
Abstract
Background
Sustaining evidence-based practices (EBPs) is crucial to ensuring care quality and addressing health disparities. Approaches to identifying factors related to sustainability are critically needed. One such approach is Matrixed Multiple Case Study (MMCS), which identifies factors and their combinations that influence implementation. We applied MMCS to identify factors related to the sustainability of the evidence-based Collaborative Chronic Care Model (CCM) at nine Department of Veterans Affairs (VA) outpatient mental health clinics, 3–4 years after implementation support had concluded.
Methods
We conducted a directed content analysis of 30 provider interviews, using 6 CCM elements and 4 Integrated Promoting Action on Research Implementation in Health Services (i-PARIHS) domains as codes. Based on CCM code summaries, we designated each site as high/medium/low sustainability. We used i-PARIHS code summaries to identify relevant factors for each site, the extent of their presence, and the type of influence they had on sustainability (enabling/neutral/hindering/unclear). We organized these data into a sortable matrix and assessed sustainability-related cross-site trends.
Results
CCM sustainability status was distributed among the sites, with three sites each being high, medium, and low. Twenty-five factors were identified from the i-PARIHS code summaries, of which 3 exhibited strong trends by sustainability status (relevant i-PARIHS domain in square brackets): “Collaborativeness/Teamwork [Recipients],” “Staff/Leadership turnover [Recipients],” and “Having a consistent/strong internal facilitator [Facilitation]” during and after active implementation. At most high-sustainability sites only, (i) “Having a knowledgeable/helpful external facilitator [Facilitation]” was variably present and enabled sustainability when present, while (ii) “Clarity about what CCM comprises [Innovation],” “Interdisciplinary coordination [Recipients],” and “Adequate clinic space for CCM team members [Context]” were somewhat or less present with mixed influences on sustainability.
Conclusions
MMCS revealed that CCM sustainability in VA outpatient mental health clinics may be related most strongly to provider collaboration, knowledge retention during staff/leadership transitions, and availability of skilled internal facilitators. These findings have informed a subsequent CCM implementation trial that prospectively examines whether enhancing the above-mentioned factors within implementation facilitation improves sustainability. MMCS is a systematic approach to multi-site examination that can be used to investigate sustainability-related factors applicable to other EBPs and across multiple contexts.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
The sustainability of evidence-based practices (EBPs) over time is crucial to maximize the public health impact of EBPs implemented into routine care. Implementation evaluators focus on sustainability as a central implementation outcome, and funders of implementation efforts seek sustained long-term returns on their investment. Furthermore, practitioners and leadership at implementation sites face the task of sustaining an EBP’s usage even after implementation funding, support, and associated evaluation efforts conclude. The circumstances and influences contributing to EBP sustainability are therefore of high interest to the field of implementation science.
Sustainability depends on the specific EBP being implemented, the individuals undergoing the implementation, the contexts in which the implementation takes place, and the facilitation of (i.e., support for) the implementation. Hence, universal conditions that invariably lead to sustainability are challenging to establish. Even if a set of conditions could be identified as being associated with high sustainability “on average,” its usefulness is questionable when most real-world implementation contexts may deviate from “average” on key implementation-relevant metrics.
Thus, when seeking a better understanding of EBP sustainability, there is a critical need for methods that examine the ways in which sustainability varies in diverse contexts. One such method is Matrixed Multiple Case Study (MMCS) [1], which is beginning to be applied in implementation research to identify factors related to implementation [2,3,4,5]. MMCS capitalizes on the many contextual variations and heterogeneous outcomes that are expected when an EBP is implemented across multiple sites. Specifically, MMCS provides a formalized sequence of steps for cross-site analysis by arranging data into an array of matrices, which are sorted and filtered to test for expected factors and identify less expected factors influencing an implementation outcome of interest.
Although the MMCS represents a promising method for systematically exploring the “black box” of the ways in which implementation is more or less successful, it has not yet been applied to investigate the long-term sustainability of implemented EBPs. Therefore, we applied MMCS to identify factors related to the sustainability of the evidence-based Collaborative Chronic Care Model (CCM), previously implemented using implementation facilitation [6,7,8], at nine VA medical centers’ outpatient general mental health clinics. An earlier interview-based investigation of CCM provider perspectives had identified key determinants of CCM sustainability at the sites, yet characteristics related to the ways in which CCM sustainability differed at the sites are still not well understood. For this reason, our objective was to apply MMCS to examine the interview data to determine factors associated with CCM sustainability at each site.
Methods
Clinical and implementation contexts
CCM-based care aims to ensure that patients are treated in a coordinated, patient-centered, and anticipatory manner. This project’s nine outpatient general mental health clinics had participated in a hybrid CCM effectiveness-implementation trial 3 to 4 years prior, which had resulted in improved clinical outcomes that were not universally maintained post-implementation (i.e., after implementation funding and associated evaluation efforts concluded) [7, 9]. This lack of aggregate sustainability across the nine clinics is what prompted the earlier interview-based investigation of CCM provider perspectives that identified key determinants of CCM sustainability at the trial sites [10].
These prior works were conducted in VA outpatient mental health teams, known as Behavioral Health Interdisciplinary Program (BHIP) teams. While there was variability in the exact composition of each BHIP team, all teams consisted of a multidisciplinary set of frontline clinicians (e.g., psychiatrists, psychologists, social workers, nurses) and support staff, serving a panel of about 1000 patients each.
This current project applied MMCS to examine the data from the earlier interviews [10] for the ways in which CCM sustainability differed at the sites and the factors related to sustainability. The project was determined to be non-research by the VA Boston Research and Development Service, and therefore did not require oversight by the Institutional Review Board (IRB). Details regarding the procedures undertaken for the completed hybrid CCM effectiveness-implementation trial, which serves as the context for this project, have been previously published [6, 7]. Similarly, details regarding data collection for the follow-up provider interviews have also been previously published [10]. We provide a brief overview of the steps that we took for data collection and describe the steps that we took for applying MMCS to analyze the interview data. Additional file 1 outlines our use of the Consolidated Criteria for Reporting Qualitative Research (COREQ) Checklist [11].
Data collection
We recruited 30 outpatient mental health providers across the nine sites that had participated in the CCM implementation trial, including a multidisciplinary mix of mental health leaders and frontline staff. We recruited participants via email, and we obtained verbal informed consent from all participants. Each interview lasted between 30 and 60 min and focused on the degree to which the participant perceived care processes to have remained aligned to the CCM’s six core elements: work role redesign, patient self-management support, provider decision support, clinical information systems, linkages to community resources, and organizational/leadership support [12,13,14]. Interview questions also inquired about the participant’s perceived barriers and enablers influencing CCM sustainability, as well as about the latest status of CCM-based care practices. Interviews were digitally recorded and professionally transcribed. Additional details regarding data collection have been previously published [10].
Data analysis
We applied MMCS’ nine analytical steps [1] to the interview data. Each step described below was led by one designated member of the project team, with subsequent review by all project team members to reach a consensus on the examination conducted for each step.
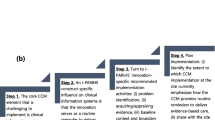
We established the evaluation goal (step 1) to identify the ways in which sustainability differed across the sites and the factors related to sustainability, defining sustainability (step 2) as the continued existence of CCM-aligned care practices—namely, that care processes remained aligned with the six core CCM elements. Table 1 shows examples of care processes that align with each CCM element. As our prior works directly leading up to this project (i.e., design and evaluation of the CCM implementation trial that involved the very sites included in this project [6, 15, 16]) were guided by the Integrated Promoting Action on Research Implementation in Health Services (i-PARIHS) framework [17] and i-PARIHS positions facilitation (the implementation strategy that our trial was testing) as the core ingredient that drives implementation [17], we selected i-PARIHS’ four domains—innovation, recipients, context, and facilitation—as relevant domains under which to examine factors influencing sustainability (step 3). i-PARIHS posits that the successful implementation of an innovation and its sustained use by recipients in a context is enabled by facilitation (both the individuals doing the facilitation and the process used for facilitation). We examined the data on both sustainability and potentially relevant i-PARIHS domains (step 4) by conducting directed content analysis [18] of the recorded and professionally transcribed interview data. We used the six CCM elements and the four i-PARIHS domains as a priori codes.
Additional file 2 provides an overview of data input, tasks performed, and analysis output for MMCS steps 5 through 9 described below. We assessed sustainability per site (step 5) by generating CCM code summaries per site, and reached a consensus on whether each site exhibited high, medium, or low sustainability relative to other sites based on the summary data. We assigned a higher sustainability level for sites that exhibited more CCM-aligned care processes, had more participants consistently mention those processes, and considered those processes more as “just the way things are done” at the site. Namely, (i) high sustainability sites had concrete examples of CCM-aligned care processes (such as the ones shown in Table 1) for many of the six CCM elements, which multiple participants mentioned as central to how they deliver care, (ii) low sustainability sites had only a few concrete examples of CCM-aligned care processes, mentioned by only a small subset of participants and/or inconsistently practiced, and (iii) medium sustainability sites matched neither of the high nor low sustainability cases, having several concrete examples of CCM-aligned care process for some of the CCM elements, varying in whether they are mentioned by multiple participants or how consistently they are a part of delivering care. For the CCM code summaries per site, one project team member initially reviewed the coded data to draft the summaries including exemplar quotes. Each summary and relevant exemplar quotes were then reviewed by and refined with input from all six project team members during recurring team meetings to finalize the high, medium, or low sustainability designation to use in the subsequent MMCS steps. Reviewing and refining the summaries for the nine sites took approximately four 60-min meetings of the six project team members, with each site’s CCM code summary taking approximately 20–35 min to discuss and reach consensus on. We referred to lists of specific examples of how the six core CCM elements were operationalized in our CCM implementation trial [19, 20]. Refinements occurred mostly around familiarizing the newer members of the project team (i.e., those who had not participated in our prior CCM-related work) with the examples and definitions. We aligned to established qualitative analysis methods for consensus-reaching discussions [18, 21]. Recognizing the common challenge faced by such discussions in adequately accounting for everyone’s interpretations of the data [22], we drew on Bens’ meeting facilitation techniques [23] that include setting ground rules, ensuring balanced participation from all project team members, and accurately recording decisions and action items.
We then identified influencing factors per site (step 6), by generating i-PARIHS code summaries per site and identifying distinct factors under each domain of i-PARIHS (e.g., Collaborativeness and teamwork as a factor under the Recipients domain). For the i-PARIHS code summaries per site, one project team member initially reviewed the coded data to draft the summaries including exemplar quotes. They elaborated on each i-PARIHS domain-specific summary by noting distinct factors that they deemed relevant to the summary, proposing descriptive wording to refer to each factor (e.g., “team members share a commitment to their patients” under the Recipients domain). Each summary, associated factor descriptions, and relevant exemplar quotes were then reviewed and refined with input from all six project team members during recurring team meetings to finalize the relevant factors to use in the subsequent MMCS steps. Finalizing the factors included deciding which similar proposed factor descriptions from different sites to consolidate into one factor and which wording to use to refer to the consolidated factor (e.g., “team members share a commitment to their patients,” “team members collaborate well,” and “team members know each other’s styles and what to expect” were consolidated into the Collaborativeness and teamwork factor under the Recipients domain). It took approximately four 60-min meetings of the six project team members to review and refine the summaries and factors for the nine sites, with each site’s i-PARIHS code summary and factors taking approximately 20–35 min to discuss and reach consensus on. We referred to lists of explicit definitions of i-PARIHS constructs that our team members had previously developed and published [16, 24]. We once again aligned to established qualitative analysis methods for consensus-reaching discussions [18, 21], drawing on Bens’ meeting facilitation techniques [23] to adequately account for everyone’s interpretations of the data [22].
We organized the examined data (i.e., the assessed sustainability and identified factors per site) into a sortable matrix (step 7) using Microsoft Excel [25], laid out by influencing factor (row), sustainability (column), and site (sheet). We conducted within-site analysis of the matrixed data (step 8), examining the data on each influencing factor and designating whether the factor (i) was present, somewhat present, or minimally present [based on aggregate reports from the site’s participants; used “minimally present” when, considering all available data from a site regarding a factor, the factor was predominantly weak (e.g., predominantly weak Ability to continue patient care during COVID at a medium sustainability site); used “somewhat present” when, considering all available data from a site regarding a factor, the factor was neither predominantly strong nor predominantly weak (e.g., neither predominantly strong nor predominantly weak Collaborativeness and teamwork at a low sustainability site)], and (ii) had an enabling, hindering, or neutral/unclear influence on sustainability (designated as “neutral” when, considering all available data from a site regarding a factor, the factor had neither a predominantly enabling nor a predominantly hindering influence on sustainability). These designations of factors’ presence and influence are conceptually representative of what is commonly referred to as magnitude and valence, respectively, by other efforts that construct scoring for qualitative data (e.g., [26, 27]). Like the team-based consensus approach of earlier MMCS steps, factors’ presence and type of influence per site were initially proposed by one project team member after reviewing the matrix’s site-specific data, then refined with input from all project team members during recurring team meetings that reviewed the matrix. Accordingly, similar to the earlier MMCS steps, we aligned to established qualitative methods [18, 21] and meeting facilitation techniques [23] for these consensus-reaching discussions.
We then conducted a cross-site analysis of the matrixed data (step 9), assessing whether factors and their combinations were (i) present across multiple sites, (ii) consistently associated with higher or lower sustainability, and (iii) emphasized at some sites more than others. We noted that any factor may have not come up during interviews with a site because either it is not pertinent or it is pertinent but still did not come up, although we asked an open-ended question at the end of each interview about whether there was anything else that the participant wanted to share regarding sustainability. To adequately account for these possibilities, we decided as a team to regard a factor or a combination of factors as being associated with high/medium/low sustainability if it was identified at a majority (i.e., even if not all) of the sites designated as high/medium/low sustainability (e.g., if the Collaborativeness and teamwork factor is identified at a majority, even if not all, of the high sustainability sites, we would find it to be associated with high sustainability). Like the team-based consensus approach of earlier MMCS steps, cross-site patterns were initially proposed by one project team member after reviewing the matrix’s cross-site data, then refined with input from all project team members during recurring team meetings that reviewed the matrix. Accordingly, similar to the earlier MMCS steps, we aligned to established qualitative methods [18, 21] and meeting facilitation techniques [23] for these consensus-reaching discussions. We acknowledged the potential existence of additional factors influencing sustainability that may not have emerged during our interviews and also may vary substantially between sites. For example, adaptation of the CCM, characteristics of the patient population, and availability of continued funding, which are factors that extant literature reports as being relevant to sustainability [28, 29], were not seen in our interview data. To maintain our analytic focus on the factors seen in our data, we did not add these factors to our analysis.
Results
For the nine sites included in this project, we found the degree of CCM sustainability to be split evenly across the sites—three high-, three medium-, and three low-sustainability. Twenty-five total influencing factors were identified under the i-PARIHS domains of Innovation (6), Recipients (6), Context (8), and Facilitation (5). Table 2 shows these identified influencing factors by domain. Figure 1 shows 11 influencing factors that were identified for at least two sites within a group of high/medium/low sustainability sites—e.g., the factor “consistent and strong internal facilitator” is shown as being present at high sustainability sites with an enabling influence on sustainability, because it was identified as such at two or more of the high sustainability sites. Of these 11 influencing factors, four were identified only for sites with high CCM sustainability and two were identified only for sites with medium or low CCM sustainability.

Influencing factors that were identified for at least two sites within a group of high/medium/low sustainability sites
Key trends in influencing factors associated with high, medium, and/or low CCM sustainability
Three factors across two i-PARIHS domains exhibited strong trends by sustainability status. They were the Collaborativeness and teamwork and Turnover of clinic staff and leadership factors under the Recipients domain, and the Having a consistent and strong internal facilitator factor under the Facilitation domain.
Recipients-related factors
Collaborativeness and teamwork was present with an enabling influence on CCM sustainability at most high and medium sustainability sites, while it was only somewhat present with a neutral influence on CCM sustainability at most low sustainability sites. When asked what had made their BHIP team work well, a participant from a high sustainability site said,
“Just a collaborative spirit.” (Participant 604)
A participant from a medium sustainability site said,
“We joke that [the BHIP teams] are even family, that the teams really do function pretty tightly and they each have their own personality.” (Participant 201)
At the low sustainability sites, willingness to work as a team varied across team members; a participant from a low sustainability site said,
“… I think it has to be the commitment of the people who are on the team. So those that are regularly attending, we get a lot more out of it than those that probably don't ever come [to team meetings].” (Participant 904)
Collaborativeness and teamwork of BHIP team members were often perceived as the highlight of pursuing interdisciplinary care.
Turnover of clinic staff and leadership was present with a hindering influence on CCM sustainability at most high, medium, and low sustainability sites.
“We’ve lost a lot of really, really good providers here in the time I’ve been here …,” (Participant 102)
said a participant from a low-sustainability site that had to reconfigure its BHIP teams due to clinic staff shortages. Turnover of mental health clinic leadership made it difficult to maintain CCM practices, especially beyond the teams that participated in the original CCM implementation trial. A participant from a medium sustainability site said,
“Probably about 90 percent of the things that we came up with have fallen by the wayside. Within our team, many of those remain but again, that hand off towards the other teams that I think partly is due to the turnover rate with program managers, supervisors, didn’t get fully implemented.” (Participant 703)
Although turnover was an issue for high sustainability sites as well, there was also indication of the situation improving in recent years; a participant from a high sustainability site said,
“… our attrition rollover rate has dropped quite a bit and I would really attribute that to [the CCM being] more functional and more sustainable and tolerable for the providers.” (Participant 502)
As such, staff and leadership turnover was deemed a major challenge for CCM sustainability for all sites regardless of the overall level of sustainability.
Facilitation-related factor
Having a consistent and strong internal facilitator was present with an enabling influence on CCM sustainability at high sustainability sites, not identified as an influencing factor at most of the medium sustainability sites, and variably present with a hindering, neutral, or unclear influence on CCM sustainability at low sustainability sites. Participants from a high sustainability site perceived that it was important for the internal facilitator to understand different BHIP team members’ personalities and know the clinic’s history. A participant from another high sustainability site shared that, as an internal facilitator themselves, they focused on recognizing and reinforcing the progress of team members:
“… I'm often the person who kind of [starts] off with, ‘Hey, look at what we've done in this location,’ ‘Hey look at what the team's done this month.’” (Participant 402)
A participant from a low sustainability site had also served as an internal facilitator and recounted the difficulty and importance of readying the BHIP team to function in the long run without their assistance:
“I should have been able to get out sooner, I think, to get it to have them running this themselves. And that was just a really difficult process.” (Participant 301)
Participants, especially from the high and low sustainability sites, attributed their BHIP teams’ successes and challenges to the skills of the internal facilitator.
Influencing factors identified only for sites with high CCM sustainability
Four factors across four i-PARIHS domains were identified for high sustainability sites and not for medium or low sustainability sites. They were the factors Details about the CCM being well understood (Innovation domain), Interdisciplinary coordination (Recipients domain), Having adequate clinic space for CCM team members (Context domain), and Having a knowledgeable and helpful external facilitator (Facilitation domain).
Innovation-related factor
Details about the CCM being well understood was minimal to somewhat present with an unclear influence on CCM sustainability.
“We’ve … been trying to help our providers see the benefit of team-based care and the episodes-of-care idea, and I would say that is something our folks really have continued to struggle with as well,” (Participant 401)
said a participant from a high sustainability site. “What is considered CCM-based care?” continued to be a question on providers’ minds. A participant from a high sustainability site asked during the interview,
“Is there kind of a clearing house of some of the best practices for [CCM] that you guys have … or some other collection of resources that we could draw from?” (Participant 601)
Although such references are indeed accessible online organization-wide, participants were not always aware of those resources or what exactly CCM entails.
Recipients-related factor
Interdisciplinary coordination was somewhat present with a hindering, neutral, or unclear influence on CCM sustainability. Coordination between psychotherapy and psychiatry providers was deemed difficult by participants from high-sustainability sites. A participant said,
“We were initially kind of top heavy on the psychiatry so just making sure we have … therapy staff balancing that out [has been important].” (Participant 501)
Another participant perceived that BHIP teams were helpful in managing.
… ‘sibling rivalry’ between different disciplines … because [CCM] puts us all in one team and we communicate.” (Participant 505)
Interdisciplinary coordination was understood by the participants as being necessary for effective CCM-based care yet difficult to achieve.
Context-related factor
Having adequate clinic space for CCM team members was minimal to somewhat present with a hindering, neutral, or unclear influence on CCM sustainability. COVID-19 led to changes in how clinic space was used/assigned. A participant from a high sustainability site remarked,
“Pre-COVID everything was in a room instead of online. And now all our meetings are online and so it's actually really easy for the supervisors to be able to rotate through them and then, you know, they can answer programmatic questions ….” (Participant 402)
Participants from another high sustainability site found that issues regarding limited clinic space were both exacerbated and alleviated by COVID, with the mental health service losing space to vaccine clinics but more mental health clinicians teleworking and in less need of clinic space. Virtual connections were seen to alleviate some physical workspace-related concerns.
Facilitation-related factor
Having a knowledgeable and helpful external facilitator was variably present; when present, it had an enabling influence on CCM sustainability. Participants from a high sustainability site noted how many of the external facilitator’s efforts to change the BHIP team’s work processes very much remained over time. An example of a change was to have team meetings be structured to meet evolving patient needs. Team members came to meetings with the shared knowledge and expectation that,
“… we need to touch on folks who are coming out of the hospital, we need to touch on folks with higher acuity needs.” (Participant 402)
Implementation support that sites received from their external facilitator mostly occurred during the time period of the original CCM implementation trial; correspondence with the external facilitator after that trial time period was not common for sites. Participants still largely found the external facilitator to provide helpful guidance and advice on delivering CCM-based care.
Influencing factors identified only for sites with medium or low CCM sustainability
Two factors were identified for medium or low sustainability sites and not for high sustainability sites. They were the factors Ability to continue patient care during COVID and Adequate resources/capacity for care delivery. These factors were both under i-PARIHS’ Context domain, unlike the influencing factors above that were identified only for high sustainability sites, which spanned all four i-PARIHS domains.
Context-related factors
Ability to continue patient care during COVID had a hindering influence on CCM sustainability when minimally present. Participants felt that their CCM work was challenged when delivering care through telehealth was made difficult—e.g., at a medium sustainability site, site policies during the pandemic required a higher number of in-person services than the BHIP team providers expected or desired to deliver. On the other hand, this factor had an enabling influence on CCM sustainability when present. A participant at a low sustainability site mentioned the effect of telehealth on being able to follow up more easily with patients who did not show up for their appointments:
“… my no-show rate has dropped dramatically because if people don’t log on after a couple minutes, I call them. They're like ‘oh, I forgot, let me pop right on,’ whereas, you know, in the face-to-face space, you know, you wait 15 minutes, you call them, it’s too late for them to come in so then they're no shows.” (Participant 102)
The advantages of virtual care delivery, as well as the challenges of getting approvals to pursue it to varying extents, were well recognized by the participants.
Adequate resources/capacity for care delivery was minimally present at medium sustainability sites with a hindering influence on CCM sustainability. At a medium sustainability site, although leadership was supportive of CCM, resources were being used to keep clinics operational (especially during COVID) rather than investing in building new CCM-based care delivery processes.
“I think that if my boss came to me, [and asked] what could I do for [the clinics] … I would say even more staff,” (Participant 202)
said a participant from a medium sustainability site. At the same time, the participant, as many others we interviewed, understood and emphasized the need for BHIP teams to proceed with care delivery even when resources were limited:
“… when you’re already dealing with a very busy clinic, short staff and then you’re hit with a pandemic you handle it the best that you can.” (Participant 202)
Participants felt the need for basic resource requirements to be met in order for CCM-based care to be feasible.
Discussion
In this project, we examined factors influencing the sustainability of CCM-aligned care practices at general mental health clinics within nine VA medical centers that previously participated in a CCM implementation trial. Guided by the core CCM elements and i-PARIHS domains, we conducted and analyzed CCM provider interviews. Using MMCS, we found CCM sustainability to be split evenly across the nine sites (three high, three medium, and three low), and that sustainability may be related most strongly to provider collaboration, knowledge retention during staff/leadership transitions, and availability of skilled internal facilitators.
In comparison to most high sustainability sites, participants from most medium or low sustainability sites did not mention a knowledgeable and helpful external facilitator who enabled sustainability. Participants at the high sustainability sites also emphasized the need for clarity about what CCM-based care comprises, interdisciplinary coordination in delivering CCM-aligned care, and adequate clinic space for BHIP team members to connect and collaborate. In contrast, in comparison to participants at most high sustainability sites, participants at most medium or low sustainability sites emphasized the need for better continuity of patient-facing activities during the COVID-19 pandemic and more resources/capacity for care delivery. A notable difference between these two groups of influencing factors is that the ones emphasized at most high sustainability sites are more CCM-specific (e.g., external facilitator with CCM expertise, knowledge, and structures to support delivery of CCM-aligned care), while the ones emphasized at most medium or low sustainability sites are factors that certainly relate to CCM sustainability but are focused on care delivery operations beyond CCM-aligned care (e.g., COVID’s widespread impacts, limited staff availability). In short, an emphasis on immediate, short-term clinical needs in the face of the COVID-19 pandemic and staffing challenges appeared to sap sites’ enthusiasm for sustaining more collaborative, CCM-consistent care processes.
Our previous qualitative analysis of these interview data suggested that in order to achieve sustainability, it is important to establish appropriate infrastructure, organizational readiness, and mental health service- or department-wide coordination for CCM implementation [10]. The findings from the current project augment these previous findings by highlighting the specific factors associated with higher and lower CCM sustainability across the project sites. This additional knowledge provides two important insights into what CCM implementation efforts should prioritize with regard to the previously recommended appropriate infrastructure, readiness, and coordination. First, for knowledge retention and coordination during personnel changes (including any changes in internal facilitators through and following implementation), care processes and their specific procedures should be established and documented in order to bring new personnel up to speed on those care processes. Management sciences, as applied to health care and other fields, suggest that such organizational knowledge retention can be maximized when there are (i) structures set up to formally recognize/praise staff when they share key knowledge, (ii) succession plans to be applied in the event of staff turnover, (iii) opportunities for mentoring and shadowing, and (iv) after action reviews of conducted care processes, which allow staff to learn about and shape the processes themselves [30,31,32,33]. Future CCM implementation efforts may thus benefit from enacting these suggestions alongside establishing and documenting CCM-based care processes and associated procedures.
Second, efforts to implement CCM-aligned practices into routine care should account for the extent to which sites’ more fundamental operational needs are met or being addressed. That information can be used to appropriately scope the plan, expectations, and timeline for implementation. For instance, ongoing critical staffing shortages or high turnover [34] at a site are unlikely to be resolved through a few months of CCM implementation. In fact, in that situation, it is possible that CCM implementation efforts could lead to reduced team effectiveness in the short term, given the effort required to establish more collaborative and coordinated care processes [35]. Should CCM implementation move forward at a given site, implementation goals ought to be set on making progress in realms that are within the implementation effort’s control (e.g., designing CCM-aligned practices that take staffing challenges into consideration) [36, 37] rather than on factors outside of the effort’s control (e.g., staffing shortages). As healthcare systems determine how to deploy support (e.g., facilitators) to sites for CCM implementation, they would benefit from considering whether it is primarily CCM expertise that the site needs at the moment, or more foundational organizational resources (e.g., mental health staffing, clinical space, leadership enhancement) [38] to first reach an operational state that can most benefit from CCM implementation efforts at a later point in time. There is growing consensus across the field that the readiness of a healthcare organization to innovate is a prerequisite to successful innovation (e.g., CCM implementation) regardless of the specific innovation [39, 40]. Several promising strategies specifically target these organizational considerations for implementing evidence-based practices (e.g., [41, 42]). Further, recent works have begun to more clearly delineate leadership-related, climate-related, and other contextual factors that contribute to organizations’ innovation readiness [43], which can inform healthcare systems’ future decisions regarding preparatory work leading to, and timing of, CCM implementation at their sites.
These considerations informed by MMCS may have useful implications for implementation strategy selection and tailoring for future CCM implementation efforts, especially in delineating the target level (e.g., system, organizational, clinic, individual) and timeline of implementation strategies to be deployed. For instance, of the three factors found to most notably trend with CCM sustainability, Collaborativeness and teamwork may be strengthened through shorter-term team-building interventions at the organizational and/or clinic levels [38], Turnover of clinic staff and leadership may be mitigated by aiming for longer-term culture/climate change at the system and/or organizational levels [44,45,46], and Having a consistent and strong internal facilitator may be ensured more immediately by selecting an individual with fitting expertise/characteristics to serve in the role [15] and imparting innovation/facilitation knowledge to them [47]. Which of these factors to focus on, and through what specific strategies, can be decided in partnership with an implementation site—for instance, candidate strategies can be identified based on ones that literature points to for addressing these factors [48], systematic selection of the strategies to move forward can happen with close input from site personnel [49], and explicit further specification of those strategies [50] can also happen in collaboration with site personnel to amply account for site-specific contexts [51].
As is common for implementation projects, the findings of this project are highly context-dependent. It involves the implementation of a specific evidence-based practice (the CCM) using a specific implementation strategy (implementation facilitation) at specific sites (BHIP teams within general mental health clinics at nine VA medical centers). For such context-dependent findings to be transferable [52, 53] to meaningfully inform future implementation efforts, sources of variation in the findings and how the findings were reached must be documented and traceable. This means being explicit about each step and decision that led up to cross-site analysis, as MMCS encourages, so that future implementation efforts can accurately view and consider why and how findings might be transferable to their own work. For instance, beyond the finding that Turnover of clinic staff and leadership was a factor present at most of the examined sites, MMCS’ traceable documentation of qualitative data associated with this factor at high sustainability sites also allowed highlighting the perception that CCM implementation is contributing to mitigating turnover of providers in the clinic over time, which may be a crucial piece of information that fuels future CCM implementation efforts.
Furthermore, to compare findings and interpretations across projects, consistent procedures for setting up and conducting these multi-site investigations are indispensable [54,55,56]. Although many projects involve multiple sites and assess variations across the sites, it is less common to have clearly delineated protocols for conducting such assessments. MMCS is meant to target this very gap, by offering a formalized sequence of steps that prompt specification of analytical procedures and decisions that are often interpretive and left less specified. MMCS uses a concrete data structure (the matrix) to traceably organize information and knowledge gained from a project, and the matrix can accommodate various data sources and conceptual groundings (e.g., guiding theories, models, and frameworks) that may differ from project to project – for instance, although our application of MMCS aligned to i-PARIHS, other projects applying MMCS [2, 5] use different conceptual guides (e.g., Consolidated Framework for Implementation Research [57], Theoretical Domains Framework [58]). Therefore, as more projects align to the MMCS steps [1] to identify factors related to implementation and sustainability, better comparisons, consolidations, and transfers of knowledge between projects may become possible.
This project has several limitations. First, the high, medium, and low sustainability assigned to the sites were based on the sites’ CCM sustainability relative to one another, rather than based on an external metric of sustainability. As measures of sustainability such as the Program Sustainability Assessment Tool [59, 60] and the Sustainment Measurement System Scale [61] become increasingly developed and tested, future projects may consider the feasibility of incorporating such measures to assess each site’s sustainability. In our case, we worked on addressing this limitation by using a consensus approach within our project team to assign sustainability levels to sites, as well as by confirming that the sites that we designated as high sustainability exhibited CCM elements that we had previously observed at the end of their participation in the original CCM implementation trial [19]. Second, we did not assign strict thresholds above/below which the counts or proportions of data regarding a factor would automatically indicate whether the factor (i) was present, somewhat present, or minimally present and (ii) had an enabling, hindering, or neutral/unclear influence on sustainability. This follows widely accepted qualitative analytical guidance that discourages characterizing findings solely based on the frequency with which a notion is mentioned by participants [62,63,64], in order to prevent unsubstantiated inferences or conclusions. We sought to address this limitation in two ways: We carefully documented the project team’s rationale for each consensus reached, and we reviewed all consensuses reached in their entirety to ensure that any two factors with the same designation (e.g., “minimally present”) do not have associated rationale that conflict across those factors. These endeavors we undertook closely adhere to established case study research methods [65], which MMCS builds on, that emphasize strengthening the validity and reliability of findings through documenting a detailed analytic protocol, as well as reviewing data to ensure that patterns match across analytic units (e.g., factors, interviewees, sites). Third, our findings are based on three sites each for high/medium/low sustainability, and although we identified single factors associated with sustainability, we found no specific combinations of factors’ presence and influence that were repeatedly existent at a majority of the sites designated as high/medium/low sustainability. Examining additional sites on the factors identified through this work (as we will for our subsequent CCM implementation trial described below) will allow more opportunities for repeated combinations and other factors to emerge, making possible firmer conclusions regarding the extent to which the currently identified factors and absence of identified combinations are applicable beyond the sites included in this study. Fourth, the identified influencing factor “leadership support for CCM” (under the Context domain of the i-PARIHS framework) substantially overlaps in concept with the core “organizational/leadership support” element of the CCM. To avoid circular reasoning, we used leadership support-related data to inform our assignment of sites’ high, medium, or low CCM sustainability, rather than as a reason for the sites’ CCM sustainability. In reality, strong leadership support may both result from and contribute to implementation and sustainability [16, 66], and thus causal relationships between the i-PARIHS-aligned influencing factors and the CCM elements (possibly with feedback loops) warrant further examination to most appropriately use leadership support-related data in future analyses of CCM sustainability. Fifth, findings may be subject to both social desirability bias in participants providing more positive than negative evidence of sustainability (especially participants who are responsible for implementing and sustaining CCM-aligned care at their site) and the project team members’ bias in interpreting the findings to align to their expectations of further effort being necessary to sustainably implement the CCM. To help mitigate this challenge, the project interviewers strove to elicit from participants both positive and negative perceptions and experiences related to CCM-based care delivery, both of which were present in the examined interview data.
Future work stemming from this project is twofold. Regarding CCM implementation, we will conduct a subsequent CCM implementation trial involving eight new sites to prospectively examine how implementation facilitation with an enhanced focus on these findings affects CCM sustainability. We started planning for sustainability prior to implementation, looking to this work for indicators of specific modifications needed to the previous way in which we used implementation facilitation to promote the uptake of CCM-based care [67]. Findings from this work suggest that sustainability may be related most strongly to (i) provider collaboration, (ii) knowledge retention during staff/leadership transitions, and (iii) availability of skilled internal facilitators. Hence, we will accordingly prioritize developing procedures for (i) regular CCM-related information exchange amongst BHIP team members, as well as between the BHIP team and clinic leadership, (ii) both translating knowledge to and keeping knowledge documented at the site, and (iii) supporting the sites’ own personnel to take the lead in driving CCM implementation.
Regarding MMCS, we will continuously refine and improve the method by learning from other projects applying, testing, and critiquing MMCS. Outside of our CCM-related projects, examinations of implementation data using MMCS are actively underway for various implementation efforts including that of a data dashboard for decision support on transitioning psychiatrically stable patients from specialty mental health to primary care [2], a peer-led healthy lifestyle intervention for individuals with serious mental illness [3], screening programs for intimate partner violence [4], and a policy- and organization-based health system strengthening intervention to improve health systems in sub-Saharan Africa [5]. As MMCS is used by more projects that differ from one another in their specific outcome of interest, and especially in light of our MMCS application that examines factors related to sustainability, we are curious whether certain proximal to distal outcomes are more subject to heterogeneity in influencing factors than other outcomes. For instance, sustainability outcomes, which are tracked following a longer passage of time than some other outcomes, may be subject to more contextual variations that occur over time and thus could particularly benefit from being examined using MMCS. We will also explore MMCS’ complementarity with coincidence analysis and other configurational analytical approaches [68] for examining implementation phenomena. We are excited about both the step-by-step traceability that MMCS can bring to such methods and those methods’ computational algorithms that can be beneficial to incorporate into MMCS for projects with larger numbers of sites. For example, Salvati and colleagues [69] described both the inspiration that MMCS provided in structuring their data as well as how they addressed MMCS’ visualization shortcomings through their innovative data matrix heat mapping, which led to their selection of specific factors to include in their subsequent coincidence analysis. Coincidence analysis is an enhancement to qualitative comparative analysis and other configurational analytical methods, in that it is formulated specifically for causal inference [70]. Thus, in considering improved reformulations of MMCS’ steps to better characterize examined factors as explicit causes to the outcomes of interest, we are inspired by and can draw on coincidence analysis’ approach to building and evaluating causal chains that link factors to outcomes. Relatedly, we have begun to actively consider the potential contribution that MMCS can make to hypothesis generation and theory development for implementation science. As efforts to understand the mechanisms through which implementation strategies work are gaining momentum [71,72,73], there is an increased need for methods that help decompose our understanding of factors that influence the mechanistic pathways from strategies to outcomes [74]. Implementation science is facing the need to develop theories, beyond frameworks, which delineate hypotheses for observed implementation phenomena that can be subsequently tested [75]. The methodical approach that MMCS offers can aid this important endeavor, by enabling data curation and examination of pertinent factors in a consistent way that allows meaningful synthesis of findings across sites and studies. We see these future directions as concrete steps toward elucidating the factors related to sustainable implementation of EBPs, especially leveraging data from projects where the number of sites is much smaller than the number of factors that may matter—which is indeed the case for most implementation projects.
Conclusions
Using MMCS, we found that provider collaboration, knowledge retention during staff/leadership transitions, and availability of skilled internal facilitators may be most strongly related to CCM sustainability in VA outpatient mental health clinics. Informed by these findings, we have a subsequent CCM implementation trial underway to prospectively test whether increasing the aforementioned factors within implementation facilitation enhances sustainability. The MMCS steps used here for systematic multi-site examination can also be applied to determining sustainability-related factors relevant to various other EBPs and implementation contexts.
Availability of data and materials
The data analyzed during the current project are not publicly available because participant privacy could be compromised.
Abbreviations
- BHIP:
-
Behavioral Health Interdisciplinary Program
- CCM:
-
Collaborative Chronic Care Model
- COREQ:
-
Consolidated Criteria for Reporting Qualitative Research
- COVID:
-
coronavirus disease
- EBP:
-
evidence-based practice
- IRB:
-
Institutional Review Board
- i-PARIHS:
-
Integrated Promoting Action on Research Implementation in Health Services
- MMCS:
-
Matrixed Multiple Case Study
- VA:
-
United States Department of Veterans Affairs
References
Kim B, Sullivan JL, Ritchie MJ, Connolly SL, Drummond KL, Miller CJ, et al. Comparing variations in implementation processes and influences across multiple sites: What works, for whom, and how? Psychiatry Res. 2020;283:112520.
Hundt NE, Yusuf ZI, Amspoker AB, Nagamoto HT, Kim B, Boykin DM, et al. Improving the transition of patients with mental health disorders back to primary care: A protocol for a partnered, mixed-methods, stepped-wedge implementation trial. Contemp Clin Trials. 2021;105:106398.
Tuda D, Bochicchio L, Stefancic A, Hawes M, Chen J-H, Powell BJ, et al. Using the matrixed multiple case study methodology to understand site differences in the outcomes of a Hybrid Type 1 trial of a peer-led healthy lifestyle intervention for people with serious mental illness. Transl Behav Med. 2023;13(12):919–27.
Adjognon OL, Brady JE, Iverson KM, Stolzmann K, Dichter ME, Lew RA, et al. Using the Matrixed Multiple Case Study approach to identify factors affecting the uptake of IPV screening programs following the use of implementation facilitation. Implement Sci Commun. 2023;4(1):145.
Seward N, Murdoch J, Hanlon C, Araya R, Gao W, Harding R, et al. Implementation science protocol for a participatory, theory-informed implementation research programme in the context of health system strengthening in sub-Saharan Africa (ASSET-ImplementER). BMJ Open. 2021;11(7):e048742.
Bauer MS, Miller C, Kim B, Lew R, Weaver K, Coldwell C, et al. Partnering with health system operations leadership to develop a controlled implementation trial. Implement Sci. 2016;11:22.
Bauer MS, Miller CJ, Kim B, Lew R, Stolzmann K, Sullivan J, et al. Effectiveness of implementing a Collaborative Chronic Care Model for clinician teams on patient outcomes and health status in mental health: a randomized clinical trial. JAMA Netw Open. 2019;2(3):e190230.
Ritchie MJ, Dollar KM, Miller CJ, Smith JL, Oliver KA, Kim B, et al. Using Implementation Facilitation to Improve Healthcare (Version 3): Veterans Health Administration, Behavioral Health Quality Enhancement Research Initiative (QUERI). 2020.
Bauer MS, Stolzmann K, Miller CJ, Kim B, Connolly SL, Lew R. Implementing the Collaborative Chronic Care Model in mental health clinics: achieving and sustaining clinical effects. Psychiatr Serv. 2021;72(5):586–9.
Miller CJ, Kim B, Connolly SL, Spitzer EG, Brown M, Bailey HM, et al. Sustainability of the Collaborative Chronic Care Model in outpatient mental health teams three years post-implementation: a qualitative analysis. Adm Policy Ment Health. 2023;50(1):151–9.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Von Korff M, Gruman J, Schaefer J, Curry SJ, Wagner EH. Collaborative management of chronic illness. Ann Intern Med. 1997;127(12):1097–102.
Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74(4):511–44.
Coleman K, Austin BT, Brach C, Wagner EH. Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009;28(1):75–85.
Connolly SL, Sullivan JL, Ritchie MJ, Kim B, Miller CJ, Bauer MS. External facilitators’ perceptions of internal facilitation skills during implementation of collaborative care for mental health teams: a qualitative analysis informed by the i-PARIHS framework. BMC Health Serv Res. 2020;20(1):165.
Kim B, Sullivan JL, Drummond KL, Connolly SL, Miller CJ, Weaver K, et al. Interdisciplinary behavioral health provider perceptions of implementing the Collaborative Chronic Care Model: an i-PARIHS-guided qualitative study. Implement Sci Commun. 2023;4(1):35.
Harvey G, Kitson A. PARIHS revisited: from heuristic to integrated framework for the successful implementation of knowledge into practice. Implement Sci. 2016;11:33.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Sullivan JL, Kim B, Miller CJ, Elwy AR, Drummond KL, Connolly SL, et al. Collaborative Chronic Care Model implementation within outpatient behavioral health care teams: qualitative results from a multisite trial using implementation facilitation. Implement Sci Commun. 2021;2(1):33.
Miller CJ, Sullivan JL, Kim B, Elwy AR, Drummond KL, Connolly S, et al. Assessing collaborative care in mental health teams: qualitative analysis to guide future implementation. Adm Policy Ment Health. 2019;46(2):154–66.
Miles MB, Huberman AM. Qualitative data analysis: an expanded sourcebook: sage. 1994.
Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311(7001):376–80.
Bens I. Facilitating with Ease!: core skills for facilitators, team leaders and members, managers, consultants, and trainers. Hoboken: John Wiley & Sons; 2017.
Ritchie MJ, Drummond KL, Smith BN, Sullivan JL, Landes SJ. Development of a qualitative data analysis codebook informed by the i-PARIHS framework. Implement Sci Commun. 2022;3(1):98.
Excel: Microsoft. Available from: https://www.microsoft.com/en-us/microsoft-365/excel. Accessed 15 Feb 2024.
Madrigal L, Manders OC, Kegler M, Haardörfer R, Piper S, Blais LM, et al. Inner and outer setting factors that influence the implementation of the National Diabetes Prevention Program (National DPP) using the Consolidated Framework for Implementation Research (CFIR): a qualitative study. Implement Sci Commun. 2022;3(1):104.
Wilson HK, Wieler C, Bell DL, Bhattarai AP, Castillo-Hernandez IM, Williams ER, et al. Implementation of the Diabetes Prevention Program in Georgia Cooperative Extension According to RE-AIM and the Consolidated Framework for Implementation Research. Prev Sci. 2023;Epub ahead of print.
Proctor E, Luke D, Calhoun A, McMillen C, Brownson R, McCrary S, et al. Sustainability of evidence-based healthcare: research agenda, methodological advances, and infrastructure support. Implement Sci. 2015;10:88.
Fathi LI, Walker J, Dix CF, Cartwright JR, Joubert S, Carmichael KA, et al. Applying the Integrated Sustainability Framework to explore the long-term sustainability of nutrition education programmes in schools: a systematic review. Public Health Nutr. 2023;26(10):2165–79.
Guptill J. Knowledge management in health care. J Health Care Finance. 2005;31(3):10–4.
Gammelgaard J. Why not use incentives to encourage knowledge sharing. J Knowledge Manage Pract. 2007;8(1):115–23.
Liebowitz J. Knowledge retention: strategies and solutions. Boca Raton: CRC Press; 2008.
Ensslin L, CarneiroMussi C, RolimEnsslin S, Dutra A, Pereira Bez Fontana L. Organizational knowledge retention management using a constructivist multi-criteria model. J Knowledge Manage. 2020;24(5):985–1004.
Peterson AE, Bond GR, Drake RE, McHugo GJ, Jones AM, Williams JR. Predicting the long-term sustainability of evidence-based practices in mental health care: an 8-year longitudinal analysis. J Behav Health Serv Res. 2014;41(3):337–46.
Miller CJ, Griffith KN, Stolzmann K, Kim B, Connolly SL, Bauer MS. An economic analysis of the implementation of team-based collaborative care in outpatient general mental health clinics. Med Care. 2020;58(10):874–80.
Silver SA, Harel Z, McQuillan R, Weizman AV, Thomas A, Chertow GM, et al. How to begin a quality improvement project. Clin J Am Soc Nephrol. 2016;11(5):893–900.
Dixon-Woods M. How to improve healthcare improvement-an essay by Mary Dixon-Woods. BMJ. 2019;367:l5514.
Miller CJ, Kim B, Silverman A, Bauer MS. A systematic review of team-building interventions in non-acute healthcare settings. BMC Health Serv Res. 2018;18(1):146.
Robert G, Greenhalgh T, MacFarlane F, Peacock R. Organisational factors influencing technology adoption and assimilation in the NHS: a systematic literature review. Report for the National Institute for Health Research Service Delivery and Organisation programme. London; 2009.
Kelly CJ, Young AJ. Promoting innovation in healthcare. Future Healthc J. 2017;4(2):121–5.
Aarons GA, Ehrhart MG, Farahnak LR, Hurlburt MS. Leadership and organizational change for implementation (LOCI): a randomized mixed method pilot study of a leadership and organization development intervention for evidence-based practice implementation. Implement Sci. 2015;10:11.
Ritchie MJ, Parker LE, Kirchner JE. Facilitating implementation of primary care mental health over time and across organizational contexts: a qualitative study of role and process. BMC Health Serv Res. 2023;23(1):565.
van den Hoed MW, Backhaus R, de Vries E, Hamers JPH, Daniëls R. Factors contributing to innovation readiness in health care organizations: a scoping review. BMC Health Serv Res. 2022;22(1):997.
Melnyk BM, Hsieh AP, Messinger J, Thomas B, Connor L, Gallagher-Ford L. Budgetary investment in evidence-based practice by chief nurses and stronger EBP cultures are associated with less turnover and better patient outcomes. Worldviews Evid Based Nurs. 2023;20(2):162–71.
Jacob RR, Parks RG, Allen P, Mazzucca S, Yan Y, Kang S, et al. How to “start small and just keep moving forward”: mixed methods results from a stepped-wedge trial to support evidence-based processes in local health departments. Front Public Health. 2022;10:853791.
Aarons GA, Conover KL, Ehrhart MG, Torres EM, Reeder K. Leader-member exchange and organizational climate effects on clinician turnover intentions. J Health Organ Manag. 2020;35(1):68–87.
Kirchner JE, Ritchie MJ, Pitcock JA, Parker LE, Curran GM, Fortney JC. Outcomes of a partnered facilitation strategy to implement primary care-mental health. J Gen Intern Med. 2014;29 Suppl 4(Suppl 4):904–12.
Strategy Design: CFIR research team-center for clinical management research. Available from: https://cfirguide.org/choosing-strategies/. Accessed 15 Feb 2024.
Kim B, Wilson SM, Mosher TM, Breland JY. Systematic decision-making for using technological strategies to implement evidence-based interventions: an illustrated case study. Front Psychiatry. 2021;12:640240.
Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. 2013;8:139.
Lewis CC, Scott K, Marriott BR. A methodology for generating a tailored implementation blueprint: an exemplar from a youth residential setting. Implement Sci. 2018;13(1):68.
Maher C, Hadfield M, Hutchings M, de Eyto A. Ensuring rigor in qualitative data analysis: a design research approach to coding combining NVivo with traditional material methods. Int J Qual Methods. 2018;17(1):1609406918786362.
Holloway I. A-Z of qualitative research in healthcare. 2nd ed. Oxford: Wiley-Blackwell; 2008.
Reproducibility and Replicability in Research: National Academies. Available from: https://www.nationalacademies.org/news/2019/09/reproducibility-and-replicability-in-research. Accessed 15 Feb 2024.
Chinman M, Acosta J, Ebener P, Shearer A. “What we have here, is a failure to [Replicate]”: ways to solve a replication crisis in implementation science. Prev Sci. 2022;23(5):739–50.
Vicente-Saez R, Martinez-Fuentes C. Open Science now: a systematic literature review for an integrated definition. J Bus Res. 2018;88:428–36.
Consolidated Framework for Implementation Research: CFIR Research Team-Center for Clinical Management Research. Available from: https://cfirguide.org/. Accessed 15 Feb 2024.
Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77.
Luke DA, Calhoun A, Robichaux CB, Elliott MB, Moreland-Russell S. The Program Sustainability Assessment Tool: a new instrument for public health programs. Prev Chronic Dis. 2014;11:130184.
Calhoun A, Mainor A, Moreland-Russell S, Maier RC, Brossart L, Luke DA. Using the Program Sustainability Assessment Tool to assess and plan for sustainability. Prev Chronic Dis. 2014;11:130185.
Palinkas LA, Chou CP, Spear SE, Mendon SJ, Villamar J, Brown CH. Measurement of sustainment of prevention programs and initiatives: the sustainment measurement system scale. Implement Sci. 2020;15(1):71.
Sandelowski M. Real qualitative researchers do not count: the use of numbers in qualitative research. Res Nurs Health. 2001;24(3):230–40.
Wood M, Christy R. Sampling for Possibilities. Qual Quant. 1999;33(2):185–202.
Chang Y, Voils CI, Sandelowski M, Hasselblad V, Crandell JL. Transforming verbal counts in reports of qualitative descriptive studies into numbers. West J Nurs Res. 2009;31(7):837–52.
Yin RK. Case study research and applications. Los Angeles: Sage; 2018.
Bauer MS, Weaver K, Kim B, Miller C, Lew R, Stolzmann K, et al. The Collaborative Chronic Care Model for mental health conditions: from evidence synthesis to policy impact to scale-up and spread. Med Care. 2019;57 Suppl 10 Suppl 3(10 Suppl 3):S221-s7.
Miller CJ, Sullivan JL, Connolly SL, Richardson EJ, Stolzmann K, Brown ME, et al. Adaptation for sustainability in an implementation trial of team-based collaborative care. Implement Res Pract. 2024;5:26334895231226197.
Curran GM, Smith JD, Landsverk J, Vermeer W, Miech EJ, Kim B, et al. Design and analysis in dissemination and implementation research. In: Brownson RC, Colditz GA, Proctor EK, editors. Dissemination and Implementation Research in Health: Translating Science to Practice. 3 ed. New York: Oxford University Press; In press.
Salvati ZM, Rahm AK, Williams MS, Ladd I, Schlieder V, Atondo J, et al. A picture is worth a thousand words: advancing the use of visualization tools in implementation science through process mapping and matrix heat mapping. Implement Sci Commun. 2023;4(1):43.
Whitaker RG, Sperber N, Baumgartner M, Thiem A, Cragun D, Damschroder L, et al. Coincidence analysis: a new method for causal inference in implementation science. Implement Sci. 2020;15(1):108.
Lewis CC, Powell BJ, Brewer SK, Nguyen AM, Schriger SH, Vejnoska SF, et al. Advancing mechanisms of implementation to accelerate sustainable evidence-based practice integration: protocol for generating a research agenda. BMJ Open. 2021;11(10):e053474.
Kilbourne AM, Geng E, Eshun-Wilson I, Sweeney S, Shelley D, Cohen DJ, et al. How does facilitation in healthcare work? Using mechanism mapping to illuminate the black box of a meta-implementation strategy. Implement Sci Commun. 2023;4(1):53.
Kim B, Cruden G, Crable EL, Quanbeck A, Mittman BS, Wagner AD. A structured approach to applying systems analysis methods for examining implementation mechanisms. Implementation Sci Commun. 2023;4(1):127.
Geng EH, Baumann AA, Powell BJ. Mechanism mapping to advance research on implementation strategies. PLoS Med. 2022;19(2):e1003918.
Luke DA, Powell BJ, Paniagua-Avila A. Bridges and mechanisms: integrating systems science thinking into implementation research. Annu Rev Public Health. In press.
Acknowledgements
The authors sincerely thank the project participants for their time, as well as the project team members for their guidance and support. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Funding
This project was funded by VA grant QUE 20–026 and was designed and conducted in partnership with the VA Office of Mental Health and Suicide Prevention.
Author information
Authors and Affiliations
Contributions
Concept and design: BK, JS, and CM. Acquisition, analysis, and/or interpretation of data: BK, JS, MB, SC, ES, and CM. Initial drafting of the manuscript: BK. Critical revisions of the manuscript for important intellectual content: JS, MB, SC, ES, HB, LS, KW, and CM. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project was determined to be non-research by the VA Boston Research and Development Service, and therefore did not require oversight by the Institutional Review Board (IRB).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
COREQ (COnsolidated criteria for REporting Qualitative research) Checklist.
Additional file 2.
Data input, tasks performed, and analysis output for MMCS Steps 5 through 9.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, B., Sullivan, J.L., Brown, M.E. et al. Sustaining the collaborative chronic care model in outpatient mental health: a matrixed multiple case study. Implementation Sci 19, 16 (2024). https://doi.org/10.1186/s13012-024-01342-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13012-024-01342-2