patients with intervertebral disc degeneration at the lower adjacent segments would not be eligible for this kind of treatment. Results in our study showed that noncontinuous CDA could increase ROMs of lateral bending at implanted levels. In contrast, it would limit the ROMs of lateral bending in the upper adjacent segments. This might be explained by the relatively lower center of rotations (CORs) in Prodisc-C artificial discs [33]. The limitation of lateral bending in the upper adjacent segments could preserve the facet joints from degeneration, considering larger lateral bending ROM could increase facet joint forces [34]. This might be one of the reasons why CDA could reduce the stress of facet joints.
The results of comparison of IDP between each of the two groups in our study showed that noncontinuous CDA could preserve IDP at the adjacent and intermediate levels to maintain the kinematics of cervical spine near preoperative values. However, Wu et al. [8] stated that noncontinuous CDA could slightly increase the IDPs at the superior, intermediate, and inferior adjacent levels. The possible explanation might be that they only discussed one standard symmetric FEM to draw conclusion without statistical analysis; our study analyzed eight FEMs and ran a statistical analysis to compare the differences between each of the two groups. Therefore, our results might be more convincing. In addition, the artificial intervertebral discs we used in this study were Prodisc-C artificial discs, which were different with Prestige LP artificial discs in previous studies [1, 8, 12, 13]. Previous studies reported that design concepts of artificial discs could reveal different biomechanical characteristics for the treatment of CDDD [20]. The design of Prestige LP is metal-on-metal joint without polymercore. Previous study reported that the posteriorly positioned metal-on-metal joint of Prestige LP could, even in flexion, posteriorly impose a high stress level [2]. However, Prodisc-C has a polyethylene core with much higher modulus. Compared with Prestige LP, its stress transmission could be less and its distribution of loads could be more even [2]. Therefore, the application of Prodisc-C in noncontinuous CAD may have more advantages. However, noncontinuous ACDF would significantly increase IPD at adjacent and intermediate levels. This was mainly related to the fact that ACDF reduced the ROM of surgical segments, while increased the compensation of adjacent segments, resulting in a decreased stress buffering capacity and an increased stress concentration [8].
Facet degeneration has been proved to be most important cause of neck pain [16]. Progression of facet degeneration could result from too large loading [35]. Fusion cervical model needs bigger bending moment than the intact cervical model to reach a reasonable ROM. It was reported that bigger bending moment could increase facet joint forces and segmental rotation in all adjacent segments of the fusion model [34]. Similarly, our results showed that noncontinuous ACDF would increase the contact forces of facet joints at the adjacent and intermediate levels. Therefore, our study proved that the degeneration of facet joints could be deteriorated by noncontinuous ACDF. Lee et al. [33] stated that artificial discs could increase the stresses sustained by the facet joints. The ligamentous FEM used in their study could cause several limitations in their conclusions. They found that contact forces of facet joints increased by 107% with the Prodisc-C model, which was a surprising phenomenon. Our study constructed eight FEMs based on CT images and carried out the experiment based on displacement-control test protocol, which could handle the limitations mentioned above. The results in our study showed that noncontinuous CDA could reduce facet joint forces to reach the value of intact cervical spine. It could even make the facet joint forces at adjacent levels less than that in intact cervical spine. This might be explained by the intervertebral distractive effect of Prodisc-C, which could distribute the stress of facet joints [2].
Recent studies showed that hybrid surgery (HS), which incorporated CDA at the mobile segment with ACDF at the spondylotic segment, could preserve the mobility of cervical spine to produce satisfactory clinical outcomes and reducing ASD [10, 11, 36,37,38]. Considering multilevel CDDD can have different degenerative status at each level, HS may not always be appropriate to treat this kind of disease [12]. Most of the studies on HS focused on the treatment of continuous CDDD; however, there is a lack of study on the treatment of noncontiguous CDDD [8]. Previous study reported that noncontinuous HS could cause the collapse of IS [3]. Therefore, the use of HS in the treatment of noncontinuous CDDD might be risky.
There are several limitations in our study. First, the data discussed in this study depend on eight FEMs. The biomechanics of our FEMs may not completely simulate the pathology of CDDD in vivo, considering the number of ISs may be more than one and the ISs may not always be located in C3/4. Second, the elastic modulus and Poisson’s ratio of degenerative cervical soft tissues have not been reported in the previous studies. Therefore, the simulation of real CDDD via the analysis of FEMs is very difficult. However, our study is the first to conduct statistical analysis of multiple models, which can improve the accuracy of the results. Even so, our results can only provide an estimate of the trend rather than the actual value in the real situations. Third, patients may belong to different cervical sagittal classifications. Even though we have constructed eight FEMs to reduce the influence of cervical sagittal classifications on our results, the biomechanical characteristics of cervical sagittal classifications, and their influence on surgical treatment still needs to be discussed separately in the future researches.
Conclusion
The analysis of FEMs shows that the overall therapeutic effect of noncontinuous CDA is better than that of noncontinuous ACDF in the treatment of noncontinuous CDDD. Noncontinuous CDA requires high biomechanical properties of the lower adjacent intervertebral discs. Patients with intervertebral disc degeneration at the lower adjacent segments would not be eligible for this kind of treatment. Noncontinuous CDA could preserve IDP and facet joint forces at the adjacent and intermediate levels to maintain the kinematics of cervical spine near preoperative values. However, noncontinuous ACDF would increase degenerative risks at adjacent and intermediate levels. In addition, the application of Prodisc-C in noncontinuous CAD may have more advantages than that of Prestige LP. A large number of in vivo studies are still needed to draw more reliable conclusions.
Availability of data and materials
Please contact author for data requests.
Abbreviations
- CDDD:
-
Cervical degenerative disc disease
- ACDF:
-
Anterior cervical discectomy and fusion
- IS:
-
Intermediate segment
- ASD:
-
Adjacent segment degeneration
- CDA:
-
Cervical disc arthroplasty
- FEMs:
-
Finite element models
- ALL:
-
Anterior longitudinal ligament
- PLL:
-
The posterior longitudinal ligament
- LF:
-
The ligamentum flavum
- IL:
-
The interspinous ligament
- CL:
-
Capsular ligament
- ROM:
-
Range of motion
- SD:
-
Standard deviation
- ANOVA:
-
One-way analysis of variance
- IDP:
-
Intervertebral disc pressure
- CORs:
-
Center of rotations
- HS:
-
Hybrid surgery
References
Wu TK, Wang BY, Cheng D, Rong X, Lou JG, Hong Y, Liu H. Clinical and radiographic features of hybrid surgery for the treatment of skip-level cervical degenerative disc disease: a minimum 24-month follow-up. J CLIN NEUROSCI. 2017;40:102–8 https://doi.org/10.1016/j.jocn.2017.02.030.
Lin CY, Kang H, Rouleau JP, Hollister SJ, Marca FL. Stress analysis of the interface between cervical vertebrae end plates and the Bryan, Prestige LP, and ProDisc-C cervical disc prostheses: an in vivo image-based finite element study. Spine (Phila Pa 1976). 2009;34(15):1554–60 https://doi.org/10.1097/BRS.0b013e3181aa643b.
Bertagnoli R, Yue JJ, Kershaw T, Shah RV, Pfeiffer F, Fenk-Mayer A, Nanieva R, Karg A, Husted DS, Emerson JW. Lumbar total disc arthroplasty utilizing the ProDisc prosthesis in smokers versus nonsmokers: a prospective study with 2-year minimum follow-up. Spine (Phila Pa 1976). 2006;31(9):992–7 https://doi.org/10.1097/01.brs.0000214970.07626.68.
Hilibrand AS, Fye MA, Emery SE, Palumbo MA, Bohlman HH. Increased rate of arthrodesis with strut grafting after multilevel anterior cervical decompression. Spine (Phila Pa 1976). 2002;27(2):146–51.
Wang JC, McDonough PW, Kanim LE, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for three-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 2001;26(6):643–6 646-647. https://doi.org/10.1097/00007632-200103150-00015.
Yang Y, Ma L, Liu H, Liu Y, Hong Y, Wang B, Ding C, Deng Y, Song Y, Liu L. Comparison of the incidence of patient-reported post-operative dysphagia between ACDF with a traditional anterior plate and artificial cervical disc replacement. Clin Neurol Neurosurg. 2016;148:72–8 https://doi.org/10.1016/j.clineuro.2016.07.020.
Wang HR, Li XL, Dong J, Yuan FL, Zhou J. Skip-level anterior cervical discectomy and fusion with self-locking stand-alone PEEK cages for the treatment of 2 noncontiguous levels of cervical spondylosis. J SPINAL DISORD TECH. 2013;26(7):E286–92 https://doi.org/10.1097/BSD.0b013e31828679b3.
Wu TK, Meng Y, Wang BY, Rong X, Hong Y, Ding C, Chen H, Liu H. Biomechanics following skip-level cervical disc arthroplasty versus skip-level cervical discectomy and fusion: a finite element-based study. BMC Musculoskelet Disord. 2019;20(1):49 https://doi.org/10.1186/s12891-019-2425-3.
Pimenta L, McAfee PC, Cappuccino A, Cunningham BW, Diaz R, Coutinho E. Superiority of multilevel cervical arthroplasty outcomes versus single-level outcomes: 229 consecutive PCM prostheses. Spine (Phila Pa 1976). 2007;32(12):1337–44 https://doi.org/10.1097/BRS.0b013e318059af12.
Ren X, Chu T, Jiang T, Wang W, Wang J, Li C, Zhang Z. Cervical disk replacement combined with cage fusion for the treatment of multilevel cervical disk herniation. CLIN SPINE SURG. 2016;29(6):218–25 https://doi.org/10.1097/BSD.0b013e31826994bb.
Shin DA, Yi S, Yoon DH, Kim KN, Shin HC. Artificial disc replacement combined with fusion versus two-level fusion in cervical two-level disc disease. Spine (Phila Pa 1976). 2009;34(11):1153–9 1160-1161. https://doi.org/10.1097/BRS.0b013e31819c9d39.
Wu TK, Wang BY, Deng MD, Hong Y, Rong X, Chen H, Meng Y, Liu H. A comparison of anterior cervical discectomy and fusion combined with cervical disc arthroplasty and cervical disc arthroplasty for the treatment of skip-level cervical degenerative disc disease: a retrospective study. Medicine (Baltimore). 2017;96(41):e8112 https://doi.org/10.1097/MD.0000000000008112.
Wu T, Wang B, Ding C, Meng Y, Lou J, Yang Y, Liu H. Artificial cervical disc replacement with the Prestige-LP prosthesis for the treatment of non-contiguous 2-level cervical degenerative disc disease: a minimum 24-month follow-up. Clin Neurol Neurosurg. 2017;152:57–62 https://doi.org/10.1016/j.clineuro.2016.11.015.
Rong X, Wang B, Ding C, Deng Y, Chen H, Meng Y, Yan W, Liu H. The biomechanical impact of facet tropism on the intervertebral disc and facet joints in the cervical spine. SPINE J. 2017;17(12):1926–31 https://doi.org/10.1016/j.spinee.2017.07.009.
Denoziere G, Ku DN. Biomechanical comparison between fusion of two vertebrae and implantation of an artificial intervertebral disc. J BIOMECH. 2006;39(4):766–75 https://doi.org/10.1016/j.jbiomech.2004.07.039.
Rong X, Liu Z, Wang B, Chen H, Liu H. The facet orientation of the subaxial cervical spine and the implications for cervical movements and clinical conditions. Spine (Phila Pa 1976). 2017;42(6):E320–5 https://doi.org/10.1097/BRS.0000000000001826.
Completo A, Nascimento A, Ramos A, Simoes J. Failure analysis of C-5 after total disc replacement with ProDisc-C at 1 and 2 levels and in combination with a fusion cage: finite-element and biomechanical models. J Neurosurg Spine. 2015;22(6):639–46 https://doi.org/10.3171/2014.10.SPINE14217.
Lee MJ, Dumonski M, Phillips FM, Voronov LI, Renner SM, Carandang G, Havey RM, Patwardhan AG. Disc replacement adjacent to cervical fusion: a biomechanical comparison of hybrid construct versus two-level fusion. Spine (Phila Pa 1976). 2011;36(23):1932–9 https://doi.org/10.1097/BRS.0b013e3181fc1aff.
Liu Q, Guo Q, Yang J, Zhang P, Xu T, Cheng X, Chen J, Guan H, Ni B. Subaxial cervical intradiscal pressure and segmental kinematics following atlantoaxial fixation in different angles. WORLD NEUROSURG. 2016;87:521–8 https://doi.org/10.1016/j.wneu.2015.09.025.
Panjabi MM, Crisco JJ, Vasavada A, Oda T, Cholewicki J, Nibu K, Shin E. Mechanical properties of the human cervical spine as shown by three-dimensional load-displacement curves. Spine (Phila Pa 1976). 2001;26(24):2692–700.
Li Y, Zhu J, Liao Z, Zhang Z, Liu W. Hybrid constructs for performing three-level hybrid surgery. A finite element study. World Neurosurg. 2018;114:e1302–9 https://doi.org/10.1016/j.wneu.2018.03.202.
De la Garza-Ramos R, Xu R, Ramhmdani S, Kosztowski T, Bydon M, Sciubba DM, Wolinsky JP, Witham TF, Gokaslan ZL, Bydon A. Long-term clinical outcomes following 3- and 4-level anterior cervical discectomy and fusion. J Neurosurg Spine. 2016;24(6):885–91 https://doi.org/10.3171/2015.10.SPINE15795.
Swank ML, Lowery GL, Bhat AL, McDonough RF. Anterior cervical allograft arthrodesis and instrumentation: multilevel interbody grafting or strut graft reconstruction. EUR SPINE J. 1997;6(2):138–43 https://doi.org/10.1007/bf01358747.
Lowery GL, McDonough RF. The significance of hardware failure in anterior cervical plate fixation. Patients with 2- to 7-year follow-up. Spine (Phila Pa 1976). 1998;23(2):181–6 186-187. https://doi.org/10.1097/00007632-199801150-00006.
Park MS, Ju YS, Moon SH, Kim TH, Oh JK, Makhni MC, Riew KD. Reoperation rates after anterior cervical discectomy and fusion for cervical spondylotic radiculopathy and myelopathy: a national population-based study. Spine (Phila Pa 1976). 2016;41(20):1593–9 https://doi.org/10.1097/BRS.0000000000001590.
Burkhardt BW, Brielmaier M, Schwerdtfeger K, Sharif S, Oertel JM. Smith-Robinson procedure with an autologous iliac crest graft and Caspar plating. Report of 65 patients with an average follow-up of 22 years. WORLD NEUROSURG. 2016;90:244–50 https://doi.org/10.1016/j.wneu.2016.02.074.
Geisler FH, Caspar W, Pitzen T, Johnson TA. Reoperation in patients after anterior cervical plate stabilization in degenerative disease. Spine (Phila Pa 1976). 1998;23(8):911–20 https://doi.org/10.1097/00007632-199804150-00013.
Song KJ, Yoon SJ, Lee KB. Three- and four-level anterior cervical discectomy and fusion with a PEEK cage and plate construct. Eur Spine J. 2012;21(12):2492–7 https://doi.org/10.1007/s00586-012-2447-0.
Chung JY, Kim SK, Jung ST, Lee KB. Clinical adjacent-segment pathology after anterior cervical discectomy and fusion: results after a minimum of 10-year follow-up. SPINE J. 2014;14(10):2290–8 https://doi.org/10.1016/j.spinee.2014.01.027.
Hisey MS, Bae HW, Davis RJ, Gaede S, Hoffman G, Kim KD, Nunley PD, Peterson D, Rashbaum RF, Stokes J, et al. Prospective, Randomized comparison of cervical total disk replacement versus anterior cervical fusion: results at 48 months follow-up. J SPINAL DISORD TECH. 2015;28(4):E237–43 https://doi.org/10.1097/BSD.0000000000000185.
Lu Y, McAnany SJ, Hecht AC, Cho SK, Qureshi SA. Utilization trends of cervical artificial disc replacement after FDA approval compared with anterior cervical fusion: adoption of new technology. Spine (Phila Pa 1976). 2014;39(3):249–55 https://doi.org/10.1097/BRS.0000000000000113.
McAnany SJ, Baird EO, Overley SC, Kim JS, Qureshi SA, Anderson PA. A meta-analysis of the clinical and fusion results following treatment of symptomatic cervical pseudarthrosis. Global Spine J. 2015;5(2):148–55 https://doi.org/10.1055/s-0035-1544176.
Lee JH, Park WM, Kim YH, Jahng TA. A biomechanical analysis of an artificial disc with a shock-absorbing core property by using whole-cervical spine finite element analysis. Spine (Phila Pa 1976). 2016;41(15):E893–901 https://doi.org/10.1097/BRS.0000000000001468.
Erbulut DU, Zafarparandeh I, Hassan CR, Lazoglu I, Ozer AF. Determination of the biomechanical effect of an interspinous process device on implanted and adjacent lumbar spinal segments using a hybrid testing protocol: a finite-element study. J Neurosurg Spine. 2015;23(2):200–8 https://doi.org/10.3171/2014.12.SPINE14419.
Bogduk N. On cervical zygapophysial joint pain after whiplash. Spine (Phila Pa 1976). 2011;36(25 Suppl):S194–9 https://doi.org/10.1097/BRS.0b013e3182387f1d.
Shi JS, Lin B, Xue C, Zhang HS, Chen ZD, Zhao ZS. Clinical and radiological outcomes following hybrid surgery in the treatment of multi-level cervical spondylosis: over a 2-year follow-up. J ORTHOP SURG RES. 2015;10:185 https://doi.org/10.1186/s13018-015-0330-5.
Ding C, Gong Q, Hong Y, Wang BY, Liu H. Cervical disc arthroplasty combined with interbody fusion for the treatment of cervical myelopathy with diffuse idiopathic skeletal hyperostosis: a case report. Chin Med J (Engl). 2016;129(15):1877–9 https://doi.org/10.4103/0366-6999.186628.
Chen J, Xu L, Jia YS, Sun Q, Li JY, Zheng CY, Bai CX, Yu QS. Cervical anterior hybrid technique with bi-level Bryan artificial disc replacement and adjacent segment fusion for cervical myelopathy over three consecutive segments. J CLIN NEUROSCI. 2016;27:59–62 https://doi.org/10.1016/j.jocn.2015.07.030.
Acknowledgements
This research was performed mainly at the Department of Orthopaedics of Xuanwu Hospital Capital Medical University and in the National Clinical Research Center for Geriatric Diseases.
Funding
This study was funded by China Scholarship Council (no. 201908110337), National Natural Science Foundation of China (no. 81672201, no. 81871794), and Beijing Municipal Commission of Health and Family Planning (no. PXM2017 026283 000002).
Author information
Authors and Affiliations
Contributions
XS designed the study and constructed FEMs. SL, XL, and JZD collected the crucial background information. WW collected the data. CK analyzed the data. SS interpreted the data and did the figure editing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethics Committee of the Xuanwu Hospital Capital Medical University approved this study. The approval number is clinical study review [2018] 083. This research was registered in the Chinese Clinical Trial Registry (ChiCTR1900020513). Written informed consent of each patient was obtained prior to the study. All patients included in the study provided their informed consent at enrolment on the use of patients’ data for research.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sun, X., Sun, S., Zhang, T. et al. Biomechanical comparison of noncontiguous cervical disc arthroplasty and noncontiguous cervical discectomy and fusion in the treatment of noncontinuous cervical degenerative disc disease: a finite element analysis. J Orthop Surg Res 15, 36 (2020). https://doi.org/10.1186/s13018-020-1549-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-020-1549-3